Embed Size (px)
Citation preview

Influence of infection on patent ductus arteriosus and chronic lung disease in premature infants weighing 1000 grams er less
AIvaro Gonzalez, MD, a Ilene R, S. Sesenko, MD, Jay Chandar , MD, Helmut Hummler, MD, Nelson Claure, MS, and Eduardo Bancalari, MD
From the Department of Pediatrics, Divisions of Neonatology and Pediatric Cardiology, University of Miami School of Medicine, Miami, Florida
Objective: To test the hypotheses that (I) infection increases ductal dilatory pros- taglandins and infiammatory mediators that may influence the closure of a patent ductus arteriosus (PDA), increasing the incidence of late episodes of PDA (after 7 days) and the rate of closure failures, and (2) the concurrence of PDA and infec- tion increases the risk of chronic lung disease (CLD). Methods: One hundred fourteen premature infants (birth weight, 500 to 1000 gm) were prospectively assessed for PDA and infection. Serum levels of 6-ketopros- taglandin FI« and tumor necrosis factor alpha were measured routinely in all in- fants and when PDA or infection was present. Multivariate assessment of risk fac- tors for PDA closure failure and for CLD was done by Iogistic regression, and expressed as an odds ratio and as 95% confidence intervals. Results: Late PDA episodes were more frequent in infants with infection than in those without infection. A temporally related infection (<5 days between both di- agnoses) was associated with an increased risk of PDA closure failure (odds ratio, 19. I [confidence interval, 4 to 90]). In addition to birth weight and the severity of initial respiratory failure, PDA and infection increased the risk of CLD (odds ratio, 11.7 [confidence interval, 1.7 to 81] for PDA; odds ratio, 3.1 [confidence interval, I to 1 I] for infection). Furthermore, when both factors were temporally related, they further increased the risk of CLD (odds ratio, 29.6 (confidence interval, 4.5 to >100]). Infants with infection and those with PDA had higher levels of 6-ketopros- taglandin F ic than did control subjects. Levels of tumor necrosis factor alpha were also elevated in infants with infection and in those with late PDA. Conclusions: Infection adversely influences PDA outcome by increasing the risk of late ductal reopening and PDA closure failures. Increased levels of prostaglan- dins and tumor necrosis factor alpha in infants with infection may explain the poor PDA outcome. The concurrence of PDA and infection potentiates their negative effects on the risk of CLD. (J PEDIATR 1996;128:470-8)
Partially supported by University of Miami Project: New Bom, and by a National Institutes of Health-Biomedical Research Support Grant Shared Instrumentation Grant, "Ultrasonographic Imaging System With Color-Flow Doppler" (grant No. 1 S 10 RR06523-01). Presented in part at the annual meeting of the Society for Pediatric Research, San Diego, Calif., May 1995. Submitted for publication Aug. 17, 1995; accepted Jan. 3, 1996.
Reprint requests: Eduardo Bancalari, MD, Department of Pediatrics (R131), Division of Neonatology, PO Box 016960, Miami, FL 33101.
apresenüy at the Catholic University of Chile, Santiago.
Copyright © 1996 by Mosby-Year Book, Inc.
0022-3476/96/$5.00 + 0 9/20/71604
4 7 0

The Journal of Pediatrics Gonzalez et al. 4 7 1 Volume 128, Number 4
Patent ductus arteriosus and infections are frequent clinical events in preterm infants, 1-3 and because of their high prev- alence, it is reasonable to question whether a relationship is present between both complications. We have reported an epidemiologic association of these two events with the de- velopment of chronic lung disease in premature infants, and an apparent interaction when both factors are present simul- taneously. 4 Among the possible explanations for this poten- tial interaction is that infections may increase prostaglandin levels along with other inflammatory mediators, 5, 6 thus fa- voring persistent ductal patency or reopening.
We undertook the present study specifically to test the hypothesis that the presence of infection in the premature infant increases ductal dilatory prostaglandins (prostacyclin) and inflammatory mediators (e.g., tumor necrosis factor al- pha) that may negatively modify the outcome of the PDA and therefore increase the incidence of late-onset PDA (after 7 days) and ductal recurrences, and increase the rate
CLD Chronic lung disease 6-keto-PGFlc, 6-Ketoprostaglandin Flc, PDA Patent ductus arteriosus RDS Respiratory distress syndrome TNFet Tumor necrosis factor alpha
of PDA closure failures after treatment. Furthermore, we hypothesized that the concurrence of PDA and infection has a deleterious effect on the evolution of the infants' respira- tory course, and results in an increased incidence of CLD.
METItODS Study patients. We prospectively assessed consecutively
born preterm infants with birth weights between 500 and 1000 gm delivered at the University of Miami/Jackson Me- morial Medical Center between November 1992 and March 1994. Excluded from the study were patients with congen- ital anomalies, congenital infections, and intrauterine growth retardation, and infants who died during the first 72 hours after birth. The protocol was approved by the University of Miami Committee for the Protection of Human Subjects, and informed consent was obtained from the parents.
PDA surveillanee, diagnosis, and treatment. The pres- ence of PDA was determined in all infants by two- dimensional color-Doppler echocardiograms obtalned rou- tinely between days 3 and 5 after birth. A second evaluation was performed between days 15 and 20 regardless of clin- ical status. These studies were performed with a Toshiba 270-SSA ultrasonographic system with color-flow Doppler (Toshiba Medical Co., Ltd., Tokyo, Japan). Infants were ex- amined at least daily for clinical signs of PDA, and additional echocardiograms were obtained if PDA was suspected on the basis of one of the following criteria: (1) the presence of a systolic or continuous heart murmur and (2) the presence of
at least two of the following clinical signs: hyperactive pre- cordium, bounding pulses, wide pulse pressure (>25 mm Hg), persistent tachycardia (heart rate >160 beats/min), and radiographic evidence of pulmonary edema or cardiomeg- aly. Symptomatic PDA was diagnosed when there was echocardiographic evidence of left-to-right shunting through the ductus arteriosus associated with at least one of the clin- ical criteria. To evaluate the relationship between infection and PDA development, we obtained additional echocardio- grams of infants with proven or suspected infection within 72 hours of the initial clinical diagnosis.
Infants with symptomatic PDA received the usual in- domethacin treatment as described previously. 4 A follow-up echocardiogram was obtalned when infants received in- domethacin, between 48 and 72 hours after this therapy was started. Ifthe PDA remalned open according to the echocar- diographic evaluation done after the first course of in- domethacin, a second course was given and the echocardio- gram was repeated every 48 to 72 hours until closure was documented. If there was no PDA closure after the second course of indomethacin, surgical ligation was considered. Surgery was also performed in infants with symptomatic PDA in whom indomethacin was contraindicated.
Infeetion surveillance and diagnosis. Patients were also examined closely for signs of infection. Infection was diag- nosed when the three following criteria were met: (1) a pos- itive result on at least one blood, cerebrospinal fluid, or su- prapubic urine culture, (2) association with one or more of six clinical signs (arterial hypotension, hypothermia, apnea, respiratory deterioration, lethargy, and hypotonia)and blood cell count changes (leukocytosis, with a leukocyte count >25 x 109/L [>25,000/mm3]; leukopenia, with a leukocyte count <7.5 x 109/L [<7500/mm3]; increase in the proportion of immature forms [immature/mature granulocyte ratio >0.3]; or thrombocytopenia, with a platelet count < 100 x 109/ L [<100,000/mm3]), and (3) conviction of the clinical team caring for the infant of the diagnosis of infection, resulting in the infant's receiving antibiotics for at least 7 days. We attempted to document more than one positive blood culture result in these infants, especially if a Staphylococcus epider- midis was identified. Symptom-free infants with a single blood culture positive for S. epidermidis were not considered infected. Infants with two or more blood cultures positive for the same microorganism were considered infected regardless of symptoms. Infants for whom the diagnosis of infection was not conclusive (i.e., infants with an isolated blood cul- ture positive for S. epidermidis but without symptoms, as weil as infants with clinical signs of infection but negative culture results) were excluded from the analyses.
Inf lammatory mediators. Blood samples for levels of 6-ketoprostaglandin FI~, a stable metabolite of the ductal vasodilator prostacyclin, and for levels of tumor necrosis

4 7 2 Gonzalez et al. The Journal of Pediatrics April 1996
factor alpha were drawn in three clinical situations: (1) when an infant had clinical signs of infection (initial samples drawn along with diagnostic blood samples for culture, fol- low-up samples drawn 7 days after antibiotic therapy was initiated), (2) when PDA was diagnosed (samples drawn be- fore and then 3 and 7 days after indomethacin treatment), (3) when an infant (control subject) had neither infection nor PDA (samples drawn simultaneously with routine echocar- diographic evaluations, the first between days 3 and 5 and the second between days 15 and 20 after birth). Blood sam- ples (0.6 tal) were coUected and immediately decanted into chilled tubes that contained indomethacin and ethylenedi- aminetetraacetic acid, and then centrifuged at 2000g for 15 minutes. The plasma was separated and stored at -70 ° C for later radioimmunoassay. Specific radioimmunoassay kits were used to measure 6-keto-PGFl« (Advanced Magnetics, Inc., Cambridge, Mass.), and TNF« (Medgenix, Brussels, Belgium).
Data collection and end points. We collected general clinical data, including matemal history, the presence of complications associated with prematurity, and possible confounding variables such as medications, and fluid man- agement, as weil as respiratory data on each patient. All in- formation was entered into a computerized database for subsequent analysis.
For each PDA episode, the following variables were an, alyzed and related to the presence or absence of infection: (1) fallure of closure, if the PDA remalned open by echocar- diography for at least 10 days or required surgical ligation because of unresponsiveness or contraindication of in- domethacin therapy, (2) recurrence of PDA (appearance of clinical and echocardiographic signs of PDA after it had closed), (3) early PDA (occurrence during the first 7 days after birth), and (4) late PDA (appearance after the first week after birth). For the purpose of the analysis we defined a temporal relation between infection and PDA as infection preceding the PDA diagnosis or developing while the duc- tus was symptomatic, with a time interval no longer than 5 days between both diagnoses.
Chronic lung disease was defined as the need for supple- mental oxygen for 28 days or longer dunng the first 2 months of life, in association with persistent chest radiographic findings.
Statistical analysis. To examine whether infections were associated with failure Of PDA closure, we estimated that the sample should comprise 31 patients with PDA and tempo- rally related infection, and 31 with PDA and without infec- tion to achieve a power of 80% at a level o fp = 0.05, with an expected increase in the fallure rate from 30% to 65% when infection was present. These calculations were based on data of previous years. The observed PDA incidence was 60% in infants weighing less than 1000 gm (45% in infants
without infection, 75% in infants with infection), and the observed closure failure rate was 43% (24% in infants with- out infection, 68% in infants with infection). On the basis o f these numbers, a total of 110 patients were needed to be en- rolled in the study, 41 with infection (with the expectation that 75% [31 infants] would have PDA) and 69 without in- fection (with the expectation that 45% [31 infants] would have PDA).
Categorical variables were analyzed with the chi-square test, the Malm-Whitney rank-sum test, and the Mantel- Haenszel test when it was necessary to adjust for birth weight. Differences in continuous variables were assessed by the Student t test and analysis of variance. Statistical signif- icance was considered as p less than 0.05.
To define the role of specific factors that may affect PDA closure and the development of CLD, we performed multi- variate analyses. For this step we used backward Stepwise Logistic Regression Analysis (BMDP statistical software, University of Califomia, Los Angeles). 7 The initial model for failure of PDA closure included the following variables: birth weight, gender, race, postnatal age, Apgar score, incomplete or no indomethacin course given, excessive fluid intake (>140 ml/kg per day during the first 2 weeks after birth), and the presence of a temporally related infection. The model for CLD included the following variables: birth weight, gender, race, Apgar score, severity of initial RDS (based on the mean of the product of the mean airway pres- sure multiplied by the fraction of inspired oxygen during the first 3 days after birth) of 2.4 or more, excessive fluid intake, the presence of air leak (pneumothorax or pulmonary inter- stifial emphysema), severe intracranial hemorrhage (grades III and IV), episodes of infection, and PDA. Another logis- tic model was used to analyze the temporal interaction be- tween PDA and infection and the development of CLD, which, in addition to considering the significant variables selected in the previous step, included the following four categories: no PDA or infection, PDA temporally related to infection, PDA not temporally related to infection, and in- fection alone.
R E S U L T S
Patient population. A total of 172 infants with birth weights between 500 and 1000 gm were bom during the study period. Of these, 23 infants (13%) died during the first 72 hours and 12 infants met other exclusion criteria. For 23 (17%) of 137 eligible infants, we were unable to obtain con- sent. Therefore 114 infants were included in the final anal- ysis.
PDA outcome. Of the 114 infants analyzed, symptomatic PDA was diagnosed in 84 infants (74%). Of these 84 infants with symptomatic PDA, 43 (51%) had late PDA episodes (after the first week of life); in addition, of these 84 infants,

The Journal of Pediatrics Gonzalez et al. 4 7 3 Volume 128, Number 4
100
Z ~ 80
W ,~ 60
LL 0 UJ 40 o Z IJJ E3 20 o Z
O ~ / y
2/2
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9/14 4/6 4/6
3/13
BIRTH WEIGHT (g)
P < 0.025 MANTEL-HAENSZEL TES
Figù 1. Incidence of late episodes of PDA in relation to the presence of infection. Comparison of infants with proven in- fection during the first month versus infants without infection. Infants with doubtful infections, as well as those whose PDAs underwent ligation during the first week, and those who died were not included in this analysis.
Table . Odds ratio for failure of PDA closure
Variable OR 95% CI p
Birth weight --<-750 gm 2.84 1.5-5.6 <0.001 Infection temporally related 19.1 4 . 0 - 9 0 <0.001 High fluid intake 4.7 0.8-26.7 0.06 Incomplete or no indomethacin 4.1 0.5-32.5 0.15 PDA at >-8 days 5.6 1.0-31.9 <0.04
OR, Odds ratio; CI, confidence interval.
68 (81%) had their PDA closed initially with indomethacin, whereas 16 required ligation either because of failure of PDA closure after indomethacin therapy or because indomethacin therapy was contraindicated. Of the 68 infants whose PDA initially closed with indomethacin, 36 (53%) had a reopen- ing of their PDA. Of these 36 infants whose PDA reopened, 16 responded to a repeated indomethacin course, followed by PDA closure, whereas 20 required surgical ligation (be- cause of failure of indomethacin therapy or contraindication to indomethacin therapy).
Influenee of infeetion on PDA outeome. Of the 114 in- fants studied, 40 infants (36%) had the diagnosis ofinfection. Thirty-eight infants (33%) had both conditions, infection and PDA, and in 31 these two events were temporally related. The majority of these 31 episodes of infection temporally
retated to PDA (77%) preceded the diagnosis of PDA or oc- curred on the same day.
Among all cultures with positive results, the most com- mon microorganisms isolated were S. epidermidis, 25 (55%); Candida species, 15 (33%); group B streptococcus, 2 (4%); and gram-negative organisms, 3 (7%). Two infants had two episodes of infection, and three had cultures posi- tive for Candida and S. epidermidis simultaneously. Thirteen of the S. epidermidis infection episodes (52%) had two blood cultures with positive results.
Infants with a proven infection during the first month demonstrated a significantly higher incidence of late PDA episodes than did infants without evidence of infection, in- dependent of birth weight (Fig. 1). Similarly, those infants whose PDA was temporally related to an episode of infec- tion (31 infants) also had a significantly higher rate of PDA closure failure: 21 (68%) of 31 infants, compared with those infants with PDA but without infection (5 [17%] of 29 in- fants; p <0.02). Of the 21 infants with failure of PDA clo- sure associated with temporally related infection, 13 (62%) completed one or more indomethacin treatment courses without response, 3 received an incomplete course, and 5 did not receive indomethacin because of contraindications.
The multiple logistic regression analysis indicated that the presence of a temporally related infection was associated with a significant increase in the risk of failure of PDA clo-

4 7 4 Gonzalez et al. The Journal of Pediatrics April 1996
1000 T 700 t
E 4004-
o 100
o~ 80 Q. V
o 70 t -
O . 60 0
EL. 50
a_ 40 0
30 I 2O
( . 0 10
ù.
0 0
J J
OD OO
i ' !
° t D O
-" £ ICJgO ~ 0 ~
.¢
Controls Early PDA Laie PDA Infection median 14 59 64 82
(range) ( 4 - 7 8 ) ( 7 - 6 0 5 ) ( 2 9 - 1 0 0 0 ) ( 2 3 - 1 0 0 0 )
Fig. 2. Serum levels of 6-keto-PGFloL during PDA or infection episodes. Infants with either early or late episodes of PDA, as well as those with infection, had significantly higher levels than control subjects (* =p <0.05). The open squares rep- resent PDA episodes with a temporally related infection.
sure, independent of birth weight, postnatal age, indometha- cin use, fluid intake, and the remaining variables in the model. Birth weight and a postnatal age of PDA presenta- tion greater than or equal to 8 days were also significant variables (Table).
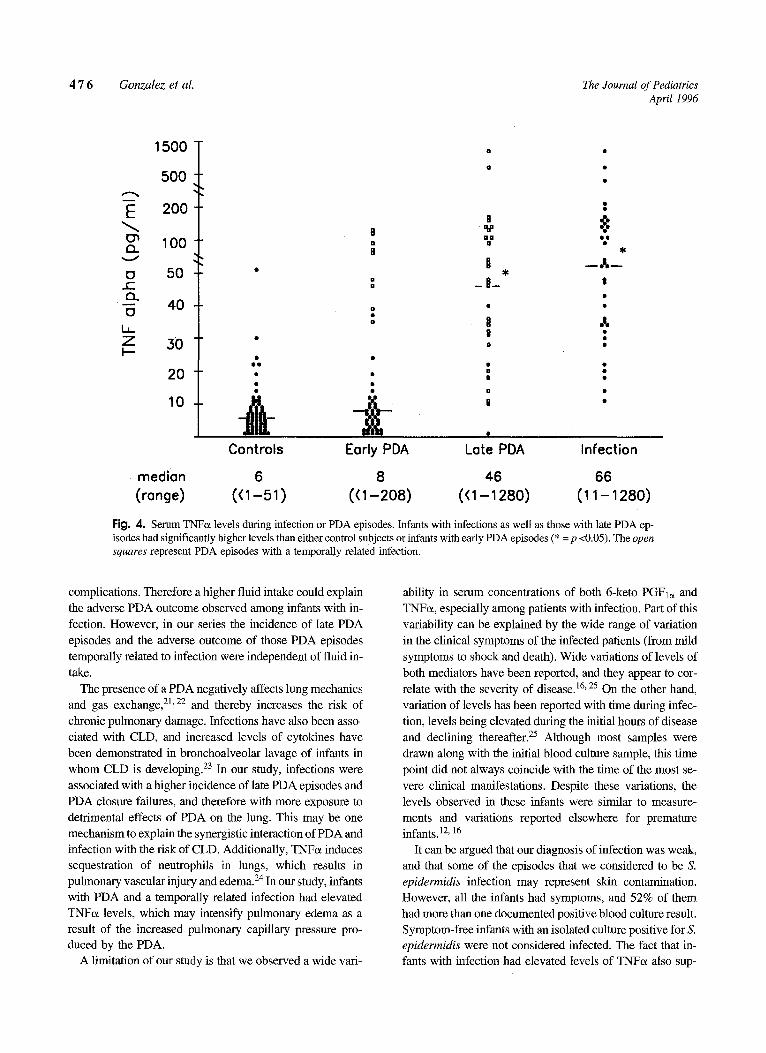
Levels of 6-keto PGFI« and TNFŒ levels. Infants with early or late episodes of PDA and those with infection had significantly higher levels of prostaglandins than control subjects had (Fig. 2). Infants with a PDA and a temporally related infection had significantly higher levels of prostag- landin than infants with PDA without infection (Fig. 2). Furthermore, even after indomethacin therapy and although prostaglandin levels decreased, the levels in these infants re- mained significantly elevated, whereas in infants with PDA without infection, prostaglandin levels decreased to values similar to those of control subjects (Fig. 3). TNF« levels were significantly increased in infants with infection and in those with late PDA epis0des, supporting the association between most late episodes of PDA and infection (Fig. 4). There was a significant positive correlation between pros- taglandin and TNF« levels in infants with infection (r = 0.72; p <0.01).
CLD end point. Of 105 infants who survived 28 or more days after birth, CLD developed in 46 (44%). Logistic
regression analysis showed that in addition to birth weight and the initial RDS severity, PDA (odds ratio, 11.7 [confi- dence interval, 1.7 to 81]) and infection (odds ratio, 3.1 [confidence interval, 1.0 to 10.6]) were associated with an increased risk of CLD after adjustment for the remaining variables in the model (Fig. 5). The subsequent model, which included interactions, showed that when PDA and infection were temporally related, they had a synergistic effect, potentiating their impact on the risk of CLD (odds ratio, 29.6 [confidence interval, 4.5 to >100]).
D I S C U S S I O N
This study indicates that systemic infections are associated with an adverse outcome of a PDA in small premature in- fants, leading to an increased risk of laie PDA episodes and medical-treatment closure failures. This, in turn, potentiates the impact of PDA on the risk of CLD damage, as shown by the higher levels of 6-keto PGFI« observed in infants with infection, which may be one mechanism that explains the poor PDA outcome. The higher TNF« levels observed in infants with laie PDA episodes also support the association of these episodes with infection.
There are several possible explanations for the interaction between infection and the ductus. Ductal tissue is sensitive

The Journal of Pediatrics Gonzalez et al. 4 7 5 Volume 128, Number 4
250
E
Q- 200
O
¢0 r'- 150 Q .
LL loo
I:L
0 ,4,--I
0 . ~ 50
I
PDA + Infection
Infection
Controls Pre Indo 72 h post Indo
Fi 9. 3. Serum levels of 6-keto-PGFl~ before (Pre lndo) and after (post Indo) indomethacin therapy, with comparison of infants with PDA with and without a temporally related infection. Values are means _+ SEM (* = p <0.05).
to the dilating effects of prostaglandins, 8' 9 and elevated lev- eis of prostaglandins have been associated with ductal patency in preterm infants, l°-12 In addition, levels of pros-
taglandins have been reported to increase in response to bacterial infections both in experimental animals and in hu- man amnion cells. 5,6,13 We observed elevated levels of 6-keto-PGFl« in infants with infection, and this finding was associated with an increased number of late PDA episodes and unresponsiveness to indomethacin therapy. That the prostaglandin levels remained elevated, despite indometha- cin use, in infants with PDA temporally related to infection may explain the unresponsiveness of PDA to therapy. The sensitivity of the ductal tissue to prostaglandins decreases with advancing postnatal age, therefore increasing the rate of unresponsiveness to indomethacin. 9, 14 Although most of the episodes of PDA temporally related to infection in our se- fies were late (after 7 days), the higher rate of closure failure in these episodes was independent of the postnatal age.
Other inflammatory mediators associated with infection may also play a role in ductal patency. TNFa is a well rec- ognized inflammatory cytokine, levels of which are elevated in systemic infections in human beings, including neo- nates.15, 16 As expected, we observed elevated levels of this cytokine in infants with infection. Elevated levels were also observed in infants with late episodes of PDA, which sup- ports the association of most of these episodes with infection. TNF« might also have a direct or indirect effect on ductal tissue, favoring its dilation and failure to respond to
cyclooxygenase inhibitors. TNFe~ induces several other in- flammatory factors in a complex cascade that, in mm, am- plifies its biologic effects. The list of TNFc~-inducible fac- tors is long and includes prostaglandins, endothelium- deilved factors, and reactive oxygen intermediates, 17 all of which might affect ductal closure.
Another possible explanation is that complications asso- ciated with infection, such as thrombocytopenia and renal failure, orten represent contraindications to indomethacin therapy and thereby interfere with the management of PDA. In this study, however, most infants with PDA temporally related to infection that failed to close received a complete indomethacin course. As the logistic regression demon- strated, the increased fisk of failure of PDA closure in in- fants with infection was independent of indomethacin use. Frequently surgery was delayed because of the infec- tion, resulting in a longer duration of PDA symptoms and therefore more exposure to its detrimental effects on the lung.
Indomethacin may increase the risk of infection 18' 19 and,
by this mechanism, may contribute to the interacUon between infection and PDA. In our seiles, however, most infections (77%) preceded the development of a PDA epi- sode or occurred simultaneously, making a significant impact on ductal outcome by this mechanism unlikely.
The detrimental effects of high fluid intake on PDA are weil established. 2° In addition, large amounts of fluids are offen part of infection treatment to reverse hemodynamic
4 7 6 Gonzalez et al. The Journal of Pediatrics April 1996
E cr~ El_
13 ..E El.
13 La_ 7 I --
1500
500
200
100
50
40
30
20
10
O0 ° •
0 •
0 •
Y =,= . ,
§ - - / , _ §_ II
a ,,,
• •
i I
Il •
B •
Controls Early PDA Lote PDA Infection
median 6 8 46 66 (range) ( (1 -51) ( (1 -208) ( (1 -1280) (11-1280)
Fig. 4. Serum TNFc~ levels during infection or PDA episodes. Infants with infections as weil as those with late PDA ep- isodes had significantly higher levels than either control subjects or infants with early PDA episodes (* = p <0.05). The open squares represent PDA episodes with a temporal!y related infection.
complications. Therefore a higher fluid intake could explain the adverse PDA outcome observed among infants with in- fection. However, in our seiles the incidence of late PDA episodes and the adverse outcome of those PDA episodes temporally related to infection were independent of fluid in- take.
The presence of a PDA negatively affects lung mechanics and gas exchange, 21' 22 and thereby increases the risk of
chronic pulmonary damage. Infections have also been asso- ciated with CLD, and increased levels of cytokines have been demonstrated in bronchoalveolar lavage of infants in whom CLD is developing. 23 In our study, infections were
associated with a higher incidence of late PDA episodes and PDA closure failures, and therefore with more exposure to detrimental effects of PDA on the lung. This may be one mechanism to explain the synergistic interaction of PDA and infection with the risk of CLD. Additionally, TNF« induces sequestration of neutrophils in lungs, which results in pulmonary vascular injury and edema. 24 In our study, infants with PDA and a temporally related infection had elevated TNFe~ levels, which may intensify pulmonary edema as a result of the increased pulmonary capillary pressure pro- duced by the PDA.
A limitation of our study is that we observed a wide vari-
ability in serum concentrations of both 6-keto PGFI« and TNF«, especially among patients with infection. Part of this variability can be explained by the wide range of variation in the clinical symptoms of the infected patients (from mild symptoms to shock and death). Wide vailations of levels of both mediators have been reported, and they appear to cor- relate with the severity of disease. 16' 25 On the other hand, variation of levels has been reported with time during infec- tion, levels being elevated during the initial hours of disease and declining thereafter. 25 Although most samples were drawn along with the initial blood culture sample, this time point did not always coincide with the time of the most se- vere clinical manifestations. Despite these variations, the levels observed in these infants were similar to measure- ments and variations reported elsewhere for premature infants.12, 16
It can be argued that our diagnosis of infection was weak, and that some of the episodes that we considered to be S. epidermidis infection may represent skin contamination. However, all the infants had symptoms, and 52% of them had more than one documented positive blood culture result. Symptom-free infants with an isolated culture positive for S. epidermidis were not considered infected. The fact that in- fants with infection had elevated levels of TNF« also sup-

The Journal of Pediatrics Gonzalez et aL 4 7 7 Volume 128, Number 4
Bir th w e i g h t
M a l e g e n d e r
W h i t e R a c e
5' A p g a r < 5
S e v e r e R D S
I n f e c t i o n
P D A
H igh F lu id i n t a k e
Air Leak
I V H G r I I I o r I V
P D A + l n f e c t i o n
X :
j )~( I
X I
YK
X
I I I I
0.1 1.0 10 30 100
Fig. 5. Odds ratios (*) and their 95% confidence intervals for CLD, with logistic regression analysis of infants who sur- vived 28 or more days after birth (n = 105). We analyzed birth weight per 100-gram decrement; air leaks include pneumothorax and pulmonary interstitial emphysema; infections include episodes at any time point during the first month. Odds ratio for PDA + lnfection (temporally related) were obtained from a second logistic model (see Methods section).
ports the contention that most episodes were associated with
a significant inflammatory response and strengthens our di-
agnosis of infection.
Our data demonstrate the importance of systemic infection
in the evolution of PDA in extreme!y premature infants, and
the interaction of infection and PDA in increasing the risk
of CLD. Clinicians should be aware of this association be-
tween infection and poor PDA outcome and should monitor
these infants closely for early diagnosis and treatment of
these complications. Further studies are needed to evaluate
more efficient therapeutic approaches to PDA in infected
patients.
We thank Dr. Orlando Gomez-Marin for his invaluable assistance in the statistical analysis, Ms. Rosa Nufiez and Ms. Silvia Martinez for their assistance in data collection, and Ms. Lalitha Price and Mr.
Miguel Martinez for their help in the radioimmunoassay measure- ments. We also thank Dr Julienne Prineas for her critical review of this manuscript, and the fellows, attending physicians, and person- nel of the divisions of neonatology and pediatric cardiology for their help in the study.
R E F E R E N C E S
1. Ellison RC, Peckham GJ, Lang P, et al. Evaluation of the pre- term infant for patent ductus arteriosus. Pediatrics 1983;7 1:364- 72.
2. Gonzalez A, Ventura-Junca P. Incidence of patent ductus arte- riosus in premature infants less than 2000 g. Rev Chil Pediatr 1991;62:354-8.
3. Hack M, Horbar JD, Malloy MH, et al. Very low birth weight outcome of National Institute of Child Health and Human De- velopment Neonatal Network. Pediatrics 1991;87:587-97.
4. Rojas M, Gonzalez A, Bancalari E, Claure N, Poole C, Silva-

4 7 8 Gonzalez et al. The Journal of Pediatrics April 1996
Neto G. Changing trends in the epidemiology and pathogenesis of neonatal chronic lung disease. J PED~TR 1995;126:605-10.
5. Lamont RF, Rose M, Elder MG. Effect of bacterial products on prostaglandin E production by amnion cells. Lancet 1985;2: 1331-3.
6. Fletcher JR.The role of prostaglandins in sepsis. Scand J Infect Dis 1982;3 l(suppl):55-60.
7. Dixon WJ, Brown MB, Engelman L, Jenrich RI, eds. BMDP statistical software manual; vol 1. Berkeley: University of Cal- ifomia Press, 1990 revision.
8. Coceani F, Olley PM. The response of the ductus arteriosus to prostaglandins. Can J Physiol Pharmacol 1973;51:220-5.
9. Clyman RI, Mauray F, Rudolph AM, Heymann MA. Age-de- pendent sensitivity of the lamb ductus arteriosus to indometha- cin and prostaglandins. J PEDtATR 1980;96:94-8~
10. Hutchison A, Ogletree M, Palme J, et al. Plasma 6-keto-pros- taglandin FI« and thromboxane B2 in sick preterm neonates. Prostaglandins Leukotrienes and Medicine 1985;18:163-81.
11. Lucas M, Mitchell A. Plasma prostaglandins in preterm neonates before and after treatment for patent ductus arteriosus. Lancet 1978;2:130-2.
12. Hammerrnan C, Zaia W, Berger S, et al. Prostaglandin levels: predictors of indomethacin responsiveness. Pediatr Cardiol 1986;7:61-5.
13. Runlde B, Goldberg RN, Streitfeld MM, et al. Cardiovascular changes in group B streptococcal sepsis in the piglet: response to indomethacin and relationship to prostacyclin and throm- boxane A» Pediätr Res 1984;18:874-8.
14. Gersony WM, Peckham GJ, Ellison RC, Miettinen OS, Nadas AS. Effects of indomethacin in premature infants with patent ductus arteriosus: results of a national collaborative study. J PEDIATR 1983;102:895-906.
15. Girardin EP, Berner ME, Grau GE, Suter S, Lacourt G, Pau- niet L. Serum tumor necrosis factor in newboms at risk for in- fections. Eur J Pediatr 1990;149:645-7.
16. de Bont ES, Martens A, van Raan J, et al. Diagnostic value of tumor necrosis factor (TNF«) and interleukin-6 (IL-6) in new- boms with sepsis. Acta Paediatr 1994;83:696-9.
17. Tracey KJ. Tumor necrosis factor (cachectin) in the biology of septic shock syndrome. Circulatory Shock 1991 ;35:123-8.
18. Horan TD, Noujaim AA, McPherson TA. Effect of indometha- cin on human neutrophil chemoluminescence and microbicidal activity. Immunopharmacology 1983;6:97-106.
19. Herson VC, Krause PJ, Eisenfeld LI, Pontius L, Maderazo EG. Indomethacin-associated sepsis in very-low-birth-weight in- fants. Arch Pediatr Adolesc Med [Am J Dis Child] 1988; 142:555-8.
20. Bell EF, Warburton D, Stonestreet BS, Oh W. Effect of fluid administration on the development of symptomatic patent duc- tus arteriosus and congestive heart failure in premature infants. N Engl J Med 1980;302:598-604.
21. Gerhardt T, Bancalari E. Lung compliance in newborns with patent ductus arteriosus before and after surgical ligation. Biol Neonate 1980;38:96-105.
22. Stefano JL, Abbasi S, Pearlman SA, et al. Closure of the ductus arteriosus with indomethacin in ventilated neonates with respiratory distress syndrome: effects on pulmonary compliance and ventilafion. Am Rev Respir Dis 1991;143: 236-9.
23. Bagghi.A, Viscardi RM, Taciak V, et al. Increased activity of interleukin-6 but not tumor necrosis factor--a in lung lavage of premature infants associated with the development of bron- chopulmonary dysplasia. Pediatr Res 1994;36:244-52.
24. Lo SK, Everitt J, Gu J, Malik AB. Tumor necrosis factor me- diates experimental pulmonary edema by ICAM-1 and CD18- dependent mechanims. J Clin Invest 1992;89:981-8.
25. Harris RH, Zmudka M, Maddox Y, Ramwell PW, Fletcher JR. Relationships of TXB2 and 6-keto PGFI« to the hemodynamic changes during baboon endotoxic shock. Adv Prostaglandin Thromboxane Res 1980;7:843-9.





























