Embed Size (px)
Citation preview
Infectious Disease Epidemiology: Outbreak Control &
Investigation
With a focus on the Singapore experience
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018GlobaLab.biz 1
With a focus on the Singapore experience
Gowri Gopalakrishna, PhD (Epidemiology)
Session 1: Infectious diseases in the Singapore setting
Session 2: SARS Case Study: Lessons learnt from the Singapore
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018GlobaLab.biz 2
SARS Case Study: Lessons learnt from the Singapore experience
Session 3: Readiness for Future Outbreaks
Lesson Objectives
1. Concept of outbreak investigation & Operational steps in outbreak investigation
2. Outbreak control and investigation: the Singapore context using SARS as an example
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
example
3. Emergency preparedness & Hospital Readiness in the era of Emerging Infectious Diseases
3
Terminology – what’s in a name?
• Epidemic: the occurrence of more cases of disease, injury, or other health condition than expected in a given area or among a specific group of persons during a particular period. Usually, the cases are presumed to have a common cause or to be related to one another in some way (see also outbreak)
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
• Epidemic curve: a histogram that displays the course of an outbreak or epidemic by plotting the number of cases according to time of onset
• Epidemic period: the time span of an outbreak or epidemic
4
• Outbreak: Sometimes distinguished from an epidemic as more localized, or the term less likely to evoke public panic (see also epidemic)
• Common-source: results from persons being exposed to the same harmful influence (e.g., an infectious agent or toxin). The exposure period can be brief or can extend over days, weeks, or longer, with the exposure being either intermittent or continuous (e.g. work related
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
exposure being either intermittent or continuous (e.g. work related toxin)
• Outbreak, point-source: a common source outbreak in which the exposure period is relatively brief so that all cases occur within one incubation period (e.g. food outbreaks)
• Outbreak, propagated: an outbreak that spreads from person to person rather than from a common source (e.g. SARS)
5
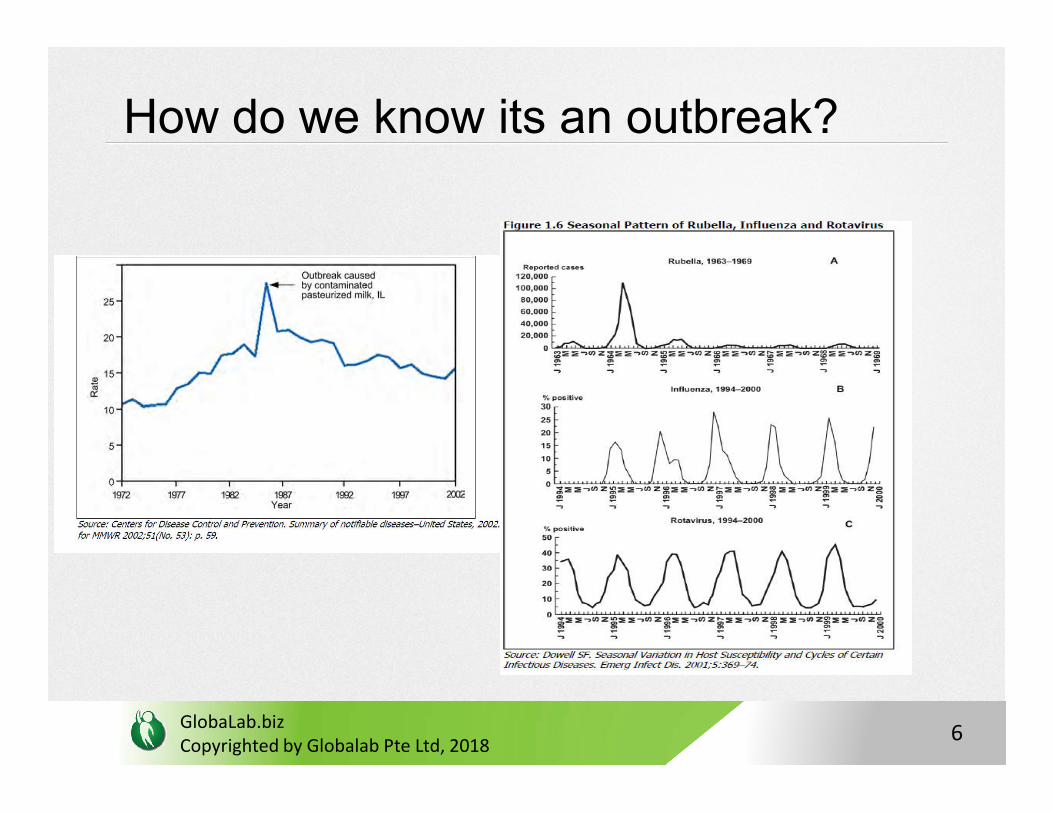
How do we know its an outbreak?
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
6
How do we detect one?
• Routine surveillance : the 5 Ws of descriptive epi
“the what, who, where, when and the how”
• What = is the health issue of concern
• Who = population/person(s) affected
• Where= place/location
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
• Where= place/location
• When= time
• Why/how = cause/tranmission mode..
TIME, PLACE, PERSON
7
Time, Place, Person
• Time
- Disease occurence changes with time eg. influenza = seasonal changes >> implement control measure in time e.g. Vaccination, mosquito spraying
- Diseases that can occur any time e.g. Salmonellosis, Hep B,
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
- Diseases that can occur any time e.g. Salmonellosis, Hep B, other food borne, zoonotic outbreaks
- >> important to establish this is an outbreak needing intervention
8
• Place
- Provides insight into the geographic extent of the problem and its geographic variation
- Refers not only to place of residence but to any geographic location relevant to disease occurrence e.g. site of
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
location relevant to disease occurrence e.g. site of employment, school district, hospital unit, or recent travel destinations
- Unit may be as large as a continent or country or as small as a street address, hospital wing, or operating room
9
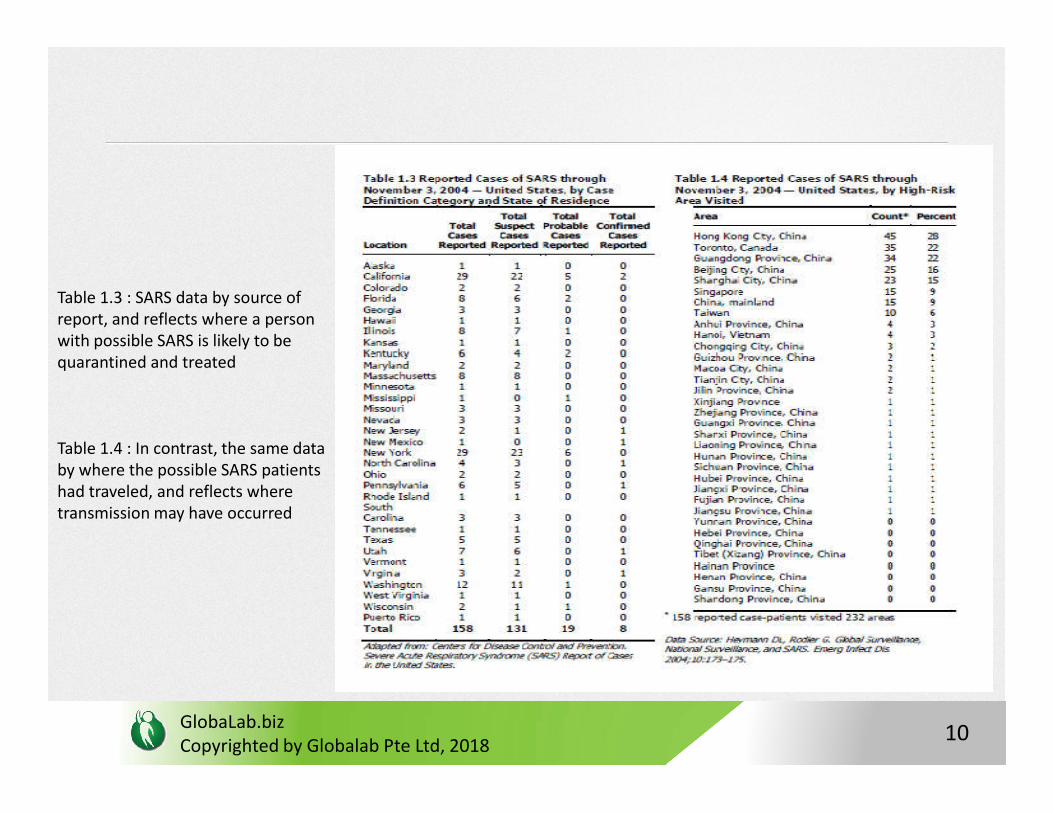
Table 1.3 : SARS data by source of report, and reflects where a person with possible SARS is likely to be quarantined and treated
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
Table 1.4 : In contrast, the same data by where the possible SARS patients had traveled, and reflects where transmission may have occurred
10
• Maps can also be used inplace of tables to describe place
>> provides a more striking visual display of place data
>> On a map, different numbers or rates of disease can be depicted using different shadings, colors, or line patterns
Spot maps >> used for clusters or outbreaks with a limited number of cases. A dot or X is placed on the location that is most relevant, usually where each victim lived or worked; details like points of exposure can be included on map
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
11
Why is analysing by place useful?
• For implementing control meausres and understanding spread
>> identify communities at increased risk of disease by generating hypotheses to test with additional studies. E.g:
Is a community at increased risk because of characteristics of the people in the community such as genetic susceptibility, lack of immunity, risky behaviors, or exposure to local toxins or contaminated food?
Can the increased risk be attributed to a particularly virulent strain, hospitable
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
Can the increased risk be attributed to a particularly virulent strain, hospitable breeding sites, or availability of the vector that transmits the organism to humans?
Can the increased risk be attributed to the environment that brings the agent and the host together, such as crowding in urban areas, or more homes being built in wooded areas close to vectors that can spread disease to humans?
12
• Person
- Refers to personal characteristics which may affect illness:
e.g. age, sex, race, biologic characteristics (immune status), activities (occupation, leisure activities, use of medications/tobacco/drugs), or the conditions under which they live (socioeconomic status, access to medical care)
- Age and sex: two most commonly analyzed “person” characteristics
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
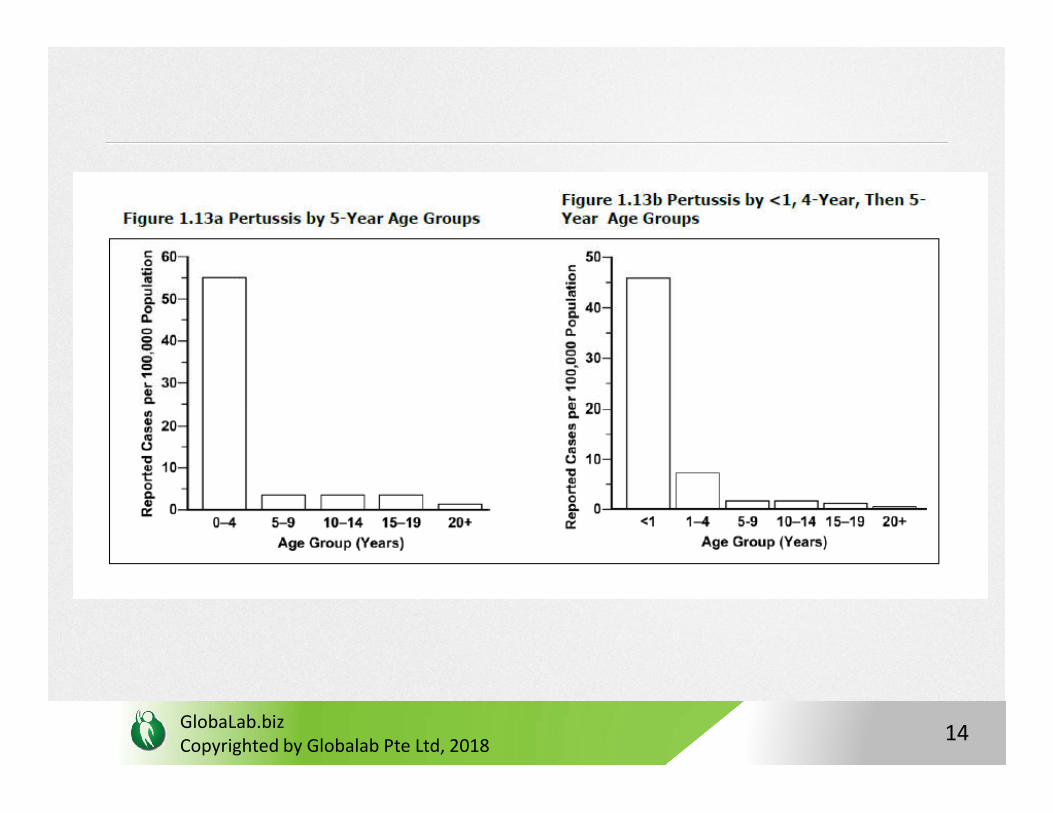
Age: factors vary with age include: susceptibility, opportunity for exposure, latency or incubation period of the disease, and physiologic response (which affects disease development).
When analyzing data by age, use age groups that are narrow enough to detect any age-related patterns that may be present
13
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
14
- Ethnic, racial factors: race, nationality, religion, or social groups such as tribes and other geographically or socially isolated groups
Differences may reflect differences in susceptibility or exposure
- Socioeconomic factors: difficult to quantify, made up of many variables e.g. occupation, family income, educational achievement, living conditions, and social standing.
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
standing.
But may not accurately reflect the overall concept. Nevertheless, occupation, family income, and educational achievement commonly used
In general, frequency adverse health conditions increases with decreasing socioeconomic status
15
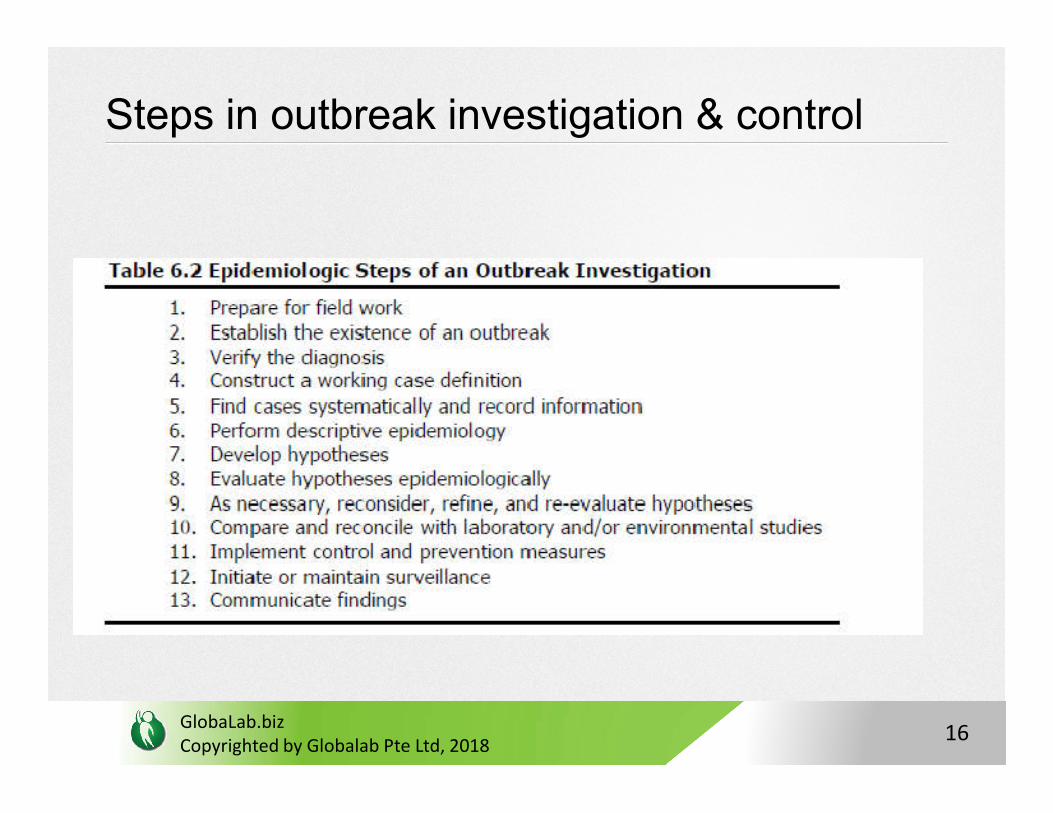
Steps in outbreak investigation & control
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
16
• Steps in conceptual order;
• In practice, several steps may be done at the same time, or the circumstances of the outbreak may dictate that a different order be followed
For example, first three listed steps is highly variable — a health department often verifies the diagnosis and establishes the existence of an outbreak before deciding that a field investigation is warranted
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
that a field investigation is warranted
Conceptually, control measures come after hypotheses have been confirmed, but in practice control measures are usually implemented as soon as the source and mode of transmission are known, which may be early or late in investigation
17
Setting the scene: Play between Infectious Diseases and
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
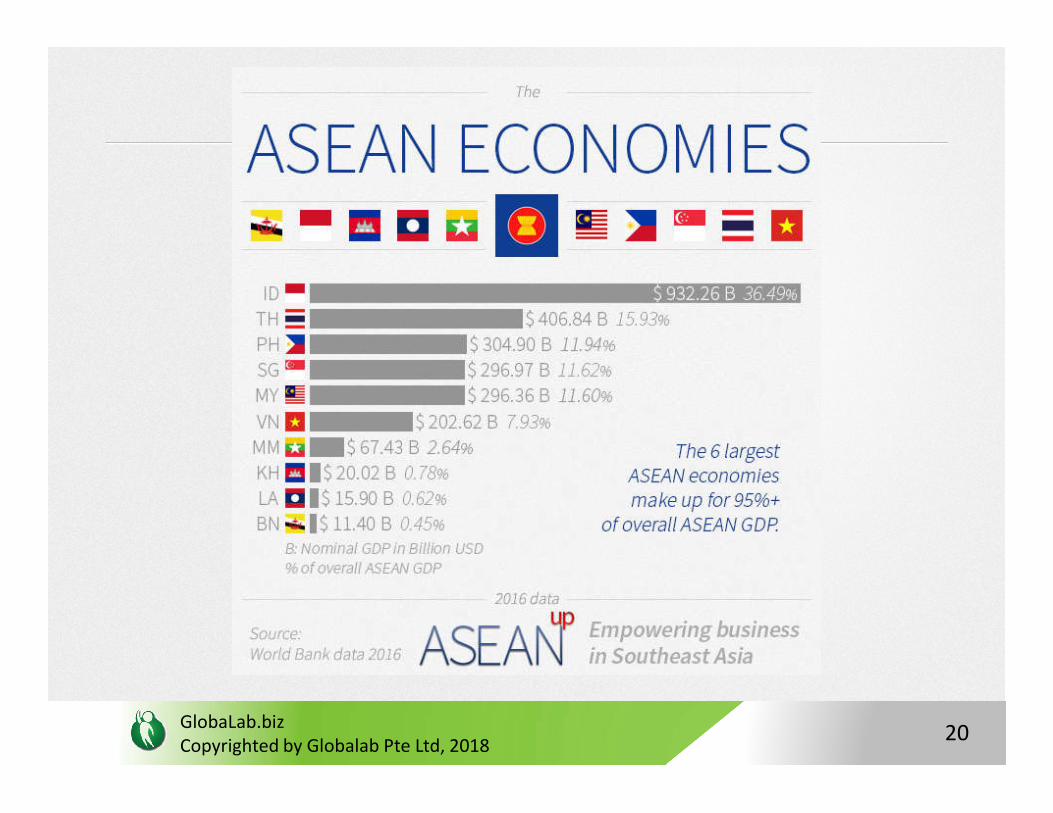
Play between Infectious Diseases and Economics
18

GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
19
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
20
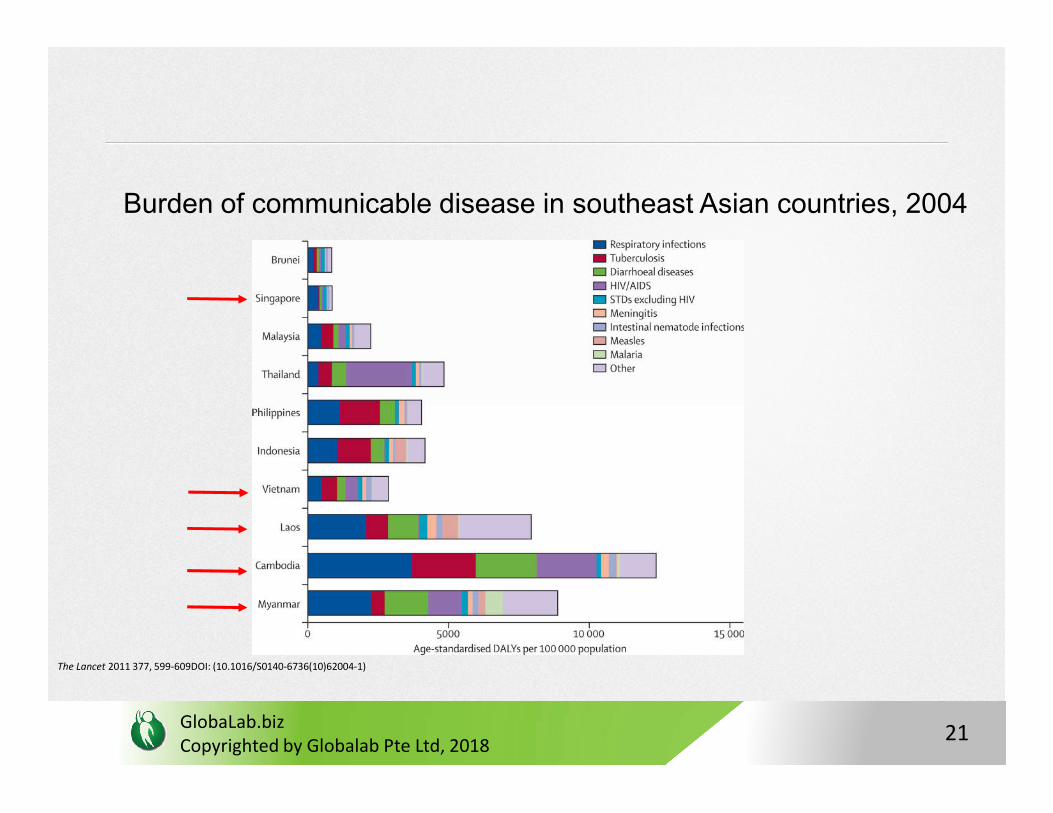
Burden of communicable disease in southeast Asian countries, 2004
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
The Lancet 2011 377, 599-609DOI: (10.1016/S0140-6736(10)62004-1)
21
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
22
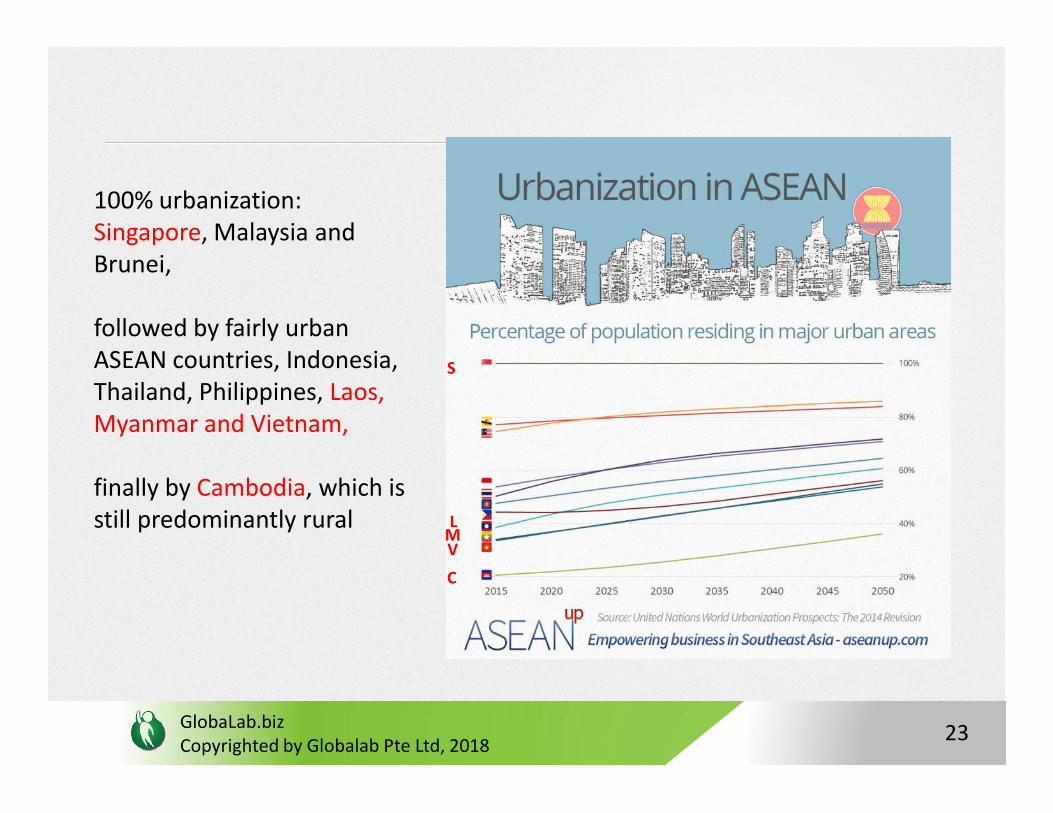
100% urbanization: Singapore, Malaysia and Brunei,
followed by fairly urban ASEAN countries, Indonesia, Thailand, Philippines, Laos,
S
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
Thailand, Philippines, Laos, Myanmar and Vietnam,
finally by Cambodia, which is still predominantly rural
VM
C
L
23
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
24
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
25
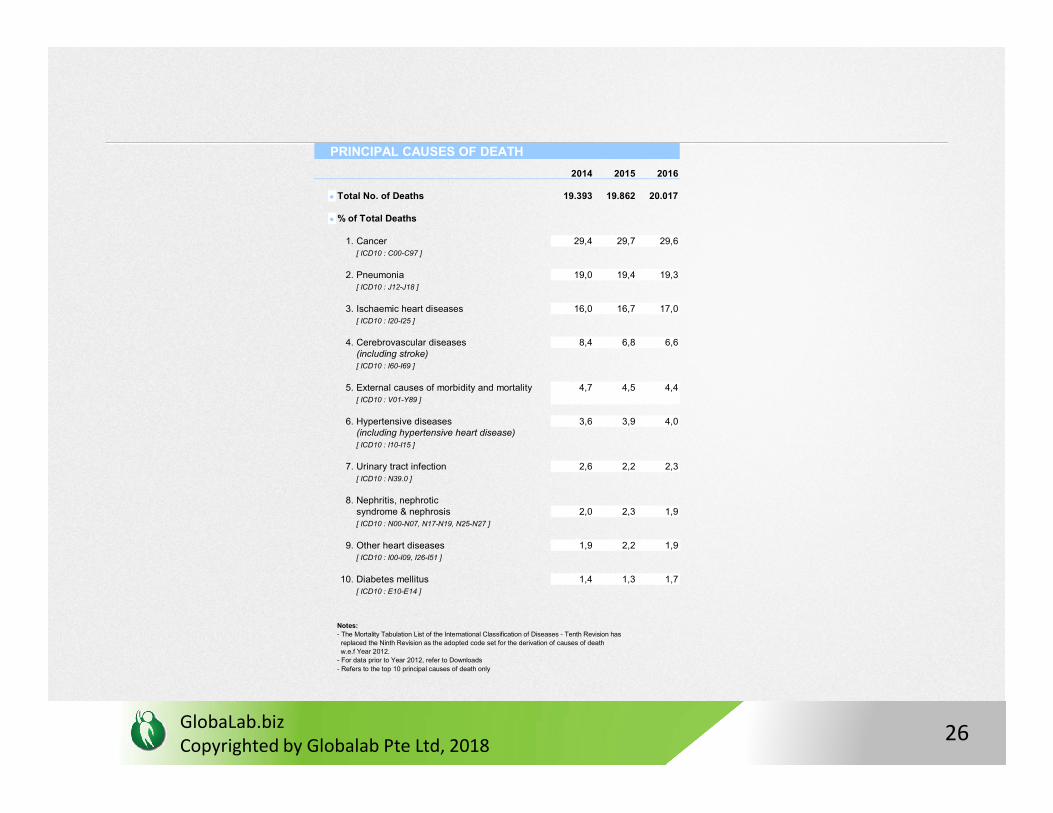
PRINCIPAL CAUSES OF DEATH
2014 2015 2016
Total No. of Deaths 19.393 19.862 20.017
% of Total Deaths
1. Cancer 29,4 29,7 29,6[ ICD10 : C00-C97 ]
2. Pneumonia 19,0 19,4 19,3[ ICD10 : J12-J18 ]
3. Ischaemic heart diseases 16,0 16,7 17,0[ ICD10 : I20-I25 ]
4. Cerebrovascular diseases 8,4 6,8 6,6(including stroke)[ ICD10 : I60-I69 ]
5. External causes of morbidity and mortality 4,7 4,5 4,4[ ICD10 : V01-Y89 ]
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
6. Hypertensive diseases 3,6 3,9 4,0(including hypertensive heart disease)[ ICD10 : I10-I15 ]
7. Urinary tract infection 2,6 2,2 2,3[ ICD10 : N39.0 ]
8. Nephritis, nephrotic syndrome & nephrosis 2,0 2,3 1,9[ ICD10 : N00-N07, N17-N19, N25-N27 ]
9. Other heart diseases 1,9 2,2 1,9[ ICD10 : I00-I09, I26-I51 ]
10. Diabetes mellitus 1,4 1,3 1,7[ ICD10 : E10-E14 ]
Notes:
- The Mortality Tabulation List of the International Classification of Diseases - Tenth Revision has
replaced the Ninth Revision as the adopted code set for the derivation of causes of death
w.e.f Year 2012.
- For data prior to Year 2012, refer to Downloads
- Refers to the top 10 principal causes of death only
26
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
27
Infectious Disease Outbreaks:The Singapore Context
• Infectious Diseases Act (IDA) governs the list of notifiable diseases stipulated under the First Schedule. As of 2016, six diseases viz. botulism, tetanus, leptospirosis, murine typhus, rabies and Japanese encephalitis were added to the list of 43
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
28
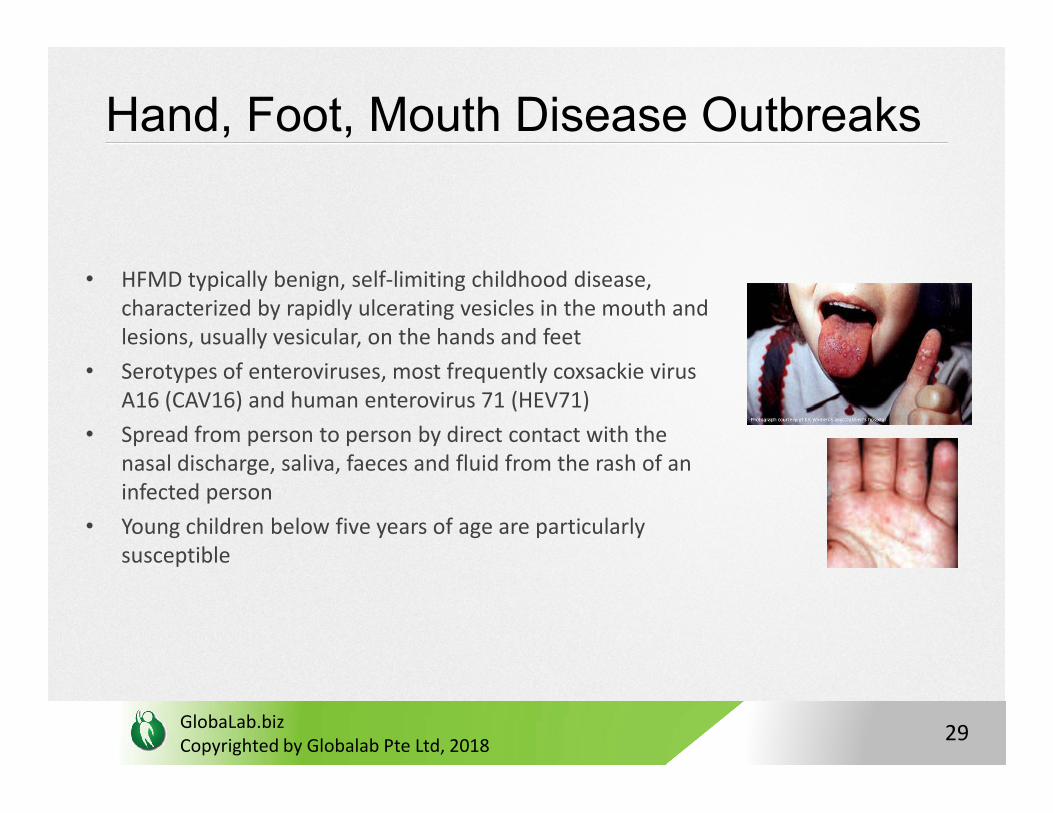
Hand, Foot, Mouth Disease Outbreaks
• HFMD typically benign, self-limiting childhood disease, characterized by rapidly ulcerating vesicles in the mouth and lesions, usually vesicular, on the hands and feet
• Serotypes of enteroviruses, most frequently coxsackie virus A16 (CAV16) and human enterovirus 71 (HEV71)
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
A16 (CAV16) and human enterovirus 71 (HEV71)
• Spread from person to person by direct contact with the nasal discharge, saliva, faeces and fluid from the rash of an infected person
• Young children below five years of age are particularly susceptible
29
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
30
Control & Prevention Measures
• System of surveillance for the disease, based on notifications from child-care centers, in April 1998
• Reporting legally mandatory on October 1, 2000
• Concurrent with the intensified surveillance, an interministry and interhospitalHFMD Task Force, composed of representatives from various Ministries, as well as virologists and pediatricians >> formulate a preparedness response plan to monitor and manage severe HFMD outbreaks in Singapore
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
monitor and manage severe HFMD outbreaks in Singapore
• Since 2010, additional measures: Childcare centres or kindergartens with prolonged HFMD transmission had their names published on the MOH website and were subsequently closed for ten days if disease transmission was prolonged for more than 16 days.
• Public education enhanced
31
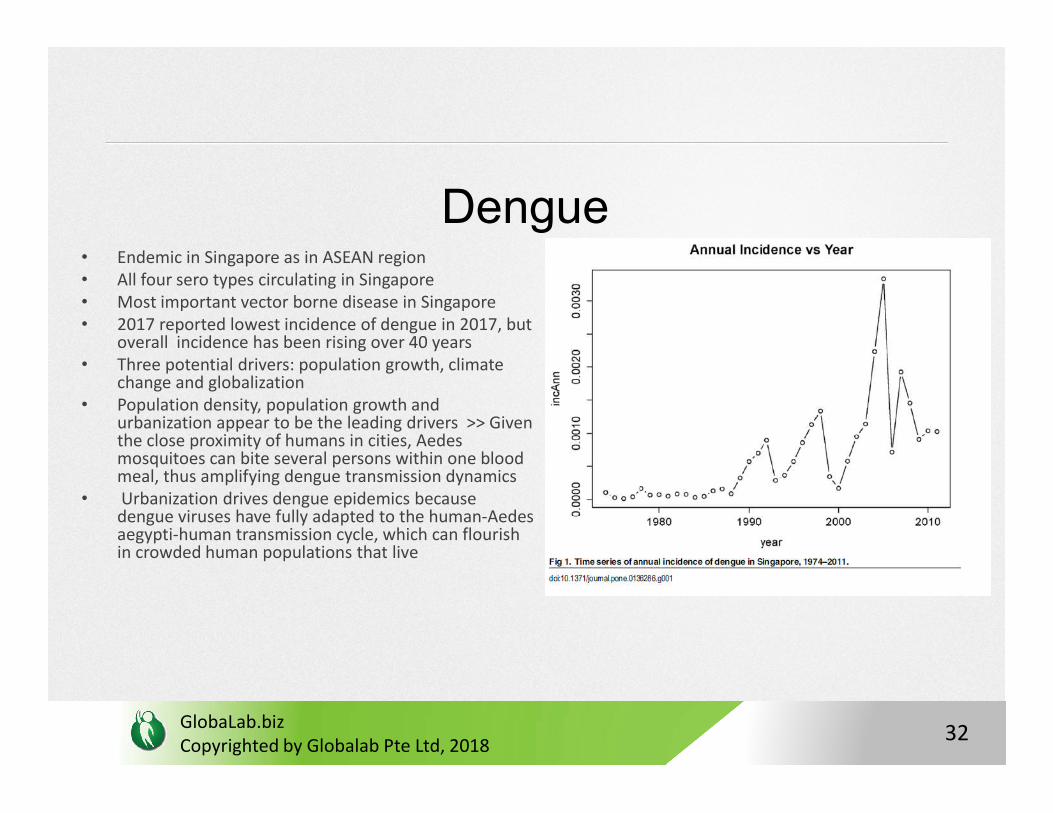
Dengue• Endemic in Singapore as in ASEAN region• All four sero types circulating in Singapore• Most important vector borne disease in Singapore• 2017 reported lowest incidence of dengue in 2017, but
overall incidence has been rising over 40 years• Three potential drivers: population growth, climate
change and globalization• Population density, population growth and
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
• Population density, population growth and urbanization appear to be the leading drivers >> Given the close proximity of humans in cities, Aedesmosquitoes can bite several persons within one blood meal, thus amplifying dengue transmission dynamics
• Urbanization drives dengue epidemics because dengue viruses have fully adapted to the human-Aedesaegypti-human transmission cycle, which can flourish in crowded human populations that live
32
Control & Prevention
• Suppressing vector population is the key
• Vector control carried out by National Environmental Agency (NEA); clinical case management and surveillance by Ministry of Health (MOH)
• Close coordination between two sectors imperative to tackle >> daily communication of surveillance data enables prompt vector control response by
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
communication of surveillance data enables prompt vector control response by NEA
• NEA’s Environmental Health Institute (EHI) has studied various novel mosquito control methods over the past six years >> Wolchabia suppression technology over the A. aegypti
33
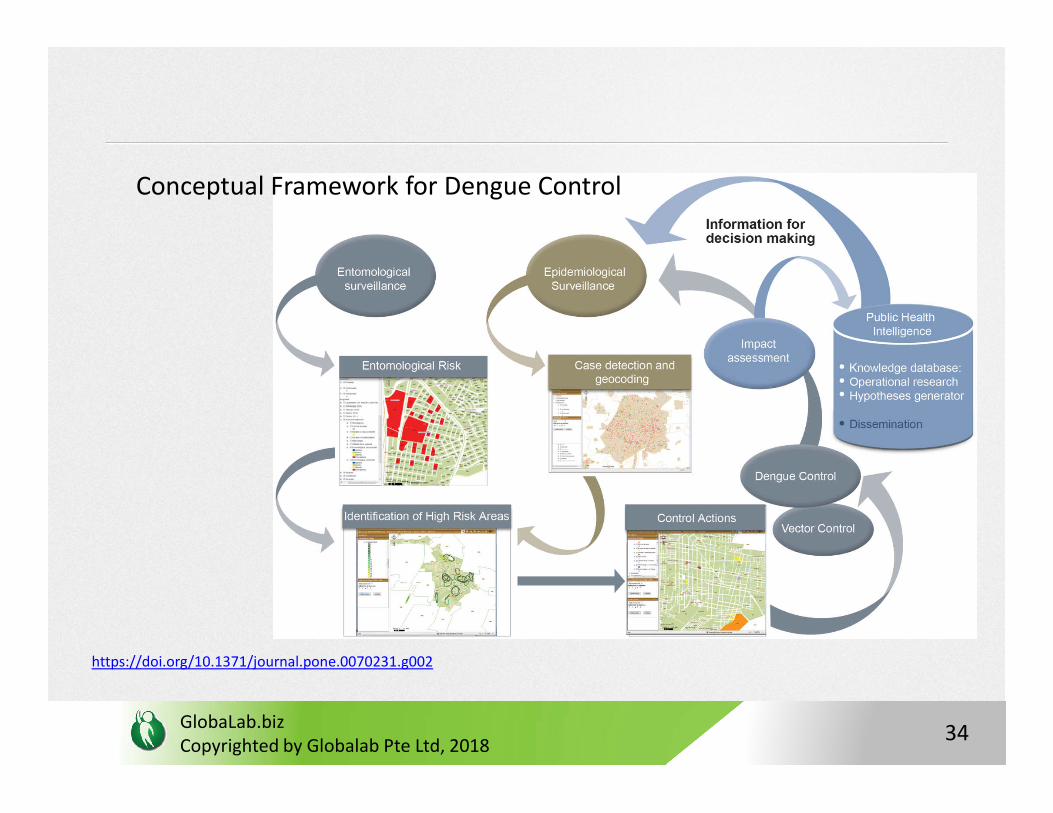
Conceptual Framework for Dengue Control
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
https://doi.org/10.1371/journal.pone.0070231.g002
34
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
35
Specific measures during outbreak include:
1. Enhanced case surveillance measures for those with clinical symptoms plus subsizided laboratory testing service set up during 2013-14 outbreak
2. Projection of case numbers based on the statistical model projection >> allowed for extension of diagnostic services, stockpiling diagnostic reagents, hospitals to plan for extra consultations and admissions
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
consultations and admissions
3. Expansion of virus surveillance for targeted vector control >> GIS combined with expanded serotype and genotype surveillance data allowed for detailed understanding of spatial & temporal spread, targeted vector control at new sites
36
Specific measures during outbreak include:
4. Early launch of the dengue campaign to promote community awareness of dengue situation and prevention, colour-coded alert system launched through Dengue Community Alert System to keep residents informed about active disease clusters, dengue volunteers to support community outreach activities through seminars, talks, roadshows and media
5. Enhanced source reduction for mosquito breeding through an accelerated
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
5. Enhanced source reduction for mosquito breeding through an accelerated premise inspection programme >> Apart from homes, daily checks on common ground areas, public areas and congregation areas for potential mosquito breeding spots, inspection frequency accelerated to cover all premises within the boundary of disease clusters
37
6. Integrated 3P taskforce set up >> Inter-Agency Dengue Task Force comprising 27 stakeholders from the 3P sectors to ensure the planning and implementation of operational activities within each sector was aligned
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
38
Duke NUS Video on Dengue
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
39
Hepatitis C Cluster Outbreak 2015
• Unique outbreak of acute Hep C in a cluster of 25 renal transplant patients in one hospital
• Represents a cluster outbreak of a hospital acquired infection (HAI)
• Investigations showed main cause of outbreak was due to lapses in infection control practices among hospital staff in
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
lapses in infection control practices among hospital staff in two wards
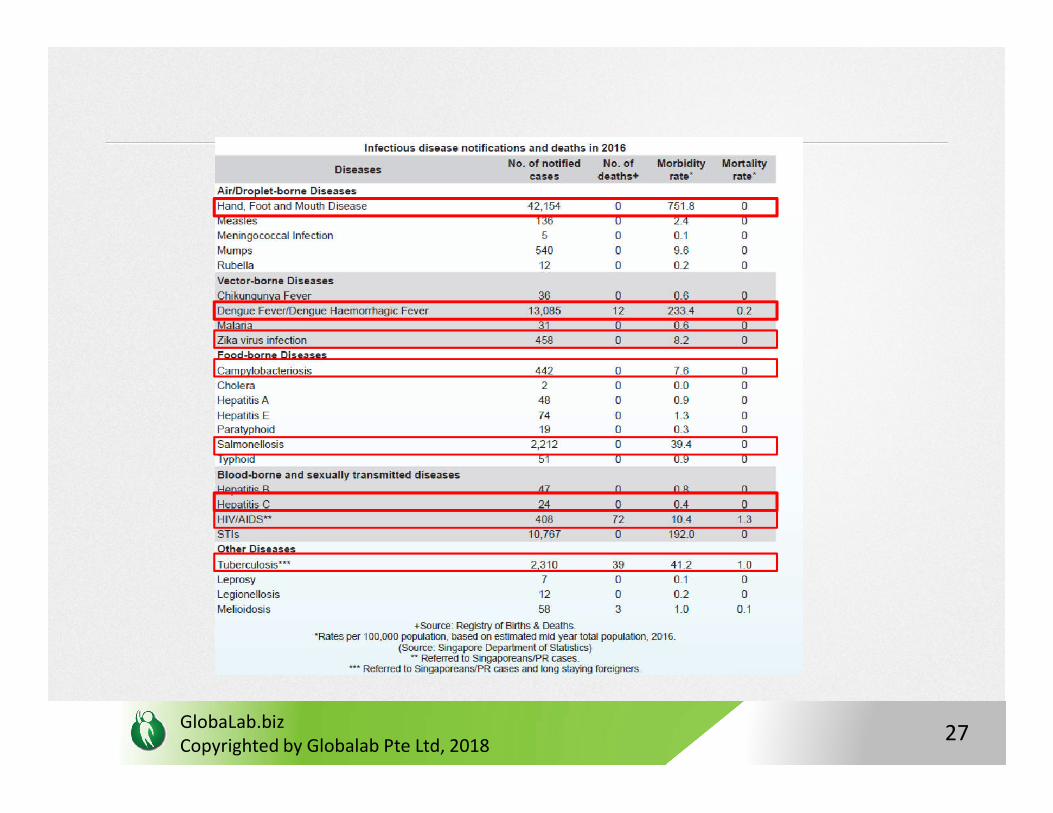
• Hep C in itself is not endemic with a low case number annually (n=24 in 2016; morbidity <1 and 0 mortality)
40
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
41
HAI and Cluster Outbreak 2015 : Lessons Learnt
• Singapore’s current surveillance system works well for community outbreaks of known infectious diseases, however the HCV outbreak highlighted a gap in dealing with unusual HAI outbreaks, resulting in delays
• Independent Review Committee Set Up and the following
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
• Independent Review Committee Set Up and the following recommendations were made to strength the system
42
(i) improvements to be made in infection control practices and compliance in all healthcare institutions;
(ii) improvements to be made in how HAIs are monitored and responded to at the national level;
(iii) designation of a single team within MOH to carry out surveillance, identify and investigate potential outbreaks, ensure
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
surveillance, identify and investigate potential outbreaks, ensure adequate expertise nationally to facilitate outbreak investigation; and
(iv) strengthening of the escalation framework for HAIs and events of unusual risk
43
Session 2:SARS Case Study: Lessons learnt from
the Singapore experience
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
44
Index Case
• Index case A: 22-year-old female
• Local resident who reported ill with fever and dry cough on her way home from a “free-and-easy” holiday in Hong Kong on 25 February 2003
• Admitted into TTSH hospital on 1 March 2003 with atypical pneumonia
• Had been staying at the same hotel in HK as the source case
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
• Had been staying at the same hotel in HK as the source case
• A total of 109 cases were eventually infected by Index A out of the 238 total number of cases (46%)
45
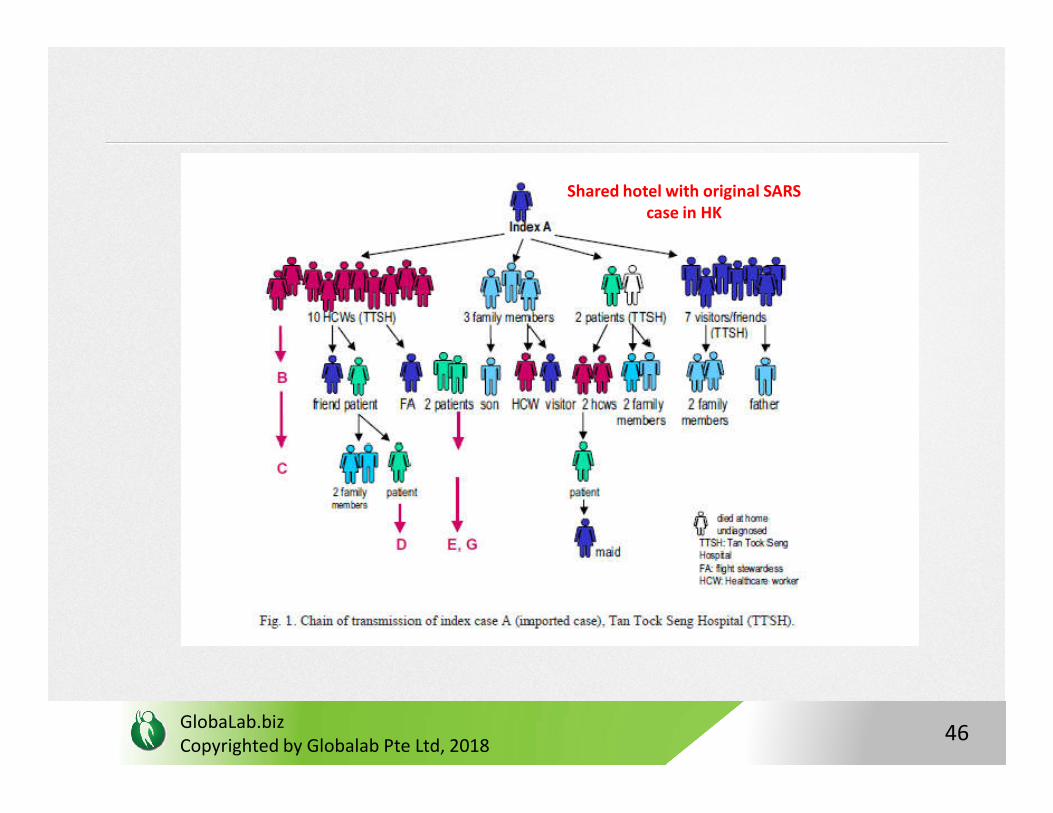
Shared hotel with original SARS case in HK
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
46
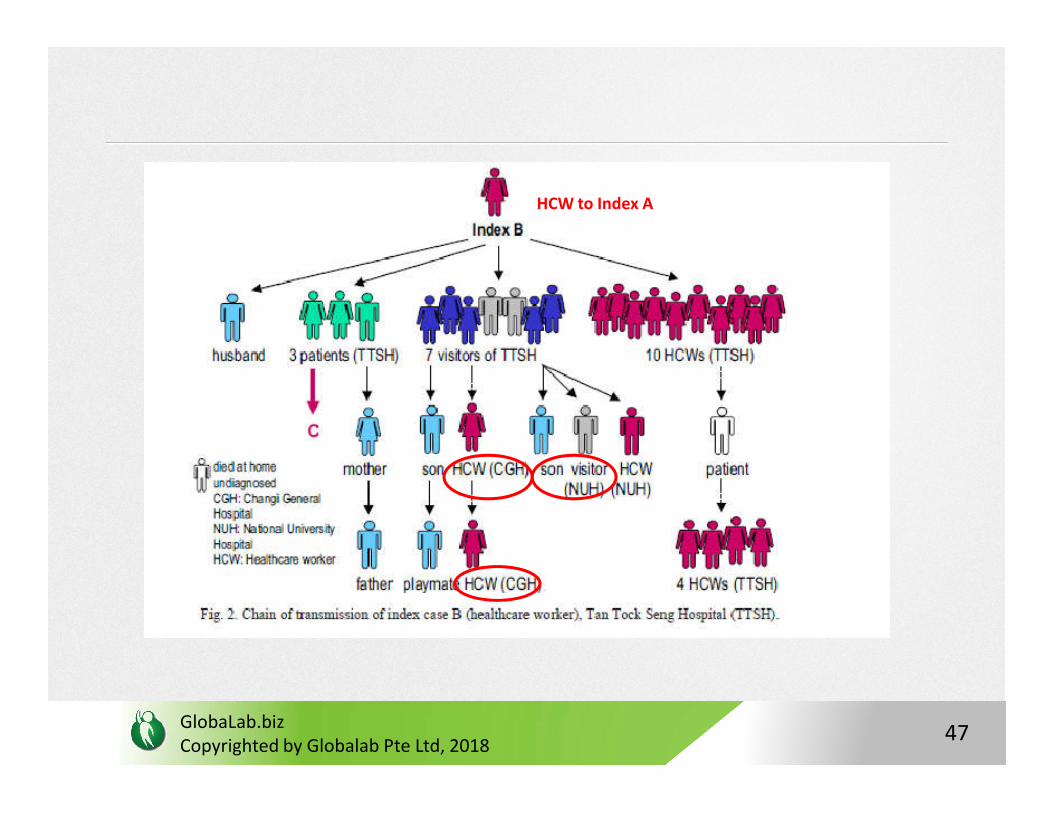
HCW to Index A
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
47
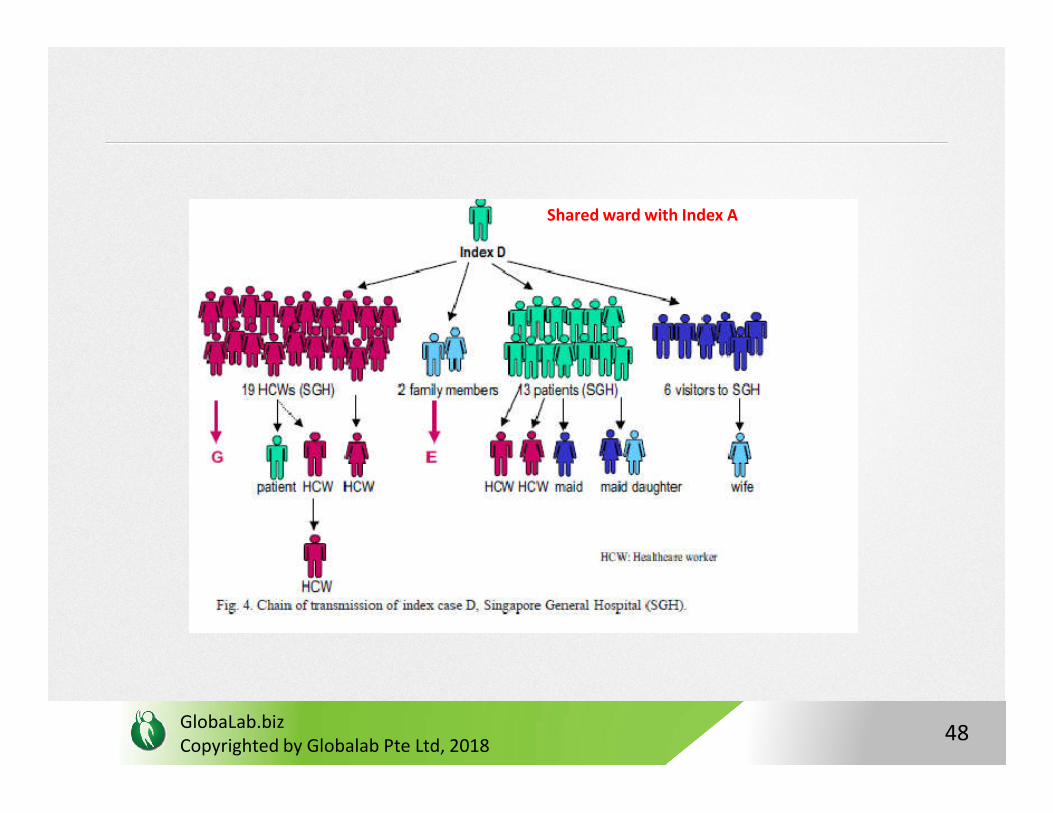
Shared ward with Index A
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
48
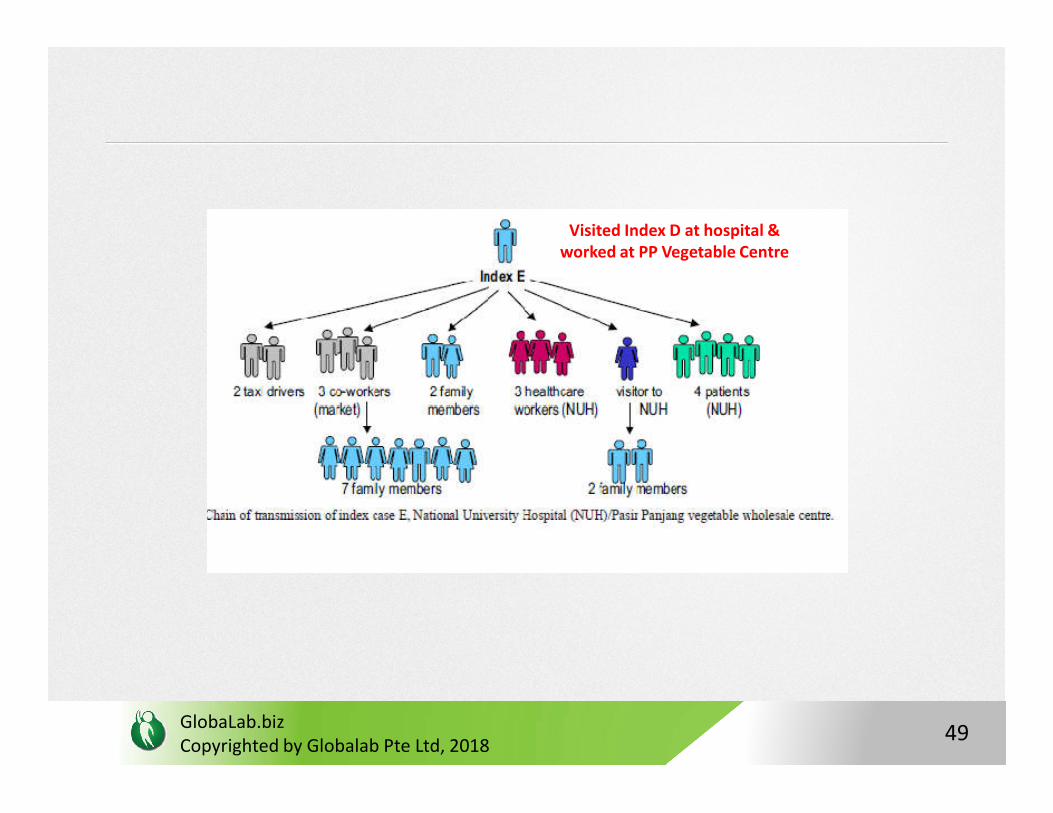
Visited Index D at hospital & worked at PP Vegetable Centre
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
49
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
50
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
51
Infe
ctio
n c
on
tro
l me
asu
res
imp
lem
en
ted
in T
TSH
Pat
ien
t A
iso
late
d
Pat. A diagnosed
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
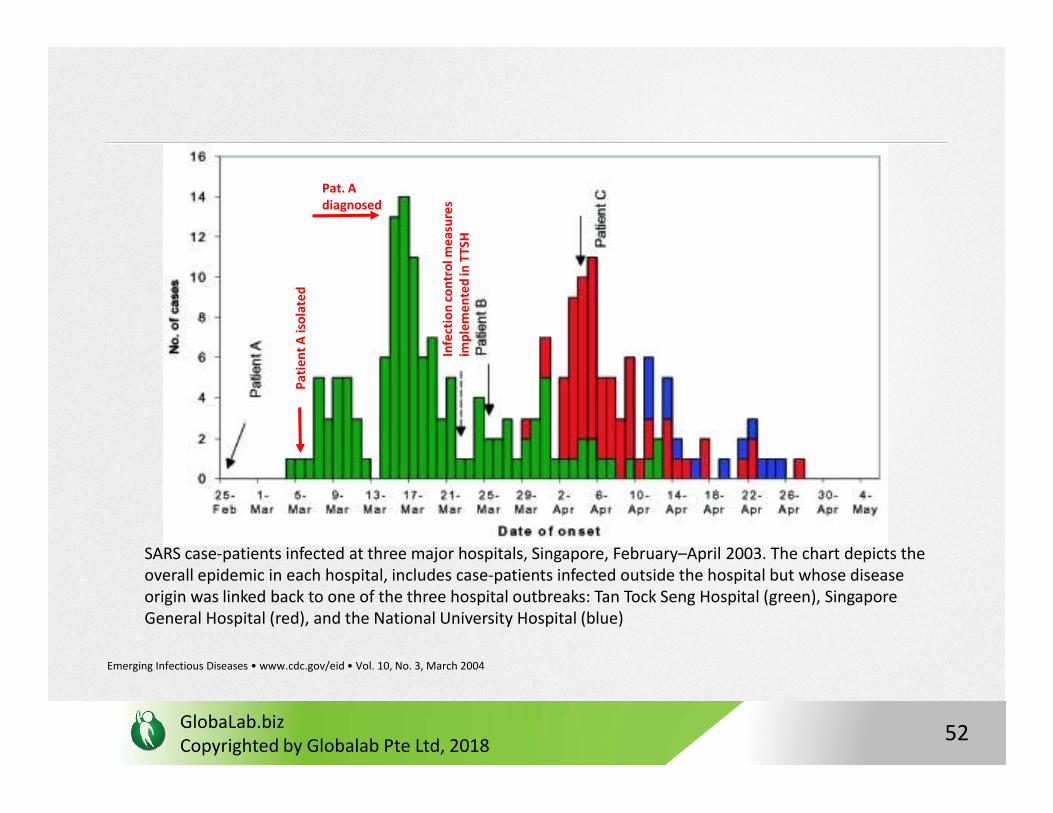
SARS case-patients infected at three major hospitals, Singapore, February–April 2003. The chart depicts the overall epidemic in each hospital, includes case-patients infected outside the hospital but whose disease origin was linked back to one of the three hospital outbreaks: Tan Tock Seng Hospital (green), Singapore General Hospital (red), and the National University Hospital (blue)
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 10, No. 3, March 2004
52
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
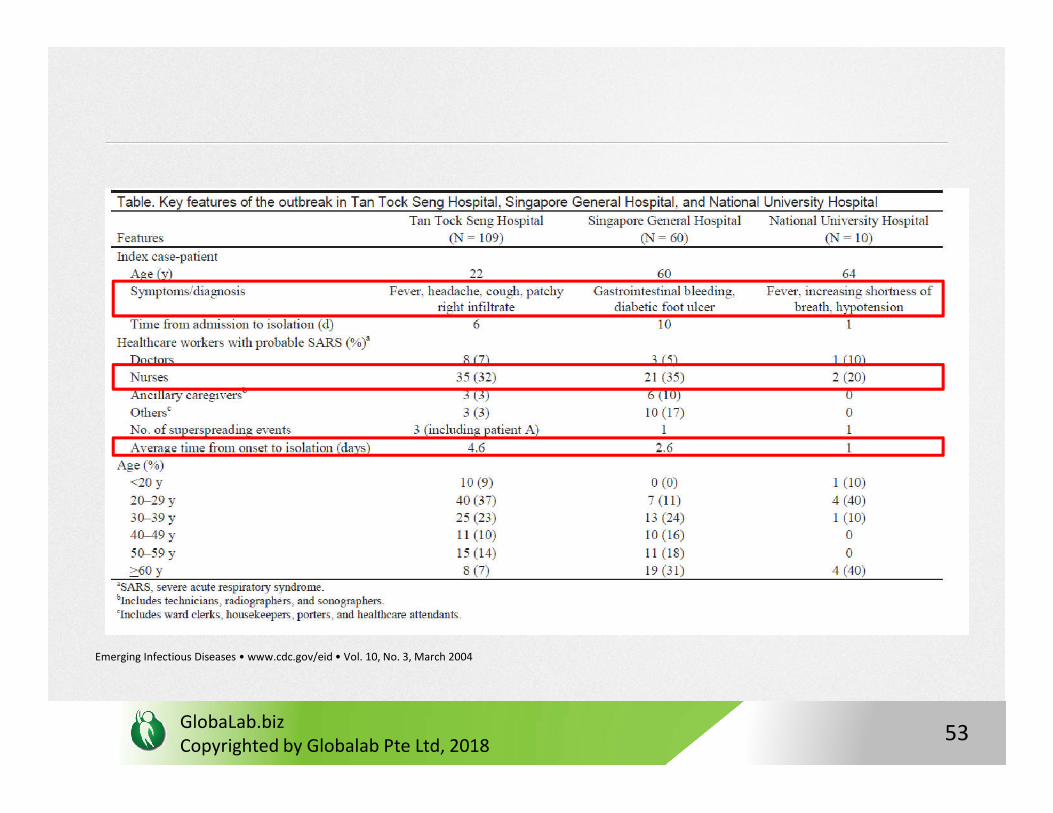
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 10, No. 3, March 2004
53
Prevention & Control Measures
1. Three inter-agency high level committees/ Taskforces were set up:
i. MOH SARS Task Force, which was formed on 15 March 2003 (same time as diagnosis of Index A) = all chief executive officers of all hospitals, chairmen of medical boards, infectious disease physicians, epidemiologists and virologists
ii. Ministerial Committee on SARS (chaired by the Minister for Home Affairs) was established on 7 April to provide political guidance and quick strategic decisions to minimise the socioeconomic impact of SARS
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
to minimise the socioeconomic impact of SARS
iii. Ministerial SARS Combat Unit appointed to work closely with the public and private hospitals and other healthcare institutions to prevent and control SARS
2.Effective implementation of control measures through IDA and Private Hospitals and Medical Clinics Act
54
3. Stringen infection control procedures @ hospitals, Nursing homes and healthcare institutions
4. Triage @ POC e.g. hospital emergency, outpatient clinics
5. Widening surveillance net through expanded case
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
5. Widening surveillance net through expanded case definition
6. Case finding intensified with thrice-daily temperature surveillance of all HCWs in every institution and active surveillance for clusters of febrile patients, especially among the immunocompromised, and staff from the same work area
55
7.Special Hospital Containment Measures implemented:
i. TTSH dedicated SARS hospital;
ii. Strict enforcement of the proper use of PPE (test-fitted N95 mask, gowns, gloves and goggles/protective eye gear and powered air purified respirator for high-risk procedures such as intubation),
iii. Control of visitors, restriction of movements of HCWs (including
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
iii. Control of visitors, restriction of movements of HCWs (including confining their practice to one institution) and patients (readmission to the same hospital within 21 days after discharge), and close monitoring of discharged patients from SARS-affected wards
iv. All inpatients with chronic medical conditions were placed on home quarantine for 10 days upon discharge
56
8. Border Checkpointsi. Health alert advising travellers to avoid SARS-affected countriesii. Limit importation of new cases through intensive screening at air, land and sea entry portalsiii. SARS Health declaration cards for contact tracing
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
9. Contact Tracing Centre established and home quarantine orders issued
10. Operations Division set up within MOH responsible for the prevention and control of outbreaks of major infectious diseases, and command and control of all medical resources during a crisis.
57
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
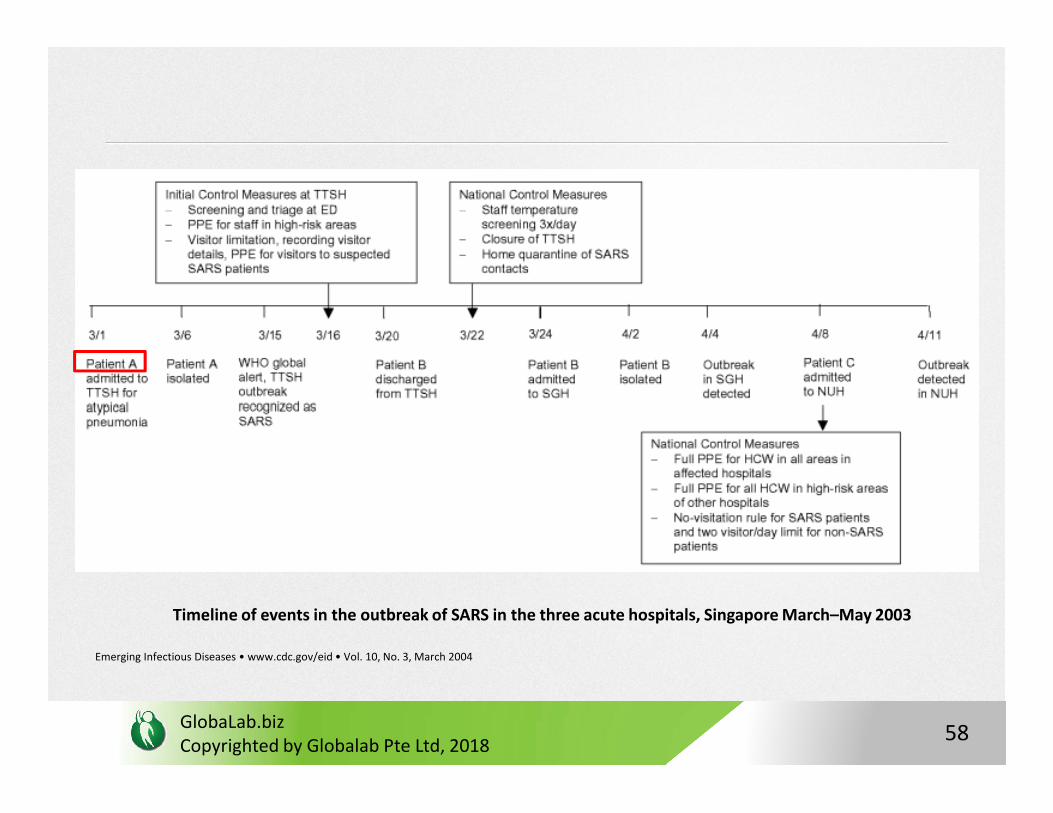
Timeline of events in the outbreak of SARS in the three acute hospitals, Singapore March–May 2003
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 10, No. 3, March 2004
58
Session 3:
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
Readiness for Future Outbreaks
59
Challenges for a city/state
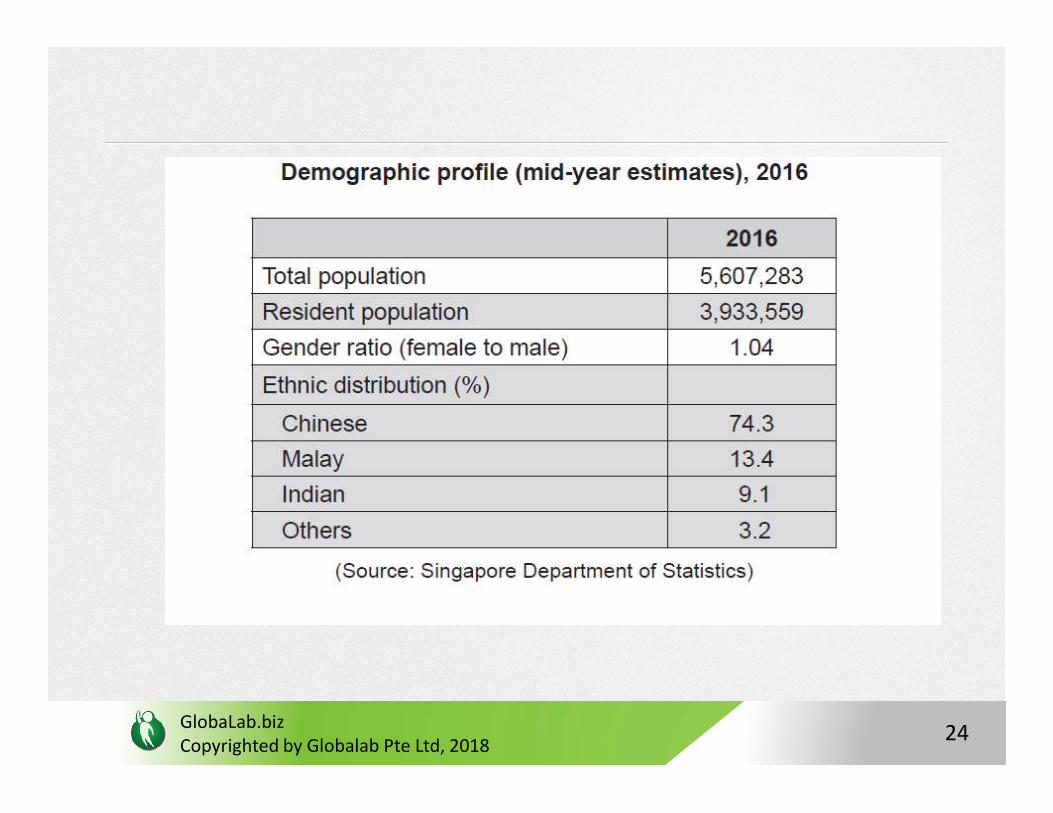
• An island city state with a population of about 5.6 million
• As Singapore continues to develop into a major global trade and travel hub, it is imperative that Singapore remains vigilant to public health threats, both locally and overseas, to safeguard the health of our population.
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
safeguard the health of our population.
60
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
61
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
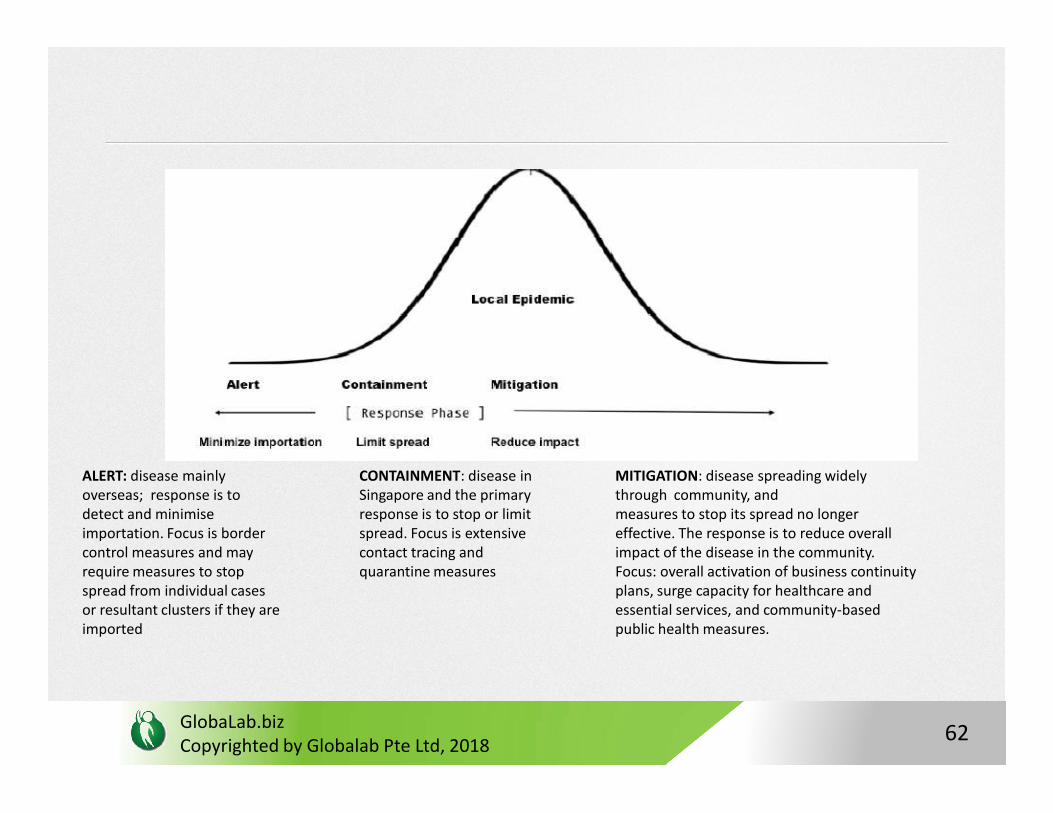
ALERT: disease mainly overseas; response is to detect and minimiseimportation. Focus is border control measures and mayrequire measures to stop spread from individual cases or resultant clusters if they are imported
CONTAINMENT: disease in Singapore and the primaryresponse is to stop or limit spread. Focus is extensive contact tracing and quarantine measures
MITIGATION: disease spreading widely through community, andmeasures to stop its spread no longer effective. The response is to reduce overall impact of the disease in the community. Focus: overall activation of business continuity plans, surge capacity for healthcare and essential services, and community-based public health measures.
62
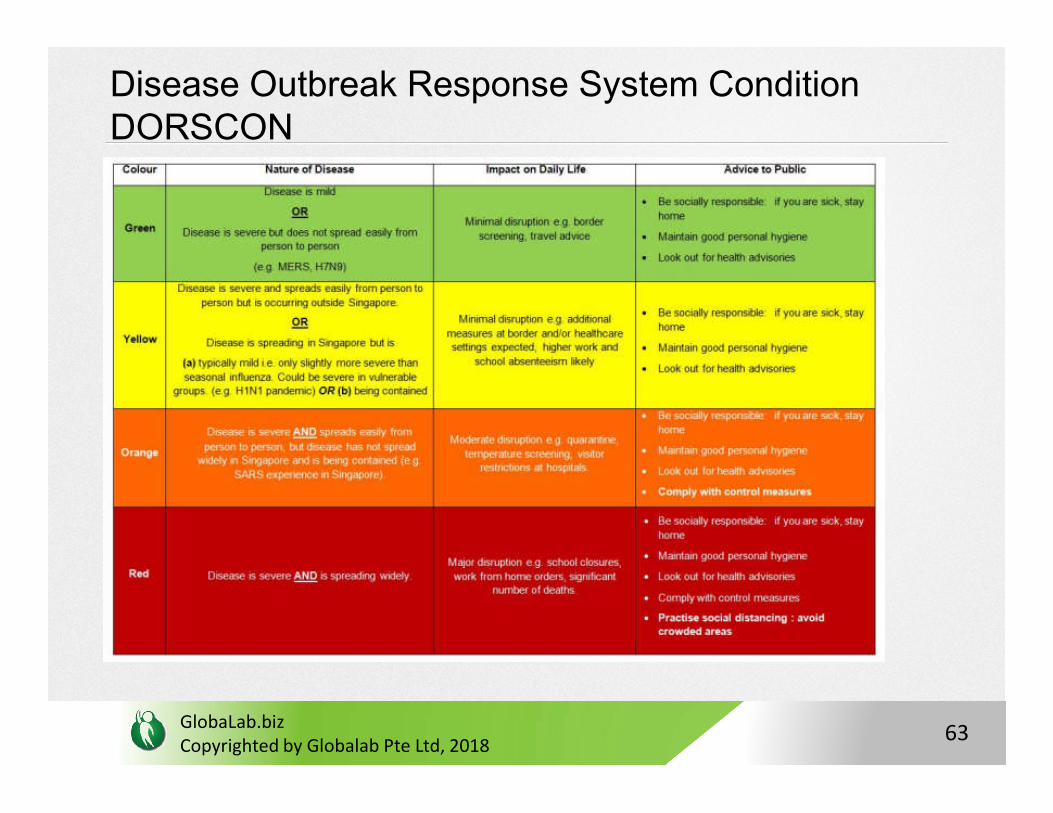
Disease Outbreak Response System Condition DORSCON
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
63
Homefront Crisis Management System
• HCMS: national framework for coordinating whole-of-government planning and response during a homefront crisis that has national significance and impact
• The HCMS is led by a Homefront Crisis Ministerial Commitee(HCMC) which is chaired by the Minister for Home Affairs to
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
(HCMC) which is chaired by the Minister for Home Affairs to provide strategic and political guidance during a crisis
64
SARS Success in Singapore
1. Timely global alerts, travel advisories, border screening at land, sea, air entry points
2. Heightened vigilance in healthcare facilities
3. National concerted effort via Taskforce, Inter-Ministry coordination
4. Operations Command Centre
5. Dedicated Containment Hospital
6. Continued surveillance and strict compliance with guidelines for
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
6. Continued surveillance and strict compliance with guidelines for
infection control
>> proper biosafety containment<<
65
SARS Success In Singapore
General preventive public health measures were very effective in preventing the transmission to community:
• Early case detection e.g., daily temperature monitoring during outbreaks,
• Rapid isolation,
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
• Effective contact tracing,
• Quarantine of exposed persons,
• Surveillance of fever clusters and atypical pneumonia,
• Dedicated ambulance service to transport all possible cases to a SARS-designated hospital.
66
Spread through Healthcare workers
• Among the SARS affected countries, Vietnam (57%, 36/63), Canada (43%, 109/251), and Singapore (41%, 97/238) had the largest % of HCW SARS cases
• Control was crucial at healthcare centres to prevent them becoming epicenters and spread to community
- HCW surveillance and immediate isolation of new cases >>
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
- HCW surveillance and immediate isolation of new cases >> CRUCIAL
- If inadvertently exposed, unprotected, then a quarantined for 10 days before return to work
67
Hospital Readiness in Outbreaks
• In an epidemic, healthcare personnel and facilities stretched. Impertative to prevent attrition of healthcare professionals or the closure of health facilities
>> self-administered questionnaire among frontline HCWs
• found 57% experienced significant psychological stress during the SARS crisis. Prevalent fear was danger to personal health
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
the SARS crisis. Prevalent fear was danger to personal health
>>Adequate protective facilities and equipment paramount<<
68
Stockpiling resources
• About 1 in 5 patients required ICU care in SARS. This number is helpful in projecting ICU manpower and bed requirement
• Based on incidence of various complications, project the amount and type of medical supplies and equipment needed in an outbreak
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
69
Post Epidemic Surveillance
• Post SARS, Govt. Implemented post surveillance measures for a defined period of time
• Key to control outbreak >> prompt diagnosis and appropriate isolation of febrile individuals with pneumonia not responding to standard therapy
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
70
Adequate healthcare facilities
• CDC recommends airborne infection isolation whenever possible for SARS patients
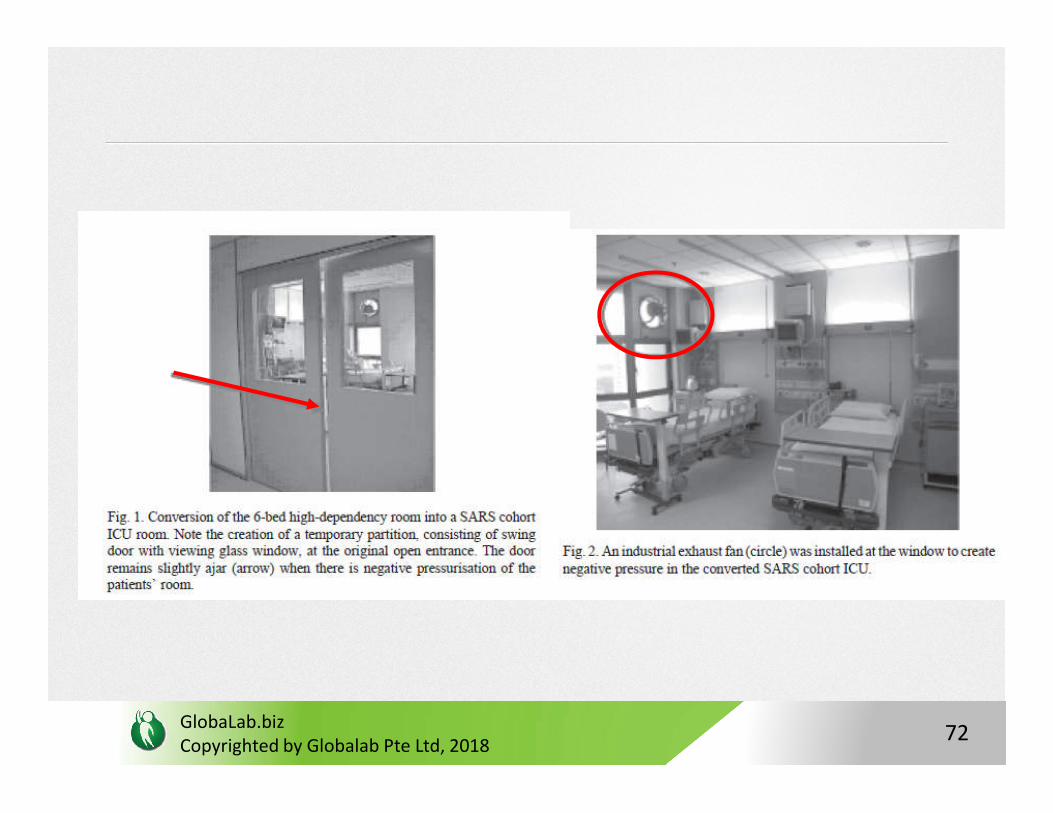
• However, during large outbreak, hospital facilities may be inadequate >> consider alternatives
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
e.g. One alternative to constructing new airborne infection isolation rooms is the creation of a “SARS unit” where SARS patients could be cohorted
>> advantage of a dedicated SARS unit is it allows concentration of resources and equipment, such as portable X-ray machines to reduce fomite transmission
71
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
72
Peacetime preparedness crucial
• SARS required high ICU care: as high of 45.5 % of patients needed ICU care globally, with 20-30% as an average (Singapore >20%)
• Median length of stay 14.5%; more than a quarter needing mechanical ventilation
• Patients needed ICU in 2nd week of admission giving only 1
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
• Patients needed ICU in 2nd week of admission giving only 1 week lead time for preparation and training on PPE
>>training programmes and mask fitting carried out during peacetime with periodic checks<<
73
Surveillance
Comprehensive novel pathogen surveillance comprises the following main components:
• a. Community Surveillance: Community-wide surveillance of acute respiratory infections (ARI) has been well established in Singapore. Weekly reports are compiled from the public-sector hospitals and polyclinics.
• b. Laboratory Surveillance: Surveillance of influenza viruses and other acute respiratory infections is routinely performed by the National Public Health Laboratory on respiratory samples from hospitals and polyclinics.
• c. Hospital Surveillance: Hospitals continue to support the post-SARS epidemic surveillance system. Patients fulfilling the surveillance criteria are reported to MOH.
• d. Disease Notification: For novel agents, gazetting the disease under the Infectious
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
• d. Disease Notification: For novel agents, gazetting the disease under the Infectious Diseases Act may be necessary to mandate notification by doctors and laboratories.
• e. Veterinary Surveillance: The Agri-Food and Veterinary Authority (AVA) carries out surveillance on poultry and other animals, based on the assumption that poultry and animal infection and deaths may precede human infection.
• f. External Surveillance: MOH performs continuous monitoring of infectious disease situations in the region and globally, via various sources, to identify external health risks and threats. Where incidents of concern emerge in a given country, clarification is directly sought through international contacts.
74
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
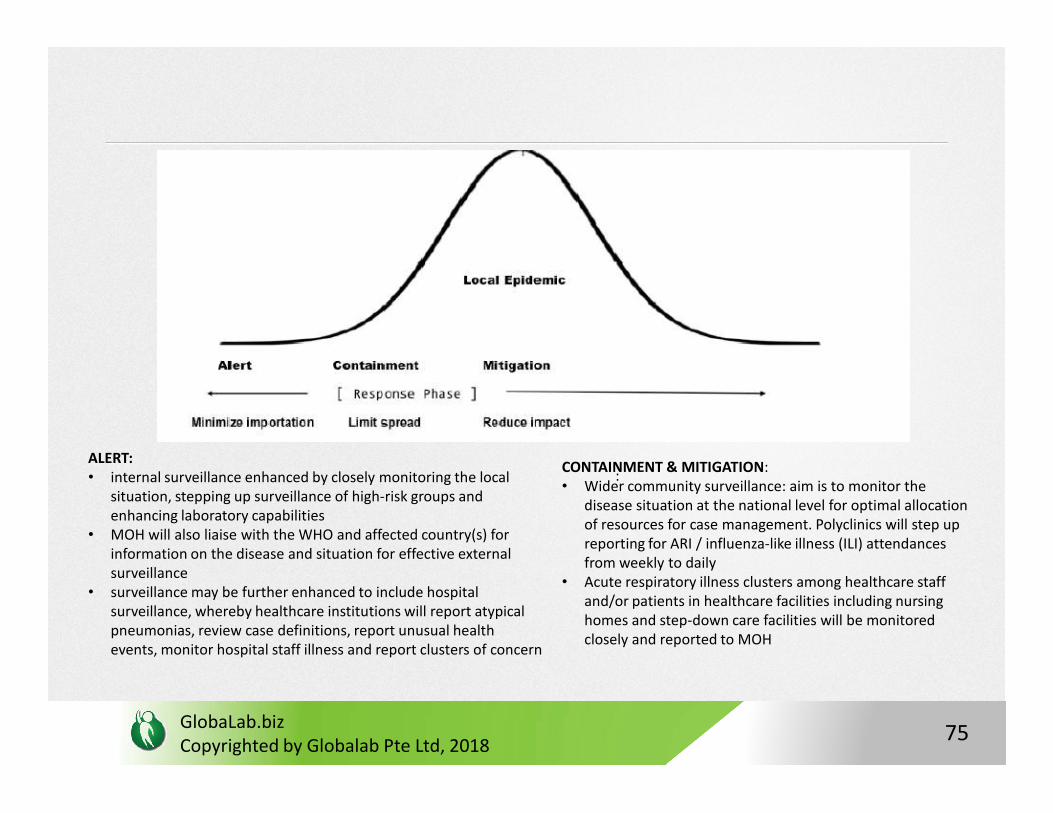
ALERT: • internal surveillance enhanced by closely monitoring the local
situation, stepping up surveillance of high-risk groups and enhancing laboratory capabilities
• MOH will also liaise with the WHO and affected country(s) for information on the disease and situation for effective external surveillance
• surveillance may be further enhanced to include hospital surveillance, whereby healthcare institutions will report atypical pneumonias, review case definitions, report unusual health events, monitor hospital staff illness and report clusters of concern
CONTAINMENT & MITIGATION:• Wider community surveillance: aim is to monitor the
disease situation at the national level for optimal allocation of resources for case management. Polyclinics will step up reporting for ARI / influenza-like illness (ILI) attendances from weekly to daily
• Acute respiratory illness clusters among healthcare staff and/or patients in healthcare facilities including nursing homes and step-down care facilities will be monitored closely and reported to MOH
:
75
Surveillance
• Electronic Notification System (ENS): web-based application that allows medical practitioners and laboratory personnel to submit on-line notifications of infectious diseases in a rapid and secure fashion to the relevant surveillance agencies.
• Real-time notification important in times of disease outbreaks
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
• Real-time notification important in times of disease outbreaks so that prompt and appropriate public health measures can be instituted to control spread
76
Information Technology Systems
• New SARS IT infrastructure: provides MOH and other agencies with integrated information of all SARS cases in Singapore
• Infectious Disease Alert and Clinical Database System integrates clinical, laboratory and contact tracing information on SARS
• Health Check System: HPCs in hospitals and clinics to identify patients who may have been exposed to SARS.
• Contact Tracing System: captures SARS cases, contact history
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
• Contact Tracing System: captures SARS cases, contact history and HQO to facilitate speedier generation of HQO reports, contact listings, and listings for external agencies automatically.
• e-Quarantine Management System: better management in processing and enforcement of HQOs
77
Improving Internal Capability & Research
• Singapore Field Epidemiology Training Programmeinstitutionalized in 2010. Administered by the Communicable Diseases Division of the Ministry of Health and modelled after the US Centers for Disease Control and Prevention’s Epidemic Intelligence Service
• Courses conducted biannually
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
• Courses conducted biannually
• Saw Swee Hock School of Public Health aims to produce future public health leaders and fulfil a unique niche in utilising new technologies to provide local solutions to infectious disease control, advance research and education in areas of infectious disease control, health systems, and chronic diseases with an Asian focus
78
Communicable Disease Centre: clinical management of outbreaks integrated into a new purpose-built state of-the-art facility for
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
built state of-the-art facility for the isolation and management of patients with infectious diseases
79
South East Asia & Its Unique Challenges in Disease OutbreaksConsidered a hotspot for new and emerging infectious diseases at three levels:
(1) as a region containing diverse zoonotic and vector-borne pathogens, and thus a primary source of emerging infectious disease;
(2) as a region in which the high density, proximity, and mobility of human beings and animal reservoirs provide fertile conditions for
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
human beings and animal reservoirs provide fertile conditions for transmission between species, within human populations, and across geographic areas;
(3) as a region with ecological factors that allow rapid pathogen mutation and host adaptation—for example, Dengue, reassortmentsof influenza virus, and emergence of drug resistance
80
Economic Impact of Outbreaks
• Estimated cost of SARS to east and southeast Asia was US$18 billion, which is roughly US$2 million per person infected.
• Tourist industry was affected less by H5N1 but the poultry industry, by contrast, was profoundly affected.
• In southeast Asia, sudden collapse in demand for the service industry was a dominant feature in this cost, particularly in
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
industry was a dominant feature in this cost, particularly in view of a tourist industry reliant on the 35 million tourists arriving every year from outside the region.
• Fear, anxiety, and changes in behaviour and the effect on tourist industry have unpredictable consequences.
81
Establishing Surveillance Challenges
• absence of specific government policies and legal frameworks for surveillance and control of zoonoses,
• inadequate resources, insufficient animal–human public health cooperation, coordination, and collaboration, frail laboratory facilities, and weak and disconnected reporting systems
• Outbreaks have been opportunities for strengthening systems
e.g. in the wake of H5N1 influenza outbreaks, the governments of Vietnam,
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
e.g. in the wake of H5N1 influenza outbreaks, the governments of Vietnam, Thailand, Indonesia, Cambodia, Malaysia, and the Philippines have all set up new institutional bodies, strengthened diagnostic laboratory capacity, and improved coordination mechanisms.
Although gaps in national planning and surveillance systems persist, countries in southeast Asia have made substantial progress towards effective prevention and control of infectious diseases
82
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018
83
GlobaLab.bizCopyrighted by Globalab Pte Ltd, 2018GlobaLab.biz 84
Thank youQuestion and Answer Session