Embed Size (px)
Citation preview

INFECTION AND IMMUNITY, June 2010, p. 2418–2428 Vol. 78, No. 60019-9567/10/$12.00 doi:10.1128/IAI.00170-10Copyright © 2010, American Society for Microbiology. All Rights Reserved.
Inflammatory Cytokine Response to Bacillus anthracis PeptidoglycanRequires Phagocytosis and Lysosomal Trafficking�
Janaki K. Iyer,1 Taruna Khurana,2 Marybeth Langer,3 Christopher M. West,4 Jimmy D. Ballard,5Jordan P. Metcalf,3 Tod J. Merkel,2 and K. Mark Coggeshall1*
Immunobiology and Cancer Program, Oklahoma Medical Research Foundation, 825 NE 13th Street, Oklahoma City,Oklahoma 731041; Laboratory of Respiratory Pathogens, Division of Bacterial Products, CBER, FDA, Building 29,
Room 419, 29 Lincoln Drive, Bethesda, Maryland 208922; Pulmonary and Critical Care Division, Department ofMedicine, University of Oklahoma Health Sciences Center, 800 N. Research Pkwy., Oklahoma City,
Oklahoma 73104 3; Oklahoma Center for Medical Glycobiology, Department of Biochemistry andMolecular Biology, 940 Stanton L. Young Blvd., BMSB 853, University of Oklahoma Health Sciences Center,
Oklahoma City, Oklahoma 731044; and Department of Microbiology and Immunology, The University ofOklahoma Health Sciences Center, Oklahoma City, Oklahoma 731045
Received 19 February 2010/Returned for modification 3 March 2010/Accepted 4 March 2010
During advanced stages of inhalation anthrax, Bacillus anthracis accumulates at high levels in the blood-stream of the infected host. This bacteremia leads to sepsis during late-stage anthrax; however, the mecha-nisms through which B. anthracis-derived factors contribute to the pathology of infected hosts are poorlydefined. Peptidoglycan, a major component of the cell wall of Gram-positive bacteria, can provoke symptomsof sepsis in animal models. We have previously shown that peptidoglycan of B. anthracis can induce theproduction of proinflammatory cytokines by cells in human blood. Here, we show that biologically activepeptidoglycan is shed from an active culture of encapsulated B. anthracis strain Ames in blood. Peptidoglycanis able to bind to surfaces of responding cells, and internalization of peptidoglycan is required for theproduction of inflammatory cytokines. We also show that the peptidoglycan traffics to lysosomes, and lysosomalfunction is required for cytokine production. We conclude that peptidoglycan of B. anthracis is initially boundby an unknown extracellular receptor, is phagocytosed, and traffics to lysosomes, where it is degraded to aproduct recognized by an intracellular receptor. Binding of the peptidoglycan product to the intracellularreceptor causes a proinflammatory response. These findings provide new insight into the mechanism by whichB. anthracis triggers sepsis during a critical stage of anthrax disease.
Inhalation anthrax, caused by Bacillus anthracis, is an insid-ious disease with a poor prognosis. Infections occur when en-dospores of the bacterium are phagocytosed by macrophages,carried to regional lymph nodes, and escape from the lungenvironment. During the course of infection, the bacteria growrapidly and enter the bloodstream. In an acute infection, levelsof bacteria as high as 108 bacteria per ml of blood have beenrecorded (7). If the disease is unabated, vegetative bacteria canbe found in almost every organ, presenting a life-threateningsituation that is difficult to treat (15, 19). Indeed, death isthought to occur due to toxemia (50) and/or septicemia (47)that results from a high bacterial load in the infected host.Despite exceptional advances in characterizing the early stagesof anthrax infection and the effects of the toxin, very little isknown about the B. anthracis factors which contribute to sepsisas the disease progresses.
In humans, sepsis is caused by an exaggerated proinflamma-tory response. For Gram-negative organisms, the proximalcause is the ability of an endotoxin, a lipopolysaccharide (LPS),to stimulate innate immune cells via Toll-like receptor 4(TLR4) (51). Gram-positive bacteria also cause sepsis, and theproximal cause is often attributable to superantigens derived
from Staphylococcus or Streptococcus species, which stimulatepolyclonal T-cell activation through their antigen receptors tocause toxic shock syndrome (11). More recent studies of thecauses of Gram-positive sepsis have revealed roles for lipotei-choic acid (LTA) (21), a Toll-like receptor 2 (TLR2) agonist(38), triacylated lipopeptides (17), an agonist for TLR2, TLR4,and TLR6 (44, 49), and peptidoglycan (PGN) (22), whoseproducts bind to nucleotide oligomerization domain (NOD)receptors (4, 12–14). The PGN products include N-acetylatedmuramic acid-alanine-glutamine-diaminopimelic acid (M-Tri-DAP) and N-acetylated muramic acid-alanine-glutamic acid(MDP). Thus, PGN from B. anthracis is a prime candidate forthe factor that causes sepsis during advanced stages of systemicanthrax.
We previously reported that B. anthracis cell wall extractswere able to induce production of proinflammatory cytokinesin cells in human blood (26). The cell wall extracts lackeddetectable LTA, and the biological activity was sensitive tolysozyme, suggesting that the biologically active material wasPGN. Here, we used B. anthracis PGN whose purity was veryhigh to examine the molecular and cellular mechanism bywhich this molecule stimulates inflammatory responses. Ourfindings indicate that B. anthracis PGN interacts with an ex-tracellular receptor on select hematopoietically derived cellsand that receptor endocytosis or phagocytosis is required forthe induction of proinflammatory cytokines. Endocytosed orphagocytosed PGN was found to traffic to lysosomes, and an
* Corresponding author. Mailing address: Oklahoma Medical Re-search Foundation, 825 NE 13th Street, Oklahoma City, OK 73104.Phone and fax: (405) 271-7209. E-mail: [email protected].
� Published ahead of print on 22 March 2010.
2418
on July 24, 2020 by guesthttp://iai.asm
.org/D
ownloaded from

acidified lysosome was also required for PGN biological activ-ity. In contrast to these results for human cells, mouse macro-phages were found to be less dependent on internalization ofPGN and of acidified lysosomes to mount a proinflammatoryresponse, and NOD-deficient and wild-type macrophages re-sponded equivalently. The data are consistent with a model inwhich B. anthracis PGN is engaged by human cells, internal-ized, and degraded in order to trigger a potent inflammatoryresponse. In addition, critical differences in this process be-tween human and mouse cells suggest that more focused stud-ies directed at primate and human models are important forunderstanding this aspect of anthrax disease in humans.
MATERIALS AND METHODS
Materials. Fluorochrome-conjugated antibodies to human CD14, CD3, andCD19 were purchased from Invitrogen, while CD14 conjugated to phycoerythrinwas purchased from eBioscience. Antibody to human CD16b was purchasedfrom Accurate Chemical & Scientific Corporation, and lysosome-associatedmembrane protein 1 (LAMP1) conjugated to Alexa Fluor 647 was purchasedfrom Santa Cruz. Human IgG was purchased from Lampire Biological Labora-tories. A monocyte isolation II kit was purchased from Miltenyi Biotech. Phal-loidin conjugated to Alexa Fluor 633 was purchased from Molecular Probes. Theenzymes proteinase K and DNase I and a SuperScript III first-strand synthesis kitwere purchased from Invitrogen. RNase A was purchased from Qiagen, and Sybrgreen PCR master mixture was obtained from Applied Biosystems. Brefeldin Awas purchased from eBioscience, and a Cambrex Limulus amebocyte lysate assaykit was purchased from Lonza. Ultrapure lipopolysaccharide (LPS), saponin,guanidine HCl, iodoacetamide, and heparin were purchased from Sigma. Asilkworm larvae plasma test kit was purchased from Wako Chemicals.
Preparation of B. anthracis peptidoglycan. Peptidoglycan was isolated from B.anthracis strain �Sterne, which lacks the capsule and toxins, as described byLanger et al. (26). Briefly, PGN was isolated from overnight cultures of thebacteria grown on tryptic soy broth plates. The bacteria were boiled in 8% SDSfor 30 min, which was followed by centrifugation. The pellet obtained was washedwith endotoxin-free water and subjected to DNase I and RNase A treatment for15 min at room temperature. The sample was boiled again in 4% SDS for 30 minand then washed three times with endotoxin-free water. The pellet was treatedwith 2 M NaCl and then washed six times with endotoxin-free water. The pelletwas then dried, weighed, and resuspended in endotoxin-free water.
Treatment of PGN with proteinase K and amino acid analysis. PGN wastreated with HF to remove the polysaccharide associated with the PGN asdescribed previously (8). Following HF treatment, the water-washed PGN wassubjected to treatment with a denaturing buffer (50 mM Tris [pH 8.0], 6 Mguanidine HCl, 25 mM dithiothreitol [DTT]) at 60°C for 1 h. Iodoacetamide wasadded to a final concentration of 75 mM and the preparation was incubated for15 min in the dark to alkylate Cys residues. The reaction was stopped by addingDTT to a final concentration of 40 mM. The PGN was resuspended in a buffercontaining 50 mM Tris (pH 7.5), 1 M guanidine HCl, and 5 mM CaCl2 and wastreated with 20 �g proteinase K (added every 12 h for 36 h) at 50°C for 36 h. ThePGN was washed three times with endotoxin-free water, dried, weighed, andresuspended in endotoxin-free water.
For amino acid analysis, 200 �g of PGN was dried with norleucine as aninternal standard and treated with 6 N HCl in sealed vacuum tubes for 20 to 24 hat 110°C. The hydrolysate was then subjected to cation-exchange high-perfor-mance liquid chromatography (HPLC) with ninhydrin detection to determinethe amino acid content of PGN. The amino acid analysis was performed at theMolecular Biology-Proteomics Facility at the University of Oklahoma HealthScience Center.
For labeling with fluorescein, PGN was treated with fluorescein isothiocyanate(FITC) at a ratio of 1:2 (wt/wt) in 100 mM NaHCO3 at pH 8.0. After 30 min ofincubation at room temperature, the labeled PGN was washed thoroughly withendotoxin-free water and resuspended in water.
Culture of peripheral blood and isolation of peripheral blood mononuclearcells, neutrophils, and monocytes. Heparinized peripheral blood (PB) was ob-tained by venipuncture after signed consent of healthy human volunteers; thevenipuncture protocol was approved by an internal review board. The blood wasdiluted 1:3 with Dulbecco’s modified Eagle’s medium and cultured in non-tissue-culture 24-well plates. PB mononuclear cells were obtained by Ficoll-Hypaquedensity gradient centrifugation. Neutrophils were separated from the red blood
cells by brief incubation in ACK lysis buffer (155 mM ammonium chloride, 10mM KHCO3, 0.1 mM EDTA). Monocytes were purified from PB mononuclearcells by using a monocyte isolation II kit according to the manufacturer’s instruc-tions.
Mice and cell culture. Wild-type mice with a C57BL/6 background were usedfor experiments. Bones were obtained from NOD1�/� (4), NOD2�/� (25), andNOD1�/� NOD2�/� (41) mice that had a C57BL/6 background. Bone marrowwas flushed from the femurs and tibias and cultured in RPMI 1640 mediumsupplemented with 10% fetal bovine serum, macrophage colony-stimulating fac-tor (M-CSF), penicillin, streptomycin, and glutamine for 7 days as describedpreviously (36). From day 7 on bone marrow-derived macrophages (BMDM)expressed the mature macrophage markers Mac-1 and Fc�RII/III, and they werecytokine starved prior to treatment with PGN (10 �g/ml) or LPS (1 �g/ml).
Detection of PGN in blood. Defibrinated sheep blood was infected with asingle mucoid colony of B. anthracis strain Ames 34 and incubated at 37°Covernight in the presence of 20% CO2 to obtain actively growing capsulatedbacteria. The following day, the blood was diluted 1:10 in fresh defibrinatedblood and incubated for an additional 6 h at 37°C. Serum was collected afterincubation by centrifugation, filtered through a 0.22-�m filter, and heated at80°C for 10 min. The serum was then incubated with silkworm larva plasmareagent at 30°C for 90 min. Peptidoglycan was detected spectrophotometricallyat 650 nm and was quantitated using a standard curve.
Flow cytometry analysis. For detection of cytokines and chemokines by flowcytometry, diluted blood was treated with PGN (10 �g/ml) or LPS (1 �g/ml) for6 h in the presence of brefeldin A (3 �g/ml) to inhibit secretion of cytokines andchemokines. Following treatment, the cells were suspended in 100 �l of fluores-cence-activated cell sorting buffer (1� phosphate-buffered saline [PBS], 3% fetalbovine serum) containing brefeldin A and incubated with human IgG for 10 minon ice to block Fc receptors (36). Cells were then incubated with appropriate cellsurface antibodies for 20 min on ice. The samples were treated with ACK lysisbuffer for 5 min at room temperature to lyse the red blood cells. The white bloodcells (WBC) were then washed with PBS containing brefeldin A, fixed with 2%formaldehyde, and permeabilized with 0.5% saponin. The permeabilized cellswere stained with antibodies against tumor necrosis factor alpha (TNF-�), in-terleukin-1� (IL-1�), or IL-8. The cells positive for the cytokines or chemokineswere identified by flow cytometry analysis by collecting 200,000 events per sam-ple. In experiments in which inhibitors were used, the diluted blood was firstpreincubated with the inhibitors for 30 min and then treated with PGN or LPS.
Microscopy. To observe internalization of PGN in WBC, diluted blood wastreated with 10 �g/ml of fluorescein isothiocyanate (FITC)-conjugated PGN(PGN-FITC) for 30 min at 37°C. The WBC were stained with unique cell surfacemarkers, fixed in 2% formaldehyde, and sorted by flow cytometry to obtain�98% pure populations of monocytes, neutrophils, and B lymphocytes. The cellswere permeabilized and stained with phalloidin conjugated to Alexa Fluor 633and 4,6-diamidino-2-phenylindole (DAPI). The cells were observed with aZeiss inverted deconvolution microscope or a Zeiss LSM 510 confocal micro-scope using a 63� oil objective.
For colocalization experiments, diluted blood was treated with 10 �g/ml ofPGN-FITC for 60 min at 37°C. The WBC were stained with unique cell surfacemarkers, fixed in 2% formaldehyde, and sorted by flow cytometry to obtain�98% pure populations of monocytes and neutrophils. The cells were thenpermeabilized, blocked with 3% bovine serum albumin (BSA) in PBS, andstained with an antibody against LAMP1 conjugated to Alexa Fluor 647. Thecells were then observed with a Zeiss LSM 510 confocal microscope. All micros-copy images were prepared using Adobe Photoshop.
Semiquantitative PCR analysis. Purified monocytes, neutrophils, B lympho-cytes, and T lymphocytes were obtained by flow cytometry and were lysed inTrizol. Total RNA was isolated, and cDNA was synthesized from 1 �g of RNAusing the Superscript First Strand synthesis system for reverse transcription-PCR(RT-PCR). Semiquantitative PCR was performed using Sybr green PCR mastermixture and primers corresponding to the actin, NOD1, or NOD2 sequence. Thefollowing primers were used for amplification of actin: forward primer 5-ACAACGGCTCCGGCATGTGCAA-3 and reverse primer 5-CATGTCGTCCCAGTTGGTGACGAT-3. The NOD primers have been described previously (24).Their sequences are as follows: for NOD1, forward primer 5-TCCAAAGCCAAACAGAAACTC-3 and reverse primer 5-CAGCATCCAGATGAACGTG-3; and for NOD2, forward primer 5-GAAGTACATCCGCACCGAG-3 andantisense primer 5-GACACCATCCATGAGAAGACAG-3. DNA was ampli-fied with the 7500 real-time PCR system (Applied Biosystems, Foster City, CA)using the following parameters: 10 min at 95°C, followed by 40 cycles of 95°C for15 s and 60°C for 1 min. Analysis of relative gene expression was performed asdescribed by Livak and Schmittgen (29).
VOL. 78, 2010 PHAGOCYTOSIS OF PGN 2419
on July 24, 2020 by guesthttp://iai.asm
.org/D
ownloaded from

Statistical analysis. All statistical analyses were performed using MicrosoftExcel. Statistical significance was determined by using a t test, and a P value of0.05 was considered statistically significant.
RESULTS
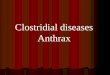
PGN is biologically available in actively growing encapsu-lated B. anthracis. Since the poly-D-glutamic acid capsule formsthe outermost layer of B. anthracis, PGN may not be biologi-cally available to stimulate immune cells. Yet, it is also formallypossible that PGN is released during growth and division of B.anthracis. To distinguish between these possibilities, we inoc-ulated defibrinated sheep blood with B. anthracis strain Ames,a fully encapsulated anthrax strain, and incubated the bacteriafor 6 h. The blood was centrifuged, and the serum was col-lected and filtered to remove vegetative bacteria. Encapsula-tion of the growing bacteria was confirmed by microscopy (datanot shown). We determined the presence of PGN in the serumby using a commercial reagent that can detect the presence ofpeptidoglycan based on the insect prophenol oxidase signalingcascade (54). As shown in Fig. 1, PGN was detected readily inthe serum of sheep infected with B. anthracis Ames and min-imally in the uninfected blood sample. These findings showthat, despite the presence of the capsule, PGN is shed andhence is accessible to immune cells during infection.
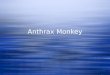
Further purification of peptidoglycan. We reported previ-ously that B. anthracis-derived PGN was a potent inducer ofproinflammatory cytokines from cells in whole human blood(26). Although the PGN biological activity was sensitive tolysozyme and not sensitive to proteases, analysis of the aminoacid composition of the PGN revealed a complex array ofamino acids, suggesting that there was contamination withbacterially derived protein. To improve the purity of B. anthra-cis PGN, we treated the SDS-extracted material with hydroflu-oric acid (HF) to remove the bound polysaccharide, as de-scribed previously (8), and treated the HF-digested productwith proteinase K. The amino acid compositions of the PGNbefore and after proteinase K treatment are shown in Fig. 2A.
We noted that the amount of pimelic acid did not decreaseafter this treatment, while the amounts of the vast majority ofthe other amino acids were greatly decreased. The majoramino acids that were present in the proteinase K-treatedsample were pimelic acid, alanine, and glutamic acid/glu-tamine, which is consistent with the amino acid residues in thePGN stem peptide of members of the family Bacillaceae (45).We next compared the ability of the proteinase K-treated PGNto elicit proinflammatory cytokines to the ability of the protein-contaminated material that we used in our previous study toelicit proinflammatory cytokines. For this experiment, wetreated human blood with the PGN preparations for 6 h, fixedand permeabilized the white blood cells, and measured theTNF-� in the cells by flow cytometry. The data are expressedhere as the percentage of CD14� monocytes that were positivefor TNF-�. The results (Fig. 2B) show that PGN inducedmonocytes to make TNF-� and that there was a minimal de-crease in the percentage of monocytes that were positive forTNF-� production following proteinase K treatment of thestimulating PGN. Lastly, we used the proteinase K-treatedmaterial in a dose-response experiment to determine the min-imal amount needed to elicit TNF-� production by humanblood monocytes. We found (Fig. 2C) that TNF-� was readilydetected with doses of PGN greater than 5 �g/ml, which issimilar to the dose needed for the undigested material andreported previously (26). This dose is comparable to the dosesof PGN used for other bacterial strains in studies evaluatingthe inflammatory role of PGN (5, 52). The data are consistentwith our previous conclusion that the biological activity in a B.anthracis PGN preparation is due to PGN itself and not to anycontaminating material.
We reported previously that blood cells produced largeamounts of TNF-�, IL-6, IL-1�, and IL-8 and that bloodmonocytes were the sole source of the TNF-� (26), yet the celltypes that released the other cytokines were not determined.We resolved the different hematopoietic populations in bloodusing unique cell surface markers (monocytes [CD14�
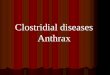
CD16b�], neutrophils [CD14� CD16b�], B lymphocytes[CD19� CD3�], and T lymphocytes [CD19� CD3�]), com-bined with forward and side scatter properties. Using this gat-ing strategy together with intracellular cytokine staining, weexamined which blood cell population produced TNF-�, IL-6,IL-1�, and IL-8. The primary data for cytoplasmic staining ofIL-8 in the four gated blood cell populations are shown in Fig.3A, and a summary for all of the cytokines and cell populationsis shown in Fig. 3B. We found that only monocytes producedIL-6 and IL-1�, while both monocytes and neutrophils pro-duced IL-8 in response to PGN. Neither lymphocyte popula-tion responded to PGN treatment.
Monocytes, neutrophils, and B lymphocytes bind to PGN.We hypothesized that lymphocytes do not respond to B. an-thracis PGN because the cells do not bind PGN. We labeledthe PGN with fluorescein isothiocyanate (FITC) to determinewhich blood cell population was able to bind PGN. First, to testwhether FITC labeling of PGN altered its biological activity,we compared unlabeled PGN and FITC-labeled PGN for in-duction of TNF-�. We found (Fig. 4A) that the percentages ofTNF-�-expressing monocytes were similar (�40%) for the twoforms of PGN, confirming that the labeling procedure did notrender the PGN inactive.
FIG. 1. PGN is shed into the serum of blood infected with activelygrowing B. anthracis strain Ames. Defibrinated sheep blood was in-fected with a single mucoid colony of B. anthracis strain Ames (Ames-34) and incubated at 37°C for 6 h. Following the incubation period,serum was obtained and tested for the presence of PGN by using thesilkworm larva plasma test. Serum obtained from uninfected blood wasused as a negative control (Uninfected). The data are the averages andstandard errors of triplicate samples, and the entire experiment wasrepeated twice.
2420 IYER ET AL. INFECT. IMMUN.
on July 24, 2020 by guesthttp://iai.asm
.org/D
ownloaded from

We evaluated the binding of PGN-FITC to WBC by incu-bating diluted peripheral blood with PGN-FITC for 30 min at4°C to prevent internalization. Following PGN incubation, thecells were stained with the distinguishing cell surface markers,and PGN-FITC binding to each individual population wasdetermined by flow cytometry. We found that in the 30-minassay, PGN bound about 40 to 50% of the neutrophils (Fig.4B) and monocytes (Fig. 4C) and about 30% of the B lympho-cytes (Fig. 4E), while T lymphocytes were not bound (Fig. 4D).A summary of the binding properties of these cells is shown inFig. 4F.
To test if the same cells that bind PGN-FITC also makeTNF-�, we electronically gated on CD14� monocytes andmeasured the levels of PGN-FITC and cytoplasmic TNF-�(Fig. 4G to I). We found (Fig. 4I) that the vast majority (91%)of TNF-�-producing monocytes also bound PGN (3% PGN�
TNF-�� cells, compared with 31% PGN� TNF-�� cells).Overall, the data show that the cells that produce proinflam-matory cytokines (monocytes and neutrophils) bind PGN,while a significant fraction of B lymphocytes bind PGN yet failto produce any detectable cytokine.
Internalization of PGN is required for TNF-� and IL-8production. PGN binding alone or binding followed by inter-nalization might induce the production of proinflammatorycytokines in blood cells. To determine whether PGN internal-ization was needed for a biological response, we treated thewhole blood with an inhibitor of actin reorganization (cytocha-lasin D or latrunculin A) and measured the percentage of
TNF-�� cells (for monocytes) or IL-8� cells (for neutrophils).We used LPS as a control since LPS responses are due tostimulation of surface CD14 and TLR4 and do not requireendocytosis. The results shown in Fig. 5A and 5B reveal thatboth of the actin reorganization inhibitors were able to blockPGN-triggered cytokine production, while neither inhibitorwas able to block the response to LPS. These findings showthat internalization of the PGN is critical for production ofTNF-� and IL-8.
We also evaluated the subcellular location of PGN in thesecells by microscopy. Peripheral blood cells were treated withPGN-FITC for 30 min at 37°C to allow complete internaliza-tion in the majority of cells. We then sorted monocytes(CD14� CD16b�), neutrophils (CD14� CD16�), and B lym-phocytes (CD19�) by flow cytometry. The sorted cells werefixed, permeabilized, and stained with Alexa Fluor 633-conju-gated phalloidin and DAPI and observed by microscopy. Oneof the optical sections (Fig. 5C upper panels) showed that thePGN-FITC was internalized by the monocyte and neutrophilpopulations. More than 80% of these cells internalized at leastone PGN particle. We also found PGN-FITC in �80% of Blymphocytes (data not shown), but due to the very narrowcytoplasm we cannot be certain that the PGN-FITC was trulyinternalized. Treatment of the cells with cytochalasin D re-sulted in disruption of the actin cytoskeleton, as expected, andblocked internalization of PGN-FITC (Fig. 5C, lower panels).Nevertheless, PGN-FITC was still able to bind to monocytesand neutrophils in the presence of cytochalasin D (Fig. 5D).
FIG. 2. PGN that is treated with proteinase K can induce TNF-� production. (A) PGN was subjected to HF treatment followed by proteinaseK digestion. The amino acid content was analyzed prior to (�proteinase K) and following (�proteinase K) proteinase K digestion. The data arerepresentative of the data from three independent experiments. Except for the amino acids alanine, tyrosine, and pimelic acid, there werestatistically significant reductions in the amounts of the amino acids following proteinase K digestion (P 0.05). (B) PB was stimulated withundigested PGN (No proteinase K) or with PGN digested with 10 �g/ml proteinase K (proteinase K) for 6 h. Different cell populations wereidentified using surface markers. TNF-� production was measured by intracellular cytokine staining and flow cytometry. The data are the averagesof three independent experiments performed using three different donors. (C) PB was treated with various doses of PGN or LPS for 6 h. TNF-�production in monocytes was measured by intracellular cytokine staining and flow cytometry. The data are the averages of three independentexperiments performed using three different donors.
VOL. 78, 2010 PHAGOCYTOSIS OF PGN 2421
on July 24, 2020 by guesthttp://iai.asm
.org/D
ownloaded from

These results are consistent with the data shown in Fig. 5A and5B indicating that the induction of cytokines requires PGNinternalization.
Lysosomal processing is required for PGN-induced TNF-�and IL-8 production. Because the PGN particle is internalized,we hypothesized that PGN traffics to the lysosome for hydro-lysis and that PGN hydrolysis is required for production ofproinflammatory cytokines by the responding cells. To test thishypothesis, we used two lysosomotropic agents, ammoniumchloride and chloroquine, and examined their effects on cyto-kine production. As shown in Fig. 6A and B, both lysosomo-tropic agents caused significant reductions in the percentage ofmonocytes expressing TNF-� and the percentage of neutro-phils expressing IL-8 following treatment with PGN. There wasno significant reduction in TNF-� production in monocytesthat were treated with LPS in the presence of these two lyso-somotropic agents, supporting the notion that LPS inducesbiological responses via surface receptors. However, we didobserve a significant reduction in IL-8 production in neutro-phils following LPS treatment in the presence of chloroquinebut not in the presence of ammonium chloride. Chloroquinecan inhibit the activity of mitogen-activated protein kinases in
some cells (53). Thus, it is possible that neutrophils are moresensitive to the effect of chloroquine than monocytes.
The results described above suggest that, after internaliza-tion, PGN traffics to the lysosome for hydrolysis. To test thispossibility, we treated cells with PGN-FITC for 1 h. Monocytesand neutrophils that bound PGN-FITC were sorted by flowcytometry by gating on the appropriate surface-stained popu-lations. The cells were then fixed, permeabilized, stained withan antibody against lysosome-associated membrane protein 1(LAMP1), and observed with a confocal microscope. Wefound that �70% of the FITC� monocytes (Fig. 6C) and�50% of the FITC� neutrophils (Fig. 6D) showed colocaliza-tion of PGN-FITC in LAMP1-containing vesicles. Thus, afterits internalization, PGN traffics to the lysosome, and both thetrafficking and lysosome function are required for productionof TNF-� in monocytes and for IL-8 production in neutrophils.
NOD expression in WBC. Our data suggest that internaliza-tion and degradation of PGN are required for recognition byan intracellular receptor. The cytoplasmic NOD receptors bindto lysosomal degradation products of PGN to stimulate cyto-kine production in the blood cells and are obvious candidatesfor this process. We first measured the levels of NOD1 and
FIG. 3. PGN can induce the production of TNF-�, IL-6, and IL-1� in monocytes and the production of IL-8 in monocytes and neutrophils.(A) PB was treated with 10 �g/ml of PGN (lower panels) for 6 h. Monocytes, neutrophils, B lymphocytes, and T lymphocytes were identified usingcell surface markers. IL-8 production was determined by flow cytometry after intracellular cytokine staining. (B) The percentages of WBCexpressing IL-8, IL-1�, TNF-�, and IL-6 following treatment with PGN or LPS were determined by flow cytometry after intracellular cytokinestaining. The data are data from three independent experiments performed using three different donors. There were statistically significant (P 0.05) increases in the percentages of monocytes that were positive for TNF-�, IL-6, and IL-1� production following PGN and LPS treatment, whileboth monocytes and neutrophils showed statistically significant increases in the percentage of cells positive for IL-8.
2422 IYER ET AL. INFECT. IMMUN.
on July 24, 2020 by guesthttp://iai.asm
.org/D
ownloaded from

NOD2 mRNA in WBC by semiquantitative PCR. Peripheralblood mononuclear cells were isolated from blood by densitygradient centrifugation and purified further by flow cytometry.Based on surface marker expression, we obtained �97% purepopulations of monocytes, neutrophils, B lymphocytes, and Tlymphocytes. RNA extracted from these cells was used to de-termine the levels of NOD1 and NOD2 mRNA by semiquan-titative real-time PCR using actin as a control. We found (Fig.7) that B lymphocytes and T lymphocytes had significantlyhigher levels of NOD1 than monocytes and neutrophils. Con-versely, monocytes and neutrophils had significantly higherlevels of NOD2 than the lymphocyte populations. We tried toevaluate the role of NODs in cytokine and chemokine produc-tion by silencing the expression of NODs using small interfer-ing RNA or short hairpin RNA in monocytes. Unfortunately,transfection of either RNA interference reagent resulted in
upregulation of the levels of both NODs following transfection(data not shown), which may have been a cellular response toexogenous nucleic acids.
Use of murine bone marrow-derived macrophages to studythe role of NODs in the PGN-induced cytokine response. In analternative approach, we used mouse bone marrow-derivedmacrophages (BMDM) from animals lacking NOD1, NOD2,or both NOD1 and NOD2. This model is a compromise sincewe were not able to cause differentiation of human monocytesto macrophages and could not isolate sufficient mouse bloodmonocytes. BMDM of wild-type animals responded to B. an-thracis PGN by producing TNF-�, although the responses weremarkedly lower than those in human cells (�20% TNF-��
murine cells compared with �50% TNF-�� human cells) (Fig.8A). Surprisingly, analysis of BMDM from NOD1�/�,NOD2�/�, and NOD1�/� NOD2�/� mice showed no differ-
FIG. 4. FITC-labeled PGN (FITC-PGN) can bind to monocytes, neutrophils, and B lymphocytes. (A) PB was treated with 10 �g/ml of PGN,PGN-FITC, or LPS for 6 h. TNF-� production in monocytes (CD14� cells) was measured by intracellular staining and flow cytometry. The dataare data from three different donors. There were statistically significant (P 0.05) increases in the percentages of monocytes that were positivefor TNF-� following treatment with PGN, PGN-FITC, or LPS compared to the unstimulated samples (NS). However, there was not a significantdifference (P � 0.05) between the percentage of monocytes positive for TNF-� treated with PGN and the percentage of monocytes positive forTNF-� treated with PGN-FITC. (B to E) PB was treated with 10 �g/ml of PGN or PGN-FITC for 30 min. Monocytes, neutrophils, B lymphocytes,and T lymphocytes (C, B, E, and D, respectively) were identified using cell surface markers, and binding of PGN-FITC to the cells was measuredby flow cytometry. (F) Percentages of cells that bound to PGN-FITC. The data are data from three independent experiments performed using threedifferent donors. There were significant increases in the percentages of monocytes, neutrophils, and B lymphocytes positive for PGN-FITC bindingcompared to the results for cells treated with unlabeled PGN. (G to I) PB was not treated (G) or was treated with PGN (H) or PGN-FITC (I) for6 h. TNF-� production in monocytes that bound to PGN-FITC was measured by intracellular cytokine staining and flow cytometry.
VOL. 78, 2010 PHAGOCYTOSIS OF PGN 2423
on July 24, 2020 by guesthttp://iai.asm
.org/D
ownloaded from

ence in the percentage of TNF-�-positive BMDM (Fig. 8A).This finding suggests that neither NOD1 nor NOD2 plays arole in PGN sensing or that there are other proteins in additionto these NODs that can sense the PGN and generate the
production of proinflammatory cytokines. We tested the latterpossibility by using cytochalasin D and ammonium chloridewith the mouse BMDM and measuring TNF-� productionfollowing PGN treatment. We found only a �50% reduction inthe percentage of murine BMDM expressing TNF-� in thepresence of either cytochalasin D or ammonium chloride (Fig.
FIG. 5. TNF-� and IL-8 production in monocytes and neutrophilsfollowing PGN treatment requires internalization of PGN. (A) PB waspretreated with dimethyl sulfoxide (DMSO), 2 �M latrunculin A (LatrA), or 10 �M cytochalasin D (Cyto D) for 30 min, which was followed byno treatment (no stimulus) or by treatment with PGN or LPS for 6 h.TNF-� production in monocytes (CD14� cells) was measured by intra-cellular staining and flow cytometry. The data are data from three inde-pendent experiments performed with three different donors. There was astatistically significant (P 0.05) decrease in the percentage of monocytesexpressing TNF-� following PGN treatment in the presence of cytocha-lasin D or latrunculin A. Such a decrease was not observed followingtreatment with LPS. NT, no pretreatment. (B) IL-8 production in neu-trophils (CD16b� cells) was measured by intracellular staining and flowcytometry following treatment with PGN or LPS in the presence of cy-tochalasin D or latrunculin A. The data are data from three independentexperiments performed with three different donors. There was a statisti-cally significant (P 0.05) decrease in the percentage of neutrophilsexpressing IL-8 following PGN treatment in the presence of cytochalasinD or latrunculin A. Such a decrease was not observed following treatmentwith LPS. (C) PB was treated with PGN-FITC (green) for 30 min at 37°Cin the presence or absence of cytochalasin D. The cell populations indi-cated were identified using cell surface markers and were sorted usingflow cytometry. Cells were fixed, permeabilized, and stained with phalloi-din (red) and DAPI (blue). Internalization of PGN-FITC was observed byusing optical sectioning. One optical section is shown. (D) PB was treatedwith PGN-FITC in the presence or absence of cytochalasin D for 30 minat 37°C. The percentages of monocytes and neutrophils that bound toPGN-FITC were determined by flow cytometry. The data shown arerepresentative data from three independent experiments performed usingthree different donors.
FIG. 6. TNF-� and IL-8 production in monocytes and neutrophilsfollowing PGN treatment is inhibited in the presence of lysosomo-tropic agents. (A) PB was pretreated with 30 mM ammonium chloride(NH4Cl) or 50 �M chloroquine (Chlq) for 30 min, which was followedby no treatment (no stimulus), PGN treatment, or LPS treatment for6 h. TNF-� production in monocytes (CD14� cells) was measured byintracellular staining and flow cytometry. The data are data from threeindependent experiments performed with three different donors.There was a statistically significant (P 0.05) decrease in the percent-age of monocytes expressing TNF-� following PGN treatment in thepresence of ammonium chloride or chloroquine. Such a decrease wasnot observed following treatment with LPS. NT, no pretreatment.(B) IL-8 production in neutrophils (CD16b� cells) was measured byintracellular staining and flow cytometry following treatment withPGN or LPS in the presence of ammonium chloride or chloroquine.The data are data from three independent experiments performedusing three different donors. There was a statistically significant (P 0.05) decrease in the percentage of neutrophils expressing IL-8 fol-lowing PGN treatment in the presence of ammonium chloride orchloroquine. A significant decrease was also observed following treat-ment with LPS in the presence of chloroquine but not in the presenceof ammonium chloride. (C and D) PB was treated with PGN-FITC(green) for 60 min at 37°C. Monocytes (C) and neutrophils (D) wereidentified by unique cell surface markers and were sorted using flowcytometry. Cells were fixed, permeabilized, and stained with LAMP1antibody (red). Colocalization of PGN-FITC and LAMP1 was ob-served using a confocal microscope by using optical sectioning. Oneoptical section is shown.
2424 IYER ET AL. INFECT. IMMUN.
on July 24, 2020 by guesthttp://iai.asm
.org/D
ownloaded from

8B and inset), while human cells were �90% inhibited. Theseresults suggest that mouse BMDM recognize PGN of B. an-thracis using an extracellular receptor, similar to LPS, in aprocess distinct from the process used by human monocytes,which appear to use only a cytoplasmic receptor and not anextracellular receptor.
DISCUSSION
In inhalation anthrax, B. anthracis produces an extraordi-narily high number of bacteria, which is probably facilitatedby anthrax toxins and the poly-D-glutamic acid capsule. Wereasoned that the high bacterial load should be accompa-nied by a high level of circulating cell wall components ofthe vegetative bacteria, including PGN. We reported previ-ously (26) that the PGN of B. anthracis is able to elicit aproinflammatory response in cells in human peripheralblood. We showed that the response was not due to thepresence of a PGN-associated polysaccharide, introducedcontaminants like Gram-negative endotoxin, bacterial nu-cleic acids, teichoic acids, or bacterial proteins that may beassociated with the PGN. However, the molecular mecha-
nism by which PGN is able to cause such a response is notclear for any Gram-positive organism. In the present study,we expanded the previous findings and examined the mo-lecular and cellular mechanisms through which B. anthracisPGN induces inflammatory responses in human WBC.
Here, we established that PGN within the cell wall of B.anthracis is bioavailable to the host, despite the fact that theorganism is surrounded by a poly-D-glutamic acid capsule. Wealso showed that PGN binds to an unidentified surface recep-tor on responding cells, but binding is not sufficient to inducecytokine production. PGN internalization, trafficking to lyso-somes, and lysosome hydrolysis are required for PGN to in-
FIG. 7. Differential expression of NOD1 and NOD2 mRNA wasobserved in WBC. Purified populations of monocytes, neutrophils, Blymphocytes, and T lymphocytes were obtained by cell sorting. cDNAwas synthesized from total RNA and subjected to PCR amplificationusing primers specific for actin, NOD1, and NOD2. The PCR mixtureswere run on a 1% agarose gel containing ethidium bromide (A).(B) Semiquantitative real-time PCR was also performed with thecDNA to determine the levels of expression of NOD1 and NOD2 invarious WBC populations. The data are data from three independentexperiments performed using three different donors. There were sta-tistically significant (P 0.05) lower levels of NOD1 mRNA in mono-cytes and neutrophils than in lymphocytes. Conversely, there werestatistically significant elevated levels of NOD2 mRNA in monocytesand neutrophils compared to lymphocytes.
FIG. 8. Mouse bone marrow-derived macrophages signal differ-ently than human monocytes. (A) TNF-� production was evaluatedby flow cytometry using mouse BMDM (obtained from wild-type,NOD1�/�, NOD2�/�, and NOD1�/� NOD2�/� mice) that weretreated with 10 �g/ml PGN or 1 �g/ml LPS for 6 h or were nottreated (NS). The data are data from two independent experimentsperformed in duplicate. There was a statistically significant (P 0.05) increase in the percentage of BMDM expressing TNF-� fol-lowing treatment with PGN or LPS compared to the results for theunstimulated samples. (B) Mouse BMDM or human monocyteswere treated with PGN in the presence or absence of DMSO,cytochalasin D, or ammonium chloride (NH4Cl). TNF-� productionwas measured by intracellular cytokine staining and flow cytometry.The data are data from three independent experiments. The data inpanel B were analyzed to evaluate the percent reductions in thenumber of human monocytes or mouse BMDM expressing TNF-�following treatment with PGN in the presence of cytochalasin D orammonium chloride (inset). There was a statistically significant(P 0.05) decrease in the percentage of human monocytes ormouse BMDM expressing TNF-� following PGN treatment in thepresence of cytochalasin D or ammonium chloride.
VOL. 78, 2010 PHAGOCYTOSIS OF PGN 2425
on July 24, 2020 by guesthttp://iai.asm
.org/D
ownloaded from

duce a biological response. This is the first report to show thatPGN from a Gram-positive organism requires internalizationand lysosomal trafficking to trigger a host response in the formof production of proinflammatory cytokines and chemokines.Mouse macrophages had a distinct mechanism for activation ofproinflammatory cytokines in that the response was less de-pendent than that of human cells on internalization and acid-ified lysosomes. While a comparison between mouse macro-phages and human monocytes is not ideal, monocytes are themacrophage precursors and the two types of cells express sim-ilar types of TLRs (20) and NODs (30). The biological re-sponse in humans was associated with cells that express NOD2,and we were not able to determine that any NOD sensor isrequired for PGN to induce cytokine production in humanblood cells. First, RNA interference strategies designed toknock down NOD expression caused upregulation of NODmRNA instead. Second, NOD-deficient mouse macrophagesresponded as well as macrophages from wild-type mice, prob-ably because PGN responses are less dependent on a cytoplas-mic sensor in mice.
In nature, B. anthracis is known to have a complex cell wallarchitecture that includes a thick peptidoglycan, a polysaccha-ride associated with the PGN, S-layer proteins, and a poly-D-glutamic acid-containing capsule (9, 10). Since the capsuleforms the outermost layer of the cell wall, it is possible that thePGN may not be accessible to the immune cells of the host.There have been several reports for other members of thefamily Bacillaceae, like Bacillus subtilis, Bacillus megaterium,and Bacillus cereus, establishing that the organisms shed PGNfragments during the logarithmic growth phase (3, 34, 35).Therefore, it is likely that B. anthracis PGN encounters humanblood cells as it grows to produce the high levels of bacteriathat have been reported (7).
PGN required internalization and trafficking to a lysosomalcompartment to induce cytokine production by blood cells.The observation that biological responses to PGN can beblocked by chemical agents that neutralize the lysosome pHsuggests that lysosomal enzymes degrade PGN to a more sim-ple moiety that can be recognized by a cytoplasmic sensor andthat PGN itself is not the stimulus for the sensor. This notionis consistent with findings that NOD ligands are lysozymeproducts of PGN digestion, including M-Tri-DAP and MDP(4, 12–14). Innate immune cells like neutrophils (6) and mono-cytes/macrophages (27) contain lysozyme in their lysosomes.Although there are no recent studies, a survey over 30 yearsago of human B-cell lymphomas (Raji, Daudi, and Ramos) andthree Epstein-Barr virus-transformed human B cells showedthat lysozyme was not present (42). Thus, human B cells maybe capable of internalizing PGN and trafficking it to lysosomesbut may not be capable of degrading it to a moiety that can berecognized by a cytoplasmic sensor.
The observation that PGN bound some cells but not othercells suggests that there is a receptor on the surface of thefraction of cells that bind. Given the dose relative to theamount of LPS that is needed to elicit proinflammatory cyto-kines from human cells with a myeloid origin, we speculate thatthe receptor has lower affinity and may not be specific forPGN. Mouse cells appear to use surface TLR2 to bind PGNfrom a variety of Gram-positive bacteria (48), although thishypothesis is controversial. Human TLR2 is able to bind PGN
(18), but whether TLR2 is an actual PGN receptor is compli-cated by the fact that previous studies often used PGN con-taminated by LTA (28). We tested the role of TLR2 in theTNF-� response to PGN by using blocking antibodies. Wefound that although neutralizing anti-TLR2 antibodies did notprevent TNF-� production with our PGN preparation, theantibodies also did not block TNF-� production induced by theknown TLR2 ligands LTA and Pam3CSK4 (data not shown).However, we observed that there was no increase in PGNbinding to HEK293 cells stably expressing TLR2 compared tothe binding to untransfected HEK293 cells, suggesting thatTLR2 many not be involved in the proinflammatory responseto PGN (data not shown). In any case, our finding that thebiological response to PGN requires internalization and lyso-somal trafficking is inconsistent with the hypothesis that PGNengages a surface TLR that induces intracellular signalingevents. This hypothesis for PGN is in contrast to the findingsfor LPS, which signals via CD14 and TLR4, is known to utilizeMyD88, and did not require internalization or lysosomal traf-ficking (Fig. 5 and 6).
The cytoplasmic NOD-like receptor (NLR) family mem-bers NOD1 and NOD2, which recognize M-Tri-DAP andMDP, are strong candidate cytoplasmic sensors for humanneutrophils and monocytes responding to PGN. Recently,another NLR family member, Nalp3, was shown to recog-nize muramyl dipeptide (32). Nalp3 is expressed in innateimmune cells and, interestingly, is not present in B cells(31). Both M-Tri-DAP and MDP are degradation compo-nents of peptidoglycan, making these proteins ideal candi-dates for sensing peptidoglycan. Although the innate im-mune cells express mRNA corresponding to NOD1 andNOD2, we were unable to inactivate either sensor with RNAinterference strategies and could not use a murine modelsince the cell biological features of PGN responses weredifferent in mice and humans (Fig. 8).
Death due to anthrax has been considered to be primarilydue to toxemia (1). However, since toxin-deficient B. anthracisstrains are lethal in animal models (16), it is possible that septicshock may play a larger role. There is abundant evidence thatPGN can cause pathological features similar to those caused byGram-negative endotoxin (for a review, see reference 39). Forexample, infusion of PGN from several Gram-positive organ-isms into pigs (43) or rats (40) caused production of proin-flammatory cytokines and evidence of the development of tol-erance, two features shared by Gram-negative LPS (for areview, see reference 2). PGN rapidly induces procoagulantactivity in monocytes by causing the expression of tissue factor(33), a property shared with LPS (37). Likewise, Staphylococ-cus aureus PGN can directly cause platelet aggregation in vitro(23), a feature that could contribute to disseminated intravas-cular coagulation, a clinical characteristic of severe septicemia(46). Guinea pigs infused with �90 �g PGN/100 mg (bodyweight) showed evidence of disseminated intravascular coagu-lation, and 25% of the PGN-challenged animals died within24 h (22). Our finding that PGN internalization and lysosomaltrafficking are required for a proinflammatory response revealsnew points of intervention and should help future studies ofpharmacological intervention in the treatment of B. anthracisinfections and of Gram-positive sepsis.
2426 IYER ET AL. INFECT. IMMUN.
on July 24, 2020 by guesthttp://iai.asm
.org/D
ownloaded from

ACKNOWLEDGMENT
This work was supported by NIH grant 2U19 AI062629.
REFERENCES
1. Baldari, C. T., F. Tonello, S. R. Paccani, and C. Montecucco. 2006. Anthraxtoxins: a paradigm of bacterial immune suppression. Trends Immunol. 27:434–440.
2. Biswas, S. K., and E. Lopez-Collazo. 2009. Endotoxin tolerance: new mech-anisms, molecules and clinical significance. Trends Immunol. 30:475–487.
3. Chaloupka, J., and P. Kreckova. 1971. Turnover of mucopeptide during thelife cycle of Bacillus megaterium. Folia Microbiol. (Praha) 16:372–382.
4. Chamaillard, M., M. Hashimoto, Y. Horie, J. Masumoto, S. Qiu, L. Saab, Y.Ogura, A. Kawasaki, K. Fukase, S. Kusumoto, M. A. Valvano, S. J. Foster,T. W. Mak, G. Nunez, and N. Inohara. 2003. An essential role for NOD1 inhost recognition of bacterial peptidoglycan containing diaminopimelic acid.Nat. Immunol. 4:702–707.
5. Chau, T. A., M. L. McCully, W. Brintnell, G. An, K. J. Kasper, E. D. Vines,P. Kubes, S. M. Haeryfar, J. K. McCormick, E. Cairns, D. E. Heinrichs, andJ. Madrenas. 2009. Toll-like receptor 2 ligands on the staphylococcal cellwall downregulate superantigen-induced T cell activation and prevent toxicshock syndrome. Nat. Med. 15:641–648.
6. Cho, J. H., I. P. Fraser, K. Fukase, S. Kusumoto, Y. Fujimoto, G. L. Stahl,and R. A. Ezekowitz. 2005. Human peptidoglycan recognition protein S is aneffector of neutrophil-mediated innate immunity. Blood 106:2551–2558.
7. Dixon, T. C., M. Meselson, J. Guillemin, and P. C. Hanna. 1999. Anthrax.N. Engl. J. Med. 341:815–826.
8. Ekwunife, F. S., J. Singh, K. G. Taylor, and R. J. Doyle. 1991. Isolation andpurification of cell wall polysaccharide of Bacillus anthracis (delta Sterne).FEMS Microbiol. Lett. 66:257–262.
9. Fouet, A., and S. Mesnage. 2002. Bacillus anthracis cell envelope compo-nents. Curr. Top. Microbiol. Immunol. 271:87–113.
10. Fouet, A., S. Mesnage, E. Tosi-Couture, P. Gounon, and M. Mock. 1999.Bacillus anthracis surface: capsule and S-layer. J. Appl. Microbiol. 87:251–255.
11. Fraser, J. D., and T. Proft. 2008. The bacterial superantigen and superanti-gen-like proteins. Immunol. Rev. 225:226–243.
12. Girardin, S. E., I. G. Boneca, J. Viala, M. Chamaillard, A. Labigne, G.Thomas, D. J. Philpott, and P. J. Sansonetti. 2003. Nod2 is a general sensorof peptidoglycan through muramyl dipeptide (MDP) detection. J. Biol.Chem. 278:8869–8872.
13. Girardin, S. E., M. Jehanno, D. Mengin-Lecreulx, P. J. Sansonetti, P. M.Alzari, and D. J. Philpott. 2005. Identification of the critical residues in-volved in peptidoglycan detection by Nod1. J. Biol. Chem. 280:38648–38656.
14. Girardin, S. E., L. H. Travassos, M. Herve, D. Blanot, I. G. Boneca, D. J.Philpott, P. J. Sansonetti, and D. Mengin-Lecreulx. 2003. Peptidoglycanmolecular requirements allowing detection by Nod1 and Nod2. J. Biol.Chem. 278:41702–41708.
15. Guarner, J., J. A. Jernigan, W. J. Shieh, K. Tatti, L. M. Flannagan, D. S.Stephens, T. Popovic, D. A. Ashford, B. A. Perkins, and S. R. Zaki. 2003.Pathology and pathogenesis of bioterrorism-related inhalational anthrax.Am. J. Pathol. 163:701–709.
16. Heninger, S., M. Drysdale, J. Lovchik, J. Hutt, M. F. Lipscomb, T. M.Koehler, and C. R. Lyons. 2006. Toxin-deficient mutants of Bacillus anthra-cis are lethal in a murine model for pulmonary anthrax. Infect. Immun.74:6067–6074.
17. Henneke, P., S. Dramsi, G. Mancuso, K. Chraibi, E. Pellegrini, C. Thei-lacker, J. Hubner, S. Santos-Sierra, G. Teti, D. T. Golenbock, C. Poyart, andP. Trieu-Cuot. 2008. Lipoproteins are critical TLR2 activating toxins ingroup B streptococcal sepsis. J. Immunol. 180:6149–6158.
18. Iwaki, D., H. Mitsuzawa, S. Murakami, H. Sano, M. Konishi, T. Akino, andY. Kuroki. 2002. The extracellular Toll-like receptor 2 domain directly bindspeptidoglycan derived from Staphylococcus aureus. J. Biol. Chem.277:24315–24320.
19. Jernigan, J. A., D. S. Stephens, D. A. Ashford, C. Omenaca, M. S. Topiel, M.Galbraith, M. Tapper, T. L. Fisk, S. Zaki, T. Popovic, R. F. Meyer, C. P.Quinn, S. A. Harper, S. K. Fridkin, J. J. Sejvar, C. W. Shepard, M.McConnell, J. Guarner, W. J. Shieh, J. M. Malecki, J. L. Gerberding, J. M.Hughes, and B. A. Perkins. 2001. Bioterrorism-related inhalational anthrax:the first 10 cases reported in the United States. Emerg. Infect. Dis. 7:933–944.
20. Juarez, E., C. Nunez, E. Sada, J. J. Ellner, S. K. Schwander, and M. Torres.2010. Differential expression of Toll-like receptors on human alveolar mac-rophages and autologous peripheral monocytes. Respir. Res. 11:2.
21. Kengatharan, K. M., S. De Kimpe, C. Robson, S. J. Foster, and C. Thiemer-mann. 1998. Mechanism of gram-positive shock: identification of peptidogly-can and lipoteichoic acid moieties essential in the induction of nitric oxidesynthase, shock, and multiple organ failure. J. Exp. Med. 188:305–315.
22. Kessler, C. M., E. Nussbaum, and C. U. Tuazon. 1991. Disseminated intra-vascular coagulation associated with Staphylococcus aureus septicemia ismediated by peptidoglycan-induced platelet aggregation. J. Infect. Dis. 164:101–107.
23. Kessler, C. M., E. Nussbaum, and C. U. Tuazon. 1987. In vitro correlation ofplatelet aggregation with occurrence of disseminated intravascular coagula-tion and subacute bacterial endocarditis. J. Lab. Clin. Med. 109:647–652.
24. Kim, J. G., S. J. Lee, and M. F. Kagnoff. 2004. Nod1 is an essential signaltransducer in intestinal epithelial cells infected with bacteria that avoidrecognition by Toll-like receptors. Infect. Immun. 72:1487–1495.
25. Kobayashi, K. S., M. Chamaillard, Y. Ogura, O. Henegariu, N. Inohara, G.Nunez, and R. A. Flavell. 2005. Nod2-dependent regulation of innate andadaptive immunity in the intestinal tract. Science 307:731–734.
26. Langer, M., A. Malykhin, K. Maeda, K. Chakrabarty, K. S. Williamson,C. L. Feasley, C. M. West, J. P. Metcalf, and K. M. Coggeshall. 2008. Bacillusanthracis peptidoglycan stimulates an inflammatory response in monocytesthrough the p38 mitogen-activated protein kinase pathway. PLoS One3:e3706.
27. Lemansky, P., and A. Hasilik. 2001. Chondroitin sulfate is involved in lyso-somal transport of lysozyme in U937 cells. J. Cell Sci. 114:345–352.
28. Li, H., M. M. Nooh, M. Kotb, and F. Re. 2008. Commercial peptidoglycanpreparations are contaminated with superantigen-like activity that stimulatesIL-17 production. J. Leukoc. Biol. 83:409–418.
29. Livak, K. J., and T. D. Schmittgen. 2001. Analysis of relative gene expressiondata using real-time quantitative PCR and the 2(-Delta Delta C(T)) method.Methods 25:402–408.
30. Loving, C. L., M. Osorio, Y. G. Kim, G. Nunez, M. A. Hughes, and T. J.Merkel. 2009. Nod1/Nod2-mediated recognition plays a critical role in in-duction of adaptive immunity to anthrax after aerosol exposure. Infect.Immun. 77:4529–4537.
31. Manji, G. A., L. Wang, B. J. Geddes, M. Brown, S. Merriam, A. Al-Garawi,S. Mak, J. M. Lora, M. Briskin, M. Jurman, J. Cao, P. S. DiStefano, and J.Bertin. 2002. PYPAF1, a PYRIN-containing Apaf1-like protein that assem-bles with ASC and regulates activation of NF-kappa B. J. Biol. Chem.277:11570–11575.
32. Martinon, F., L. Agostini, E. Meylan, and J. Tschopp. 2004. Identification ofbacterial muramyl dipeptide as activator of the NALP3/cryopyrin inflamma-some. Curr. Biol. 14:1929–1934.
33. Mattsson, E., T. Hartung, S. Morath, and A. Egesten. 2004. Highly purifiedlipoteichoic acid from Staphylococcus aureus induces procoagulant activityand tissue factor expression in human monocytes but is a weak inducer inwhole blood: comparison with peptidoglycan. Infect. Immun. 72:4322–4326.
34. Mauck, J., L. Chan, and L. Glaser. 1971. Turnover of the cell wall ofGram-positive bacteria. J. Biol. Chem. 246:1820–1827.
35. Mauck, J., and L. Glaser. 1970. Turnover of the cell wall of Bacillus subtilisW-23 during logarithmic growth. Biochem. Biophys. Res. Commun. 39:699–706.
36. Mehta, H., M. Glogauer, S. Becart, A. Altman, and K. M. Coggeshall. 2009.Adaptor protein SLAT modulates Fcgamma receptor-mediated phagocyto-sis in murine macrophages. J. Biol. Chem. 284:11882–11891.
37. Meszaros, K., S. Aberle, R. Dedrick, R. Machovich, A. Horwitz, C. Birr, G.Theofan, and J. B. Parent. 1994. Monocyte tissue factor induction by lipo-polysaccharide (LPS): dependence on LPS-binding protein and CD14, andinhibition by a recombinant fragment of bactericidal/permeability-increasingprotein. Blood 83:2516–2525.
38. Morath, S., A. Geyer, and T. Hartung. 2001. Structure-function relationshipof cytokine induction by lipoteichoic acid from Staphylococcus aureus. J.Exp. Med. 193:393–397.
39. Myhre, A. E., A. O. Aasen, C. Thiemermann, and J. E. Wang. 2006. Pepti-doglycan—an endotoxin in its own right? Shock 25:227–235.
40. Myhre, A. E., J. F. Stuestol, M. K. Dahle, G. Overland, C. Thiemermann,S. J. Foster, P. Lilleaasen, A. O. Aasen, and J. E. Wang. 2004. Organ injuryand cytokine release caused by peptidoglycan are dependent on the struc-tural integrity of the glycan chain. Infect. Immun. 72:1311–1317.
41. Park, J. H., Y. G. Kim, C. McDonald, T. D. Kanneganti, M. Hasegawa, M.Body-Malapel, N. Inohara, and G. Nunez. 2007. RICK/RIP2 mediates innateimmune responses induced through Nod1 and Nod2 but not TLRs. J. Im-munol. 178:2380–2386.
42. Ralph, P., M. A. Moore, and K. Nilsson. 1976. Lysozyme synthesis by estab-lished human and murine histiocytic lymphoma cell lines. J. Exp. Med.143:1528–1533.
43. Ruud, T. E., Y. Gundersen, J. E. Wang, S. J. Foster, C. Thiemermann, andA. O. Aasen. 2007. Activation of cytokine synthesis by systemic infusions oflipopolysaccharide and peptidoglycan in a porcine model in vivo and in vitro.Surg. Infect. (Larchmt.) 8:495–503.
44. Sato, S., F. Nomura, T. Kawai, O. Takeuchi, P. F. Muhlradt, K. Takeda, andS. Akira. 2000. Synergy and cross-tolerance between Toll-like receptor(TLR) 2- and TLR4-mediated signaling pathways. J. Immunol. 165:7096–7101.
45. Schleifer, K. H., and O. Kandler. 1972. Peptidoglycan types of bacterial cellwalls and their taxonomic implications. Bacteriol. Rev. 36:407–477.
46. Slofstra, S. H., C. A. Spek, and H. ten Cate. 2003. Disseminated intravascularcoagulation. Hematol. J. 4:295–302.
47. Stearns-Kurosawa, D. J., F. Lupu, F. B. Taylor, Jr., G. Kinasewitz, and S.Kurosawa. 2006. Sepsis and pathophysiology of anthrax in a nonhumanprimate model. Am. J. Pathol. 169:433–444.
VOL. 78, 2010 PHAGOCYTOSIS OF PGN 2427
on July 24, 2020 by guesthttp://iai.asm
.org/D
ownloaded from

48. Takeuchi, O., K. Hoshino, T. Kawai, H. Sanjo, H. Takada, T. Ogawa, K.Takeda, and S. Akira. 1999. Differential roles of TLR2 and TLR4 in recog-nition of gram-negative and gram-positive bacterial cell wall components.Immunity 11:443–451.
49. Takeuchi, O., T. Kawai, P. F. Muhlradt, M. Morr, J. D. Radolf, A. Zychlin-sky, K. Takeda, and S. Akira. 2001. Discrimination of bacterial lipoproteinsby Toll-like receptor 6. Int. Immunol. 13:933–940.
50. Tournier, J. N., A. Quesnel-Hellmann, A. Cleret, and D. R. Vidal. 2007.Contribution of toxins to the pathogenesis of inhalational anthrax. Cell.Microbiol. 9:555–565.
51. Triantafilou, M., and K. Triantafilou. 2005. The dynamics of LPS recogni-tion: complex orchestration of multiple receptors. J. Endotoxin Res. 11:5–11.
52. Wang, J. E., P. F. Jorgensen, M. Almlof, C. Thiemermann, S. J. Foster, A. O.Aasen, and R. Solberg. 2000. Peptidoglycan and lipoteichoic acid fromStaphylococcus aureus induce tumor necrosis factor alpha, interleukin 6(IL-6), and IL-10 production in both T cells and monocytes in a humanwhole blood model. Infect. Immun. 68:3965–3970.
53. Weber, S. M., J. M. Chen, and S. M. Levitz. 2002. Inhibition of mitogen-activated protein kinase signaling by chloroquine. J. Immunol. 168:5303–5309.
54. Yoshida, H., K. Kinoshita, and M. Ashida. 1996. Purification of a pepti-doglycan recognition protein from hemolymph of the silkworm, Bombyxmori. J. Biol. Chem. 271:13854–13860.
Editor: S. R. Blanke
2428 IYER ET AL. INFECT. IMMUN.
on July 24, 2020 by guesthttp://iai.asm
.org/D
ownloaded from