Embed Size (px)
Citation preview
CIC
Influence of Donor Smoking on Midterm OutcomesAfter Lung TransplantationAnton Sabashnikov, MD, Nikhil P. Patil, MCh, Prashant N. Mohite, MCh,Diana García S�aez, MD, Bartlomiej Zych, MD, Aron-Frederik Popov, MD, PhD,Alexander Weymann, MD, Thorsten Wahlers, MD, PhD, Fabio De Robertis, MD,Toufan Bahrami, MD, Mohamed Amrani, MD, PhD, and Andr�e R. Simon, MD, PhDDepartment of Cardiothoracic Transplantation and Mechanical Circulatory Support, Royal Brompton & Harefield NHS FoundationTrust, Harefield Hospital, Harefield, Middlesex, United Kingdom; and Department of Cardiothoracic Surgery, University Hospital ofCologne, Cologne, Germany
GENERALTHORA
Background. Lung transplantation (LTx) is significantlylimited by donor organ shortage. Donor smoking historyof more than 20 pack-years is considered an extendeddonor criterion. In this study, we retrospectively evalu-ated impact of donor smoking history and extent ofsmoking on midterm outcome after LTx.
Methods. In all, 237 LTx were performed in our insti-tution between 2007 and 2012. Patients were divided intothree groups, receiving lungs from 53% nonsmoking do-nors, 29% smoking donors with fewer than 20 pack-years,and 18% heavy smokers with more than 20 pack-years.
Results. Preoperative donor and recipient characteris-tics among the groups were comparable. However, do-nors from the heavy smokers group were significantlyolder (p < 0.001). The overall presence of abnormal his-tology (inflammation or metaplasia) in donor mainbronchi samples increased with the extent of smokingbut did not reach statistical significance (p [ 0.211).Although metaplasia was found in significantly moredonors from the heavy smokers group (p [ 0.037), this
Accepted for publication Nov 11, 2013.
Address correspondence to Dr Sabashnikov, Department of Cardiotho-racic Transplantation and Mechanical Circulatory Support, RoyalBrompton & Harefield NHS Foundation Trust, Hill End Rd, Harefield,Middlesex UB9 6JH, United Kingdom; e-mail: [email protected].
� 2014 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
did not translate into inferior outcomes for the recipients.There were no statistically significant differences inPaO2/FiO2 ratio after LTx, duration of mechanical venti-lation (p[ 0.136), intensive care unit stay (p[ 0.133), andtotal postoperative hospital stay (p [ 0.322). One-yearand three-year survival were comparable across all threegroups (log rank p [ 0.151). Prevalence of bronchiolitisobliterans syndrome (p [ 0.616), as well as bronchiolitisobliterans syndrome free survival (p [ 0.898) after LTxwere also comparable.Conclusions. In our experience, history and extent of
donor smoking do not significantly affect early andmidterm outcomes after LTx. Although this finding doesnot obviate the need for longer-term observation, donorlungs from even heavy smokers may not per se contra-indicate LTx and may provide a valuable avenue forexpanding donor organ availability.
(Ann Thorac Surg 2014;97:1015–21)� 2014 by The Society of Thoracic Surgeons
ung transplantation (LTx) is a life-saving therapy for
Lpatients with end-stage lung disease, but shortage oforgan donors results in significant waiting list mor-tality. The UK Transplant Registry data show that forpatients listed for a lung transplant, only 20% receivetransplants within 6 months, rising to 51% after3 years, by which time 30% have died waiting for atransplant [1]. Because of injuries to the lung duringthe process of brain death and complications related tothe intensive care unit (ICU), only 17% of actual do-nors in the United States and 15% in the UnitedKingdom donate lungs [2, 3]. To overcome this donorshortage several techniques such as optimization ofdonor management, use of extended criteria donors,cardiocirculatory arrest donors, as well as ex-vivo lungperfusion are being utilized [4–7]. Maximizing donorselection is an important strategy to reducing waitinglist mortality.Donor smoking history is one of the major guideline
variables for donor selection, and a previously acceptedcriterion for an ideal donor is a smoking history of lessthan 20 pack-years, with a smoking history of more than20 pack-years putting the donor into the category of anextended donor [8]. Given the prevalence of smoking inthe general population, and consequently in the organdonation pool, a policy of refusal to use lung allograftsfrom smokers would have a profound impact on thenumber of available organs [9]. Conversely, the risk that apositive smoking history in lung donors could adverselyaffect transplant outcome causes concern [10]. In anattempt to address this pertinent issue, we collected andanalyzed patient and donor characteristics, as well asoutcome data, for all lung transplantations performed atour center over a 6-year period and investigated the as-sociation between donor smoking history and severalmeasures of outcome.
0003-4975/$36.00http://dx.doi.org/10.1016/j.athoracsur.2013.11.020

1016 SABASHNIKOV ET AL Ann Thorac SurgDONOR SMOKING AND OUTCOMES OF LTX 2014;97:1015–21
GENERALTHORACIC
Material and Methods
The Institutional Review Board at our center approvedthis study and waived the need for individual patientconsent.
The study design was a retrospective review of theprospectively collected data. A total of 237 LTx wereperformed at Harefield Hospital between January 2007and September 2012. Recipients were divided into threegroups depending on smoking history of the donors fromwhom they received organs: 123 (53%) nonsmoking (NS)donors, 68 (29%) smoking (S) donors who had smokedless than 20 pack-years, and 41 (18%) heavily smoking(HS) donors with a smoking history of more than 20 pack-years. One pack-year was defined as 20 cigarettes (onepack) smoked per day for 1 year. Five patients wereexcluded owing to unknown donor smoking history,leaving 232 patients for further analysis.
Endpoints of the StudyPrimary endpoints of the study were overall survival afterlung transplantation and survival free of bronchiolitisobliterans syndrome (BOS). Secondary endpointsincluded postoperative recipient characteristics: paO2/FiO2 ratio at the end of the transplant and 24, 48, and 72hours after transplant, duration of mechanical ventilation,intensive care unit (ICU) and total hospital stay, and needfor postoperative use of extracorporeal membraneoxygenation.
Organ Assessment and Organ Procurement ProtocolDonor organ assessment performed at donor hospitalsincluded radiologic assessment, fiberoptic bronchoscopy,gross organ inspection and palpation, assessment ofcompliance using deflation test, and selective blood gasanalysis from each pulmonary vein. The final decision ofproceeding with organ procurement and transplantationwas taken by the implanting surgeon. The standardpreservation solution used was low potassium dextran(Perfadex; Medisan, Uppsala, Sweden) solution aug-mented with CaCl2, 3.6% tromethamine (THAM; Hos-pira, Lake Forest, IL), and epoprostenol sodium 2.5 mL/L.For donation after brain death, 4 L of the solution wasusually administered antegradely through a Medtronic(Minneapolis, MN) 24F single-stage venous cannula and1 L retrogradely through a Medtronic 15F retrogradecannula with self-inflating balloon. For donation aftercardiac death (DCD), 3 L of pneumoplegia was adminis-tered antegrade and 2 L retrograde. During the pulmo-nary artery flush, a flushing pressure between 10 and15 mm Hg was maintained. Once the organs wereremoved from the chest, they were inspected and thenpacked for storage on ice and transported half inflatedwith FiO2 0.5. Samples of donor main bronchi were takenduring organ implantation and sent for histopathologyassessment. Also, intrabronchial swabs were collected formicrobiological analysis. The total ischemic time wasdefined as the time between cardiac arrest in DCDdonors or aortic cross-clamp in donation after brain deathdonors and reperfusion of the second implanted lung.
Detailed donor data, such as demographic variables,cause of death, current clinical status, laboratory in-vestigations, and social and medical history wereanalyzed. The information about donor smoking habitsand estimate of pack-year consumption were obtainedfrom the general practitioner or donor’s next of kin. De-mographics and perioperative recipient data as well asmidterm outcome were compared. BOS was diagnosedwhen posttransplant fraction of expired volume in 1 s(FEV1), measured on a regular basis after the transplant,permanently dropped more than 20% of the best FEV1
achieved after LTx.
Statistical AnalysisDatawere obtained fromcardiothoracic donor informationforms and recipient chart review. Statistical analysis wasperformed using IBM SPSS Statistics version 21 software(SPSS, Chicago, IL). The data are presented as continuousor categorical variables. Continuous data were evaluatedfor normality using the one-sample Kolmogorov-Smirnovtest, and are expressed as the mean � SD in cases of nor-mally distributed variables ormedian (interquartile range)in cases of nonnormally distributed variables. Categoricaldata are expressed as total numbers and percentages.Intergroup comparisonswere performed using either one-way analysis of variance or the Kruskal-Wallis test fornormal and nonnormal continuous variables, respectively.Pearson’sc2 or Fisher’s exact testswereused for categoricaldata depending on the minimum expected count in eachcross tabulation. A p value less than 0.05 was consideredstatistically significant. Kaplan-Meier actuarial survivalcurves were generated to analyze post-LTx survival andsurvival free of BOS.
Results
Of 237 LTx performed between January 2007 andSeptember 2012, 214 (90.3%) were double-lung trans-plantations and 23 (9.7%) were single-lung trans-plantations. Lungs were retrieved from 237 donors whomet the assessment criteria for lung transplantation. In 45cases (19%), lungs were retrieved from DCD donors.Organ procurement was performed by six designatedlung transplant centers in the United Kingdom, includingours, within the specified geographic region of eachcenter. Overall, 147 organs (60.03%) were procured by ourretrieval team whereas 90 organs (37.97%) were procuredby other five centers and sent to Harefield Hospital forfurther lung transplantation. The lungs were matched tothe recipients according to blood group, height, total lungcapacity, time on the waiting list, and clinical status of therecipient at the time of transplantation.After exclusion of patients who received transplants
using organs from donors with unknown smoking history(n ¼ 5, 2.11%), donors from the NS, S, and HS groups hadcomparable baseline characteristics, except for signifi-cantly higher donor age in the HS group: 47.93 � 7.03years, compared with 37.75 � 11.55 years in the S groupand 42.46 � 13.91 years in the NS group (p < 0.001). Aspresented in Table 1, there were no statistically significant
Table 1. Donor Baseline and Organ Procurement Data
Donor Data NS Donor S Donor HS Donor p Value
Age, years 42.5 � 13.9 37.8 � 11.5 47.9 � 7.0 <0.001Female 45 (36.6%) 29 (42.6%) 15 (36.6%) 0.688Height, cm 168.8 � 11.1 171.5 � 9.9 167.7 � 8.8 0.172Weight, kg 73.0 � 16.3 71.7 � 11.8 71.6 � 11.8 0.801PaO2 preretrieval, kPa 57.7 � 13.8 57.2 � 13.9 55.7 � 13.5 0.725Total lung capacity 5.4 (5.0–6.9) 5.8 (5.2–7.1) 5.4 (5.0–6.7) 0.074Ventilation duration, days 2 (1–3) 1.5 (1–2.8) 1 (1–4) 0.610Total ischemic time, min 369.1 � 129.2 350.1 � 140.3 353.2 � 151.9 0.610Use of ex vivo lung perfusion 4 (3.3%) 2 (2.9%) 2 (4.9%) 0.853Donation after cardiac death 25 (20.3%) 15 (22.1%) 4 (9.8%) 0.242Cardiac arrest 25 (20.7%) 13 (19.1%) 10 (24.4%) 0.804Abnormal chest radiograph 33 (28.2%) 17 (25.0%) 8 (19.5%) 0.542Abnormal bronchoscopy 24 (20.2%) 20 (29.4%) 11 (28.2%) 0.303Positive culture (bronchial) 53 (58.9%) 36 (62.1%) 22 (61.1%) 0.923Abnormal histology (bronchial) 72 (71.3%) 46 (75.4%) 35 (85.4%) 0.211
Inflammation 72 (72.7%) 45 (73.8%) 34 (82.9%) 0.427Metaplasia 1 (1.0%) 2 (3.3%) 4 (9.8%) 0.037
Cause of deathIntracranial hemorrhage 74 (60.2%) 47 (69.1%) 33 (80.5%) 0.049Hypoxic brain injury 17 (13.8%) 5 (7.4%) 4 (9.8%) 0.378Trauma 13 (10.6%) 7 (10.3%) 3 (7.3%) 0.827Cerebrovascular accident 10 (8.1%) 6 (8.8%) 1 (2.4%) 0.410Meningitis 6 (4.9%) 3 (4.4%) 0 0.361Other 3 (2.4%) 1 (1.5%) 0 0.572
HS ¼ heavy smoking (>20 pack-years); NS ¼ nonsmoking; S ¼ smoking (<20 pack-years).
1017Ann Thorac Surg SABASHNIKOV ET AL2014;97:1015–21 DONOR SMOKING AND OUTCOMES OF LTX
GENERALTHORACIC
differences in donor cause of death, percentage of DCD(p ¼ 0.242), abnormal chest roentgenogram (p ¼ 0.542),bronchoscopy (p ¼ 0.303), use of ex vivo lung perfusion(p ¼ 0.853), duration of donor mechanical ventilation (p ¼0.610), last preretrieval PaO2/FiO2 ratio (p ¼ 0.725), andtotal ischemic time (p ¼ 0.610). There were no significantdifferences regarding positive intrabronchial cultures(p ¼ 0.923). Abnormal histology (inflammation or meta-plasia) in donor organs was present in 71.3%, 75.4%, and85.4% (p ¼ 0.211) for the NS, S, and HS groups, respec-tively, consisting of inflammation in 72.2%, 73.8%, and82.9% (p ¼ 0.427) and metaplasia in 1%, 3.3%, and 9.8%(p ¼ 0.037), respectively, for the NS, S, and HS groups.
Table 2 shows preoperative recipient demographicsand distribution of recipient’s diagnosis. There were nostatistically significant differences in recipient’s age (p ¼0.875), height (p ¼ 0.167), weight (p ¼ 0.358), total lungcapacity (p ¼ 0.074), and preoperative use of extracorpo-real life support (p ¼ 0.699). However, female recipientswere more present in the NS group (p ¼ 0.025). Recipientdiagnoses leading to indication for a lung transplant wereequally distributed among the three groups (Table 2).
Intraoperative variables and early postoperativeoutcomes are presented in Table 3. There were no sta-tistically significant differences in terms of off-pump oron-pump strategy (p ¼ 0.388) and proportion of patientsreceiving a single lung transplant (p ¼ 0.697). The PO2/FiO2 ratios at the end of the transplant (p ¼ 0.371), at
24 hours (p ¼ 0.466), at 48 hours (p ¼ 0.956), and at 72hours (p ¼ 0.652) after transplant were similar. Theprevalence of postoperative BOS did not differ among thethree groups: 14 (14%) in the NS group; 11 (19%) in the Sgroup; and 8 (21%) in the HS group (p ¼ 0.616). The BOS-free survival (log rank [Mantel-Cox] p ¼ 0.833; Fig 1) wasnot statistically different; and although 1-year and 3-yearsurvival estimates showed some differences, they werenot significant (Fig 2): 77.7% versus 90.8% versus 94.9%,and 68.7% versus 82.1% versus 68.2%, in the NS groupversus the S group versus the HS, respectively (log rankp ¼ 0.151).
Comment
The principal finding in this retrospective study was thattransplanting lungs from donors who smoked or wereeven heavy smokers did not yield inferior early andmidterm outcomes compared with lungs from donorswho never smoked. This finding is more pertinent in lightof the fact that donors from the HS group were found tobe significantly older than donors from the other twogroups in this study.A large body of literature now exists on the adverse
consequences of cigarette smoke inhalation, which,pertinent to this discussion, include increased suscepti-bility to postoperative pulmonary complications,decreased pulmonary function, occult malignancy (lung
Table 2. Recipient Baseline Characteristics
Recipient Characteristics NS Donor S Donor HS Donor p Value
Age, years 43.6 � 12.4 42.5 � 14.0 43.2 � 14.2 0.875Female 67 (54.5%) 24 (35.3%) 23 (56.1%) 0.025Height, cm 167.6 � 8.6 170.1 � 8.9 168.0 � 9.2 0.167Weight, kg 61.6 (53.7–78.7) 61.7 (52.7–76.4) 61.9 (52.7–81.2) 0.358Total lung capacity 5.5 (4.9–6.8) 6.3 (5.0–7.1) 5.4 (4.9–6.9) 0.074Extracorporeal life support 6 (4.9%) 12 (2.9%) 1 (2.4%) 0.699Primary diagnosis
Cystic fibrosis 42 (34.1%) 25 (36.8%) 16 (39.0%) 0.836Emphysema 36 (29.3%) 22 (32.4%) 11 (26.8%) 0.818a-1 antitrypsin deficiency 13 (10.6%) 10 (14.7%) 8 (19.5%) 0.321Pulmonary fibrosis 10 (8.1%) 4 (5.9%) 2 (4.9%) 0.719Pulmonary hypertension 8 (6.5%) 5 (7.4%) 2 (4.9%) 0.878Lymphangiomyomatosis 7 (5.7%) 0 0 0.041Sarcoidosis 3 (2.4%) 1 (1.5%) 2 (4.9%) 0.548Bronchiolitis obliterans 3 (2.4%) 1 (1.5%) 0 0.572Bronchiectasis 2 (1.6%) 1 (1.5%) 0 0.719
HS ¼ heavy smoking (>20 pack-years); NS ¼ nonsmoking; S ¼ smoking (<20 pack-years).
1018 SABASHNIKOV ET AL Ann Thorac SurgDONOR SMOKING AND OUTCOMES OF LTX 2014;97:1015–21
GENERALTHORACIC
cancer), and immunosuppression [11–19]. However, it isimportant to realize that the qualitative and quantitativeeffects of cigarette smoke might depend on the durationof smoking, as well as on the sex and ethnicity of thesubjects who are studied. Smoking-related lung injury isquite variable and the extent of changes documentedvaries significantly between studies. Some persons canhave pronounced lung damage leading to obstructivelung disease, whereas others can have preserved lungparenchyma and function despite several years ofsmoking [20]. The prevalence of donors with smokinghistory in this study was 47%. This figure is in agreementwith other studies [8, 10] from the United Kingdom,which report positive smoking history in 39% to 45% ofpotential donors, with similar rates described in theUnited States [9]. Thus, decisions regarding organs frompositive smoking donors would dramatically impact theavailable pool of lung allografts and potentially the life
Table 3. Intraoperative Data and Postoperative Outcome
Variables NS Donors
Off pump 30 (24.4%)Single-lung transplantation 12 (9.8%)PaO2/FiO2 ratio on arrival 327.7 � 134.3PaO2/FiO2 ratio 24 hours 348.9 � 109.6PaO2/FiO2 ratio 48 hours 351.4 � 112.4PaO2/FiO2 ratio 72 hours 348.0 � 120.4Ventilation, hours 35 (14–198)Intensive care unit stay, days 5 (3–19)Hospital stay, days 34 (21–51)ECMO 11 (9.0%)Bronchiolitis obliterans 14 (14.3%)
ECMO ¼ extracorporeal membrane oxygenation; HS ¼ heavy smoking (>2
expectancy of patients with end-stage lung diseaseawaiting transplantation.Conversely, transplantation of lungs from donors with
smoking history has courted media criticism [21] andeven medicolegal action [22]. As a result, patients ontransplant waiting lists are increasingly involved in thedecision about whether to accept donated organs [10].Possibly, potential recipients now have the option todecline lungs from donors with positive smokinghistories [23] and choose to wait for organs from a non-smoking donor—presumably with fewer risk factors—in the hope of increasing their chances of post-transplantation survival. However, this choice would bemade on the presumption that transplantation will occurbefore the patient dies on the waiting list or deterioratesto the extent that transplantation is no longer possible. Itwould also assume that the person’s access to trans-plantation would not be affected by logistic constraints in
S Donors HS Donors p Value
11 (16.2%) 10 (24.4%) 0.3885 (7.4%) 5 (12.2%) 0.697
334.6 � 153.2 297.7 � 104.7 0.371328.3 � 108.5 344.9 � 105.5 0.466352.8 � 123.6 346.1 � 95.4 0.956341.4 � 114.4 364.0 � 109.1 0.65250 (23–474) 34 (10–96) 0.13611 (3–26) 6 (3–19) 0.13333 (23–59) 39 (27–56) 0.3228 (11.8%) 1 (2.4%) 0.24011 (18.6%) 8 (20.5%) 0.616
0 pack-years); NS ¼ nonsmoking; S ¼ smoking (<20 pack-years).
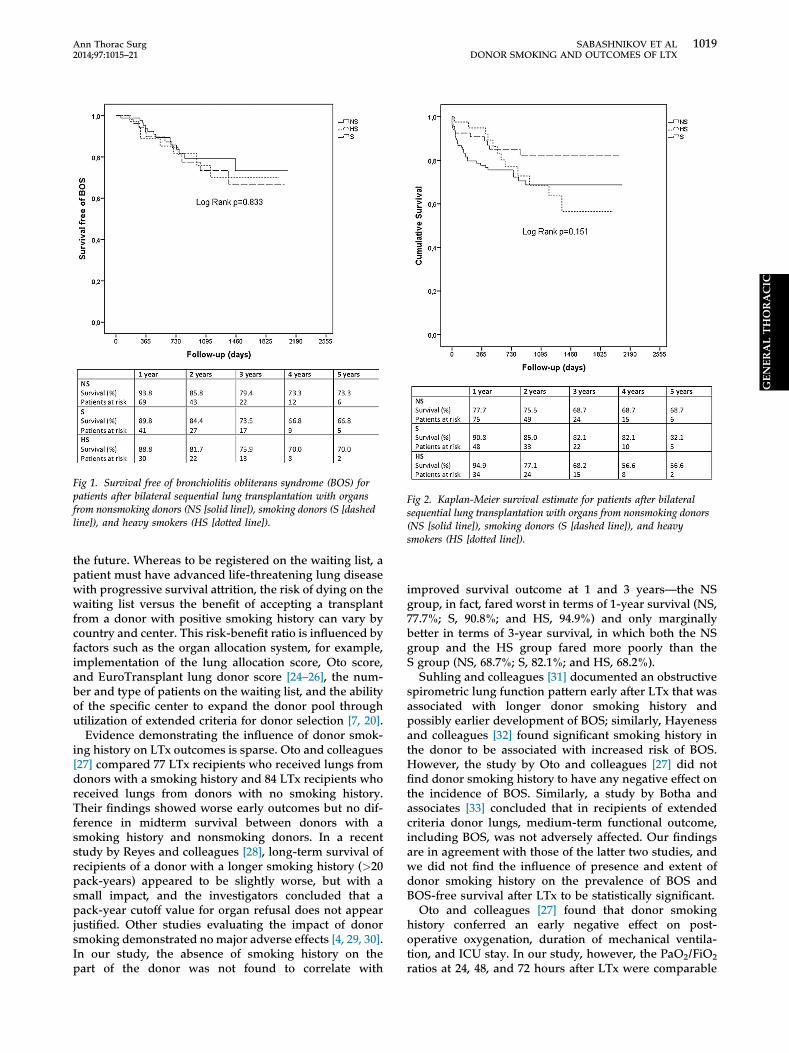
Fig 1. Survival free of bronchiolitis obliterans syndrome (BOS) forpatients after bilateral sequential lung transplantation with organsfrom nonsmoking donors (NS [solid line]), smoking donors (S [dashedline]), and heavy smokers (HS [dotted line]).
Fig 2. Kaplan-Meier survival estimate for patients after bilateralsequential lung transplantation with organs from nonsmoking donors(NS [solid line]), smoking donors (S [dashed line]), and heavysmokers (HS [dotted line]).
1019Ann Thorac Surg SABASHNIKOV ET AL2014;97:1015–21 DONOR SMOKING AND OUTCOMES OF LTX
GENERALTHORACIC
the future. Whereas to be registered on the waiting list, apatient must have advanced life-threatening lung diseasewith progressive survival attrition, the risk of dying on thewaiting list versus the benefit of accepting a transplantfrom a donor with positive smoking history can vary bycountry and center. This risk-benefit ratio is influenced byfactors such as the organ allocation system, for example,implementation of the lung allocation score, Oto score,and EuroTransplant lung donor score [24–26], the num-ber and type of patients on the waiting list, and the abilityof the specific center to expand the donor pool throughutilization of extended criteria for donor selection [7, 20].
Evidence demonstrating the influence of donor smok-ing history on LTx outcomes is sparse. Oto and colleagues[27] compared 77 LTx recipients who received lungs fromdonors with a smoking history and 84 LTx recipients whoreceived lungs from donors with no smoking history.Their findings showed worse early outcomes but no dif-ference in midterm survival between donors with asmoking history and nonsmoking donors. In a recentstudy by Reyes and colleagues [28], long-term survival ofrecipients of a donor with a longer smoking history (>20pack-years) appeared to be slightly worse, but with asmall impact, and the investigators concluded that apack-year cutoff value for organ refusal does not appearjustified. Other studies evaluating the impact of donorsmoking demonstrated nomajor adverse effects [4, 29, 30].In our study, the absence of smoking history on thepart of the donor was not found to correlate with
improved survival outcome at 1 and 3 years—the NSgroup, in fact, fared worst in terms of 1-year survival (NS,77.7%; S, 90.8%; and HS, 94.9%) and only marginallybetter in terms of 3-year survival, in which both the NSgroup and the HS group fared more poorly than theS group (NS, 68.7%; S, 82.1%; and HS, 68.2%).Suhling and colleagues [31] documented an obstructive
spirometric lung function pattern early after LTx that wasassociated with longer donor smoking history andpossibly earlier development of BOS; similarly, Hayenessand colleagues [32] found significant smoking history inthe donor to be associated with increased risk of BOS.However, the study by Oto and colleagues [27] did notfind donor smoking history to have any negative effect onthe incidence of BOS. Similarly, a study by Botha andassociates [33] concluded that in recipients of extendedcriteria donor lungs, medium-term functional outcome,including BOS, was not adversely affected. Our findingsare in agreement with those of the latter two studies, andwe did not find the influence of presence and extent ofdonor smoking history on the prevalence of BOS andBOS-free survival after LTx to be statistically significant.Oto and colleagues [27] found that donor smoking
history conferred an early negative effect on post-operative oxygenation, duration of mechanical ventila-tion, and ICU stay. In our study, however, the PaO2/FiO2
ratios at 24, 48, and 72 hours after LTx were comparable

1020 SABASHNIKOV ET AL Ann Thorac SurgDONOR SMOKING AND OUTCOMES OF LTX 2014;97:1015–21
GENERALTHORACIC
across all groups. Whereas the S group was found to havethe longest durations of mechanical ventilation and ICUstay, the HS group had the longest mean duration ofhospital stay, but these differences did not attain statis-tical significance. Likewise, although the use of extracor-poreal membrane oxygenation was lowest in the HSgroup, this was not statistically significant.
Despite the excellent work documented in thesestudies, the authors were unable to find in contemporaryliterature any details of histopathologic analyses fromsmokers’ donor lungs at the time of implantation.Nevertheless, review of histopathologic analyses from ourstudy showed that the overall distribution of abnormalhistology (inflammation or metaplasia) in donor organswas directly proportional to the extent of smoking,although this did not reach statistical significance (p ¼0.211). The overwhelming reason for histology to beconsidered “abnormal” was inflammation, which waspresent in more than 70% specimens from all threegroups. While the presence of inflammation in more than70% of specimens from even nonsmoking donors mayinitially seem incongruous, one must be mindful thatmost donors have usually been intubated and mechani-cally ventilated for a considerable length of time, whichmight account for these findings. Although the differencein the proportion of inflammation documented in the NS,S, and HS groups was not statistically significant (p ¼0.427), metaplasia was found to be significantly more indonor lungs from the HS group (9.8%) as compared to theS group (3.3%) and the NS group (1%; p ¼ 0.037).Although these histologic findings did not translate intoactual inferior or outlier outcomes at early or midtermanalysis after LTx, they serve as a measure of the “actualand demonstrable” effect of smoking on donor organquality and underscore the need for vigilance and longer-term evaluation. Conversely, these findings also providereal-world figures for the perceived “risk” of implantationof lungs from donors with even a heavy smoking historyand bear testimony that such donor lungs may provide amuch-needed lease on life to the critically ill patientwhose chances of survival diminish with every day orweek that passes by on the waiting list.
Study LimitationsThis study is an analysis of prospectively collected reg-istry data. Smoking history pertaining to the potentialdonor smoking is inevitably third-party information andverification is not possible. Quantification of smoking isdifficult in this clinical setting, and estimates can bemisclassified. Data for the smoking status of recipientsbefore and after transplantation were not available foranalysis.
In conclusion, in our experience, history and extent ofdonor smoking do not significantly affect early andmidterm outcomes after LTx. Although that does notobviate the need for longer-term observation, donorlungs from even heavy smokers may not per se contra-indicate LTx and may provide a valuable avenue forexpanding donor organ availability.
References
1. Transplant activity in the UK—NHS blood and transplant:activity report 2009/10. Available at: http://www.nhsbt.nhs.uk/downloads/pdfs/temp/report.pdf. Accessed September19, 2013.
2. De Perrot M, Liu M, Waddell T, Keshavjee S. Ischemia-reperfusion induced lung injury. Am J Respir Cell Mol Biol2003;28:616–25.
3. The U.S. Organ Procurement and Transplantation Networkand the Scientific Registry of Transplant Recipients. 2009OPTN/SRTR annual report. Available at: http://optn.transplant.hrsa.gov/ar2009/. Accessed September 19, 2013.
4. Gabbay E, Williams TJ, Griffiths AP, et al. Maximizing theutilization of donor organs offered for lung transplantation.Am J Respir Crit Care Med 1999;160:265–71.
5. Schiavon M, Falcoz PE, Santelmo N, Massard G. Does theuse of extended criteria donors influence early and long-term results of lung transplantation? Interact CardiovascThorac Surg 2012;14:183–7.
6. Cypel M, Sato M, Yildirim E, et al. Initial experience withlung donation after cardiocirculatory death in Canada.J Heart Lung Transplant 2009;28:753–8.
7. Zych B, Popov AF, Stavri G, et al. Early outcomes of bilateralsequential single lung transplantation after ex-vivo lungevaluation and reconditioning. J Heart Lung Transplant2012;31:274–81.
8. Berman M, Goldsmith K, Jenkins D, et al. Comparisonof outcomes from smoking and nonsmoking donors:thirteen-year experience. Ann Thorac Surg 2010;90:1786–92.
9. Castleberry AW, Hartwig MG. The trade-off of usingpositive-smoking donor lungs. Semin Thorac CardiovascSurg 2012;24:151–2.
10. Bonser RS, Taylor R, Collett D, Thomas HL, Dark JH,Neuberger J. Effect of donor smoking on survival after lungtransplantation: a cohort study of a prospective registry.Lancet 2012;380:747–55.
11. Shigemura N, Toyoda Y, Bhama JK, et al. Donor smokinghistory and age in lung transplantation: a revisit. Trans-plantation 2013;95:513–8.
12. Xu X, Dockery DW,Ware JH, Speizer FE, Ferris BG. Effects ofcigarette smoking on rate of loss of pulmonary function inadults: a longitudinal assessment. Am Rev Respir Dis1992;146:1345–8.
13. Sopori M. Effects of cigarette smoke on the immune system.Nat Rev Immunol 2002;2:372–7.
14. Nuorti JP, Butler JC, Farley MM, et al. Cigarette smoking andinvasive pneumococcal disease. Active Bacterial Core Sur-veillance. N Engl J Med 2000;342:681–9.
15. Holt PG. Immune and inflammatory function in cigarettesmokers. Thorax 1987;42:241–9.
16. Burnham EL, Kovacs EJ, Davis CS. Pulmonary cytokinecomposition differs in the setting of alcohol use disordersand cigarette smoking. Am J Physiol Lung Cell Mol Physiol2013;304:L873–82.
17. Gualano RC, Hansen MJ, Vlahos R, et al. Cigarette smokeworsens lung inflammation and impairs resolution of influ-enza infection in mice. Respir Res 2008;9:53.
18. Arnson Y, Shoenfeld Y, Amital H. Effects of tobacco smoke onimmunity, inflammation and autoimmunity. J Autoimmun2010;34:258–65.
19. Singh JA, Hawn M, Campagna EJ, Henderson WG,Richman J, Houston TK. Mediation of smoking-associatedpostoperative mortality by perioperative complications inveterans undergoing elective surgery: data from VeteransAffairs Surgical Quality Improvement Program (VASQIP)—acohort study. BMJ Open 2013;3:e002157.
20. Cypel M, Keshavjee S. Expansion of the donor lung pool: useof lungs from smokers. Lancet 2012;380:709–11.
21. BBC News. Cystic fibrosis woman died with smoker’s donorlungs. Available at: http://www.bbc.co.uk/news/uk-england-essex-20762437. Accessed September 19, 2013.

1021Ann Thorac Surg SABASHNIKOV ET AL2014;97:1015–21 DONOR SMOKING AND OUTCOMES OF LTX
NERALTHORACIC
22. Estate of Tony Grier by Administrator Emma Grier V. Uni-versity of Pennsylvania Health System, et al. Civil Action No.07-4224. United States District Court for the Eastern Districtof Pennsylvania. Filed June 11, 2009. Available at: http://www.gpo.gov/fdsys/pkg/uscourts-paed-2_07-cv-04224/pdf/uscourts-paed-2_07-cv-04224-0.pdf. Accessed September 19,2013.
23. NHS Blood and Transplant—British Transplantation So-ciety. Guidelines for consent for solid organ trans-plantation in adults 2013. Available at: http://www.nhsbt.nhs.uk/pdf/guidelines_for_consent.pdf. Accessed September19, 2013.
24. Thabut G, Christie JD, Mal H, et al. Survival benefit of lungtransplant for cystic fibrosis since lung-allocation-scoreimplementation. Am J Respir Crit Care Med 2013;187:1335–40.
25. Oto T, Levvey BJ, Whitford H, et al. Feasibility and utility of alung donor score: correlation with posttransplant outcome.Ann Thorac Surg 2007;83:257.
26. Smits JM, Van der Bij W, Van Raemdonck D, et al. Definingan extended criteria donor lung: an empirical approachbased on the Eurotransplant experience. Transpl Int 2011;24:393–400.
� 2014 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
27. Oto T, Griffiths AP, Levvey B, et al. A donor history ofsmoking affects early but not late outcome in lung trans-plantation. Transplantation 2004;78:599–606.
28. Reyes KG, Mason DP, Thuita L, et al. Guidelines for donorlung selection: time for revision? Ann Thorac Surg 2010;89:1756–64.
29. Bhorade SM, Vigneswaran W, McCabe MA, Garrity ER.Liberalization of donor criteria may expand the donor poolwithout adverse consequence in lung transplantation. J HeartLung Transplant 2000;19:1199–204.
30. Sundaresan S, Semenkovich J, Ochoa L, et al. Successfuloutcome of lung transplantation is not compromised by theuse of marginal donor lungs. J Thorac Cardiovasc Surg1995;109:1075–80.
31. Suhling H, Dettmer S, Rademacher J, et al. Spirometricobstructive lung function pattern early after lung trans-plantation. Transplantation 2012;93:230–5.
32. Hennessy SA, Hranjec T, Swenson BR, et al. Donor factorsare associated with bronchiolitis obliterans syndrome afterlung transplantation. Ann Thorac Surg 2010;89:1555–62.
33. Botha P, Trivedi D, Weir CJ, et al. Extended donor criteria inlung transplantation: impact on organ allocation. J ThoracCardiovasc Surg 2006;131:1154–60.
GE
INVITED COMMENTARY
In this article, Sabashnikov and associates [1] seek toaddress the very controversial and provocative question ofdonor smoking history as a guideline variable for donorselection in the framework of lung transplantation (LTx).In a retrospective review of a prospectively collecteddatabase, they analyzed patient and donor characteristics,as well as outcome data, for all LTx performed in theirinstitution. Their main criteria of judgment were theimpact of donor history and extent of smoking onmidtermoutcome. For this, 237 patients having undergone a LTxwere included and classified into three groups dependingon smoking history of the donors from whom theyreceived organs. Sabashnikov and colleagues [1]concluded that history and extent of donor smoking donot adversely affect LTx midterm outcome.
This stimulating paper helps to clarify some of thecontroversies regarding the maximization of donor se-lection in a strategy to reducing waiting list mortality andappropriately investigates some of the dogma in this area.The results of this well-designed study may well impactthe possibility of choice of a donor in the near future.Indeed, this study clearly questions both the policy ofrefusal to use lung allografts from smokers and its impacton the number of available organs [2] and the risk that apositive history in lung donors could adversely affecttransplant outcome [3].
Why should lung transplant physicians be concernedwith the findings of this rigorous study? Not only becausethe current contribution shows an essential way toexplore the process of donor selection; rather, alsobecause this stimulating paper has successfully “openedone door leading to 10 more” in the burgeoning field oflung preservation and assessment. Indeed, using ex vivolung perfusion for the donor lung might be the clue notonly to perform a global functional assessment but alsogoing one step further to initiate treatment, such as with
pharmacologic agent (to reduce pulmonary edema andinflammation) or gene and cell therapy (to better preparethe organ to deal with the reperfusion and subsequentimmunologic insult) [4, 5].For now, Sabashnikov and associates are to be
congratulated on their contribution in this area. Theirresults will certainly prove to be most beneficial to thelung transplant community.
Pierre-Emmanuel Falcoz, MD, PhD
Department of Thoracic SurgeryUniversity Hospital1 Place de l’HopitalNouvel Hopital CivilStrasbourg 67000, Francee-mail: [email protected]
References
1. Sabashnikov A, Patil NP, Mohite PN, et al. Influence of donorsmoking on midterm outcomes after lung transplantation.Ann Thorac Surg 2014;97:1015–21.
2. Castelberry AW, Hartwig MG. The trade-off of using positive-smoking donor lungs. Semin Thorac Cardiovasc Surg 2012;24:151–2.
3. Bonser RS, Taylor R, Collett D, Thomas HL, Dark JH,Neuberger J. Effect of donor smoking on survival after lungtransplantation: a cohort study of a prospective registry.Lancet 2012;380:747–55.
4. Warnecke G, Moradiellos J, Tudorache I, et al. Normo-thermic perfusion of donor lungs for preservation andassessment with the organ care system lung before bilateraltransplantation: a pilot study of 12 patients. Lancet 2012;380:1851–8.
5. Cypel M, Keshavjee S. Strategies for safe donor expansion:donor management, donations after cardiac death, ex-vivolung perfusion. Curr Opin Organ Transplant 2013 August 29[E-Pub ahead of print].
0003-4975/$36.00http://dx.doi.org/10.1016/j.athoracsur.2013.12.013