Embed Size (px)
Citation preview

GHENT UNIVERSITY FACULTY OF VETERINARY MEDICINE
ACADEMIC YEAR 2015-2016
Case report: Infective endocarditis in a dog by
Janine Nathalie DE KONING Promotors: Dr. Pascale Smets Case report as part of the Dr. Valérie Bavegems Master’s Dissertation

ii

iii
Disclaimer Universiteit Gent, its employees and/or students, give no warranty that the information provided in this thesis is accurate or exhaustive, nor that the content of this thesis will not constitute or result in any infringement of third-party rights. Universiteit Gent, its employees and/or students do not accept any liability or responsibility for any use which may be made of the content or information given in the thesis, nor for any reliance which may be placed on any advice or information provided in this thesis.

© 2016 Janine Nathalie de Koning
GHENT UNIVERSITY FACULTY OF VETERINARY MEDICINE
ACADEMIC YEAR 2015-2016
Case report: Infective endocarditis in a dog by
Janine Nathalie DE KONING Promotors: Dr. Pascale Smets Case report as part of the Dr. Valérie Bavegems Master's Dissertation

ii
Voorwoord Allereerst wil ik graag mijn dank betuigen aan mijn promotor Dr. Pascale Smets voor al haar hulp en inzet om deze masterproef tot een mooi eind te brengen. Daarnaast wil ik ook mijn copromotor Valérie Bavegems bedanken. Ook wil ik Dr. Hilde De Cock bedanken voor het opsturen van de pathologische beelden, mevrouw Steffelaar DVM voor het opsturen van de bloedonderzoeken en Emelie Stock DVM voor het opsturen van alle RX en echo beelden. Heel veel dank wil ik betuigen aan Dr. David Davis voor het kritische nakijken van mijn masterproef en het geven van extra tips. Daarnaast wil ik mijn ouders, Peter en Thea de Koning, bedanken voor het nakijken van mijn masterproef en het geven van zowel emotionele als financiële support. Ten laatste wil ik mijn lief Jeremy de Kok en al mijn vrienden bedanken voor de emotionele support. Dankzij jullie stond ik er niet alleen voor in deze opleiding en was het een periode om met een goed gevoel naar terug te kijken.
i
Table of contents Abstract ................................................................................................................................................... 1 Samenvatting .......................................................................................................................................... 1 1. Introduction .......................................................................................................................................... 3 2. Literature ............................................................................................................................................. 4
2.1. Predisposition ............................................................................................................................... 4 2.2. Aetiology ....................................................................................................................................... 4 2.3. General physical examination ...................................................................................................... 4 2.4. Specific cardiac examination ........................................................................................................ 4 2.5. Specific examinations ................................................................................................................... 5
2.5.1. Echocardiography and electrocardiography .......................................................................... 5 2.5.2. Radiology .............................................................................................................................. 7 2.5.3. Ultrasound ............................................................................................................................. 7 2.5.4. Blood culture ......................................................................................................................... 7 2.5.5. Blood analysis ....................................................................................................................... 8 2.5.6. Urine analysis and culture ..................................................................................................... 8 2.5.7. Arthrocenthesis ..................................................................................................................... 9 2.5.8. Cerebrospinal fluid ................................................................................................................ 9 2.5.9. Histopathologic examination ................................................................................................. 9 2.5.10. Necropsy ............................................................................................................................. 9
2.6. Differential diagnoses ................................................................................................................. 10 2.7. Treatment ................................................................................................................................... 10 2.8. Prognosis ................................................................................................................................... 11 2.9. Follow-up .................................................................................................................................... 11 2.10. Complications ........................................................................................................................... 12
3. Clinical case ...................................................................................................................................... 13 3.1. Signalment ................................................................................................................................. 13 3.2. Anamnesis .................................................................................................................................. 13 3.3. General physical examination .................................................................................................... 13 3.4. Specific cardiorespiratory examination ....................................................................................... 13 3.5. Problem list ................................................................................................................................. 13 3.6. Differential Diagnoses ................................................................................................................ 14 3.7 Diagnostic plan ............................................................................................................................ 15 3.8. Results ....................................................................................................................................... 15
3.8.1. Blood analysis ..................................................................................................................... 15 3.8.2. Blood culture ....................................................................................................................... 15 3.8.3. Echocardiography ............................................................................................................... 15 3.8.4. Radiology ............................................................................................................................ 17 3.8.5. Ultrasound ........................................................................................................................... 17 3.8.6. Fine needle aspirate ............................................................................................................ 19 3.8.7. Urine analysis ...................................................................................................................... 19
3.9. Diagnosis .................................................................................................................................... 19 3.10. Treatment ................................................................................................................................. 20 3.11. Hospitalisation .......................................................................................................................... 20 3.12. Blood analyses ......................................................................................................................... 21 3.13. Complications and abnormalities ............................................................................................. 22
3.13.4. Ovarian stumps culture ..................................................................................................... 24 3.13.5. Histopathologic examination after surgery ........................................................................ 24
3.14. New diagnosis .......................................................................................................................... 25 3.15. New treatment .......................................................................................................................... 25 3.16. Follow-up .................................................................................................................................. 25 3.12. Prognosis ................................................................................................................................. 26
4. Discussion ......................................................................................................................................... 26 References ............................................................................................................................................ 28
1
Abstract A flat coated retriever bitch, aged five years and ten months, showed clinical signs of fever, systolic murmur at the level of the mitral valve, tachypnoea, tachycardia, lethargy, vomiting, and diarrhoea. These symptoms arose three days after an ovariectomy. A severely thickened septal leaflet of the mitral valve with moderate regurgitation was observed using 2D echocardiography and colour Doppler respectively, and confirmed the diagnosis of infectious endocarditis. Blood analysis showed an inflammation and blood culture was positive for Enterobacteriaceae species. These pathogens were also cultured from the ovarian stumps, indicating that the ovariectomy may have been the route of infection. Inflammation of the left cranial uterus horn as well as a possible hematoma or abscess at the left ovarian stump were visible on ultrasound of the abdomen. Histopathologic examination confirmed this inflammation of the genital system. The complication of arterial thromboembolism occurred two days after being presented at the clinic. This thrombus was localised in the mesenterica cranialis resulting in local necrosis of the small intestines. This suspicion was raised by a smaller visible vegetation on echocardiography, intestinal necrosis and steatitis on abdominal ultrasound. These results lead to an explorative celiotomy with enterectomy and hysterectomy. Presumably, the bacteria entered the bloodstream during ovariectomy, causing septicaemia, and leading to colonization of the septal leaflet of the mitral valve. The patient was treated with enrofloxacin intra-venously for one week, then subcutaneously for another week, and orally for another five weeks.
Samenvatting Infectieuze endocarditis is een pathologische aandoening van de hartkleppen die voornamelijk voorkomt bij (middel)grote hondenrassen met een jaarlijkse incidentie van 0,03-0,1%. In deze casus wordt de aandoening beschreven bij een flatcoated retriever teef van vijf jaar en tien maanden oud, die klinische symptomen van koorts, een systolisch hartruis ter hoogte van de mitralisklep (met een graad 2/6), lethargie, braken en diarree vertoonde. Deze symptomen traden op drie dagen nadat een ovariëctomie was uitgevoerd. De etiologie van deze aandoening is het optreden van een tijdelijke of persisterende bacteriëmie. Bij deze patiënt traden de bacteriën vermoedelijk het lichaam binnen via de bloedstroom tijdens de uitvoering van voornoemde ovariëctomie, hetgeen resulteerde in een septicemie en uiteindelijk leidde tot een kolonisatie ter hoogte van het septale blad van de mitralis klep. De diagnose van een infectieuze endocarditis werd bevestigd aan de hand van echocardiografische beelden en een bloed- en weefselcultuur. Deze onderzoeken helpen om de endocarditis te differentiëren van een mitralisklependocardiose. Deze laatste aandoening komt echter voornamelijk voor bij kleine hondenrassen waarbij de vegetaties voornamelijk continu met de klep bewegen in plaats van oscillerend. Een sterk verdikt septaal blad van de mitralis klep in combinatie met een matige regurgitatie werd geconstateerd bij deze patiënt aan de hand van respectievelijk een 2D echocardiografie en een
2
kleuren Doppler, en aldus werd aan twee voornaamste criteria voor de diagnose van endocarditis voldaan. Bij bloedonderzoek waren niet-specifieke veranderingen zichtbaar zoals een non-regeneratieve anemie, leucocytose, monocytose, neutrofilie en een thrombocytopenie. Uit deze bloedstaal kon eveneens de weinig voorkomende Enterobacteriaceae bacterie worden gecultiveerd. De bacterie werd overigens ook gecultiveerd vanuit de ovariumstompen, wat erop duidde dat de ovariëctomie zeer waarschijnlijk de route van infectie was. Bloedcultuur is niet alleen belangrijk voor de diagnose maar ook om de meest effectieve antibiotica behandeling te bepalen. Daarnaast zijn radiografische beelden belangrijk om andere thoracale aandoeningen op te sporen en zowel linker congestief hartfalen als de hartgrootte te evalueren. Geen afwijkingen waren zichtbaar op radiografie van de thorax van deze patiënt. Echografie van het abdomen is een onderzoek dat wordt uitgevoerd om de etiologie van de infectieuze endocarditis te achterhalen. Bij deze patiënt waren bij abdominale echografie zowel een inflammatie van de linker craniale uterus als een mogelijk hematoom of abces ter hoogte van de linker ovariumstomp zichtbaar. Histopathologisch onderzoek bevestigde deze inflammatie van het genitaal stelsel. Een arteriële trombo-embolie als complicatie van de infectieuze endocarditis trad op twee dagen nadat de hond was aangeboden. Deze trombus was gelokaliseerd in de arteria mesenterica cranialis en leidde tot een lokale necrose van de dunne darm. Het vermoeden van deze trombo-embolie werd bevestigd aan de hand van zichtbaar verkleinde klepvegetaties op echocardiografie, en een intestinale necrose en steatitis op de echografie van het abdomen, wat leidde tot de keuze om een exploratieve laparotomie uit te voeren. Het doel van de behandeling is het uitroeien van het infectieuze agens door middel van een langdurige behandeling met een hoge concentratie antibiotica en het behandelen van secundaire complicaties. Terwijl er werd gewacht op de resultaten van het bloedonderzoek werd allereerst een empirische breed-spectrum antibioticum behandeling met meronem opgestart. Nadat de resultaten van het bloedonderzoek bekend waren, werd de patiënt behandeld met enrofloxacine intra-veneus voor één week, gevolgd door subcutane toediening voor de opvolgende week, en vervolgens oraal voor nog eens vijf weken. Daarnaast werd er een enterectomie uitgevoerd om de gevolgen van de complicatie, het genecrotiseerde deel van de dunne darm, te verwijderen. Wat de opvolging van deze patiënt betreft, werd de echocardiografie herhaald zowel tijdens de behandeling als na het beëindigen ervan, om de evolutie van de klepletsels (vegetatie en grootte van de regurgitatie) op te volgen. Idealiter wordt de bloedcultuur tijdens en na het stopzetten van de behandeling herhaald, wat bij deze patiënt niet uitgevoerd werd, gezien de duidelijk positieve therapeutische respons. De behandeling van de patiënt had een positieve uitkomst daar de klepinsufficiëntie en de vegetaties verkleinden en de patiënt klinisch stabiel was. De prognose van infectieuze endocarditis is meestal slecht, maar na 2,5 jaar leeft de patiënt nog altijd en ondanks de blijvende systolische hartruis heeft ze niet langer klinische symptomen. Ook de enterectomie heeft geen verdere gevolgen gehad.
3
1. Introduction Infective endocarditis is caused by bacterial invasion of the valvular endothelium. Mechanical lesions or inflammatory disease can promote these colonizing bacteria within the endothelium. During the disruption of the endothelium, extracellular matrix proteins, thromboplastin and the tissue factors trigger coagulation on the damaged endothelium. This coagulum sequentially binds bacteria and activates inflammatory factors. The organisms that have the highest ability to adhere to damaged valves, such as Staphyloccocus and Streptococcus species, commonly cause infective endocarditis. A gram-negative bacteraemia often results in a (per)acute clinical manifestation whereas a gram-positive bacteraemia results in a subacute or chronic condition. Inflammatory diseases can however also be the cause of infective endocarditis. They induce endothelial cell expression of integrins that bind bacteria and fibronectin to the extracellular matrix (Ettinger and Feldman, 2010; Bonagura and Twedt, 2014). Additionally, these colonizing bacteria can excrete enzymes that lead to the destruction of the valve tissue and the proliferation of a local vegetative lesion together with the inflammatory process. These fibrinous vegetative lesions shield the bacteria from the bloodstream and inflammatory cells. Furthermore, they provide a challenging obstacle for antibiotic penetration (Ettinger and Feldman, 2010; Bonagura and Twedt, 2014). These proliferative or erosive lesions can consequently produce a valvular insufficiency or obstruction. These consequences depend on several factors such as the virulence of the infective agent, the site of infection, the degree of valvular destruction, the influence of vegetation on valvular function, the production of exo- or endotoxins, the interaction with the immune system with the formation of immunocomplexes, and the development of thromboembolism and metastatic infections (Ettinger and Feldman, 2010). The insufficiency can be noticed on auscultation as a cardiac murmur. Even though degenerative myxomatous valvular disease is a much more common underlying disease of cardiac murmurs in older dogs, infective endocarditis should be a differential diagnosis especially in large breed dogs. This case report will discuss a patient with infective endocarditis together with its most common complication. Successively the signalment, anamnesis, general clinical examination, specific cardiorespiratory examination, problem list, differential diagnoses, diagnostic plan, results of the additional examinations, treatment and the follow-up will be discussed. The most interesting aspect of this case is that the underlying pathogen has been found in both blood culture and at the site that probably caused the infective endocarditis, as well as the site and management of the thromboembolism.
4
2. Literature
2.1. Predisposition Infective endocarditis is mainly seen in middle sized to large breed dogs such as Labrador retrievers, Golden retrievers, German Shepherds, Mastiffs, Bernese Mountain Dogs, Boxers, Australian Shepherds, Shetland Sheepdogs, Great Danes, Airedale Terriers and Newfoundlanders, mostly at the age of five years and older. Most of these breeds weigh more than fifteen kilograms (Breitschwerdt et al., 1995; Junius et al., 2004; MacDonald et al., 2004; Sykes et al., 2006a; Chomel et al., 2009). The overall annual incidence of all dogs with infective endocarditis ranges from 0.03% up to 0.1% (Sykes et al., 2006a).
2.2. Aetiology Infective endocarditis can only develop if a transient or persistent bacteraemia is present in the body (Häggström, 2010). Periodontal diseases can be the source of the bacteriaemia. The risk of endocarditis is six times higher for dogs with an attachment loss (up to 50%) or alveolar loss with periodontal pockets, possible gingival recession and root exposure, than dogs with just an acute gingival inflammation (Glickman et al., 2009). Tooth root abscess can also predispose an individual to this condition (Sykes et al., 2006b). Other possible predisposing factors could be: acquired defects of innate or adaptive immunity, pneumonia, pancreatitis, peritonitis, prostatitis, pyometra, discospondylitis, sternebral osteomyelitis, urinary tract infection, pyelonephritis, recurrent haemorrhagic gastroenteritis, neoplastic diseases, cystitis, deep pyoderma, skin abscesses and wound infection, gastric dilatation with a volvulus, abdominal surgery, sub-aortic stenosis treated by balloon dilation and long-term indwelling central venous catheters (DeBowes et al., 1996; MacDonald et al., 2004; Sykes et al., 2006b; MacDonald, 2010). Another possible risk is associated if corticosteroids, alone or together with azathioprine, are used (Calvert, 1982; Sykes et al., 2006b). Furthermore the condition has also been associated with sub-aortic stenosis and high-velocity shunting diseases such as patent ductus arteriosus and ventricular septal defect (Sisson and Thomas, 1984; Sykes et al., 2006b).
2.3. General physical examination The most common symptoms are: lethargy, decreased appetite, fever, tachypnoea, tachycardia, arrhythmia, and a heart murmur. However, also other symptoms such as anorexia, (shifting) leg lameness, swollen limbs and joints, coughing, respiratory difficulty, increased lung sounds, epistaxis, vomiting, and weakness/collapse are not uncommon for infective endocarditis (Breitschwerdt et al., 1995; Chomel et al., 2001; Junius et al., 2004; MacDonald et al., 2004; Kelly et al., 2006; Sykes et al., 2006a; Dunn et al., 2007; Chomel et al., 2009; Ettinger and Feldman, 2010; Häggström, 2010). Neurological symptoms may also be present and include: ataxia, deficits of conscious proprioception, strabismus, vestibular signs, obtundation and anisocoria, and unilateral facial nerve paresis (Chomel et al., 2001; Sykes et al., 2006a; Häggström, 2010).
2.4. Specific cardiac examination Tachycardia, arrhythmia (mostly ventricular) and a systolic murmur are cardiac abnormalities commonly auscultated on physical examination of patients with infective endocarditis. In the literature most murmurs are graded from two to four out of six. If there is an endocarditis of the mitral valves, the
5
point of maximal intensity is at the left apex. The intensity of this murmur is roughly parallel to the severity of the regurgitation of the mitral valve. If there is an endocarditis of the aortic valve with an aortic insufficiency, a soft diastolic murmur at the left base of the heart can be heard. This diastolic murmur is sometimes combined with a systolic basilar ejection murmur due to the underlying sub-aortic stenosis, narrowed aortic lumen due to the vegetative lesion, or an increased stroke volume as a result of the enormous aortic insufficiency. Other cardiovascular abnormalities that might be detected are red, pale or cyanotic mucous membranes and absent pulses. (Breitschwerdt et al., 1995; Chomel et al., 2001; Junius et al., 2004; MacDonald et al., 2004; Kelly et al., 2006; Sykes et al., 2006a). Arterial pulses are generally hyperdynamic and can be accompanied by arterial pulse deficits associated with occasional premature beats (Breitschwerdt et al., 1995).
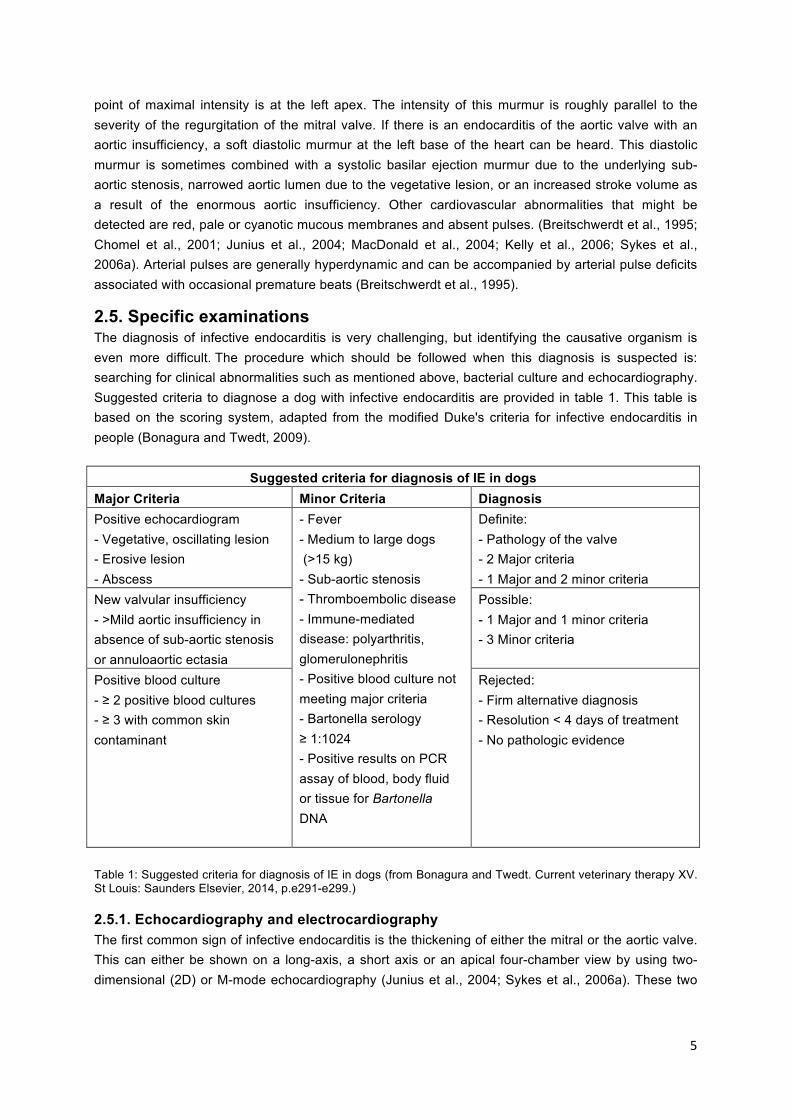
2.5. Specific examinations The diagnosis of infective endocarditis is very challenging, but identifying the causative organism is even more difficult. The procedure which should be followed when this diagnosis is suspected is: searching for clinical abnormalities such as mentioned above, bacterial culture and echocardiography. Suggested criteria to diagnose a dog with infective endocarditis are provided in table 1. This table is based on the scoring system, adapted from the modified Duke's criteria for infective endocarditis in people (Bonagura and Twedt, 2009).
Suggested criteria for diagnosis of IE in dogs Major Criteria Minor Criteria Diagnosis Positive echocardiogram - Vegetative, oscillating lesion - Erosive lesion - Abscess
- Fever - Medium to large dogs (>15 kg) - Sub-aortic stenosis - Thromboembolic disease - Immune-mediated disease: polyarthritis, glomerulonephritis - Positive blood culture not meeting major criteria - Bartonella serology ≥ 1:1024 - Positive results on PCR assay of blood, body fluid or tissue for Bartonella DNA
Definite: - Pathology of the valve - 2 Major criteria - 1 Major and 2 minor criteria
New valvular insufficiency - >Mild aortic insufficiency in absence of sub-aortic stenosis or annuloaortic ectasia
Possible: - 1 Major and 1 minor criteria - 3 Minor criteria
Positive blood culture - ≥ 2 positive blood cultures - ≥ 3 with common skin contaminant
Rejected: - Firm alternative diagnosis - Resolution < 4 days of treatment - No pathologic evidence
Table 1: Suggested criteria for diagnosis of IE in dogs (from Bonagura and Twedt. Current veterinary therapy XV. St Louis: Saunders Elsevier, 2014, p.e291-e299.)
2.5.1. Echocardiography and electrocardiography The first common sign of infective endocarditis is the thickening of either the mitral or the aortic valve. This can either be shown on a long-axis, a short axis or an apical four-chamber view by using two-dimensional (2D) or M-mode echocardiography (Junius et al., 2004; Sykes et al., 2006a). These two
6
modes can also be used to distinguish secondary changes in the size of the heart (Ettinger and Feldman, 2010; Häggström, 2010). Detection of an irregular hyperechoic lesion on the valve by means of echocardiography is the principal indication of infective endocarditis. Smaller lesions are often most obvious on the valvular surface facing the blood flow. These small lesions might however be too difficult to distinguish from endocardiosis (Peddle and Sleeper, 2007; Ettinger and Feldman, 2010; Häggström, 2010). These thickened valves contain vegetative lesions that can be oscillating, vibratory or mobile and move independently from the valve. They could have a nodular change, a fluffy, an irregular-shaped or a moth-eaten appearance. Furthermore, these lesions could vary from being focal to discrete. (Breitschwerdt et al., 1995; Junius et al., 2004; Sykes et al., 2006a; Ettinger and Feldman, 2010; MacDonald, 2010; Bonagura and Twedt, 2014). Other valvular abnormalities are: valvular hyperechogenicity, irregularity, erosion and proliferative lesions (Sykes et al., 2006a; Häggström, 2010; MacDonald, 2010). Abscesses may appear as heterogenic and thickened regions or masses in the myocardium or the annulus. If the abscess has ruptured, a fistula or a septal defect can be seen between the two chambers (MacDonald, 2010). Regurgitation is another common sign of infective endocarditis on echocardiographic examination. This is described in literature from being mild to severe by means of the colour-flow Doppler. This valvular insufficiency can be identified by observing a turbulent regurgitation jet from the left ventricle into the left atrium with mitral regurgitation or from the aortic valve into the left ventricle with aortic insufficiency (Breitschwerdt et al., 1995; Junius et al., 2004; Sykes et al., 2006a; Ettinger and Feldman, 2010; MacDonald, 2010; Häggström, 2010). Sub-aortic stenosis can be present and is diagnosed through a 2D image of fibrotic narrowing of the left ventricular outflow tract. Its severity is also measured through the aortic outflow velocity by continuous wave Doppler in the left apical five-chamber view. Severity of the aortic insufficiency is estimated by the width of the jet origin, length of the insufficiency jet on colour flow Doppler and by the slope of the aortic insufficiency on continuous wave Doppler (Ettinger and Feldman, 2010; MacDonald, 2010; Bonagura and Twedt, 2014). As a result of the chronic regurgitation the heart will undergo remodelling. This is seen as left ventricular eccentric hypertrophy with reduced systolic functional indices such as shortening fraction. However, also mild to moderate left atrial enlargement is reported (Breitschwerdt et al., 1995; Sykes et al., 2006a; Häggström, 2010; MacDonald, 2010).. Complications of infective endocarditis seen on echocardiographic examination are: valve prolapse, acquired valve stenosis, defects in mitral valve leaflets and aortic valve cusps, ruptured mitral valve chorda tendineae, acquired interventricular septal defect, avulsion of the noncoronary cusp of the aortic valve, or mild pericardial effusion (Sykes et al., 2006a; Häggström, 2010; MacDonald, 2010). Furthermore, echocardiography is not only useful for detecting complications, but also in monitoring the response during treatment (Sykes et al., 2006a). Published reports of echocardiography studies indicate that the septal leaflet alone is affected in 50% of cases, only the mural leaflet in 4% while both leaflets are affected in the remainder. Also the mitral valve is more commonly affected than the aortic valve (Sykes et al., 2006a). If infective endocarditis is the most probable diagnosis following clinical examination, but no characteristic abnormalities are seen on a transthoracic echocardiography, the procedure should be repeated after a few days or a transesophageal echocardiography should be performed to better
7
evaluate the valve morphology (Sykes et al., 2006a; Ettinger and Feldman, 2010; MacDonald, 2010; Bonagura and Twedt, 2014). An electrocardiogram can be taken to detect arrhythmias, ventricular premature complexes, supraventricular tachycardia, third-degree atrioventricular block, ventricular tachycardia, and atrial fibrillation. Deviation in the ST segment suggests myocardial hypoxia and may indicate coronary artery embolism or ischaemia due to heart failure (Breitschwerdt et al., 1995; Chomel et al., 2001; MacDonald et al., 2004; Ettinger and Feldman, 2010).
2.5.2. Radiology Radiographs of the thorax are usually taken to exclude the presence of coexisting thoracic diseases, to assess global cardiac size and to evaluate left-sided congestive heart failure. Severe mitral or aortic insufficiency leads to elevated left ventricular end diastolic pressure, left atrial pressure, and pulmonary capillary pressure. This, as a consequence, results in pulmonary oedema. An increase in a perihilar to caudodorsal interstitial, bronchointerstitial or an alveolar pulmonary pattern can sometimes be seen (Breitschwerdt et al., 1995; MacDonald et al., 2004; Kelly et al., 2006; Sykes et al., 2006a; Häggström, 2010). However, also abnormalities such as generalized cardiomegaly or microcardia, vascular attenuation, left atrial and ventricular enlargement, pulmonary venous distention, pleural effusion, or bronchiectasis were sometimes detected in dogs with infective endocarditis (MacDonald et al., 2004; Kelly et al., 2006; Sykes et al, 2006a; MacDonald, 2010).
2.5.3. Ultrasound An ultrasound of the abdomen can be performed to detect the underlying cause of the infective endocarditis. Sykes et al. (2006a) described that a bacterial urinary tract infection for example may be a cause of infective endocarditis. However, ultrasound of the abdomen can also be used to detect consequences of infective endocarditis such as occlusive thromboembolism. If thrombosis of the supplying branches of the renal artery occurs, infarcts of the kidneys will be seen on ultrasound. But if thromboembolism obstructs the iliac artery or the aorta, problems in the hind limbs will occur. The same can happen to the front limbs if an obstruction of the cephalic vein occurs (Breitschwerdt et al., 1995; Sykes et al., 2006a).
2.5.4. Blood culture Positive blood cultures help to confirm the infective endocarditis and also help to give a proper selection in choosing the correct antimicrobial treatment (MacDonald, 2010). The bacteraemia associated with the infective endocarditis is a continuous event rather than an intermittent event. Large volumes of preferably more than ten millilitres of blood increase the likelihood of growth because the concentration of bacterial organisms within blood is usually very low (Peddle and Sleeper, 2007). Ideally, three to four blood samples should be collected aseptically from different venous sites, 30 to 60 minutes apart and then all submitted for aerobic and anaerobic bacterial cultivation (Ettinger and Feldman, 2010; Häggström, 2010). The most common organisms causing the infective endocarditis are: Bartonella (vinsonii subspecies berkhoffi, clarridgeiae, clarridgeiaelike, quintana), Staphylococcus species (aureus, intermedius, coagulase positive and negative), Streptococcus species (canis, bovis and β-haemolytic), and Escherichia coli. Less common causing bacteria are: Pseudomonas aeruginosa, Erysipelothrix rhusiopathiae, Enterobacter, Pasteurella canis, Corynebacterium, Enterococcus (faecium and faecium var zymogenes), and Proteus. Rare bacteria are Bordetella avium-like organisms, Actinomyces
8
turicensis, Erysipelothrix tonsillarum, Citrobacter freundii, Salmonella arizonae, and Mycobacterium (Junius et al., 2004; MacDonald et al., 2004; Kelly et al., 2006; Sykes et al., 2006b; MacDonald, 2010). However, some bacteria cannot be cultured directly from the blood, but only from a sample of the heart valve itself. Examples of these bacteria are Bartonella and Mycobacterium that can be diagnosed with Polymerase Chain Reaction (PCR) heart valve analysis (Breitschwerdt, 1995; Chomel et al., 2001; MacDonald et al., 2004; Kelly et al., 2006; Sykes et al., 2006b; Chomel, 2009). If the blood culture is negative, Bartonella often is the causative agent (MacDonald, 2010). However, also a positive blood culture for Bartonella is sometimes mentioned in the literature (Chomel et al., 2001). A titre of ≥1: 1024 serum antibodies is strongly suggestive for bartonellosis (Häggström, 2010). Besides bacterial infection also fungal infections can be the cause of infective endocarditis. Aspergillus species are the only microorganisms so far described in literature (Sykes et al., 2006b). All these various types of micro-organisms preferentially colonise different valves, cause different increases of body temperature, do or do not give a neutrophilic polyarthritis, or do or do not cause a congestive heart failure (Sykes et al., 2006b).
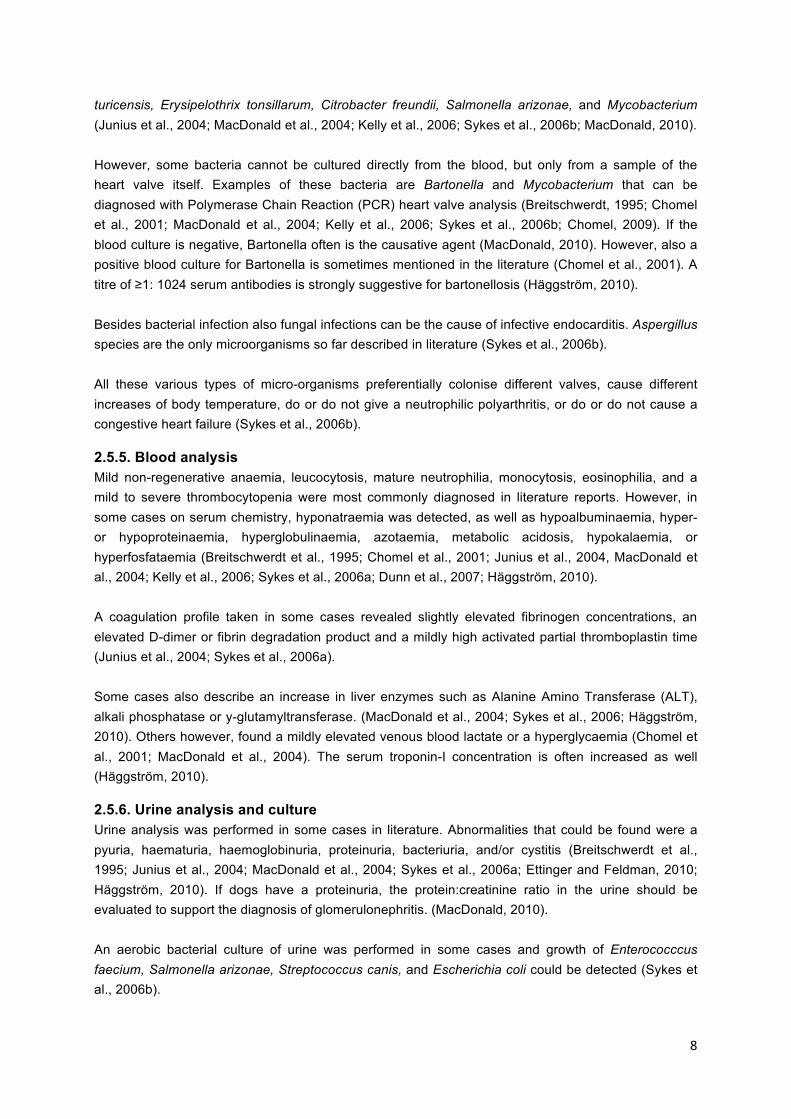
2.5.5. Blood analysis Mild non-regenerative anaemia, leucocytosis, mature neutrophilia, monocytosis, eosinophilia, and a mild to severe thrombocytopenia were most commonly diagnosed in literature reports. However, in some cases on serum chemistry, hyponatraemia was detected, as well as hypoalbuminaemia, hyper- or hypoproteinaemia, hyperglobulinaemia, azotaemia, metabolic acidosis, hypokalaemia, or hyperfosfataemia (Breitschwerdt et al., 1995; Chomel et al., 2001; Junius et al., 2004, MacDonald et al., 2004; Kelly et al., 2006; Sykes et al., 2006a; Dunn et al., 2007; Häggström, 2010). A coagulation profile taken in some cases revealed slightly elevated fibrinogen concentrations, an elevated D-dimer or fibrin degradation product and a mildly high activated partial thromboplastin time (Junius et al., 2004; Sykes et al., 2006a). Some cases also describe an increase in liver enzymes such as Alanine Amino Transferase (ALT), alkali phosphatase or y-glutamyltransferase. (MacDonald et al., 2004; Sykes et al., 2006; Häggström, 2010). Others however, found a mildly elevated venous blood lactate or a hyperglycaemia (Chomel et al., 2001; MacDonald et al., 2004). The serum troponin-I concentration is often increased as well (Häggström, 2010).
2.5.6. Urine analysis and culture Urine analysis was performed in some cases in literature. Abnormalities that could be found were a pyuria, haematuria, haemoglobinuria, proteinuria, bacteriuria, and/or cystitis (Breitschwerdt et al., 1995; Junius et al., 2004; MacDonald et al., 2004; Sykes et al., 2006a; Ettinger and Feldman, 2010; Häggström, 2010). If dogs have a proteinuria, the protein:creatinine ratio in the urine should be evaluated to support the diagnosis of glomerulonephritis. (MacDonald, 2010). An aerobic bacterial culture of urine was performed in some cases and growth of Enterococccus faecium, Salmonella arizonae, Streptococcus canis, and Escherichia coli could be detected (Sykes et al., 2006b).
9
2.5.7. Arthrocenthesis Arthrocenthesis is a technique that is performed if there are symptoms of polyarthritis, such as lameness or a joint effusion. Arthrocenthesis and cytologic analysis of synovial fluid can show inflammation, and sometimes there is bacterial growth in culture. Examples of these organisms are Salmonella arizonae and Streptococcus canis (Junius et al., 2004; Sykes et al., 2006a,b; MacDonald, 2010).
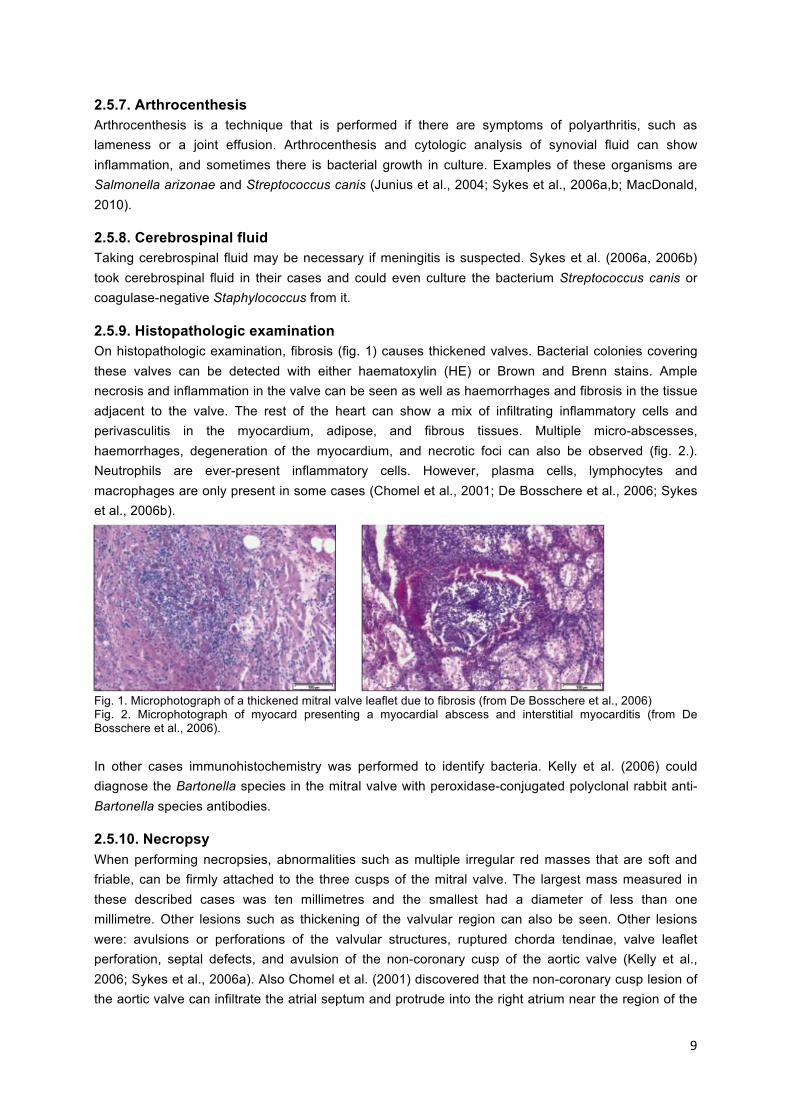
2.5.8. Cerebrospinal fluid Taking cerebrospinal fluid may be necessary if meningitis is suspected. Sykes et al. (2006a, 2006b) took cerebrospinal fluid in their cases and could even culture the bacterium Streptococcus canis or coagulase-negative Staphylococcus from it.
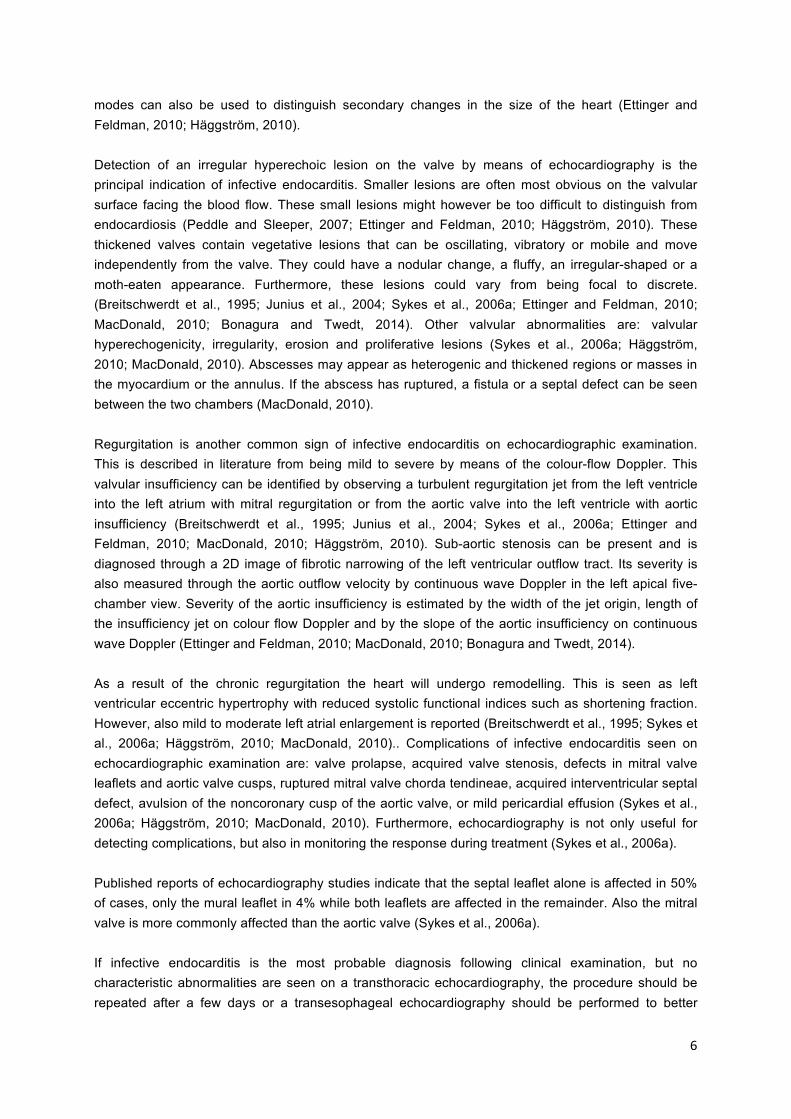
2.5.9. Histopathologic examination On histopathologic examination, fibrosis (fig. 1) causes thickened valves. Bacterial colonies covering these valves can be detected with either haematoxylin (HE) or Brown and Brenn stains. Ample necrosis and inflammation in the valve can be seen as well as haemorrhages and fibrosis in the tissue adjacent to the valve. The rest of the heart can show a mix of infiltrating inflammatory cells and perivasculitis in the myocardium, adipose, and fibrous tissues. Multiple micro-abscesses, haemorrhages, degeneration of the myocardium, and necrotic foci can also be observed (fig. 2.). Neutrophils are ever-present inflammatory cells. However, plasma cells, lymphocytes and macrophages are only present in some cases (Chomel et al., 2001; De Bosschere et al., 2006; Sykes et al., 2006b).
Fig. 1. Microphotograph of a thickened mitral valve leaflet due to fibrosis (from De Bosschere et al., 2006) Fig. 2. Microphotograph of myocard presenting a myocardial abscess and interstitial myocarditis (from De Bosschere et al., 2006). In other cases immunohistochemistry was performed to identify bacteria. Kelly et al. (2006) could diagnose the Bartonella species in the mitral valve with peroxidase-conjugated polyclonal rabbit anti-Bartonella species antibodies.
2.5.10. Necropsy When performing necropsies, abnormalities such as multiple irregular red masses that are soft and friable, can be firmly attached to the three cusps of the mitral valve. The largest mass measured in these described cases was ten millimetres and the smallest had a diameter of less than one millimetre. Other lesions such as thickening of the valvular region can also be seen. Other lesions were: avulsions or perforations of the valvular structures, ruptured chorda tendinae, valve leaflet perforation, septal defects, and avulsion of the non-coronary cusp of the aortic valve (Kelly et al., 2006; Sykes et al., 2006a). Also Chomel et al. (2001) discovered that the non-coronary cusp lesion of the aortic valve can infiltrate the atrial septum and protrude into the right atrium near the region of the
10
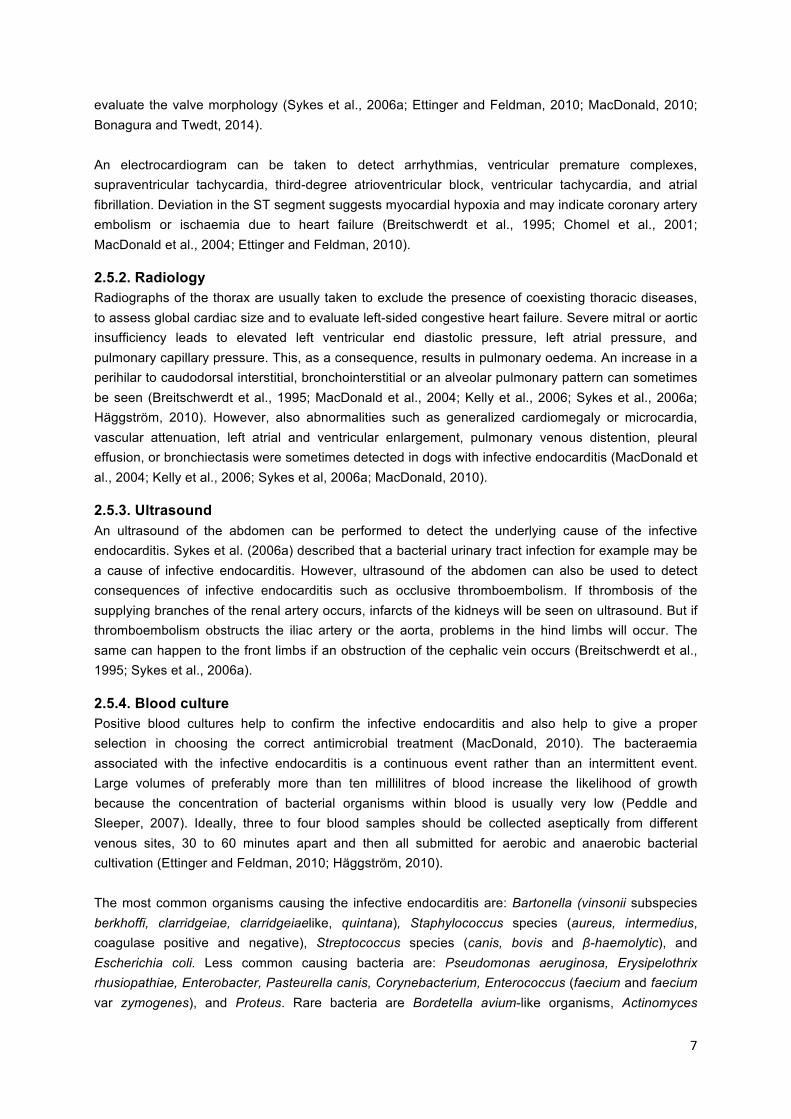
atrioventricular node. Furthermore, they discovered a mild fibrous sub-aortic ring and a moderate left ventricular concentric hypertrophy. Additionally, Chomel et al. (2009) describe a case in which there was a massive defect in the supravalvular region of the mitral valve (fig. 3 and 4).
Fig. 3. Perforation mitral valve (from Chomel et al., 2009) Fig. 4. Mitral valve with major perforation in the supravalvular region of the mitral valve (from Chomel et al., 2009) Consequences of the endocarditis were observed by De Bosschere et al. (2006). They noticed a moderate dilatation of the left ventricle and a myocardial hypertrophy that affected the left ventricle. Additional multiple jet lesions on the endocardium of the left atrium and fibrosis above the mitral valve were visible.
2.6. Differential diagnoses One of the main differential diagnoses of infective endocarditis on echocardiography is myxomatous valve degeneration (also called endocardiosis) that causes proliferative valvular changes. This disease however is mainly seen in small breeds instead of medium to large breeds. Another difference with myxomatous valve degeneration is that no oscillating shaggy mass-type lesions are observed. Also the valvular thickening moves continuously with the valve rather than oppositely and oscillating. Furthermore, the prognosis of myxomatous valve degeneration is by far better than infective endocarditis (MacDonald, 2010; Bonagura and Twedt, 2014). Another differential diagnosis is an extraskeletal osteosarcoma of the heart that mimicked the symptoms of infective endocarditis in a dog (Timian et al., 2011).
2.7. Treatment The goals are to both eradicate the infective pathogen and to treat all secondary complications. A successful therapy is based on early diagnosis as well as aggressive long-term antibiotics treatment. The ideal duration of the therapy is unknown, but should at least be four to six weeks according to some authors but eight to sixteen weeks according to others (Häggström, 2010; MacDonald, 2010). Initially, the antibiotics should be administered intravenously for a week, followed by an oral intake. Selection of the type of antibiotic is based on blood culture and sensitivity testing. High serum concentrations of antibiotics with good cell, fibrin and tissue penetration are needed for the antibiotic to enter the vegetative lesions and kill the bacteria. High doses of antibiotics are therefore often required. While the culture results are pending or when the causal microorganism is unknown, empirical treatment with a broad-spectrum antibiotic is recommended. Aminopenicillines such as ampicillin and fluoroquinolones such as enrofloxacin are contra-indicated by some authors in acute first line of defence because of resistance against antibiotics. However, they are indicated by other authors to be used if the causative agent is unknown. Examples of antibiotics that could be administered in acute first line defence are: aminoglycosides and beta-lactam aminopenicillines or fluoroquinolones alone or

11
in combination with other antibiotics. These other antibiotics could be: cephalosporins, , doxycycline, or metronidazole (MacDonald et al., 2004; Kelly et al., 2006; Ettinger and Feldman, 2010; Häggström, 2010; MacDonald, 2010; Bonagura and Twedt, 2014). The empirical choice of antibiotics after culture and sensitivity testing of particular causative pathogens depends on the clinic and the country and their local antibiotic resistance patterns. Patients should be administered fluids when aminoglycosides are indicated. Aminoglycosides however, are contra-indicated in animals with congestive heart failure due to the aminoglycoside nephrotoxicity that is exaggerated by furosemide therapy (Ettinger and Feldman, 2010; Häggström, 2010; MacDonald, 2010; Bonagura and Twedt, 2014).
Some authors advise the addition of carprofen to the treatment with broad-spectrum antibiotics (Junius et al., 2004). Others advise to provide an anticoagulant therapy, but this is not recommended since it results in increased bleeding episodes. Furthermore, it gives absence of benefit in vegetation resolution or reduced embolic events in humans with infective endocarditis that are treated with aspirin (Baddour et al., 2005). However, it is also important to identify possible secondary problems, such as heart or renal failure, which can affect choice of antibiotic, which may need specific therapy, or which may indicate a worse prognosis (Ettinger and Feldman, 2010).
2.8. Prognosis The median survival time of dogs with mitral valve infective endocarditis is longer than for those with the aortic valve infective endocarditis, with respectively 476 days and three days. Also the Bartonella species has been associated with a shorter median and mean survival time than non-Bartonella species, respectively three and 45 days compared with 330 and 375 days (MacDonald et al., 2004). Other authors mention a median survival time of 54 days and a mortality rate of 56%. Thrombocytopenia, high serum creatinine concentration and thromboembolic complications are negative prognostic factors linked to a significant decrease in the survival time (Sykes et al., 2006a). Euthanasia should be considered if the isolated bacterium is multi-resistant or if there is a high risk of spread of the pathogen to other dogs and humans. Besides euthanasia, also sudden death and congestive heart failure are the most common short-term causes of death (Häggström, 2010).
2.9. Follow-up Ettinger and Feldman (2010), MacDonald (2010) and Bonagura and Twedt (2014) suggest that in patients with a positive blood culture, a repetition of the culture is recommended one to two weeks after starting the antibiotic treatment and two weeks following termination of the antibiotic therapy. An echocardiogram should be obtained after two, four, and six weeks of antibiotic treatment, and two weeks after termination of the antibiotic therapy to assess the size of the vegetative lesion and the severity of the valvular insufficiency. It is a challenge to decide when to stop the long-term antibiotic therapy, because the affected valve often has residual thickening even with a sterile lesion. However, a lack of improvement in an oscillating vegetative lesion after the first week of antibiotic therapy, without a previous bacterial isolate and MIC, may indicate a more aggressive and resistant bacterium, which requires a change or addition of antibiotics. Additional blood and urine analyses and monitoring of body temperature are recommended during and after the antibiotic treatment to monitor the therapeutic success and identify possible complications. During long-term therapy, the presence of a recurrent fever, a leucocytosis, or positive follow-up urine

12
or blood cultures require a continuation of long-term antibiotics therapy, possibly with a different antibiotic combination (MacDonald, 2010). Also other clinicians such as Junius et al. (2004) advise to do a re-evaluation four weeks after starting the medication for the infective endocarditis. While doing a re-evaluation with echocardiographic imaging special attention must be paid to regurgitation, size of the vegetative lesions, thickness of the interventricular septum and left ventricular free-wall, the left atrial and ventricular diameter, and the left atrium: aorta ratio.
2.10. Complications Owing to the fact that a small part of the valves can break, complications such as thromboembolisms can occur. Dogs with an endocarditis of the mitral valve are more likely to have a thromboembolism than dogs with aortic valve involvement. Observations of proliferative, mobile or shaggy lesion during echocardiography cannot predict the occurrence of thromboembolism (Sykes et al., 2006a). Depending on where this thromboembolism obstruction is, different pathologies will happen. Examples are infarction of the kidneys, liver, spleen, pancreas, lungs, myocardium, brain, or systemic arteries. However, thromboembolisms can also occur in the thoracic and pelvic limbs causing cold extremities, cyanotic nail beds, pain and lameness, absence pulses, and firm musculature of the affected limb. However, also haemorrhage with numerous intravascular fibrin thrombi can appear (Breitschwerdt et al., 1995; MacDonald et al., 2004; De Bosschere et al., 2006; Sykes et al., 2006a; MacDonald, 2010; Kelly et al., 2006; Chomel et al., 2009; Ettinger and Feldman, 2010). Another rare complication described in a case series of four dogs with infective endocarditis was a vascular encephalopathy (Cook et al., 2005). Other sequelae due to the infective endocarditis are congestive heart failure, arrhythmia, glomerulonephritis, protein-losing nephropathy, pulmonary haemorrhage, and septic polyarthritis (Sykes et al., 2006a; MacDonald, 2010). Hypertrophic osteopathy is also a very rare effect of infective endocarditis in dogs. Inflammatory pathologies such as infective endocarditis result in platelet activation. This activation leads to the formation of platelet clumps that could detach from the vegetative endocardial lesion and obstruct peripheral arterial circulation. These platelet clumps subsequently release platelet-derived-growth factor (PDGF) which increases the vascular permeability and is chemotactic to neutrophils, monocytes and fibroblasts. This increased blood flow in the extremities, triggers the overgrowth of vascular connective tissue and subsequently formation of fibrochondroid metaplasia and subperiosteal new bone, starting in the metacarpi and the metatarsi progressing proximally (Dunn et al., 2007).
13
3. Clinical case
3.1. Signalment This case describes a flat-coated retriever bitch of five years and ten months old. This patient was presented to the veterinary cardiology Department of Ghent University.
3.2. Anamnesis The patient was presented with clinical signs of fever, coughing and lethargy that had started six days earlier. These symptoms had started three days after the dog underwent an ovariectomy. Furthermore, one droplet of blood had been seen appearing from the vagina post-operatively. Additionally, a tachypnoea and a tachycardia were noticed by the owners of the dog. The fever was treated with one injection of amoxicillin and a three-day oral treatment with amoxicillin-clavulanate, both without success. On the contrary, the patient also started to vomit and developed diarrhoea. The vomiting was treated with metoclopramide orally. An injection of meloxicam was given for the persistent fever, but this did not give any improvement either. The body temperature remained around 40°C, the patient had no appetite and an amoxicillin injection was repeated. The day before the dog was presented at the faculty, a blood examination had been performed. The results showed a leucocytosis and a neutrophilia. Moreover, there was a hypoglycaemia, a thrombocytopenia, and a mild increase of alkaline phosphatase. Furthermore, an electrocardiogram was performed on which an ST depression was seen. Additionally, there was a family history of dilated cardiomyopathy.
3.3. General physical examination The patient was calm, but responsive, weighed 24.4 kilograms and had a body condition score of 5/9. The mucosae were pink and the capillary refill-time was less than two seconds. Lymph nodes were unremarkable. The respiratory rate was 28 breaths per minute, the respiratory type was normal and nothing abnormal was heard on lung auscultation. The heart rate was 112 beats per minute and heart auscultation revealed a murmur and a sinus arrhythmia. The murmur was systolic and was graded two out of six. The femoral pulse quality was good. The dog had a fever with a body temperature of 40.3°C.
3.4. Specific cardiorespiratory examination On heart auscultation a heart rate of 112 beats per minute was heard, together with a systolic murmur grade two out of six. The punctum maximum of the murmur was localised on the left side of the animal at intercostal space five and six, at the level of the mitral valve. Furthermore, the femoral pulse quality was good , symmetrical, with even filling and without deficit. However, a sinus arrhythmia could be felt. On abdominal palpation the liver was normal in size, there were no signs of abdominal effusion and no distention of the jugular veins. No abnormalities were noticed during respiratory examination. The breathing movements, the lung auscultation and the airstream through the nose were all normal. Also the planum nasale was moist.
3.5. Problem list Fever, systolic murmur at the level of the mitral valve (graded two out of six), lethargy, acute vomiting, and acute diarrhoea were the problems listed from important to less important.

14
3.6. Differential Diagnoses The differential diagnoses of fever are: infection, inflammation, immunological disease, tissue destruction, neoplasia, or a metabolic disorder. A metabolic disorder was less likely since no abnormalities were seen on the biochemistry profile performed by the referring veterinarian. A neoplasia was possible, although the dog was not considered geriatric at an age of only five years and ten months. It was therefore concluded that the most probable aetiologies were infection, inflammation, or immune-mediated disease or tissue destruction. For a left apical systolic murmur at the level of the mitral valve the main differential diagnoses are mitral valve insufficiency due to myxomatous mitral valve disease, valvular endocarditis, valvular dysplasia or another valve disrupting pathology such as a tumour. Myxomatous mitral valve disease was less likely since it typically develops in old small breed dogs (<15kg). Mitral dysplasia is a congenital defect and in that case the murmur would have been present since birth. This was unlikely considering that the cardiac murmur was newly discovered and the dog endured cardiac auscultation multiple times in the past. Neoplasia of the mitral valve is extremely rare, therefore infective endocarditis was the most probable diagnosis. Acute vomiting is a clinical indicator that can be caused by a disease with an intra-gastrointestinal or extra-gastrointestinal origin Possible intra-gastrointestinal causes are: inflammation, neoplasia, foreign object ingestion, obstruction, intussusception, volvulus, dilatation, motility disorder, or infection. Neoplasia is possible, but since the dog was not geriatric it was less likely. Foreign object ingestion was unlikely according to the owners. An obstruction, intussusception, volvulus, dilatation or motility disorder was possible, but an inflammation or infection was most likely since there was a leucocytosis on blood analysis. Especially infection was very likely since this could also have been the cause of the infective endocarditis. Extra-gastrointestinal causes of acute vomiting can be divided into intra-abdominal and extra-abdominal problems. Intra-abdominal problems might be hepatitis, pancreatitis, kidney disease, peritonitis or pyometra. Hepatitis, pancreatitis and kidney disease were unlikely because liver enzymes, amylase, urea and creatinine concentrations were within the normal ranges on blood analysis. Peritonitis and pyometra are pathologies that were possible but did not explain the heart murmur. Extra-abdominal problems might have a metabolic, neurologic or endocrine origin (hypoadrenocorticism), but can also be intoxication. A metabolic disorder was less likely since no abnormalities were seen on the biochemistry profile. Furthermore, the dog was slightly too old to be predisposed to have hypoadrenocorticism. Intoxication was also unlikely according to the owners and a neurologic problem does not correspond with the murmur heard on auscultation. Acute diarrhoea is a clinical indicator that could have an primary underlying intra-gastrointestinal problem or could a systemic disorder. Intra-gastrointestinal causes are: diet mistakes, infection, sub-obstruction or intoxication. The diet had not been changed and the patient had not been fed any leftovers from the table and intoxication was impossible. A sub-obstruction was possible, but only the infectious component could explain the occurrence of the heart murmur. Hypoadrenocorticism, uraemia or pancreatitis are pathologies that are examples of systemic disorders that inflict acute vomiting. However as stated in the previous paragraph, all three of them were unlikely to be the cause of the symptoms in this patient.

15
3.7 Diagnostic plan First of all an echocardiography should be performed to detect the cause of the murmur. The left atrium and left ventricle are checked for dilatation to determine if left congestive heart failure is present. Colour and spectral Doppler are used to check the severity of the insufficiency. Thoracic radiographs can be taken to determine the effects of an underlying pathology or for detection of congestive left heart failure. Furthermore, an ultrasound of the abdomen should be performed to search for the underlying cause of an infective endocarditis, since this is the most probable diagnosis. Additionally, samples for blood culture should be taken to look for a causative bacterial agent. If the culture is positive it must be repeated after the start of treatment to check the effectiveness of the antibiotic. Preferably, the culture must also be repeated after terminating the antibiotic treatment. Also urine analysis and culture are recommended to check for underlying disease and causative bacteria. It is essential to monitor the temperature, respiration rate, heart rate and in this case also vaginal discharge, vomiting and diarrhoea.
3.8. Results
3.8.1. Blood analysis Initially, no blood analysis was performed since this had already been done by the owner’s own veterinarian. This vet concluded that there was a mild increase of alkaline phosphatase and an inflammation with a mild leucocytosis and a neutrophilia. Moreover, there was a mild hypoglycaemia, and a thrombocytopenia.
3.8.2. Blood culture Nevertheless, blood was taken to perform a blood culture and look for a causative pathogen. The pathogen that was found were the Enterobacteriaceae and were positive on five out of nine using the BACTEC blood culture system since the dog had already been treated with antibiotics. Furthermore, an antibiogram was performed to determine the optimal antibiotic treatment. The Enterobacteriaceae were resistant to Cloxacillin-Nafcillin, Ampicillin-Amoxycillin, Amoxycillin-Clavulate, Lincomycin, Clindamycin, Doxycyclin, and Nitrofurans and were intermediately resistant to Ceftiofur-cefquinome and Neo-, Kana-, Fram- and Paromomycine. The only antibiotics being efficacious were: Meronem, Gentamycin, Amikacin, Fluoroquinolones, Sulphonamids and Trimethoprim.
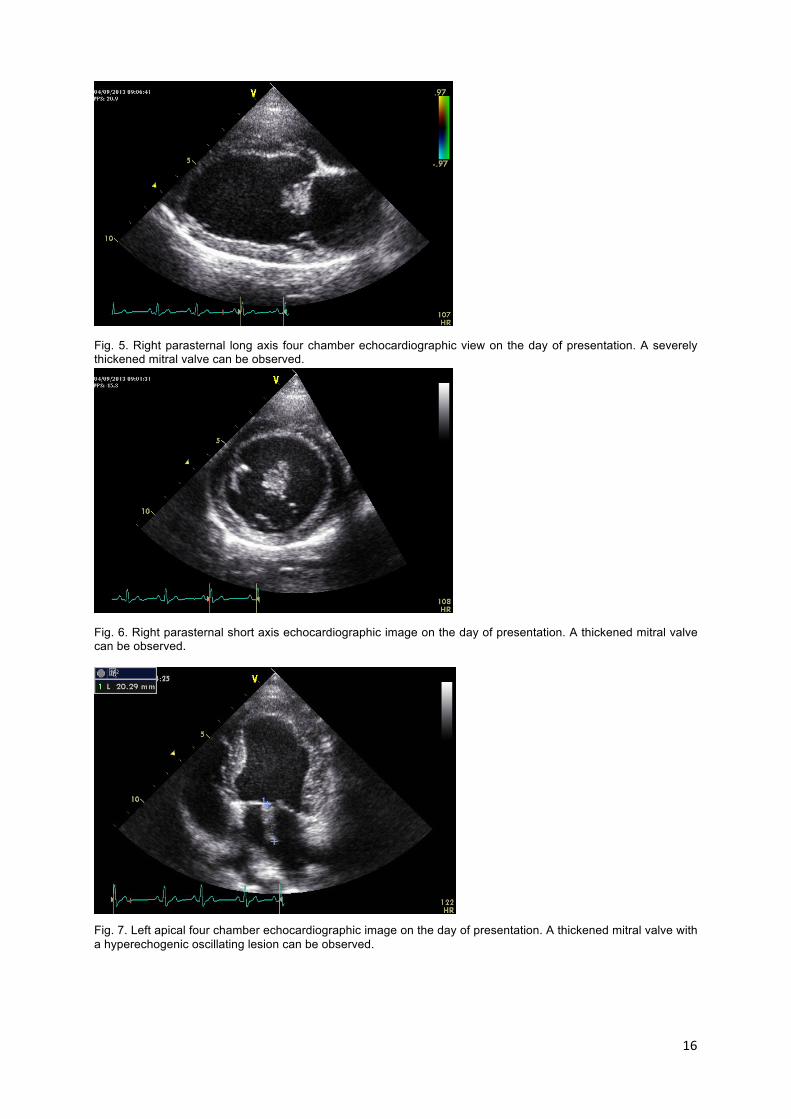
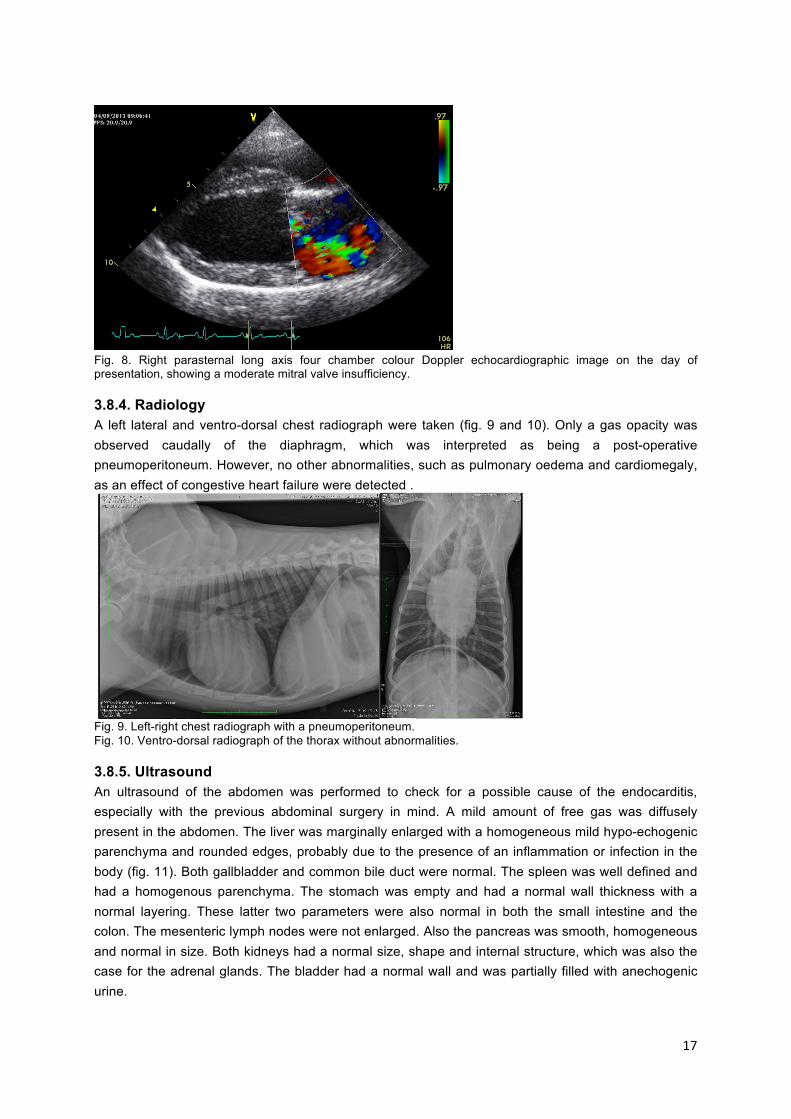
3.8.3. Echocardiography An echocardiogram was performed at initial presentation. A standard echocardiographic protocol was followed. In multiple echocardiographic views (right parasternal long-axis four chamber, right parasternal short axis at the level of the mitral valve, left apical four chamber view) severe thickening of the valve can be observed (fig.5, 6 and 7). Colour Doppler of the long axis image showed moderate regurgitation of the mitral valve (fig. 8). As a result these echocardiographic images were strongly suspicious of infective mitral valve endocarditis; the septal leaflet of the mitral valve was most severely affected.
16
Fig. 5. Right parasternal long axis four chamber echocardiographic view on the day of presentation. A severely thickened mitral valve can be observed.
Fig. 6. Right parasternal short axis echocardiographic image on the day of presentation. A thickened mitral valve can be observed.
Fig. 7. Left apical four chamber echocardiographic image on the day of presentation. A thickened mitral valve with a hyperechogenic oscillating lesion can be observed.
17
Fig. 8. Right parasternal long axis four chamber colour Doppler echocardiographic image on the day of presentation, showing a moderate mitral valve insufficiency.
3.8.4. Radiology A left lateral and ventro-dorsal chest radiograph were taken (fig. 9 and 10). Only a gas opacity was observed caudally of the diaphragm, which was interpreted as being a post-operative pneumoperitoneum. However, no other abnormalities, such as pulmonary oedema and cardiomegaly, as an effect of congestive heart failure were detected .
Fig. 9. Left-right chest radiograph with a pneumoperitoneum. Fig. 10. Ventro-dorsal radiograph of the thorax without abnormalities.
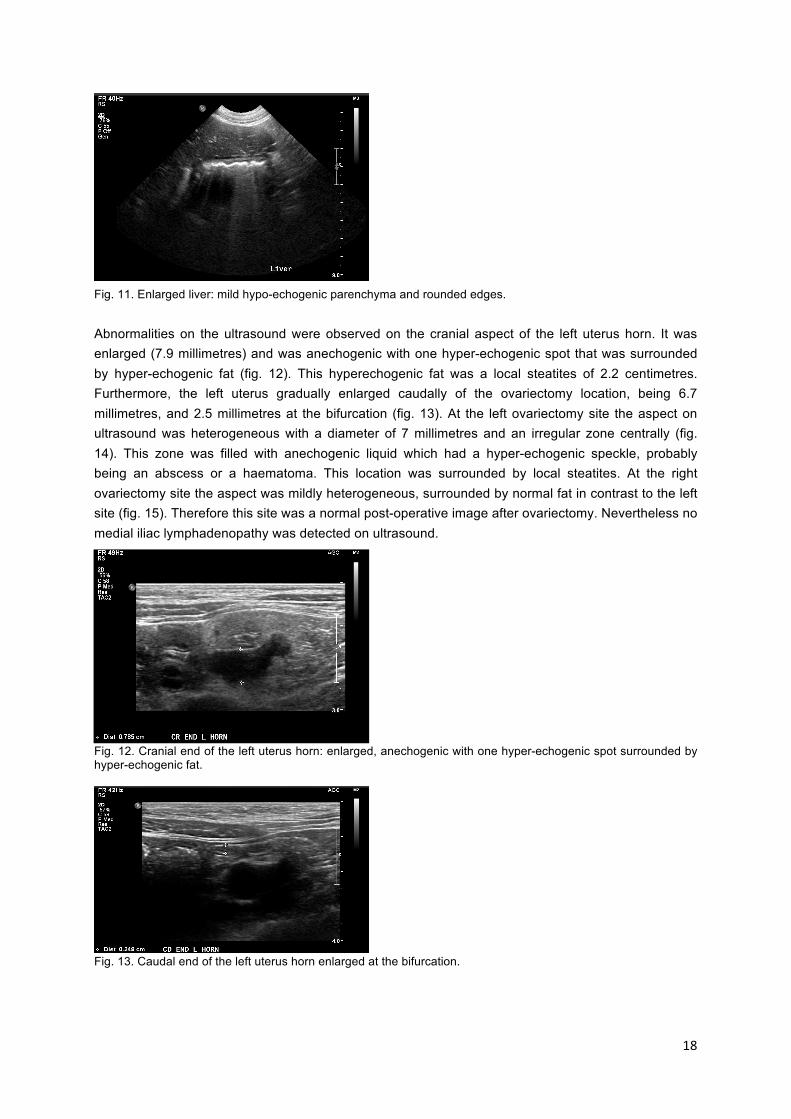
3.8.5. Ultrasound An ultrasound of the abdomen was performed to check for a possible cause of the endocarditis, especially with the previous abdominal surgery in mind. A mild amount of free gas was diffusely present in the abdomen. The liver was marginally enlarged with a homogeneous mild hypo-echogenic parenchyma and rounded edges, probably due to the presence of an inflammation or infection in the body (fig. 11). Both gallbladder and common bile duct were normal. The spleen was well defined and had a homogenous parenchyma. The stomach was empty and had a normal wall thickness with a normal layering. These latter two parameters were also normal in both the small intestine and the colon. The mesenteric lymph nodes were not enlarged. Also the pancreas was smooth, homogeneous and normal in size. Both kidneys had a normal size, shape and internal structure, which was also the case for the adrenal glands. The bladder had a normal wall and was partially filled with anechogenic urine.
18
Fig. 11. Enlarged liver: mild hypo-echogenic parenchyma and rounded edges.
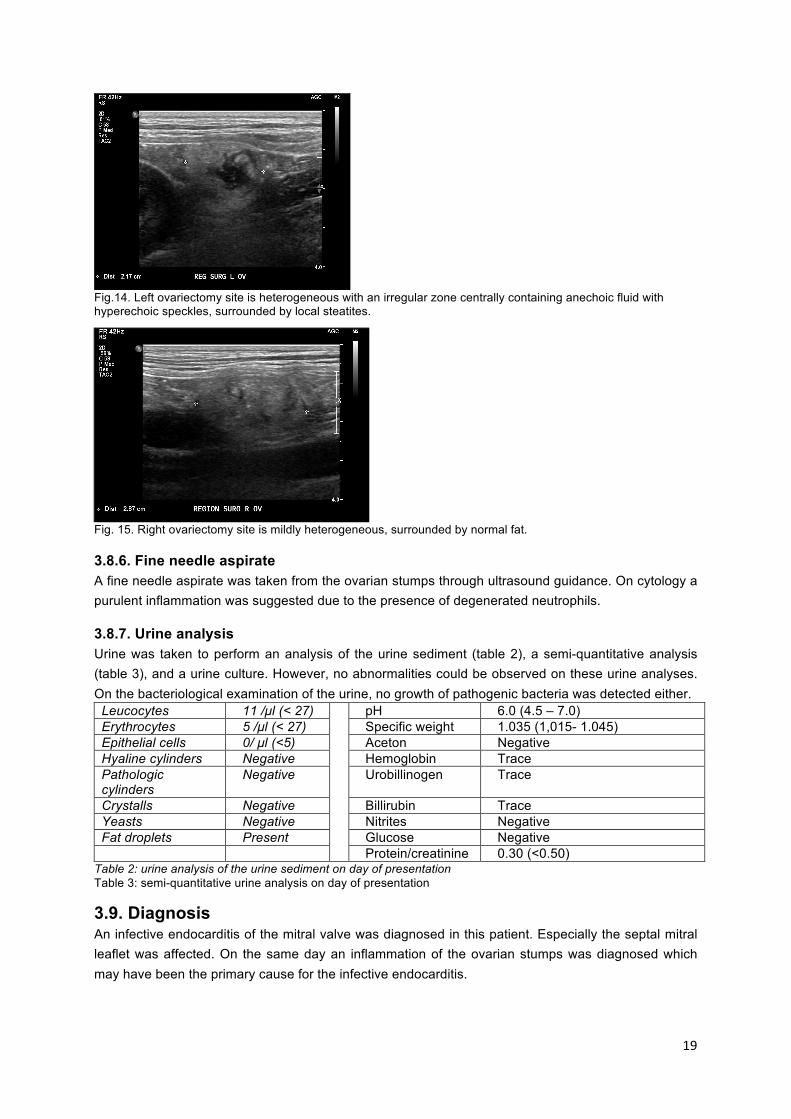
Abnormalities on the ultrasound were observed on the cranial aspect of the left uterus horn. It was enlarged (7.9 millimetres) and was anechogenic with one hyper-echogenic spot that was surrounded by hyper-echogenic fat (fig. 12). This hyperechogenic fat was a local steatites of 2.2 centimetres. Furthermore, the left uterus gradually enlarged caudally of the ovariectomy location, being 6.7 millimetres, and 2.5 millimetres at the bifurcation (fig. 13). At the left ovariectomy site the aspect on ultrasound was heterogeneous with a diameter of 7 millimetres and an irregular zone centrally (fig. 14). This zone was filled with anechogenic liquid which had a hyper-echogenic speckle, probably being an abscess or a haematoma. This location was surrounded by local steatites. At the right ovariectomy site the aspect was mildly heterogeneous, surrounded by normal fat in contrast to the left site (fig. 15). Therefore this site was a normal post-operative image after ovariectomy. Nevertheless no medial iliac lymphadenopathy was detected on ultrasound.
Fig. 12. Cranial end of the left uterus horn: enlarged, anechogenic with one hyper-echogenic spot surrounded by hyper-echogenic fat.
Fig. 13. Caudal end of the left uterus horn enlarged at the bifurcation.
19
Fig.14. Left ovariectomy site is heterogeneous with an irregular zone centrally containing anechoic fluid with hyperechoic speckles, surrounded by local steatites.
Fig. 15. Right ovariectomy site is mildly heterogeneous, surrounded by normal fat.
3.8.6. Fine needle aspirate A fine needle aspirate was taken from the ovarian stumps through ultrasound guidance. On cytology a purulent inflammation was suggested due to the presence of degenerated neutrophils.
3.8.7. Urine analysis Urine was taken to perform an analysis of the urine sediment (table 2), a semi-quantitative analysis (table 3), and a urine culture. However, no abnormalities could be observed on these urine analyses. On the bacteriological examination of the urine, no growth of pathogenic bacteria was detected either.
Leucocytes 11 /µl (< 27) pH 6.0 (4.5 – 7.0) Erythrocytes 5 /µl (< 27) Specific weight 1.035 (1,015- 1.045) Epithelial cells 0/ µl (<5) Aceton Negative Hyaline cylinders Negative Hemoglobin Trace Pathologic cylinders
Negative Urobillinogen Trace
Crystalls Negative Billirubin Trace Yeasts Negative Nitrites Negative Fat droplets Present Glucose Negative
Protein/creatinine 0.30 (<0.50) Table 2: urine analysis of the urine sediment on day of presentation Table 3: semi-quantitative urine analysis on day of presentation
3.9. Diagnosis An infective endocarditis of the mitral valve was diagnosed in this patient. Especially the septal mitral leaflet was affected. On the same day an inflammation of the ovarian stumps was diagnosed which may have been the primary cause for the infective endocarditis.
20
3.10. Treatment Meropenem was started intra-venously empirically awaiting blood and urine culture sensitivity testing. This antibiotic is effective against aerobic or anaerobic gram positive and negative bacteria. Furthermore, every four hours single doses of methadone were administered as analgesics and metoclopramide (0.5-1.0 mg/kg) against nausea and for its gastro-intestinal prokinetic effect. Also, a one-time maintenance of Ringer’s lactate solution was provided intra-venously.
3.11. Hospitalisation The patient was hospitalised and besides treatment with antibiotic meronem IV she received the following additional treatment:
- Anti-emetics: maropitant (2 mg/kg) and metoclopramide (0.5-1.0 mg/kg; initially IV boluses followed by constant rate infusion) since she started vomiting again;
- Gastro-protectant: omeprazole (0.5-1.5 mg/kg; IV every 24 hours); - Analgesia: methadone IV (1 mg/kg every 4 hours); - Fluid therapy: Lactated Ringer’s (rate: maintenance with 100% correction).
The respiratory rate, heart rate and arrhythmias, pulse quality, mucosal membranes, abdominal pain, and urine production were monitored regularly. Despite this treatment the nausea and vomiting were not controlled and the dog appeared to be in pain despite analgesia with methadone. She was uncomfortable on cranial abdominal palpation, tachycardic and tachypnoeic. Analgesia was increased (lidocaine constant rate infusion and methadone increased from single, to double, and even to triple doses). A small haemorrhagic outflow from the vagina remained. Cytology of this outflow was performed, but no inflammation was detected. At this time-point, the echocardiography and abdominal ultrasound were repeated to search for an underlying cause of the abdominal pain, such as gastrointestinal thromboembolism. After confirmation of this gastrointestinal thromboembolism, an explorative surgery of the abdomen was performed two days after presentation. As a result of the surgery the patient stopped vomiting and started eating well but remained nauseous. She was also still hypotens, tachycardic and had tachympoea. The medication mentioned earlier was continued together with a plasma-replacer to correct the blood volume, heparine to prevent the occurrence of disseminated intravascular coagulation after surgery, and sterofundin to balance the electrolytes. Three days after surgery the patient was still slightly sensitive to abdominal palpation, but was now very alert and responsive. Her cardiovascular symptoms were stable and she no longer had tachypnoea and tachycardia. Therefore, the sterofundin was terminated, the metoclopramide was adjusted to administering doses intra-venously and the omeprazole was changed to oral treatment (10mg T.I.D.). All other treatment stated earlier remained the same. Four days after surgery the results of the blood culture and the antibiogram were received. The bacteria were sensitive to fluoroquinolones. The maropitant was discontinued and besides enrofloxacin (5 mg/kg) IV she received the following additional treatment:
- Anti-emtics: metoclopramide IV (0.5-1.0 mg/kg) - Gastro-protectant: omeprazole orally (0.5-1.5 mg/kg) - Analgesia: methadone (1mg/kg) - Fluid therapy: Lactated Ringer’s (rate: maintenance with 100% correction)
21
As a result of the treatment the patient was alert, had a good appetite and no longer had abdominal pain. She was cardiovascularly stable, but a murmur of two out of six with a punctum maximum at the mitral valves remained.
3.12. Blood analyses The second blood analysis of this patient was carried out two days after presentation. Analysis of the biochemical, haematologic and coagulation factors was performed (table 5). The abnormalities in this analysis were: leucocytosis, monocytosis, neutrophilia, thrombocytopenia, mild microcytaire anaemia, and severe elevation of D-dimer concentration. The leucocytosis is caused by an infection in the body. Monocytosis and neutrophilia are two principle types of leucocytosis and are caused by a bacterial infection specifically, which was the case in this patient. The mild microcytaire anaemia can be explained by the fact that erythrocytes are forced through small meshworks of fibrin in the region of the mitral valves. A positive D-dimer result indicates the presence of a high level of fibrin degradation products. It indicates that there may be a thrombus formation and breakdown in the body, for example in disseminated intravascular coagulation or thromboembolism. However, it can also be observed in an infection. These blood parameters remained the same three days after presentation, but the thrombocytopenia became less severe (table 4). Four days after the presentation the anaemia became more severe. The albumin and total protein levels in the blood were tested and both showed hypoalbuminaemia as well as hypoproteneamia (table 4). Five days after presentation the hypoalbuminaemia became less severe, and hypoproteinaemia was no longer present (table 4). Furthermore, a blood smear test revealed 7-10 thrombocytes per high power field which excludes a thrombocytopenia (standard range is 8-20 thrombocytes per high power field).
Table 4: Blood analyses day two to five after presentation
Day 2 Day 3 Day 4 Day 5 Reference Biochemistry Urea 4.4 4.1 2.5 - 9.6 mmol/L
Creatinine 60 69 44-159 µmol/L Albumin 16 19 23-40 g/L Total protein 43 53 52-82 g/L
Haematology Leucocytes 35.01 35.07 5.05-16.76 x 109/ L Lymphocytes 1.83 2.39 1.05-5.1 x 109/ L Monocytes 1.8 1.9 0.16-1.12 x 109/ L Neutrophils 31.24 30.65 2.95-11.64 x 109/ L Eosinophils 0.11 0.08 0.06-1.23 x 109/ L Basophils 0.03 0.05 0-0.1 x 109/ L Haematocrit 32.9% 26.6% 21% at 15:00 and
19% at 19:00 25% 37.3-61.7%
Reticulocytes 16.4 13.1 10-110 K/µL MCV 56.3 56.7 61.6-73.5 fL Platelets 4 49 148-484 K/µL Fibrinogen 386 100-460 mg/dL D-dimers 3.85 0.00-0.50 mg/L
Coagulation cit-PT 14 13 11-17 seconds cit-aPTT 91 109 72-102 seconds
22
3.13. Complications and abnormalities
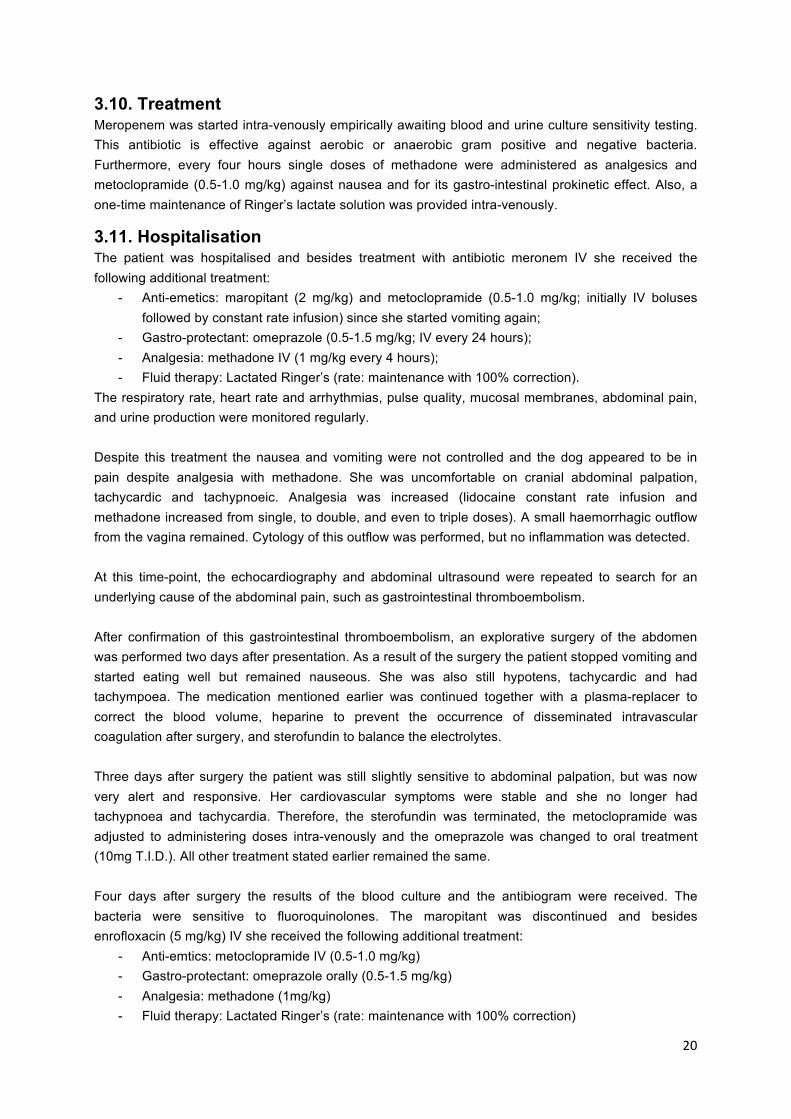
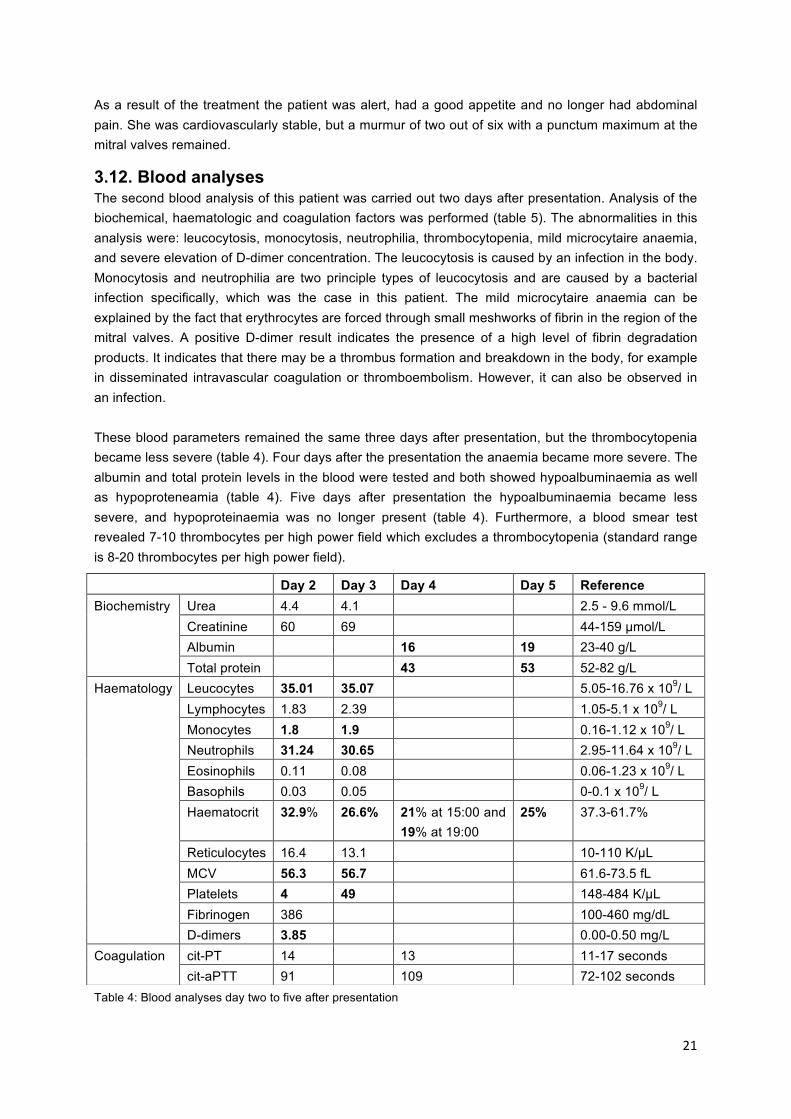
3.13.1. Echocardiography Two days after presentation the echocardiographic examination was repeated to check the vegetative lesions of the mitral valve because there was a suspicion of a thromboembolism. The severe elevated D-dimer concentration was a reason for this suspicion, but also that the patient remained uncomfortable on abdominal palpation despite analgesia, and continued vomiting. On both the long axis image (fig. 16) and the short axis image (fig. 17) this vegetation had become drastically smaller (from two centimetres to six millimetres). The explanation for this is that indeed part of the valvular lesion broke off and confirmed the occurrence of a gastrointestinal thromboembolism, which explained the start of the severe gastrointestinal signs .
Fig. 16. Long axis echocardiographic image four days after presentation. A less thickened mitral valve can be observed, due the fact that part of the valvular lesion broke off.
Fig. 17. Short axis echocardiographic image four days after presentation. A less thickened mitral valve can be observed, due the fact that part of the valvular lesion broke off.
3.13.2. Ultrasound
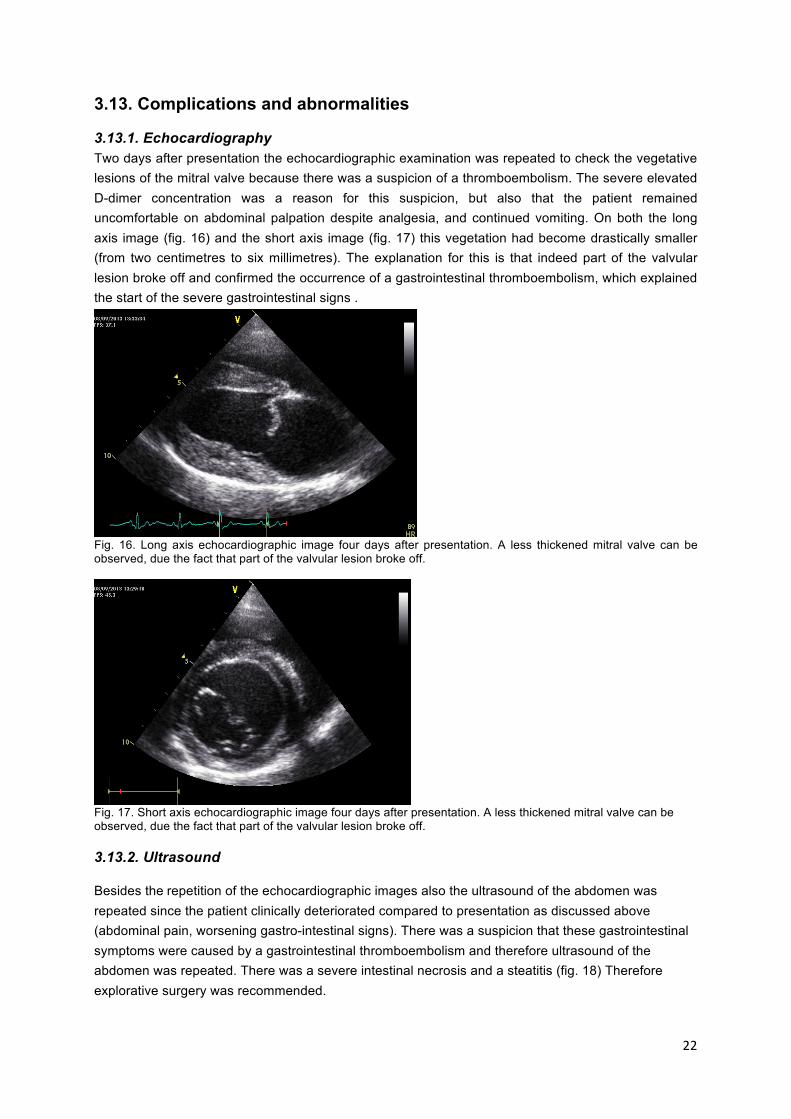
Besides the repetition of the echocardiographic images also the ultrasound of the abdomen was repeated since the patient clinically deteriorated compared to presentation as discussed above (abdominal pain, worsening gastro-intestinal signs). There was a suspicion that these gastrointestinal symptoms were caused by a gastrointestinal thromboembolism and therefore ultrasound of the abdomen was repeated. There was a severe intestinal necrosis and a steatitis (fig. 18) Therefore explorative surgery was recommended.
23
Fig. 18. Intestinal necrosis and steatitis of the jejunum two days after presentation.
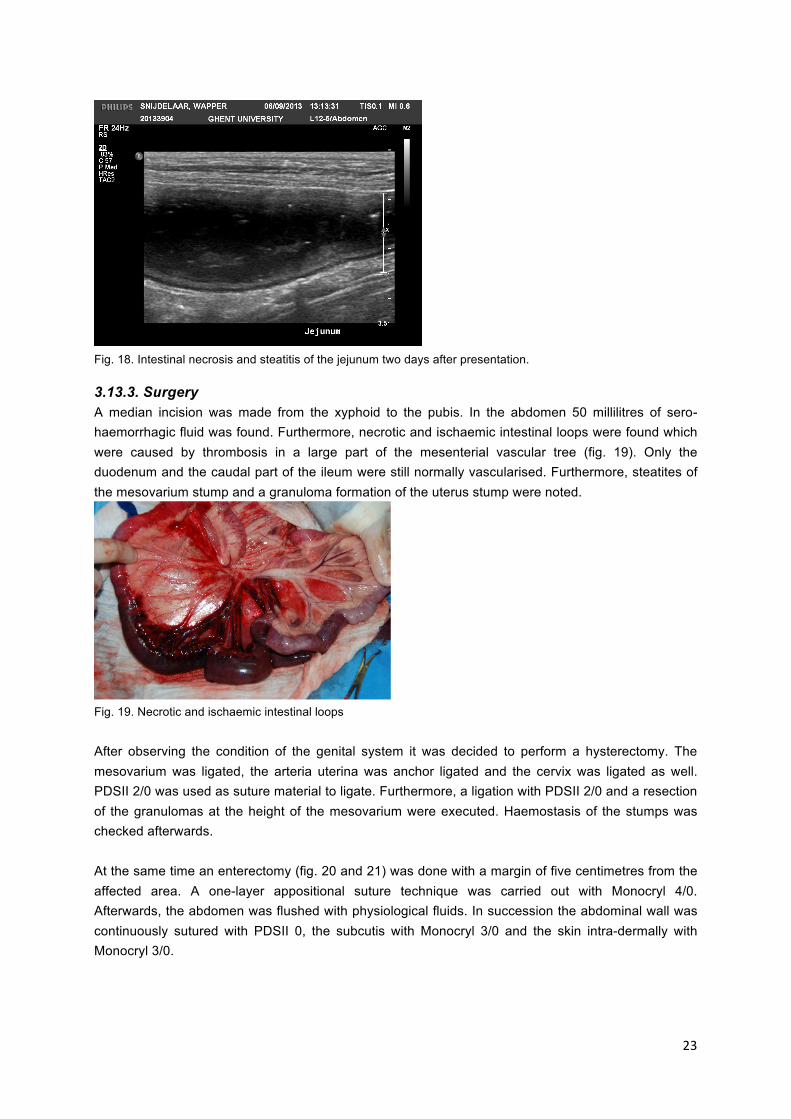
3.13.3. Surgery A median incision was made from the xyphoid to the pubis. In the abdomen 50 millilitres of sero-haemorrhagic fluid was found. Furthermore, necrotic and ischaemic intestinal loops were found which were caused by thrombosis in a large part of the mesenterial vascular tree (fig. 19). Only the duodenum and the caudal part of the ileum were still normally vascularised. Furthermore, steatites of the mesovarium stump and a granuloma formation of the uterus stump were noted. Fig. 19. Necrotic and ischaemic intestinal loops
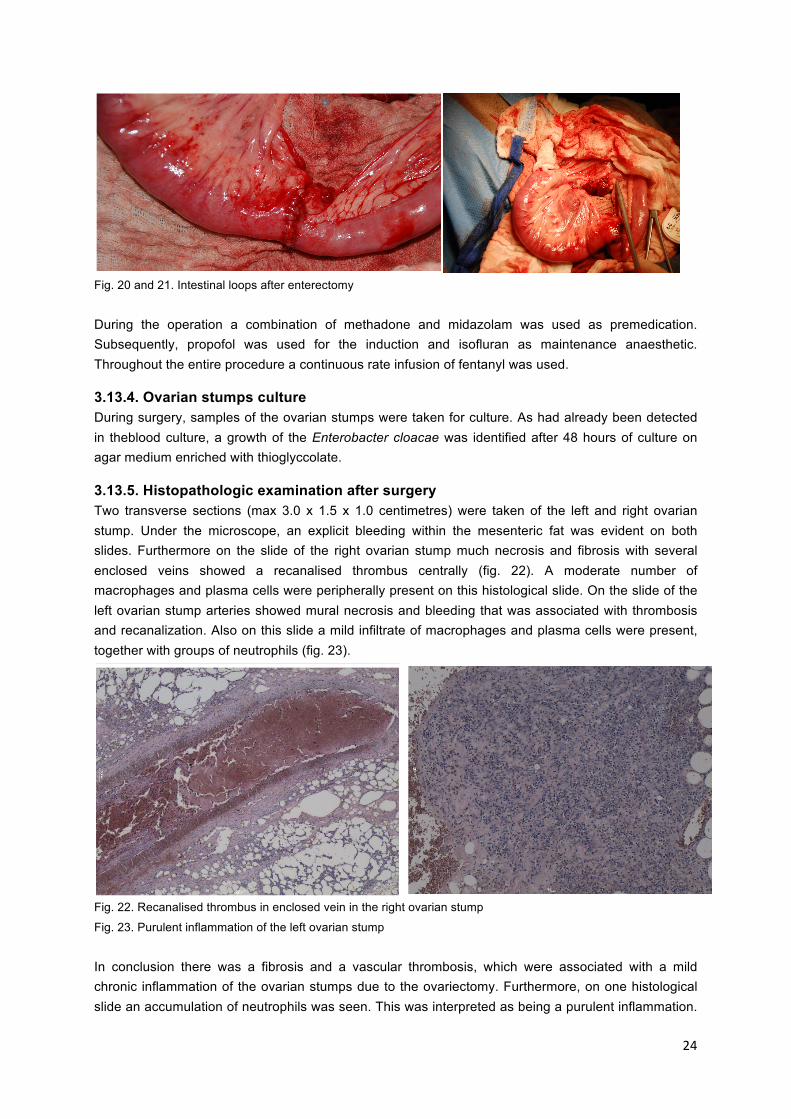
After observing the condition of the genital system it was decided to perform a hysterectomy. The mesovarium was ligated, the arteria uterina was anchor ligated and the cervix was ligated as well. PDSII 2/0 was used as suture material to ligate. Furthermore, a ligation with PDSII 2/0 and a resection of the granulomas at the height of the mesovarium were executed. Haemostasis of the stumps was checked afterwards. At the same time an enterectomy (fig. 20 and 21) was done with a margin of five centimetres from the affected area. A one-layer appositional suture technique was carried out with Monocryl 4/0. Afterwards, the abdomen was flushed with physiological fluids. In succession the abdominal wall was continuously sutured with PDSII 0, the subcutis with Monocryl 3/0 and the skin intra-dermally with Monocryl 3/0.
24
Fig. 20 and 21. Intestinal loops after enterectomy
During the operation a combination of methadone and midazolam was used as premedication. Subsequently, propofol was used for the induction and isofluran as maintenance anaesthetic. Throughout the entire procedure a continuous rate infusion of fentanyl was used.
3.13.4. Ovarian stumps culture During surgery, samples of the ovarian stumps were taken for culture. As had already been detected in theblood culture, a growth of the Enterobacter cloacae was identified after 48 hours of culture on agar medium enriched with thioglyccolate.
3.13.5. Histopathologic examination after surgery Two transverse sections (max 3.0 x 1.5 x 1.0 centimetres) were taken of the left and right ovarian stump. Under the microscope, an explicit bleeding within the mesenteric fat was evident on both slides. Furthermore on the slide of the right ovarian stump much necrosis and fibrosis with several enclosed veins showed a recanalised thrombus centrally (fig. 22). A moderate number of macrophages and plasma cells were peripherally present on this histological slide. On the slide of the left ovarian stump arteries showed mural necrosis and bleeding that was associated with thrombosis and recanalization. Also on this slide a mild infiltrate of macrophages and plasma cells were present, together with groups of neutrophils (fig. 23).
Fig. 22. Recanalised thrombus in enclosed vein in the right ovarian stump
Fig. 23. Purulent inflammation of the left ovarian stump In conclusion there was a fibrosis and a vascular thrombosis, which were associated with a mild chronic inflammation of the ovarian stumps due to the ovariectomy. Furthermore, on one histological slide an accumulation of neutrophils was seen. This was interpreted as being a purulent inflammation.
25
However, it was not certain whether or not this was a primary infection of the ovarian stump or secondary to the embolic spread of an infection.
3.14. New diagnosis The new diagnosis of this patient is infective mitral valve endocarditis with secondary thromboembolism in the arteria mesenterica cranialis that resulted in small intestinal necrosis.
3.15. New treatment Enrofloxacin was given subcutaneously for one week and then continued orally for at least 4 weeks. Metoclopramide (0.3mg/kg orally every 8 hours for three days), and omeprazole (1mg/kg orally every 24 hours for 5 days) were continued Postoperative analgesia consisted of Tramadol (50mg orally every 8 hours) for three days. A gastro-intestinal diet was advised owing to the enterectomy. Hill’s i/d or Royal Canine intestinal were the preferred options.
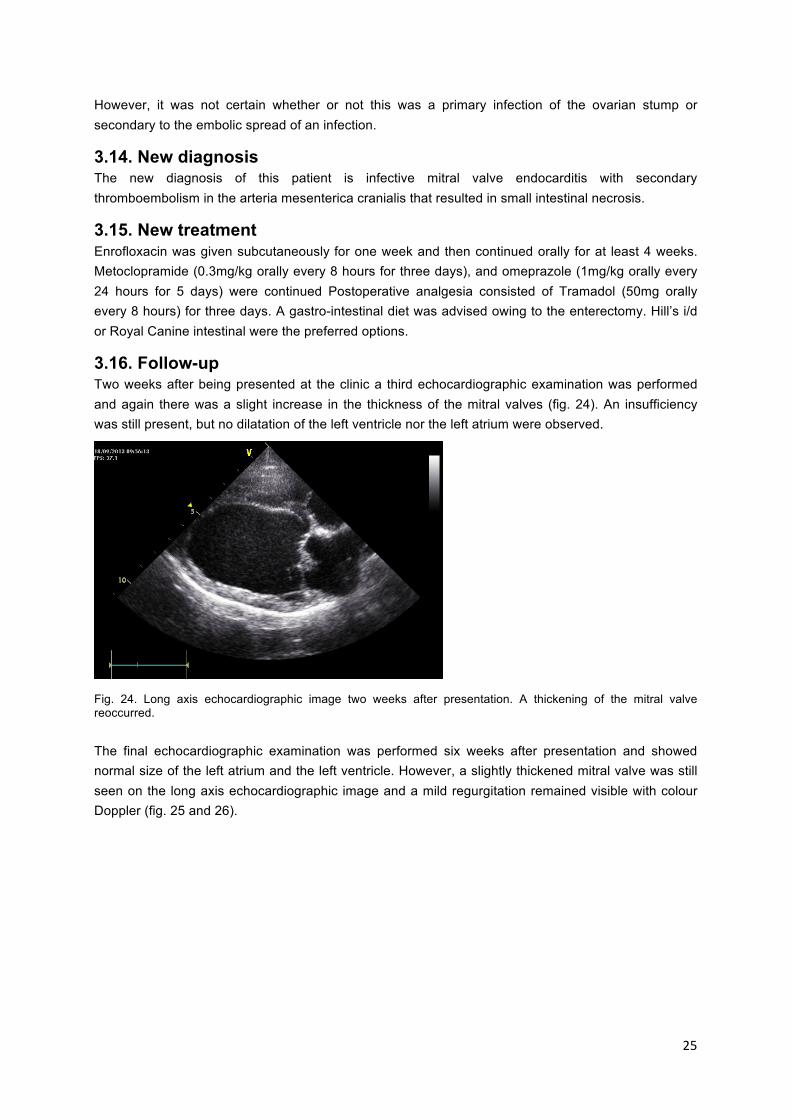
3.16. Follow-up Two weeks after being presented at the clinic a third echocardiographic examination was performed and again there was a slight increase in the thickness of the mitral valves (fig. 24). An insufficiency was still present, but no dilatation of the left ventricle nor the left atrium were observed.
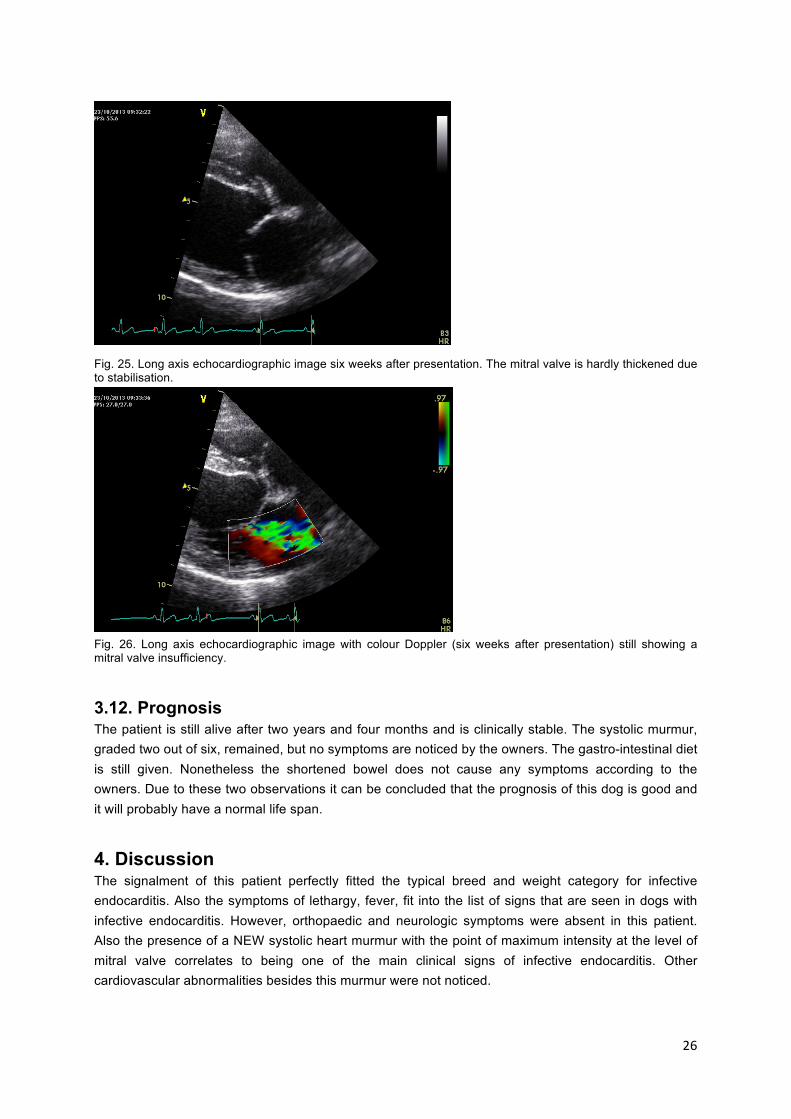
Fig. 24. Long axis echocardiographic image two weeks after presentation. A thickening of the mitral valve reoccurred. The final echocardiographic examination was performed six weeks after presentation and showed normal size of the left atrium and the left ventricle. However, a slightly thickened mitral valve was still seen on the long axis echocardiographic image and a mild regurgitation remained visible with colour Doppler (fig. 25 and 26).
26
Fig. 25. Long axis echocardiographic image six weeks after presentation. The mitral valve is hardly thickened due to stabilisation.
Fig. 26. Long axis echocardiographic image with colour Doppler (six weeks after presentation) still showing a mitral valve insufficiency.
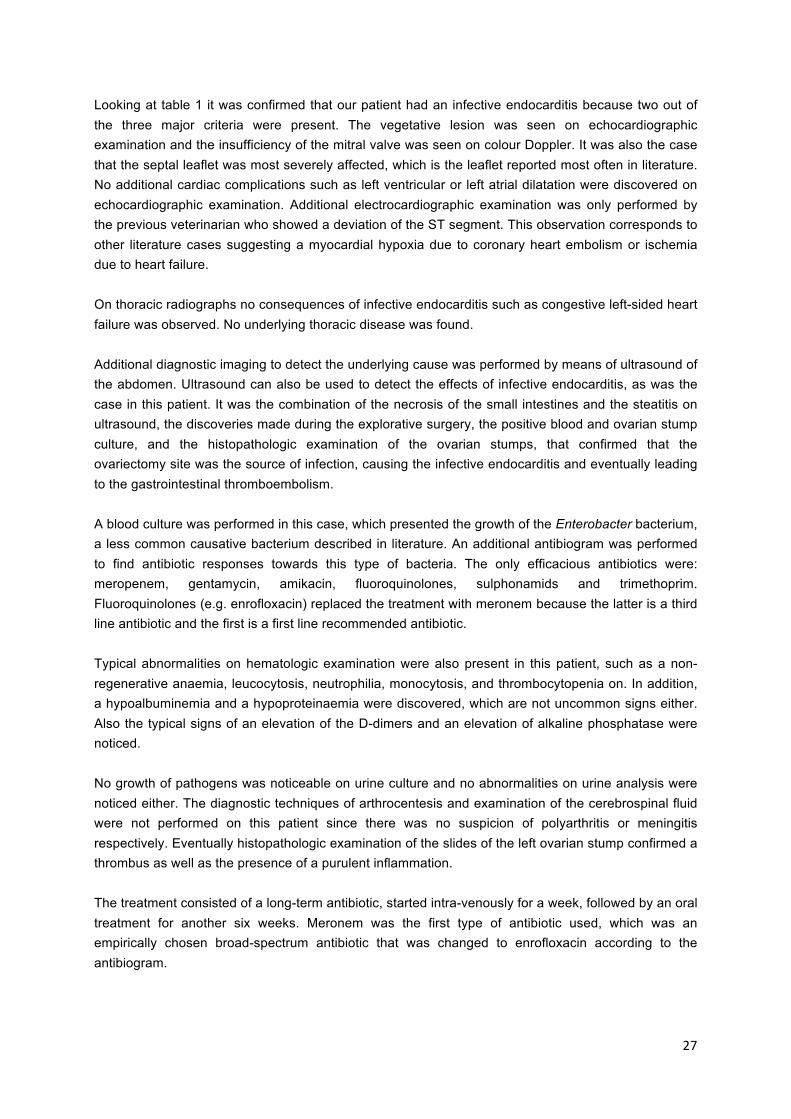
3.12. Prognosis The patient is still alive after two years and four months and is clinically stable. The systolic murmur, graded two out of six, remained, but no symptoms are noticed by the owners. The gastro-intestinal diet is still given. Nonetheless the shortened bowel does not cause any symptoms according to the owners. Due to these two observations it can be concluded that the prognosis of this dog is good and it will probably have a normal life span.
4. Discussion The signalment of this patient perfectly fitted the typical breed and weight category for infective endocarditis. Also the symptoms of lethargy, fever, fit into the list of signs that are seen in dogs with infective endocarditis. However, orthopaedic and neurologic symptoms were absent in this patient. Also the presence of a NEW systolic heart murmur with the point of maximum intensity at the level of mitral valve correlates to being one of the main clinical signs of infective endocarditis. Other cardiovascular abnormalities besides this murmur were not noticed.
27
Looking at table 1 it was confirmed that our patient had an infective endocarditis because two out of the three major criteria were present. The vegetative lesion was seen on echocardiographic examination and the insufficiency of the mitral valve was seen on colour Doppler. It was also the case that the septal leaflet was most severely affected, which is the leaflet reported most often in literature. No additional cardiac complications such as left ventricular or left atrial dilatation were discovered on echocardiographic examination. Additional electrocardiographic examination was only performed by the previous veterinarian who showed a deviation of the ST segment. This observation corresponds to other literature cases suggesting a myocardial hypoxia due to coronary heart embolism or ischemia due to heart failure. On thoracic radiographs no consequences of infective endocarditis such as congestive left-sided heart failure was observed. No underlying thoracic disease was found. Additional diagnostic imaging to detect the underlying cause was performed by means of ultrasound of the abdomen. Ultrasound can also be used to detect the effects of infective endocarditis, as was the case in this patient. It was the combination of the necrosis of the small intestines and the steatitis on ultrasound, the discoveries made during the explorative surgery, the positive blood and ovarian stump culture, and the histopathologic examination of the ovarian stumps, that confirmed that the ovariectomy site was the source of infection, causing the infective endocarditis and eventually leading to the gastrointestinal thromboembolism. A blood culture was performed in this case, which presented the growth of the Enterobacter bacterium, a less common causative bacterium described in literature. An additional antibiogram was performed to find antibiotic responses towards this type of bacteria. The only efficacious antibiotics were: meropenem, gentamycin, amikacin, fluoroquinolones, sulphonamids and trimethoprim. Fluoroquinolones (e.g. enrofloxacin) replaced the treatment with meronem because the latter is a third line antibiotic and the first is a first line recommended antibiotic. Typical abnormalities on hematologic examination were also present in this patient, such as a non-regenerative anaemia, leucocytosis, neutrophilia, monocytosis, and thrombocytopenia on. In addition, a hypoalbuminemia and a hypoproteinaemia were discovered, which are not uncommon signs either. Also the typical signs of an elevation of the D-dimers and an elevation of alkaline phosphatase were noticed. No growth of pathogens was noticeable on urine culture and no abnormalities on urine analysis were noticed either. The diagnostic techniques of arthrocentesis and examination of the cerebrospinal fluid were not performed on this patient since there was no suspicion of polyarthritis or meningitis respectively. Eventually histopathologic examination of the slides of the left ovarian stump confirmed a thrombus as well as the presence of a purulent inflammation. The treatment consisted of a long-term antibiotic, started intra-venously for a week, followed by an oral treatment for another six weeks. Meronem was the first type of antibiotic used, which was an empirically chosen broad-spectrum antibiotic that was changed to enrofloxacin according to the antibiogram.

28
Unfortunately, this patient developed one of the main complications that come along with an infective endocarditis, i.e. thromboembolism. There was a higher risk of this complication due to the big size of the vegetative mitral valve lesion. Despite this complication the dog is still alive after almost 2.5 years, which is a longer survival time than generally found in literature. The median survival time varies in literature from being 54 to 476 days, but the fact that this patient already survived more than 900 days proves that prolonged survival can be possible with adequate diagnostics and therapy. Additional blood culture two weeks after start of the antibiotic treatment and two weeks following termination of the antibiotic therapy were not performed for unknown reasons. However, the follow-up by means of echocardiographic examination was performed two weeks and six weeks after being presented at the clinic. Small vegetative lesions as well as a mild regurgitation were localised at the mitral valve, but had significantly decreased in size and severity. These observations confirm that efficacious antibiotic treatment was used. In conclusion, the bacteria presumably entered the bloodstream during the ovariectomy , causing a septicaemia, leading to colonization of the septal leaflet of the mitral valve. Another theory is that this bacterium could have been in the blood stream before the sterilisation, colonizing both the mitral valve and the ovarian stump, however in that case the initial route of bacterial entry is unclear. It is certain that there was an infective endocarditis, but whether the bacteria entered during ovariectomy or in another way cannot be fully elucidated. It is due to early diagnosis and aggressive long-term antibiotics treatment that this patient was saved.
References 1. Baddour LM, Wilson WR, Bayer AS, et al. IE: diagnosis, antimicrobial therapy, and
management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America. Circulation 2005;111:e394–434.
2. Bonagura B.D., Twedt D.C. (2014). Kirk’s Current Veterinary Therapy XV. St Louis: Saunders Elsevier, p. 291-e299.
3. Breitschwerdt E.B., Kordick D.L., Malarkey D.E., Keene B., Hadfield T.L., Wilson K. (1995). Endocarditis in a Dog Due to Infection with a Novel Bartonella Subspecies. Journal of Clinical Microbiology, 33 (1), 154-160.
4. Calvert C.A. (1982). Valvular bacterial endocarditis in the dog. Journal of the American Veterinary Medical Association 180, 1080-1084. Source: BSAVA Manuel of the Caine and Feline Cardiorespiraotory Medicine, 2nd edition (2010), ref. 3, p. 195.
5. Chomel B.B., MacDonald K.A., Kasten R.W., Chang C.C., Wey A.C., Foley J.E., Thomas W.P., Kittleson M.D. (2001). Aortic Valve Endocarditis in a Dog Due to Bartonella clarridgeiae. Journal of Clinical microbiology 39 (10), 3548-3554.
6. Chomel B.B., Kasten R.W., Williams C., Wey A.C., Henn J.B., Maggi R., Carrasco S., Mazet J., Boulois H.J., Maillard R., Breitschwerdt E.B. (2009). Bartonella endocarditis: a pathology shared by animal reservoirs and patients . Annals of the New York Academy of Sciences 1166, 120-126.
7. Cook L.B., Coates J.R., Dewey C.W., Gordon S., Miller M.W., Bahr A. (2005). Vascular Encephalopathy Associated With Bacterial Endocarditis in Four Dogs. Journal of the American Animal Hospital Association: 41 (4), 252-258.
29
8. De Bossche H., Roels S., Vanopdenbosch E. (2006). Verrucous valvular endocarditis due to Pasteurella multocida in a cat. Vlaams Diergeneeskundig Tijdschrift (in druk), 75, 457-460.
9. DeBowes L.J., Mosier D., Logan E., Harvey C.E., Lowry S., Richardson D.C. (1996). Association of periodontal disease and histological lesions in multiple organs from 45 dogs. Journal of Veterinary Dentistry, Published by the American Veterinary Dental Society, Volume 13, Number 2, June 1996.
10. Dunn M.E., Blond L., Letard D., DiFruscia R (2007). Hypertrophic osteopathy associated with infective endocarditis in an adult boxer dog. Journal of small animal practice 48, 99-103.
11. Ettinger S.J., Feldman E.C. (2010). Textbook of veterinary internal medicine, 7th edition, volume 2, Saunders Elsevier, St Louis, p. 490-496.
12. Glickman L.T., Glickman N.W., Moore G.E., Goldstein G.S., Lewis H.B. (2009). Evaluation of the risk of endocarditis and other cardiovascular events on the basis of the severity of periodontal disease in dogs. JAVMA 234 (4), 486-494.
13. Häggström J. (2010). Infective endocarditis. In: Fuentes V.L., Johnson L.R. and Dennis S. (Editors) BSAVA Manuel of Canine and Feline Cardiorespiratory Medicine, 2nd edition, British Small Animal Veterinary Association, Quedgeley, p. 195-199.
14. Junius G, Bavegems V., Stalpaert M., Binst D., Schrauwen E. (2004). Mitral Valve Endocarditis in a Labrador Retriever Caused by an Actinomyces Species Identified as Actinomyces turicensis. J Vet Intern Med 2004;18:899–901.
15. Kelly P., Rolain J.M., Maggi R., Sontakke S., Kenee B., Hunter S., Lepidi H., Breitschwerdt K.T., Breitschwerdt E.B., Raoult D. (2006). Bartonella quintana endocarditis in dogs. Emerging infectious diseases 12 (12), 1869-1872.
16. MacDonald K.A., Chomel B.B., Kittleson M.D., Kasten R.W., Thomas W.P., Pesavento P. (2004). A Prospective Study of Canine Infective Endocarditis in Northern California (1999–2001): Emergence of Bartonella as a Prevalent Etiologic Agent. Journal Veterinary Internal medicine 18, 56-64.
17. MacDonald, K.A. (2010). Infective endocarditis is dogs: diagnosis and therapy. Veterinary Clinics of North America: Small Animal Practice, 40, 665–684.
18. Peddle G., Sleeper M.M. (2007). Canine bacterial endocarditis: a review. American Animal Hospital Association, 43, 258-263.
19. Sisson D., Tomas W.P. (1984). Endocarditis of the aortic valve in the dog. American Veterinary Medical Association 184, 570-577. Source: BSAVA Manuel of the Caine and Feline Cardiorespiraotory Medicine, 2nd edition (2010), ref. 8, p. 195.
20. Sykes J.E., Kittleson M.D., Chomel B.B., MacDonald K.A., Pesavento P.A. (2006a). Clinicopathologic findings and outcome in dogs with Infective Endocarditis: 71 cases (1992-2005). JAVMA, Vol 228, No. 11, 1735-1747.
21. Sykes J.E., Kittleson M.D., Pesavento P.A., Byrne B.A., MacDonald K.A., Chomel B.B. (2006b). Evaluation of the relationship between causative organisms and clinical characteristics of infective endocarditis in dogs: 71 cases (1992–2005). JAVMA, 228 (11), 1723-1734.
22. Timian J., Yoshimoto S.K., Bruyette D.S. (2011). Extraskeletal osteosarcoma of the heart presenting as infective endocarditis. American animal hospital association 47 (2), 129-132.

GHENT UNIVERSITY
FACULTY OF VETERINARY MEDICINE
ACADEMIC YEAR 2015-2016
Case report: Misplaced microchip implantation in a puppy with fatal consequences
by
Janine Nathalie DE KONING
Promotors: Dr. Leen Van Brantegem Case report as part of the
Prof. Dr. Koen Chiers Master’s Dissertation

ii

iii
Disclaimer
Universiteit Gent, its employees and/or students, give no warranty that the information provided in this
thesis is accurate or exhaustive, nor that the content of this thesis will not constitute or result in any
infringement of third-party rights.
Universiteit Gent, its employees and/or students do not accept any liability or responsibility for any use
which may be made of the content or information given in the thesis, nor for any reliance which may
be placed on any advice or information provided in this thesis.

© 2016 Janine Nathalie de Koning
GHENT UNIVERSITY
FACULTY OF VETERINARY MEDICINE
ACADEMIC YEAR 2015-2016
Case report: Misplaced microchip implantation in a puppy with fatal consequences
by
Janine Nathalie DE KONING
Promotors: Dr. Leen Van Brantegem Case report as part of the
Prof. Dr. Koen Chiers Master’s Dissertation
i
Voorwoord
Allereerst wil ik graag mijn dank betuigen aan mijn promoter Dr. Leen Van Brantegem voor het
aanbieden van deze interessante casus en voor al haar hulp en inzet om deze masterproef tot een
mooi eind te brengen. Daarnaast wil ik ook mijn copromotor professor Koen Chiers bedanken.
Ook wil ik Astra Dhanijns bedanken voor het opsturen van de macroscopische beelden. Heel veel
dank wil ik betuigen aan Dr. David Davis voor het kritisch nakijken van mijn masterproef en het geven
van extra tips.
Daarnaast wil ik mijn ouders, Peter en Thea de Koning, bedanken voor het nakijken van mijn
masterproef en het geven van zowel emotionele als financiële support. Ten laatste wil ik mijn lief
Jeremy de Kok en al mijn vrienden bedanken voor de emotionele support. Dankzij jullie stond ik er niet
alleen voor in deze opleiding en was het een periode om met een goed gevoel naar terug te kijken.
ii
Table of contents
Abstract .................................................................................................................................................... 1
Samenvatting ........................................................................................................................................... 1
1. Introduction .......................................................................................................................................... 3
2. Literature.............................................................................................................................................. 4
2.1. General physical examination ...................................................................................................... 4
2.2. Neurological examination ............................................................................................................. 4
2.3. Specific examinations ................................................................................................................... 4
2.3.1. Radiology ............................................................................................................................... 4
2.3.2. Myelography .......................................................................................................................... 5
2.3.3. Computed tomography .......................................................................................................... 6
2.4 Differential diagnoses .................................................................................................................... 7
2.4.1. Respiratory dysfunction due to spinal cord injury .................................................................. 7
2.4.2. Brain-heart syndrome ............................................................................................................ 8
2.5. Surgery ......................................................................................................................................... 9
2.6. Magnetic resonance imaging...................................................................................................... 10
2.7. Therapy....................................................................................................................................... 10
2.8. Follow-up .................................................................................................................................... 11
2.9. Prognosis .................................................................................................................................... 11
2.10. Additional complications after microchip implantation .............................................................. 11
3. Clinical Case ...................................................................................................................................... 12
3.1. Signalment .................................................................................................................................. 12
3.2. Anamnesis .................................................................................................................................. 12
3.3. Problem list ................................................................................................................................. 12
3.4. Pathologic report ........................................................................................................................ 12
3.4.1. Macroscopic examination .................................................................................................... 12
3.4.2. Histopathologic examination................................................................................................ 14
3.4.3. Bacteriological examination ................................................................................................. 16
3.5. New problem list ......................................................................................................................... 16
3.6. Differential diagnoses ................................................................................................................. 17
3.6. Pathological end result ............................................................................................................... 18
4. Discussion ......................................................................................................................................... 19
References ............................................................................................................................................ 21
1
Abstract Keywords: microchip - spinal cord - brain-heart syndrome - dyspnoea – cardiac arrest
A Kooikerhondje puppy, aged six weeks, showed clinical signs of dyspnoea and a pale tongue five
minutes after microchip implantation. Shortly after these symptoms cardiac arrest followed, which was
fatal.
On macroscopic examination during necropsy several tissues and organs had a slightly pale
appearance. A mild dilatation of the right ventricle and serohaemorrhagic fluid in the pericardium were
present. The lungs were oedematic, congested and contained multifocal petechial haemorrhages.
Additional observations were frothy fluid in the trachea, starting from the bifurcation. There was also a
congestion of the meninges. But the most important discovery was a microchip protruding between the
third (C3) and fourth (C4) cervical vertebra after removal of the cervical musculature. The microchip
had penetrated the spinal cord and was perpendicularly positioned. Haemorrhages were found in the
cervical muscles, spine, and spinal cord due to the trauma induced by the pathway the microchip had
followed during insertion.
Histopathologic examination showed multifocal haemorrhages in the grey matter of the spinal cord
between C3 and C4. Additional congestion, obstructive atelectasis and protein-rich fluid in the lungs
were detected.
The pathological final diagnosis is fatality due to brain-heart syndrome following iatrogenic microchip
implantation in the spinal cord canal between C3 and C4 with acute trauma of the spinal cord. Another
differential diagnosis could be respiratory dysfunction due to interruption of the nervus phrenicus. This
could cause a paralysis of the inspiration and expiration musculature.
In the literature this is the first case reported in which a dog almost instantaneously dies upon the
procedure of implanting a microchip and in which the patient did not show any neurologic symptoms
either.
Samenvatting Kernwoorden: microchip – ruggenmerg – brain-heart syndroom - dyspnee – hartstilstand
Een Kooikerhondje puppy, van zes weken oud, vertoonde klinische symptomen van dyspnee en een
bleke tong vijf minuten nadat er een microchip was geplaatst. Kort nadat deze symptomen zich
voordeden, volgde een hartstilstand met fatale gevolgen.
Bij macroscopisch onderzoek tijdens de necropsie hadden verschillende weefsels en organen een
bleek aspect. Een milde dilatatie van het rechter ventrikel en serohemorrhagisch vocht in het pericard
waren aanwezig. De longen waren oedemateus, gestuwd en bevatten multifocale puntbloedingen.
Aanvullende waarnemingen waren spumeus vocht in de trachea, startend vanaf de bifurcatie.
Daarnaast waren er ook gestuwde hersenvliezen aanwezig. Maar nadat de nekspieren verwijderd
waren, was de meest belangrijke bevinding een uitstekende microchip tussen de derde en vierde
nekwervel. Deze microchip penetreerde het ruggenmerg en was loodrecht hierop gepositioneerd.
Bloedingen waren aanwezig ter hoogte van de nekspieren, de wervelkolom en het ruggenmerg als
gevolg van het trauma dat de microchip had veroorzaakt tijdens het implanteren ervan.
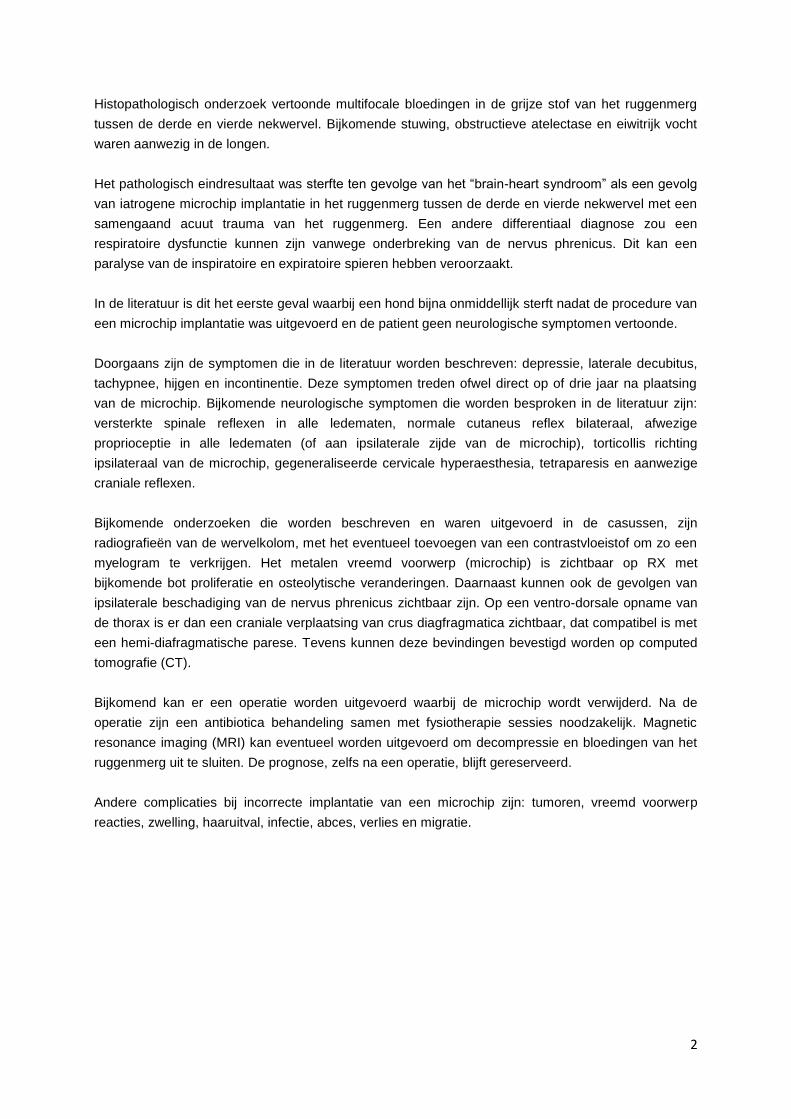
2
Histopathologisch onderzoek vertoonde multifocale bloedingen in de grijze stof van het ruggenmerg
tussen de derde en vierde nekwervel. Bijkomende stuwing, obstructieve atelectase en eiwitrijk vocht
waren aanwezig in de longen.
Het pathologisch eindresultaat was sterfte ten gevolge van het “brain-heart syndroom” als een gevolg
van iatrogene microchip implantatie in het ruggenmerg tussen de derde en vierde nekwervel met een
samengaand acuut trauma van het ruggenmerg. Een andere differentiaal diagnose zou een
respiratoire dysfunctie kunnen zijn vanwege onderbreking van de nervus phrenicus. Dit kan een
paralyse van de inspiratoire en expiratoire spieren hebben veroorzaakt.
In de literatuur is dit het eerste geval waarbij een hond bijna onmiddellijk sterft nadat de procedure van
een microchip implantatie was uitgevoerd en de patient geen neurologische symptomen vertoonde.
Doorgaans zijn de symptomen die in de literatuur worden beschreven: depressie, laterale decubitus,
tachypnee, hijgen en incontinentie. Deze symptomen treden ofwel direct op of drie jaar na plaatsing
van de microchip. Bijkomende neurologische symptomen die worden besproken in de literatuur zijn:
versterkte spinale reflexen in alle ledematen, normale cutaneus reflex bilateraal, afwezige
proprioceptie in alle ledematen (of aan ipsilaterale zijde van de microchip), torticollis richting
ipsilateraal van de microchip, gegeneraliseerde cervicale hyperaesthesia, tetraparesis en aanwezige
craniale reflexen.
Bijkomende onderzoeken die worden beschreven en waren uitgevoerd in de casussen, zijn
radiografieën van de wervelkolom, met het eventueel toevoegen van een contrastvloeistof om zo een
myelogram te verkrijgen. Het metalen vreemd voorwerp (microchip) is zichtbaar op RX met
bijkomende bot proliferatie en osteolytische veranderingen. Daarnaast kunnen ook de gevolgen van
ipsilaterale beschadiging van de nervus phrenicus zichtbaar zijn. Op een ventro-dorsale opname van
de thorax is er dan een craniale verplaatsing van crus diagfragmatica zichtbaar, dat compatibel is met
een hemi-diafragmatische parese. Tevens kunnen deze bevindingen bevestigd worden op computed
tomografie (CT).
Bijkomend kan er een operatie worden uitgevoerd waarbij de microchip wordt verwijderd. Na de
operatie zijn een antibiotica behandeling samen met fysiotherapie sessies noodzakelijk. Magnetic
resonance imaging (MRI) kan eventueel worden uitgevoerd om decompressie en bloedingen van het
ruggenmerg uit te sluiten. De prognose, zelfs na een operatie, blijft gereserveerd.
Andere complicaties bij incorrecte implantatie van een microchip zijn: tumoren, vreemd voorwerp
reacties, zwelling, haaruitval, infectie, abces, verlies en migratie.
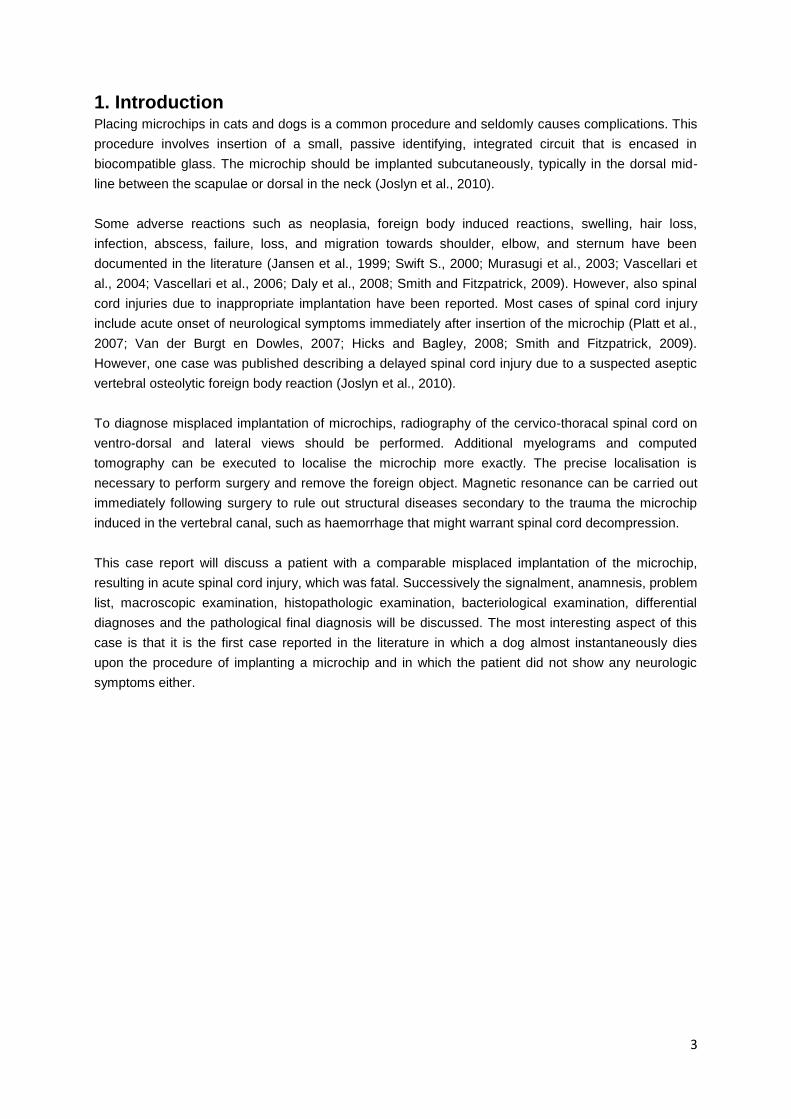
3
1. Introduction Placing microchips in cats and dogs is a common procedure and seldomly causes complications. This
procedure involves insertion of a small, passive identifying, integrated circuit that is encased in
biocompatible glass. The microchip should be implanted subcutaneously, typically in the dorsal mid-
line between the scapulae or dorsal in the neck (Joslyn et al., 2010).
Some adverse reactions such as neoplasia, foreign body induced reactions, swelling, hair loss,
infection, abscess, failure, loss, and migration towards shoulder, elbow, and sternum have been
documented in the literature (Jansen et al., 1999; Swift S., 2000; Murasugi et al., 2003; Vascellari et
al., 2004; Vascellari et al., 2006; Daly et al., 2008; Smith and Fitzpatrick, 2009). However, also spinal
cord injuries due to inappropriate implantation have been reported. Most cases of spinal cord injury
include acute onset of neurological symptoms immediately after insertion of the microchip (Platt et al.,
2007; Van der Burgt en Dowles, 2007; Hicks and Bagley, 2008; Smith and Fitzpatrick, 2009).
However, one case was published describing a delayed spinal cord injury due to a suspected aseptic
vertebral osteolytic foreign body reaction (Joslyn et al., 2010).
To diagnose misplaced implantation of microchips, radiography of the cervico-thoracal spinal cord on
ventro-dorsal and lateral views should be performed. Additional myelograms and computed
tomography can be executed to localise the microchip more exactly. The precise localisation is
necessary to perform surgery and remove the foreign object. Magnetic resonance can be carried out
immediately following surgery to rule out structural diseases secondary to the trauma the microchip
induced in the vertebral canal, such as haemorrhage that might warrant spinal cord decompression.
This case report will discuss a patient with a comparable misplaced implantation of the microchip,
resulting in acute spinal cord injury, which was fatal. Successively the signalment, anamnesis, problem
list, macroscopic examination, histopathologic examination, bacteriological examination, differential
diagnoses and the pathological final diagnosis will be discussed. The most interesting aspect of this
case is that it is the first case reported in the literature in which a dog almost instantaneously dies
upon the procedure of implanting a microchip and in which the patient did not show any neurologic
symptoms either.
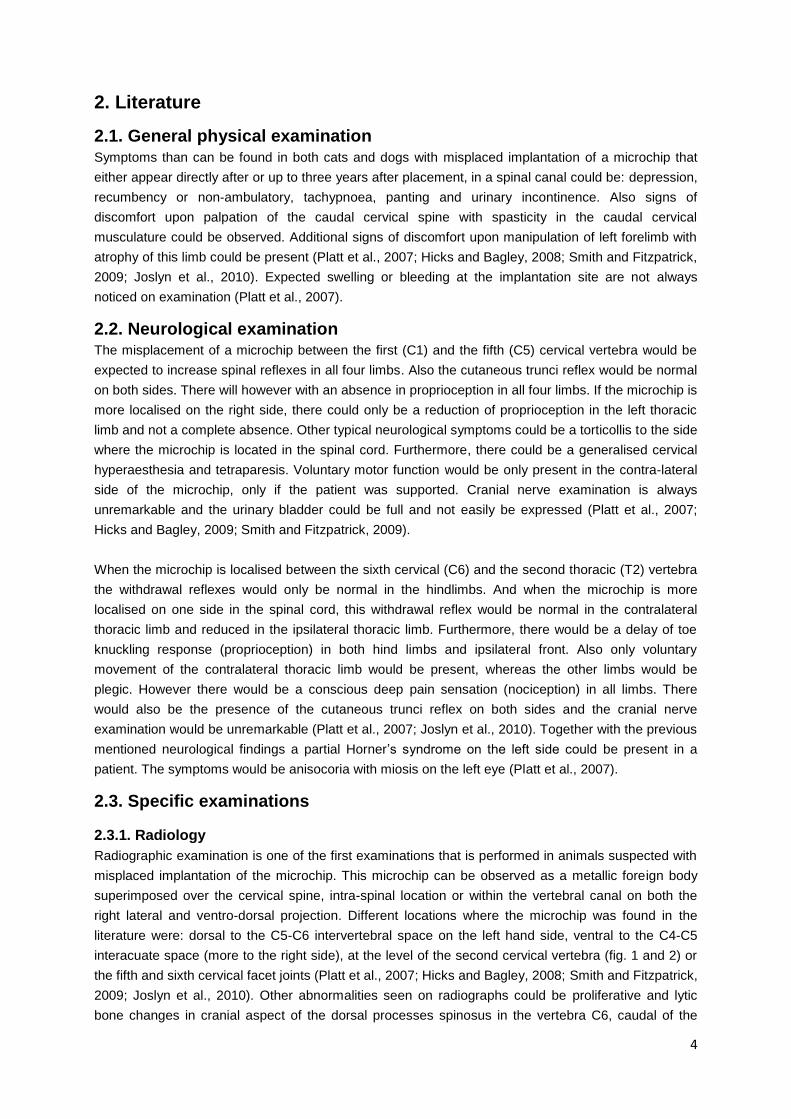
4
2. Literature
2.1. General physical examination Symptoms than can be found in both cats and dogs with misplaced implantation of a microchip that
either appear directly after or up to three years after placement, in a spinal canal could be: depression,
recumbency or non-ambulatory, tachypnoea, panting and urinary incontinence. Also signs of
discomfort upon palpation of the caudal cervical spine with spasticity in the caudal cervical
musculature could be observed. Additional signs of discomfort upon manipulation of left forelimb with
atrophy of this limb could be present (Platt et al., 2007; Hicks and Bagley, 2008; Smith and Fitzpatrick,
2009; Joslyn et al., 2010). Expected swelling or bleeding at the implantation site are not always
noticed on examination (Platt et al., 2007).
2.2. Neurological examination The misplacement of a microchip between the first (C1) and the fifth (C5) cervical vertebra would be
expected to increase spinal reflexes in all four limbs. Also the cutaneous trunci reflex would be normal
on both sides. There will however with an absence in proprioception in all four limbs. If the microchip is
more localised on the right side, there could only be a reduction of proprioception in the left thoracic
limb and not a complete absence. Other typical neurological symptoms could be a torticollis to the side
where the microchip is located in the spinal cord. Furthermore, there could be a generalised cervical
hyperaesthesia and tetraparesis. Voluntary motor function would be only present in the contra-lateral
side of the microchip, only if the patient was supported. Cranial nerve examination is always
unremarkable and the urinary bladder could be full and not easily be expressed (Platt et al., 2007;
Hicks and Bagley, 2009; Smith and Fitzpatrick, 2009).
When the microchip is localised between the sixth cervical (C6) and the second thoracic (T2) vertebra
the withdrawal reflexes would only be normal in the hindlimbs. And when the microchip is more
localised on one side in the spinal cord, this withdrawal reflex would be normal in the contralateral
thoracic limb and reduced in the ipsilateral thoracic limb. Furthermore, there would be a delay of toe
knuckling response (proprioception) in both hind limbs and ipsilateral front. Also only voluntary
movement of the contralateral thoracic limb would be present, whereas the other limbs would be
plegic. However there would be a conscious deep pain sensation (nociception) in all limbs. There
would also be the presence of the cutaneous trunci reflex on both sides and the cranial nerve
examination would be unremarkable (Platt et al., 2007; Joslyn et al., 2010). Together with the previous
mentioned neurological findings a partial Horner’s syndrome on the left side could be present in a
patient. The symptoms would be anisocoria with miosis on the left eye (Platt et al., 2007).
2.3. Specific examinations
2.3.1. Radiology
Radiographic examination is one of the first examinations that is performed in animals suspected with
misplaced implantation of the microchip. This microchip can be observed as a metallic foreign body
superimposed over the cervical spine, intra-spinal location or within the vertebral canal on both the
right lateral and ventro-dorsal projection. Different locations where the microchip was found in the
literature were: dorsal to the C5-C6 intervertebral space on the left hand side, ventral to the C4-C5
interacuate space (more to the right side), at the level of the second cervical vertebra (fig. 1 and 2) or
the fifth and sixth cervical facet joints (Platt et al., 2007; Hicks and Bagley, 2008; Smith and Fitzpatrick,
2009; Joslyn et al., 2010). Other abnormalities seen on radiographs could be proliferative and lytic
bone changes in cranial aspect of the dorsal processes spinosus in the vertebra C6, caudal of the
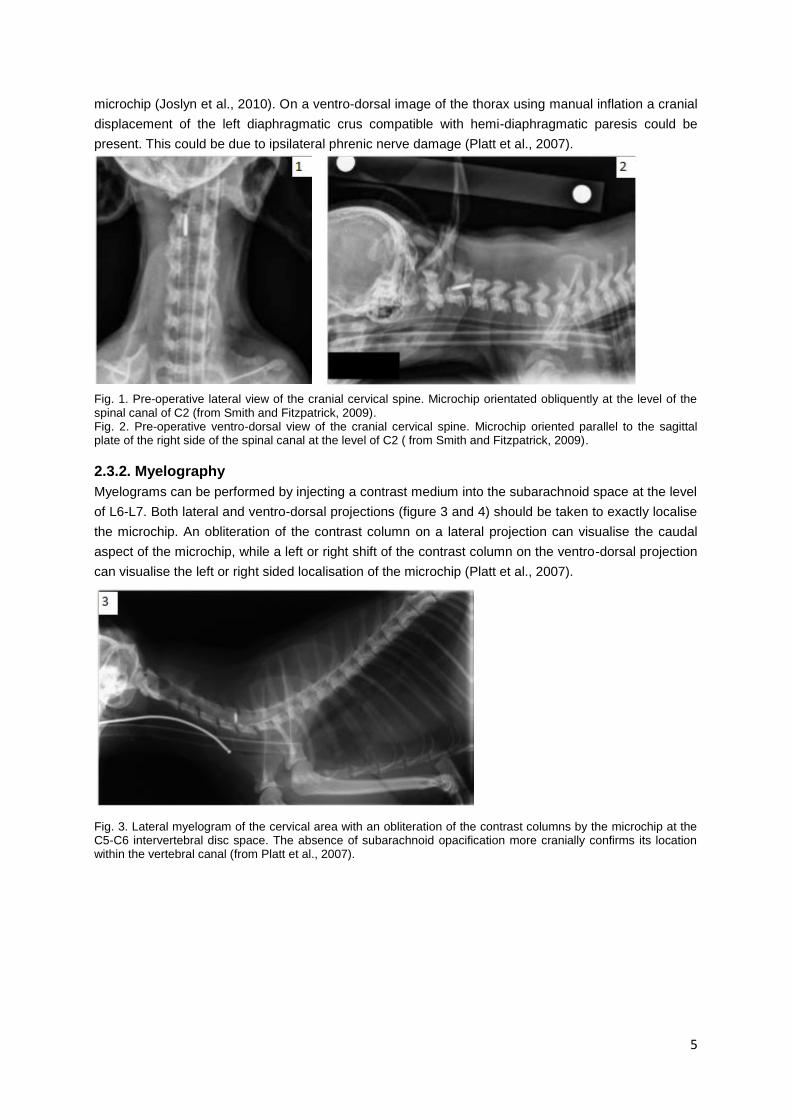
5
microchip (Joslyn et al., 2010). On a ventro-dorsal image of the thorax using manual inflation a cranial
displacement of the left diaphragmatic crus compatible with hemi-diaphragmatic paresis could be
present. This could be due to ipsilateral phrenic nerve damage (Platt et al., 2007).
Fig. 1. Pre-operative lateral view of the cranial cervical spine. Microchip orientated obliquently at the level of the spinal canal of C2 (from Smith and Fitzpatrick, 2009). Fig. 2. Pre-operative ventro-dorsal view of the cranial cervical spine. Microchip oriented parallel to the sagittal plate of the right side of the spinal canal at the level of C2 ( from Smith and Fitzpatrick, 2009).
2.3.2. Myelography
Myelograms can be performed by injecting a contrast medium into the subarachnoid space at the level
of L6-L7. Both lateral and ventro-dorsal projections (figure 3 and 4) should be taken to exactly localise
the microchip. An obliteration of the contrast column on a lateral projection can visualise the caudal
aspect of the microchip, while a left or right shift of the contrast column on the ventro-dorsal projection
can visualise the left or right sided localisation of the microchip (Platt et al., 2007).
Fig. 3. Lateral myelogram of the cervical area with an obliteration of the contrast columns by the microchip at the C5-C6 intervertebral disc space. The absence of subarachnoid opacification more cranially confirms its location within the vertebral canal (from Platt et al., 2007).

6
Fig. 4. Ventro-dorsal myelogram of the cervical region where there is a slight lateral shift of the right contrast column and attenuation of the left side by the microchip . This confirms the left sided localisation of the microchip. (from Platt et al., 2007).
2.3.3. Computed tomography
Computed tomography (CT) can be performed to identify the exact location of the foreign body. A
bone algorithm and one millimetre axial contiguous slices are the best option according to Joslyn et
al., (2010). The microchip can be identified on CT as a hyperattenuating metallic foreign body. Both
lateral as well as cranial and dorsal projections may be required (fig. 5, 6 and 7). The main reason for
taking the CT was to see the exact location of the microchip with the vertebral canal and so plan
surgery and to assess the caudal cervical vertebrae (Joslyn et al., 2010).
Fig. 5. Volume-rendered, 3D, right lateral projection of the CT study of the caudal cervical vertebrae. The microchip is marked with a white arrow and can be encroached on the left dorsolateral vertebral canal in the region of the left lamina of C6. The right aspect of the spinal column has been digitally removed showing the tip of the microchip projecting into the vertebral canal. C6 is identified by the ventral tubercle (from Joslyn et al., 2010).
Fig. 6. Volume-rendered, 3D, cranial projection of the CT study of C6. The image shows the foreign body (arrow) protruding into the vertebral canal through a caudo-lateral trajectory (from Joslyn et al., 2010).
Fig. 7. Volume-rendered, 3D, dorsal projection of the CT study of C6. The ventral aspect of the vertebral body has been cropped, and the foreign body has been omitted based on its density, showing only the dorsal aspect of the vertebra. Note the asymmetry of the cranial lamina with deficits on the left aspect (osteolysis) (from Joslyn et al., 2010).
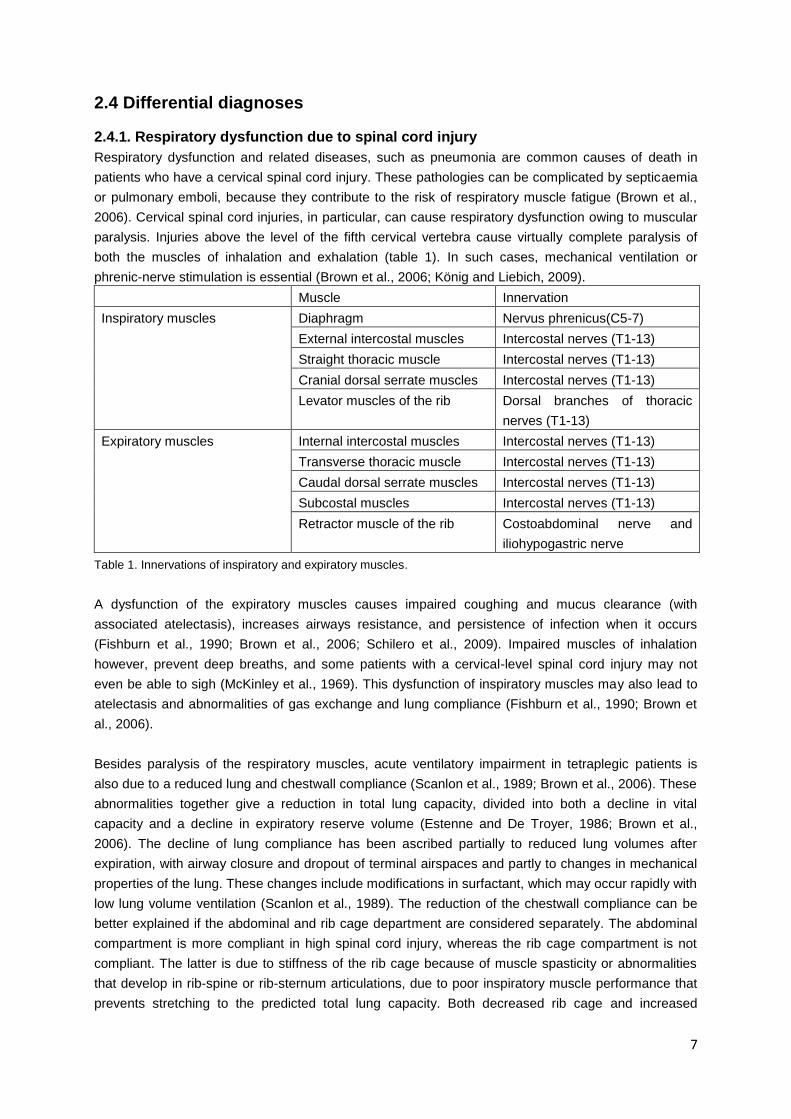
7
2.4 Differential diagnoses
2.4.1. Respiratory dysfunction due to spinal cord injury
Respiratory dysfunction and related diseases, such as pneumonia are common causes of death in
patients who have a cervical spinal cord injury. These pathologies can be complicated by septicaemia
or pulmonary emboli, because they contribute to the risk of respiratory muscle fatigue (Brown et al.,
2006). Cervical spinal cord injuries, in particular, can cause respiratory dysfunction owing to muscular
paralysis. Injuries above the level of the fifth cervical vertebra cause virtually complete paralysis of
both the muscles of inhalation and exhalation (table 1). In such cases, mechanical ventilation or
phrenic-nerve stimulation is essential (Brown et al., 2006; König and Liebich, 2009).
Muscle Innervation
Inspiratory muscles Diaphragm Nervus phrenicus(C5-7)
External intercostal muscles Intercostal nerves (T1-13)
Straight thoracic muscle Intercostal nerves (T1-13)
Cranial dorsal serrate muscles Intercostal nerves (T1-13)
Levator muscles of the rib Dorsal branches of thoracic
nerves (T1-13)
Expiratory muscles Internal intercostal muscles Intercostal nerves (T1-13)
Transverse thoracic muscle Intercostal nerves (T1-13)
Caudal dorsal serrate muscles Intercostal nerves (T1-13)
Subcostal muscles Intercostal nerves (T1-13)
Retractor muscle of the rib Costoabdominal nerve and
iliohypogastric nerve
Table 1. Innervations of inspiratory and expiratory muscles.
A dysfunction of the expiratory muscles causes impaired coughing and mucus clearance (with
associated atelectasis), increases airways resistance, and persistence of infection when it occurs
(Fishburn et al., 1990; Brown et al., 2006; Schilero et al., 2009). Impaired muscles of inhalation
however, prevent deep breaths, and some patients with a cervical-level spinal cord injury may not
even be able to sigh (McKinley et al., 1969). This dysfunction of inspiratory muscles may also lead to
atelectasis and abnormalities of gas exchange and lung compliance (Fishburn et al., 1990; Brown et
al., 2006).
Besides paralysis of the respiratory muscles, acute ventilatory impairment in tetraplegic patients is
also due to a reduced lung and chestwall compliance (Scanlon et al., 1989; Brown et al., 2006). These
abnormalities together give a reduction in total lung capacity, divided into both a decline in vital
capacity and a decline in expiratory reserve volume (Estenne and De Troyer, 1986; Brown et al.,
2006). The decline of lung compliance has been ascribed partially to reduced lung volumes after
expiration, with airway closure and dropout of terminal airspaces and partly to changes in mechanical
properties of the lung. These changes include modifications in surfactant, which may occur rapidly with
low lung volume ventilation (Scanlon et al., 1989). The reduction of the chestwall compliance can be
better explained if the abdominal and rib cage department are considered separately. The abdominal
compartment is more compliant in high spinal cord injury, whereas the rib cage compartment is not
compliant. The latter is due to stiffness of the rib cage because of muscle spasticity or abnormalities
that develop in rib-spine or rib-sternum articulations, due to poor inspiratory muscle performance that
prevents stretching to the predicted total lung capacity. Both decreased rib cage and increased
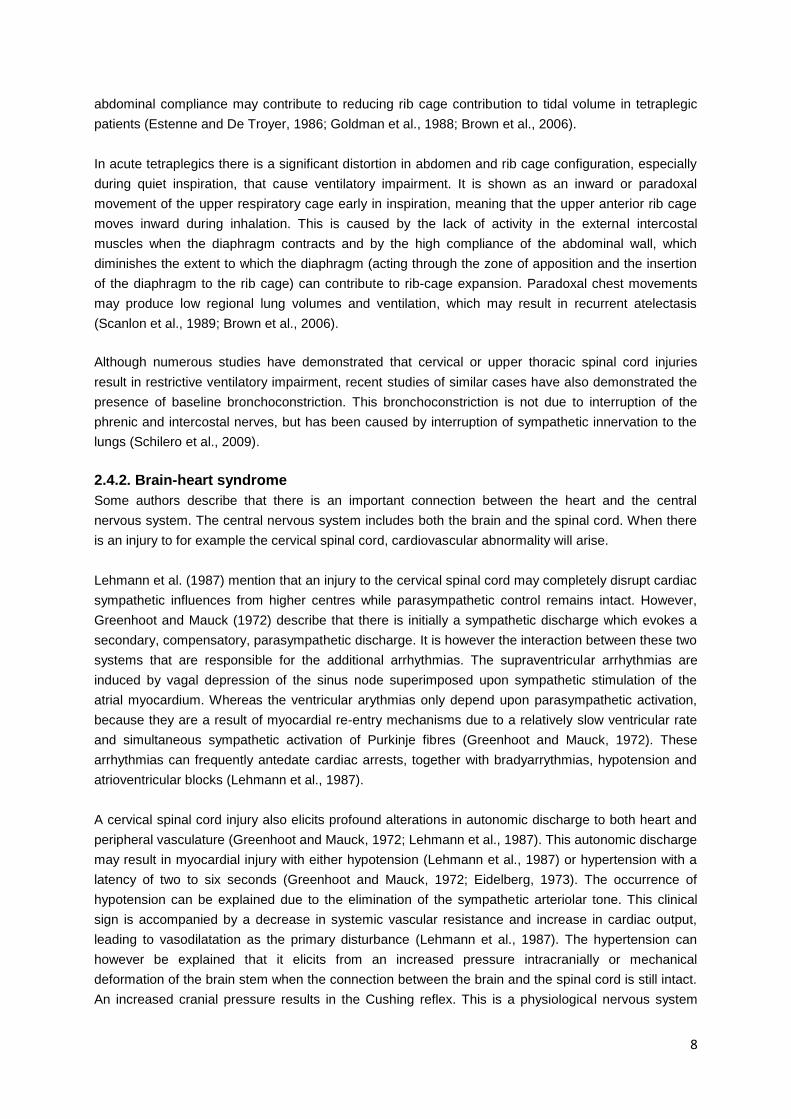
8
abdominal compliance may contribute to reducing rib cage contribution to tidal volume in tetraplegic
patients (Estenne and De Troyer, 1986; Goldman et al., 1988; Brown et al., 2006).
In acute tetraplegics there is a significant distortion in abdomen and rib cage configuration, especially
during quiet inspiration, that cause ventilatory impairment. It is shown as an inward or paradoxal
movement of the upper respiratory cage early in inspiration, meaning that the upper anterior rib cage
moves inward during inhalation. This is caused by the lack of activity in the external intercostal
muscles when the diaphragm contracts and by the high compliance of the abdominal wall, which
diminishes the extent to which the diaphragm (acting through the zone of apposition and the insertion
of the diaphragm to the rib cage) can contribute to rib-cage expansion. Paradoxal chest movements
may produce low regional lung volumes and ventilation, which may result in recurrent atelectasis
(Scanlon et al., 1989; Brown et al., 2006).
Although numerous studies have demonstrated that cervical or upper thoracic spinal cord injuries
result in restrictive ventilatory impairment, recent studies of similar cases have also demonstrated the
presence of baseline bronchoconstriction. This bronchoconstriction is not due to interruption of the
phrenic and intercostal nerves, but has been caused by interruption of sympathetic innervation to the
lungs (Schilero et al., 2009).
2.4.2. Brain-heart syndrome
Some authors describe that there is an important connection between the heart and the central
nervous system. The central nervous system includes both the brain and the spinal cord. When there
is an injury to for example the cervical spinal cord, cardiovascular abnormality will arise.
Lehmann et al. (1987) mention that an injury to the cervical spinal cord may completely disrupt cardiac
sympathetic influences from higher centres while parasympathetic control remains intact. However,
Greenhoot and Mauck (1972) describe that there is initially a sympathetic discharge which evokes a
secondary, compensatory, parasympathetic discharge. It is however the interaction between these two
systems that are responsible for the additional arrhythmias. The supraventricular arrhythmias are
induced by vagal depression of the sinus node superimposed upon sympathetic stimulation of the
atrial myocardium. Whereas the ventricular arythmias only depend upon parasympathetic activation,
because they are a result of myocardial re-entry mechanisms due to a relatively slow ventricular rate
and simultaneous sympathetic activation of Purkinje fibres (Greenhoot and Mauck, 1972). These
arrhythmias can frequently antedate cardiac arrests, together with bradyarrythmias, hypotension and
atrioventricular blocks (Lehmann et al., 1987).
A cervical spinal cord injury also elicits profound alterations in autonomic discharge to both heart and
peripheral vasculature (Greenhoot and Mauck, 1972; Lehmann et al., 1987). This autonomic discharge
may result in myocardial injury with either hypotension (Lehmann et al., 1987) or hypertension with a
latency of two to six seconds (Greenhoot and Mauck, 1972; Eidelberg, 1973). The occurrence of
hypotension can be explained due to the elimination of the sympathetic arteriolar tone. This clinical
sign is accompanied by a decrease in systemic vascular resistance and increase in cardiac output,
leading to vasodilatation as the primary disturbance (Lehmann et al., 1987). The hypertension can
however be explained that it elicits from an increased pressure intracranially or mechanical
deformation of the brain stem when the connection between the brain and the spinal cord is still intact.
An increased cranial pressure results in the Cushing reflex. This is a physiological nervous system

9
response that gives hypertension, irregular breathing and bradycardia (Eidelberg, 1973). These
hypertensions result in rotation of the heart electrical axis and prominent ventricular ectopic beats
(Eidelberg, 1973).
Besides these cardiovascular abnormalities, a compression of the spinal cord may also result in sinus
tachycardia, followed by sinus pauses, shifting sinus pacemaker, nodal escape beats, brief runs of
atrial fibrillation, multifocal ventricular premature contractions, ventricular tachycardia, and S-T and T
wave changes (Greenhoot and Mauck, 1972). However, Lehmann et al. (1987) and Eidelberg (1973)
describe the occurrence of bradycardia instead of the earlier mentioned tachycardia.
Furthermore, a modest rise in serum glutamic oxalacetic transaminase can be observed in patients,
because it is consistent with subendocardial ischaemia (Greenhoot and Mauck, 1972).
2.5. Surgery Misplaced microchips can be removed surgically. The patient should be positioned in sternal
recumbence with the neck in mild ventroflexion and the head supported for surgical procedures. A
dorsal approach with a dorsal laminectomy of the cervical vertebral column should be performed to
allow locating and removing the microchip as well as gross assessment of the spinal cord, associated
meninges and decompression. An approach to the cranial cervical column is advised if the microchip
is located between C2 and C3, to the mid-cervical vertebral column if between C4 and C5 (fig. 8), and
to the caudal cervical spine if between C5 and C6. If the microchip is located more on the right side or
the left side a hemi-laminectomy in the left, respectively right lamina, should be performed after a
dorsal mid-line incision. Gentle traction should applied to the microchip with a mosquito forceps to be
able to remove it. After removal of the microchip a pedicle-free fat graft or an absorbable gelatine
sponge should be placed over the puncture wound at the location of the microchip extraction in the
spinal cord. The incision should be closed routinely (Platt et al., 2007; Hicks and Bagley, 2008; Smith
and Fitzpatrick, 2009; Joslyn et al., 2010).
In the case described by Platt et al. (2007) no dural pathology or extra-dural haemorrhage was
noticed, whereas in the case of Smith and Fitzpatrick (2009) there was a significant haemorrhage
noted while removing the microchip. This difference could be explained by either a different insertion
trajectory and associated pattern of vascular damage during initial implantation, or the increased
vascular plexus in the more cranial location in the cervical spinal canal. The bleeding was however
controlled with a topical placement of bovine collagen under light pressure.
Fig. 8. Intra-operative view after a dorsal approach to the mid-cervical spine. The tip of the microchip is seen protruding from the vertebral column and associated muscle (from Hicks and Bagley, 2008).
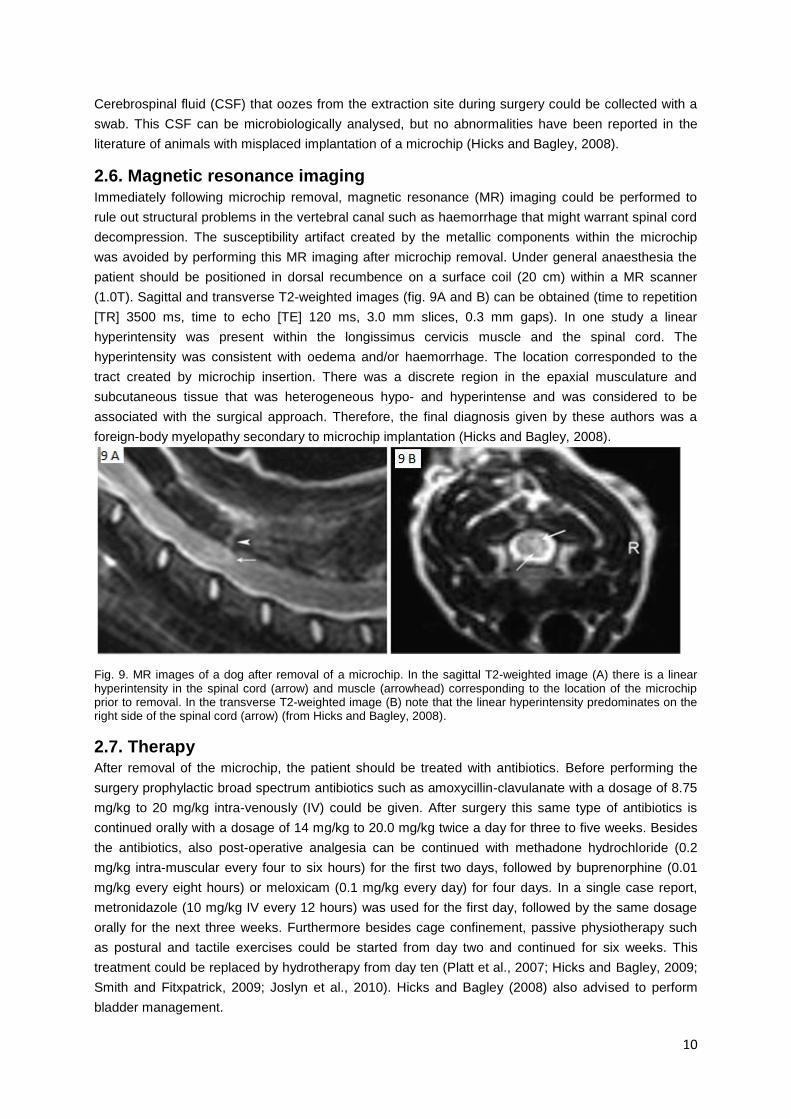
10
Cerebrospinal fluid (CSF) that oozes from the extraction site during surgery could be collected with a
swab. This CSF can be microbiologically analysed, but no abnormalities have been reported in the
literature of animals with misplaced implantation of a microchip (Hicks and Bagley, 2008).
2.6. Magnetic resonance imaging Immediately following microchip removal, magnetic resonance (MR) imaging could be performed to
rule out structural problems in the vertebral canal such as haemorrhage that might warrant spinal cord
decompression. The susceptibility artifact created by the metallic components within the microchip
was avoided by performing this MR imaging after microchip removal. Under general anaesthesia the
patient should be positioned in dorsal recumbence on a surface coil (20 cm) within a MR scanner
(1.0T). Sagittal and transverse T2-weighted images (fig. 9A and B) can be obtained (time to repetition
[TR] 3500 ms, time to echo [TE] 120 ms, 3.0 mm slices, 0.3 mm gaps). In one study a linear
hyperintensity was present within the longissimus cervicis muscle and the spinal cord. The
hyperintensity was consistent with oedema and/or haemorrhage. The location corresponded to the
tract created by microchip insertion. There was a discrete region in the epaxial musculature and
subcutaneous tissue that was heterogeneous hypo- and hyperintense and was considered to be
associated with the surgical approach. Therefore, the final diagnosis given by these authors was a
foreign-body myelopathy secondary to microchip implantation (Hicks and Bagley, 2008).
Fig. 9. MR images of a dog after removal of a microchip. In the sagittal T2-weighted image (A) there is a linear hyperintensity in the spinal cord (arrow) and muscle (arrowhead) corresponding to the location of the microchip prior to removal. In the transverse T2-weighted image (B) note that the linear hyperintensity predominates on the right side of the spinal cord (arrow) (from Hicks and Bagley, 2008).
2.7. Therapy After removal of the microchip, the patient should be treated with antibiotics. Before performing the
surgery prophylactic broad spectrum antibiotics such as amoxycillin-clavulanate with a dosage of 8.75
mg/kg to 20 mg/kg intra-venously (IV) could be given. After surgery this same type of antibiotics is
continued orally with a dosage of 14 mg/kg to 20.0 mg/kg twice a day for three to five weeks. Besides
the antibiotics, also post-operative analgesia can be continued with methadone hydrochloride (0.2
mg/kg intra-muscular every four to six hours) for the first two days, followed by buprenorphine (0.01
mg/kg every eight hours) or meloxicam (0.1 mg/kg every day) for four days. In a single case report,
metronidazole (10 mg/kg IV every 12 hours) was used for the first day, followed by the same dosage
orally for the next three weeks. Furthermore besides cage confinement, passive physiotherapy such
as postural and tactile exercises could be started from day two and continued for six weeks. This
treatment could be replaced by hydrotherapy from day ten (Platt et al., 2007; Hicks and Bagley, 2009;
Smith and Fitxpatrick, 2009; Joslyn et al., 2010). Hicks and Bagley (2008) also advised to perform
bladder management.
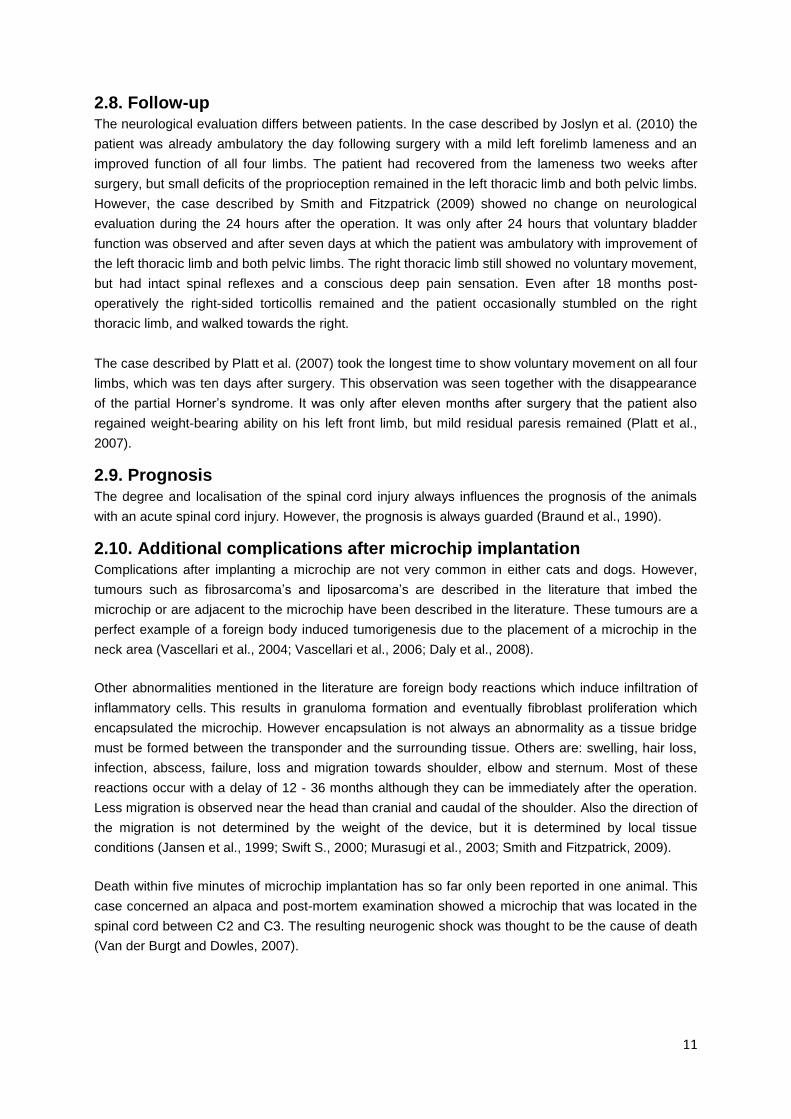
11
2.8. Follow-up The neurological evaluation differs between patients. In the case described by Joslyn et al. (2010) the
patient was already ambulatory the day following surgery with a mild left forelimb lameness and an
improved function of all four limbs. The patient had recovered from the lameness two weeks after
surgery, but small deficits of the proprioception remained in the left thoracic limb and both pelvic limbs.
However, the case described by Smith and Fitzpatrick (2009) showed no change on neurological
evaluation during the 24 hours after the operation. It was only after 24 hours that voluntary bladder
function was observed and after seven days at which the patient was ambulatory with improvement of
the left thoracic limb and both pelvic limbs. The right thoracic limb still showed no voluntary movement,
but had intact spinal reflexes and a conscious deep pain sensation. Even after 18 months post-
operatively the right-sided torticollis remained and the patient occasionally stumbled on the right
thoracic limb, and walked towards the right.
The case described by Platt et al. (2007) took the longest time to show voluntary movement on all four
limbs, which was ten days after surgery. This observation was seen together with the disappearance
of the partial Horner’s syndrome. It was only after eleven months after surgery that the patient also
regained weight-bearing ability on his left front limb, but mild residual paresis remained (Platt et al.,
2007).
2.9. Prognosis The degree and localisation of the spinal cord injury always influences the prognosis of the animals
with an acute spinal cord injury. However, the prognosis is always guarded (Braund et al., 1990).
2.10. Additional complications after microchip implantation Complications after implanting a microchip are not very common in either cats and dogs. However,
tumours such as fibrosarcoma’s and liposarcoma’s are described in the literature that imbed the
microchip or are adjacent to the microchip have been described in the literature. These tumours are a
perfect example of a foreign body induced tumorigenesis due to the placement of a microchip in the
neck area (Vascellari et al., 2004; Vascellari et al., 2006; Daly et al., 2008).
Other abnormalities mentioned in the literature are foreign body reactions which induce infiltration of
inflammatory cells. This results in granuloma formation and eventually fibroblast proliferation which
encapsulated the microchip. However encapsulation is not always an abnormality as a tissue bridge
must be formed between the transponder and the surrounding tissue. Others are: swelling, hair loss,
infection, abscess, failure, loss and migration towards shoulder, elbow and sternum. Most of these
reactions occur with a delay of 12 - 36 months although they can be immediately after the operation.
Less migration is observed near the head than cranial and caudal of the shoulder. Also the direction of
the migration is not determined by the weight of the device, but it is determined by local tissue
conditions (Jansen et al., 1999; Swift S., 2000; Murasugi et al., 2003; Smith and Fitzpatrick, 2009).
Death within five minutes of microchip implantation has so far only been reported in one animal. This
case concerned an alpaca and post-mortem examination showed a microchip that was located in the
spinal cord between C2 and C3. The resulting neurogenic shock was thought to be the cause of death
(Van der Burgt and Dowles, 2007).
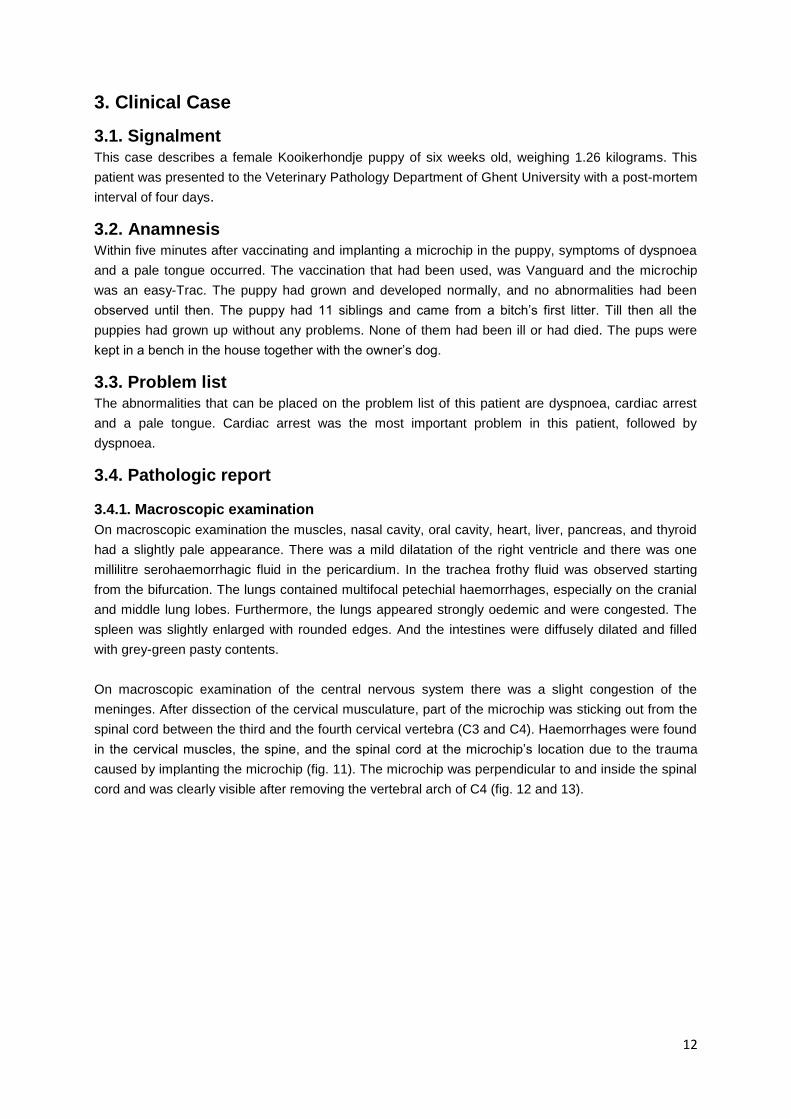
12
3. Clinical Case
3.1. Signalment This case describes a female Kooikerhondje puppy of six weeks old, weighing 1.26 kilograms. This
patient was presented to the Veterinary Pathology Department of Ghent University with a post-mortem
interval of four days.
3.2. Anamnesis Within five minutes after vaccinating and implanting a microchip in the puppy, symptoms of dyspnoea
and a pale tongue occurred. The vaccination that had been used, was Vanguard and the microchip
was an easy-Trac. The puppy had grown and developed normally, and no abnormalities had been
observed until then. The puppy had 11 siblings and came from a bitch’s first litter. Till then all the
puppies had grown up without any problems. None of them had been ill or had died. The pups were
kept in a bench in the house together with the owner’s dog.
3.3. Problem list The abnormalities that can be placed on the problem list of this patient are dyspnoea, cardiac arrest
and a pale tongue. Cardiac arrest was the most important problem in this patient, followed by
dyspnoea.
3.4. Pathologic report
3.4.1. Macroscopic examination
On macroscopic examination the muscles, nasal cavity, oral cavity, heart, liver, pancreas, and thyroid
had a slightly pale appearance. There was a mild dilatation of the right ventricle and there was one
millilitre serohaemorrhagic fluid in the pericardium. In the trachea frothy fluid was observed starting
from the bifurcation. The lungs contained multifocal petechial haemorrhages, especially on the cranial
and middle lung lobes. Furthermore, the lungs appeared strongly oedemic and were congested. The
spleen was slightly enlarged with rounded edges. And the intestines were diffusely dilated and filled
with grey-green pasty contents.
On macroscopic examination of the central nervous system there was a slight congestion of the
meninges. After dissection of the cervical musculature, part of the microchip was sticking out from the
spinal cord between the third and the fourth cervical vertebra (C3 and C4). Haemorrhages were found
in the cervical muscles, the spine, and the spinal cord at the microchip’s location due to the trauma
caused by implanting the microchip (fig. 11). The microchip was perpendicular to and inside the spinal
cord and was clearly visible after removing the vertebral arch of C4 (fig. 12 and 13).
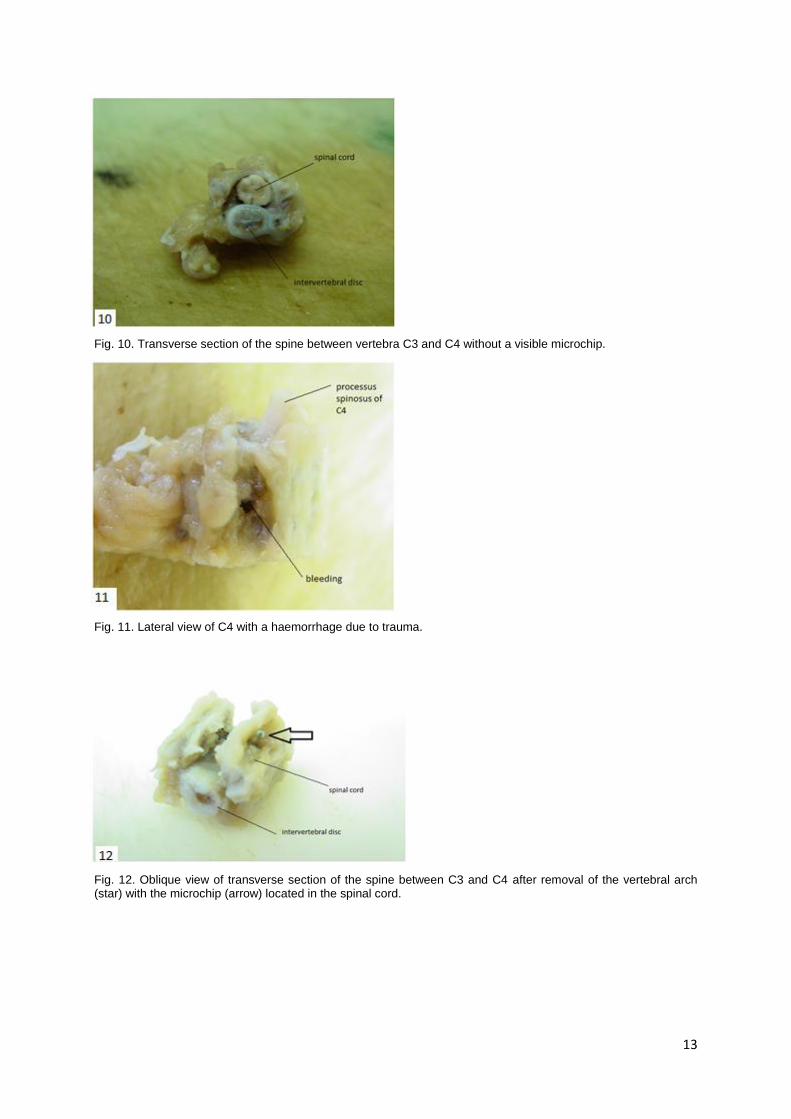
13
Fig. 10. Transverse section of the spine between vertebra C3 and C4 without a visible microchip.
Fig. 11. Lateral view of C4 with a haemorrhage due to trauma.
Fig. 12. Oblique view of transverse section of the spine between C3 and C4 after removal of the vertebral arch (star) with the microchip (arrow) located in the spinal cord.
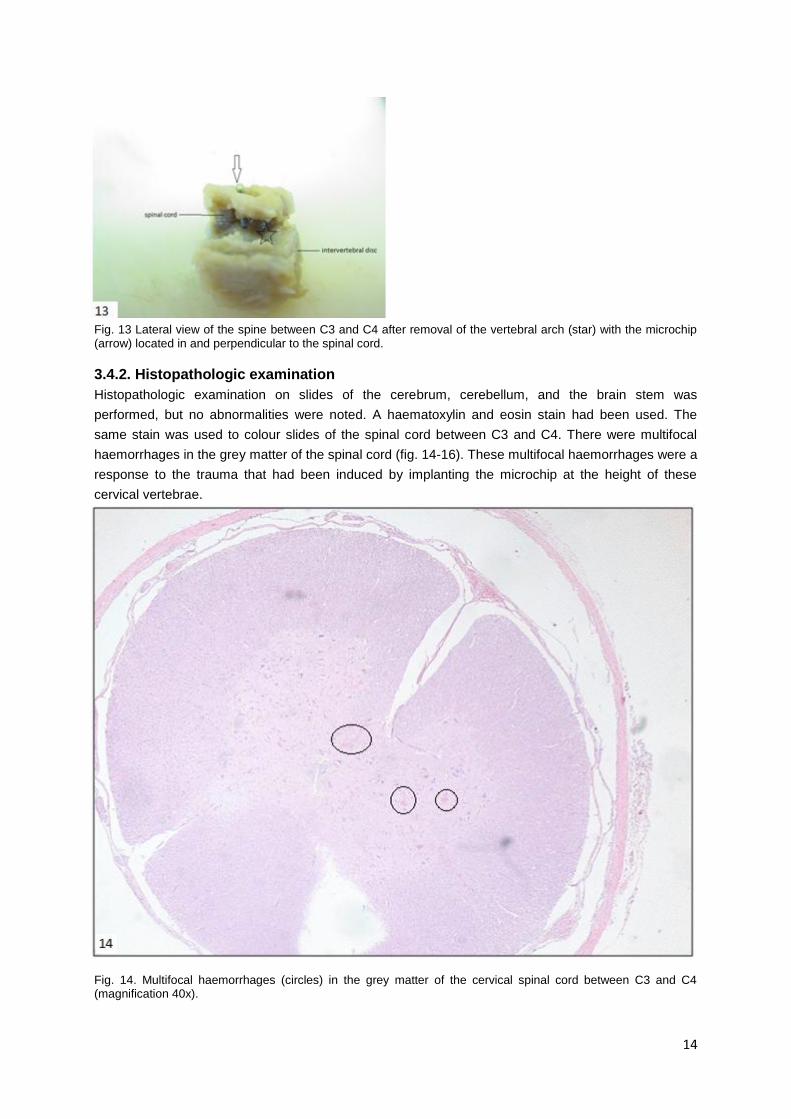
14
Fig. 13 Lateral view of the spine between C3 and C4 after removal of the vertebral arch (star) with the microchip (arrow) located in and perpendicular to the spinal cord.
3.4.2. Histopathologic examination
Histopathologic examination on slides of the cerebrum, cerebellum, and the brain stem was
performed, but no abnormalities were noted. A haematoxylin and eosin stain had been used. The
same stain was used to colour slides of the spinal cord between C3 and C4. There were multifocal
haemorrhages in the grey matter of the spinal cord (fig. 14-16). These multifocal haemorrhages were a
response to the trauma that had been induced by implanting the microchip at the height of these
cervical vertebrae.
Fig. 14. Multifocal haemorrhages (circles) in the grey matter of the cervical spinal cord between C3 and C4 (magnification 40x).
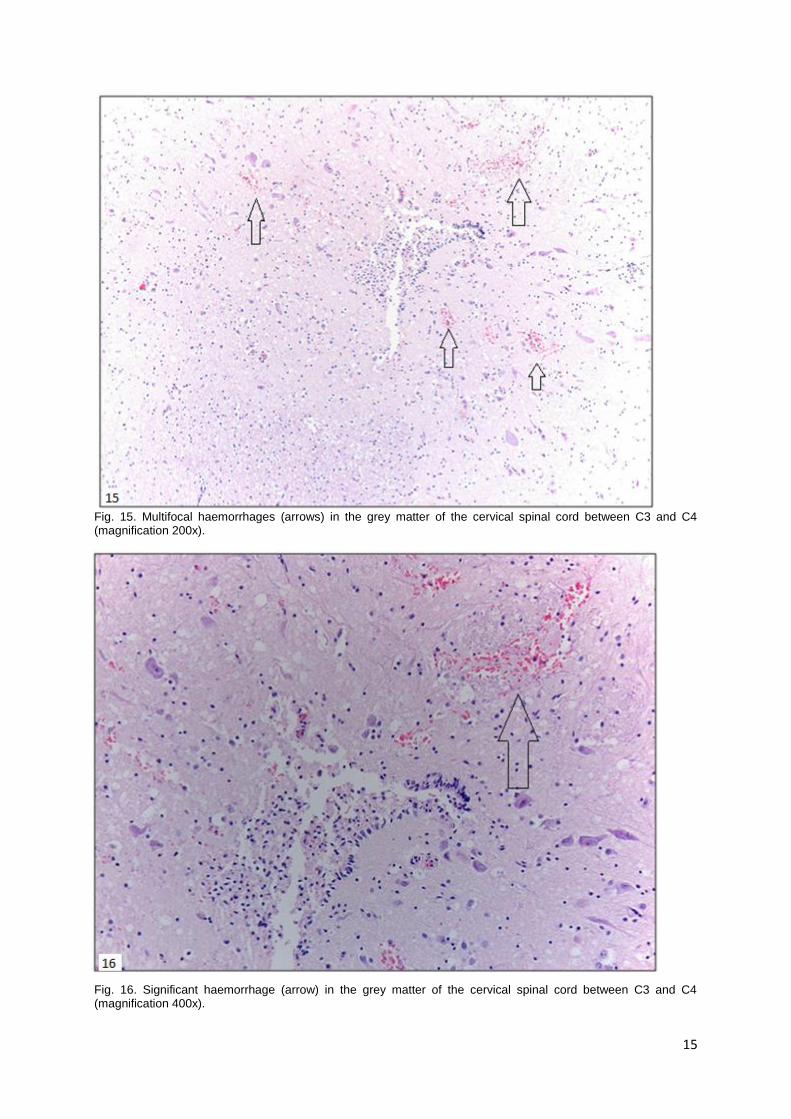
15
Fig. 15. Multifocal haemorrhages (arrows) in the grey matter of the cervical spinal cord between C3 and C4 (magnification 200x).
Fig. 16. Significant haemorrhage (arrow) in the grey matter of the cervical spinal cord between C3 and C4 (magnification 400x).
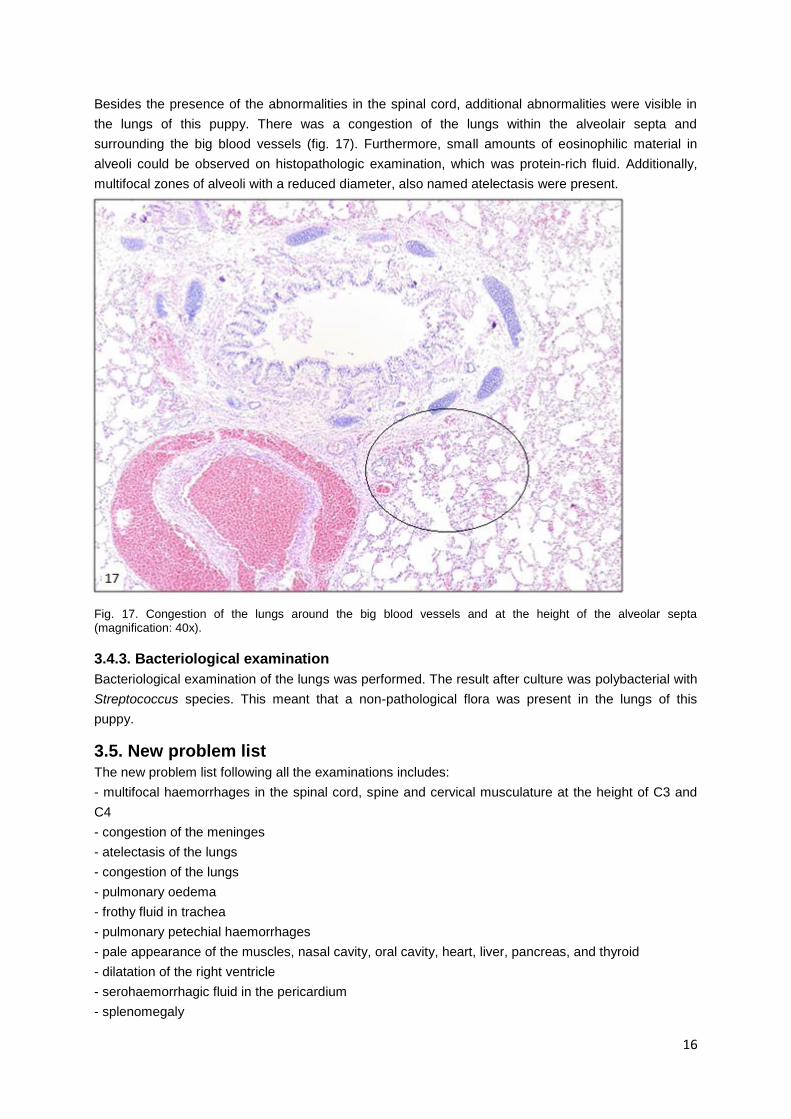
16
Besides the presence of the abnormalities in the spinal cord, additional abnormalities were visible in
the lungs of this puppy. There was a congestion of the lungs within the alveolair septa and
surrounding the big blood vessels (fig. 17). Furthermore, small amounts of eosinophilic material in
alveoli could be observed on histopathologic examination, which was protein-rich fluid. Additionally,
multifocal zones of alveoli with a reduced diameter, also named atelectasis were present.
Fig. 17. Congestion of the lungs around the big blood vessels and at the height of the alveolar septa (magnification: 40x).
3.4.3. Bacteriological examination
Bacteriological examination of the lungs was performed. The result after culture was polybacterial with
Streptococcus species. This meant that a non-pathological flora was present in the lungs of this
puppy.
3.5. New problem list The new problem list following all the examinations includes:
- multifocal haemorrhages in the spinal cord, spine and cervical musculature at the height of C3 and
C4
- congestion of the meninges
- atelectasis of the lungs
- congestion of the lungs
- pulmonary oedema
- frothy fluid in trachea
- pulmonary petechial haemorrhages
- pale appearance of the muscles, nasal cavity, oral cavity, heart, liver, pancreas, and thyroid
- dilatation of the right ventricle
- serohaemorrhagic fluid in the pericardium
- splenomegaly
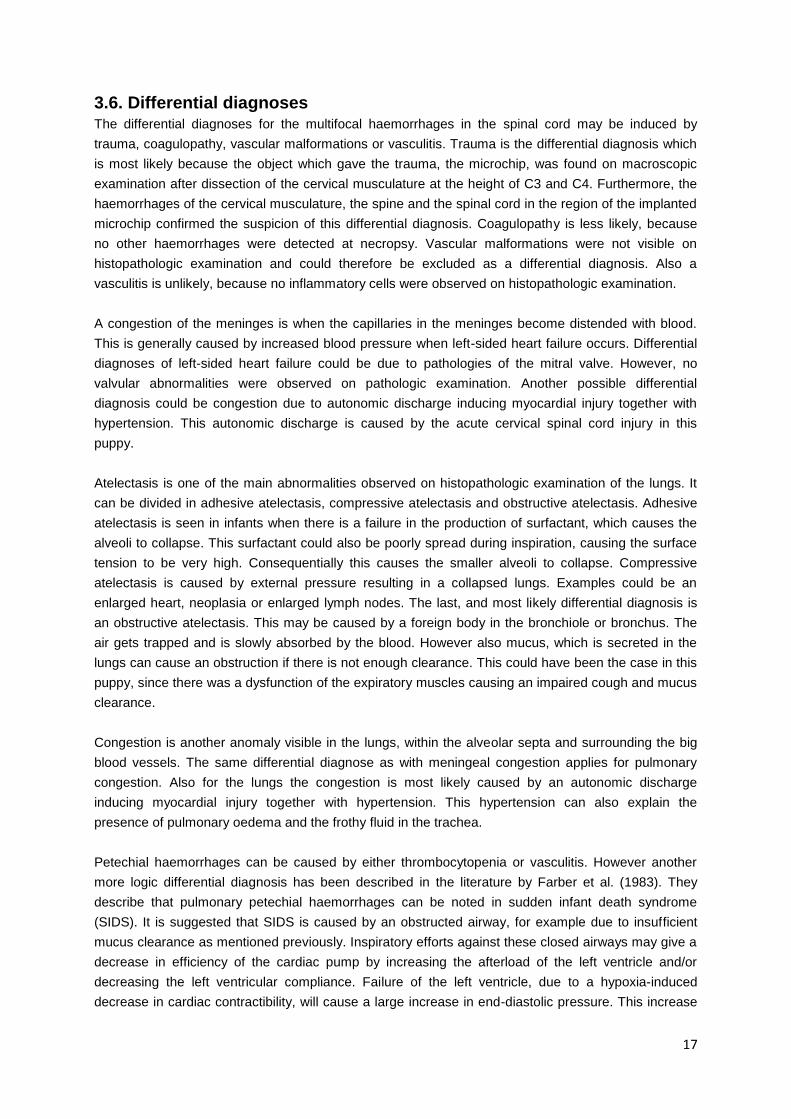
17
3.6. Differential diagnoses The differential diagnoses for the multifocal haemorrhages in the spinal cord may be induced by
trauma, coagulopathy, vascular malformations or vasculitis. Trauma is the differential diagnosis which
is most likely because the object which gave the trauma, the microchip, was found on macroscopic
examination after dissection of the cervical musculature at the height of C3 and C4. Furthermore, the
haemorrhages of the cervical musculature, the spine and the spinal cord in the region of the implanted
microchip confirmed the suspicion of this differential diagnosis. Coagulopathy is less likely, because
no other haemorrhages were detected at necropsy. Vascular malformations were not visible on
histopathologic examination and could therefore be excluded as a differential diagnosis. Also a
vasculitis is unlikely, because no inflammatory cells were observed on histopathologic examination.
A congestion of the meninges is when the capillaries in the meninges become distended with blood.
This is generally caused by increased blood pressure when left-sided heart failure occurs. Differential
diagnoses of left-sided heart failure could be due to pathologies of the mitral valve. However, no
valvular abnormalities were observed on pathologic examination. Another possible differential
diagnosis could be congestion due to autonomic discharge inducing myocardial injury together with
hypertension. This autonomic discharge is caused by the acute cervical spinal cord injury in this
puppy.
Atelectasis is one of the main abnormalities observed on histopathologic examination of the lungs. It
can be divided in adhesive atelectasis, compressive atelectasis and obstructive atelectasis. Adhesive
atelectasis is seen in infants when there is a failure in the production of surfactant, which causes the
alveoli to collapse. This surfactant could also be poorly spread during inspiration, causing the surface
tension to be very high. Consequentially this causes the smaller alveoli to collapse. Compressive
atelectasis is caused by external pressure resulting in a collapsed lungs. Examples could be an
enlarged heart, neoplasia or enlarged lymph nodes. The last, and most likely differential diagnosis is
an obstructive atelectasis. This may be caused by a foreign body in the bronchiole or bronchus. The
air gets trapped and is slowly absorbed by the blood. However also mucus, which is secreted in the
lungs can cause an obstruction if there is not enough clearance. This could have been the case in this
puppy, since there was a dysfunction of the expiratory muscles causing an impaired cough and mucus
clearance.
Congestion is another anomaly visible in the lungs, within the alveolar septa and surrounding the big
blood vessels. The same differential diagnose as with meningeal congestion applies for pulmonary
congestion. Also for the lungs the congestion is most likely caused by an autonomic discharge
inducing myocardial injury together with hypertension. This hypertension can also explain the
presence of pulmonary oedema and the frothy fluid in the trachea.
Petechial haemorrhages can be caused by either thrombocytopenia or vasculitis. However another
more logic differential diagnosis has been described in the literature by Farber et al. (1983). They
describe that pulmonary petechial haemorrhages can be noted in sudden infant death syndrome
(SIDS). It is suggested that SIDS is caused by an obstructed airway, for example due to insufficient
mucus clearance as mentioned previously. Inspiratory efforts against these closed airways may give a
decrease in efficiency of the cardiac pump by increasing the afterload of the left ventricle and/or
decreasing the left ventricular compliance. Failure of the left ventricle, due to a hypoxia-induced
decrease in cardiac contractibility, will cause a large increase in end-diastolic pressure. This increase
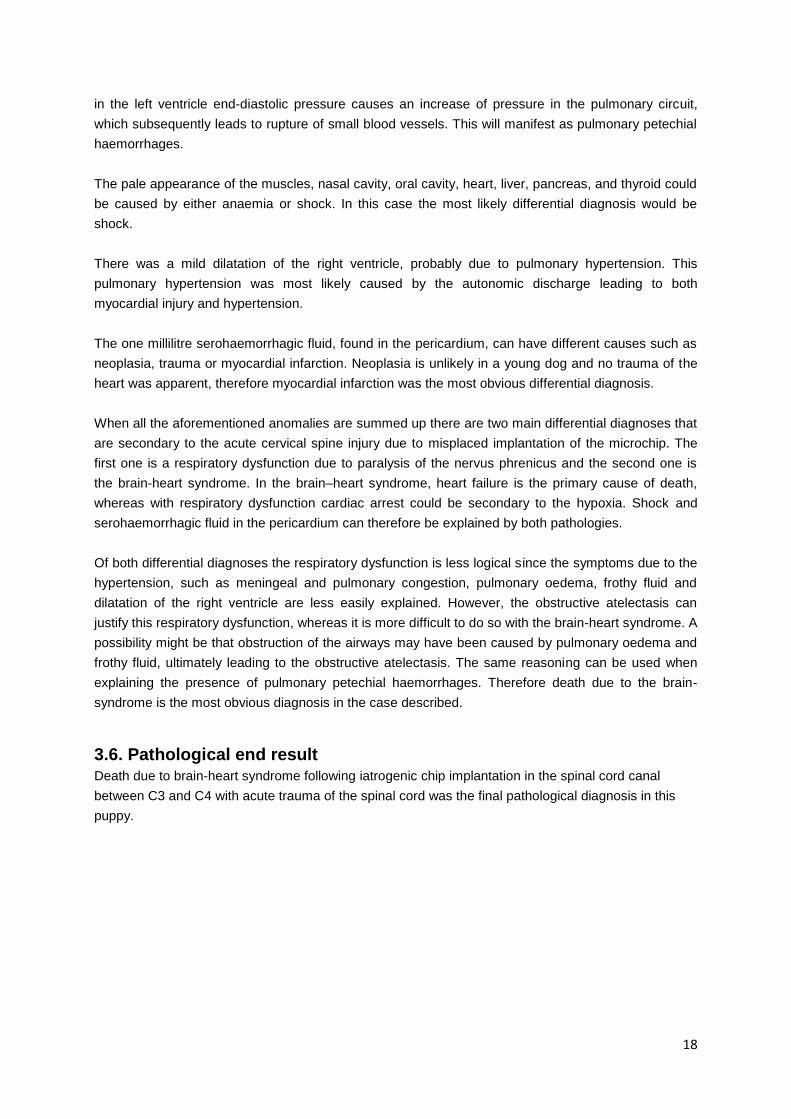
18
in the left ventricle end-diastolic pressure causes an increase of pressure in the pulmonary circuit,
which subsequently leads to rupture of small blood vessels. This will manifest as pulmonary petechial
haemorrhages.
The pale appearance of the muscles, nasal cavity, oral cavity, heart, liver, pancreas, and thyroid could
be caused by either anaemia or shock. In this case the most likely differential diagnosis would be
shock.
There was a mild dilatation of the right ventricle, probably due to pulmonary hypertension. This
pulmonary hypertension was most likely caused by the autonomic discharge leading to both
myocardial injury and hypertension.
The one millilitre serohaemorrhagic fluid, found in the pericardium, can have different causes such as
neoplasia, trauma or myocardial infarction. Neoplasia is unlikely in a young dog and no trauma of the
heart was apparent, therefore myocardial infarction was the most obvious differential diagnosis.
When all the aforementioned anomalies are summed up there are two main differential diagnoses that
are secondary to the acute cervical spine injury due to misplaced implantation of the microchip. The
first one is a respiratory dysfunction due to paralysis of the nervus phrenicus and the second one is
the brain-heart syndrome. In the brain–heart syndrome, heart failure is the primary cause of death,
whereas with respiratory dysfunction cardiac arrest could be secondary to the hypoxia. Shock and
serohaemorrhagic fluid in the pericardium can therefore be explained by both pathologies.
Of both differential diagnoses the respiratory dysfunction is less logical since the symptoms due to the
hypertension, such as meningeal and pulmonary congestion, pulmonary oedema, frothy fluid and
dilatation of the right ventricle are less easily explained. However, the obstructive atelectasis can
justify this respiratory dysfunction, whereas it is more difficult to do so with the brain-heart syndrome. A
possibility might be that obstruction of the airways may have been caused by pulmonary oedema and
frothy fluid, ultimately leading to the obstructive atelectasis. The same reasoning can be used when
explaining the presence of pulmonary petechial haemorrhages. Therefore death due to the brain-
syndrome is the most obvious diagnosis in the case described.
3.6. Pathological end result Death due to brain-heart syndrome following iatrogenic chip implantation in the spinal cord canal
between C3 and C4 with acute trauma of the spinal cord was the final pathological diagnosis in this
puppy.

19
4. Discussion Usually symptoms of acute injury to the cervical spinal cord can be placed under the nominative
cervical spinal syndrome. Anomalies associated with this syndrome are: neck pain, Horner’s
syndrome, torticollis, normal or elevated spinal reflexes in front and hind limbs, normal cutaneous
trunci reflex, normal cranial nerves reflexes, reduced or absent proprioception of front and hind limbs,
breathing problems, inability to urinate, and tetraplegia, tetraparesis, or ataxia. In the anamnesis of this
puppy only breathing problems were mentioned. The absence of all other symptoms can be explained
by the fact that due to instant death after dyspnoea and cardiac arrest there was no time to notice the
presence of the other anomalies. Both the symptoms of dyspnoea and cardiac arrest as well as shock
could explain the lateral decubitus and were not necessarily caused by tetraparesis or tetraplegia. No
neurological tests were performed to test proprioception, spinal reflexes, Horner’s syndrome and neck
pain. Also the ability to urinate was not paid attention to because of the acuteness of this case.
Usually symptoms of misplaced implantation of the microchip occur acutely, as was the case with this
puppy, because the microchip comes in contact with the spinal cord at once. However, Joslyn et al.
(2010) mention that neurological symptoms can also start to develop after as many as three years.
Slow erosion of the dorsal surface of the lamina of C6 during these three years, eventually leading to
exposure of the spinal cord to the microchip, could be the reason for the delayed development of
symptoms. This microchip was suspected to be implanted within the C5-C6 interacuate ligament and
epaxial muscles, possibly in contact with the dorsal surface of the cranial left dorsal lamina of C6. It
was suggested that contact and micro-motion at the glass-bone interface caused damage of the
periosteal blood supply and surrounding tissue. This would have resulted in gradual osteolysis due to
activated macrophages, osteoclasts and the release of osteolytic factors eventually enabling contact
between the microchip and the spinal cord.
If only the puppy would have been stabilised beforehand, radiology, myelography, Computed
Tomography, and surgery could have been performed. Mechanical ventilation could have been
administered, together with a dosage of adrenaline and atropine intra-venously. After cardiac arrest
heart massage could have resuscitated the puppy. Also blood pressure should have been checked
regularly for the presence of hypertension. Furthermore, an electrocardiogram could have been
connected to check for (supra)ventricular arrhythmias, bradyarrythmias and atrioventricular blocks.
Cardiac anomalies could have forecasted the cardiac arrest. Finally, additional blood analysis could
have been performed to evaluate the concentration of serum glutamic oxalacetic transaminase. A
moderate rise would have indicated subendocardial ischaemia.
Besides the alpaca mentioned earlier and this patient, no other cases of animals acutely dying
secondary to the event of symptoms linked to the misplaced insertion of the microchip, have been
reported in the literature. The reason why it happened in this puppy could be that the connection
between the brain stem and the spinal cord was still intact, causing the Cushing reflex with secondary
breathing problems. Other options would be the different location in the spinal cord or the force used
to insert the microchip. Furthermore, a non-observed underlying heart condition could have been an
additional factor for the brain-heart syndrome to manifest itself.
Generally a microchip should be placed subcutaneously in the neck of a pet, while properly lifting the
skin. Thus it would be impossible to insert the microchip in the spinal cord. The puppy however, may
have been struggling while inserting the microchip, which resulted in accidently placing the microchip

20
in the spinal cord. Further research on how to prevent such mistakes are required, because cases not
being described in the literature does not mean it never happens. Further research on how to react to
such acute cases is very useful for the veterinary practitioners as well.
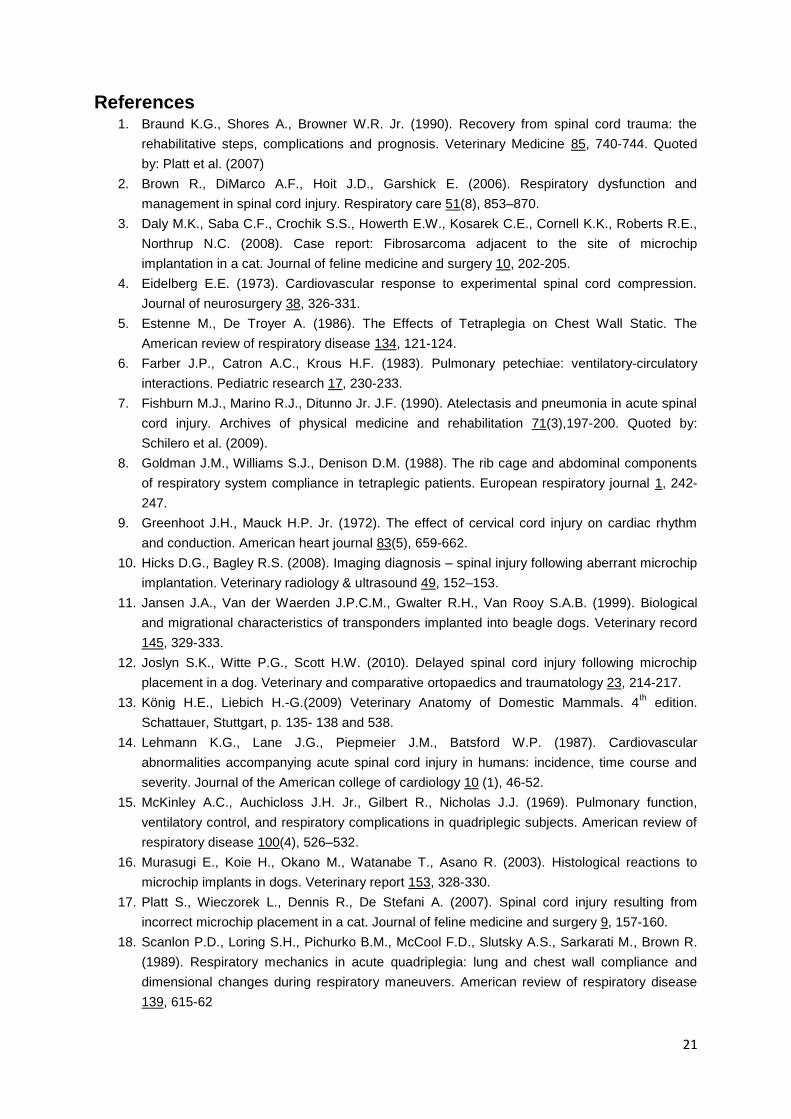
21
References 1. Braund K.G., Shores A., Browner W.R. Jr. (1990). Recovery from spinal cord trauma: the
rehabilitative steps, complications and prognosis. Veterinary Medicine 85, 740-744. Quoted
by: Platt et al. (2007)
2. Brown R., DiMarco A.F., Hoit J.D., Garshick E. (2006). Respiratory dysfunction and
management in spinal cord injury. Respiratory care 51(8), 853–870.
3. Daly M.K., Saba C.F., Crochik S.S., Howerth E.W., Kosarek C.E., Cornell K.K., Roberts R.E.,
Northrup N.C. (2008). Case report: Fibrosarcoma adjacent to the site of microchip
implantation in a cat. Journal of feline medicine and surgery 10, 202-205.
4. Eidelberg E.E. (1973). Cardiovascular response to experimental spinal cord compression.
Journal of neurosurgery 38, 326-331.
5. Estenne M., De Troyer A. (1986). The Effects of Tetraplegia on Chest Wall Static. The
American review of respiratory disease 134, 121-124.
6. Farber J.P., Catron A.C., Krous H.F. (1983). Pulmonary petechiae: ventilatory-circulatory
interactions. Pediatric research 17, 230-233.
7. Fishburn M.J., Marino R.J., Ditunno Jr. J.F. (1990). Atelectasis and pneumonia in acute spinal
cord injury. Archives of physical medicine and rehabilitation 71(3),197-200. Quoted by:
Schilero et al. (2009).
8. Goldman J.M., Williams S.J., Denison D.M. (1988). The rib cage and abdominal components
of respiratory system compliance in tetraplegic patients. European respiratory journal 1, 242-
247.
9. Greenhoot J.H., Mauck H.P. Jr. (1972). The effect of cervical cord injury on cardiac rhythm
and conduction. American heart journal 83(5), 659-662.
10. Hicks D.G., Bagley R.S. (2008). Imaging diagnosis – spinal injury following aberrant microchip
implantation. Veterinary radiology & ultrasound 49, 152–153.
11. Jansen J.A., Van der Waerden J.P.C.M., Gwalter R.H., Van Rooy S.A.B. (1999). Biological
and migrational characteristics of transponders implanted into beagle dogs. Veterinary record
145, 329-333.
12. Joslyn S.K., Witte P.G., Scott H.W. (2010). Delayed spinal cord injury following microchip
placement in a dog. Veterinary and comparative ortopaedics and traumatology 23, 214-217.
13. König H.E., Liebich H.-G.(2009) Veterinary Anatomy of Domestic Mammals. 4th edition.
Schattauer, Stuttgart, p. 135- 138 and 538.
14. Lehmann K.G., Lane J.G., Piepmeier J.M., Batsford W.P. (1987). Cardiovascular
abnormalities accompanying acute spinal cord injury in humans: incidence, time course and
severity. Journal of the American college of cardiology 10 (1), 46-52.
15. McKinley A.C., Auchicloss J.H. Jr., Gilbert R., Nicholas J.J. (1969). Pulmonary function,
ventilatory control, and respiratory complications in quadriplegic subjects. American review of
respiratory disease 100(4), 526–532.
16. Murasugi E., Koie H., Okano M., Watanabe T., Asano R. (2003). Histological reactions to
microchip implants in dogs. Veterinary report 153, 328-330.
17. Platt S., Wieczorek L., Dennis R., De Stefani A. (2007). Spinal cord injury resulting from
incorrect microchip placement in a cat. Journal of feline medicine and surgery 9, 157-160.
18. Scanlon P.D., Loring S.H., Pichurko B.M., McCool F.D., Slutsky A.S., Sarkarati M., Brown R.
(1989). Respiratory mechanics in acute quadriplegia: lung and chest wall compliance and
dimensional changes during respiratory maneuvers. American review of respiratory disease
139, 615-62
22
19. Schilero G.J., Spungen A.M., Bauman W.A., Radulovic M., Lesser M. (2009). Pulmonary
function and spinal cord injury. Respiratory physiology and neurobiology 166, 129-141.
20. Smith T.J., Fitzpatrick N. (2009). Surgical removal of a microchip from a puppy's spinal canal.
Veterinary and comparative orthopaedics and traumatology 22, 63–65.
21. Swift S. (2000). Microchip adverse reactions. Journal of small animal practice, 41, 232.
22. Van der Burgt G., Dowles H. (2007). Microchip insertion in alpacas. Veterinary record 160,
204.
23. Vascellari M., Mutinelli F., Cossettini R., Altinier E. (2004). Liposarcoma at the site of an
implanted microchip in a dog. The veterinary journal 168, 188-190.
24. Vascellari M., Melchiotti E., Mutinelli F. (2006). Fibrosarcoma with typical features of
postinjection sarcoma at site of microchip implant in a dog: histologic and
immunohistochemical study. Veterinary pathology 43, 545-548.


