Embed Size (px)
Citation preview
Inflammatory Abdominal Aortic Aneurysms:A Report of Thirty-Seven Cases
J. Hill, MB, ChB, D. Charlesworth, DSc, FRCS Manchester, UnitedKingdom
Of a total of 780 patients with abdominal aortic aneurysms, 37 patients (4.7 01&) hadInflammatory aneurysms. Presenting symptoms included back and abdominal pain(76%), leg edema, melena, uremia, claudication and pancreatitis. Mean erythrocyte sedimentation rate was 45 mm/hr. Weight loss and anorexia were common.Elevated urea and creatinine were seen on 11 patients, nine of whom had obstructive uropathy. Average aneurysm size was 9.3 em. Thirty-six patients were treatedsurgically and one was observed. Involvement of the suprarenal (nine cases) orthoracic (three cases) aorta was common. Elective operations included resectionand grafting in 21 patients and axillofemoral bypass in four patients. Patients withureteral entrapment underwent simultaneous ureterolysis. Among the electiveoperations four deaths were noted (1501&). Ten emergency operations were donefor posterior rupture (four cases), aortoduodenal fistula (one case), inferior venacava obstruction or fistula (two cases), hemorrhage into the aneurysmal wall (twocases), or presumed rupture (one case). There were seven deaths (70%) in thisgroup. The operation of choice for inflammatory aneurysm is a bifurcation graftcombined with ureterolysis.
KEY WORDS: Aneurysms; inflammatory abdominal aortic aneurysms; ureterolysis, combined with bifurcation graft.
Inflammatory abdominal aortic aneurysm is nowrecognized as a clinical entity distinct from the morecommon atherosclerotic aneurysm. As they constituteonly 5-150/0 [1-4] of all abdominal aortic aneurysms,most surgeons have only a limited experience withtheir management and the technical difficulties thatthey present.
.These difficulties result from the dense adherence ofadjacent structures to the aorta such as duodenum,inferior vena cava, and ureter.
Most published series of inflammatory aneurysms
From the Department of Surgery, University Hospital ofSouth Manchester, West Didsbury, Manchester, UnitedKingdom.
Reprint requests: D. Charlesworth, D.Sc., Department ofSurgery, University Hospital of South Manchester, WestDidsbury, Manchester, United Kingdom, M20 8LR.
352
have involved small numbers of patients from whom ithas been difficult to draw conclusions.
Therapeutic dilemmas currently exist as to whetherto treat the aneurysms surgically or with steroids andhow best to manage the patient with associatedobstructive uropathy.
We report our experience of 37 patients with theinflammatory type of abdominal aortic aneurysm.
PATIENTS AND METHODS
Seven hundred-eighty patients with abdominal aortic aneurysms presented to the Vascular Unit of theUniversity Hospital of South Manchester between1975 and 1987. Thirty-seven of these patients (4.74%)were diagnosed as having inflammatory aortic aneurysms as first described by Walker and associates [1].
VOLUME 2No 4 - 1988 INFLA~fMATORYAAA~ 353
There were 33 men and four women patients. Theirages at diagnosis ranged from 52 to 81 years with amean of 66.03 years. Fourteen patients were aged over70 years. Twenty-four patients were smokers, eighthad smoked previously and only five were nonsmokers. Average length of history was 6.9 months.
Presenting symptoms were pain, both abdominaland in the back in 28 (75.70/0), bilateral edema of theleg in two, claudication in one, melaena in one, uremiain two, and acute pancreatitis in one. Two patientswere asymptomatic but were noted to have a pulsationin the abdomen on routine medical examination.
Weight loss and anorexia were common complaints.Notably, 41% of patients had an average weight lossof 7.7 kg prior to admission. The only other author tohave commented on these as presenting symptoms wasCrawford and colleagues [5]. Only four patients gavea history of intermittent claudication.
Examination revealed an aortic aneurysm in allpatients. Eleven patients (29.7%) had a tender aneurysm on palpation. In 26 patients (70.3%) all theperipheral pulses were present. Hypertension occurredin 16% of patients.
INVESTIGATIONS
The mean white blood cell count was 9.13 X 1061mm' and mean hemoglobin was 13.12 g/dl, Bloodurea and creatinine levels were elevated in 11 patients,nine of whom had an obstructive uropathy. The meanerythrocyte sedimentation rate (ESR) was 45.1 mmlhr.
SPECIAL STUDIES
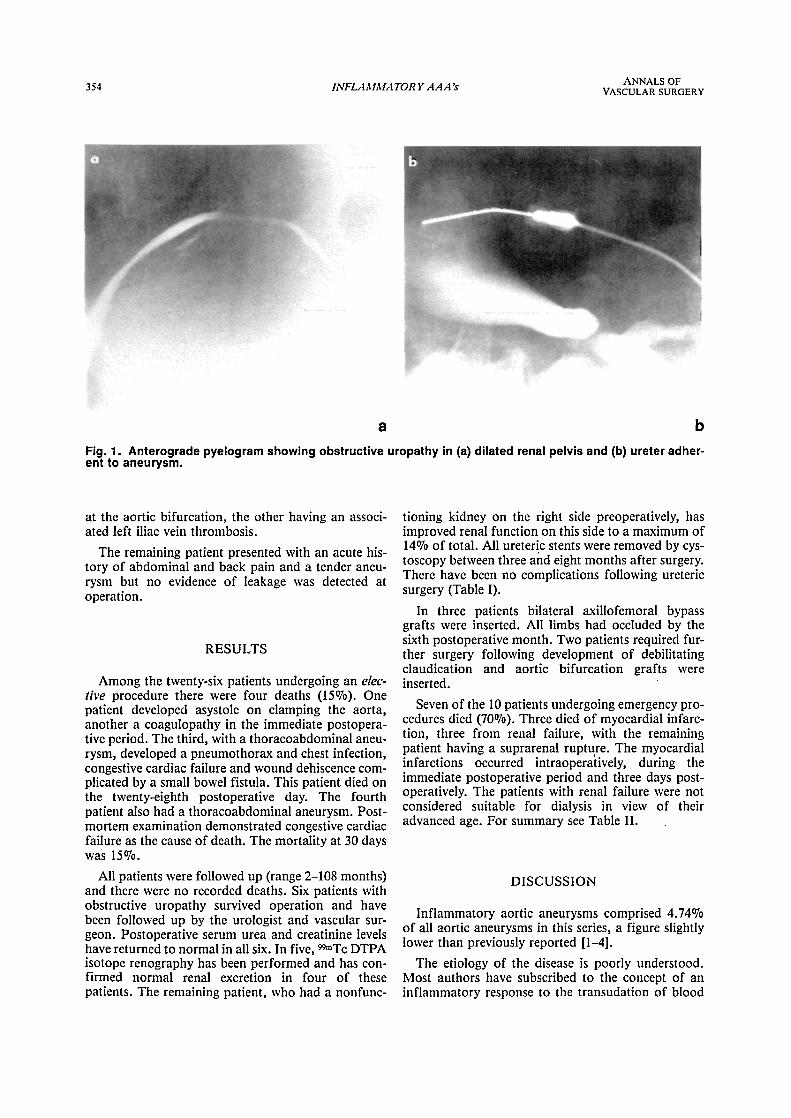
Abdominal ultrasound was performed in 12patients and CT scans of the abdomen in 10 patients.CT scanning showed the typical thick wall and smalllumen and also demonstrated obstructive uropathy inseven. Intravenous urography was performed preoperatively in 13 patients, demonstrating hydronephrosisin nine patients (bilateral in seven and unilateral intwo). (Fig. 1) These nine patients had raised serumurea and creatinine levels. We performed 99mTc DTPAisotope renography in seven of the nine patients withhydronephrosis and confirmed obstruction in eachcase. In one case an arteriogram had been performed11 years prior to operation when the patient was aged48 years and demonstrated a fusiform dilatation at thelower end of the abdominal aorta.
CT scanning and ultrasound enabled measurementof the size ofthe aneurysms which ranged from 4.5 emto 20 cm with an average of 9.3 ern.
TREATMENT
Thirty-six patients were treated surgically and onecoriservatively. The disease involved the distal thoracicaorta in three, extended above the renal arteries in six,with the infrarenal portion of the abdominal aorta in28 patients (75.6%). The iliac arteries were involved innine patients (24.3%).
Elective cases
There were 27 patients with 26 operativeprocedures.
Technique
In 22 patients aortic bifurcation grafts were insertedand attached either to the common iliac arteries, or ifthese were aneurysmal or involved in arterioscleroticdisease, the graft was extended to the common femoral arteries. Bilateral axillofemoral bypass was performed in three patients at the beginning of the series,a technique no longer employed. A straight graft wasused in one patient.
The patients with ureteric entrapment andobstructed kidneys were managed jointly by a vascularsurgeon and urologist. Cystoscopy was performed atthe beginning of the operation and an attempt made atpassing ureteric stents. Following insertion of the vascular graft, the urologist performed the ureterolysis,with omental wrapping and lateralization of the ureters. A ureteric stent was inserted through a ureterotomy if cystoscope insertion was unsuccessful. Of 12stents inserted, seven were through the cystoscope andfive through ureterotomy.
Two patients presented with a preoperative ureagreater than 20 mmol/l. Both had decompression ofthe renal tracts to improve renal function prior to surgery. In one patient this was achieved by ureteric stenting, in the other by nephrostomy drainage.
Emergency cases
Ten emergency operations were performed. Fourwere for ruptured aneurysms (10.8% of all the aneurysms in the series), one being suprarenal and threeinfrarenal. The rupture had occurred posteriorly in all.In the remaining six cases there was evidence of acutehemorrhage into the wall of the aneurysm at the timeof operation in two, in one the aneurysm was denselyadherent to the third part of the duodenum and hadformed an aortoduodenal fistula. That aneurysm wasdissected from the duodenum and the defect in theduodenal wall oversewn. Two patients had inferiorvena caval obstruction, one with an aortocaval fistula
354 INFLAMMATORY AAA~ ANNALS OFVASCULAR SURGERY
a b
Fig. 1. Anterograde pyelogram showing obstructive uropathy in (a) dilated renal pelvis and (b) ureter adherent to aneurysm.
at the aortic bifurcation, the other having an associated left iliac vein thrombosis.
The remaining patient presented with an acute history of abdominal and back pain and a tender aneurysm but no evidence of leakage was detected atoperation.
RESULTS
Among the twenty-six patients undergoing an elective procedure there were four deaths (15%). Onepatient developed asystole on clamping the aorta,another a coagulopathy in the immediate postoperative period. The third, with a thoracoabdominal aneurysm, developed a pneumothorax and chest infection,congestive cardiac failure and wound dehiscence complicated by a small bowel fistula. This patient died onthe twenty-eighth postoperative day. The fourthpatient also had a thoracoabdominal aneurysm. Postmortem examination demonstrated congestive cardiacfailure as the cause of death. The mortality at 30 dayswas 150/0.
All patients were followed up (range 2-108 months)and there were no recorded deaths. Six patients withobstructive uropathy survived operation and havebeen followed up by the urologist and vascular surgeon. Postoperative serum urea and creatinine levelshave returned to normal in all six. In five 99mTc DTPAisotope renography has been performed 'and has confirmed normal renal excretion in four of thesepatients. The remaining patient, who had a nonfunc-
tioning kidney on the right side preoperatively, hasimproved renal function on this side to a maximum of140/0 of total. All ureteric stents were removed by cystoscopy between three and eight months after surgery.There have been no complications following uretericsurgery (Table I).
In three patients bilateral axillofemoral bypassgrafts were inserted. All limbs had occluded by thesixth postoperative month. Two patients required further surgery following development of debilitatingclaudication and aortic bifurcation grafts wereinserted.
Seven of the 10 patients undergoing emergency procedures died (70%). Three died of myocardial infarction, three from renal failure, with the remainingpatient having a suprarenal rupture. The myocardialinfarctions occurred intraoperatively, during theimmediate postoperative period and three days postoperatively. The patients with renal failure were notconsidered suitable for dialysis in view of theiradvanced age. For summary see Table II.
DISCUSSION
Inflammatory aortic aneurysms comprised 4.74%of all aortic aneurysms in this series, a figure slightlylower than previously reported [1-4].
The etiology of the disease is poorly understood.Most authors have subscribed to the concept of aninflammatory response to the transudation of blood
VOLUME 2No 4 - 1988
INFLAMMATORY AAA:S 355
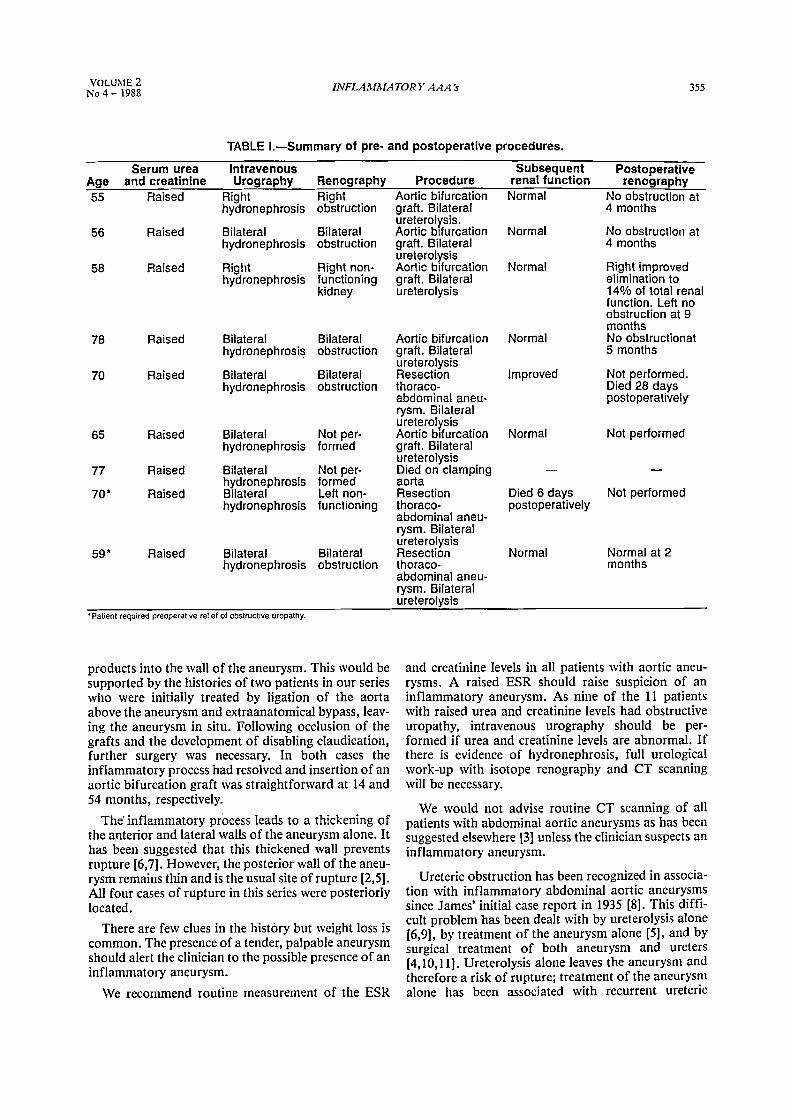
TABLE I.-Summary of pre- and postoperative procedures.
Serum urea Intravenous Subsequent PostoperativeAge and creatinine Urography Renography Procedure renal function renography55 Raised Right Right Aortic bifurcation Normal No obstruction at
hydronephrosis obstruction graft. Bilateral 4 months
Raised Bilateral Bilateralureterolysis.
Normal No obstruction at56 Aortic bifurcationhydronephrosis obstruction graft. Bilateral 4 months
ureterolysis58 Raised Right Right non- Aortic bifurcation Normal Right improved
hydronephrosis functioning graft. Bilateral elimination tokidney ureterolysis 14% of total renal
function. Left noobstruction at 9months
78 Raised Bilateral Bilateral Aortic bifurcation Normal No obstructionathydronephrosls obstruction graft. Bilateral 5 months
ureterolysis70 Raised Bilateral Bilateral Resection Improved Not performed.
hydronephrosis obstruction thoraco- Died 28 daysabdominal aneu- postoperativelyrysm. Bilateralureterolysis
65 Raised Bilateral Not per- Aortic bifurcation Normal Not performedhydronephrosis formed graft. Bilateral
ureterolysis77 Raised Bilateral Not per- Died on clamping
hydronephrosis formed aorta70· Raised Bilateral Left non- Resection Died 6 days Not performed
hydronephrosis functioning thoraco- postoperativelyabdominal aneu-rysm. Bilateralureterolysis
59* Raised Bilateral Bilateral Resection Normal Normal at 2hydronephrosis obstruction thoraco- months
abdominal aneu-rysm. Bilateralureterolysis
•Patient required preoperative relief of obstructive uropathy.
products into the wall of the aneurysm. This would besupported by the histories of two patients in our serieswho were initially treated by ligation of the aortaabove the aneurysm and extraanatomical bypass, leaving the aneurysm in situ. Following occlusion of thegrafts and the development of disabling claudication,further surgery was necessary. In both cases theinflammatory process had resolved and insertion of anaortic bifurcation graft was straightforward at 14 and54 months, respectively.
The' inflammatory process leads to a thickening ofthe anterior and lateral walls of the aneurysm alone. Ithas been suggested that this thickened wall preventsrupture [6,7]. However, the posterior wall of the aneurysm remains thin and is the usual site of rupture [2,5].All four cases of rupture in this series were posteriorlylocated.
There are few clues in the history but weight loss iscommon. The presence of a tender, palpable aneurysmshould alert the clinician to the possible presence of aninflammatory aneurysm.
We recommend routine measurement of the ESR
and creatinine levels in all patients with aortic aneurysms. A raised ESR should raise suspicion of aninflammatory aneurysm. As nine of the 11 patientswith raised urea and creatinine levels had obstructiveuropathy, intravenous urography should be performed if urea and creatinine levels are abnormal. Ifthere is evidence of hydronephrosis, full urologicalwork-up with isotope renography and CT scanningwill be necessary.
We would not advise routine CT scanning of allpatients with abdominal aortic aneurysms as has beensuggested elsewhere [3] unless the clinician suspects aninflammatory aneurysm.
Ureteric obstruction has been recognized in association with inflammatory abdominal aortic aneurysmssince James' initial case report in 1935 [8]. This difficult problem has been dealt with by ureterolysis alone[6,9], by treatment of the aneurysm alone [5], and bysurgical treatment of both aneurysm and ureters[4,10,11]. Ureterolysis alone leaves the aneurysm andtherefore a risk of rupture; treatment of the aneurysmalone has been associated with recurrent ureteric
356 INFLAMMATORY AAA:S ANNALS OFVASCULAR SURGERY
Elective
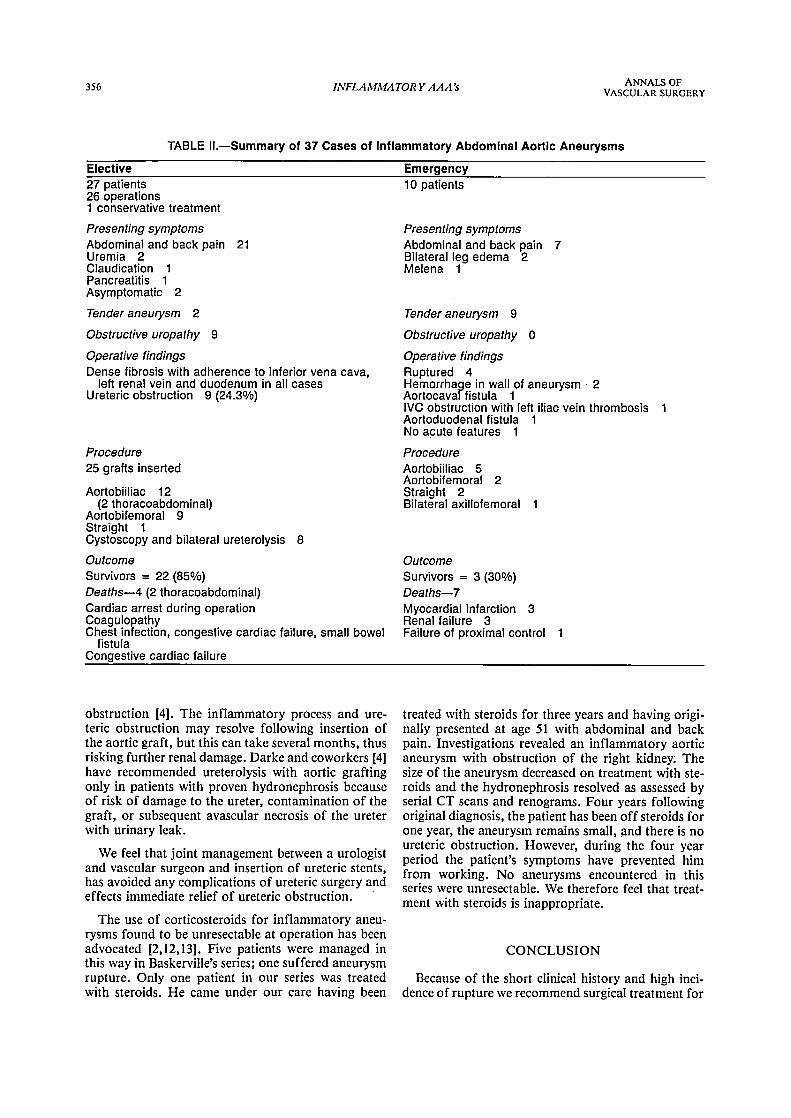
TABLE H.-Summary of 37 Cases of Inflammatory Abdominal Aortic Aneurysms
Emergency27 patients26 operations1 conservative treatment
Presenting symptomsAbdominal and back pain 21Uremia 2Claudication 1Pancreatitis 1Asymptomatic 2
Tender aneurysm 2
Obstructive uropathy 9
Operative findingsDense fibrosis with adherence to inferior vena cava,
left renal vein and duodenum in all casesUreteric obstruction 9 (24.3%)
Procedure25 grafts inserted
Aortobiiliac 12(2 thoracoabdominal)
Aortobifemoral 9Straight 1Cystoscopy and bilateral ureterolysis 8
OutcomeSurvivors = 22 (85%)Deaths-4 (2 thoracoabdominal)Cardiac arrest during operationCoagulopathyChest infection, congestive cardiac failure, small bowel
fistulaCongestive cardiac failure
obstruction [4]. The inflammatory process and ureteric obstruction may resolve following insertion ofthe aortic graft, but this can take several months, thusrisking further renal damage. Darke and coworkers [4]have recommended ureterolysis with aortic graftingonly in patients with proven hydronephrosis becauseof risk of damage to the ureter, contamination of thegraft, or subsequent avascular necrosis of the ureterwith urinary leak.
We feel that joint management between a urologistand vascular surgeon and insertion of ureteric stents,has avoided any complications of ureteric surgery andeffects immediate relief of ureteric obstruction. .
The use of corticosteroids for inflammatory aneurysms found to be unresectable at operation has beenadvocated [2,12,13]. Five patients were managed inthis way in Baskerville's series; one suffered aneurysmrupture. Only one patient in our series was treatedwith steroids. He came under our care having been
10 patients
Presenting symptomsAbdominal and back pain 7Bilateral leg edema 2Melena 1
Tender aneurysm 9
Obstructive uropathy 0
Operative findingsRuptured 4Hemorrhage in wall of aneurysm 2Aortocavar fistula 1IVC obstruction with left iliac vein thrombosis 1Aortoduodenal fistula 1No acute features 1
ProcedureAortobiiliac 5Aortobifemoral 2Straight 2Bilateral axillofemoral
OutcomeSurvivors = 3 (30%)Deaths-7Myocardial infarction 3Renal failure 3Failure of proximal control 1
treated with steroids for three years and having originally presented at age 51 with abdominal and backpain. Investigations revealed an inflammatory aorticaneurysm with obstruction of the right kidney: Thesize of the aneurysm decreased on treatment with steroids and the hydronephrosis resolved as assessed byserial CT scans and renograms. Four years followingoriginal diagnosis, the patient has been off steroids forone year, the aneurysm remains small, and there is noureteric obstruction. However, during the four yearperiod the patient's symptoms have prevented himfrom working. No aneurysms encountered in thisseries were unresectable. We therefore feel that treatment with steroids is inappropriate.
CONCLUSION
Because of the short clinical history and high incidence of rupture we recommend surgical treatment for
VOLUME 2No4 - 1988 INFLAMMATORYAAAs 357
these aneurysms. When an inflammatory aneurysm isassociated with ureteric obstruction a combined bifurcation graft and ureterolysis gives excellent results.
REFERENCES
I. WALKER D, BLOOR K, WILLIAMS G, GILLIE I. Inflammatory aneurysms of the abdominal aorta. Br J Surg 1972;59:609-614.
2. GOLDSTONE J, MALONE JM, MOORE WS. Inflammatoryaneurysms of the abdominal aorta. Surgery 1978; 83:425-430.
3. BASKERVILLE PA, BLAKENEY CG, TOUNG AE,BROWNE NL. The diagnosis and treatment of periaortic fibrosis ('inflammatory aneurysms'). Br J Surg 1983; 70:381-385.
4. DARKE SG, GLASS RE, EADIE DA. Abdominal aortic aneurysm, perianeurysmal fibrosis and ureteric obstruction and deviation. Br J Surg 1977; 64:649-652.
5. BARR H, CAVE·BIGLEY OJ, HARRIS PL. The managementof inflammatory abdominal aortic aneurysms. J Royal CoilSurg Edin 1985;30:217-220.
6. CRAWFORD JL, STOWE CL, SAFI HJ, HALLMAN CH,
CRAWFORD E,S.·Inflammatory aneurysms of the aorta. JVasc Surg 1985; 2:113-124.
7. ABBOTT DL, SKINNER DG, YALOWITZ PA, MULDERDO. Retroperitoneal fibrosis associated with abdominal aorticaneurysms: an approach to management. J Urol 1973;109:987-989.
8. ALMGREW B, ERIKSSON R, FORSBERG 10, NORDLIN·DER H. Abdominal aortic aneurysm with perianeurysmalfibrosis. Acta Chir Scand 1981; 147:539-543.
9. JAMES TGI. Uremia due to aneurysm of the abdominal aorta.Br J Uro11935; 7:157.
10. ABERCROMBIE EF, HENDRY DF. Ureteric obstruction dueto perianeurysmal fibrosis. Br J Uro11971; 43:170-173.
II. SCHUMACKER HB, GARRETT R. Obstructive uropathyfrom abdominal aortic aneurysm. Surg Gynecol Obstet 1955;100:758-761.
12. HENRY LG, DOUST B, KERNS ME, BERNHARD VM.Abdominal aortic aneurysm and retroperitoneal fibrosis. ArchSurg 1978; 113:1456-1460.
13. CLYNE CA, ABERCROMBIE ER. Perianeurysmal retroperitoneal fibrosis; two cases responding to steroids. Br J Urol1977; 49:463-467.
14. HEDGES AR, BENTLEY PG. Resection of inflammatoryaneurysm after steroid therapy. Br J Surg 1986; 73:374.
•••