Embed Size (px)
Citation preview

Inflammatory Biomarkers in Cardiovascular
diseases
By
Ståle Haugset Nymo
for
PhD Supervisor: Arne Yndestad
Research Institute of Internal Medicine
Oslo University Hospital
University of Oslo
2016

© Ståle Haugset Nymo, 2017 Series of dissertations submitted to the Faculty of Medicine, University of Oslo ISBN 978-82-8333-386-2 All rights reserved. No part of this publication may be reproduced or transmitted, in any form or by any means, without permission. Cover: Hanne Baadsgaard Utigard. Print production: Reprosentralen, University of Oslo.

3
Acknowledgment The studies this thesis is based on were performed at the Research institute of Internal
medicine at Oslo university hospital, Rikshospitalet, Oslo during the years 2010-2015, and I
greatly appreciate the outstanding working facilities provided throughout my studies. This
has been an excellent place both to work and socialize, and have made my research a lot more
fun and interesting.
To me supervisor, Arne Yndestad, I extend my profoundest gratitude. From the very first day
I came to the institute, he has always been forthcoming, helpful and available for questions
and discussions. While giving me a lot of room to experiment, he has always reined me in
when I’ve strayed too far away, and guided my back on track.
I would also extend my deepest gratitude to Pål Aukrust and Lars Gullestad, for having faith
in me when I first came to the institute, giving me the responsibility for statistics I might not
have been qualified for, and patient while I slowly found my way through the statistical
quagmire. Your feedback have been invaluable, and this thesis would have been possible
without all help and guidance.
Thor Ueland, thank you for making my time at the office so much more fun, always finding
time for discussions, advice, and conversations. Most of my work would not have been
possible without your input, and countless hours in the lab.
To all my co-workers and friends at the institute, this would not have been possible, and more
importantly, no fun without you!
Last but not least, and I want to thank my wife Kari for always being there, patiently waiting
when I’ve had to work long hours, and making my life what it is. And of course I need to
thank my daughter Ingrid for smiling most of the times I came home.
Oslo, March 2016
Ståle H. Nymo

4
Table of Contents Acknowledgment .................................................................................................................. - 3 -
Table of Contents .................................................................................................................. - 4 -
List of papers......................................................................................................................... - 7 -
Abbreviations and glossary ................................................................................................... - 8 -
1 Introduction ................................................................................................................. - 11 -
1.1 Cardiovascular diseases........................................................................................ - 11 -
1.1.1 Heart failure .................................................................................................. - 11 -
1.1.2 Acute coronary syndrome ............................................................................. - 15 -
1.1.3 Biomarkers in cardiovascular diseases ......................................................... - 17 -
1.1.4 Prognosis assessment in ACS and HF .......................................................... - 19 -
1.2 Inflammation in cardiovascular diseases.............................................................. - 20 -
1.2.1 Initiation of inflammation ............................................................................. - 21 -
1.2.2 Cytokines ...................................................................................................... - 23 -
1.2.3 Neutrophil granulocytes ................................................................................ - 23 -
1.2.4 Resolution of inflammation .......................................................................... - 25 -
1.2.5 Inflammation in chronic heart failure ........................................................... - 26 -
1.2.6 Inflammation in acute coronary syndrome ................................................... - 28 -
1.3 NGAL ................................................................................................................... - 31 -
1.3.1 General properties ......................................................................................... - 31 -
1.3.2 NGAL in disease ........................................................................................... - 31 -
1.3.3 NGAL as a biomarker ................................................................................... - 32 -
2 Aims ............................................................................................................................ - 33 -
3 Material and Methods ................................................................................................. - 34 -
3.1 Patients ................................................................................................................. - 34 -
3.1.1 The CORONA study ..................................................................................... - 34 -
3.1.2 The PRACSIS study ..................................................................................... - 34 -

5
3.2 Blood sampling .................................................................................................... - 34 -
3.3 ELISA................................................................................................................... - 35 -
3.4 Multiplex .............................................................................................................. - 35 -
3.5 Statistical methods................................................................................................ - 35 -
4 Results ......................................................................................................................... - 37 -
4.1 Paper I .................................................................................................................. - 37 -
4.2 Paper II ................................................................................................................. - 38 -
4.3 Paper III ................................................................................................................ - 39 -
4.4 Paper IV................................................................................................................ - 40 -
5 Discussion ................................................................................................................... - 41 -
5.1 Analysis of circulating biomarkers in clinical materials ...................................... - 41 -
5.1.1 Collection of samples .................................................................................... - 41 -
5.1.2 ELISA ........................................................................................................... - 42 -
5.1.3 Multiplex ....................................................................................................... - 43 -
5.2 Statistical considerations ...................................................................................... - 44 -
5.2.1 The assumptions of the cox model................................................................ - 44 -
5.2.2 Missing values .............................................................................................. - 45 -
5.2.3 A model’s discrimination: Harrell’s C statistics and NRI ............................ - 46 -
5.2.4 Validation of prognostic models ................................................................... - 47 -
5.3 Inflammation in cardiovascular disease: biomarkers, players, and potential
therapeutic targets. .......................................................................................................... - 48 -
5.3.1 Inflammatory biomarkers in HF ................................................................... - 48 -
5.3.2 NGAL; potentials and difficulties. ................................................................ - 49 -
5.3.3 Neutrophils, an important cell type in CVD? ............................................... - 50 -
5.3.4 Inflammation in HF: a way ahead? ............................................................... - 51 -
5.4 Biomarkers, any use beyond prognosis? .............................................................. - 52 -
5.4.1 Current status ................................................................................................ - 52 -

6
5.4.2 Biomarkers as pathophysiological informants .............................................. - 53 -
5.4.3 Biomarkers as source of new hypotheses ..................................................... - 53 -
5.4.4 Should there be a shift of focus in biomarker research? ............................... - 54 -
6 Concluding remarks and future work ......................................................................... - 56 -
7 References ................................................................................................................... - 58 -

7
List of papers The thesis is based on the following papers, referred to by their roman numerals:
I. The association between neutrophil gelatinase-associated lipocalin and clinical
outcome in chronic heart failure: results from CORONA. Ståle H. Nymo. Thor Ueland. Erik T. Askevold. Trude H. Flo. John Kjekshus. Johannes Hulthe. John Wikstrand.
John J.V. McMurray. Dirk J. van Veldhuisen. Lars Gullestad. Pål Aukrust. Arne Yndestad
J Intern Med. 2012; 271:436-43
II. Serum Neutrophil Gelatinase-Associated Lipocalin (NGAL) is independently
associated with mortality in acute coronary syndromes. Ståle H. Nymo, Marianne Hartford, Thor Ueland, Arne Yndestad, Erik Lorentzen, Katarina Truvé, Thomas
Karlsson, Pål Aukrust, Kenneth Caidahl
Submitted manuscript
III. Inflammatory cytokines in chronic heart failure: interleukin-8 is associated with
adverse outcome - results from CORONA. Ståle H. Nymo, Johannes Hulthe, Thor Ueland, John J.V. McMurray, John Wikstrand, Erik T. Askevold, Arne
Yndestad, Lars Gullestad, Pål Aukrust
Eur J Heart Fail. 2014; 16:68-75
IV. Limited added value of circulating inflammatory and extracellular matrix
biomarkers in multimarker models for predicting clinical outcomes in chronic heart
failure. Ståle H. Nymo, Pål Aukrust, John Kjekshus, John J.V. McMurray, John G.F. Cleland, John Wikstrand, Pieter
Muntendam, Ursula-Henrike Wienhues-Thelen, Roberto Latini, Erik T. Askevold, Jørgen Gravning, Christen P.
Dahl, Kaspar Broch, Arne Yndestad, Lars Gullestad, Thor Ueland
Submitted manuscript

8
Abbreviations and glossary
ACE Angiotensin converting enzyme
ACS Acute coronary syndrome
AKI Acute kidney injury
Apo Apolipoprotein
AT2 Angiotensin-2
BMI Body mass index
BNP Brain natriuretic peptide
CAD Coronary artery disease
CKD Chronic kidney disease
cNRI Continuous net reclassification improvement
CRP C-reactive protein
CRS Cardio-renal syndrome
CVD Cardiovascular diseases
DAMP Danger associated molecular pattern
ECM Extracellular matrix
EF Ejection fraction
eGFR Estimated glomerular filtration rate
ELISA enzyme-linked immunosorbent assay
GRACE Global registry of acute coronary event
HF Heart failure
HFpEF Heart failure with preserved ejection fraction
HFrEF Heart failure with reduced ejection fraction

9
HR Hazard ratio
IL Interleukin
IFN Interferons
LBBB Left bundle branch block
LDL Low density lipoprotein
LPS Lipopolysaccharide
LV Left ventricle
MCP Monocyte chemoattractant protein
mLDL Modified low density lipoprotein
MMP Matrix metalloproteinase
MPO Myeloperoxidase
NET Neutrophil extracellular trap
NGAL Neutrophil gelatinase-associated lipocalin
NP Natriuretic protein
NSTEMI No-ST-elevation Myocardial infarction
NT-proBNP N-terminal pro-brain natriuretic peptide
NYHA New York heart association
PCI Percutaneous coronary intervention
PDGF Platelet derived growth factor
PRR Patter recognizing receptor
RAS Renin-angiotensin-aldosterone system
ROS Reactive oxygen species
SLPI Secretory leukocyte protease inhibitor
SMC Smooth muscle cell

10
SNS Sympathetic nervous system
STEMI ST-elevation Myocardial infarction
sTNF-R Soluble TNF receptor
TGF Transforming growth factor
TIMI Thrombolysis in myocardial infarction
TLR Toll-like receptor
TNF Tumor necrosis factor
UA Unstable Angina
ΔC Change in Harrell’s C statistics

11
1 Introduction
1.1 Cardiovascular disease Cardiovascular diseases (CVD) are diseases involving the heart, the blood vessels, or both,
and are the number one cause of death globally. 17.3 million people died from CVD in 2008,
representing 30% of all deaths worldwide, and CVD is projected to remain the leading cause
of death in all foreseeable future.3, 4 While great progress has been made in both diagnostics
and treatment of CVD, the increasing number of deaths worldwide underlines the need for
further research into both pathophysiological mechanisms and treatment. While many
pathological processes are thought to be involved in CVD, several lines of evidence support
an important role for inflammation in the development and progression of these diseases.
This suggests that inflammation and inflammatory biomarkers could be a source of important
prognostic information, as well as potentially representing a therapeutic target. However, due
to the complexity of the immune system, and intricacy of the inflammatory response, this
potential is yet largely unrealized and further research is needed to entangle the meshwork of
consequences of inflammatory activity in CVD.
1.1.1 Heart failure
Definition, epidemiology and etiology
Heart failure (HF) is defined by the European Society of Cardiology as an abnormality of
cardiac structure or function leading to failure of the heart to deliver oxygen at a rate
commensurate with the requirements of the metabolizing tissues, despite normal filling
pressures (or only at the expense of increased filling pressures).5 It is further defined
clinically as a syndrome in which patients have typical symptoms (e.g. breathlessness, ankle
swelling, and fatigue) and signs (e.g. elevated jugular venous pressure, pulmonary crackles,
and displaced apex beat) resulting from an abnormality of cardiac structure or function.5
It is estimated that there are 23 million people affected by HF worldwide.6 Approximately 2%
of the adult population in developed countries has HF, with prevalence of up to 10% among
patients older than 75 years of age.7 There also seems to be an increasing prevalence of HF
probably due to better treatment of CVD, prolonged life span and improved diagnosis.8
There is a significant morbidity and mortality associated with HF. It is not only the most
common condition leading to hospital admission for people above the age of 65, the 5 year
survival rate is also poor with an estimate of 40-50% mortality.9, 10 The high morbidity,

12
multiple hospital admissions and mortality rate lead to HF being a major socioeconomic
burden, representing as much as 2% of medical expenditures in the West.11, 12
Functionally, approximately 50% of patients with HF have a reduced left ventricular ejection
fraction (HFrEF), while the remaining half has preserved left ventricular ejection fraction
(HFpEF).5, 13 While HFrEF mainly encompasses disturbance in systolic left ventricular (LV)
function, HFpEF is predominantly a diastolic failure.5, 13 In this thesis, our main focus has
been patients with HFrEF, and we will mainly discuss features of HF of this etiology. The
most common cause of HF in the Western world is ischemic heart disease accounting for
about two thirds of the HFrEF cases. Other causes are cardiomyopathy, congenital and
valvular heart disease. 5, 7
Pathogenesis of HF
HF is a progressive disorder initiated by an index event that either damages the heart muscle
or disrupts the ability of the myocardium to generate force resulting in a decline in the heart’s
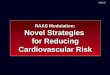
pumping capacity (Figure 1).14 This index event may be acute such as a myocardial infarction
(MI) or acute myocarditis, or it may have a gradual onset as in the case of hemodynamic
overload, for example due to
hypertension or valvular
disease. The decline in
pumping capacity leads to
activation of mechanisms that
compensate for and in many
cases restore the myocardial
function. These compensatory
mechanisms involve increased
heart contractility through
Frank-Sterling mechanisms,
activation of the sympathetic
nervous system (SNS) and the
renin-angiotensin-aldosterone
system (RAAS), as well as
remodeling of the ventricles (see
below). Over time, however,
Figure 1. Pathogenesis of HF. Myocardial injury and stresscan depress cardiac function, which in turn may cause activation of the sympathetic nervous system (SNS) and the renin-angiotensin-aldosterone system (RAAS) and the elaboration of endothelin, arginine vasopressin (AVP), and inflammatory cytokines such as tumor necrosis factor (TNF). In acute heart failure (left), these are adaptive and tend to maintain arterial pressure and cardiac function. In chronic heart failure (right), they cause maladaptive hypertrophic remodeling and apoptosis, which cause further myocardial injury and impairment of cardiac function. The horizontal line on the right shows that chronic maladaptive influences can be inhibited by angiotensin converting enzyme inhibitors, β-adrenergic blockers, angiotensin II type 1 receptor blockers, and/or aldosterone antagonists. Figure from Braunwald 20131

13
these compensatory or adaptive mechanisms may turn maladaptive, possibly due to
secondary damage to the heart, leading to a transition from asymptomatic to symptomatic and
decompensated HF.14 In HFrEF, cardiac output decreases, and leads to an increase in
angiotensin II (ATII) partly because of reduced renal arterial pressure and increased renal
venous pressure leading to renin release. Furthermore, SNS activity is increased due to fall in
systemic arterial pressure, and probably through central stimulation of the SNS by a
combination of factors including decreasing nitric oxide (NO) and increasing afferent renal
sympathetic nerve activity.15 In addition there exist positive feedback links between RAAS
and SNS, where increasing activity in one system also increases the activity in the other. This
is among other factors due to centrally stimulating effects of ATII and SNS on renal blood
flow, again increasing RAAS activity. RAAS and SNS both take part in volume retention in
HF. Several other factors as well, such as decreasing levels of NO, increased adenosine A1
receptor activation and increased vasopressin-mediated volume control all act synergistically
to increase volume.15-17 This increased sodium and water retention lead to an expansion of the
extracellular fluid that increase preload and afterload of the heart, leading to cardiac dilatation,
decrease of function and thereby worsening HF.18 This close link between renal and cardiac
function in HF have led to the coining of cardio-renal syndrome (CRS), underscoring the
importance of dysfunction in one of the organs for the function of the other. In addition to
fluid retention through activation of RAAS and SNS as well as different degrees of renal
dysfunction, immunologic and inflammatory mechanisms are also suggested to be involved
in developing and progression of HF (discussed in chapter 1.2.5).19
Myocardial remodeling
An important aspect of the compensatory response to reduced myocardial function is a
process commonly referred to as myocardial remodeling.20 The remodeling process consists
of a set of complex molecular and cellular events that lead to changes in both myocardial
structure and function. Neurohormonal activation with increased RAAS and SNS activity is
not only a direct compensatory mechanism of reduced cardiac function, but also an initiator
and mediator of cardiac remodeling.21 Studies suggest that also inflammation may influence
this process.22 The most prominent feature of myocardial remodeling is increased myocardial
mass, primarily due to hypertrophy of individual cardiomyocytes.23 On the other hand,
cardiomyocyte loss also occurs through necrosis and apoptosis. In addition to increasing its

14
mass, the ventricles dilate and change to a more spherical shape.24 A change in the quantity
and quality of the extracellular matrix is another hallmark of remodeling.25 This process both
contributes to ventricular dilation and also increased collagen deposition and interstitial
fibrosis. Finally, myocardial remodeling is characterized by reactivation of a fetal pattern of
gene expression. 26
The myocardial remodeling is initially thought to be favorable or adaptive and contribute to
preservation of the myocardial function. However, continued remodeling leads to progressive
impairment of the myocardial structure and become deleterious or maladaptive to the overall
function of the heart.21 The transition from compensated to decompensated HF is a key event
in the pathogenesis of HF, but the exact mechanism as well as the relative importance of the
various factors are far from clear, and this process represents an important area of HF
research.21, 23
Diagnosis and management of HF
Diagnosis of HF is dependent on typical symptoms and signs of HF, as well as objective
evidence of reduced systolic or diastolic function and the measurement of biomarkers, in
particular the natriuretic peptides. However, due to the non-specific nature of clinical findings,
it is not always easy to make an initial diagnosis of HF in early phases of the disease. In
addition to chest x-ray, ECG and routine blood work, echocardiogram as well as
measurement of brain natriuretic peptide (BNP) or N-terminal (NT)-proBNP are the most
useful tests in aiding the diagnosis of the disease. 5, 27
The main components of HF treatment have not changed over the last decade and are still
based on medical treatment with beta-blockers, angiotensin converting enzyme (ACE)
blocker, and diuretics.5 For end stage HF, surgical intervention is also warranted with
different left ventricular assistance devices, aortic balloon pumps, and finally heart
transplantation. Finally, there is increasing evidence for the use of resynchronization therapy
in certain forms of HF with left bundle branch block (LBBB), whereby pacemakers are used
to optimize the hearts depolarization patterns. All treatment options today except heart
transplantation, and to some extent resynchronization therapy, only delays the development
of disease, and most patients will suffer from a progressing HF despite optimal medical
treatment.5

15
1.1.2 Acute coronary syndrome
Definition and epidemiology
Acute coronary syndrome (ACS) is caused by coronary artery disease (CAD), and refers to a
group of symptoms caused by the sudden full or partial obstruction of one or more coronary
arteries. ACS typically comprises one of three conditions, i.e., ST-elevation myocardial
infarction (STEMI), no-ST elevation myocardial infarction (NSTEMI) and unstable angina
pectoris (UA). The typical symptoms are retrosternal pressure or heaviness (angina) with
possible radiation to the left or both arms, neck, or jaw, which may be intermittent (usually
lasting several minutes) or persistent. There might also be other symptoms such as
diaphoresis, nausea, abdominal pain, dyspnea, and syncope. However atypical presentations
are not uncommon.28 MI from CAD (i.e., STEMI or NSTEMI) is defined as detection of a
rise and/or fall of cardiac biomarker values (preferably cardiac troponin) with at least one
value above the 99th percentile upper reference limit (URL) and with at least one of the
following:29
Symptoms of ischemia.
New or presumed new significant ST-segment–T wave (ST–T) changes or new LBBB.
Development of pathological Q waves in the ECG.
Imaging evidence of new loss of viable myocardium or new regional wall motion
abnormality.
Identification of an intracoronary thrombus by angiography or autopsy.
Worldwide, CAD is the single most frequent cause of death, killing more than 7 million
people a year. The incidence rate of STEMI has decreased the last decade from about
120/100 000 in 1997, to approximately 80/100 000 in 2005. In the same time span, the
incidence rate of NSTEMI increased slightly from 126/100 000 to 132/100 000.30 Hospital
mortality is higher among STEMI patients (7%), than NSTEMI and UA (3-5%). However, at
6 months the mortality for the two groups are similar, at 12% and 13%, and long-term data
shows a two-fold higher mortality among NSTEMI and UA patients compared to STEMI
patients at 4 years. This however might be due to the difference in profile between the two
patient groups as NSTEMI and UA patients are in general older, with more co-morbidities
such as diabetes and renal failure.30, 31

16
Pathophysiology of ACS
ACS represents a life-threatening manifestation of atherosclerosis. Atherosclerosis is a
chronic, multifocal inflammatory, fibroproliferative disease of medium-sized and large
arteries mainly driven by lipid accumulation further discussed below.32 In ACS, there is
usually not only atherosclerosis, but also an acute worsening of the underlying atherosclerosis
caused by thrombosis, vasospasm or both. Thus the symptomatic lesion most often consists
of a variable mix of an atherosclerotic plaque as well as a thrombus.28
Several factors contribute to the development of ACS. Firstly, not all atherosclerotic plaques
are equally vulnerable. Certain plaques are more prone to instability and rupture. These
plaques often have a thinner fibrous cap and larger lipid core with more inflammatory
activity.32 Plaque vulnerability may also depend on wall stress, the size of the plaque as well
as the impact of flow on the luminal plaque surface.28 Instead of plaque rupture, there may
also be plaque erosion causing a thrombus to form in relation to the surface of the plaque.
This may contribute to rapid progression of the plaque and decreased luminal diameter.
Autopsy data has demonstrated a central role of thrombosis in ACS.28, 33 The thrombus
usually develops at the site of the vulnerable plaque when the highly thrombogenic lipid-rich
core is exposed by rupture. Thrombosis induced at the site of plaque rupture could increase
vessel occlusion dramatically and give a subtotal or complete occlusion of the coronary artery.
Spontaneous thrombolysis does however happen, and may explain some of the transient
episodes of ACS. There may also be embolization of the thrombus, leading to occlusion of
downstream arterioles and capillaries, leading to small areas of infarct as well as release of
cardiac markers.28
Diagnosis in ACS
While most patients with ACS present with some sort of chest pain, many patients presenting
with this symptom does not have an ACS. ACS is usually characterized by30:
Prolonged (>20min) angina pain at rest.
New onset severe angina.
Recent destabilization of previous angina.
Post-MI angina.
Prolonged pain is observed in 80% of patients with ACS, while de novo or accelerated angina
is observed in the remaining 20%. It is not possible to distinguish between STEMI, NSTEMI

17
and UA based on symptoms alone. The main classification of ACS depends on ECG
(presence or not of ST-elevation, or new left bundle branch block in probable STEMI), and
the rise or fall in serial measurements of cardiac specific proteins (troponin I or troponin T)
with at least one value above the 99th percentile, separating STEMI and NSTEMI from UA.30
1.2 Biomarkers in cardiovascular diseases
The idea of using information about a subject to detect subclinical disease states and to
predict future health events has great appeal, and the search for such markers in CVD has
been blooming for many years. A biomarker may be defined as “a characteristic that is
objectively measured and evaluated as an indicator of normal biological processes,
pathogenic processes, or pharmacological responses to a therapeutic intervention”.34
Biomarkers are anything that can be measured objectively and consistently and include
measurements in a biosample (e.g. blood or urine sample), recording of parameters (e.g.
ECG), or data from imaging tests. Biomarkers have several potential functions, which can
roughly be divided into indicators of disease trait (e.g. risk factors), disease state (e.g.
preclinical or clinical) or disease rate (progression of disease).35 Some are antecedent, i.e.,
measured before development of a disease. Such biomarkers can give clues on the risk of
developing the disease, work as screening methods recognizing subclinical disease states, be
diagnostic and recognize what disease causes the overt symptoms, be used in staging the
disease, and finally aid in estimating prognosis of a patient with known disease.
Several factors influence the clinical utility of a given biomarker. First of all, the accuracy of
the biomarker is important. One needs to be able to precisely estimate the levels of the
biomarker using available methods. Furthermore, the reproducibility of biomarker
measurements is important. If the measurement depends heavily on when, by whom, and how
it is computed, it will be very difficult to compare levels across time and individuals.
Measuring the biomarker must be acceptable for the patient, which partly will depend on the
usefulness of the biomarker itself. The acceptance of more invasive sampling techniques
would be greater if the biomarker significantly aids treatment. Ideally, the biomarker should
be easy to interpret by the clinician, and affect the way the patient is managed. If there is no
change in treatment related to biomarker levels, there will be no obvious benefit from
measuring the biomarker, only a cost in doing so. The biomarker should also explain a
reasonable proportion of outcome in multiple studies independent of already existing

18
predictors. If other, already implemented markers give the same information, including a new
marker do not make much sense as both methods and routines related to the old marker are
already established.35, 36 However, if the cost involved in measuring the new marker is
substantially less than the old one, the new biomarker could still be useful.
There have been an abundance of new potential biomarkers in CVD over the last decades. In
chronic HF, troponins, galectin-3, pentraxin 3, soluble ST2, as well as soluble TNF receptor
(sTNFR) 1 and 2 are some of the biomarkers more widely studied, and often associated with
outcome in these patients.37-42 However, none of these have yet made it into clinical use, and
studies conducted so far show some discrepancies in effect and importance of these
variables.39, 43
Today, only troponins and the natriuretic proteins have made it into clinical guidelines, and
then mostly for diagnostic purposes, not prognostic ones.5, 30, 31 Furthermore, while natriuretic
peptides have been suggested as potential prognostic markers in HF, they do not reflect all
underlying pathological processes in the failing heart, and only improve the prognostic power
of well-constructed models by a few percent.44 In an attempt to further improve prognostic
models, it has been suggested to implement multi-marker risk models, where a panel of
biomarkers reflecting different aspects of the disease process are evaluated together to
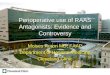
improve prognostic models. 40, 45-48 Braunwald suggested selecting biomarkers reflecting
seven different aspects of HF pathology;
that is myocardial stretch, myocyte
injury, matrix remodeling, inflammation,
renal dysfunction, neurohumoral
activation, and oxidative stress (Figure
2).1, 40 By including biomarkers covering
different areas of dysfunction in HF, the
hope is to succeed in improving current
prognostic models. Moreover, this
approach is appealing from the point of
view of pathogenesis, as they could not
only improve prognostic abilities of
models, but also be able to hint to which
processes are driving the development of
Figure 2 Braunwald’s classification of biomarkers in HF. The
seven main causes of chronic heart failure pathogenesis.

19
the disease in a given patient and could help select patients for different treatments. Several
biomarkers have been suggested as possible pieces in such a model. For example, galectin-3,
a soluble ß-galactoside– binding lectin released by activated cardiac macrophages, has been
shown to be associated with cardiac fibrosis and remodeling in a rat model of hypertrophic
HF.49 Several authors have suggested it can be used as a fibrosis marker in clinical HF as
well.50-52 And while NT-proBNP/BNP is thought to reflect myocardial wall stress, troponins
have proven a valuable marker of myocyte injury in ACS, and several studies have supported
a potential role for troponin in prognostic models of HF as well.29, 53, 54 However, no panel of
biomarkers has been thoroughly validated or reached clinical practice, and their clinical
relevance has not yet been tested.
1.2.1 Prognosis assessment in ACS and HF
ACS is an unstable coronary condition prone to complications and recurrences both in short
and long term. There is also a wide repertoire of both pharmacological and physical
interventions that could help patients, but also have serious side effects.30 The timing and
intensity of interventions should thus depend on the risk of the individual patient. There are
several tools to help classify patients according to risk, and based on this assessment select
the best treatment options
Clinical risk assessment, and especially short term risk assessment is important in ACS to
select patients for more intensive treatment. In addition to some universal risk markers such
as age, diabetes, renal failure, and other co-morbidities, the severity of the initial clinical
presentation is important for early prognosis.31 Factors such as the presence of symptoms at
rest, increasing number of episodes preceding the index event, presence of tachycardia, and
hypotension are all linked to higher risk, and warrant rapid diagnosis and aggressive
management. ECG is also an important source of information, where ST-elevation is the most
significant finding which should lead to emergency percutaneous coronary intervention (PCI)
or antithrombotic treatment. Other findings, such as ST-depression and abnormal T-waves
also signify a higher risk than patients presenting with a normal ECG. In patients with no
symptoms at rest after admission, stress ECG may provide further information.31 Continuous
ST-segment monitoring can reveal transient ST-depression in patients with NSTEMI or UA,
signifying increased risk.55 There are also useful biomarkers in the acute setting of ACS,
where troponins have gained the most central role over the last decade. Not only does

20
dynamic change in troponin levels in most cases alone confirm the presence of cardiac
necrosis, but troponin levels are also associated with short term and long term risk of
mortality and recurrent MI.31 Also other biomarkers may give additional information to ECG,
clinical presentation and troponins in the diagnosis of ACS. Among others, C-reactive protein
(CRP) and NT-proBNP have been extensively validated.56 While CRP seems to give
significant information on short and long term prognosis, NT-proBNP may help separate
cardiac causes from other causes of dyspnea. Also blood glucose and other hematological
parameters such as hemoglobin, platelet count and white blood cell count have been shown to
give additional prognostic information.31
Several risk scores have been developed to facilitate the separation of patients into risk
groups, aiding further follow-up. The two most widely used today are the thrombolysis in
myocardial infarction (TIMI) score and the global registry of acute coronary event (GRACE)
score.57 While the TIMI score is easier in use, the GRACE score has shown itself to provide
the most accurate risk stratification. However, as the GRACE score requires a computer to
calculate the final score, it is more complicated to apply in the clinic.58
There are some risk scores available for HF as well, but their predictive power is lower than
those for ACS.5, 59 These include the Seattle heart failure score (SHFS), heart failure survival
score (HFSS) and EFFECT model.60, 61 Common for these scores are the usage of clinical
data such as age, sex, New-York heart association (NYHA) class and body mass index (BMI)
that gives important prognostic information. Furthermore, echocardiography, chest x-rays, as
well as standard biochemical data on kidney function, blood hemoglobin, white blood cells
are also added to some of the models .46, 47, 59, 62, 63 As discussed above, the role of other
biomarkers on risk assessment of HF patients is still only in its infancy, and only the
natriuretic proteins for diagnosing HF is in widespread clinical use.
1.3 Inflammation in cardiovascular diseases
Inflammation is vital for the host to protect against invading pathogens, but also to promote
repair during tissue damage. In response to a pathogen or a sterile injury, a cascade of signals
leads to recruitment of inflammatory cells and activation of the immune system.64 The
immune system consists of cellular and humoral components that work in concert in response
to infection or injury in an attempt to maintain homeostasis.65 This involves both an ability to

21
respond effectively against invading pathogens and self-injury, as well as regulatory
pathways to keep the inflammatory cascade from spiraling out of control and properly resolve
inflammation when the stimulus is removed, and inflammation no longer is needed.65
The immune system is commonly divided into two main components, the innate and the
acquired immune system. Although these two systems are highly interconnected, and their
separation might not be as clear cut as originally envisaged, this division can still be
conceptually useful.66 The innate immune system mainly consists of leukocytes, natural killer
cells, complement, and inflammatory mediators such as chemokines, cytokines, and acute
phase proteins, which provides immediate host defense based on the recognition of different
molecular patterns. The adaptive immune system on the other hand consist of antigen-
specific reactions through T and B lymphocytes.66
1.3.1 Initiation of inflammation
The innate immune system is usually considered the first responder (Figure 3).66 It responds
to general molecular patterns or signals from pathogens as well as tissue damage. These first
signals acts trough pattern recognizing receptors such as the toll-like receptor (TLR) family,
activating cells such as mast cells, tissue macrophages, neutrophils and others.67 In addition,
molecules primarily present in the fluid phase such as the complement system can bind
pathogens and activate an immune response.68 An influx of cells of the innate as well as
acquired immune system to the site of inflammation is initiated through vasodilation,
expression of adhesion molecules by nearby endothelial cells, and chemotactic molecules
from endothelial cells as well as tissue residing cells and the activation of fluid phase danger
signals.69 Altogether, these pathways lead to upregulation and recruitment of cells and
mediators that may be helpful in eradicating the cause of inflammation, and restoring tissue
homeostasis. The immune system is not only important in pathogen eradication, but also
plays a pivotal role in tissue and wound repair. The inflammatory response to trauma,
ischemia-reperfusion injury and chemically induced injury are coined “sterile inflammation”
as it is induced in the absence of any microorganisms.64 Cellular damage is sensed by the
innate immune system through many of the same pathways as pathogens. Molecules released
from dying cells, so called damage associated molecular patterns (DAMPs), are recognized
by pattern recognition receptors such as TLRs, Nod-like receptors, RIG-1-like receptors and
C-type lectin receptors, as well as circulating molecules such as the complement system.67

22
This leads to activation of immune cascades recruiting neutrophils and
monocytes/macrophages, and production of inflammatory cytokines and chemokines.
Activation of the immune system leads to removal of cellular debris, and scar tissue
formation. However, the invasion of neutrophils with the release of proteases, growth factors
and reactive oxygen species (ROS), also leads to collateral damage with tissue destruction as
well as fibroblast proliferation and aberrant collagen accumulation. Hence, the regulation of
the response with quick resolution of inflammation when no longer needed is paramount, and
unresolved chronic inflammation can have many detrimental effects as exemplified by
Figure 3 Cardiac injury and sensing damaged tissue. The figure shows a coronary artery occlusion (black) that leads to ischemic (US-eng i tekst vs UK-eng i
legend) tissue injury (grey zone). From within the ischemic area, cell necrosis, extracellular matrix
(ECM) degradation and recruitment of immune cells all lead to the production of specific damage-
associated molecular patterns (DAMPs), which are recognized by pattern recognition receptors. This
leads to the generation of inflammatory responses to internal injury signals. CpG, CpG dinucleotides;
dsRNA, double-stranded RNA; HMGB1, high-mobility group box 1; HSP, heat shock protein; IL,
interleukin; IL-1R, IL-1 receptor; NLRP3, NOD-, LRRand pyrin domain-containing 3; P2Y, P2Y
purinoceptor; P2X, P2X purinoceptor; RAGE, receptor for advanced glycation end-products; TLR, Toll-
like receptor.2

23
several inflammatory diseases, such as atherosclerosis, Crohn’s disease, ulcerative colitis, and
systemic lupus erythematosus.64
1.3.2 Cytokines
Cytokines are soluble, intercellular signaling molecules produced to a varying extent by
virtually all cells. Most are soluble signaling molecules, but some may be membrane-
bound.66 They can exert autocrine, paracrine and endocrine functions, producing a wide range
of responses such as cell activation, proliferation, differentiation, movement, survival or
death. Cytokines are classified in different ways, where the classification into various
families based on the structure of their receptors is the most frequently used. According to
this classification, the largest family is the hematopoietin receptor family (type I cytokine
receptor family) and includes the receptors for most ILs. Other cytokine families include the
interferon (IFN), IL-1, TNF, chemokine and transforming growth factor (TGF)-β receptor
families.70 Immune cells are major contributors to the cytokine pool, but also other cell types
such as endothelial cells and fibroblasts contribute significantly to cytokine production in
several conditions. One of the main roles of cytokines is to regulate the activity of immune
cells. Hence, some cytokines are coined pro-inflammatory and others anti-inflammatory
according to their main effect on immune activity. However, several cytokines may exert
both pro- and anti-inflammatory effects, at least partly dependent on co-stimuli and the
degree of cellular pre-activation.71 Moreover, the activity and response to cytokines can be
modulated by the presence of not only other cytokines, but also of endogenous cytokine
modulators such as soluble cytokine receptors and receptor antagonists underscoring the
complexity of this cytokine network. 70 In addition, cytokines not only exert influence on
immune cells, but also play an important role in the interaction between the immune system
and other systems, such as the central nervous system.72 Given the importance of
neurohormones in HF, the interplay between cytokines and the neuroendocrine system may
be of particular relevance to this disease.
1.3.3 Neutrophil granulocytes
Recruitment and phagocytosis
Neutrophil granulocytes play an important role in initiation of an immune response mediated
through 1) phagocytosis, 2) release of anti-microbial peptides and proteases, and 3) formation
of neutrophil extracellular traps (NETs).73, 74 In early stages of infection or tissue damage, a
wide range of cytokines are released from resident mast cells and macrophages, as well as

24
other native tissue cells.66 Some of these cytokines (e.g., TNF, IL-1β) upregulate adhesion
molecules (E-selectin and ICAM-1) on nearby vascular endothelial cells.75 Circulating
neutrophils attaches to these adhesion molecules, and diapedeses out of the circulation
through spaces between, and sometimes through, the endothelial cells, attracted by powerful
chemoattractants such as leukotriene B4, IL-8 and C5a.66, 76 Outside of the vascular space,
they move along concentration gradients of chemokines until they reach the site of
inflammation. A major role at the site of inflammation is to phagocytose pathogens.75 The
neutrophils achieve this by engulfing the pathogens in pseudopodia, thus internalizing the
pathogens.66 Once inside the cells, the membrane bound phagosome fuses with lysosomes
forming phagolysosomes in which the pathogens are broken down by two main
mechanisms.77 The first depend on creation of toxic oxygen radicals by NADPH oxidase. The
other mechanism is independent of oxygen, and dependent on toxic cationic proteins and
enzymes such as myeloperoxidase (MPO) and lysozyme. The ingestion and killing of
pathogens are greatly amplified if the particle is opsonized with complement or specific
antibodies, binding to specific receptors on the neutrophil, enhancing its uptake and priming
the cell for efficient removal and digestion.66
Other functions
Neutrophils do not only phagocytose pathogens at the site of inflammation. They play several
other decisive roles, helping to resolve inflammation, but at the cost of self-damage.78, 79
While some neutrophils find and digest pathogens at arrival on site, others release their
granulas into their surroundings.79 These serve many different purposes. The first granulas to
be released are the peroxidase-negative granulas containing among other proteins several
matrix metalloproteinases (MMPs; MMP-8, -9 and -25), as well as neutrophil gelatinase-
associated lipocalin (NGAL), LL-37, lactoferrin and many others.78, 80 Neutrophils proceed to
release their α-granulas containing four α-defensins and MPO. The combination of lactoferrin,
an iron binding protein, and NGAL, a siderophore binding protein, help starve invading
bacteria of needed iron. The MMPs liquefies the extracellular matrix, making it easier for
immune cells to invade the area, and might hamper with the bacteria’s ability to escape the
site of infection. Finally MPO released from the primary granules converts the relatively
innocuous H2O2 into more powerful antiseptics, thereby potentiating the toxic soup.78
Recently, another role of the neutrophils has been suggested. Instead of undergoing apoptosis,
neutrophils have the ability to instead undergo “NETosis”, in which it releases its nuclear

25
DNA as an extracellular trap (NETs).81, 82 These NETs may have a multitude of function, of
which one seems to be the ability to trap pathogens in tissue or capillaries, preventing them
from disseminating to other areas of the body.83 In addition, the NETs also contain some of
the cytotoxic enzymes found in neutrophil granulas, which might help in quickly killing
attached pathogens.81
1.3.4 Resolution of inflammation
The problem with the immune system is not how often it is activated, but rather how often it
fails to subdue.84 While the immune system is activated as a response to inflammatory stimuli,
the resolution of inflammation is to a large extent dependent on signals from the immune
system itself as well as removal of the original cause of inflammation.84 One important factor
in resolving inflammation, are the inflammatory cells themselves. Neutrophils attracted to a
site of inflammation will at some point undergo apoptosis. Apoptotic cells are mainly
ingested by macrophages, in a process termed efferocytosis, and this triggers these cells to
release anti-inflammatory cytokines such as TGF-β and IL-10. 85, 86 The phagocytosis of
apoptotic cells is further enhanced by glucocorticoids, and thus enhances the release of anti-
inflammatory cytokines from macrophages.86 Factors prolonging the life of neutrophils, or
inhibiting the phagocytosis of the apoptotic cells, can thus prolong the inflammatory process.
Many soluble anti-inflammatory molecules have also been discovered in the last few decades.
Some are byproducts of the inflammatory process itself and thus constitute a negative
feedback system (e.g. oxygenated or nitrogenated lipids), while others are released by cells of
the immune systems.84 For example, secretory leukocyte protease inhibitor (SLPI) is secreted
by macrophages late in the response to an inflammatory stimulus. SLPI suppresses the ability
of neutrophils to be activated by TNF, and indirectly inhibits the release of IL-8 from
epithelial cells.84 While nucleosomes main role seem to be in the initiation of inflammation,
they may also play an essential part in resolving the acute inflammatory response. Not only
can neutrophils produce pro-resolving lipid mediators (e.g., lipoxin A4, resolvin E1 and
protectin D1) inhibiting further neutrophil recruitment, they also function as cytokine
scavenging cells, removing several important cytokines present, further decreasing the
inflammatory activation signals.73, 87 Moreover, neutrophils may release cytokine antagonists,
e.g., IL-1 receptor antagonist and also express cytokine decoy receptors, e.g., IL-1RII73 The
resolution of inflammation is an incredibly complicated process where we are only starting to
understand some of the pathways involved. Its importance is however evident, as illustrated
below.84, 88

26
1.3.5 Inflammation in chronic heart failure
Levine et al. reported more than 20 years ago that patients with HF had increased levels of
the inflammatory cytokine TNF.89 Since then a wide range of papers have demonstrated the
immune activation in this patient group, shown increased levels of several cytokines and
other inflammatory markers both systemically and locally in the heart, and suggested its
involvement in initiation and progression of HF.90-100 Several animal models have also shown
the potential adverse effects of increased inflammatory activity, and how this could
contribute to HF.101, 102 However, others studies have also shown the potential harmful effect
of inhibiting the immune system by certain pathways, demonstrating the difficulty in
untangling the complicated inflammatory meshwork.103
Causes of immune activation in HF
While studies suggest there is a persistent immune activation in HF patients, the causes of
this activation in developing HF are still not entirely understood.104 There are several theories
on how this persistent activation comes about. Several have suggested that increased
endotoxin levels circulating in blood could be the cause.105 Volume overload followed by
mesenteric venous congestion leads to edema in the bowel wall. Gram negative bacteria
could then translocate from the intestinal space to the circulation with release of endotoxins.
Lipopolysaccharide (LPS) is a strong activator of the immune system, and leads to a robust
increase in the production of TNF and many other cytokines. This theory is supported by
studies showing increased endotoxin levels in patients with peripheral edema, and that these
levels decrease with diuretic treatment. Systemic levels of endotoxin was also found to be
reduced after resolution of acute decompensated episodes.106
Intravascular congestion could itself also lead to cytokine production. Endothelium
stimulated by stretch produced endothelin-1 and TNF within hours of exposure, and studies
suggest that markers of inflammation such as cyclooxygenase-2 and inducible nitric oxide
synthase expression are elevated in venous endothelial cells harvested from patients with
clinical signs of congestion during decompensation of chronic HF, while production
decreased to normal levels after resolution107. Hence, endothelial stretch itself during acute
phases may be an independent source of inflammatory cytokines.
Increased activation of the neurohormonal system may also contribute to immune activation.
In HF there is increased activation of the RAAS as well as the SNS. Studies in mice as well
as humans suggest that ATII, a central effector in RAAS, increases production of

27
inflammatory cytokines in cardiomyocytes, and AT2 receptor blocking reduces circulating
levels of TNF and IL-6.108-110 Also chronic SNS activation increases the expression of
cytokines in myocardial cells as well as cardiac blood vessels, and beta-adrenergic receptor
blockade reduces TNF and IL-6 expression in the myocardium, suggesting that this treatment
might also have an anti-inflammatory component.111
Finally, the heart itself may constitute an important source of cytokines in HF (Figure 3).112
Oxidative stress, DAMPs from necrotic and apoptotic cells, as well as oxidized LDL may
work as immune activating ligands, and increase expression of several inflammatory
cytokines in cardiomyocytes as well as other resident cells in the heart.113-115 Pattern
recognition receptors (PRRs) such as TLRs are probable candidates of initiating cytokine
production and activating the immune system in the heart.67, 116, 117 TLRs are activated by
several ligands, both proteins, RNA and DNA of different types. While their main function
seems to be the recognition of exogenous ligands such as LPS from gram negative bacteria,
they have also been shown to recognize endogenous molecules such as heat shock molecules,
ROS, and self DNA and RNA.67, 116, 117
The immune cascade in the heart could potentially be activated from a combination of local
stimuli from necrotic cells, ROS and other endogenous ligands in the heart, as well as
exogenous ligands from the gut. These lead to activation of leukocytes, but potentially also
heart specific cells such as cardiomyocytes and fibroblasts which respond to these ligands by
cytokine production.118, 119
Consequences of immune activation in HF
The inflammatory status of chronic HF patients has potentially several detrimental effects and
influence heart function substantially. Inflammatory cytokines may directly affect cardiac
contractility.90 TNF, IL-6 and IL-2 can reduce contractility in a dose dependent manner,
through inhibiting Ca2+ release from the sarcomeres, and thus limiting Ca2+ concentration in
systole. Furthermore, they also produce an indirect decrease in contractility through NO-
dependent attenuation in myofibrillar sensitivity to Ca2+.90
Inflammation plays a role in the response to tissue injury as discussed above, but may also
play an important role in other aspects of HF development. Both in models of volume
overload in rats, as well as pressure overload in mice, inflammation plays an important role in
the functional changes of the heart that follows. TNF knockout mice showed improved

28
cardiac function, and less fibrosis, hypertrophy, MMP-9 activity and inflammatory response
compared to their wild type counterparts, suggesting a potential involvement of inflammation
in the induced pathology.120 Equally, volume overload in rats leads to activation of MMPs
and degradation of extracellular matrix (ECM), preceeded by inflammatory activity.121
Importantly, TNF inhibition as well as removal of mast cells in rat models of volume
overload also lead to attenuation of adverse eccentric LV remodeling and slow down the
progression of HF suggesting an inflammatory component in developing of HF in volume
overload as well.120, 121
While treatment directed against neurohormonal activation and renal function are among the
fundamental principles of HF therapy today, attempts at therapeutically influencing
inflammation has so far been unsuccessful.26, 122 Several reasons for this failure are possible.
Firstly, HF and inflammation could only be correlated with no causal link between them. In
this case targeting the inflammatory process would do little to ameliorate heart function.
Secondly, several competing, and potentially redundant, processes could be involved in the
development of HF, then targeting only one of these would not be helpful. Finally, the
immune system is an inherently complicated system with a meshwork of interconnected
pathways and signaling systems. So far attempts at immune modulation have been directed at
limiting overall inflammation by tumor necrosis factor (TNF) or interleukin (IL)-1 inhibition,
and immune modulating therapies such as intravenous immunoglobulins (IVIG) or
methotrexate treatment. In these approaches, the potential benefit of anti-inflammatory
therapy could have been limited by unintended side effects hampering the homeostatic role of
the immune system in HF.26 These reasons are of course not mutually exclusive, and a
combination of them could be the cause of the lack of effect of anti-inflammatory treatment
in HF so far.
1.3.6 Inflammation in acute coronary syndrome
The immune system plays important roles in ACS as well. Firstly, research over the last two
decades has shown us the importance of the immune system in the development of
atherosclerosis, a central component of ACS. Secondly, in the case of cardiac necrosis, the
immune system is the main player in removing dead tissue, and stimulating the scar
formation necessary to keep the organ functionally intact.

29
Atherosclerosis
Atherosclerosis is a chronic inflammatory condition in the vessel wall, involving lipids,
thrombosis, fibrosis, and immune cells.123 The vessel wall is not a static environment, but
rather serves a very important function in inhibiting coagulation and cellular adhesion, and
regulating blood flow. In addition, the vessel wall plays an important role in local injury
where it produces cytokines and upregulates adhesion molecules leading to the infiltration of
leukocytes.124 In atherosclerosis the normal function of the vessel wall is interrupted, and the
wall itself plays an important role in the formation of the atherosclerotic plaque.124
Fatty streaks and plaque progression
While plaque formation is a complex interplay of many different mechanisms over many
years, it can broadly be divided into three main processes: formation of the fatty streak,
plaque progression and plaque disruption.123 Fatty streaks appear as yellow discolorations in
the artery walls that do not protrude into the lumen.123 An important factor in forming the
fatty streaks is dysfunction of the endothelial lining of the vessel. Disrupting the normal
homeostasis of the endothelium leads to an activated state with increased permeability,
release of cytokines, decreased antithrombotic function and upregulation of adhesion
molecules.123, 125 The decreased barrier function of the endothelium leads to the entry of LDL
particles into the subendothelial space.126 Here, the particles bind to proteoglycans, and may
be modified by reactive oxidants both from the endothelium itself, but also from infiltrating
macrophages, as well as glycosylated in states of increased blood glucose such as diabetes.123
Modified LDL (mLDL) stimulates the endothelium to produce more cytokines, promoting
further recruitment of leukocytes, in particular monocytes.127 Monocytes entering the early
plaque differentiate into phagocytosing macrophages, and imbibe LDL from the
subendothelial space by phagocytosis mediated by scavenging receptors that show high
affinity for mLDL.127, 128 This process may initially be beneficial by removing the pro-
inflammatory mLDL, however the imbalance between low efflux and high influx of
macrophages leads to a buildup of cells in the plaque, forming of foam cells (fat-laden
macrophages), and increased apoptosis and necrosis of these foam cells as the plaque
develops.124
As the plaque progresses, smooth muscle cells (SMCs) infiltrates the intima, where they
proliferate and start to form ECM.123 While the mentioned factors lead to plaque growth,
resident cells also produce factors leading to the breakdown of the ECM, and inhibition of

30
SMCs. Notably foam cells stimulated by cytokines from T-lymphocytes produce MMPs, that
actively disrupts the ECM, and other cytokines from the T-lymphocytes inhibit ECM
production by SMC.123, 129 Thus the thickness of the fibrous cap protecting the core of foam
cells, lipids and cellular debris from the circulation depends on the balance between ECM
synthesis and degradation, again determined by the balance of signal molecules produced by
the resident cells.
Plaque rupture
Plaques can continue to develop over decades. Death of foam cells and SMC will however
lead to a slow buildup of cellular debris, and lipids to the plaque core. As the growing plaque
protrudes more into the lumen of the vessel, there is increased wall stress especially in the
borders between normal and dysfunctional endothelium, called the “shoulder” of the
plaque.130 In addition, there is evidence for an increased concentration of T-lymphocytes as
well as foam cells in these areas potentially leading to increased production of MMPs and
disruption of the ECM123. This may lead to increased vulnerability of the plaque in these
areas, and potentially a plaque rupture where the circulating blood gets in contact with the
plaque core activating coagulation cascades and clot formation. The partial or complete
occlusion leading to ACS mainly comes from these events.
Inflammation in cardiac ischemia
When an atherosclerotic plaque ruptures, blood flow can be altered in downstream areas,
leading to ischemia, and if perfusion is not reestablished, infarction. This leads to sterile
inflammation, with influx of neutrophils and macrophages (See section 1.3.1). Once at the
site of injury, neutrophils and macrophages have multiple roles both in sustaining and
resolving inflammation (see section 1.3.3 and 1.3.4). Traditionally, monocyte/macrophages
present in the heart during sterile inflammation have been assumed to stem from circulating
monocytes recruited to the tissue in the acute setting or in the non-acute setting as tissue
residing macrophages. However, recent studies have shown that residing macrophages
actually consist of at least three different sub-populations described by combination of level
of expression of MHC II receptors, as well as presence or absents of chemokine receptor 2
(CCR2).2 Most CCR2- cells, seem not to stem from circulation monocytes, but rather derived
from embryonic progenitors, and renew in situ. Furthermore, the function of different sub-
populations are not entirely the same, and while recruited monocytes/macrophages to a larger
extent produce inflammatory cytokines, residing, embryologically derived macrophages seem

31
to be more involved in the resolution of inflammation and initiation of scar formation. When
macrophages, and in particular cardiac residing macrophages, ingest apoptotic cells, this
induces the production of anti-inflammatory and pro-fibrotic cytokines, initiating the
transition from acute inflammation to fibrosis.131 In addition, regulatory T-cells probably play
an important role in this transition, and residing fibroblasts and cardiomyocytes could play a
part as well.2 When the acute inflammation is resolved, residing fibroblasts start the
formation of scar tissue by deposition of extracellular matrix proteins, and in this way
preserving the structural integrity of the tissue.131
1.4 NGAL
1.4.1 General properties
NGAL is a 25kDa molecule of the lipocalin family, first isolated from neutrophils.132 NGAL
is produced by a wide range of different tissues, most notably epithelia in different organs as
well as macrophages and fibroblasts.133 Systemic levels of NGAL are greatly increased in
several conditions, most notably in cardiac disease, inflammatory diseases and particularly in
kidney injury.134-137 The marked and rapid increase in acute kidney injury has made NGAL a
promising biomarker in this condition.136, 138 Others have however, shown that NGAL has
potential as biomarker in other diseases as well, both with and without kidney components,
such as HF, some forms of cancer, and chronic obstructive pulmonary disease.139-142
1.4.2 NGAL in disease
Several potential roles of NGAL have been suggested, most connected to its ability to bind
bacterial siderophores and thus influence of the iron homeostasis.137, 143-145 A study by Flo et.
al. showed that NGAL is important in limiting bacterial infection in mice due to its iron
binding properties.137 NGAL may also influence apoptosis rate in cells, and can affect
necrosis, but if this is due to its iron-binding capacity or other mechanisms is not clear.145, 146
NGAL can bind MMP-9 inhibit the inactivation of MMP-9 and thus increase its activity.147
This has been suggested as a potential role for NGAL in CVD, in particular in atherosclerotic
plaques where NGAL is upregulated and associated with increased plaque vulnerability.147,
148 There is also an increased NGAL/MMP-9 complex concentration in vulnerable plaques
co-localized with macrophages, and there is an elevated level of these complexes in plaques
with intra-plaque hemorrhage or thrombus.147, 149

32
NGAL is produced by many tissues and found both in urine and circulation in healthy
individuals as well as in disease.145 Yet the sources of NGAL may differ depending on
condition. NGAL is freely filtrated by the kidneys, but is to a large extent reabsorbed in the
proximal tubuli. However, with kidney injury, NGAL is produced by epithelial cells in the
distal tubuli and directly secreted in the urine.144, 146 Thus, urinary NGAL may mainly stem
from local production, and to a much lesser extent to be filtrated NGAL from other
sources.146 Circulating NGAL on the other hand is produced by other organs in response to
kidney injury or other conditions.150 Thus while both circulating and urinary NGAL increases
in many conditions, they may not always reflect the same pool, and their significance may
vary in different conditions.
1.4.3 NGAL as a biomarker
As mentioned, NGAL has been thoroughly studied as a potential biomarker in acute kidney
injury (AKI) over the last decade, showing promising results.138, 151, 152 In particular, urinary
NGAL shows a robust increase in levels as quickly as two hours after AKI, and thus might
help in early diagnosing this condition.138 Previously, creatinine has been the main biomarker
of AKI, but several days can pass from the initial insult to the increase in circulating
creatinine. NGAL could therefore help in substantially decreasing time from injury to
treatment. However the picture is not yet clear, and further research is needed before adoption
of NGAL in the clinic is warranted.152 In other conditions, NGAL is much less studied, and
the results more diverse. Some studies show a potential role as a biomarker in acute and
chronic HF, ACS, CKD, sepsis, chronic obstructive pulmonary disease as well as a wide
range of other conditions.134, 138, 153-160 However in these fields, there are a lot more
discrepancies in the findings and NGAL seems to be a weaker marker with less clinical
application than in AKI. One of the main problems with NGAL as a biomarker is its
induction in a wide range of normal conditions, such as most inflammatory states.145 Its
specificity for a given disease is thus limited, especially in the elderly who often have several
comorbidities.161

33
2 Aims Our overall hypothesis is that the immune system and inflammation are involved in the
pathogenesis of CVD. Taking a prime interest in the innate immune system, and in particular
neutrophils, our main aim was to shed light on the potential role of inflammatory biomarkers
as biomarkers in this condition.
In two large patient cohorts, we aimed to see if inflammatory cytokines in general and NGAL
in particular, were associated with outcome in two important and connected groups of
diseases; chronic HF and ACS. In this way we wished to both investigate the potential role as
a biomarker for these proteins, as well as further elucidating the differentiated involvement of
the immune system in both conditions.
Our specific aims were to:
1. Investigate if NGAL was a suitable biomarker for mortality and morbidity in HF
using material and data from the CORONA study.
2. Investigate if NGAL was a potential biomarker of mortality in ACS using material
and data from the PRACSIS study.
3. Investigate if other prototypical cytokines, namely IL-8, TNF, sTNF-RI and II, and
MCP-1 were associated with morbidity and mortality in HF, and could be potential
biomarkers in this disease using data from the CORONA study.
4. Investigate if a panel of biomarkers increased prognostic abilities of established
prognostic models in HF patients from the CORONA population.

34
3 Material and Methods
3.1 Patients
3.1.1 The CORONA study
The design and principal findings of the CORONA study have been described previously by
Kjekshus et al. and is also described more in detail in the method section of paper I and paper
III.158, 162, 163 Briefly, elderly patients (>60 years of age) with chronic HF of ischemic cause,
NYHA class II–IV disease and left ventricular ejection fraction (EF) <40% (35% for NYHA
II) were eligible as long as the investigator considered that they did not need treatment with a
cholesterol-lowering drug. In our studies, we included approximately 1400 patients from a
sub-study of the original 5011 patients included in the CORONA study. The trial was
approved by the ethics committees at each of the participating hospitals, and patients
provided written informed consent.
3.1.2 The PRACSIS study
The design of the PRACSIS study is described in detail elsewhere, and further details can
also be found in the method section of paper II.164 Patients with ACS, admitted to the
coronary care unit of the Sahlgrenska University Hospital, Gothenburg, Sweden from
September 1995 to February 2000 were eligible for participation. Patients who consented to
blood sampling were included consecutively. The primary outcome measure of the study was
all-cause mortality from the time of inclusion in the study to September 15, 2001. The study
protocol was approved by the regional ethics committee before the initiation of the study.
Informed consent was obtained from all participating patients.
3.2 Blood sampling
Blood samples from the CORONA and PRACSIS studies were drawn from peripheral venous
blood into pyrogen-free blood collection tubes without any additives and allowed to clot
before centrifugation. Serum samples were stored at -70°C and thawed less than three times
before measuring the biomarkers.

35
3.3 ELISA To measure NGAL, we used an enzyme-linked immunosorbent assay (ELISA). Due to its
ease of use, and high sensitivity and specificity, ELISA has been extensively used to measure
concentration of circulating biomarkers. The standard ELISA makes use of a double antibody
sandwich principle. In step one, a microtiter plate is coated with a primary antibody specific
for the molecule at interest. After saturating the unspecific binding capacity of the plate with
a non-specific protein, in our case bovine serum albumin, the plasma or serum was added to
sample wells, at the same time as a solution with a known concentration of the molecule at
interest was added in separate wells. At this step the molecule at interest will bind the
primary antibody. For NGAL, serum samples diluted 1:200 in PBS with 1% albumin were
used at this step. The wells were then washed to rinse of superfluous samples, and a second
antibody specific for the molecule at interest was added. This binds the molecule at a
different epitope (or several different epitopes). The secondary antibody was biotinylated,
and an enzyme conjugated to streptavidin binds it, which after addition of a substrate solution
catalyzed a change of color proportional to the concentration of the molecule at interest. After
stopping the enzyme reaction with acid, the color intensity were read by a spectrophotometer,
and compared with the intensity of color of the standard solutions analyzed at the same time.
Concentration was then calculated from color intensity and dilution factor.
3.4 Multiplex
In paper II, the cytokines were measured using cytokine panel 1 on Evolution multiplex
technology from Randox Laboratories (Northern Ireland). The methods are very similar to
ELISA, but instead of only measuring one substrate, several antibodies to a range of
molecules are attached to a biochip, allowing measurements of several molecules in parallel
from the same sample. For all the cytokines, the detection limits are given in the method
section of paper II, and at these levels, the intra- and interassay coefficient of variance were
less than 20%.
3.5 Statistical methods
In our studies, all our main results come from standard application of the cox proportional
hazard ratio model, or cox model for short. The cox model is a semi-parametric model where

36
time is modeled non-parametrically, while all independent variables are modeled
parametrically. The model enables the investigation of the association between a variable and
an outcome in a population with censoring. To test the assumptions of the cox model, we
used log-log plots, a formalized test using Schoenfeld residuals, as well as cubic spline plots.
In addition we used DF-beta plots to check if any outliers had a disproportionate influence on
our results. To assess the clinical relevance of our findings, we mainly used two additional
methods; the change in Harrell’s C-statistics (ΔC) as well as continuous net reclassification
improvement (cNRI).165, 166 In addition, in paper IV, we included the change in Gönen and
Heller’s K statistics (ΔK).167 To calculate prognostic scores based on estimated models, we
multiplied each variable in the model with the natural log of its HR for each patient. For
missing values in paper IV, multiple imputation was used to generate 20 new datasets, and
chained regression analysis was used to fill in missing values.168 All models were estimated
on the collection of this data using Rubin’s combination rule for combining results into one
estimate.169 All statistics in paper I, III and IV were done using Stata version 11 to 14
(StataCorp LP, College Station, TX, USA), while analyses for paper II were done using SAS
version 9.2 (SAS Institute, Cary, NC, USA).

37
4 Results
4.1 Paper I
The association between neutrophil gelatinase-associated lipocalin and clinical outcome in
chronic heart failure: results from CORONA158
In paper I we explored the prognostic value of NGAL in chronic HF of ischemic etiology
using data from 1415 patients in the CORONA study.
Our main findings, using NGAL as a continuous, log-transformed variable were:
NGAL added significant information when adjusting for clinical variables, but was no
longer significant when further adjusting for Apolipoprotein (Apo) A-1, eGFR, CRP
and NT-proBNP.
Belonging to the highest NGAL tertile was associated with more frequent
hospitalization, even after adjusting for clinical variables, GFR and ApoA-1, but not
after adjusting for CRP and NT-proBNP.
There was no interaction between rosuvastatin treatment and NGAL.
Conclusion: NGAL added no significant information to NT-proBNP and GFR in a
multivariate model for primary and secondary end-points

38
4.2 Paper II
Serum Neutrophil Gelatinase-Associated Lipocalin (NGAL) is independently associated
with mortality in acute coronary syndromes
In paper II we tested the hypothesis that circulating NGAL levels could add prognostic short-
and long-term information among patients with a range of ACS using data from 1122 patients
with ACS from the PRACSIS study. We also investigated whether any gene polymorphism
was associated with NGAL levels.
Our main findings were, all models adjusted for GRACE score, EF, CRP and BNP, and
comparing NGAL levels in top quartile with quartile 1 through 3 if not otherwise specified:
NGAL was associated with adjusted hazard ratios of 1.41 (95% confidence interval
(CI): 1.05-1.89; p=0.02) for mortality and 1.45 (95% CI: 1.20-1.81; p=0.006) for the
combined endpoint cardiovascular (CV) death, MI or HF during long-term follow-up
(median 91 months).
NGAL was also significantly associated with short-term (3 months) and late long-
term (median 129 months) mortality, with adjusted hazard ratios of 2.76 (CI: 1.35-
5.65; p=0.005) and 1.51 (CI: 1.18-1.94; p<0.001).
Relative change from baseline to 3 months, but not to 25 months, was predictive of
long-term mortality (before 2011), and patients with relative change in the top quartile
(more than 22.6% increase) had a hazard ratio of 1.60, CI: 1.06-2.40; p=0.02.
Combining NGAL with GRACE score in a combined score improved the AUC of the
model significantly from 0.681 (0.653,0.709) to 0.713 (0.682,0.743), p=0.0002 for
comparison with GRACE alone
Change in NGAL levels from baseline to three months was associated with a genomic
region on chromosome 2, and the most significantly associated single nucleotide
polymorphism was located within an intron for MYO7B, a gene mainly expressed in
the proximal tubule of the kidney.
Conclusion: NGAL is associated with both short and long-term prognosis in patients with
ACS independently of GRACE score, BNP, CRP and EF. NGAL could therefore improve the
selection of patients needing closer follow-up after admission to hospital for ACS.

39
4.3 Paper III
Inflammatory cytokines in chronic heart failure: interleukin-8 is associated with adverse
outcome - results from CORONA163
In paper III we investigated the ability of prototypical inflammatory cytokines to predict
clinical outcomes in a large population of patients with chronic systolic HF from the
CORONA study.
Our main findings in this paper were:
TNFα, sTNFR 1, sTNFR 2 and IL-8, but not MCP-1, were independent predictors of
all endpoints except the coronary endpoint in multivariable models including
conventional clinical variables.
After further adjustment for eGFR, ApoB/ApoA-1 ratio, NT-proBNP and CRP, only
IL-8 remained a significant predictor of all endpoints (except the coronary endpoint),
while sTNFR 1 remained independently associated with CV mortality.
Adding IL-8 to the full model led to a significant improvement in net reclassification
for all-cause mortality and CV-hospitalization, but only a borderline significant
improvement for the primary endpoint, CV mortality and the composite endpoint
hospitalization for worsening HF or CV mortality.
Conclusion: IL-8 was associated with the primary endpoint, all-cause and CV mortality, as
well as CV-hospitalization when adjusting for a range of clinical parameters, hsCRP and NT-
proBNP. Our findings further support the involvement of inflammation and immune
activation in the progression of HF.

40
4.4 Paper IV
Limited added value of circulating inflammatory and extracellular matrix biomarkers in
multimarker models for predicting clinical outcomes in chronic heart failure
In paper IV we investigated the ability of a panel of biomarkers to predict clinical outcomes
in a large population of patients with chronic systolic HF from the CORONA study.
Our main findings in this paper were:
Adding a panel of biomarkers to the CORONA risk model previously published does
not add significant information to the risk model’s prognostic abilities.
While a panel of biomarkers does improve prognostic abilities of Seattle heart failure
model scores in the CORONA population, most of the added predictability can be
gained by including NT-proBNP in the model.
Three months statin treatment did not lead to significant changes in inflammatory
biomarker levels compared with placebo. There might however be increased survival
with statin treatment of patients having lower levels of biomarkers.
Conclusion: Several authors have suggested that a multimarker approach may be the way
ahead to improve prognostic models in chronic HF. We were however not able to construct
such a panel from a broad range of inflammatory biomarkers in elderly patients with systolic
HF of ischemic etiology. Nor do our findings support a general anti-inflammatory effect of
statins. However, as suggested by previous studies, there seems to be some improvement of
survival with statin treatment in patients with lower biomarker scores.

41
5 Discussion
5.1 Analysis of circulating biomarkers in clinical materials Numerous factors can influence the results of serum or plasma analyses, and several pitfalls
need to be avoided both in the collection and analysis of samples.
5.1.1 Collection of samples
Firstly, contaminated collection tubes may activate blood cells and heavily influence cytokine
concentration. Hence, usage of pyrogen-free collection tubes is essential for reliable results
and was used for all blood samples in the two studies. Secondly, for many inflammatory
parameters the type of anticoagulant and the choice of plasma or serum have a potential huge
impact on final data. Heparin and citrate have been shown to influence levels of some
circulating cytokines such as IL-6 and TNF, while EDTA seem to be the most reliant
anticoagulant for cytokine measurements.170 Furthermore, many cytokines and inflammatory
biomarkers are released from circulating immune cells as well as platelets when activated.
There is also a certain binding of inflammatory molecules to some of the proteins involved in
the coagulation cascade, and these molecules could be sequestered if blood is allowed to
coagulate as when preparing serum.171, 172 For example, while highly correlated, NGAL levels
from serum and plasma cannot be directly compared, necessitating specification from what
sample type a study is conducted.173 Thirdly, storage of blood may influence concentration of
several biomarkers.172 Particularly in larger biomarker studies, samples are often stored for
several years before analysis, potentially influencing findings significantly. NGAL has been
found to be relatively stable throughout several freeze-thaw cycles as well as during storage
at -70°C, however some studies have shown a potential influence of freeze-thaw cycles on
cytokine concentration.174, 175 Since several of the samples were stored for more than two to
three years, and thawed up to three times, we cannot exclude some influence of the storage
conditions on biomarker concentration. While storage times were unequal for samples due to
different inclusion times, all samples were stored under equal conditions and thawed an equal
number of times, limiting the potential bias. In our study, the cytokines in paper III were
measured on samples not previously thawed, thus limiting this potentially influencing factor.
Finally, other factors such as time of day, fasting state, physical activity, stress and recent
weight loss or gain have been shown to influence several cytokines such as TNF, IL-6 and
IFN-γ. 170 Blood samples for the CORONA study were not fasting, or at any particular time
of the day. This is a potential source of error in our studies. However, there is no particular

42
reason to suspect that this would introduce any systematic bias. This could however attenuate
the association between the biomarkers and outcome, and thus a more strict protocol could
have given other results.
5.1.2 ELISA
ELISA is a popular method for biomarker measurement. However some important caveats
must be noted. Firstly, while ELISA is considered to have good sensitivity and specificity in
general, the individual kit properties depend upon which antibodies it uses, and their
properties. For the measurement of NGAL in paper I, we used a non-commercial ELISA kit,
developed by Trude H. Flo and previously described elsewhere.176 The primary antibody was
a rabbit affinity-purified anti-NGAL antibody developed by Trude H. Flo. The secondary
antibody was a commercially available biotinylated mouse monoclonal antibody (no.
HYB211-05; Antibody Shop, Gentofte, Denmark). The detection limit of the ELISA was
estimated to 0.06 ng/mL, and intra- and interassay coefficient of variability was <6%. For
paper II, a commercial available ELISA kit from R&D Systems (Minneapolis, MN) was
available. As the usage of commercial available systems makes it easier for others to attempt
to reproduce the data, we opted to change to this kit. The detection limit of this kit was 0.04
ng/mL, and intra- and interassay coefficient of variability was <8%. However, while intra-
and interassay properties were good for both ELISA kits, the exact levels of NGAL must be
considered with care. Different kits for NGAL measurement are not standardized, so the
exact levels may vary between kits. One reason for difference in NGAL measurements across
different kits is the specificity of the antibodies. Often the molecules at interest, such as
NGAL, do not only exist in one configuration in the circulation. NGAL exist in several
different configurations, among others as a monomer, a homodimer, as well as in complex
with MMP-9 and potentially with bacterial siderophores. In addition, antibodies of one
particular kit only bind one epitope of the molecule of interest. Which epitopes of a molecule
is available for binding may differ according to presence of other binding molecules such as
inhibitors, also influencing the measured quantity of the molecule of interest. However, in
this type of study, the main interest will be the relative level of NGAL from patient to patient,
and the exact concentration is of less importance as long as all samples are measured using
the same kit. It is not however possible to be sure that the measured quantities do reflect total
NGAL levels in a patient, but could only reflect the pool of NGAL in certain configurations
or complexes. Thus one can argue that concluding on the abilities of NGAL as such as
biomarker is somewhat erroneous, and should be limited to NGAL measured by a certain kit.

43
Secondly, with relatively large studies like CORONA and PRACSIS, it is often practically
difficult to do measurements of a biomarker on all samples the same day. While the use of a
standard curve of known concentration should limit measurement differences from day to day,
the number of steps, and complexity of the ELISA methods makes it difficult to exclude the
potential for systematical higher or lower levels from one day to another. To alleviate this
problem, we have attempted doing the measurements in as few days as possible, and have
also included control samples on every plate which makes it possible to adjust plate
measurement levels in case of significant difference between different days. Thirdly, ELISA
has a relatively small analytic range compared with multiplex technology, and biomarkers
with huge variation, such as often is the case with cytokines and other inflammatory
parameters, it can be difficult to find a dilution where all samples fit within the same standard
curve. This was not a problem for NGAL with less than 20 fold change from lowest to
highest value, but for some of the other biomarkers such as sTNF-R2 with more than a 100-
fold difference from bottom value to highest value, this could influence the final results.
5.1.3 Multiplex
Compared to ELISA, Multiplex methodology has several advantages, and a few difficulties.
Firstly, the dynamic range of multiplex kits is usually much greater than ELISA, allowing the
difference in concentration of one biomarker from sample to sample to be much larger. This
is especially important for cytokines where there is often a long upper tail of the distribution,
with some samples having thousand to several thousand fold higher levels than others.
However, the kit applied in paper III did suffer from relatively low sensitivity for some of the
biomarkers such as TNF, resulting in a lot of the samples having non-detectable levels.
Several newer kits have higher sensitivity, detecting levels ten folds lower than the kit used in
our study and could potentially have given different results for paper III. In addition, while
the dynamic range of multiplex is greater than for ELISA, there is less room to optimize
conditions as samples for all biomarkers in the multiplex assay need to be treated equally.
Using ELISA, incubation time and temperature, as well as addition of calf serum, albumin or
other reagents to dilution mediums can be optimized for each biomarker, potentially
increasing sensitivity. For example, while IL-1β often is below detection limit in current
multiplex kits, as was the case for the multiplex used for paper III, it can often be measured
by high sensitive ELISA kits. Secondly, since several biomarkers are measured in parallel in
the same sample, smaller quantities of sample are needed for analysis, and a large number of
biomarkers can be measured in much shorter time than with ELISA. However, the ease at

44
which measurements of several biomarkers can be made makes the importance of proper
statistical handling of the resulting data of uttermost importance.
5.2 Statistical considerations
5.2.1 The assumptions of the cox model
For the use of the cox model to be appropriate, some assumptions need to be met by the
population studied, and the variables investigated. Firstly, the cox model requires non-
informative censoring. This means that the reason why people drop out of the study must not
be associated with the outcome investigated. Secondly, the model requires the risk associated
with independent variables to be time independent. There should be a uniform association
over time between the independent variable and risk, which does not depend on which time
point you are at. Thirdly, it assumes the risk of all variables to be linear and additive.
While non-biased censoring is a very important assumption, there are few tests that can
assess to what extent this is the case. However, the study design for both populations used in
our studies seems to limit this problem. There were very few dropouts early in both studies,
and the PRACSIS study also used register data to gather information on endpoint status of
individuals which assured less censoring on these endpoints, and limits the potential for bias
considerably.164 Furthermore, while the CORONA study does randomize patients to receive
rosuvastatin, the dosage used is widely used in other patient groups and is considered to give
very few, serious side effects, and should therefore lead to few dropouts from medication use. 162, 177
In our studies, we mainly used a formal test utilizing the Schoenfeld’s residuals, as well as
log-log plots, to test the proportional hazards. This was deemed sufficiently satisfied for all
variables investigate.
Finally, linearity is often a problem with biomarkers. Due to their often skewed distribution,
and not necessarily linear risk association, we did several tests to assure that the variables
were transformed appropriately when needed. However, there is a risk of over-fitting
variables to the population, thus necessitating some care while transforming the data. We
have chosen two main approaches for transforming the variables. Firstly, as the distributions
were skewed for all the biomarkers investigated, we did log-transformation to make them
more normalized, and thus limiting the problem with outliers significantly influencing the
analysis. This was also checked using DF-beta plots to assure that no one observation

45
significantly changed the associations estimated. When there was evidence of a non-linear
association with the endpoints, we categorized the data. This approach has some
disadvantages by loss of potential information. In addition, it can be significantly affected by
the cutoff values chosen. The latter problem was amended by using the 33% or 66%, or
alternatively 25%, 50% and 75% percentiles as predefined cut-offs. We intentionally chose
not to try to find optimal cutoffs for the population considered, as this could over-estimate the
association severely. While not finding the optimal cutoff, as well as losing some information
when categorizing continuous data may lead to potentially lower prognostic value, it does
increase the robustness of the findings.
From the cox model, you obtain hazard ratios (HRs) associated with the variable at interest.
Hazard ratio, similarly to the odds ratio obtained in logistic regressions, describes the change
in risk associated with a one unit change in the variable. For interpretation of HRs, the unit
chosen for the variable is therefore very important. To make HRs more comparable across
different biomarkers, we have chosen to standardize the variance of all non-categorical
variables of interest where appropriate, so that their standard deviation is one.
5.2.2 Missing values
Missing values could be a problem when analyzing biomarkers in clinical material. First of
all, the normal approach to missing values is to exclude these patients from analysis. This
naturally leads to a decrease in power of the statistical model, especially when many patients
lack data on one or several variables. Furthermore, there is always a risk of the data missing
not being randomly distributed; that is data on certain variables for certain patients are
missing for reasons associated with factors relevant to the purpose of the model. In this case,
excluding patients with missing values could bias the results of the study.178, 179 For paper I-
III, there were relatively few missing values, and the risk of bias, and the loss of power by
excluding patients with missing values were therefore considered to be relatively low.
However, for paper IV, where several biomarkers where included, some of them missing in a
significant proportion of the patients, the loss of power as well as the risk of bias had to be
taken into consideration. To avoid these pitfalls, we used multiple imputations. This method
gives unbiased estimation of both coefficients and variance of coefficients without loss of
power, as long as the pattern of missing data is not associated with non-observed, relevant
variables. In our studies, missing values where mainly missing because of lack of samples, or
procedural errors while measuring biomarkers, and could therefore be assumed to be missing

46
at random.178 In hindsight, one could argue that paper I-III as well could have benefited from
similar approach; this was however not considered at the time of writing.
5.2.3 A model’s discrimination: Harrell’s C statistics and NRI
The statistical significant association with chosen endpoints is only the first step in
identifying a potential useful new biomarker. While a statistically significant association
suggests that there could be an association between the variable and the outcome, it does not
say whether this association is clinically significant or not, and it says little about the
discriminatory properties of the variables between events and no-events.165, 180 Today there is
no agreed upon measure to estimate the clinical significance of a new marker. Several
statistical methods have been developed to this end, but none of them are perfect.
Harrell’s C-statistics is a measurement of concordance between model and outcome, and is
similar to the area under the curve statistics from case-control studies. It is a number between
0-1, where 0.5 means no addition to the model whatsoever, and the closer to 1, the better the
model.181, 182 It is calculated by comparing all suitable pairs of individuals in the study
population, that is, all pairs where not both were censored. Then the proportion of pairs where
the individual with the highest estimated risk reaches an endpoint first is estimated. To
compare two different models, the difference in Harrell’s C, or for nested models, change in
Harrell’s C (ΔC) is then used. While widely used, the ΔC has several limitations. Firstly, it
greatly depends on the already existing model. The higher C-statistic of the original model,
the more difficult it is for any new parameter to improve it to any degree.183 Secondly, very
small ΔC may be statistically significant, but their clinical relevance is not certain. Thirdly,
biomarkers that could be clinically significant can lead to not significant ΔC. Fourthly, while
it compares all suitable pairs, it does not take into account the degree of difference between
the pairs; thus a difference of 0.1% estimated risk is accorded the same importance as a
difference of 50%. If a large group of patients have similar estimated risk, and reaches the
endpoint at similar time points, the exact order of which the patients reach the endpoint
influences the final C statistics substantially.184
Another measure argued to be closer to the clinical reality is net reclassification improvement
(NRI). Originally, it was developed for estimating relevance of models where there already
existed clinically used risk thresholds.165 It measures the proportion of patients who are
reclassified to a better risk group when the new biomarker is added to the model.165 NRI thus
tests a clinically meaningful reclassification of patients to a better risk group. However, for

47
conditions where no previous risk categories exist, NRI is very sensitive to the selection of
risk cutoffs, and several authors have therefore suggested a different approach in these
cases.166, 185 The most widely used today is a continuous NRI (cNRI) where instead of
looking at only patients reclassified to a new, pre-specified risk group, one looks at the
direction of change in risk, and compare it with the outcome. Thus we measure what
proportion of patients with higher estimated risk has an event, as well as how many with
lower estimated risk have no events. This continuous measure does not then depend on
already existing risk groups. There is however certain limitations with this method. As it is
relatively new, there is no consensus on what NRI should be considered a clinical meaningful
NRI. Furthermore, the way it is currently implemented, any change in risk score is measured,
meaning that a change in 0.1% count as much as a 5% change. While a 0.1% change would
have no clinical relevance, a 5% change would probably have. cNRI thus therefore suffers
from some of the same problems as ΔC. However, while none of the measures are perfectly
suited to judge clinical relevance of a new biomarker, they both add to the information
provided by the cox model, and thus may help in selecting suitable candidates that warrant
further investigation.
5.2.4 Validation of prognostic models
The approach mostly widely used for testing association of new, potential biomarkers with
outcome, is including these biomarkers in a model, adjusting for known prognostic factors.
This way, the statistical significance of the included biomarker, as well as improvement of
discrimination and calibration of the new model in comparison with a model only including
known prognostic factors, can be estimated. This was the approach we used in paper I to III.
However, while methodologically simple, this method leads to overly optimistic estimates
since the estimations are fitted and evaluated in the same population. Results therefore need
to be very carefully interpreted.186, 187 As a method of hypothesis generation, this method
could work reasonably well, however for clinical models intended for clinical use, a more
rigorous approach is needed, and validation of models is necessary.188 While the gold
standard of testing new prognostic models is external validation, a first and useful step is
internally validating the model. Several approaches have been suggested, including different
methods of subdividing the population into a training set and validation set, as well as using
methods based on jackknife or bootstrapping data.188 To retain maximum power, for example
a jackknife approach, where a prognostic score is generated based on a model estimated for
all other patients, is possible. However, we chose to randomly divide the CORONA

48
population into a training set and validation set in our study in paper IV, with some loss of
power. Since building a prognostic model was part of our aim, this approach avoided a bias
towards more optimistic results from over-fitting when the same population is used for
variable selection and model evaluation. However, due to the loss of power, one could argue
that a jackknife approach would have been as appropriate, if not more so, for Model 2 in
paper IV, where variables were not selected based on the CORONA population. While this
could have led to some of the non-significant results becoming statistically significant, the
clinical relevance of the change in discrimination would still in our opinion be very limited.
It is also important to mention that while internal validation of models are of some use,
external validation is the only way of separating useful from not useful models, and often
there is a substantial decrease in discrimination and calibration of models when applied to a
different population.187, 189
5.3 Inflammation in cardiovascular disease: biomarkers, players, and
potential therapeutic targets.
5.3.1 Inflammatory biomarkers in HF
Since the discoveries of Levine et al, an abundance of cytokines have been investigated and
found to be upregulated in HF.89, 190-192 This is some of the strongest evidence for the low-
grade, persistent inflammation assumed to be occurring in these patients. In our study we
have evaluated some of these as biomarkers. Previously, especially TNF and its receptors
have been studied extensively, but there are some discrepancies between these earlier studies
and our findings. While earlier, TNF, and TNF receptors were found to be associated with
outcome, this was not the case in our study.192-194 This could be due to the difference in the
two populations studied, or the variables adjusted for in the model. Also, TNF circulates at
low levels requiring methods with high sensitivity for reliable detection. TNF was not
detectable in a large portion of the samples, and TNF measurement could therefore have
benefited from a more sensitive, customized assay. TNF receptors were significantly
associated with outcome in our study before we adjusted for NT-proBNP levels which many
of the previous studies did not adjust for. Our patient group was also a selected group where
all patients had systolic HF of ischemic etiology, and the findings in other populations could
differ. Nevertheless, HF of ischemic origin is the most prevalent type today, and the inability

49
to reproduce earlier findings suggests that TNF and its receptors are not likely candidates as
biomarkers for chronic HF in general. Equally, no other cytokine or inflammatory marker has
managed the transition from early findings of upregulation in HF, to become a biomarker for
this condition. Of the several we have studied, only IL-8 proved statistically significant in the
model, and its clinical relevance remains doubtful. Studies of more specialized cytokines,
with the aim to find specific biomarkers unique for HF, have had no significant success either,
and we are not much closer to finding a good inflammatory biomarker of HF today than we
were a decade ago. While several authors have suggested a multimarker approach to aid in
prognostication of HF patients, we were not able to build a multimarker model from
biomarkers available in the CORONA population that to any clinical significant degree added
to the discriminatory power of a prognostic model built on clinically available data.40, 48
While some recently suggested biomarkers such as GDF-15 was not available in our data,
this still suggests that a multimarker approach might not necessarily be an easy solution, and
if such an approach is applied, the biomarkers included need to be meticulously selected, and
models carefully validated. Of course, this does not mean that no such panel of biomarkers
can be constructed, but suggest that better, more specific markers are needed if this approach
is to succeed.
5.3.2 NGAL; potentials and difficulties.
The growing interest in NGAL over the last decade primarily as biomarker, but also a
mediator, may be partly ascribed to its well documented association with kidney function.
Several studies have been published on its prognostic abilities in both chronic and acute
HF.134, 157, 158, 195-197 While some previous reports have suggested there may be an association
between NGAL levels and outcome in both conditions, we were not able to reproduce these
findings in our study of chronic HF. However, there are a number of important factors
separating these studies, such as whether NGAL is measured in the circulation or in urine, as
well as the number of patients included and how many variables are adjusted for in the
analysis. As an example, a similar study to ours on NGAL in chronic HF concluded that
NGAL was significantly and independently associated with outcome.198 They measured
NGAL in urine, and did not control for NT-proBNP, possibly explaining our different
findings. As discussed in section 1.4, the source is likely different for urinary and circulating
NGAL, and while they often are closely correlated, they could be differentially regulated in
several conditions.150 This is important to bear in mind for other studies as well, and could
explain some of the discrepancies on NGALs prognostic abilities found in the literature.

50
Furthermore, whether or not NGAL in chronic HF is a marker for a systemic inflammation as
such, or rather a more specific marker of kidney function is not yet certain. In our study in
chronic HF, NGAL was closely associated with kidney function, and adjusting the prognostic
models for eGFR removed any prognostic power of NGAL. This is further supported by
another small study suggesting the kidney function is the most important reason for NGAL
increase in patients with systolic HF.156 Importantly, we only studied patients with systolic
HF secondary to ischemic heart disease – the role of NGAL in HF of other etiologies is still
unclear. Interestingly, in the ACS population NGAL was still strongly associated with eGFR,
but including eGFR in the models did not remove NGAL’s prognostic power suggesting
other causes of increased NGAL levels may be relevant. For ACS in general, the findings on
NGAL are a bit more consistent, and suggest an association between NGAL levels and
outcome.160, 199-201 Nevertheless, further studies are needed to support our findings, and risk
models need to be externally validated. While there are plausible reasons why NGAL could
be linked to outcome in this patient group as discussed in section 1.4, many of the difficulties
with NGAL as a biomarker is equally valid for this group as for HF patients. Its increased
circulating level in a range of different diseases, suggest that there would be a lot of “noise”
when using NGAL as a biomarker for a specific condition.161 NGAL’s better prognostic
abilities in the ACS population could be due to these patients in general being younger, and
having fewer comorbidities, but it cannot be excluded that it also reflects a closer link
between NGAL levels and the development of the disease.
5.3.3 Neutrophils, an important cell type in CVD?
In our studies, we have among other evaluated IL-8 and NGAL, two proteins linked with
neutrophils. One of the main functions of IL-8 is as a chemoattractant for neutrophils, and
NGAL is actively secreted by neutrophils partly in complexes with MMP-9. Similarly, other
studies have found upregulation of MPO, another neutrophil-secreted enzyme, in the
circulation of acute and chronic HF patients as well as patients with ACS, and that the
concentration reflects the severity of the disease.202-205 Others have found worse prognosis for
patients with higher levels of circulating neutrophils, or higher neutrophil to lymphocyte ratio
in patients with ACS as well as acute and chronic HF further.206 Together these findings
suggest that the neutrophils and neutrophil activity is associated with, and could be involved
in the development of CVD. However, this is of course no evidence for neutrophil
involvement and furthermore, even if assuming they are involved in the pathogenesis, there is
no way from these results to conclude if their influence is positive or negative. Some recent

51
findings do however suggest that neutrophils do more than simply correlate with disease in
these patients. As mentioned previously, NGAL and MMP9 are correlated with increased
vulnerability of atherosclerotic plaques (See section 1.4.2). Recent findings have also
demonstrated the presence of pro-thrombotic NETs in culprit lesions in STEMI, suggesting
that neutrophils may not only play a role in the destabilization of plaques, but also in forming
the thrombus when a plaque ruptures.207 Furthermore, a recent study has also shown that the
quantity of NETs in culprit lesions in STEMI correlates negatively with ST resolution and
positively with size of infarction further supporting this notion.208 Our findings together with
others do suggest that neutrophils may be one cell group that warrants a closer examination in
relation to CVD.
5.3.4 Inflammation in HF: a way ahead?
Inflammation is characterized by the complexity of the system, multiple redundancies, and
molecules serving several different roles according to situation and other stimuli present. We
find that some inflammatory markers such as IL-8 are more closely linked to outcome than
others. While our findings do not support a role as biomarker for any of the molecules studied,
they do suggest that a more nuanced view on inflammation in HF is needed. The
discrepancies of findings between our studies and other studies also suggest that HF
populations are not equal, and cytokine levels do not necessarily have the same importance in
all of them. There could be subgroups where higher levels of some cytokines are more linked
with outcome than others. The activation of the immune system in chronic HF is well
established. However, what part of, and when this activation is advantageous or
counterproductive are only partly understood. It is even likely that some parts of the system
may do both, according to the degree of activation, and balance between inflammatory and
anti-inflammatory signals. It is interesting to note that different cytokines seems to be
differential regulated, and while some like IL-6, TNF and CRP are closely correlated (data
not published), others like IL-8 and CRP are not, suggesting that there are differences in
immune regulation and activity among patients. One could speculate that mapping several
cytokines, and looking at the cytokine profile of patients would permit further classification
of patients according to inflammatory profile.190 In addition, further understanding of the role
of inflammation in HF could help towards finding more useful inflammatory biomarkers, or
subpopulations where already suggested biomarkers are more powerful, and could aid in
clinical decision-making.

52
So far, only anti-inflammatory treatments have been attempted in HF patients. Resolving
inflammation is, however, an active process and could be another potential target for
therapy.209 While many of the inflammatory cytokines are closely investigated, and their
potential role in HF mapped to some extent, this is not equally the case for molecules
involved in resolving inflammation. The persistent inflammation seen in HF might be due to
the lack of removal of an inflammatory stimulus, but could just as well be due to failure of
mechanisms in resolution of inflammation itself. This is another path that warrants
exploration, and where findings could both be inspired by, and help further research into
inflammatory biomarkers.
5.4 Biomarkers, any use beyond prognosis?
5.4.1 Current status
As mentioned above, a good biomarker should be possible to measure accurately and
repeatedly, preferably to a reasonable cost and turnaround time. Furthermore, it should
provide additional information to already existing models, and help medical decision
making.35 None of the biomarkers investigated in our studies comes close to fulfilling all
these requirements. Indeed, few if any of the suggested biomarkers for HF in the literature do.
The best candidates so far have been the natriuretic peptides (NPs), notably NT-proBNP and
BNP.40 These have consistently been significantly and independently associated with
outcomes in many studies of chronic HF, and there are some promising studies on NP-guided
therapy, suggesting that these may fulfill the above mentioned criteria, at least in subgroups
of HF patients hospitalized for HF related reasons.210-212 While there have been plenty of
suggested inflammatory biomarkers in HF, few of these have been verified in large enough
studies, or against already existing models. In particular, few have been verified to give
clinically significant data in addition to the NPs. As discussed in paper III, relatively well-
studied inflammatory biomarkers such as TNF, and sTNFR-1 and -2, while associated with
outcomes independent of regular clinical markers, loses this association when adjusting for
NT-proBNP. In this respect, the results of the extensive research on inflammatory biomarkers
in HF are disappointing.
In particular when investigating prototypical inflammatory cytokines, as we do in paper III,
their relevance as potential prognostic biomarkers may be further diminished as these are

53
cytokines upregulated in most diseases with immune activation. While we do show that one
of these, IL-8, demonstrate some potential, it is an important caveat that the typical
population investigated in these studies are from clinical trials, often only including patients
without any other serious comorbidities. However, as HF patients often are elderly, in an
unselected group of patients, there are good reasons to suspect the presence of other
conditions that influence immune activation as well. A reduction of the prognostic abilities of
such prototypical inflammatory markers should thus be expected in unselected populations, at
least for cause specific CV outcomes.
5.4.2 Biomarkers as pathophysiological informants
Part of what makes predicting a likely progression to HF so difficult, is that so many different
processes can lead to its emergence. Several have suggested that, while inflammatory as well
as other biomarkers may not turn out to be strong biomarkers in HF as such, they may
provide significant information on the pathophysiology of the condition.26, 90, 213 Braunwald
proposed six broad categories, later extended to seven, for the classification of researched
biomarkers into classes of different pathological systems. 40, 214 These categories –
inflammation, neurohormonal activation, oxidative stress, matrix remodeling, myocyte injury,
myocardial stress and later added renal dysfunction – illustrate the possible usefulness of
biomarkers to give information on some of the potential pathological causes of HF. While
earlier approaches to the classification of HF has focused on the pathological cause (i.e.
coronary heart disease, cardiomyopathy etc.), and the pathophysiological characteristic (i.e.
preservation or reduction in EF), biomarkers may add a third dimension to this
characterization scheme, reflecting different pathways involved in progression of the
condition. The potential usefulness is not only limited to the experimental setting, but also
underlines the fact that HF patients are not identical, and different underlying etiologies may
profit from tailored treatment and prognostication.
5.4.3 Biomarkers as source of new hypotheses
Findings from biomarker studies may not only suggest pathways involved in the disease, but
also be an inspiration to further research into these pathways. An example may be the
realization that TNF was increased in HF in the early 90s, leading to a wide range of studies
on the influence of TNF on the cardiac system as such.89 While later trials on anti-TNF
therapy may have failed, illustrating the complexity of immune involvement in progression of
HF, this research has given important insights.103 Furthermore, the failure of TNF therapy to

54
significantly improve HF prognosis, does not prove that this approach to finding new
potential targets for HF therapy could not work in the future.103 Biomarker studies could
therefore be regarded as potentially important sources of hypotheses. It is also important to
notice that in our study, TNF, as well as the TNF receptors where not independently
associated with most of the outcomes. If only biomarkers fulfilling the characteristic above
where of scientific interest, the last decades of TNF and HF research would potentially not
have been initiated.
5.4.4 Should there be a shift of focus in biomarker research?
The seven categories mentioned above also illustrate another important aspect. While many
of the parameters included in prognostic models of HF today increases power of the models,
many of them reflect the symptoms and results of HF deterioration, rather than the causes.
This is the case of among others EF, NYHA-class, as well as partly for NT-proBNP and
troponins. While independence of these variables is important when considering the potential
usefulness of a new clinical prognostic biomarker, this is not as evident when using
biomarker studies as an approach to further understand the development of the disease. A
multi-marker approach to study HF patients could be useful even if it did not improve on
already existing prognostication models if it leads to new ways to categorize HF patient, and
potentially aid in therapy selection. After all, choice of therapy is not only a question of how
likely a patient is to die, but also how that patient is likely to respond to the treatment. This
does not necessarily follow from the prognosticated risk. Therefore, while investigating
whether or not a new biomarker adds clinical significant value to existing prognostic models
is important, limiting biomarker research to this aspect may preclude us from important
discoveries. One could for example also consider therapy response and development of
disease according to baseline levels of markers. This could be an argument for putting more
focus on this potential aspect of biomarkers in further studies, and put less weight on the pure
prognostic aspect.
While investigating the seven proposed categories of biomarker could be useful, assuming all
inflammatory markers in the inflammation category give the same type of information is
somewhat premature. Inflammation is an incredibly complex process, and the outcome is
often decided by the balance of different pathways. Looking at only one inflammatory
biomarker may not be enough, and several biomarkers may be needed to entangle the effect.
It is not necessary that the same level of an inflammatory cytokine in one patient will have

55
the same effect as an equal level in another patient, depending on levels of other cytokines
and activity of other systems. This interconnectedness makes the search for inflammatory
biomarkers inherently difficult, and the use of panels of cytokines, or more complicated
systems approaches may be needed.88, 190

56
6 Concluding remarks and future work The results presented in this thesis have further extended our knowledge on the role of some
important inflammatory markers in heart disease. We have assessed the potential as
biomarkers of NGAL in both ACS and HF, as well as several cytokines such as TNF and
related soluble receptors, and IL-8 in HF. Our main conclusions may be summarized as
follows:
Circulating NGAL is not independently associated with mortality and morbidity in
elderly patients with systolic HF of ischemic etiology. While there is a significant
association between NGAL and outcomes when adjusting only for clinical parameters,
including eGFR, CRP and NT-proBNP in the model reveal that NGAL does not seem
to be a good prognostic biomarker for this condition.
However, circulating NGAL at the time of hospitalization for ACS is independently
associated with both short and long term mortality. This is true even when adjusting
for GRACE score as well as other relevant cardiac and inflammatory markers of
disease (EF, CRP and BNP). NGAL leads to a small, non-significant increase in C-
statistics, but a significant increase in NRI. Its potential role as a prognostic biomarker
thus seems to be somewhat limited. However, our findings support further research
into NGAL’s potential role in development and progression of ACS.
When looking at IL-8, MCP-1, TNF and sTNF-R1 and -2, only IL-8 was
independently associated with mortality and morbidity in elderly patients with systolic
HF of ischemic etiology. All variables were however associated with several of the
outcomes when only adjusting for clinical variables. While IL-8 was independently
associated with all outcomes, only a minor non-significant increase in NRI and C-
statistics suggest that IL-8 may not be a very good prognostic biomarker for this
condition. However, our findings support the involvement of inflammation in chronic
HF, and suggest that inflammatory pathways may be differentially regulated. While
others have suggested that TNF and its receptors may be potentially prognostic
biomarkers in chronic HF, our findings do not support this.
While there was some improvement in discriminatory power of the models when
including a panel of multiple biomarkers in addition to previous prognostic models in
HF, the gains were modest and the clinical relevance doubtful. Our findings do not
support the notion that adding biomarkers representing different aspects of HF

57
pathology improves the prognostic abilities of existing risk scores. We cannot,
however, exclude that other panels of biomarkers or similar panels of biomarkers in
other more heterogeneous HF population would result in different results. We also
found no correlation between changes in inflammatory and ECM-related biomarkers
and treatment with rosuvastatin, suggesting that statin treatment in this population has
limited anti-inflammatory effects. There was, however, a tendency for patients with
lower biomarkers scores at baseline to have beneficial effects of rosuvastatin
treatment.
CVD is the leading cause of death in the world today, and there has been some progress in
our understanding of these diseases over the last few decades. In this thesis we have argued
that inflammation, and in particular the innate immune system spearheaded by neutrophils
may be involved in development and progression of both HF and ACS. In particular,
neutrophils could play an important role in plaque vulnerability, and their potential role in
destabilizing atherosclerotic plaques needs further research. While the search for new,
prognostic biomarkers in HF and ACS may not have been very fruitful so far, these studies
may still play a role in mapping systems and molecules potentially involved in the
pathogenesis of the diseases. Further exploitation of this potential could increase the utility of
these studies and help bring research on CVD forward.

58
7 References 1. Braunwald E. Heart failure. JACC Heart failure. 2013;1:1-20. 2. Epelman S, Liu PP and Mann DL. Role of innate and adaptive immune mechanisms in cardiac injury and repair. Nat Rev Immunol. 2015;15:117-129. 3. World Health Organization. Cardiovascular diseases (CVDs). 2013;2013. 4. Mathers CD and Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3:e442. 5. McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Bohm M, Dickstein K, Falk V, Filippatos G, Fonseca C, Gomez-Sanchez MA, Jaarsma T, Kober L, Lip GY, Maggioni AP, Parkhomenko A, Pieske BM, Popescu BA, Ronnevik PK, Rutten FH, Schwitter J, Seferovic P, Stepinska J, Trindade PT, Voors AA, Zannad F, Zeiher A and Guidelines ESCCfP. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012;33:1787-847. 6. Bui AL, Horwich TB and Fonarow GC. Epidemiology and risk profile of heart failure. Nat Rev Cardiol. 2011;8:30-41. 7. Mosterd A and Hoes AW. Clinical epidemiology of heart failure. Heart. 2007;93:1137-46. 8. Lloyd-Jones DM, Larson MG, Leip EP, Beiser A, D'Agostino RB, Kannel WB, Murabito JM, Vasan RS, Benjamin EJ, Levy D and Framingham Heart S. Lifetime risk for developing congestive heart failure: the Framingham Heart Study. Circulation. 2002;106:3068-72. 9. DeFrances CJ, Lucas CA, Buie VC and Golosinskiy A. 2006 National Hospital Discharge Survey. National health statistics reports. 2008:1-20. 10. Levy D, Kenchaiah S, Larson MG, Benjamin EJ, Kupka MJ, Ho KK, Murabito JM and Vasan RS. Long-term trends in the incidence of and survival with heart failure. N Engl J Med. 2002;347:1397-402. 11. Liao L, Allen LA and Whellan DJ. Economic burden of heart failure in the elderly. Pharmacoeconomics. 2008;26:447-62. 12. Lee WC, Chavez YE, Baker T and Luce BR. Economic burden of heart failure: a summary of recent literature. Heart Lung. 2004;33:362-71. 13. Udelson JE. Heart failure with preserved ejection fraction. Circulation. 2011;124:e540-3. 14. Mann DL, Deswal A, Bozkurt B and Torre-Amione G. New therapeutics for chronic heart failure. Annu Rev Med. 2002;53:59-74. 15. Braam B, Cupples WA, Joles JA and Gaillard C. Systemic arterial and venous determinants of renal hemodynamics in congestive heart failure. Heart Fail Rev. 2012;17:161-75. 16. Fu Q, Cao L, Li H, Wang B and Li Z. Cardiorenal syndrome: pathophysiological mechanism, preclinical models, novel contributors and potential therapies. Chin Med J (Engl). 2014;127:3011-8. 17. Braam B, Joles JA, Danishwar AH and Gaillard CA. Cardiorenal syndrome--current understanding and future perspectives. Nature reviews Nephrology. 2014;10:48-55. 18. Triposkiadis F, Starling RC, Boudoulas H, Giamouzis G and Butler J. The cardiorenal syndrome in heart failure: cardiac? renal? syndrome? Heart Fail Rev. 2012;17:355-66. 19. Braunwald E. Heart Failure. JACC: Heart Failure. 2013;1:1-20. 20. Swynghedauw B. Molecular mechanisms of myocardial remodeling. Physiol Rev. 1999;79:215-62. 21. Cohn JN, Ferrari R and Sharpe N. Cardiac remodeling--concepts and clinical implications: a consensus paper from an international forum on cardiac remodeling. Behalf of an International Forum on Cardiac Remodeling. J Am Coll Cardiol. 2000;35:569-82. 22. Mann DL. Inflammatory Mediators and the Failing Heart: Past, Present, and the Foreseeable Future. Circ Res. 2002;91:988-998. 23. Knoll R, Iaccarino G, Tarone G, Hilfiker-Kleiner D, Bauersachs J, Leite-Moreira AF, Sugden PH, Balligand JL and European Society of C. Towards a re-definition of 'cardiac hypertrophy' through a

59
rational characterization of left ventricular phenotypes: a position paper of the Working Group 'Myocardial Function' of the ESC. Eur J Heart Fail. 2011;13:811-9. 24. Heusch G, Libby P, Gersh B, Yellon D, Bohm M, Lopaschuk G and Opie L. Cardiovascular remodelling in coronary artery disease and heart failure. Lancet. 2014;383:1933-43. 25. Li YY, McTiernan CF and Feldman AM. Interplay of matrix metalloproteinases, tissue inhibitors of metalloproteinases and their regulators in cardiac matrix remodeling. Cardiovasc Res. 2000;46:214-24. 26. Mann DL. Innate immunity and the failing heart: the cytokine hypothesis revisited. Circ Res. 2015;116:1254-68. 27. Kirkpatrick JN, Vannan MA, Narula J and Lang RM. Echocardiography in heart failure: applications, utility, and new horizons. J Am Coll Cardiol. 2007;50:381-96. 28. Bassand J-P, Hamm CW, Ardissino D, Boersma E, Budaj A, Fernández-Avilés F, Fox KAA, Hasdai D, Ohman EM, Wallentin L, Wijns W, Vahanian A, Camm J, De Caterina R, Dean V, Dickstein K, Filippatos G, Kristensen SD, Widimsky P, McGregor K, Sechtem U, Tendera M, Hellemans I, Gomez JLZ, Silber S, Funck-Brentano C, Kristensen SD, Andreotti F, Benzer W, Bertrand M, Betriu A, De Caterina R, DeSutter J, Falk V, Ortiz AF, Gitt A, Hasin Y, Huber K, Kornowski R, Lopez-Sendon J, Morais J, Nordrehaug JE, Silber S, Steg PG, Thygesen K, Tubaro M, Turpie AGG, Verheugt F and Windecker S. Guidelines for the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes: The Task Force for the Diagnosis and Treatment of Non-ST-Segment Elevation Acute Coronary Syndromes of the European Society of Cardiology. Eur Heart J. 2007;28:1598-1660. 29. Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, Writing Group on the Joint ESCAAHAWHFTFftUDoMI, Thygesen K, Alpert JS, White HD, Jaffe AS, Katus HA, Apple FS, Lindahl B, Morrow DA, Chaitman BA, Clemmensen PM, Johanson P, Hod H, Underwood R, Bax JJ, Bonow RO, Pinto F, Gibbons RJ, Fox KA, Atar D, Newby LK, Galvani M, Hamm CW, Uretsky BF, Steg PG, Wijns W, Bassand JP, Menasche P, Ravkilde J, Ohman EM, Antman EM, Wallentin LC, Armstrong PW, Simoons ML, Januzzi JL, Nieminen MS, Gheorghiade M, Filippatos G, Luepker RV, Fortmann SP, Rosamond WD, Levy D, Wood D, Smith SC, Hu D, Lopez-Sendon JL, Robertson RM, Weaver D, Tendera M, Bove AA, Parkhomenko AN, Vasilieva EJ, Mendis S and Guidelines ESCCfP. Third universal definition of myocardial infarction. Eur Heart J. 2012;33:2551-67. 30. Members ATF, Steg PG, James SK, Atar D, Badano LP, Lundqvist CB, Borger MA, Di Mario C, Dickstein K, Ducrocq G, Fernandez-Aviles F, Gershlick AH, Giannuzzi P, Halvorsen S, Huber K, Juni P, Kastrati A, Knuuti J, Lenzen MJ, Mahaffey KW, Valgimigli M, van't Hof A, Widimsky P, Zahger D, Guidelines ECfP, Bax JJ, Baumgartner H, Ceconi C, Dean V, Deaton C, Fagard R, Funck-Brentano C, Hasdai D, Hoes A, Kirchhof P, Knuuti J, Kolh P, McDonagh T, Moulin C, Popescu BA, Reiner Ž, Sechtem U, Sirnes PA, Tendera M, Torbicki A, Vahanian A, Windecker S, Reviewers D, Hasdai D, Astin F, Åström-Olsson K, Budaj A, Clemmensen P, Collet J-P, Fox KA, Fuat A, Gustiene O, Hamm CW, Kala P, Lancellotti P, Maggioni AP, Merkely B, Neumann F-J, Piepoli MF, Van de Werf F, Verheugt F and Wallentin L. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC). Eur Heart J. 2012;33:2569-2619. 31. Hamm CW, Bassand J-P, Agewall S, Bax J, Boersma E, Bueno H, Caso P, Dudek D, Gielen S, Huber K, Ohman M, Petrie MC, Sonntag F, Uva MS, Storey RF, Wijns W, Zahger D, Bax JJ, Auricchio A, Baumgartner H, Ceconi C, Dean V, Deaton C, Fagard R, Funck-Brentano C, Hasdai D, Hoes A, Knuuti J, Kolh P, McDonagh T, Moulin C, Poldermans D, Popescu BA, Reiner Ž, Sechtem U, Sirnes PA, Torbicki A, Vahanian A, Windecker S, Windecker S, Achenbach S, Badimon L, Bertrand M, Bøtker HE, Collet J-P, Crea F, Danchin N, Falk E, Goudevenos J, Gulba D, Hambrecht R, Herrmann J, Kastrati A, Kjeldsen K, Kristensen SD, Lancellotti P, Mehilli J, Merkely B, Montalescot G, Neumann F-J, Neyses L, Perk J, Roffi M, Romeo F, Ruda M, Swahn E, Valgimigli M, Vrints CJ and Widimsky P. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes (ACS) in patients

60
presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2011;32:2999-3054. 32. Libby P. Inflammation in atherosclerosis. Nature. 2002;420:868-874. 33. Falk E. Unstable angina with fatal outcome: dynamic coronary thrombosis leading to infarction and/or sudden death. Autopsy evidence of recurrent mural thrombosis with peripheral embolization culminating in total vascular occlusion. Circulation. 1985;71:699-708. 34. Biomarkers Definitions Working Group. Biomarkers and surrogate endpoints: preferred definitions and conceptual framework. Clin Pharmacol Ther. 2001;69:89-95. 35. Vasan RS. Biomarkers of cardiovascular disease: molecular basis and practical considerations. Circulation. 2006;113:2335-62. 36. Aukrust P, Halvorsen B, Yndestad A, Ueland T, Oie E, Otterdal K, Gullestad L and Damas JK. Chemokines and cardiovascular risk. Arterioscler Thromb Vasc Biol. 2008;28:1909-19. 37. Bayes-Genis A, Richards AM, Maisel AS, Mueller C and Ky B. Multimarker testing with ST2 in chronic heart failure. Am J Cardiol. 2015;115:76B-80B. 38. Gaggin HK, Szymonifka J, Bhardwaj A, Belcher A, De Berardinis B, Motiwala S, Wang TJ and Januzzi JL, Jr. Head-to-head comparison of serial soluble ST2, growth differentiation factor-15, and highly-sensitive troponin T measurements in patients with chronic heart failure. JACC Heart failure. 2014;2:65-72. 39. Broch K, Ueland T, Nymo SH, Kjekshus J, Hulthe J, Muntendam P, McMurray JJ, Wikstrand J, Cleland JG, Aukrust P and Gullestad L. Soluble ST2 is associated with adverse outcome in patients with heart failure of ischaemic aetiology. Eur J Heart Fail. 2012;14:268-77. 40. Braunwald E. Biomarkers in heart failure. N Engl J Med. 2008;358:2148-59. 41. Hartupee J and Mann DL. Positioning of inflammatory biomarkers in the heart failure landscape. J Cardiovasc Transl Res. 2013;6:485-92. 42. Bozkurt B, Mann D and Deswal A. Biomarkers of inflammation in heart failure. Heart Fail Rev. 2010;15:331-341. 43. Srivatsan V, George M and Shanmugam E. Utility of galectin-3 as a prognostic biomarker in heart failure: where do we stand? European journal of preventive cardiology. 2015;22:1096-110. 44. Levy WC. Can B-type natriuretic peptides replace heart failure risk models? Eur J Heart Fail. 2008;10:224-5. 45. Morrow DA and de Lemos JA. Benchmarks for the assessment of novel cardiovascular biomarkers. Circulation. 2007;115:949-52. 46. Ketchum ES and Levy WC. Establishing prognosis in heart failure: a multimarker approach. Prog Cardiovasc Dis. 2011;54:86-96. 47. Ketchum ES and Levy WC. Multivariate risk scores and patient outcomes in advanced heart failure. Congest Heart Fail. 2011;17:205-12. 48. Ky B, French B, Levy WC, Sweitzer NK, Fang JC, Wu AHB, Goldberg LR, Jessup M and Cappola TP. Multiple Biomarkers for Risk Prediction in Chronic Heart Failure / Clinical Perspective. Circulation: Heart Failure. 2012;5:183-190. 49. Sharma UC, Pokharel S, van Brakel TJ, van Berlo JH, Cleutjens JP, Schroen B, Andre S, Crijns HJ, Gabius HJ, Maessen J and Pinto YM. Galectin-3 marks activated macrophages in failure-prone hypertrophied hearts and contributes to cardiac dysfunction. Circulation. 2004;110:3121-8. 50. Lala RI, Puschita M, Darabantiu D and Pilat L. Galectin-3 in heart failure pathology--"another brick in the wall"? Acta Cardiol. 2015;70:323-31. 51. McCullough PA. Practical experience using galectin-3 in heart failure. Clin Chem Lab Med. 2014;52:1425-31. 52. de Boer RA, Yu L and van Veldhuisen DJ. Galectin-3 in cardiac remodeling and heart failure. Curr Heart Fail Rep. 2010;7:1-8. 53. McKie PM, AbouEzzeddine OF, Scott CG, Mehta R, Rodeheffer RJ, Redfield MM, Burnett JC, Jr. and Jaffe AS. High-sensitivity troponin I and amino-terminal pro--B-type natriuretic peptide predict heart failure and mortality in the general population. Clin Chem. 2014;60:1225-33.

61
54. Gravning J, Askevold ET, Nymo SH, Ueland T, Wikstrand J, McMurray JJ, Aukrust P, Gullestad L, Kjekshus J and Group CS. Prognostic effect of high-sensitive troponin T assessment in elderly patients with chronic heart failure: results from the CORONA trial. Circ Heart Fail. 2014;7:96-103. 55. Scirica BM, Morrow DA, Budaj A, Dalby AJ, Mohanavelu S, Qin J, Aroesty J, Hedgepeth CM, Stone PH and Braunwald E. Ischemia detected on continuous electrocardiography after acute coronary syndrome: observations from the MERLIN-TIMI 36 (Metabolic Efficiency With Ranolazine for Less Ischemia in Non-ST-Elevation Acute Coronary Syndrome-Thrombolysis In Myocardial Infarction 36) trial. J Am Coll Cardiol. 2009;53:1411-21. 56. James SK, Lindahl B, Siegbahn A, Stridsberg M, Venge P, Armstrong P, Barnathan ES, Califf R, Topol EJ, Simoons ML and Wallentin L. N-terminal pro-brain natriuretic peptide and other risk markers for the separate prediction of mortality and subsequent myocardial infarction in patients with unstable coronary artery disease: a Global Utilization of Strategies To Open occluded arteries (GUSTO)-IV substudy. Circulation. 2003;108:275-81. 57. Bawamia B, Mehran R, Qiu W and Kunadian V. Risk scores in acute coronary syndrome and percutaneous coronary intervention: a review. Am Heart J. 2013;165:441-50. 58. Aragam KG, Tamhane UU, Kline-Rogers E, Li J, Fox KA, Goodman SG, Eagle KA and Gurm HS. Does simplicity compromise accuracy in ACS risk prediction? A retrospective analysis of the TIMI and GRACE risk scores. PLoS ONE. 2009;4:e7947. 59. Alba AC, Agoritsas T, Jankowski M, Courvoisier D, Walter SD, Guyatt GH and Ross HJ. Risk prediction models for mortality in ambulatory patients with heart failure: a systematic review. Circ Heart Fail. 2013;6:881-9. 60. Ketchum ES and Levy WC. Multivariate Risk Scores and Patient Outcomes in Advanced Heart Failure. Congest Heart Fail. 2011;17:205-212. 61. Goldraich L, Beck-da-Silva L and Clausell N. Are scores useful in advanced heart failure? Expert Rev Cardiovasc Ther. 2009;7:985-97. 62. Pocock SJ, Wang D, Pfeffer MA, Yusuf S, McMurray JJ, Swedberg KB, Ostergren J, Michelson EL, Pieper KS and Granger CB. Predictors of mortality and morbidity in patients with chronic heart failure. Eur Heart J. 2006;27:65-75. 63. Levy WC, Mozaffarian D, Linker DT, Sutradhar SC, Anker SD, Cropp AB, Anand I, Maggioni A, Burton P, Sullivan MD, Pitt B, Poole-Wilson PA, Mann DL and Packer M. The Seattle Heart Failure Model: prediction of survival in heart failure. Circulation. 2006;113:1424-33. 64. Chen GY and Nuñez G. Sterile inflammation: sensing and reacting to damage. Nat Rev Immunol. 2010;10:826-837. 65. Sirisinha S. Insight into the mechanisms regulating immune homeostasis in health and disease. Asian Pac J Allergy Immunol. 2011;29:1-14. 66. Parkin J and Cohen B. An overview of the immune system. The Lancet. 2001;357:1777-1789. 67. Takeuchi O and Akira S. Pattern recognition receptors and inflammation. Cell. 2010;140:805-20. 68. Ricklin D, Hajishengallis G, Yang K and Lambris JD. Complement: a key system for immune surveillance and homeostasis. Nature immunology. 2010;11:785-97. 69. Delves PJ and Roitt IM. The immune system. First of two parts. N Engl J Med. 2000;343:37-49. 70. Dy M, Vazquez A, Bertoglio J and Thèze J. General aspects of cytokine properties and functions. In: J. Thèze, ed. The Cytokine Network and Immune Functions: Oxford University Press; 1999: 1-13. 71. Muhl H and Pfeilschifter J. Anti-inflammatory properties of pro-inflammatory interferon-gamma. Int Immunopharmacol. 2003;3:1247-55. 72. Webster JI, Tonelli L and Sternberg EM. Neuroendocrine regulation of immunity. Annu Rev Immunol. 2002;20:125-63. 73. Jaillon S, Galdiero MR, Del Prete D, Cassatella MA, Garlanda C and Mantovani A. Neutrophils in innate and adaptive immunity. Seminars in immunopathology. 2013;35:377-94.

62
74. Kolaczkowska E and Kubes P. Neutrophil recruitment and function in health and inflammation. Nat Rev Immunol. 2013;13:159-75. 75. Borregaard N. Neutrophils, from Marrow to Microbes. Immunity. 2010;33:657-670. 76. Muller WA. Mechanisms of leukocyte transendothelial migration. Annu Rev Pathol. 2011;6:323-44. 77. Flannagan RS, Cosio G and Grinstein S. Antimicrobial mechanisms of phagocytes and bacterial evasion strategies. Nat Rev Microbiol. 2009;7:355-66. 78. Nathan C. Neutrophils and immunity: challenges and opportunities. Nat Rev Immunol. 2006;6:173-82. 79. Nathan CF. Neutrophil activation on biological surfaces. Massive secretion of hydrogen peroxide in response to products of macrophages and lymphocytes. J Clin Invest. 1987;80:1550-60. 80. Borregaard N, Kjeldsen L, Lollike K and Sengelov H. Granules and secretory vesicles of the human neutrophil. Clin Exp Immunol. 1995;101 Suppl 1:6-9. 81. Brinkmann V and Zychlinsky A. Neutrophil extracellular traps: Is immunity the second function of chromatin? J Cell Biol. 2012;198:773-83. 82. Matoszka N, Dzialo J, Tokarz-Deptula B and Deptula W. NET and NETosis - new phenomenon in immunology. Postepy Hig Med Dosw (Online). 2012;66:437-45. 83. Kaplan MJ and Radic M. Neutrophil extracellular traps: double-edged swords of innate immunity. J Immunol. 2012;189:2689-95. 84. Nathan C and Ding A. Nonresolving inflammation. Cell. 2010;140:871-82. 85. Huynh ML, Fadok VA and Henson PM. Phosphatidylserine-dependent ingestion of apoptotic cells promotes TGF-beta1 secretion and the resolution of inflammation. J Clin Invest. 2002;109:41-50. 86. Kennedy AD and DeLeo FR. Neutrophil apoptosis and the resolution of infection. Immunol Res. 2009;43:25-61. 87. Mantovani A, Cassatella MA, Costantini C and Jaillon S. Neutrophils in the activation and regulation of innate and adaptive immunity. Nat Rev Immunol. 2011;11:519-31. 88. Serhan CN. Systems approach to inflammation resolution: identification of novel anti-inflammatory and pro-resolving mediators. J Thromb Haemost. 2009;7 Suppl 1:44-8. 89. Levine B, Kalman J, Mayer L, Fillit HM and Packer M. Elevated circulating levels of tumor necrosis factor in severe chronic heart failure. N Engl J Med. 1990;323:236-41. 90. Kalogeropoulos AP, Georgiopoulou VV and Butler J. From risk factors to structural heart disease: the role of inflammation. Heart Fail Clin. 2012;8:113-23. 91. Wu CK, Lee JK, Chiang FT, Yang CH, Huang SW, Hwang JJ, Lin JL, Tseng CD, Chen JJ and Tsai CT. Plasma levels of tumor necrosis factor-alpha and interleukin-6 are associated with diastolic heart failure through downregulation of sarcoplasmic reticulum Ca2+ ATPase. Crit Care Med. 2011;39:984-92. 92. von Haehling S, Schefold JC, Lainscak M, Doehner W and Anker SD. Inflammatory Biomarkers in Heart Failure Revisited: Much More than Innocent Bystanders. Heart Failure Clinics. 2009;5:549-560. 93. Celis R, Torre-Martinez G and Torre-Amione G. Evidence for activation of immune system in heart failure: is there a role for anti-inflammatory therapy? Curr Opin Cardiol. 2008;23:254-60. 94. Chen D, Assad-Kottner C, Orrego C and Torre-Amione G. Cytokines and acute heart failure. Crit Care Med. 2008;36:S9-16. 95. Parish RC and Evans JD. Inflammation in Chronic Heart Failure. The Annals of Pharmacotherapy. 2008;42:1002-1016. 96. Torre-Amione G. Immune activation in chronic heart failure. Am J Cardiol. 2005;95:3C-8C; discussion 38C-40C. 97. Mari D, Di Berardino F and Cugno M. Chronic heart failure and the immune system. Clin Rev Allergy Immunol. 2002;23:325-40. 98. Sharma R and Anker SD. Immune and neurohormonal pathways in chronic heart failure. Congest Heart Fail. 2002;8:23-8, 48.

63
99. Sharma R, Al-Nasser FO and Anker SD. The importance of tumor necrosis factor and lipoproteins in the pathogenesis of chronic heart failure. Heart failure monitor. 2001;2:42-7. 100. Paulus WJ. Cytokines and heart failure. Heart failure monitor. 2000;1:50-6. 101. Bryant D, Becker L, Richardson J, Shelton J, Franco F, Peshock R, Thompson M and Giroir B. Cardiac failure in transgenic mice with myocardial expression of tumor necrosis factor-alpha. Circulation. 1998;97:1375-81. 102. Kubota T, McTiernan CF, Frye CS, Slawson SE, Lemster BH, Koretsky AP, Demetris AJ and Feldman AM. Dilated cardiomyopathy in transgenic mice with cardiac-specific overexpression of tumor necrosis factor-alpha. Circ Res. 1997;81:627-35. 103. Gullestad L and Aukrust P. Review of trials in chronic heart failure showing broad-spectrum anti-inflammatory approaches. Am J Cardiol. 2005;95:17C-23C; discussion 38C-40C. 104. von Haehling S, Doehner W and Anker SD. The roles of immunity and autoimmunity in chronic heart failure. Ernst Schering Research Foundation workshop. 2006:155-68. 105. Anker SD, Egerer KR, Volk HD, Kox WJ, Poole-Wilson PA and Coats AJ. Elevated soluble CD14 receptors and altered cytokines in chronic heart failure. Am J Cardiol. 1997;79:1426-30. 106. Conraads V. Pro-inflammatory cytokines and their receptors in chronic heart failure: do they really matter? Acta Cardiol. 2006;61:161-8. 107. Colombo PC, Ganda A, Lin J, Onat D, Harxhi A, Iyasere JE, Uriel N and Cotter G. Inflammatory activation: cardiac, renal, and cardio-renal interactions in patients with the cardiorenal syndrome. Heart Fail Rev. 2012;17:177-90. 108. Tsutamoto T, Wada A, Maeda K, Mabuchi N, Hayashi M, Tsutsui T, Ohnishi M, Sawaki M, Fujii M, Matsumoto T and Kinoshita M. Angiotensin II type 1 receptor antagonist decreases plasma levels of tumor necrosis factor alpha, interleukin-6 and soluble adhesion molecules in patients with chronic heart failure. J Am Coll Cardiol. 2000;35:714-21. 109. Ruiz-Ortega M, Ruperez M, Lorenzo O, Esteban V, Blanco J, Mezzano S and Egido J. Angiotensin II regulates the synthesis of proinflammatory cytokines and chemokines in the kidney. Kidney Int Suppl. 2002:S12-22. 110. Kalra D, Sivasubramanian N and Mann DL. Angiotensin II induces tumor necrosis factor biosynthesis in the adult mammalian heart through a protein kinase C-dependent pathway. Circulation. 2002;105:2198-205. 111. Prabhu SD, Chandrasekar B, Murray DR and Freeman GL. beta-adrenergic blockade in developing heart failure: effects on myocardial inflammatory cytokines, nitric oxide, and remodeling. Circulation. 2000;101:2103-9. 112. Fildes JE, Shaw SM, Yonan N and Williams SG. The immune system and chronic heart failure: is the heart in control? J Am Coll Cardiol. 2009;53:1013-20. 113. Frantz S, Bauersachs J and Ertl G. Post-infarct remodelling: contribution of wound healing and inflammation. Cardiovasc Res. 2009;81:474-81. 114. Yndestad A, Damås J, Øie E, Ueland T, Gullestad L and Aukrust P. Role of inflammation in the progression of heart failure. Curr Cardiol Rep. 2007;9:236-241. 115. Yndestad A, Kristian Damås J, Øie E, Ueland T, Gullestad L and Aukrust P. Systemic inflammation in heart failure – The whys and wherefores. Heart Fail Rev. 2006;11:83-92. 116. Kawasaki T, Kawai T and Akira S. Recognition of nucleic acids by pattern-recognition receptors and its relevance in autoimmunity. Immunol Rev. 2011;243:61-73. 117. Takeda K and Akira S. Regulation of innate immune responses by Toll-like receptors. Jpn J Infect Dis. 2001;54:209-19. 118. Boyd JH, Mathur S, Wang Y, Bateman RM and Walley KR. Toll-like receptor stimulation in cardiomyoctes decreases contractility and initiates an NF-kappaB dependent inflammatory response. Cardiovasc Res. 2006;72:384-93. 119. Frantz S, Ertl G and Bauersachs J. Mechanisms of disease: Toll-like receptors in cardiovascular disease. Nat Clin Pract Cardiovasc Med. 2007;4:444-54.

64
120. Sun M, Chen M, Dawood F, Zurawska U, Li JY, Parker T, Kassiri Z, Kirshenbaum LA, Arnold M, Khokha R and Liu PP. Tumor necrosis factor-alpha mediates cardiac remodeling and ventricular dysfunction after pressure overload state. Circulation. 2007;115:1398-407. 121. Chen Y, Pat B, Zheng J, Cain L, Powell P, Shi K, Sabri A, Husain A and Dell'italia LJ. Tumor necrosis factor-alpha produced in cardiomyocytes mediates a predominant myocardial inflammatory response to stretch in early volume overload. J Mol Cell Cardiol. 2010;49:70-8. 122. von Haehling S and Anker SD. Future prospects of anticytokine therapy in chronic heart failure. Expert Opin Investig Drugs. 2005;14:163-76. 123. Strom JB and Libby P. Atherosclerosis. In: L. S. Lilly, ed. Pathophysiology of heart disease. 5 ed.: Lippincott Williams & Wilkins; 2011. 124. Libby P. Inflammation in atherosclerosis. Arterioscler Thromb Vasc Biol. 2012;32:2045-51. 125. Guzik TJ, West NE, Black E, McDonald D, Ratnatunga C, Pillai R and Channon KM. Vascular superoxide production by NAD(P)H oxidase: association with endothelial dysfunction and clinical risk factors. Circ Res. 2000;86:E85-90. 126. Nielsen LB. Transfer of low density lipoprotein into the arterial wall and risk of atherosclerosis. Atherosclerosis. 1996;123:1-15. 127. Mitra S, Goyal T and Mehta JL. Oxidized LDL, LOX-1 and atherosclerosis. Cardiovasc Drugs Ther. 2011;25:419-29. 128. Galkina E and Ley K. Immune and inflammatory mechanisms of atherosclerosis (*). Annu Rev Immunol. 2009;27:165-97. 129. Raffetto JD and Khalil RA. Matrix metalloproteinases and their inhibitors in vascular remodeling and vascular disease. Biochem Pharmacol. 2008;75:346-59. 130. Gijsen F, van der Giessen A, van der Steen A and Wentzel J. Shear stress and advanced atherosclerosis in human coronary arteries. J Biomech. 2013;46:240-7. 131. Frangogiannis NG. The inflammatory response in myocardial injury, repair, and remodelling. Nat Rev Cardiol. 2014;11:255-65. 132. Kjeldsen L, Johnsen AH, Sengeløv H and Borregaard N. Isolation and primary structure of NGAL, a novel protein associated with human neutrophil gelatinase. J Biol Chem. 1993;268:10425-10432. 133. Virzi GM, Clementi A, de Cal M, Cruz DN and Ronco C. Genomics and biological activity of neutrophil gelatinase-associated lipocalin in several clinical settings. Blood Purif. 2013;35:139-43. 134. Iqbal N, Choudhary R, Chan J, Wentworth B, Higginbotham E and Maisel AS. Neutrophil gelatinase-associated lipocalin as diagnostic and prognostic tool for cardiovascular disease and heart failure. Expert opinion on medical diagnostics. 2013;7:209-20. 135. Bolignano D, Coppolino G, Lacquaniti A and Buemi M. From kidney to cardiovascular diseases: NGAL as a biomarker beyond the confines of nephrology. Eur J Clin Invest. 2010;40:273-276. 136. Bolignano D, Donato V, Coppolino G, Campo S, Buemi A, Lacquaniti A and Buemi M. Neutrophil Gelatinase-Associated Lipocalin (NGAL) as a Marker of Kidney Damage. Am J Kidney Dis. 2008;52:595-605. 137. Flo TH, Smith KD, Sato S, Rodriguez DJ, Holmes MA, Strong RK, Akira S and Aderem A. Lipocalin 2 mediates an innate immune response to bacterial infection by sequestrating iron. Nature. 2004;432:917-921. 138. Devarajan PRAS. Review: Neutrophil gelatinase-associated lipocalin: A troponin-like biomarker for human acute kidney injury. Nephrology. 2010;15:419-428. 139. Damman K, Masson S, Hillege HL, Maggioni AP, Voors AA, Opasich C, van Veldhuisen DJ, Montagna L, Cosmi F, Tognoni G, Tavazzi L and Latini R. Clinical outcome of renal tubular damage in chronic heart failure. Eur Heart J. 2011. 140. Yndestad A, Landrø L, Ueland T, Dahl CP, Flo TH, Vinge LE, Espevik T, Frøland SS, Husberg C, Christensen G, Dickstein K, Kjekshus J, Øie E, Gullestad L and Aukrust P. Increased systemic and myocardial expression of neutrophil gelatinase-associated lipocalin in clinical and experimental heart failure. Eur Heart J. 2009;30:1229-1236.

65
141. Eagan T M, Damås J, Ueland T, Voll-Aanerud M, Mollnes T, Hardie J, Bakke P and Aukrust aP. Neutrophil Gelatinase-Associated Lipocalin: A Biomarker in COPD. Chest. 2010;138:888-895. 142. Bolignano D, Donato V, Lacquaniti A, Fazio MR, Bono C, Coppolino G and Buemi M. Neutrophil gelatinase-associated lipocalin (NGAL) in human neoplasias: A new protein enters the scene. Cancer Lett. 2010;288:10-16. 143. Paragas N, Qiu A, Hollmen M, Nickolas TL, Devarajan P and Barasch J. NGAL-Siderocalin in kidney disease. Biochim Biophys Acta. 2012;1823:1451-8. 144. Schmidt-Ott KM, Mori K, Li JY, Kalandadze A, Cohen DJ, Devarajan P and Barasch J. Dual Action of Neutrophil Gelatinase-Associated Lipocalin. J Am Soc Nephrol. 2007;18:407-413. 145. Chakraborty S, Kaur S, Guha S and Batra SK. The multifaceted roles of neutrophil gelatinase associated lipocalin (NGAL) in inflammation and cancer. Biochimica et Biophysica Acta (BBA) - Reviews on Cancer. 2012;1826:129-169. 146. Mori K, Lee HT, Rapoport D, Drexler IR, Foster K, Yang J, Schmidt-Ott KM, Chen X, Li JY, Weiss S, Mishra J, Cheema FH, Markowitz G, Suganami T, Sawai K, Mukoyama M, Kunis C, D’Agati V, Devarajan P and Barasch J. Endocytic delivery of lipocalin-siderophore-iron complex rescues the kidney from ischemia-reperfusion injury. The Journal of Clinical Investigation. 2005;115:610-621. 147. Te Boekhorst BC, Bovens SM, Hellings WE, van der Kraak PH, van de Kolk KW, Vink A, Moll FL, van Oosterhout MF, de Vries JP, Doevendans PA, Goumans MJ, de Kleijn DP, van Echteld CJ, Pasterkamp G and Sluijter JP. Molecular MRI of murine atherosclerotic plaque targeting NGAL: a protein associated with unstable human plaque characteristics. Cardiovasc Res. 2010. 148. Forsblad J, Gottsater A, Persson K, Jacobsson L and Lindgarde F. Clinical manifestations of atherosclerosis in an elderly population are related to plasma neopterin, NGAL and endothelin-1, but not to Chlamydia pneumoniae serology. Int Angiol. 2002;21:173-9. 149. Hemdahl AL, Gabrielsen A, Zhu C, Eriksson P, Hedin U, Kastrup J, Thoren P and Hansson GK. Expression of neutrophil gelatinase-associated lipocalin in atherosclerosis and myocardial infarction. Arterioscler Thromb Vasc Biol. 2006;26:136-42. 150. Grigoryev DN, Liu M, Hassoun HT, Cheadle C, Barnes KC and Rabb H. The Local and Systemic Inflammatory Transcriptome after Acute Kidney Injury. J Am Soc Nephrol. 2008;19:547-558. 151. McCullough PA, Shaw AD, Haase M, Bouchard J, Waikar SS, Siew ED, Murray PT, Mehta RL and Ronco C. Diagnosis of acute kidney injury using functional and injury biomarkers: workgroup statements from the tenth Acute Dialysis Quality Initiative Consensus Conference. Contrib Nephrol. 2013;182:13-29. 152. Vanmassenhove J, Vanholder R, Nagler E and Van Biesen W. Urinary and serum biomarkers for the diagnosis of acute kidney injury: an in-depth review of the literature. Nephrol Dial Transplant. 2013;28:254-73. 153. Lindberg S, Pedersen SH, Mogelvang R, Jensen JS, Flyvbjerg A, Galatius S and Magnusson NE. Prognostic Utility of Neutrophil Gelatinase-Associated Lipocalin in Predicting Mortality and Cardiovascular Events in Patients With ST-Segment Elevation Myocardial Infarction Treated With Primary Percutaneous Coronary Intervention. J Am Coll Cardiol. 2012;60:339-45. 154. Ramos-Mozo P, Madrigal-Matute J, Vega de Ceniga M, Blanco-Colio LM, Meilhac O, Feldman L, Michel JB, Clancy P, Golledge J, Norman PE, Egido J and Martin-Ventura JL. Increased plasma levels of NGAL, a marker of neutrophil activation, in patients with abdominal aortic aneurysm. Atherosclerosis. 2012;220:552-6. 155. Dwipa L, Soelaeman R, Roesli RM, Martanto E and Adhiarta IG. Cardiometabolic risk factors and acute kidney injury based on urinary neutrophil gelatinase associated lipocalin (NGALu) in acute coronary syndrome patients. Acta Med Indones. 2012;44:3-9. 156. Shrestha K, Borowski AG, Troughton RW, Thomas JD, Klein AL and Tang WH. Renal dysfunction is a stronger determinant of systemic neutrophil gelatinase-associated lipocalin levels than myocardial dysfunction in systolic heart failure. J Card Fail. 2011;17:472-8. 157. Maisel AS, Mueller C, Fitzgerald R, Brikhan R, Hiestand BC, Iqbal N, Clopton P and van Veldhuisen DJ. Prognostic utility of plasma neutrophil gelatinase-associated lipocalin in patients with

66
acute heart failure: The NGAL EvaLuation Along with B-type NaTriuretic Peptide in acutely decompensated heart failure (GALLANT) trial. Eur J Heart Fail. 2011;13:846-851. 158. Nymo SH, Ueland T, Askevold ET, Flo TH, Kjekshus J, Hulthe J, Wikstrand J, McMurray J, Van Veldhuisen DJ, Gullestad L, Aukrust P and Yndestad A. The association between neutrophil gelatinase-associated lipocalin and clinical outcome in chronic heart failure: results from CORONA(*). J Intern Med. 2011. 159. Soylu K, Aksan G, Nar G, Ozdemir M, Gulel O, Inci S, Aksakal A, Soylu AI and Yilmaz O. Serum neutrophil gelatinase-associated lipocalin levels are correlated with the complexity and the severity of atherosclerosis in acute coronary syndrome. Anatolian journal of cardiology. 2015;15:450-5. 160. Helanova K, Littnerova S, Kubena P, Ganovska E, Pavlusova M, Kubkova L, Jarkovsky J, Pavkova Goldbergova M, Lipkova J, Gottwaldova J, Kala P, Toman O, Dastych M, Spinar J and Parenica J. Prognostic impact of neutrophil gelatinase-associated lipocalin and B-type natriuretic in patients with ST-elevation myocardial infarction treated by primary PCI: a prospective observational cohort study. BMJ open. 2015;5:e006872. 161. Martensson J and Bellomo R. The rise and fall of NGAL in acute kidney injury. Blood Purif. 2014;37:304-10. 162. Kjekshus J, Apetrei E, Barrios V, Böhm M, Cleland JGF, Cornel JH, Dunselman P, Fonseca C, Goudev A, Grande P, Gullestad L, Hjalmarson Å, Hradec J, Jánosi A, Kamenský G, Komajda M, Korewicki J, Kuusi T, Mach F, Mareev V, McMurray JJV, Ranjith N, Schaufelberger M, Vanhaecke J, van Veldhuisen DJ, Waagstein F, Wedel H and Wikstrand J. Rosuvastatin in Older Patients with Systolic Heart Failure. N Engl J Med. 2007;357:2248-2261. 163. Nymo SH, Hulthe J, Ueland T, McMurray J, Wikstrand J, Askevold ET, Yndestad A, Gullestad L and Aukrust P. Inflammatory cytokines in chronic heart failure: interleukin-8 is associated with adverse outcome. Results from CORONA. Eur J Heart Fail. 2014;16:68-75. 164. Omland T, Persson A, Ng L, O'Brien R, Karlsson T, Herlitz J, Hartford M and Caidahl K. N-terminal pro-B-type natriuretic peptide and long-term mortality in acute coronary syndromes. Circulation. 2002;106:2913-8. 165. Pencina MJ, D'Agostino RB and Vasan RS. Statistical methods for assessment of added usefulness of new biomarkers. Clin Chem Lab Med. 2010;48:1703-11. 166. Pencina MJ, D'Agostino RB and Steyerberg EW. Extensions of net reclassification improvement calculations to measure usefulness of new biomarkers. Stat Med. 2011;30:11-21. 167. Gönen M and Heller G. Concordance probability and discriminatory power in proportional hazards regression. Biometrika. 2005;92:965-970. 168. White IR, Royston P and Wood AM. Multiple imputation using chained equations: Issues and guidance for practice. Stat Med. 2011;30:377-399. 169. Rubin D. Multiple Imputation for nonresponse in surveys.: John Wiley & Sons; 1987. 170. Zhou X, Fragala MS, McElhaney JE and Kuchel GA. Conceptual and methodological issues relevant to cytokine and inflammatory marker measurements in clinical research. Curr Opin Clin Nutr Metab Care. 2010;13:541-7. 171. Thavasu PW, Longhurst S, Joel SP, Slevin ML and Balkwill FR. Measuring cytokine levels in blood. Importance of anticoagulants, processing, and storage conditions. J Immunol Methods. 1992;153:115-24. 172. Keustermans GC, Hoeks SB, Meerding JM, Prakken BJ and de Jager W. Cytokine assays: an assessment of the preparation and treatment of blood and tissue samples. Methods. 2013;61:10-7. 173. Itenov TS, Bangert K, Christensen PH, Jensen JU, Bestle MH, Procalcitonin and Survival Study -study g. Serum and plasma neutrophil gelatinase associated lipocalin (NGAL) levels are not equivalent in patients admitted to intensive care. J Clin Lab Anal. 2014;28:163-7. 174. de Jager W, Bourcier K, Rijkers GT, Prakken BJ and Seyfert-Margolis V. Prerequisites for cytokine measurements in clinical trials with multiplex immunoassays. BMC Immunol. 2009;10:52.

67
175. Pedersen KR, Ravn HB, Hjortdal VE, Nørregaard R and Povlsen JV. Neutrophil Gelatinase-Associated Lipocalin (NGAL): Validation of commercially available ELISA. Scand J Clin Lab Invest. 2010;70:374-382. 176. Landrø L, Damås JK, Flo TH, Heggelund L, Ueland T, Tjønnfjord GE, Espevik T, Aukrust P and Frøland SS. Decreased serum lipocalin-2 levels in human immunodeficiency virus-infected patients: increase during highly active anti-retroviral therapy. Clin Exp Immunol. 2008;152:57-63. 177. Shepherd J, Hunninghake DB, Stein EA, Kastelein JJ, Harris S, Pears J and Hutchinson HG. Safety of rosuvastatin. Am J Cardiol. 2004;94:882-8. 178. Donders AR, van der Heijden GJ, Stijnen T and Moons KG. Review: a gentle introduction to imputation of missing values. J Clin Epidemiol. 2006;59:1087-91. 179. Burton A and Altman DG. Missing covariate data within cancer prognostic studies: a review of current reporting and proposed guidelines. Br J Cancer. 2004;91:4-8. 180. Pepe MS, Janes H, Longton G, Leisenring W and Newcomb P. Limitations of the odds ratio in gauging the performance of a diagnostic, prognostic, or screening marker. Am J Epidemiol. 2004;159:882-90. 181. Uno H, Cai T, Pencina MJ, D'Agostino RB and Wei LJ. On the C-statistics for evaluating overall adequacy of risk prediction procedures with censored survival data. Stat Med. 2011;30:1105-17. 182. Gail MH and Pfeiffer RM. On criteria for evaluating models of absolute risk. Biostatistics. 2005;6:227-39. 183. Widera C, Pencina MJ, Bobadilla M, Reimann I, Guba-Quint A, Marquardt I, Bethmann K, Korf-Klingebiel M, Kempf T, Lichtinghagen R, Katus HA, Giannitsis E and Wollert KC. Incremental Prognostic Value of Biomarkers beyond the GRACE (Global Registry of Acute Coronary Events) Score and High-Sensitivity Cardiac Troponin T in Non-ST-Elevation Acute Coronary Syndrome. Clin Chem. 2013. 184. Cook NR. Use and misuse of the receiver operating characteristic curve in risk prediction. Circulation. 2007;115:928-35. 185. Steyerberg EW, Pencina MJ, Lingsma HF, Kattan MW, Vickers AJ and Van Calster B. Assessing the incremental value of diagnostic and prognostic markers: a review and illustration. Eur J Clin Invest. 2012;42:216-28. 186. Mallett S, Royston P, Dutton S, Waters R and Altman DG. Reporting methods in studies developing prognostic models in cancer: a review. BMC Med. 2010;8:20. 187. Royston P and Altman D. External validation of a Cox prognostic model: principles and methods. BMC Med Res Methodol. 2013;13:33. 188. Collins GS, Reitsma JB, Altman DG and Moons KG. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD statement. BMJ. 2015;350:g7594. 189. Bleeker SE, Moll HA, Steyerberg EW, Donders AR, Derksen-Lubsen G, Grobbee DE and Moons KG. External validation is necessary in prediction research: a clinical example. J Clin Epidemiol. 2003;56:826-32. 190. Vistnes M, Christensen G and Omland T. Multiple cytokine biomarkers in heart failure. Expert Rev Mol Diagn. 2010;10:147-57. 191. Hedayat M, Mahmoudi MJ, Rose NR and Rezaei N. Proinflammatory cytokines in heart failure: double-edged swords. Heart Fail Rev. 2010;15:543-62. 192. Deswal A, Petersen NJ, Feldman AM, Young JB, White BG and Mann DL. Cytokines and Cytokine Receptors in Advanced Heart Failure : An Analysis of the Cytokine Database from the Vesnarinone Trial (VEST). Circulation. 2001;103:2055-2059. 193. Dunlay SM, Weston SA, Redfield MM, Killian JM and Roger VL. Tumor necrosis factor-alpha and mortality in heart failure: a community study. Circulation. 2008;118:625-31. 194. Ferrari R, Bachetti T, Confortini R, Opasich C, Febo O, Corti A, Cassani G and Visioli O. Tumor Necrosis Factor Soluble Receptors in Patients With Various Degrees of Congestive Heart Failure. Circulation. 1995;92:1479-1486.

68
195. Singer E, Marko L, Paragas N, Barasch J, Dragun D, Muller DN, Budde K and Schmidt-Ott KM. Neutrophil gelatinase-associated lipocalin: pathophysiology and clinical applications. Acta Physiol. 2013. 196. Macdonald S, Arendts G, Nagree Y and Xu XF. Neutrophil Gelatinase-Associated Lipocalin (NGAL) predicts renal injury in acute decompensated cardiac failure: a prospective observational study. BMC Cardiovasc Disord. 2012;12:8. 197. Damman K, van Veldhuisen DJ, Navis G, Voors AA and Hillege HL. Urinary neutrophil gelatinase associated lipocalin (NGAL), a marker of tubular damage, is increased in patients with chronic heart failure. Eur J Heart Fail. 2008;10:997-1000. 198. Damman K, Van Veldhuisen DJ, Navis G, Vaidya VS, Smilde TD, Westenbrink BD, Bonventre JV, Voors AA and Hillege HL. Tubular damage in chronic systolic heart failure is associated with reduced survival independent of glomerular filtration rate. Heart. 2010;96:1297-302. 199. Kafkas N, Demponeras C, Zoubouloglou F, Spanou L, Babalis D and Makris K. Serum levels of gelatinase associated lipocalin as indicator of the inflammatory status in coronary artery disease. International journal of inflammation. 2012;2012:189797. 200. Akcay AB, Ozlu MF, Sen N, Cay S, Ozturk OH, Yalcn F, Bilen P, Kanat S, Karakas MF, Isleyen A, Demir AD, Sogut S, Covic A and Kanbay M. Prognostic significance of neutrophil gelatinase-associated lipocalin in ST-segment elevation myocardial infarction. J Investig Med. 2012;60:508-13. 201. Sahinarslan A, Kocaman SA, Bas D, Akyel A, Ercin U, Zengin O and Timurkaynak T. Plasma neutrophil gelatinase-associated lipocalin levels in acute myocardial infarction and stable coronary artery disease. Coron Artery Dis. 2011;22:333-8. 202. Anatoliotakis N, Deftereos S, Bouras G, Giannopoulos G, Tsounis D, Angelidis C, Kaoukis A and Stefanadis C. Myeloperoxidase: expressing inflammation and oxidative stress in cardiovascular disease. Curr Top Med Chem. 2013;13:115-38. 203. Tang WH, Brennan ML, Philip K, Tong W, Mann S, Van Lente F and Hazen SL. Plasma myeloperoxidase levels in patients with chronic heart failure. Am J Cardiol. 2006;98:796-9. 204. Yonezawa K, Morimoto N, Matsui K, Tenjin T, Yoneda M, Emoto T, Sawada T, Nomura T, Okamoto H, Takarada A, Ikeda H and Ito M. Significance of the neutrophil myeloperoxidase index in patients with atherosclerotic diseases. Kobe J Med Sci. 2012;58:E128-37. 205. Reichlin T, Socrates T, Egli P, Potocki M, Breidthardt T, Arenja N, Meissner J, Noveanu M, Reiter M, Twerenbold R, Schaub N, Buser A and Mueller C. Use of myeloperoxidase for risk stratification in acute heart failure. Clin Chem. 2010;56:944-51. 206. Bhat T, Teli S, Rijal J, Bhat H, Raza M, Khoueiry G, Meghani M, Akhtar M and Costantino T. Neutrophil to lymphocyte ratio and cardiovascular diseases: a review. Expert Rev Cardiovasc Ther. 2013;11:55-9. 207. Stakos DA, Kambas K, Konstantinidis T, Mitroulis I, Apostolidou E, Arelaki S, Tsironidou V, Giatromanolaki A, Skendros P, Konstantinides S and Ritis K. Expression of functional tissue factor by neutrophil extracellular traps in culprit artery of acute myocardial infarction. Eur Heart J. 2015;36:1405-14. 208. Mangold A, Alias S, Scherz T, Hofbauer T, Jakowitsch J, Panzenbock A, Simon D, Laimer D, Bangert C, Kammerlander A, Mascherbauer J, Winter MP, Distelmaier K, Adlbrecht C, Preissner KT and Lang IM. Coronary neutrophil extracellular trap burden and deoxyribonuclease activity in ST-elevation acute coronary syndrome are predictors of ST-segment resolution and infarct size. Circ Res. 2015;116:1182-92. 209. Buckley CD, Gilroy DW, Serhan CN, Stockinger B and Tak PP. The resolution of inflammation. Nat Rev Immunol. 2013;13:59-66. 210. De Vecchis R, Esposito C and Cantatrione S. Natriuretic peptide-guided therapy : Further research required for still-unresolved issues. Herz. 2013. 211. Januzzi JL, Jr. The role of natriuretic peptide testing in guiding chronic heart failure management: review of available data and recommendations for use. Archives of cardiovascular diseases. 2012;105:40-50.

69
212. Xin W, Lin Z and Mi S. Does B-type natriuretic peptide-guided therapy improve outcomes in patients with chronic heart failure? A systematic review and meta-analysis of randomized controlled trials. Heart Fail Rev. 2015;20:69-80. 213. Bouras G, Giannopoulos G, Hatzis G, Alexopoulos D, Leventopoulos G and Deftereos S. Inflammation and chronic heart failure: from biomarkers to novel anti-inflammatory therapeutic strategies. Med Chem. 2014;10:682-99. 214. Braunwald E. Biomarkers in heart failure. Preface. Heart Fail Clin. 2009;5:xiii-xiv.