Embed Size (px)
Citation preview

c© 2012 Wiley Periodicals, Inc. 1
CASE REPORT
Inflammatory PseudotumorArising from the RightVentricular Outflow TractCausing Pulmonary Stenosis
Nageswar Rao, Trushar Gajjar,
Nandita Ghosal, and Neelam Desai
Sri Sathya Sai Institute of Higher MedicalSciences, District Anantapur,Andhra Pradesh, India
ABSTRACT Inflammatory pseudotumor (also known
as inflammatory myofibroblastic tumor) is an un-
common spindle cell lesion that was initially rec-
ognized in the lung and is now known to occur
in virtually every major organ of the body. We re-
port a case of a seven-year-old male who had an
inflammatory pseudotumor of the right ventricu-
lar outflow tract involving the pulmonary valve
causing pulmonary stenosis. doi: 10.1111/j.1540-8191.2012.01460.x (J Card Surg 2012;**:1-3)
INTRODUCTION
Inflammatory pseudotumor (IPT) was first observedin the lung and described by Brunn in 1939 and wasso named by Umiker et al. in 1954 because of itspropensity to clinically and radiologically mimic a ma-lignant process.1 We report a case of a seven-year-oldmale who had an IPT of the right ventricular outflowtract involving the pulmonary valve causing pulmonarystenosis.
CASE REPORT
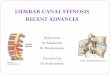
A seven-year-old male presented with dyspnea andpalpitations for six months. On examination there wasa grade 3/6 ejection systolic murmur in the left sec-ond intercostal space. Chest X-ray showed a cardio-thoracic ratio of 55%. Transthoracic echocardiogramshowed a 1.5 × 4 × 1.6 cm sized pedunculated andglobular mass, arising from the right ventricular out-flow tract and base of the pulmonary valve (Fig. 1A),causing a right ventricular outflow gradient of 31/16mm of Hg (Fig. 1B) with normal ventricular function.The patient was referred for surgery. A standard mid-
Conflict of interest: None.Address for correspondence: Nageswar Rao, CTVS Department,Sri Sathya Sai Institute of Higher Medical Sciences, Prasanthigram515134, District Anantapur, Andhra Pradesh, India. Fax: +91-08555-287388; e-mail: [email protected]
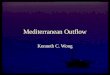
line sternotomy approach was used. Cardiopulmonarybypass was established with aortic and bicaval cannu-lation. The main pulmonary artery was opened verti-cally in an empty beating heart. There was a globular2 × 4 × 2 cm mass attached to the ventricular sep-tum near the right ventricular outflow tract which wasadherent to the cusps of the pulmonary valve (Fig. 2).Total excision of the tumor along with the excision ofthe adherent pulmonary valve leaflet was performed.Reconstruction of the pulmonary valve was not per-formed, in view of intact normal pulmonary annulusand presence of at least one well-formed normal pul-monary cusp. The postoperative course was unevent-ful and an echocardiogram showed no residual tumor,trivial tricuspid and pulmonary regurgitation, no rightventricular outflow obstruction, and good biventricularfunction.
The pathological examination revealed a very firmyellowish-white smooth mass 1.8 × 1.8 × 2 cm withfocal mucoid/gelatinous and hemorrhagic areas. Micro-scopically it showed marked fibrosis with hyalinization,fibroblastic proliferation, focal neovascularization, areasof fibrinoid necrosis, hemorrhage, and edema. Therewas a chronic inflammatory infiltrate composed of lym-phocytes, plasma cells, macrophages, eosinophils withfocal smooth muscle proliferation, and myofibroblasticspindle cells (Fig. 3).
After three months, the patient was asymptomaticand transthoracic echocardiography showed no recur-rence of tumor, and mild pulmonary regurgitation withgood ventricular function.
DISCUSSION
IPT is a quasineoplastic lesion consisting of inflam-matory cells and myofibroblastic spindle cells1 andit most commonly involves the lung and the orbit.Very few cases of cardiac IPT have been describedin the literature. Cardiac sites involved by IPT haveincluded the right and left atrium, right and left ven-tricle, pulmonary and tricuspid valves, septum, rightand left coronary arteries, superior vena cava, coro-nary sinus, and the atrioventricular groove.1 The exactcause of IPT is unknown. Various theories have beenpostulated which include transformation from a low-grade fibrosarcoma, inflammation following trauma, anautoimmune mechanism, vasculitis, and infection.2,3
Immunohistochemical studies of T- and B-cell subpop-ulations may be helpful in distinguishing IPT from lym-phoma. IPTs usually contain both T cells and B cells,whereas in lymphoma, a (clonal) B- or T-cell popu-lation predominates.2 The common clinical manifes-tations of cardiac IPT are fever, chest pain, pallor,diaphoresis, dyspnea, decreased oral intake, thrombo-cytosis, hypergammaglobulinemia, and collapse. Two-dimensional echocardiography remains a highly reliableimaging diagnostic tool, but precise information on thetumor histology is not attainable by echocardiography.

2 RAO, ET AL.INFLAMMATORY PSEUDOTUMOR
J CARD SURG2012;**:1-3
Figure 1. Transthoracic echocardiography. (A) Parasternal short axis view showing a pedunculated and globular mass arising fromthe right ventricular outflow tract and base of the pulmonary valve. (B) A mass arising from pulmonary leaflet producing rightventricular outflow gradient.
Various treatment options have been suggested, de-pending on the size, site, and involvement of the sur-rounding structures.4-8 If, at the time of surgery, thetumor is large and invading structures such as car-diac valves or coronary vessels, and the histologicaldiagnosis has been confirmed, then conservative treat-ment is advisable.4 Whenever feasible, surgical resec-tion should be the mainstay of treatment.5 If surgi-cal resection is not possible, conservative manage-ment includes observation and prednisone, 1 mg/kgof body weight per day.4,6 Most IPTs behave in abenign fashion. These tumors never metastasize, buta small percentage have the potential for malignant
transformation over a period of time.9,10 At present,there are no reliable clinical or pathologic predictors forthe behavior of IPTs. However, tumors with cytologi-cal atypia or increased mitotic activity should be treatedaggressively with gross resection and reconstruction.5
Till now only one documented case of recurrence isreported, likely due to inadequate excision of tissue.7
Cardiac IPTs are usually benign lesions with a favorableprognosis. Despite the evidence that most of thesetumors show a benign clinical course, it is clear thatthese tumors can have mediastinal invasion, local re-currences, metastases, and sarcomatous degenerationwith poor prognosis.9,10

J CARD SURG2012;**:1-3
RAO, ET AL.INFLAMMATORY PSEUDOTUMOR
3
Figure 2. (A) External appearance of heart with tumor popping in and out of pulmonary artery (arrow). (B) Opened pulmonaryartery showing tumor involving pulmonary valve cusp (arrows). (C) Tumor arising from the septal portion of right ventricular outflowtract involving pulmonary valve cusp. (D) Excised tumor.
Figure 3. Paraffin section showing (A) myocardium with infiltration by eosinophils and macrophages, (B) high power view of thesame with eosinophils (curved arrow), and (C) myofibres showing loss of striations. [Hematoxylin & Eosin: (A)×100; (B),(C) × 400.]
REFERENCES
1. Umiker WO, Iverson LC: Post inflammatory tumor of thelung: Report of four cases simulating xanthoma, fibromaor plasma cell granuloma. J Thorac Surg 1954;28:55-62.
2. Dehner LP. The enigmatic inflammatory pseudotumors:The current state of our understanding, or misunder-standing (editorial). J Pathol 2000;192:277-279.
3. Coffin CM, Watterson J, Priest JR, et al: Extrapulmonaryinflammatory myofibroblastic tumor (inflammatory pseu-dotumor): A clinicopathologic and immunohistochemicalstudy of 84 cases. Am J Surg Pathol 1995;19:859-872.
4. Tomiyama M, Nakatani S, Ueda HI, Yutani C, YamagishiM. Inflammatory pseudotumor of the heart. Ann InternMed 2007;147:351-352
5. Solomon B, Grossi EA, Monteith D, et al: Extendedcardiac resection for obstructing pseudotumor due
to Ormond disease. Ann Thorac Surg 2010;90:636-638.
6. Pearson PJ, Smithson WA, Driscoll DJ, et al: Inopera-ble plasma cell granuloma of the heart: Spontaneous de-crease in size during an 11-month period. Mayo Clin Proc1988;63(10):1022-1025.
7. Hartyanszky IL, Kadar K, Hubay M. Rapid recurrence ofan inflammatory myofibroblastic tumor in the right ven-tricular outflow tract. Cardiol Young 2000;10(3):271-274.
8. Narla LD, Siddiqi NH, Hingsbergen EA. Inflamma-tory pseudotumor of the right atrium. Pediatr Radiol2001;31:351-353.
9. Chou P, Gonzalez-Crussi F, Cole R, et al: Plasma cellgranuloma of the heart. Cancer 1988;62:1409-1413.
10. Li L, Cerilli LA, Wick MR. Inflammatory pseudotumor(myofibroblastic tumor) of the heart. Ann Diagn Pathol2002;6:116-121.