Embed Size (px)
Citation preview

1
Infective Meningitis Caused by Phialemonium curvatum: a Case Report 1
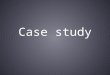
Yueli Zou 1†, Yuhai Bi 2†*, Hui Bu 1, Yunying He 1, Li Guo1, Dongyan Shi 1* 2
3
1. The Second Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050000, China 4
2. CAS Key Laboratory of Pathogenic Microbiology and Immunology (CASPMI), Institute of Microbiology, Chinese Academy 5
of Sciences, Beijing 100101, China. 6
7
8
9
10
Running title: Phialemonium curvatum meningitis 11
12
* Corresponding author: 13
Dongyan Shi, [email protected]; Tel. (+86) 311 66002710; Fax. (+86) 311 66002851. Mailing address: Department of 14
Clinical Lab, The Second Hospital of Hebei Medical University, Shijiazhuang, 050000, Hebei, China. 15
Yuhai Bi, [email protected]; Tel. (+86) 10 64806013; Fax (+86) 10 64806247. Mailing address: CAS Key Laboratory of 16
Pathogenic Microbiology and Immunology (CASPMI), Institute of Microbiology, Chinese Academy of Sciences, Beichenxi 17
Road, Chaoyang District, Beijing 100101, China. 18
19
† These authors contributed equally to this work. 20
21
JCM Accepts, published online ahead of print on 21 May 2014J. Clin. Microbiol. doi:10.1128/JCM.00419-14Copyright © 2014, American Society for Microbiology. All Rights Reserved.
on June 4, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

2
Infections caused by rarely encountered fungal pathogens have increased in recent decades. 22
Phialemonium species are widely distributed in the environment and are also involved in human 23
infections, affecting both immunocompromised and immunocompetent patients. The present 24
study describes a case of meningitis caused by Phialemonium curvatum. 25
CASE REPORT 26
A 42-year-old male patient was admitted to the hospital for continuous headache without 27
nausea and fever, with a maximum temperature of 39°C during the past 30 days. He was a 28
poultry farmer and had experienced head trauma at the age of 19. The patient was conscious and 29
claimed acroanesthesia. He denied any systemic disease, history of immunosuppression, or 30
recent travel. When the patient was first admitted to the hospital, his physical examination 31
showed that he had stable vitals, the neurological assessments were unremarkable, and no neck 32
stiffness was noted. A routine blood test revealed a white blood cell (WBC) count of 11.6×109/l 33
(53.7% neutrophils and 36.3% lymphocytes). The first lumbar puncture was performed under 34
local anesthesia, revealing 110×106/l WBCs, 0.3 g/l protein, 3.1 mmol/l glucose, and 117 mmol/l 35
chloride. The pressure of the cerebrospinal fluid (CSF) was 250 mmH2O. CSF cytology 36
demonstrated the presence of approximately 70% lymphocytes and 30% neutrophilic 37
granulocytes. A computed tomography scan of the head and a chest radiograph showed no 38
alterations. Cranial magnetic resonance imaging was normal. An echocardiogram revealed that 39
the left ventricle had a normal size and function, and no vegetation was detected. In addition, a 40
serum test for human immunodeficiency virus (HIV) was negative. Aricine staining and India 41
ink staining of the CSF were also negative. He was initially diagnosed with viral encephalitis 42
on June 4, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

3
and tuberculous meningitis and received antiviral therapy (Ganciclovir, 0.25 g twice a day) for 43
10 days, as well as a standard 15-day course of anti-tuberculosis therapy (isoniazid, 0.9 g/24 h, 44
rifampin, 0.6 g q.d., and pyrazinamide, 0.25 g t.i.d.). However, the treatment had little effect, 45
and the patient still complained of a heavy headache. Measurements of CSF and blood 46
(1-3)–β-D-glucan were 151 pg/ml and 466 pg/ml, respectively (with a cut-off value <100 pg/ml). 47
The later culture test showed that the four blood cultures were negative. Two of the CSF cultures 48
became positive after 4 days of incubation in blood culture bottles (BacT/ALERT, aerobic bottle; 49
BioMerieux) without antibiotics. Subculturing of the positive CSF cultures revealed mold 50
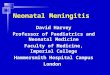
growth after 72 h of incubation. On traditional Sabouraud agar, the colonies were white, 51
reaching 10-15 mm in diameter after 10 days at 25°C. Colonies were cream colored, and small 52
areas of the colonies became light yellow after 30 days (Fig. 1). Microscopically, vegetative 53
hyphae and conidia were hyaline. Accumulation of hyaline conidia was observed at the apex, 54
and most of them were allantoid (Fig. 2). Scanning electron microscopy (SEM) images revealed 55
that the shape of the conidia was either allantoid or obovate (Fig. 3). DNA was extracted using a 56
TIANamp Yeast DNA kit (Tiangen, Beijing, China) 10 days after fungal growth was detected in 57
the CSF cultures. Five microliters of the extracted DNA was used to amplify the 28 S rRNA and 58
internal transcribed spacer (ITS) genes using the primers P1 (forward, 59
5′-GATAGCGAACAAGTAGAGTGA-3′) and P2 (reverse, 60
5′-GTCCGTGTTTCAAGACGGGC-3′) and primers ITS1 (forward, 61
5’-TCCGTAGGTGAACCTGCGG-3’) and ITS4 (reverse, 62
5’-TCCTCCGCTTATTGATATGC-3’), respectively. PCR was performed with a Bio-Rad 63
on June 4, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

4
MyCycler thermal cycler (Bio-Rad, Hercules, CA) as follows: 30 cycles of 30 s at 95°C, 45 s at 64
55°C, and 45 s at 72°C, followed by a final extension of 10 min at 72°C (1). The sizes of the 65
PCR products were estimated using a standard DNA ladder and sequenced with an automated 66
ABI Prism 377 DNA Sequencer (Applied Biosystems Corp, Foster City, CA). Then, the 67
sequences were analyzed by nucleotide-nucleotide basic local alignment search tool (BLAST) 68
searches and DNAMAN 5.2 (Lynnon Biosoft, Pointe-Claire, Quebec). We found that the two 69
amplified DNA fragments were 514 and 252 bp (GenBank accession numbers KF318613 and 70
KF318614, respectively), which matched the P. curvatum sequences (GenBank AB568605) with 71
high (99%) similarity. Ultimately, the patient was diagnosed with P. curvatum meningitis. In 72
vitro antifungal susceptibility was determined by the broth dilution method. The MICs of the 73
strain against fluconazole (FLC), itraconazole (ITC), voriconazole (VRC), amphotericin B 74
(AMB), and caspofungin were 32, 1, 0.5, 2, and ≥16 μg/ml, respectively. 75
The patient was treated with intravenous VRC (0.40 g/12 h on day 1, and 0.20 g/12 h 76
thereafter) for 2 weeks and subsequently made good progress toward recovery. Indeed, the 77
symptoms of headache and fever decreased during the course of VRC treatment. However, the 78
patient refused to continue this treatment due to his economic conditions. Thus, we treated him 79
with FLC (0.40 g/24 h on day 1, and 0.20 g/24 h thereafter) and AMB (0.02 mg/kg/day 80
increased to 0.6 mg/kg/d) for approximately 2 months. Examination of CSF revealed 10×106/l 81
WBCs (77% lymphocytes, 8% monocytes, and 15% neutrophils), 0.58 g/l protein, 4.00 mmol/l 82
glucose, and 112 mmol/l chloride after 2 months of treatment. The CSF pressure was 150 83
mmH2O. Cultures of blood and CSF were both negative. The levels of CSF and blood 84
on June 4, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

5
(1-3)-β-D-glucan were 15 and <5 pg/ml, respectively. The patient continued medication (0.20 85
g/d FLC) after discharge. After 1 year of follow-up, the patient could work but still complained 86
of acroanesthesia. 87
—————————— 88
Phaeohyphomycosis is an infection caused by a large number of dematiaceous fungi, which 89
affect cutaneous and subcutaneous tissues, the ocular region, the frontal and maxillary sinuses, 90
lungs, bones, and the heart (i.e., endocarditis). The majority of Phialemonium infections are 91
invasive, and the most frequent infections include peritonitis endocarditis, osteomyelitis, and 92
cutaneous infections of wounds that may occur after a burn (2-6). In this case, the only 93
theoretical factor that might raise doubts about the patient’s complete immunological integrity 94
was his occupation bringing him in frequent contact with chickens and the head trauma at the 95
age of 19. In reported Phialemonium infection cases, the filamentous fungus is mainly isolated 96
from blood samples obtained from patients with primary fungemia (3-5). In the current case, the 97
diagnosis of meningitis caused by P. curvatum was confirmed by CSF culturing, but the blood 98
cultures were negative. 99
Initially, clinicians misdiagnosed him with common encephalitis because he presented 100
nonspecific signs and symptoms and denied any prior steroid use. Phialemonium is often 101
mistaken as a yeast on Gram stains of blood and CSF specimens, and similar phenomena have 102
been observed in cases of infection caused by Fusarium and Acremonium (4, 9). In recent years, 103
molecular diagnostic tools such as PCR have been used to analyze fungal pathogens, especially 104
Aspergillus and Candida species (10). In clinical samples, these sensitive and specific methods 105
on June 4, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

6
utilize primer pairs that are complementary to the highly conserved 18 S, 5.8 S, and 28 S regions 106
of the fungal rRNA genes and ITS regions, which enable differentiation of many fungal species. 107
Using specific primer pairs for quick molecular detection of Phialemonium is expected to be the 108
most therapeutically effective. The measurement of plasma (1-3)–β-D-glucan can also provide 109
early and reliable information on deep fungal infections. In this case, plasma (1-3)–β-D-glucan 110
measurement was sensitive for the diagnosis of fungemia. 111
In the current case, the antifungal susceptibility results for the case isolate were similar to 112
those previously reported in the literature (1, 5, 8), i.e., the strain was sensitive to VRC. Due to 113
his economic condition, we initially treated him with VRC but then used FLC and AMB for 114
longer-term therapy. His headache and fever improved, however the patient still complained of 115
acroanesthesia after 1 year of follow-up. We attribute his recovery to the use of antifungal drugs 116
and the improvement of his living standard. Nevertheless, we do not know whether the use of 117
FLC and AMB was effective in the present case. 118
To our knowledge, this is the first case of meningitis infection due to P. curvatum reported in 119
China. Phialemonium infections may be misdiagnosed initially because of the nonspecific 120
clinical manifestations and lack of accurate identification. Our study demonstrates that 121
molecular biological techniques and morphological observation contribute to the proper 122
diagnosis of rare pathogens. In addition, we also alert clinicians about the rarity of the case and 123
the increasing occurrence of emerging fungi in immunocompromised patients. 124
Acknowledgments: This work was supported by Jin Yu in Peking University First 125
Hospital. 126
on June 4, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

7
No Conflict of Interest 127
REFERENCES 128
1. Perdomo H, Sutton DA, García D, Fothergill AW, Gené J, Cano J, Summerbell RC, 129
Rinaldi MG, Guarro J. 2011. Molecular and Phenotypic Characterization of Phialemonium 130
and Lecythophora Isolates from Clinical Samples. J. Clin. Microbiol. 49:1209-1216. 131
2. Guarro J, Nucci M, Akiti T, Gené J, Cano J, Barreiro MD, Aguilar C. 1999. 132
Phialemonium fungemia: two documented nosocomial cases. J. Clin. Microbiol. 133
37:2493–2497. 134
3. Heins-Vaccari EM, Machado CM, Saboya RS, Silva RL, Dulley FL, Lacaz CS, Freitas 135
Leite RS, Hernandez Arriagada GL. 2001. Phialemonium curvatum infection after bone 136
marrow transplantation. Rev. Inst. Med. Trop. Sao. Paulo.43:163-166. 137
4. Gavin PJ, Sutton DA, Katz BZ. 2002. Fatal endocarditis in a neonate caused by the 138
dematiaceous fungus Phialemonium obovatum: case report and review of the literature. J. Clin. 139
Microbiol. 40:2207–2212. 140
5. Proia LA, Hayden MK, Kammeyer PL, Ortiz J, Sutton DA, Clark T, Schroers 141
HJ, Summerbell RC. 2004. Phialemonium: an emerging mold pathogen that caused 4 cases 142
of hemodialysis-associated endovascular infection. Clin. Infect. Dis. 39:373–379. 143
6. Strahilevitz J, Rahav G, Schroers HJ, Summerbell RC, Amitai Z, Goldschmied-Reouven 144
A, Rubinstein E, Schwammenthal Y, Feinberg MS, Siegman-Igra Y,Bash E, Polacheck 145
I, Zelazny A, Howard SJ, Cibotaro P, Shovman O, Keller N. 2005. An outbreak of 146
Phialemonium infective endocarditis linked to intracavernous penile injections for the 147
on June 4, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

8
treatment of impotence. Clin. Infect. Dis. 40:781–786. 148
7. Rivero M, Hidalgo A, Alastruey-Izquierdo A, Cía M, Torroba L, Rodríguez-Tudela JL. 149
2009. Infections due to Phialemonium species: case report and review. Med. Mycol. 150
47:766-774. 151
8. Sutton DA, Wickes BL, Thompson EH, Rinaldi MG, Roland RM, Libal MC, Russell 152
K, Gordon S. 2008. Pulmonary Phialemonium curvatum phaeohyphomycosis in a Standard 153
Poodle dog. Medical Mycology. 46:355-359. 154
9. King D, Pasarell L, Dixon DM, McGinnis MR, and Merz WG. 1993. A 155
phaeohyphomycotic cyst and peritonitis caused by Phialemonium species and a reevaluation 156
of its taxonomy. J. Clin. Microbiol. 31:1804–1810. 157
10. Schabereiter-Gurtner C, Selitsch B, Rotter ML, Hirschl AM, Willinger B. 2007. 158
Development of novel real-time PCR assays for detection and differentiation of eleven 159
medically important Aspergillus and Candida species in clinical specimens. J. Clin. 160
Microbiol. 45:906-914. 161
Legends 162
Fig.1 Culture on Sabouraud agar showed light yellow after 30 days 163
Fig.2 Microscopically, vegetabative hyphae were hyaline, conidia were hyaline (×1000) 164
Fig.3 The shape of the conidia was either allantoid or obovate (×6000) 165
on June 4, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from