Embed Size (px)
Citation preview

7/24/2014
1
Infectious Diseases Potpourri
Nick Gilpin, DO
Section Head, Infectious Diseases
Beaumont Health Systems – Grosse Pointe
Assistant Clinical Professor, OUWBSOM
Assistant Clinical Professor, MSUCOM
Presented for the MAOFP Conference
August 1-3, 2014
Traverse City, MI
Disclosures
• No conflict of interest to disclose
Pot-pour-ri \,pō-pu̇-’rē\ noun
: A mixture of dried flower petals, leaves,
and spices used to make a room smell
pleasant
: A miscellaneous collection

7/24/2014
2
Overview
• Discuss evaluation and management
(including antibiotic selection) for a variety
of commonly encountered infectious
diseases:
– Cellulitis; skin and soft tissue infections
– Pneumonia (community acquired)
– UTIs
– Diabetic Foot Infections; osteomyelitis
Scenario #1:
“Cellulitis”
Case Presentation
• 44 y/o male with history of “pre-diabetes”
• 3 day history of progressive swelling,
redness, pain involving his RUE…
• Discovered upon awakening…
• No fevers, chills, other symptoms..
• No history of prior cellulitis…

7/24/2014
3
Buzzwords!
• “I got bit by a spider…”
• “There’s this red streaking…”
• “It’s been itching like crazy…”
• “I had a DVT a while ago…”
• “My dog bit me…”
• “A person bit me…”
• “I was swimming in the ocean…”
• “I was cleaning my fishtank…”
• “I got this infection after a mud run…”
S. aureus (MRSA)
Group A strep (S. pyogenes)
Contact dermatitis?
Venous insufficiency?
Pasteurella multocida
Eikenella corrodens
Vibrio vulnificus
Mycobacterium marinum
“Fish-Tank granuloma”
Aeromonas hydrophila
An Evidence-Based Approach• First, is it NON-PURULENT or
PURULENT:– Non-purulent? – Think Group A Strep
• Fiery red, well-demarcated
• Lymphangitis or “streaking”
• No obvious “portal of entry”
– Purulent? – Think S. aureus• Redness surrounding some purulent focus
• Patient may have some historical clue (e.g., fitness club, close contact, etc.)
• Blood cultures, skin swabs, and biopsies are LOW YIELD!– Helpful if an abscess is present
– May help diagnose infectious mimics (pyoderma)
– They may be useful in immunocompromised patients, patients with penetrating trauma, or bites…
IDSA Practice Guidelines for SSTIs. Clinical Infectious Diseases. 2014; 1-43

7/24/2014
4
An Evidence-Based Approach
• Without systemic signs/symptoms (mild)– Oral therapy
– PCN, Dicloxacillin, Cephalosporin, Clindamycin
• With systemic signs/symptoms(moderate)– Consider hospitalization, IV
antibiotics
– PCN, Cefazolin, Clindamycin
• With severe
signs/symptoms
(sepsis), trauma, or
suspicion of MRSA
(severe)
– Consider imaging,
debridement
– IV antibiotics
– Vanco PLUS Zosyn (broad
spectrum antibiotics)
• For non-purulent cellulitis (Group A Strep):
IDSA Practice Guidelines for SSTIs. Clinical Infectious Diseases. 2014; 1-43
An Evidence-Based Approach
• Small abscess without
systemic illness (mild)
– I+D only
– Culture is optional
• Abscess/cellulitis with
systemic illness
(moderate)
– I+D, culture
– Oral antibiotics: Bactrim or
Doxycycline
– Maybe Clindamycin?
• With severe
signs/symptoms
(sepsis), hypotension
(severe)
– I+D, culture
– IV antibiotics: Vanco,
Linezolid, Daptomycin, etc.
• For purulent cellulitis (Staph aureus, MRSA):
IDSA Practice Guidelines for SSTIs. Clinical Infectious Diseases. 2014; 1-43
IDSA Practice Guidelines for SSTIs. Clinical Infectious Diseases. 2014; 1-43

7/24/2014
5
Remember Adjunctive Therapies
• Elevate the leg to promote gravity drainage of edema
• Warm compresses to facilitate drainage of purulent abscesses
• Limit ambulation
• Corticosteroids may be beneficial in uncomplicated cases, non-diabetics (shortens healing time by ~1 day)
• Treat underlying conditions like tinea pedis and eczema to prevent recurrences
• Decolonization with topical chlorhexidine and intranasal mupirocin may be useful in cases of recurrent MRSA abscesses– 5 days of intranasal mupirocin twice daily plus daily
chlorhexidine washes
Clinical Infectious Diseases 2005; 41:1373–406
IDSA Practice Guidelines for SSTIs. Clinical Infectious Diseases. 2014; 1-43
“How long should I treat??”
• Depends…– Uncomplicated cellulitis: About 5 days (maybe more)
– “Complicated” (hospitalized) cellulitis: 7-14 days
• May be significantly longer in patients with “unusual” pathogens like mycobacteria, fungi, Nocardia, etc.
• How I approach cellulitis:
– Oral therapy is preferred
– If hospitalization/parenteral is required, treat until 60-70% improvement in cellulitis, then transition to oral therapy
Clinical Infectious Diseases 2005; 41:1373–406
IDSA Practice Guidelines for SSTIs. Clinical Infectious Diseases. 2014; 1-43
Scenario #2:
Pneumonia

7/24/2014
6
Case Presentation
• 70 y/o male is brought to the EC
• Increased cough, chest discomfort, SOB
• Some sputum production
• Feels “feverish”
Not so subtle…
Guidelines for
CAP
Guidelines for
HCAP

7/24/2014
7
Is it CAP or HCAP?
• HCAP
– Antibiotics within the
preceding 90 days
– Hospitalization in the
preceding 90 days
– ECF resident
– Home infusion therapy or
wound care
– Family member with MDR
pathogen
– Dialysis within past 30 days
• CAP
– No healthcare-associated
exposure…
IDSA Guidelines for CAP. Clinical Infectious Diseases 2007; 44:S27-72.
ATS Guidelines for HCAP. Am J Respir Crit Care Med ; 2005 ; 171 : 388 -416
CAP Pathogens
Outpatient Inpatient ICU
S. pneumoniae S. pneumoniae S. pneumoniae
Mycoplasma pneumoniae Mycoplasma pneumoniae S. Aureus (MRSA?)
Haemophilus influenzae Haemophilus influenzae Legionella species
Chlamydophila pneumoniae Chlamydophila pneumoniae Gram-negative bacteria
Respiratory viruses Legionella species Haemophilus influenzae
Aspiration
Respiratory viruses
Diagnosis of CAP
• Remember that pneumonia is a CLINICAL diagnosis (cough, fever, sputum production, chest pain) supported by radiographic findings!
• All patients with suspected pneumonia should have some form of imaging (CXR or CT)
• Additional testing (e.g., performing cultures) is discretionary– Cultures are often falsely negative or do not impact clinical
management
• Blood cultures are only positive 5-14% of the time…
• Sputum cultures are probably not much better…
– A good rule of thumb: Perform a test only when the result will change your management

7/24/2014
8
Clinical Infectious Diseases 2007; 44:S27–72
Management of CAP
• To admit or not to admit…
– CURB-65 (score ≥ 2 may warrant admission)
• Confusion
• Uremia (BUN ≥ 20)
• Respiratory rate ≥ 30
• Blood pressure (hypotension)
• Age > 65
• ICU admission?
– Septic shock and/or mechanical ventilation
– More than 3 criteria for “severe” pneumonia
Clinical Infectious Diseases 2007; 44:S27–72

7/24/2014
9
Treatment of CAPOutpatient Inpatient ICU• If previously healthy and
no abx in prior 3 months:
– Azithromycin or
clarithromycin alone
– Doxycycline
• If comorbidities present or
recent abx use:
– A β-lactam plus a
macrolide (e.g.,
cefuroxime plus
azithromycin)
– A respiratory
fluoroquinolone
(moxifloxacin or
levofloxacin)
• A β-lactam plus a
macrolide (e.g., ceftriaxone
plus azithromycin)
• A respiratory
fluoroquinolone
(moxifloxacin or
levofloxacin)
• A β-lactam plus either a
macrolide or respiratory
fluoroquinolone (e.g.,
ceftriaxone plus
azithromycin or
moxifloxacin/ levofloxacin)
• If PCN-allergic, consider
aztreonam plus a
respiratory fluoroquinolone
• Have a very low threshold
for adding MRSA coverage
(e.g., vancomycin or
linezolid)!
IDSA Guidelines for CAP. Clinical Infectious Diseases 2007; 44:S27-72.
HCAP Pathogens
S. aureus (especially MRSA)
Pseudomonas
E. coli
Klebsiella species
Other enteric Gram-negatives
Acinetobacter and Stenotrophomonas species
Legionella species
Aspiration pathogens
Polymicrobial
Viruses, fungal organisms
Almost
always
multi-drug
resistant!!
Pathogenesis of HCAP
• Patients are likely to be colonized with MDR
organisms
• Most cases are bacterial, with a small
percentage being polymicrobial
• The source of pathogens includes:
– The environment (hospital, ECF, etc.)
– Devices
– The transfer of microorganisms from healthcare
provider to patient
– Aspiration
ATS Guidelines for HCAP. Am J Respir Crit Care Med ; 2005 ; 171 : 388 -416

7/24/2014
10
HCAP Management Algorithm
ATS Guidelines for HCAP. Am J Respir Crit Care Med ; 2005 ; 171 : 388 -416
Treatment of HCAP
“Early” (≤ 5 days) Onset
HCAP or Low Risk of MDR
Pathogens*
“Late” Onset or Risk of
MDR Pathogens
Ceftriaxone Anti-Pseudomonal penicillin or
cephalosporin (cefepime or
piperacillin/tazobactam)
OR a respiratory fluoroquinolone PLUS a respiratory
fluoroquinolone or aminoglycoside
OR amoxicillin/clavulanate or
ampicillin/sulbactam
PLUS vancomycin or linezolid
*includes patients receiving outpatient antibiotics in the past 90 days, but is mostly discretionary
ATS Guidelines for HCAP. Am J Respir Crit Care Med ; 2005 ; 171 : 388 -416
“How long should I treat??”
• For CAP, a 5-7 day course of antibiotics is
usually enough
• For HCAP (including VAP), a 7-8 day
course is usually enough
• Research has not found prolonged
courses of antibiotics to be beneficial…

7/24/2014
11
Scenario #3:
Urinary Tract Infections
Case Presentation
• 33 y/o female presents with 4 day history
of burning with urination, fevers, and chills
• She also notes back pain, worse on the
left side
• She has had UTIs previously, with the last
one being about 6 months ago
Guidelines for Acute Cystitis
And Pyelonephritis
Guidelines for Catheter-
Associated UTIs
Guidelines for
Asymptomatic Bacteriuria

7/24/2014
12
Diagnosis of UTIs
• History
– Ask about prior infections, stones, urological
procedures, indwelling catheters, etc.
• Physical
– Look for CVA or suprapubic tenderness
• Urinalysis
• Urine culture (especially if there is
suggestion of “upper tract” involvement)
When to evaluate the urinary tract
• Pyelonephritis with bacteremia not responding to
therapy
– CT scan (abscess?)
• Nephrolithiasis
– Ultrasound or CT scan (hydronephrosis?)
• Neurogenic bladder
– Bladder/renal ultrasound (post-void residuals?)
• Men with a urinary tract infection
– Prostate exam, ultrasound, post-void residuals, etc.
Microbiology of UTIsBug Acute
uncomplicated
cystitis
Acute
uncomplicated
pyelonephritis
Complicated
UTI
Catheter-
associated
UTI
E. coli 79% 89% 32% 24%
S. saprophyticus 11% 0% 1% 0%
Proteus 2% 4% 4% 6%
Klebsiella 3% 4% 5% 8%
Enterococcus 2% 0% 22% 7%
Pseudomonas 0% 0% 20% 9%
Mixed 3% 5% 10% 11%
Other* 0% 2% 21% 46%
*includes S. epidermidis, Candida spp., and other Gram-negatives

7/24/2014
13
Treatment of
Acute Uncomplicated Cystitis• Macrobid 100 mg bid x 5 days
• TMP-SMX DS 1 bid x 3-5 days
• Fosfomycin 3g in a single dose
• Fluoroquinolones (e.g., ciprofloxacin) should generally be reserved for selected patients where 1st line therapy is not feasible
• β-lactams (cephalexin, amox-clav) should also be reserved for selected patients due to increasing failure rates
• Amoxicillin by itself should NOT be used empirically (too much E. coli resistance)
Guidelines for Acute Cystitis/Pyelonephritis. Clinical Infectious Diseases 2011;52(5):e103–e120
Treatment of
Acute Pyelonephritis• Pyelo = fever, flank pain, pyuria
• Remember to obtain a urine culture
• If hospitalization not required:– Fluoroquinolone x 7-10 days
– β-lactams x 10-14 days
– TMP-SMX x 10-14 days
• If hospitalization required:– Ampicillin/gentamicin, fluoroquinolone, or extended
spectrum β-lactams should be given intravenously initially
– You no longer need to keep the patient hospitalized until they are afebrile…
Guidelines for Acute Cystitis/Pyelonephritis. Clinical Infectious Diseases 2011;52(5):e103–e120

7/24/2014
14
Treatment of
Other Complicated UTIs
• If a renal/perinephric abscess is present, it
should be drained appropriately and
cultures
– Treatment is generally considered for 2-3
weeks based on treatment response
– Close urology follow-up is necessary
Catheter-Associated UTIs
• The diagnosis is much trickier...
– Not all pyuria and bacteriuria means infection!
– Look for “true symptoms”• New onset or worsening of fever, rigors
• Altered mental status
• Malaise or lethargy with no other identified cause
• Flank pain or costovertebral angle tenderness
• Acute hematuria
• Pelvic discomfort;
• In those whose catheters have been removed, dysuria, urgent or frequent urination, or suprapubic pain or tenderness
Guidelines for Catheter-Associated UTI. Clinical Infectious Diseases 2010; 50:625–663
Treatment of
Catheter-Associated UTIs
• Selection of antibiotics should be based upon cultures (both old and new)
• Duration of treatment:
– 7 days of treatment (based on culture results) is recommended for patients with a brisk response to therapy
– 10-14 days is recommended for patients with a delayed response to therapy
– Shorter durations can be considered in some circumstances
Guidelines for Catheter-Associated UTI. Clinical Infectious Diseases 2010; 50:625–663

7/24/2014
15
What about prophylaxis for patients
with indwelling catheters?• For prevention of catheter-associated UTIs, there is no
documented benefit with:– Antibiotics
– Methenamine
– Cranberry products
– Routine catheter changing
– Enhanced meatal care
– Antimicrobials in the drainage bag
– Catheter irrigation
– Antimicrobial-coated catheters
• The best practice: use the catheter for the shortest duration feasible– For men, consider condom catheters if appropriate
– Intermittent catheterization appears to be somewhat better than indwelling catheter use
– Suprapubic catheters should be considered an alternative to long-term indwelling catheters
Guidelines for Catheter-Associated UTI. Clinical Infectious Diseases 2010; 50:625–663
What about asymptomatic
bacteriuria?• What is it?
– For asymptomatic women, bacteriuria is defined as 2 consecutive voided urine specimens with isolation of the same bacterial strain in quantitative counts >100,000 cfu/mL
– For asymptomatic men, a single, clean-catch voided urine specimen with 1 bacterial species isolated in a quantitative count >100,000 cfu/mL identifies bacteriuria
– A single catheterized urine specimen with 1 bacterial species isolated in a quantitative count >1000 cfu/mL identifies bacteriuria in women or men
• When is asymptomatic bacteriuria treated?– Pregnancy
– Persons with structural/neurological abnormalities of the urinary tract
– Persons undergoing urologic surgery
• If you’re treating asymptomatic bacteriuria, duration should be 3-7 days (same as for cystitis, based on culture results)
Guidelines for Asymptomatic Bacteriuria. Clinical Infectious Diseases 2005; 40:643–54
Dilemma #4:
Diabetic Foot Infections

7/24/2014
16
Case Presentation
• 60 y/o diabetic female
• “Cut my foot on something a while ago…”
• Progressively worsening ulceration with
drainage
• No fevers, chills
• No other complaints
How do I know if it’s infected?
How can I tell if it’s a bone infection?
• Look for “classic” signs of infection (local inflammation, purulence, and systemic signs/symptoms)
– Beware of not-so-classic signs
• Consider using a validated “scoring system” to aid in diagnosis
– Example: International Working Group on the Diabetic Foot has a scoring criteria to assist in diagnosis of osteomyelitis (versus a skin/soft tissue infection)

7/24/2014
17
Diabetic Foot Infections:
PresentationMILD MODERATE SEVERE
More than 2 of: Any of the following: Patient is systemically
toxic or unstablePurulence, erythema,
pain, tenderness,
warmth, induration
Cellulitis >2 cm
around ulcer
Any cellulitis
extending <2 cm
around ulcer
Lymphangitis
Infection is limited to
skin/superficial tissue
Deep tissue abscess
No systemic illness Gangrene
Muscle, tendon, joint,
or bone involvement
Guidelines for Diabetic Foot Infection. Clinical Infectious Diseases. 2004; 39: 885-910.
Diabetic Foot Infections:
• International Working Group on the
Diabetic Foot (IWGDF) has attempted to
formulate a criteria-based approach to
diagnosis
– Similar to other diagnostically challenging
conditions (e.g., infective endocarditis)
• Not validated in practice, but appears
promising, particularly for osteomyelitis
Definite
Positive bone culture
Pus in bone
Atraumatically detached bone fragment removed from ulcer
Intraosseous abscess on MRI
Probable
Visible bone in ulcer
MRI showing bone edema with other signs of osteomyelitis
Bone sample with positive culture but negative histology
Bone sample with positive histology but negative culture
Possible
Plain X-rays show cortical destruction
MRI shows bone edema
“Probe to bone” positive
Bone visible
ESR > 70 without a reasonable explanation
Non-healing ulcer present for >2 weeks

7/24/2014
18
SCORE PROBABILITY
OSTEOMYELITIS
IS PRESENT
MANAGEMENT
1 definite >90% Treat
2 probable
1 probable + 2
possible
4 possible
50-90% Consider
treating, but may
require further
investigation
2 possible 10-50% Further
investigation
advised before
treatment
Berendt et al. Diabetes Metab Res Rev 2008.
Who should be hospitalized?
• Patients with a severe infection
• Selected patients with a moderate
infection and significant comorbidities
• Any patient who is unable to comply with a
prescribed regimen
• Patients who fail an outpatient regimen
(maybe…)
How should cultures be obtained?
• If it’s not infected, DON’T CULTURE IT!
• For infected wounds, get the deepest and
best sample possible
– Debrided tissue or bone is best
– Preferable to get cultures OFF antibiotics
Guidelines for Diabetic Foot Infection. Clinical Infectious Diseases. 2004; 39: 885-910.

7/24/2014
19
“To swab or not to swab…”
• Generally deep cultures and/or
aspirates are preferred over superficial
swabs
• Two main reasons a swab may be
helpful:
– Identification of resistant pathogens (MRSA,
VRE) indicates need for special contact
precautions
– Isolation of MRSA often correlates with deep
cultures (other “junk”…not so much)
What other diagnostic studies
may be helpful?
• Adjunctive labs and imaging are helpful in
the following situations:
– Patient is not responding appropriately to
“correct” therapy
– Suspicion exists for a deeper infection
• All patients with a new diabetic foot
infection should have a plain radiograph
Guidelines for Diabetic Foot Infection. Clinical Infectious Diseases. 2004; 39: 885-910.
Pitfalls of Osteomyelitis
• Osteomyelitis can be a significant
diagnostic challenge
• Patients at greatest risk are typically
immunocompromised
– Less likely to have febrile/inflammatory response
• High risk diabetic patients will frequently have
absent sensation in affected areas (e.g., the
diabetic foot)
• The labs may not support your diagnosis

7/24/2014
20
Labs which may aid in the
diagnosis of osteomyelitis
• WBC (elevated?)
– Beware: this may be helpful in an acute process, but is rarely helpful in a chronic process
• ESR/CRP (elevated?)
– USUALLY elevated, but how much is enough
– Best utility may be to “trend” these data over time to monitor clinical response
• Blood cultures
– Highest yield in settings of acute hematogenous osteomyelitis or vertebral osteomyelitis
– Yield is still much less than 50%
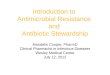
Imaging which may aid in the
diagnosis of osteomyelitis
• Plain X-ray:
– Low sensitivity (~15-
40%); moderate
specificity (~70%)
– Abnormalities are
usually seen 10-14
days after onset of
infection
Periosteal
Reaction
Imaging which may aid in the
diagnosis of osteomyelitis
• MRI:
– Very sensitive (~85%),
somewhat less specific
– High negative predictive
value in appropriate
clinical setting
– Typically regarded as the
“imaging modality of
choice”

7/24/2014
21
Imaging which may aid in the
diagnosis of osteomyelitis
• CT scan:
– Next best modality when MRI cannot be used
– Beware metallic artifact in setting of hardware
• Nuclear modalities:
– High sensitivity, generally poor specificity
– “Three phase bone scan” is reasonable in the
appropriate clinical setting
• Consider nuclear modalities in patients where MRI
or CT cannot be reasonably performed
Three Phase Bone Scan
• Uses a radionuclide tracer that accumulates in areas of bone turnover
• Scans are performed at three points following tracer: – immediately after injection (blood “flow” phase)
– 15 minutes after injection (blood pool “tissue” phase)
– 4 hours after injection (“osseous” phase)
• In osteomyelitis, expect high uptake in all three phases– Contrast with cellulitis: NO activity in the “osseous” phase
• NOT the same thing as a “Triple Tracer Bone Scan” (bone marrow scan, bone scan, WBC scan)
EARLY
Uptake occurs
in areas of the
L foot in all 3 phases –
This is consistent
with OSTEOMYELITIS

7/24/2014
22
What treatment?
• If it’s not infected, don’t treat (Duh…)
• Topical antibiotics are probably worthless
• For infected wounds, consider the severity and degree of infection:– Mild-to-moderate infections: target Gram-positive cocci (most
common), and think about MRSA…
• Keflex; Cefazolin; Vanco…
– More severe infections: go broad (target Gram-positives AND Gram-negative, and potentially anaerobes)
• Zosyn; Vanco + Zosyn; Vanco + Cefepime +/- Flagyl
– Targeting Pseudomonas is probably overrated unless your patient has risk factors or known colonization
• Once your cultures are back, treat what is growing
Guidelines for Diabetic Foot Infection. Clinical Infectious Diseases. 2004; 39: 885-910.
Principle of Antimicrobial Therapy
in Osteomyelitis/DFI
“All antimicrobials should be withheld if
possible until percutaneous aspirate or
surgical deep cultures have been
obtained.”**
**Unless patient is “sick”…
Microbiology of Osteomyelitis/DFI
COMMON
(>50%)
OCCASIONAL
(>25%)
RARE (<5%)
S. aureus Strep MTB
CoNS Enterococcus Dimorphic
fungi
Pseudomonas Candida
E. coli Aspergillus
Other
Enterobacteriaciae
Brucella
Anaerobes Salmonella

7/24/2014
23
Targeted Antimicrobial Therapy
in Osteomyelitis/DFIBug Preferred Alternative
MSSA Nafcillin
Cefazolin
Vanco (+/- Rifampin)
MRSA Vanco
Dapto
Linezolid (+/- Rifampin)
Strep PCN
Ceftriaxone
Cefazolin
Vanco
Enterococcus PCN or Amp
(+/- Gent)
Vanco
Enterobacteriaceae Ceftriaxone Cipro
Pseudomonas Cefepime, Pip-Tazo Cipro
Osteomyelitis “Buzzwords”
• Post-surgical osteo?
• Osteo in a “sickler”?
• Man in a tennis shoe steps on a
nail?
• Spinal osteo in a person from India?
• Sacroiliac joint osteo?
• Osteo in a dialysis patient?
• Osteo in IV drug users?
S. aureus or CoNS
Salmonella
Pseudomonas
MTB
S. aureus
S. aureus, MRSA
S. aureus, Pseudomonas, Candida
How long should I treat a diabetic
foot infection?
• Continue antibiotics until the infection is
resolved
– You don’t need to treat until the wound is
healed!!
– General rule: 1-2 weeks for mild infections, 2-
3 weeks for moderate-to-severe infections
Guidelines for Diabetic Foot Infection. Clinical Infectious Diseases. 2004; 39: 885-910.

7/24/2014
24
How long should I treat
osteomyelitis?
• Optimal duration is not well established…
– Lack of prospective trials
• What do we know?
– 4 weeks is better than 2 weeks
– 6 weeks is about how long it takes for debrided bone
to be covered by vascularized soft tissue
– A shorter duration may be reasonable when extensive
debridement/amputation is performed
– Treatment should be given parenterally (if feasible)
General Principles of Osteomyelitis
Treatment
• Goal: eradicate infection, restore function
• Understand that you are potentially fighting a losing battle
– Antimicrobial therapy alone is not curative in most cases of osteomyelitis
– Surgical debridement will increase your chances of cure
– Chronic osteomyelitis (devitalized bone) is virtually incurable with antibiotics alone
• Consider surgery/amputation
Thank you!
Infectious Diseases Potpourri
Nick Gilpin, DO
Infectious Disease
Beaumont Health Systems – Grosse Pointe
















![Bernard Gilpin - Houghton Le Spring Heritagehoughtonlespring.org.uk/gilpin/bernard_gilpin.pdf · 2017-07-02 · March 1557 – Bernard Gilpin [40] accepted the offer of Rector for](https://img.pdfslide.us/doc/110x75/5e2d3ac93473f82a7c24c634/bernard-gilpin-houghton-le-spring-heri-2017-07-02-march-1557-a-bernard-gilpin.jpg)