Embed Size (px)
Citation preview

Uma Mahadevan, MD, FACG
Inflammatory Bowel Disease: Updates in Therapy
Uma Mahadevan MDProfessor of MedicineProfessor of MedicineCo-Medical Director
UCSF Center of Colitis and Crohn’s Disease
’ULCERATIVE COLITIS AND CROHN’S DISEASE: THERAPEUTIC SIMILARITIES AND DIFFERENCES
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
1

Uma Mahadevan, MD, FACG
Therapeutic AgentsCrohn’s Only; UC Only
5 ASA CompoundsSulfasalazineO l 5 ASA f l ti
Biological Therapies PPD/HBV
Oral 5-ASA formulationsRectal 5-ASA
GlucocorticosteroidsSystemic steroidsTopically acting steroids (budesonide)
Antibioticsd l
/InfliximabAdlimumabCertolizumab pegolGolimumabNatalizumab (JCV Ab)Vedolizumab
Nutritional TherapiesEl t l dMetronidazole
Quinolones
ImmunosuppressivesAzathioprine or
6-mercaptopurine/TPMTMethotrexate
Elemental and polymeric formulas
Pre- and probiotics
Symptomatic AgentsAnti-diarrhealsAnti-spasmodics
Adapted from Rutgeerts PJ. Rev Gastroenterol Disord. 2004;4(suppl 3):S3-S9.
Evolving Goals of Therapy for IBD: Sustained Deep Remission and Better Long-term Outcomes
Goal Clinical Parameters Outcomes
Response
Remission
Symptoms
Endoscopy
Improved Quality of life
Hospitalization
Deep Remission Mucosal healing Avoidance of surgery Minimal/No Disability
SUSTAINED DISEASE CONTROLSame
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
2

Uma Mahadevan, MD, FACG
Sequential Therapy for UC
Disease Severityat Presentation Colectomy
Corticosteroid
Anti-TNFVedolizumabCyclosporineSevere
Moderate
AminosalicylateThiopurine
Anti-TNF/VedoImmunomod.
Therapy is stepped up according to severity at presentation or failure at prior step
Aminosalicylate
Mild
AminosalicylateInduction
Maintenance
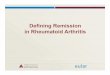
Corticosteroids: Short- and Long-term Efficacy
Complete Partial1-Month
Outcomes*(n=63)
Complete Remission
54%(n=34)
Partial Remission
30%(n=19)
No Response 16%
(n=10)
*30 days after initiating corticosteroid therapy.
Faubion W et al. Gastroenterology. 2001;121:255-260.
1-YearOutcomes
(n=63)
Steroid Dependent
22%(n=14)
Prolonged Response
49%(n=31)
Surgery 29%
(n=18)
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
3

Uma Mahadevan, MD, FACG
Infliximab in UC: The ACT1 and ACT2 Trials
Placebo 5 mg of infliximab 10 mg of infliximab
ACT 1 ACT 2100 100
**
* **
*
100
80
60
40
20
0
100
80
60
40
20
0
Pat
ien
ts w
ith
Su
stai
ned
Res
po
nse
(%
)
23.1
48.845.9
14 0
38.836.9
15.4
41.3
53.3
Rutgeerts P et al. N Engl J Med. 2005;353:2462-2476.
Response at Weeks 8 and 30
Response at Weeks 8, 30, and 54
Response at Weeks 8 and 30
*P<.001 vs placebo
14.0 15.4
100
77
IFX+AZA (n=78)
IFX (n=77)
UC Success: Combination Therapy for UC
#
40
60
80
40
77
63
22
69
55
24
50
37
( )
AZA (n=66)
Pat
ien
ts (
%)
*
#
##
0
20
Steroid-free remission Response Mucosal healing
*P < .05 compared to IFX; # P < .05 compared to AZA
Panccione R, et al. DDW 2011; Abstract 835
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
4

Uma Mahadevan, MD, FACG
Mucosal Healing and Time to Colectomy in Infliximab-treated Patients
1.00
Time to coloectomy infliximab use (weeks)
P<0.0001
endoscopy subscore = 0 endoscopy subscore = 2
0.75
0.5001 0 203 0 40 50
Colombel JF et al. Gastroenterology. 2011;141:1194-1201. 9
1 = MILD 2 = MODERATE 3 = SEVERE0 = NORMAL
endoscopy subscore = 0endoscopy subscore = 1
endoscopy subscore = 2endoscopy subscore = 3
Retrospective study of induction IFX 5mg/kg in patients who required hospitalization for acute
t id f t UC
Accelerated Infliximab Rescue Reduces Early Colectomy Rate in Acute Severe UC
severe, steroid-refractory UC
No difference in colectomy rate during IFX maintenance
Proportion of Patients Colectomy-Free Maintenance Induction
Accelerated dosing
10Gibson D, et al. Presented at DDW, May 3, 2014 Abstract 207.
dosing protects
against early colectomy in acute severe
UC
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
5

Uma Mahadevan, MD, FACG
Response: D 7Primary Objectives
Cyclosporine Versus Infliximab In Severe Acute Ulcerative Colitis Refractory To Intravenous Steroids: A Randomized Trial
p=0.97
85.4% 85.7%
40%
60%
80%
100%
Difference Cys vs. IFX: -0.3% (95%CI: -13.3 to 12.8%)
p=0.4960%
54%
40%
60%
80%
100% Difference Cys vs. IFX failure rates: -6.4% (95%CI: - 24.8 to 12.0%)
Response: Lichtiger score < 10 and decrease ≥ 3 points as compared to baseline
0%
20%
Cys (n=55) IFX (n=56)
0%
20%
Cys (n=55) IFX (n=56)
Laharie et al. Lancet. 2012 Dec
Clinical Response, Remission, Mucosal Healing at 6 Weeks
P<0.0001
P=0.0012
Vedolizumab for Ulcerative Colitis: Gemini
P=0.0009%
Δ 21.711.6, 31.7
Δ 11.54.7, 18.3
Δ 16.16.4, 25.995% CI:
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
6

Uma Mahadevan, MD, FACG
• Prospective, double blind RCT– 53 active UC patients (Mayo score ≥ 4 with
endoscopic Mayo subscore ≥ 1)– Negative for C. difficile
UC Patients Failed to Show Significant Improvement after Fecal Microbiota Therapy (FMT)
IBDQ at Week 6
g ff– 42% on steroids, 19% on immunomodulators,
and 9% on biologics– 6 weeks of once-weekly fecal microbiota therapy
delivered by retention enemas (n = 27) vs placebo delivered by water enemas (n=26)
• Results– No difference in remission between groups at
week 6 (assessed by Mayo score, IBDQ and EQ-5D)– No adverse events related to FMT
Mayo Score at Week 6
• Limitations– Short duration (6 weeks) – Small sample size
Moayeddi P, et al. Presented at DDW; May 5, 2014. Abstract 929c
Summary of UC Therapies• Mild to Moderate disease:
• Mesalamine (oral ± topical) induction and maintenance for mild-moderate disease (2.4-4.8 gm induction and maintenance)
• Topical Therapy
• Moderate to Severe disease:• Corticosteroid induction for moderate-severe disease
• Thiopurines maintain steroid-induced remission
• Anti-TNF agents for moderate to severe disease, steroid-refractory induction or steroid-dependent maintenance (± thiopurine)
• Vedolizumab: same indications as anti-TNF. Can be first line biologic
S Di• Severe Disease:• Intravenous steroids
• ? High dose infliximab
• ? Cyclosporine
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
7

Uma Mahadevan, MD, FACG
Biologic Agents in Crohn’s Disease: Dosing Recommendations
Agent RouteDosing Regimen
Induction MaintenanceInfliximab IV 5 mg/kg at weeks
0, 2, and 65 mg/kg every 8 weeks 10 mg/kg in lost response
Adalimumab SC 160 mg week 0, 80 mg week 2,40 mg week 4
40 mg every 2 weeks
g
Certolizumab SC 400 mg at weeks 0, 2, and 4
400 mg every 4 weeks
Vedolizumab IV 300 mg at weeks 0,2,6
300 mg every 8 weeks
Natalizumab IV --- 300 mg every 4 weeks
Safety of Starting Full Weight-Based Dosing vs Low-Dose Thiopurines in Normal Metabolizers (TPMT >25)
• Retrospective study of 134 adult CD patients with TPMT > 25
Complication Rates in Patients Starting Full-Dose Thiopurines vs. Controls (Gradual Increase)
CD patients with TPMT > 25 (normal metabolizers) and > 1 year follow-up
– Dose initiation at 2-2.5mg/kg AZA or 1-1.5 mg/kg 6MP (therapy) compared with gradual increase (control)
• Results– Overall similar rates of AEs
Adverse Event Comparison*
– 90% of complications in both groups occurred in first 3 months
Benmassauod A, et al. Presented at DDW; May 4, 2014. Abstract Su1416.
Starting thiopurines at full weight-based dosing in patientswith TPMT > 25 appears safe
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
8

Uma Mahadevan, MD, FACG
Risk of Lymphoma Returns to Normal after Stopping Thiopurines
• 36,891 VA patients with UC with a median f ll f 6 7 d di f 60follow up of 6.7 years and a median age of 60 years at inclusion –4,734 patients using thiopurines; median duration
of exposure : 0.97 years
Thiopurine use Incidence Rate (per 1000 py)
Unexposed 0.6
During 2.3
After stopping 0.3
• 142 confirmed lymphomacases
17
Methotrexate
• 25 mg SQ weekly shorter onset of efficacy25 mg SQ weekly, shorter onset of efficacy– 39% MTX vs 19% placebo CR (p=.025)
• Monitor CBC, liver enzymes, ?liver biopsy• Folic Acid 1 mg QD• 15 mg maintenance, 65% vs 39% (p=.04)
– Maintain with 15-25 mg q week
• Avoid use in obese, ETOH, DM, conception• **12.5 mg orally weekly as concomitant
immunomodulator (UC or CD)Feagan N Engl J Med. 2000 Jun 1;342(22):1627-32
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
9

Uma Mahadevan, MD, FACG
Induction and Maintenance of Response and Remission
Primary Endpoint100
SONIC: Corticosteroid-Free Clinical Remission at Week 26
30.6
44.4
56.8
40
60
80
100
rtio
n o
f P
atie
nts
(%
)
P<0.001
P=0.006 P=0.022
0
20
Pro
po
r
AZA + placebo IFX + placebo IFX+ AZA
52/170 75/169 96/169
Colombel N Engl J Med 2010; 362:1383-1395
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
10

Uma Mahadevan, MD, FACG
Gemini 2 and 3: Vedolizumab for Maintenance of CD
• Responders randomized 1:1:1 VDZ Q4W Q8W placebo from 6–VDZ Q4W, Q8W, placebo from 6–52 weeks
– Open-label VDZ Q4W if no clinical response at 6 weeks compared to placebo
– Extension of induction trial for 6-week responders
• Maintenance at week 52
21
– Cohorts 1+ 2– Among those with Clin Rem at
week 6, still in Clin Rem at week 52
Sandborn N Engl J Med. 2013 Aug 22;369(8):711-21
VDZ is effective as maintenance therapy in Crohn’s disease. Induction therapy may
take longer than 6 weeks.
• 21 patients with anti-TNF antibody-induced psoriasis prospectively recruited from 434 anti TNF treated IBD patients; Genotyping for IL23R and IL12B variants performed
Anti-TNF Antibody-Induced Psoriaform Skin Lesions Respond to Ustekinumab
anti-TNF treated IBD patients; Genotyping for IL23R and IL12B variants performed
• Results:– 19/331 CD – 5.7% , 2/103 UC patients – 1.3%– Predictors of skin lesions using multivariate analysis:
• Smoking ( OR 4.24, 95%CI 1.55-13.6; P=0.007)• Increased BMI (OR 1.12, CI 1.01-1.24; P=0.029)
– 7/21 with severe skin lesions and/or alopecia treated with ustekinumab – 100% response
l• Conclusions:– Anti-TNF antibody-induced psoriasiform skin lesions are not uncommon– Smoking and increased BMI are predictors– Ustekinumab can be used to successfully treat severe cases– Dose effect in development of psoriasiform lesions were not analyzed, and no dose or frequency
reduction was attempted– Genetic factors predict severe cases – IL23R and IL12B variants
Tillack C, et al. Gut. 2014 Apr;63(4):567-77
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
11

Uma Mahadevan, MD, FACG
Treatment Algorithm in IBD Patients With Clinical Symptoms (Infliximab and HACA Concentrations)
Subtherapeutic IFX Therapeutic IFX Positive HACA
Change to another anti-TNF agent
persistent disease
Increase infliximab dose or
frequency
Change to different anti-TNF
agent
concentrationconcentration
Active disease on endoscopy/radiology?
Change to Investigate
yes no
Change to non–anti-TNF agent
Change to non–
anti-TNF agent
Change to different anti-TNF
agent
Change to different anti-TNF
agent
Investigate alternate etiologies
Afif W et al. Am J Gastroenterol 2010;105:1133Slide Courtesy of Dr. EVL
Do you need to use full dose azathioprine for immunogenicity prevention?
• Cross-sectional study of IBD patients (N=72, 63% CD) receiving IFX in combination with a thiopurine for ≥4 months
Comparison Between Groups Withand Without Detectable Antibodies to IFX (ATI)
Correlation Between 6-TGN and IFX C t ti and Without Detectable Antibodies to IFX (ATI)IFX Concentrations
Higher 6-TGN levels correlate with higher IFX trough concentrations but levels of 125 may maximize IFX levels
Patients with detectable IFX abs had significantly lower 6TGN levelsYarur A, et al. Presented at DDW, May 5, 2014 Abstract 788.
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
12

Uma Mahadevan, MD, FACG
• 115 Crohn’s disease patients on combination therapySt id f i i f t l t 6 th
Can you stop anti-TNF? The STORI Trial
• Steroid-free remission for at least 6 months• Infliximab therapy stopped, immunomodulator continued
1.0
0.4
0.6
0.8
0.2po
rtio
n W
ith
ou
t R
ela
ps
e 1.0
0.4
0.6
0.8
rtio
n W
ith
ou
t R
elap
se
Number ofdeleterious
factors
2
3
4
Louis E, et al. Gastroenterology. 2012;142(1):63.
• Deleterious factors included: steroids within the year; no prior surgery; male; hemoglobin ≤ 14.5; white blood cell count > 6.0; any endoscopic activity; hsCRP ≥5; infliximab trough ≥ 2; fecal calprotectin ≥ 300μg/g
0.00 3318
Months Since Infliximab Withdrawal
Pro
p
12 309 276 243 2115
0.2
0.00 3318
Months Since Infliximab WithdrawalP
rop
o12 309 276 243 2115
4
>4
115 3849 1559 2979 32100 3247No. at risk
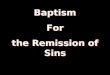
• 113 patients with luminal CD treated with > 1 year IFX/IS combination in stable steroid-
Close Monitoring of CRP and Fecal Calprotectin is Able to Predict Clinical Relapse in Patients with CD in Remission after Infliximab Withdrawal: A Sub-Analysis of
the STORI Study
95%
CI/µ
g/g
) 30
20
25
15
P<0.001
Non-relapsersR l
CRP Evolution
free remission for > 6 months (STORI), with discontinuation of IFX
• 51 (45%) with relapse at median of 10 months
• In relapsers, higher median CRP and calprotectin during follow-up but also a sudden
CR
P (
mea
n,
-14Time before relapse or end of follow-up (months)
-6 00
10
5
15
N patients withCRP measurement inrelapsers/non-relapsers
-12 -10 -8 -4 -2
3/33 6/36 5/34 12/39 14/44 27/45 31/49 41/50
Relapsers
CI/
µg
/g)
1200
1000
P=0.001
Calprotectin Evolution
pand pronounced increase in CRP and calprotectin during 4 months prior to relapse
• CRP of 6.1mg/L and calprotectin of 305mcg/g best for prediction of relapse
De Suray N, et al. Presented at DDW; May 21, 2012. Abstract 864.
Cal
pro
(m
ean
, 95%
C
-14Time before relapse or end of follow-up (months)
-6 00
400
800
200
600
N patients withCalpro measurement inrelapsers/non-relapsers
-12 -10 -8 -4 -2
4/35 6/39 6/39 9/41 11/36 27/43 33/43 37/45
Non-relapsersRelapsers
IFX, infliximab; IS, i t
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
13

Uma Mahadevan, MD, FACG
• Aim: Assessing efficacy and tolerability of adalimumab
Can you switch the anti-TNF?CD patients in remission
(HBI score <8) for >6 months on IFX (n=29)
tolerability of adalimumab (ADA) therapy after an elective switch from infliximab (IFX) in CD patients in remission. (Open-label single-center study)
• Primary endpoint: Dose intensification or termination of ADA therapy
Switch to ADA(Mean follow-up 50 weeks)
8/29 (28%) discontinued ADA therapy (50% due
to AE and 50% lost response)
21/29 (72%) remained in remission (1 patient
needed dose intensification)
of ADA therapy
4 patients were re-started on IFX (2 patients lost response;1 patient needed dose intensification)
Hoentjen F, et al. Presented at DDW; May 19, 2012. Abstract 268.
An elective switch from IFX to ADA carries the risk of losing response to IFX in a subset of patients.
AE, adverse eventHBI, Harvey-Bradshaw Index
Summary of Crohn’s Therapy
• Mesalamine does not work for CD (mild colonic ok)• Steroids/Budesonide: induction• Azathioprine/Methotrexate: steroid sparing and
concomitant immuomodulator– Full dose Aza (?), 12.5 weekly MTX
• Anti-TNF (infliximab, adalimumab, certolizumab) induction and maintenance of remission in moderate to severe disease (+/- immunomodulator)
• Vedolizumab for induction/maintenance of remission in moderate-severe Crohn’s (+/- immunomodulator)
• Natalizumab in JCV (-) patients failing anti-TNF/Vedo• Ustekinumab anecdotal evidence
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
14

Uma Mahadevan, MD, FACG
THANK YOU!
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
15