Embed Size (px)
Citation preview
Infectious Disease Cutaneous Disorders
Alison Ruiz PA-C

MRSA
• Can cause any type of skin infection
• 59% of purulent skin infections in adults • 75% of purulent skin abscesses in children
Antibiogram
http://pulse/clinicalresources/pharmacy/documents/druguseg/antimicrobial/ns/2013antibiogram.xlsx

MRSA presentation
Treatment of MRSA
• MRSA Resistance • Cephalexin
• Dicloxacillin
• 48% resistant to Clindamycin
• Group A strep is resistant to bactrim and doxycycline
• Increasing resistance to Macrolides and Fluoroquinolones
The latest microbial antibiogram:
• PULSE • Clinical resources --> Pharmacy --> Drug
Use Guidelines --> Antimicrobials (left column, middle of page) -->Antibiogram and MIC distribution
•
• Large abscesses, abscess in immune compromised pts or ones which are also cellulitic • Require with BOTH I&D AND antibiotics
• Antibiotics likely effective against MRSA • Clindamycin
• Check local susceptibility
• Bactrim
• Nearly 100% susceptible
• Doxycycline
• 82-85% susceptible

Abscess
• Often Staph aureus • MSSA or MRSA
• 75% of purulent skin abscesses were caused by MRSA
• Fluctuant, erythematous, tender nodules often with surrounding erythema
Furuncles and Carbuncles
• Single deep nodules involving the hair follicle that are often pus filled
• Multiple furuncles that drain through several openings in the skin
• Pseudomonas, Candida and other

Evaluation of Abscess
• Bedside Ultrasound distinguishes abscess from cellulitis

What is this?
Folliculitis
• Infected hair follicle
• Causative agents: Pseudomonas and Candida, Bacterial
• Hot tub folliculitis • Pseudomonas growth in hot tubs (lesions are usually >3cm) • Distribution
• Treatment • Remove offending agent and bid cleansing with mild hand soap and
usually clears • Can do topical antibiotics
• polymyxin B or bacitracin
• Severe or extensive cases • PO antibiotics against Strep, staph such as cephalexin, dicloxacillin, azithromycin

What is this?

Pilonidal Cyst
• Tender, swollen, fluctuant nodule
• I&D • Remove any debris, hair for the abscess cavity • Pack with iodoform gauze (remove in 2-3 days) • Surgical consult for possible excision

What is this?
Bartholin Gland Abscess
• When infected cause pain
• I&D and placement of the word catheter to allow drainage • Word catheter can be left in for 4 weeks • Sitz baths after 2 days • +/- antibiotics: nonSTD infections, use cephalexin plus metronidazole • Marsupialization prevents recurrence

What is this?

Cellulitis
• Most common B-hemolytic strep, S. aureaus (including MRSA), gram – aerobic bacilli.
• Erythema, tender, warm, swollen, no sharp demarcation from uninvolved skin
• Symptoms occur gradually over days • Lymphangitis and LAD can occur

Cellulitis and Peau d’orange

What is this?
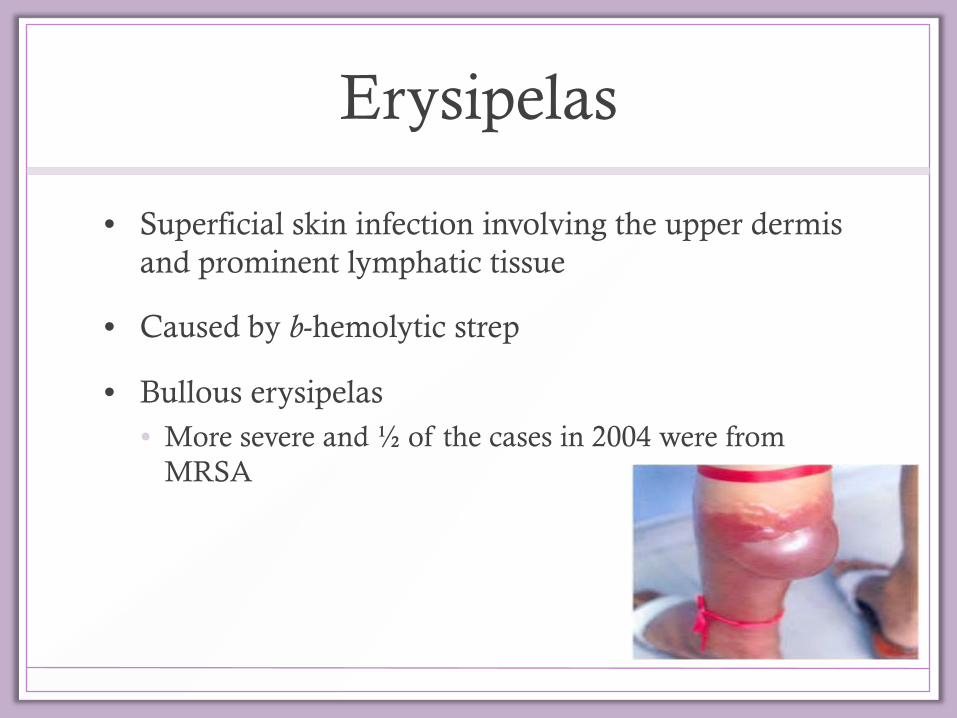
Erysipelas
• Superficial skin infection involving the upper dermis and prominent lymphatic tissue
• Caused by b-hemolytic strep
• Bullous erysipelas • More severe and ½ of the cases in 2004 were from
MRSA

Symptoms of Erysipelas
• Usually abrupt with fevers, chills & malaise in prodromal phase
• In 1-2d, small area of erythema develops & burning sensation
• Much more distinctly demarcated from the surrounding normal tissue (unlike cellulitis)

Work up
• Who needs cultures (wound and/or blood) • In toxic pt
• Immunocompromised pt
• Pt with many comorbid conditions
• Pt recurrent infections
• Xrays • If concern for osteomyelitis
or necrotizing soft tissue infections
• IN Cellulitis • Dopplers
• To distinguish from DVT

Differential Diagnosis for Cellulitis/Erysipelas
• Necrotizing soft tissue infection
• Herpes Zoster
• Bursitis
• Osteomyelitis
• Toxic Shock Syndrome
• DVT
• Superficial thrombophlebitis
• Insect tings
• Contact Dermatitis
• Gouty Arthritis
• Drug Reaction
• Malignancy

Treatment
• Antibiotics • Simple cellulitis in healthy pt
• PO
• Otherwise use IV and likely admission
• Elevation
• Surgical consult • If bullae, crepitus, pain out of proportion with
examination or rapidly progressive erythema
Antibiotic Therapy
• ORAL • Cephalexin 500mg po q6h
• Dicloxacillin 500mg po q6h
• Clindamycin 150-450mg q6h
• PARENTERAL • Cefazolin 1g IV q8h
• Oxacillin 1-2g IV q6h
• Nafcillin 1-2g IV q6h

Treatment for MRSA Cellulitis Severity of Illness Type of Infection Antibiotics
Mild Skin Abscess after I&D Cellulitis
No antibiotics OR Clindamycin 300mg tid for 7-10d OR Bactrim DS bid +/- cephalexin 500mg qid for 7-10d
Moderate Stable pt with celluiltis or abscess after I&D requiring hospitalization Worsening infection despite outpt therapy
Clindamycin 600-900mg IV q8h OR Vancomycin 1gram IV q12 h OR Linezolid 600mg IV q12 h
Severe NSTI, Sepsis, Pt with significant comorbidities
Vancomycin 1gm IV q12h +Meropenem 500-1000mg q8h IV OR Piperacillin/Tazobactam 4.5g q6h, or imipenem-cilastatin 500mg q6h

Treatment for Erysipelas
• Most often treated with parenteral antibiotics
• Cover for strep (most common organism) • Ceftriaxone 1gram IV qd OR
• Cefazolin 1-2grams IV q8h • Will also cover for staph aureus
• In the case where it is difficult to determine if the infection is erysipelas vs cellulitis
• Admit the patient

What is this?

Impetigo
• Affects children, commonly around the nose and mouth
• Direct contact with infected person or fomites
• S. aureus or S. pyogenes
• Honey yellow crusts is typical finding.
• Bullous lesions can occur.
• Treatment • Topical saline and aluminum acetate soaks followed by 2% mucpirocin ointment • Systemic involvement
• Treat with Cephalexin or macrolide • 20% is MRSA and can be treated with Clindamycin

What is this?
Necrotizing Infection
• Fulminant, extensive soft tissue necrosis
• Systemic toxicity
• High mortality
• Also known as • Fournier gangrene • Necrotizing fasciitis • Necrotizing soft tissue infection • Gas gangrene
• Mortality rate 25-35% • Bacteremia is a strong predictor of mortality • Increased risk for death are pt’s <1 yrs old or >60 yrs old

Who is at Risk for Developing Necrotizing Fasciitis?
• Advanced age
• DM
• alcoholism
• peripheral vascular disease
• heart disease
• renal failure
• HIV
• cancer
• NSAID use
• decubitus ulcers
• chronic skin infections
• IV drug abuse
• immune system impairment
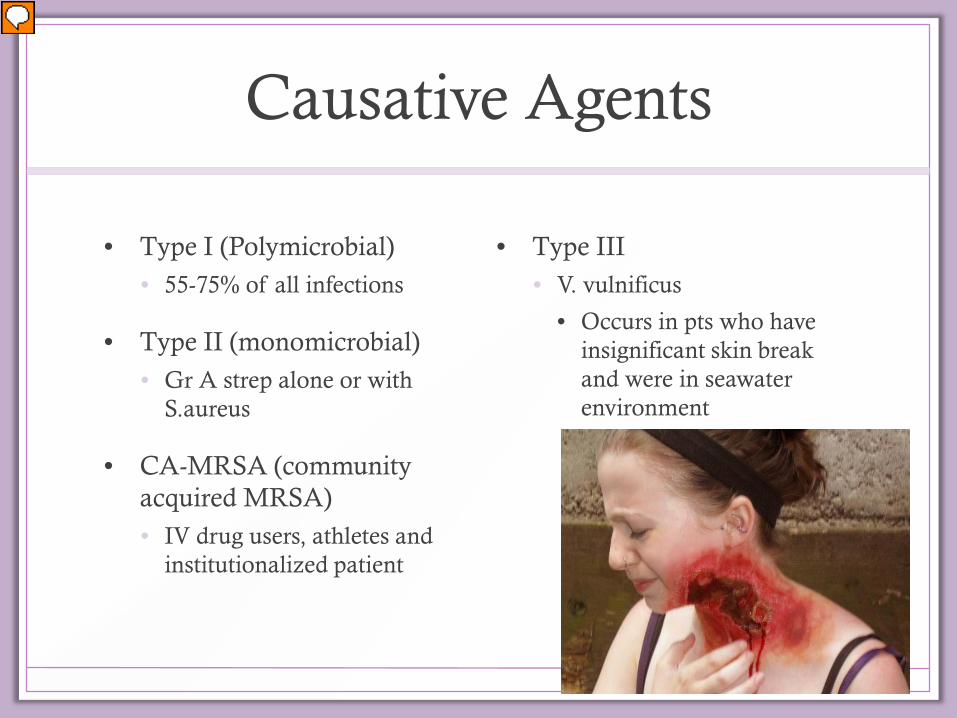
Causative Agents
• Type I (Polymicrobial) • 55-75% of all infections
• Type II (monomicrobial) • Gr A strep alone or with
S.aureus
• CA-MRSA (community acquired MRSA) • IV drug users, athletes and
institutionalized patient
• Type III • V. vulnificus
• Occurs in pts who have insignificant skin break and were in seawater environment

Pathophysiology of Necrotizing Fasciitis

Clinical Features of Necrotizing Fasciitis
• Pain
• Anxiety
• Diaphoresis
• Pt may present with no pain!
• Late finding • Bronze or brownish discoloration with
a malodorous serosanguineous discharge and bullae present
• Systemic features • low grade fever
• tachycardia out of proportion with fever

Making the Diagnosis
• It is a clinical diagnosis
• Plain x-rays • +/-SQ gas • Doesn’t show deep fascial gas
• CT is more sensitive (80%) • See fascial thickening and edema, deep tissue collections and
gas formation
• MRI is most sensitive (90%) • Availability may delay to treatment

Treatment
• Aggressive IV fluids
• Transfusion of pRBCs may be needed • Correct anemia from hemolysis
• Early surgical intervention • Operative exploration and debridement
• Fasciotomy, debridement and amputation • Mortality increases dramatically if debridement is delayed > 24 hours
• Antibiotics • Cover for MRSA and Clostridial
• Tetanus Prophylaxis PRN
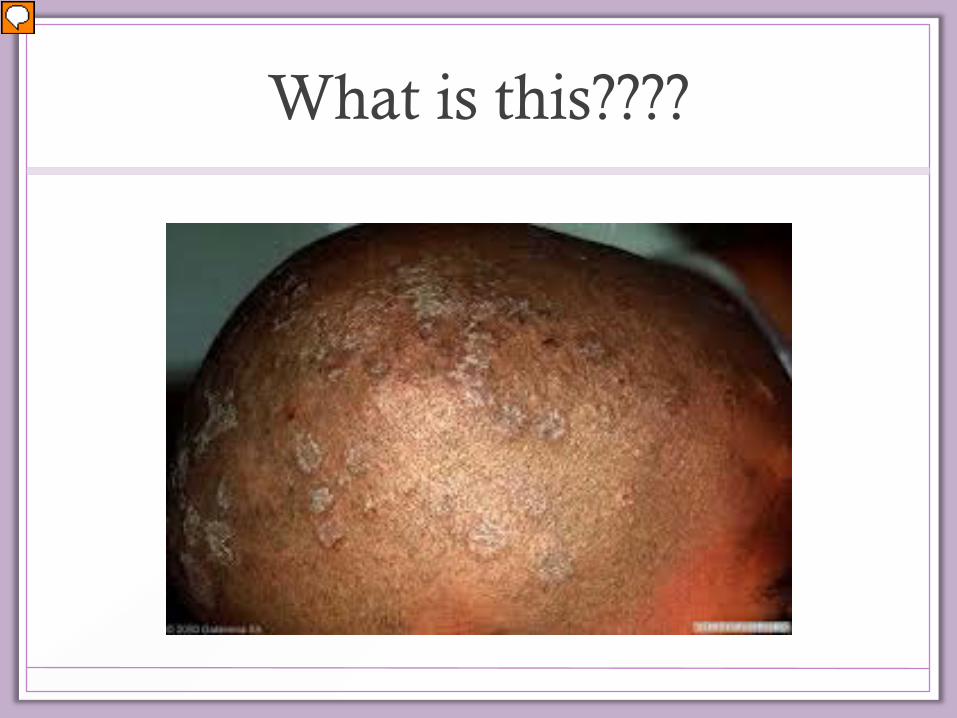
What is this????

Tinea
Tinea Capitis •Patchy, nonscarring areas of alopecia with broken hairs and scale at the periphery •Oral Griseofulvin
Tinea Corporis •1 or more sharply demarcated scaling patches •May have central clearing •Topical antifungals are treatment of choice •Oral if there is widespread tinea or invovlement of the follicles
Tinea Crusis •Symmetric erythema with peripheral annular slightly scaly edge •Groin, thighs and buttocks may be involved •Antifungal creams •Clotrimazole, ketoconazole, econazole
Tinea Pedis •Scales in the web spaces •Spares the dorsum of foot •Topical antifungals for 1 week after rash clears •Clotrimazole, miconazole, ketoconazole, econazole

Tinea Corporis Differential Diagnosis
• Pityriasis rosea
• Psoriasis
• Seborrheic dermaititis
• Syphilis
• Eczema
• Tinea versicolor
• Erythema migrans
• Lupus erythematous
• Cutaneous T cell lymphoma

??????

Pediculosis
• Ages 3-11 years most affected.
• Found in scalp, behind the ears and on back of the neck
• Transmission head to head contact
• Identify nits (oval gray white egg capsules) or adult lice • Flouresce with woods lamp
• Treatment • Permethrin cream 1% or 5%
applied to hair and left overnight followed by neutral shampoo
• Pyrethrin cream is applied for 10 minutes and then rinsed out
• Retreatement is advised in 1-2 weeks.
• www.headlice.org

Pediculosis Infestation

??????

Scabies
• Scabies appear in a tunnel or burrow like rash beneath the skin
• Eruption 30 days after exposure
• Presents with intense, intractable itching worse at night
• Head and neck are typically sparred
• Treatment • Permethrin cream 5% (cat B in pregnancy)
• Apply from neck down for 12 hours, followed by bathing with soap
• AVOID LINDANE IN CHILDREN AND PREGNANT WOMEN

What is this?

Herpes Simplex
• Treatable with antivirals • Important to recognize early to treat early
• 2 types: HSV-1 and HSV-2
• HSV-1 is the most common cause of viral encephalitis in the US. • Usually <20yrs or >50yrs • Untreated >70% mortality rate
• Neonates with HSV • High frequency of visceral involvement and CNS disease
• Encephalitis in infants is most often HSV-2 from maternal genital tract at the time of delivery
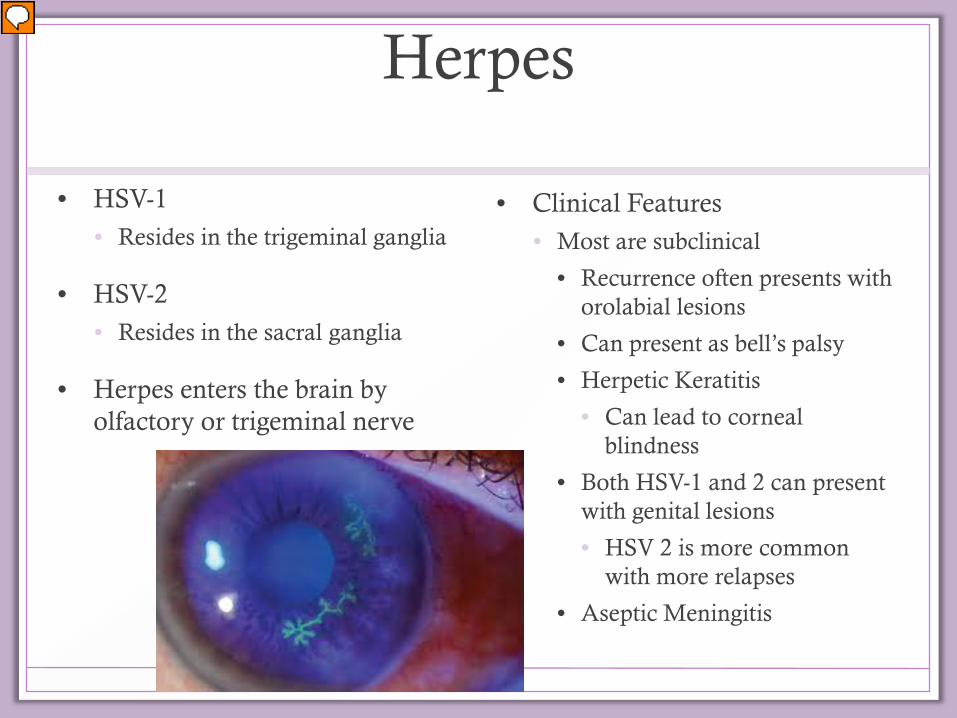
Herpes
• HSV-1 • Resides in the trigeminal ganglia
• HSV-2 • Resides in the sacral ganglia
• Herpes enters the brain by olfactory or trigeminal nerve
• Clinical Features • Most are subclinical
• Recurrence often presents with orolabial lesions
• Can present as bell’s palsy
• Herpetic Keratitis
• Can lead to corneal blindness
• Both HSV-1 and 2 can present with genital lesions
• HSV 2 is more common with more relapses
• Aseptic Meningitis

HSV
• HSV Encephalitis • Hallmark
• Is acute onset of fever and neurologic symptoms
• Hemiparesis, CN abnormalities, ataxia, focal seizures, altered mental status

Immune Compromised Host
• Including burn patients • HSV infection dissemination
with multi-organ involvement
• Esophagitis, hepatitis, colitis, pneumonia

Diagnosing HSV
• Culture • Fluid of lesion by unroofing
vesicle
• MRI/CT • See temporal lobe lesions
• EEG • shows intermittent, high-
amplitude slow waves localized to the temporal lobe
• CSF • lymphocytic pleocytosis • PCR testing is 94% sensitive and
98% specific
Treatment
• IV acyclovir • HSV encephalitis or disseminated HSV
• Consider adding IV acyclovir empirically to regimen in patients that you think may have bacterial meningitis • Hard to distinguish between bacterial and viral meningitis on
exam
• Healthy patients with HSV-1 or HSV-2
• Acyclovir, famciclovir or valacyclovir for 7-10days
• Recurrent herpes labialis usually does not require treatment
• May be on suppressive therapy

Case
• 56 y/o otherwise healthy female comes to the ED c/o left sided chest pain. She states it started 4 days ago but was mild. Pt saw her pcp 3d ago, but since symptoms have continued she has come to the ED.
• Pain is worsening and now radiates to the left side of back
• Denies sob, nausea, diaphoresis.
• Pain with movement of her left arm.
• No previous episode of chest pain or cardiac problems.

History
• PMH: none
• PSH: none
• Meds: Vitamins
• All: NKDA
• FH: Colon Ca- father 50 y/o
• SH: nonsmoker, No alcohol use

Physical Exam
• What do you want to know? • HEENT • Neck • Lungs • CV • Abd • Back • Ext • Skin • Neuro

Work up
• CBC
• BMG
• Cardiac Markers
• EKG
• CXR

????????

What if you find this on physical exam

Classical presentation of Herpes zoster

Dermatomes

Herpes Zoster
• Varicella Zoster Virus • Organism that causes both chickenpox and herpes zoster
• Who develops Herpes Zoster? • Pts whose immune system wanes
• Advanced age (immune system wanes) • Lymphoproliferative disorders • HIV • Organ transplant patients
• Clinical Presentation • Pain, itching and paraesthesias in the dermatome affected
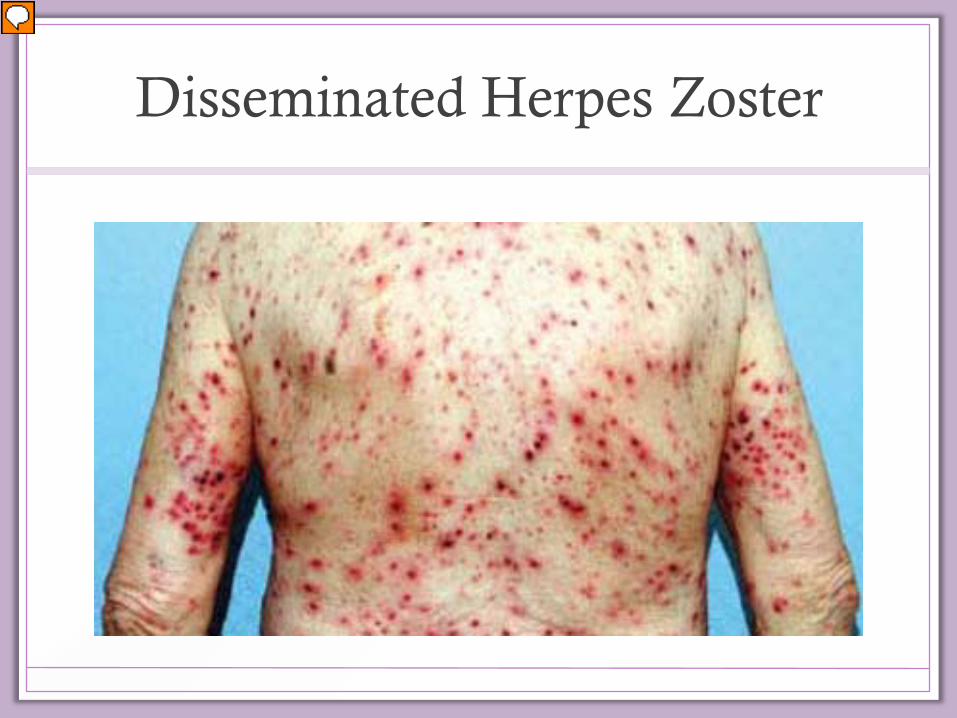
Disseminated Herpes Zoster

Postherpetic Neuralgia • Persists >30 days
• Increases with advancing age
• Pain last months to years
• Primary goal of treatment is to reduce postherp neuralgia!!!!! • Antivirals within 72 hours of onset of rash
• Treat if new vesicles are still present or still forming >72 hours
• Adjunctive corticosteroids can reduce pain but do not decrease incidence of post herpetic neuralgia
• Treat immune compromised patients regardless of time since rash onset.

Common Antivirals For Treatment
• Acyclovir 800mg po 5 times per day for 7-10d • Valacyclovir 1gram po tid 7-10d • Famiciclovir 500mg po tid for 7-10d
• Acyclovir 10mg/kg IV q 8h for 7d
• Acyclovir 10mg/kg IV q8h for 7-14d

What is this

Varicella
• Supportive care in the healthy patient • Consider Acyclovir in healthy pt because it decreases the number of lesions
and shortens the course if started within 24 hours of developing rash • High risk patients consider Acyclovir • Adults and Children >12 yrs, pts with chronic skin or pulmonary disorders,
receiving long term salicylate therapy and immunocompromised pts. • ***Famciclovir and valacyclovir are not licensed for treatment of varicella in
the US

References
• Tintanilli 1014-1031, 1630-1669