Embed Size (px)
Citation preview

Infertility 101
Dana Ambler, DO
Director, Donor Egg Program
Associate Physician
Conceptions Reproductive Associates

Myths Facts
You’ll get pregnant if. . .
you just relax
you go on vacation
you stop thinking about it
you stand on your head after intercourse
Stress– Little effect if regular
menses & ovulate– Moderate stress has
some effect on fertility– Severe stress-
problems with ovulation and fertility
Intercourse– Having it will help you
conceive

Myths Facts
Most people who get pregnant at fertility clinics, have “mutiples” (twins, triplets and more)
~ 80% patients who conceive have a singleton pregnancy
10 - 20% will have twins
<1% of all patients have triplets

Myths Facts
Most people need to have multiple tests done to first diagnose the problem even before starting treatment
Most couples need very few tests to determine the cause of the infertility– Semen analysis– Test for ovulation
(Blood tests)– Test to check fallopian
tubes

Myths Facts
Insurance never covers the cost of infertility treatment
Up to 30% of insurances cover some of the costs
15 states already have laws mandating fertility coverage
It is critical to write your legislator if you think this is important

Myths Facts
Miscarriages are caused by – Stress– Picking up something
heavy– Having intercourse
Miscarriages are usually the result of an abnormal egg and/or sperm resulting in an embryo with abnormal DNA
This cannot be prevented once the embryo has formed

Myths Facts
Egg quality decreases at the age of 32
Up to 10% chance of pregnancy per month if 35 and older
Approximately 20% chance that pregnancy will result in miscarriage
Infertility
Twelve consecutive months of unprotected intercourse without conception– >35 years old → six months– >40 years old → immediate evaluation
Worldwide, 1 in 7 couples have problems conceiving
85-90% conceive in one year
Primary Infertility and Secondary Infertility

Female30%
Male30%
Unexplained10%
Combination20%
Infertility Causes

Typical EvaluationHistory and Physical Exam (Female)– Duration of infertility? Previous treatment?– Regular menstrual cycles? Abnormal
bleeding?– Severe pain with menses or intercourse?– Sexual history? Timing? Contraception?
Lubricants?– Previous surgeries, hospitalizations,
infections?– Medical conditions?– Occupation? Tobacco, alcohol, drug use?

Typical Evaluation
Tests for Ovarian Reserve– Follicle Stimulating Hormone– Luteinizing Hormone– Estradiol– Anti-Mullerian Hormone– Ultrasound
Typical Evaluation (Female)
Tests for Ovulation (if uncertain)– 21 day progesterone– Ovulation predictor kit– Thyroid, Prolactin, vit D– Polycystic Ovarian
Syndrome
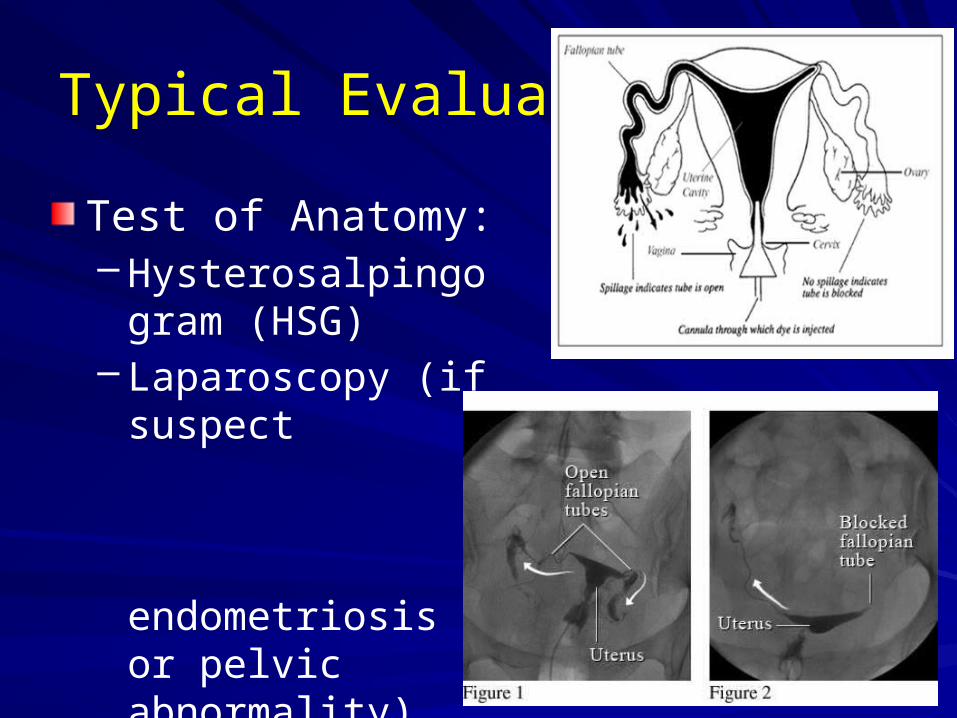
Typical Evaluation
Test of Anatomy:– Hysterosalpingogram
(HSG)– Laparoscopy (if
suspect endometriosis or pelvic abnormality)

Typical Evaluation
History and Physical Exam (Male)– Sexual history? Timing? Contraception?
Lubricants?– Prior genital injury? Surgery?– Infections?– Drug/Medication Use?– History of fathering children?– Medical conditions?– Occupation? Tobacco, alcohol, drug use?

Typical Evaluation (Male)
Tests for husband– Semen Analysis (SA)– Physical exam if SA is abnormal
Varicocele?
Normal testicular development?
Laboratory evaluation

Infertility Statistics
Age of female

Infertility TreatmentsSurgery
Superovulation or Ovulation Induction
Intra-uterine Insemination (IUI)
In vitro Fertilization– Intracytoplasmic Sperm
Injection (ICSI)– Complete
Chromosomal Screening (CCS)

Treatment of Infertility
Ovulation defect – Fertility medications– Other options
Metformin (PCOS)
Bromocriptine
Dexamethasone
Aspirin
Progesterone
DEPENDS ON AGE OF FEMALE
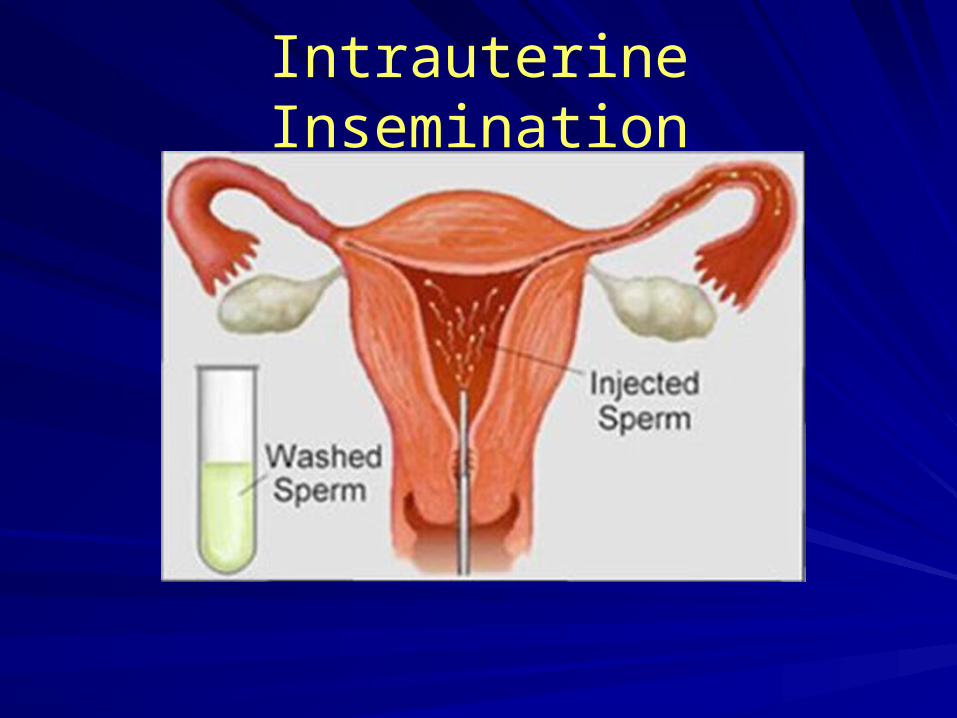
Intrauterine Insemination

In Vitro FertilizationFallopian Tube diseaseEndometriosisMale Factor InfertilityMultifactor or Unexplained InfertilityAdvanced Reproductive AgePremature Ovarian FailureMullerian anomaliesMedical DiseaseGenetic DisordersPrevious treatment failures

Treatment of InfertilityMale Factor– Referral to Urology– Antibiotics– Very little success with any treatment except
IUI and IVF (medications seldom helpful)– High dose antioxidants and multivitamins– Surgery– Boxers not briefs – No hot tubs – No smoking/drugs

Treatment of Infertility
“If every test is normal, why can’t we get pregnant?”
Unexplained Infertility– Wait and see– Clomiphene + IUI (Inseminations)– Gonadotropins + IUI– In Vitro Fertilization (IVF)





























