Embed Size (px)
Citation preview
Inflammatory Markers and Coronary Interventions: APotentially Useful Follow-Up Modality After Stenting
Giuseppe Patti, MD, Germano Di Sciascio,* MD, FSCAI, Andrea D’Ambrosio, MD,Giordano Dicuonzo, MD, Antonio Abbate, MD, and Aldo Dobrina, MD
Periprocedural levels of various inflammatory markers have been correlated with prog-nosis in patients undergoing percutaneous coronary interventions. However, long-termvariations of interleukin-1 receptor antagonist (IL-1Ra) or C-reactive protein (CRP) duringfollow-up after coronary interventions were not previously investigated. The aim of ourstudy was to perform serial evaluations of these markers before and after coronarystenting and to correlate them with clinical status. Plasma levels of IL-1Ra and CRP weremeasured at baseline and 3 and 6 months after the procedure in 31 patients withsymptomatic coronary artery disease undergoing stent implantation, who had no evi-dence of myocardial ischemia at 6-month follow-up. While at 3 months there were nosignificant variations of baseline values, 6 months after the procedure a significantdecrease from baseline was observed both in IL-1Ra and CRP levels (median �24 pg/ml,P � 0.048, and �0.13 mg/dl, P � 0.017, respectively). Six-month reduction in both IL-1Raand CRP levels was significant in patients with unstable angina (n � 18; IL-1Ra: from 175to 119 pg/ml, P � 0.001; CRP: from 0.52 to 0.18 mg/dl, P � 0.002) and nonsignificant inthose with stable angina (n � 13) on admission (IL-1Ra: from 123 to 158 pg/ml, P � 0.22;CRP: from 0.19 to 0.10 mg/dl, P � 0.44). In conclusion, a significant reduction of IL-1Raand CRP levels is observed 6 months after stent implantation in patients with preproce-dural unstable angina who remain free of ischemia. This decrease suggests a stabiliza-tion of the inflammatory process and may be associated with a favorable prognosis aftercoronary interventions. Cathet Cardiovasc Intervent 2002;56:341–345.© 2002 Wiley-Liss, Inc.
Key words: coronary artery disease; stenting; inflammation; interleukins
INTRODUCTION
Increasing evidence suggests an important role of in-flammation in the pathogenesis and destabilization ofcoronary atherosclerotic plaques [1–3] and acute-phasereactants, such as C-reactive protein (CRP), were corre-lated with a worse prognosis in patients with unstablecoronary syndromes [4,5]. More recently, interleukin-1receptor antagonist (IL-1Ra) was identified as importantprognostic factor after percutaneous coronary interven-tions [6]. The proinflammatory interleukin-1 (IL-1) isinvolved in coronary atherosclerosis, in tissue inflamma-tion/injury, and in ischemia-reperfusion injury [7–9]. IL-1Ra competitively blocks the binding of IL-1 to its mem-brane receptors [7–10] and modulates the inflammatoryresponse; hepatocytes may produce IL-1Ra in responseto inflammatory stimuli [11]. In addition, IL-1Ra couldbe released from activated endothelial cells and mono-cytes at sites of tissue damage and/or inflammation[7–9,12,13] in association with local IL-1 release. PlasmaIL-1 levels are usually very low, even in septic shockpatients [7], whereas IL-1Ra levels well correlate withseverity of inflammation [14]. Inflammation may play an
important role also in the pathogenesis of restenosis afterpercutaneous coronary interventions, particularly in theneointimal proliferation of in-stent restenosis [15–17];however, long-term plasma variations of inflammatorymarkers after percutaneous revascularization were notpreviously described. In this study, IL-1Ra and CRPplasma levels were prospectively analyzed before and 3and 6 months after successful coronary stenting in aconsecutive cohort of patients with symptomatic coro-nary artery disease.
Department of Cardiovascular Sciences, Campus Bio-MedicoUniversity, Rome, Italy
*Correspondence to: Dr. Germano Di Sciascio, Department of Car-diovascular Sciences, Campus Bio-Medico University, 00155 Rome,Italy.E-mail: [email protected]
Received 25 May 2001; Revision accepted 17 January 2002
DOI 10.1002/ccd.10201Published online in Wiley InterScience (www.interscience.wiley.com).
Catheterization and Cardiovascular Interventions 56:341–345 (2002)
© 2002 Wiley-Liss, Inc.

MATERIALS AND METHODS
Patients Population and Study Design
From January 1998, 31 consecutive patients with sig-nificant coronary artery disease, defined as reduction �70% of the lumen diameter, undergoing coronary stent-ing in our institution were enrolled in a prospectivefollow-up study to evaluate IL-1Ra and CRP plasmalevels variations 3 and 6 months after the procedure. Allpatients gave informed consent to the study. Eighteenpatients (58%) had unstable angina on admission (Braun-wald class IIB or IIIB); they were all treated with aspirin,intravenous nitrates and heparin, and beta-blocker orcalcium-antagonist drugs. Thirteen patients (42%) hadchronic stable angina for at least 12 months, with docu-mented transient inducible myocardial ischemia andwithout clinical evidence of myocardial ischemia in the72 hr preceding admission; all these patients were treatedwith aspirin, nitrates, and a calcium-antagonist or beta-blocker drug. All patients were free of myocardial in-farction (MI) in the previous 3 months. The interven-tional procedures were performed the day after theadmission with a femoral approach and conventionaltechniques were used in all patients; stent implantationwas performed electively, for bail-out or suboptimal re-sult after balloon inflations. All patients were pretreatedwith ticlopidine (250 mg/twice daily) at least for 2 daysbefore intervention. Before procedure, heparin (100 UI/kg) was given intravenously. Procedural angiographicsuccess was defined as a reduction of stenosis to less than30% residual narrowing after stent implantation. Glyco-protein IIb/IIIa antagonists were not employed in ourinstitution at the time of the study. Procedural clinicalsuccess was defined as improvement of ischemic symp-toms associated with angiographic success, without ma-
jor in-hospital complications (MI, bypass surgery, ordeath). Statin treatment was indefinitely continued in 21patients, aspirin (100 mg/daily) in all patients, and ticlo-pidine was continued for 4 weeks after the procedure. Atthe time of enrollment, no patients had clinical and/orlaboratory evidence of malignancy, infections, inflam-matory diseases, or recent (� 2 months) surgery ortrauma. Follow-up data were collected by office visit at 3,6, 12, and 18 months. Follow-up assessment includedreturn of angina, occurrence of MI, cardiac death, coro-nary revascularization, inflammatory and immune dis-eases. Rehospitalization was indicated for recurrentsymptoms and/or signs of myocardial ischemia and re-peat coronary angiography was performed if indicated.
Venous blood samples were drawn 3–6 hr before theprocedure to measure plasma levels of IL-1Ra and CRP;plasma levels of these markers were also drawn at 3- and6-month follow-up. Patients were kept fasting for at least8 hr before blood collection and at complete rest for atleast 10 min before blood collection. Blood samples weredrawn in all patients from 6:00 to 8:30 a.m. with a 16 Gneedle and the minimum of venous stasis. All proceduraland laboratory data were prospectively collected in acomputerized database.
Laboratory Assays
Venous blood samples were collected in syringes andanticoagulated with sodium citrate for detection of CRPor EDTA for detection of IL-1Ra; the blood was refrig-erated until it was centrifuged at 2,000 g at 4°C for 30min. The plasma obtained was frozen at �80°C, until itwas essayed. IL-1Ra kits were purchased from R&DSystem (MN). The assays employed the quantitativesandwich enzyme immunoassay technique. The micro-plate reader was an LP400 from Sanofi-Diagnostics Pas-teur (Milan, Italy); the lower level of detection for theassay was 49 pg/ml. CRP was determined by high-sensitivity-rate nephelometry (DADE-Behring CRP; Be-hring Institute, Scoppito, L’Aquila, Italy).
Statistical Analysis
Values are expressed as mean � standard deviation fornormally distributed variables and median and interquar-tile range for IL-1Ra and CRP plasma levels. The non-parametric Mann-Whitney U-test was used to comparenonpaired data, while Wilcoxon test for paired data. Pvalues � 0.05 were considered significant.
RESULTS
Characteristics of the 31 patients enrolled in the studyare indicated in Table I. Procedural clinical success wasachieved in all 31 patients (100%) and angiographicsuccess in all 36 treated coronary arteries (100%; 1.16
TABLE I. Patient Characteristics
n %
Demographic and clinical characteristicsMales 26 84Age (years) 60 � 10Diabetes 6 19Hypertension 14 45Hypercholesterolemia 22 71Cigarette smoking 13 42Unstable angina 18 58Stable angina 13 42Previous myocardial infarction 15 48Left ventricular ejection fraction 56% � 8%Previous bypass surgery 0
Procedural characteristicsTreated coronary arteries 36Patients with stent 31 100Implanted stents 37Patients with multivessel stenting 5 16Angiographic and clinical success 31 100
342 Patti et al.
treated vessel/patient). All patients underwent coronarystenting; this was elective in 26 patients (84%) and forbail-out or suboptimal result after balloon inflations in 5patients (16%). A total of 37 stents were deployed (1.19stent/patient). During the procedure and until discharge,there were no acute major complications; no patient died,had acute MI, or required emergency bypass surgery.
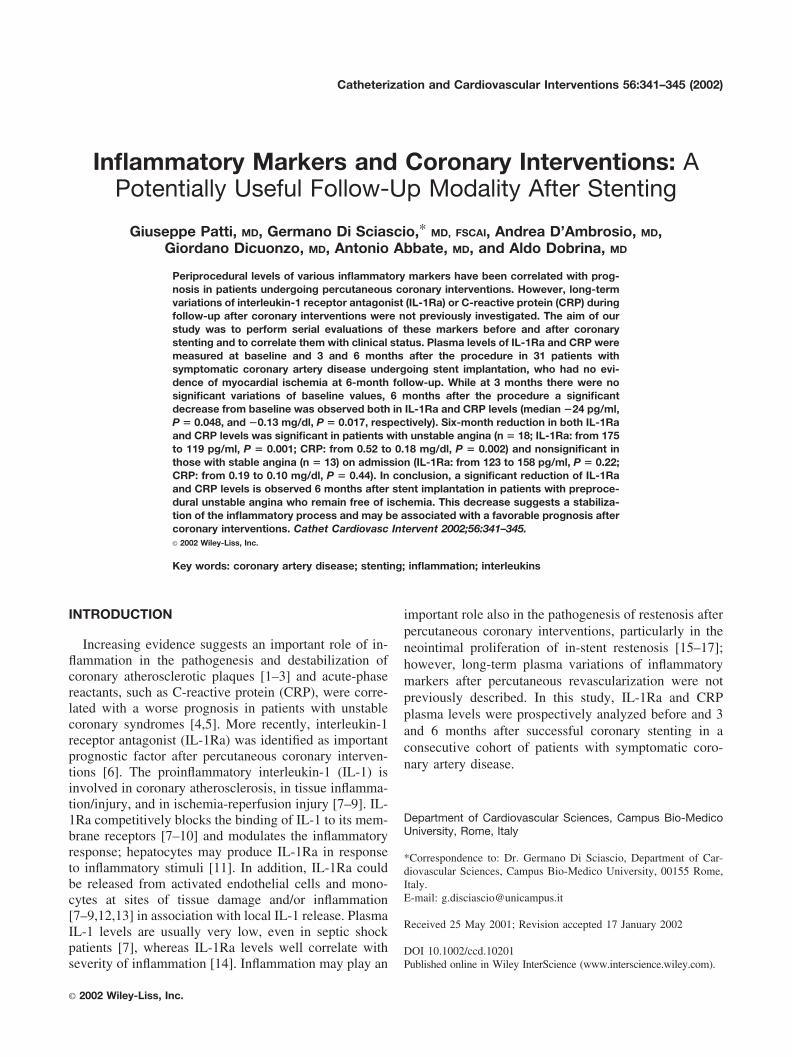
Baseline plasma IL-1Ra and CRP levels were 166pg/ml (interquartile range, 122–248) and 0.25 mg/dl(0.08–0.56), respectively. At 3 months, all patients werealive, free of MI, and asymptomatic for coronary arterydisease. At 4 months, three patients had recurrence ofangina and underwent reangioplasty because of resteno-sis; however, at 6, 12, and 18 months, all 31 patients,including those with reangioplasty, were alive, free ofMI, asymptomatic for coronary artery disease, and had afunctional study negative for transient myocardial isch-emia. During the whole follow-up period, no patientshowed evidence of systemic inflammatory or immunediseases or malignancy. No significant variations in IL-1Ra and CRP levels was evident at 3 months after theprocedure (Fig. 1), whereas at 6 months, IL-1Ra andCRP plasma levels were significantly lower compared topreprocedural levels (Fig. 1): 166 vs. 136 pg/ml (102–202), with a median reduction of �24 pg/ml (�102 to24; P � 0.048) and 0.25 vs. 0.17 mg/dl (0.03–0.33),
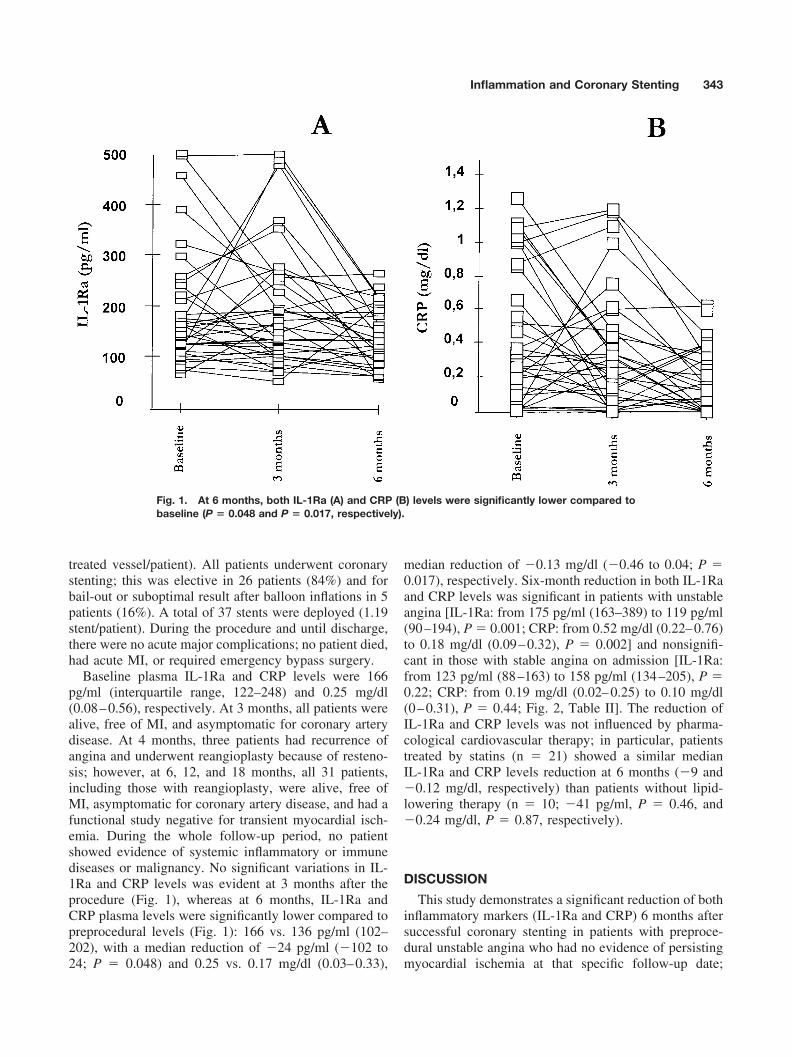
median reduction of �0.13 mg/dl (�0.46 to 0.04; P �0.017), respectively. Six-month reduction in both IL-1Raand CRP levels was significant in patients with unstableangina [IL-1Ra: from 175 pg/ml (163–389) to 119 pg/ml(90–194), P � 0.001; CRP: from 0.52 mg/dl (0.22–0.76)to 0.18 mg/dl (0.09–0.32), P � 0.002] and nonsignifi-cant in those with stable angina on admission [IL-1Ra:from 123 pg/ml (88–163) to 158 pg/ml (134–205), P �0.22; CRP: from 0.19 mg/dl (0.02–0.25) to 0.10 mg/dl(0–0.31), P � 0.44; Fig. 2, Table II]. The reduction ofIL-1Ra and CRP levels was not influenced by pharma-cological cardiovascular therapy; in particular, patientstreated by statins (n � 21) showed a similar medianIL-1Ra and CRP levels reduction at 6 months (�9 and�0.12 mg/dl, respectively) than patients without lipid-lowering therapy (n � 10; �41 pg/ml, P � 0.46, and�0.24 mg/dl, P � 0.87, respectively).
DISCUSSION
This study demonstrates a significant reduction of bothinflammatory markers (IL-1Ra and CRP) 6 months aftersuccessful coronary stenting in patients with preproce-dural unstable angina who had no evidence of persistingmyocardial ischemia at that specific follow-up date;
Fig. 1. At 6 months, both IL-1Ra (A) and CRP (B) levels were significantly lower compared tobaseline (P � 0.048 and P � 0.017, respectively).
Inflammation and Coronary Stenting 343
those patients remained asymptomatic also at the 18-month clinical follow-up after the procedure.
Recent findings [15–17] showed that inflammationmay play an important role in the pathogenesis/patho-physiology of restenosis after balloon angioplasty and inthe stimulation of neointimal proliferation of in-stentrestenosis; indeed, periprocedural CRP levels were pre-dictive of clinical recurrence in patients undergoing per-
cutaneous coronary interventions [18]. In our study, pa-tients with unstable angina who underwent successfulcoronary stenting and were without evidence of ischemiaat 6 months showed significant decrease of IL-1Ra andCRP plasma levels (32% and 65% from baseline, respec-tively), whereas such reduction was not evident in pa-tients with preprocedural stable angina. These resultssuggest that high levels of these inflammatory markers
Fig. 2. Six-month reduction from baseline in both IL-1Ra (A) and CRP (B) levels was significantin patients with unstable angina (P � 0.001 and P � 0.002, respectively) and nonsignificant inthose with stable angina on admission (P � 0.22 and P � 0.44, respectively).
TABLE II. Follow-Up IL-1Ra and CRP Plasma Levels, Median and Interquartile Range
Baseline levels
6 months
Levels Variation P
All patientsIL-1Ra (pg/ml) 166 (122–248) 136 (102–202) �24 (�102 to �24) 0.048CRP (mg/dl) 0.25 (0.08–0.56) 0.17 (0.03–0.33) �0.13 (�0.46 to 0.04) 0.017
Patients with unstable angina pectorisIL-1Ra (pg/ml) 175 (163–389) 119 (90–194) �74 (�217 to �24) 0.001CRP (mg/dl) 0.52 (0.22–0.76) 0.18 (0.09–0.32) �0.16 (�0.52 to �0.01) 0.002
Patients with stable angina pectorisIL-Ra (pg/ml) 123 (88–163) 158 (134–205) �26 (�19 to 75) 0.22CRP (mg/dl) 0.19 (0.02–0.25) 0.10 (0.01–0.31) �0.03 (�0.25 to 0.03) 0.44
344 Patti et al.

may be related to clinical presentation of coronary arterydisease and their reduction may be associated with afavorable prognosis after coronary interventions. Recentdata showed that IL-1Ra may be a specific marker ofinstability in patients with coronary disease [2]; indeed,stimulation of IL-1 system, a marker of monocyte acti-vation, plays a central role in coronary plaque destabili-zation and disruption [1] in the unstable phases of coro-nary artery disease. Moreover, IL-1 was demonstrated tobe involved in neointimal proliferation [19,20] and maypromote restenosis after percutaneous coronary interven-tions [21]. Therefore, reduced levels of IL-1Ra aftercoronary stenting, as observed in this study, may indicatea low inflammatory response and may be associated witha lower incidence of adverse events during follow-up.
In conclusion, this is the first report of a significantreduction of IL-1Ra and CRP levels 6 months aftercoronary stenting, suggesting a possible role of thesemarkers as a hallmark of stabilization of atheroscleroticplaques in patients following coronary interventions.Further studies on a greater number of patients are re-quired both to define their clinical utility in the noninva-sive monitoring of such patients and to evaluate thehypothesis whether, conversely, a lack of decrease maycorrelate to persisting myocardial ischemia or clinicalrecurrence.
REFERENCES
1. Ross R. Atherosclerosis: an inflammatory disease. N Engl J Med1999;340:115–126.
2. Patti G, Abbate A, D’Ambrosio A, Manzoli A, Dicuonzo G,Guarnirei G, Dobrina A, Di Sciascio G. IL-1 receptor antagonist:a more sensitive marker of unstable coronary syndromes thanC-reactive protein. Eur Heart J 2000;21:650.
3. Berliner JA, Navab M, Fogelman AM, Frank JS, Demer LL,Edwards PA, Watson AD, Lucis AJ. Atherosclerosis: basic mech-anisms—oxidation, inflammation and genetics. Circulation 1995;91:2488–2496.
4. Liuzzo G, Biasucci LM, Gallimore JR, Grillo RL, Rebuzzi AG,Maseri A. The prognostic value of C-reactive protein and serumamyloid A protein in severe unstable angina. N Engl J Med1994;331:417–424.
5. Morrow DA, Rifai N, Antman EM, Weiner DL, McCabe CH,Cannon CP, Braunwald E. C-reactive protein is a potent predictorof mortality independently and in combination with troponin T inacute coronary syndromes. J Am Coll Cardiol 1998;31:1460–1465.
6. D’Ambrosio A, Patti G, Abbate A, Manzoli A, Gioia G, DobrinaA, Di Sciascio G. Independent prognostic value of interleukin-1
receptor antagonist in patients undergoing percutaneous coronaryinterventions. Eur Heart J 2001;22:659.
7. Dinarello CA. Biological basis for interleukin-1 in disease. Blood1996;87:2095–2147.
8. Loppnow H, Werdan K, Reuter G, Flad HD. The interleukin-1 andinterleukin-1 converting enzyme families in the cardiovascularsystem. Eur Cytokine Netw 1998;9:675–680.
9. Rothwell N, Allan S, Toulmond S. The role of Interleukin-1 inacute neurodegeneration and stroke: pathophysiological and ther-apeutic implications. J Clin Invest 1997;100:2648–2652.
10. Arend WP. Interleukin 1 receptor antagonist: a new member of theInterleukin 1 family. J Clin Invest 1991;88:1445–1451.
11. Gabay C, Smith MF, Eidlen D, Arend WP. Interleukin-1 receptorantagonist (IL-1Ra) is an acute-phase protein. J Clin Invest 1997;99:2930–2940.
12. Gabay C, Porter B, Fantuzzi G, Arend WP. Mouse IL-1 receptorantagonist isoforms: complementary DNA coding and proteinexpression of intracellular isoform and tissue distribution of se-creted and intracellular IL-1 receptor antagonist in vivo. J Immu-nol 1997;159:5905–5913.
13. Dewberry R, Holden H, Crossman D, Francis S. Interleukin-1receptor antagonist expression in human endothelial cells andatherosclerosis. Arterioscler Thromb Vasc Biol 2000;20:2394–2400.
14. Fischer E, Van Zee KJ, Marano MA, Rock CS, Kenney JS,Poutsiaka DD, Dinarello CA, Lowry SF, Moldawer LL. Interleu-kin-1 receptor antagonist circulates in experimental inflammationand in human disease. Blood 1992;79:2196–2200.
15. Kornowski R, Hong MK, Tio FO, Bramwell O, Wu H, Leon MB.In-stent restenosis: contributions of inflammatory response andarterial injury to neointimal hyperplasia. J Am Coll Cardiol 1998;31:224–230.
16. Hoffmann R, Mintz GS, Dussaillant GR, Popma JJ, Pichard AD,Satler LF, Kent KM, Griffin J, Leon MB. Patterns and mechanismof in-stent restenosis: a serial intravascular ultrasound study. Cir-culation 1996;94:1247–1254.
17. Pietersma A, Kofflard M, de Wit LE, Stijnen T, Koster JF, SerruysPW, Sluiter W. Late lumen loss after coronary angioplasty isassociated with the activation status of circulating phagocytesbefore treatment. Circulation 1995:91:1320–1325.
18. Buffon A, Liuzzo G, Biasucci LM, Pasqualetti P, Ramazzotti V,Rebuzzi AG, Crea F, Maseri A. Preprocedural serum levels ofC-reactive protein predict early complications and late restenosisafter coronary angioplasty. J Am Coll Cardiol 1999;34:1512–1521.
19. Rectenwald JE, Moldawer LL, Huber TS, Seeger JM, Ozaki CK.Direct evidence for cytokine involvement in neointimal hyperpla-sia. Circulation 2000;102:1697–1702.
20. Libby P, Warner SJ, Friedman GB. Interleukin 1: a mitogen forhuman vascular smooth muscle cells that induces the release ofgrowth-inhibitory prostanoids. J Clin Invest 1988;81:487–498.
21. Libby P, Schwartz D, Brogi E, Tanaka H, Clinton SK. A cascademodel for restenosis: a special case of atherosclerosis progression.Circulation 1992;86:III47–III52.
Inflammation and Coronary Stenting 345



















![Coronary Computed Tomographic Angiography at 80 kVp and ... · modality for detecting and ruling out coronary artery disease (CAD) [1], but there are still ... a11111 OPEN ACCESS](https://img.pdfslide.us/doc/110x75/5fb6c266c32f8306cb3e1ff2/coronary-computed-tomographic-angiography-at-80-kvp-and-modality-for-detecting.jpg)









