Embed Size (px)
Citation preview
Infections after Transplantation of Bone Marrowor Peripheral Blood Stem Cells from UnrelatedDonorsJo-Anne H. Young, University of MinnesotaBrent R. Logan, Medical College of WisconsinJuan Wu, The EMMES CorporationJohn R. Wingard, University of FloridaDaniel J. Weisdorf, University of MinnesotaCathryn Mudrick, The EMMES CorporationKristin Knust, The EMMES CorporationMary M. Horowitz, Medical College of WisconsinDennis L. Confer, National Marrow Donor ProgramErik R. Dubberke, Washington University
Only first 10 authors above; see publication for full author list.
Journal Title: Biology of Blood and Marrow TransplantationVolume: Volume 22, Number 2Publisher: Elsevier | 2016-02-01, Pages 359-370Type of Work: Article | Post-print: After Peer ReviewPublisher DOI: 10.1016/j.bbmt.2015.09.013Permanent URL: https://pid.emory.edu/ark:/25593/rwq6j
Final published version: http://dx.doi.org/10.1016/j.bbmt.2015.09.013
Copyright information:© 2016 American Society for Blood and Marrow Transplantation.This is an Open Access work distributed under the terms of the CreativeCommons Attribution-NonCommercial-NoDerivatives 4.0 International License(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Accessed March 13, 2022 11:37 AM EDT

Infections following Transplantation of Bone Marrow or Peripheral-Blood Stem Cells from Unrelated Donors
Jo-Anne H. Young1,*, Brent R. Logan2, Juan Wu3, John R. Wingard4, Daniel J. Weisdorf1, Cathryn Mudrick3, Kristin Knust3, Mary M. Horowitz2, Dennis L. Confer5, Erik R. Dubberke6, Steven A. Pergam7, Francisco M. Marty8, Lynne M. Strasfeld9, Janice (Wes) M. Brown10, Amelia A. Langston11, Mindy G. Schuster12, Daniel R. Kaul13, Stanley I. Martin14, and Claudio Anasetti15 for the Blood and Marrow Transplant Clinical Trials Network (BMT CTN) Trial 02011Department of Medicine, University of Minnesota, Minneapolis, MN
2Medical College of Wisconsin, Milwaukee, WI
3The EMMES Corporation, Rockville, MD
4Shands Cancer Center, University of Florida, Gainesville, FL
5National Marrow Donor Program, Minneapolis, MN
6Washington University School of Medicine, St. Louis, MO
7Fred Hutchinson Cancer Research Center, Seattle, WA
8Dana-Farber Cancer Institute, Boston, MA
9Oregon Health & Science University, Portland, OR
10Stanford University, Palo Alto, CA
11Emory University, Atlanta, GA
12University of Pennsylvania, Philadelphia, PA
13Univeristy of Michigan, Ann Arbor, MI
14Ohio State University, Columbus, OH
Corresponding author: Jo-Anne H. Young, MD. Address: MMC 250, 420 Delaware St SE, Minneapolis, MN 55455. [email protected]. Phone: (612) 625-8462. Fax: (612) 625-4410.
Authorship ContributionJ.H.Y. and D.J.W. designed the infectious disease analysis for this study protocol and wrote the paper; C.A., J.R.W., M.M.H. and D.J.W. were senior advisors in the design, conduct, and analysis of the study; K.K. and C.M. organized and maintained the database, J.H.Y., J.R.W, E.R.D., S.A.P., F.M.M. L.M.S., J.M.B., A.A.L., M.G.S., D.R.K., and S.I.M. audited many infection summaries; J.W. and J.H.Y. analyzed data; B.R.L., and J.W. provided statistical analysis; all authors reviewed and provided insightful comments to better the manuscript; and J.W. and J.H.Y. drew the figures.
Disclosure of potential conflicts of interestThe authors declare no competing financial interests.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
HHS Public AccessAuthor manuscriptBiol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Published in final edited form as:Biol Blood Marrow Transplant. 2016 February ; 22(2): 359–370. doi:10.1016/j.bbmt.2015.09.013.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
15H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL
Abstract
Infection is a major complication of hematopoietic cell transplantation. Prolonged neutropenia and
graft versus host disease are the two major complications with an associated risk for infection, and
these complications differ according to the graft source. A phase 3, multicenter, randomized trial
(BMT CTN 0201) of transplantation of bone marrow (BM) versus peripheral-blood stem cells
(PBSC) from unrelated donors (URD) showed no significant differences in two-year survival
between these graft sources. In an effort to provide data regarding whether bone marrow or
peripheral-blood stem cells could be used as a preferential graft source for transplantation, we
report a detailed analysis of the infectious complications for 2 years following transplantation
from the BMT CTN 0201 trial. A total of 499 patients in this study had full audits of infection
data. A total of 1347 infection episodes of moderate or greater severity were documented in 384
(77%) patients; 201/249 (81%) of the evaluable patients had received a BM graft and 183/250
(73%) had received a PBSC graft. Of 1347 infection episodes, 373 were severe and 123 were life-
threatening and/or fatal; 710 (53%) of these episodes occurred on the BM arm and 637 (47%) on
the PBSC arm, resulting in a two-year cumulative incidence 84.7% (95% confidence interval [CI]:
79.6–89.8) for BM vs. 79.7% (95%CI, 73.9–85.5) for PBSC, P = .013. The majority of these
episodes, 810 (60%), were due to bacteria, with a two-year cumulative incidence of 72.1% and
62.9% in BM versus PBSC recipients, respectively (P = .003). The cumulative incidence of
bloodstream bacterial infections during the first 100 days was 44.8% (95%CI, 38.5–51.1) for BM
vs. 35.0% (95%CI, 28.9–41.1) for PBSC (P = .027). The total infection density (# infection
events / 100 patient days at risk) was .67 for BM and .60 for PBSC. The overall infection density
for bacterial infections was .4 in both arms; for viral infections was .2 in both arms; and for
fungal/parasitic infections was .04 and .05 for BM and PBSC, respectively. The cumulative
incidence of infection prior to engraftment was 47.9% (95%CI, 41.5–53.9) for BM vs. 32.8%
(95%CI, 27.1–38.7) for PBSC (P = .002), possibly related to quicker neutrophil engraftment using
PBSC. Infections remain frequent following URD HCT, particularly following BM grafts.
Keywords
Infection; unrelated donor transplantation; bacteremia; cytomegalovirus; aspergillosis; pre-engraftment
INTRODUCTION
Blood and Marrow Transplant Clinical Trials Network (BMT CTN) protocol 0201 was a
phase 3, multicenter, randomized trial of transplantation of bone marrow (BM) versus
granulocyte-colony stimulating factor mobilized peripheral-blood stem cells (PBSC) from
HLA compatible unrelated donors in patients with hematologic malignancies. There were no
significant differences in 2-year survival probabilities [1]. Only 5% of patients who died had
infection listed as the primary cause of death. Analysis of pre-specified secondary endpoints
showed that the median time to neutrophil engraftment was 5 days shorter for those
randomly assigned to receive PBSC. The total incidence of graft failure was 3% in the
PBSC group, compared to 9% in the BM group. These significant findings, as well as data
Young et al. Page 2
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
from other clinical trials, have led some to choose PBSC as a preferential graft source [2–6].
However, the 53% incidence of chronic graft-versus host disease at 2 years in the PBSC
group was significantly higher when compared to 41% for the BM group, a finding
confirmed by other studies [2–4,7–10]. These secondary analyses suggest that it may be
important for patients who are immunosuppressed from prior chemotherapy, and have a
lower risk of graft rejection, receive BM grafts, while patients with malignant diseases who
have never undergone cytotoxic chemotherapy, who may be at increased risk of rejection of
a BM graft, undergo transplant with a PBSC graft. In an effort to provide additional data
regarding whether BM or PBSC could be used as a preferential graft source for
transplantation, we report a detailed analysis of the infectious complications for 2 years
following transplantation from the BMT CTN 0201 trial.
METHODS
Protocol Synopsis
BMT CTN Protocol 0201 opened for accrual in March 2004 and closed in September 2009
meeting the target accrual objective of 550 donor-recipient pairs. Randomization was
performed 1:1 to either PBSC or BM and stratified by transplant center and disease risk.
Details of the treatment schemes have been reported [1]. Key baseline characteristics were
similar in the 2 treatment arms. The primary objective was to compare two-year survival
probabilities in the two study arms using an intent-to-treat analysis. Secondary objectives
included incidences of neutrophil and platelet engraftment, graft failure, acute graft-versus-
host disease (GVHD), chronic GVHD, time off all immunosuppressive therapy, relapse,
adverse events, immune reconstitution, and quality of life. Moderate or more severe
infections were reported on an event-driven Case Report Form, excluding those that
occurred pre-transplant, and were tabulated for two years following transplantation.
Infection Prophylaxis
Among the 40 participating transplant centers, infection prophylaxis followed local
protocols that were based on national guidelines [11]. Patients underwent their transplant
procedure in rooms ventilated with high efficiency particulate air filtration systems to
prevent acquisition of exogenous mold infections [12]. During periods of neutropenia,
broad-spectrum antibacterial agents were administered that included anti-pseudomonal
antibacterial agents for febrile neutropenia [13]. During periods of fever, assessment for
infection and augmentation of antimicrobial agents included empirical treatment for yeasts
and molds for persistent fever [14]. Medication to prevent Pneumocystis infections generally
started within one month after transplantation, following engraftment [15]. Acyclovir was
used to prevent herpes simplex and varicella infections. Monitoring guidelines were
followed to detect and preemptively treat cytomegalovirus (CMV) infection.[16] Diagnostic
strategies for individual pathogens, particularly viral and fungal infections, varied between
centers based on local laboratory practices.
Data Collection and Audit
Transplant centers prospectively reported infections for study subjects. Infection onset date,
organism, body site, clinical severity, and treatment were captured. Classification of
Young et al. Page 3
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
infection severity, including a fatal category, were modified from the definitions used in
previous studies [17,18]: A) Life-threatening infections were those complicated by
hypotension or any another event considered life-threatening; B) Severe infections often
required treatment with intravenous antibiotics or involved other clinical circumstances that
were considered severe.
Based on previous studies that had shown the importance of infection data auditing [17–22],
the 0201 Infection Team contacted each transplant center to audit the infection data reported
for local study patients. In 2012, a pilot audit of infectious disease data for 78 subjects at 15
centers involved with this study indicated value for a full data audit for all transplanted
subjects. The BMT CTN Infection reporting form and Instructions for the BMT CTN 0201
Infection Data Review are included as supplementary files to this manuscript. To perform
both the pilot audit and entire study audit, the Data and Coordinating Center (The EMMES
Corporation, Rockville, MD) prepared an infection summary for each study patient listing
the date, organism, body site, severity, and comments regarding each infection as
prospectively reported. The auditor confirmed database information by reviewing
electronically generated medical records of microbiology, virology, imaging, and surgical
pathology reports. Study subjects who were not audited for infection data (n=27, 5%) were
excluded from these analyses.
Staphylococcus epidermidis bloodstream infections were counted as an episode of infection
if they were treated (even when just one positive blood culture led to treatment) because the
treatment course then could have affected whether a second blood culture turned positive,
altered the flora of the subject, and created the potential for drug toxicity. CMV, human
herpes virus-6, and polyomavirus infections were differentiated as viremia or disease using
the BMT CTN Infection reporting form which specifies a body site code; a comment box to
add detail about an infection was later reviewed by the audit committee (and JHY) during
data cleaning; and the specified definitions of infection severity based on body site affected.
All Epstein Barr Virus (EBV) “infections” had the comments specifically reviewed to
categorize infections as EBV lymphoproliferative disorder, viremia, or report of a serologic
antibody status.
The BMT CTN Definitions of Infection Severity clarify that fever of undetermined origin,
upper respiratory infections presumed viral, and potential infections where antibiotics were
given without infectious etiology identified were not to be reported. If reported, they were
removed from the dataset during final data review.
Statistical Analysis
Infectious complications were analyzed by comparison of the two treatment arms (PBSC
versus BM) and adjusted by other relevant clinical risk factors. All data on time to infections
or other events were calculated from the date of transplantation. Patients were censored at
last follow-up, relapse, second transplant, or 2 years after transplant, whichever came first.
When a single organism was recovered multiple times, we followed the algorithm for
infection recurrence intervals that were specific to each microorganism, as reported
previously [17].
Young et al. Page 4
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Analysis of infection incidence (by frequency and cumulative incidence) [17] and infection
density (number of infections over time for patients with repeated infections) [20] was
performed for overall infections, bacterial infections, viral infections and fungal/parasitic
infections, over different time periods (Day 0 to Day 100, Day 100 to 6 months, 6 months to
1 year, 1 year to 2 years, and overall within 2 years of transplantation), by treatment arm.
Death was considered a competing risk in cumulative incidence analysis. Infection density
was computed by infection frequencies over 100 patient days at risk. The number of patients
with infections reported was summarized for each infection type and by treatment arm;
specific infectious organisms of interest were explored in descriptive and cumulative
incidence analyses.
Multivariate regression analyses were performed to test the contribution of the randomized
stem cell source (PBSC versus BM) and other relevant covariates to the incidence of
infections. Proportional rates/means models were used to model the infection density over
time, with a robust variance estimator to account for within subject correlation [23]. All
variables were checked for proportionality using time dependent covariates. The effect of
acute and chronic GVHD on infection density was obtained using time-dependent
covariates. Multivariate analyses were performed to test the impact of various types of
infections on overall survival following transplantation. Cox regression models were used to
model survival. The treatment arm variable was forced into all models and baseline
covariates were selected using forward stepwise algorithm. Various types of infections were
treated as time-dependent covariates in the model. SAS version 9.3 (SAS Institute) was used
for data manipulation, infection frequency analysis, and multivariate modeling. R version
2.15.1 was used for cumulative incidence analysis.
RESULTS
Study Population and Total Infections
Among 551 patients enrolled at 48 centers between 01/2004 and 10/2009, 526 patients
received a transplant. Response rate was 95% for the infection data audit (249 of the BM
arm and 250 on the PBSC arm), resulting in a study population for this analysis of 499
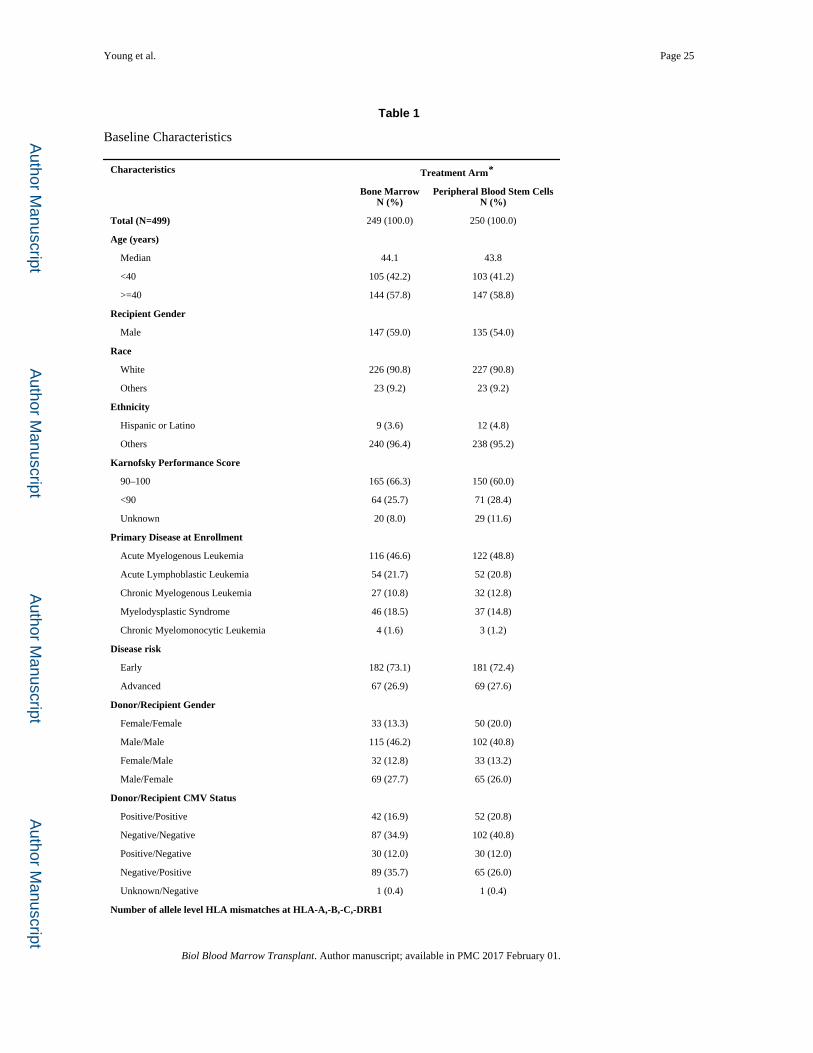
audited patients. Table 1 lists the baseline characteristics of the patients by treatment arm.
Baseline characteristics were balanced between the arms and no significant differences were
noted.
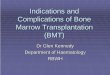
Overall, 384 patients developed infections of moderate or greater severity: 201 on the BM
arm and 183 on the PBSC arm. Of 1347 infection episodes (373 severe and 123 life-
threatening and/or fatal), 710 (53%) occurred on the BM arm and 637 (47%) on the PBSC
arm (Figure 1). The majority of infection episodes on each treatment arm were of moderate
severity (Figure 1a). However, when patients were categorized by infection of worst
severity, 84 patients on the BM arm had a severe infection as their most clinically serious
infection, compared to 68 patients on the PBSC arm (Figure 1b, p = 0.6).
Young et al. Page 5
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
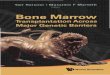
Cumulative Incidence
Cumulative incidence described the proportion of patients developing at least one infection,
with an estimated 2-year incidence of 84.7% (95% confidence interval [CI], 79.6–89.8) for
the BM arm, vs. 79.7% (95%CI, 73.9–85.5) for the PBSC arm, Gray’s test P = .013 (Figure
2). In a subset analysis of the 465 patients who engrafted (excluding 34 patients with
primary or secondary graft failure), the 2-year cumulative incidence rate was 85.3% (95%
CI: 79.2–89.7) for the BM arm, vs. 79.8% (95%CI, 73.2–85.0) for the PBSC arm (P = .014).
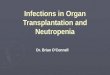
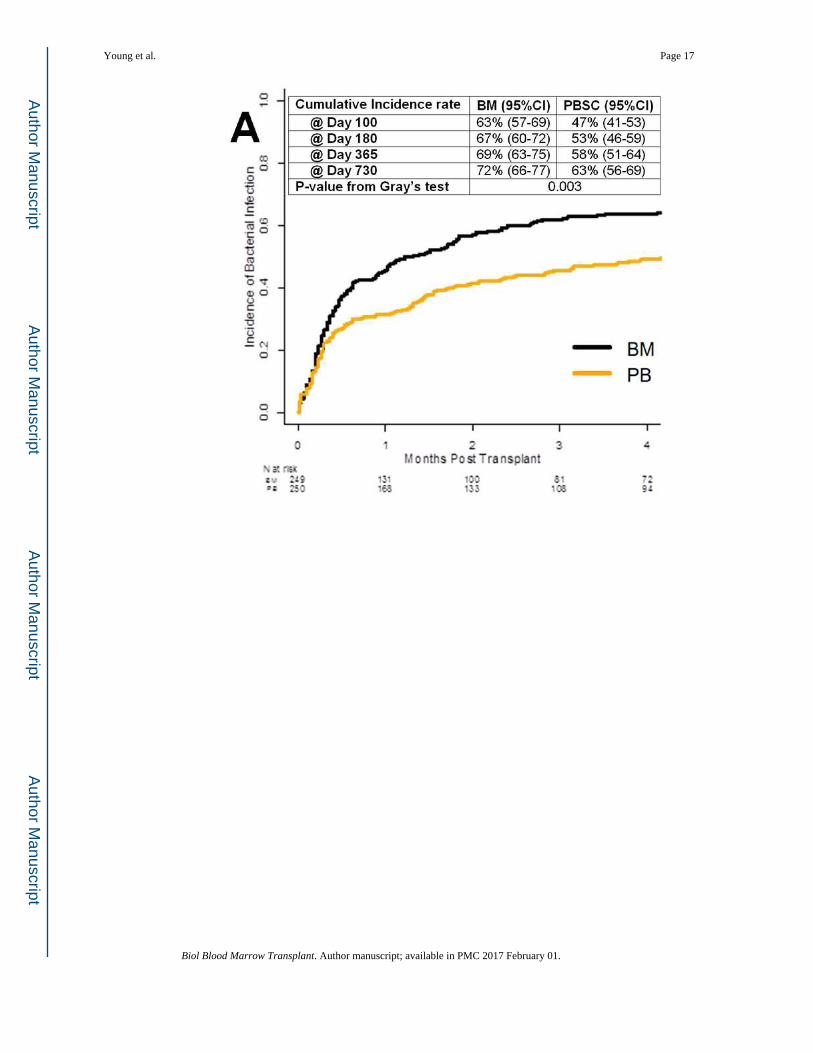
Among 810 bacterial infection episodes, 431 occurred in patients on the BM arm and 379 in
patients on the PBSC arm, with a 2-year cumulative incidence of 72.1% and 62.9%,
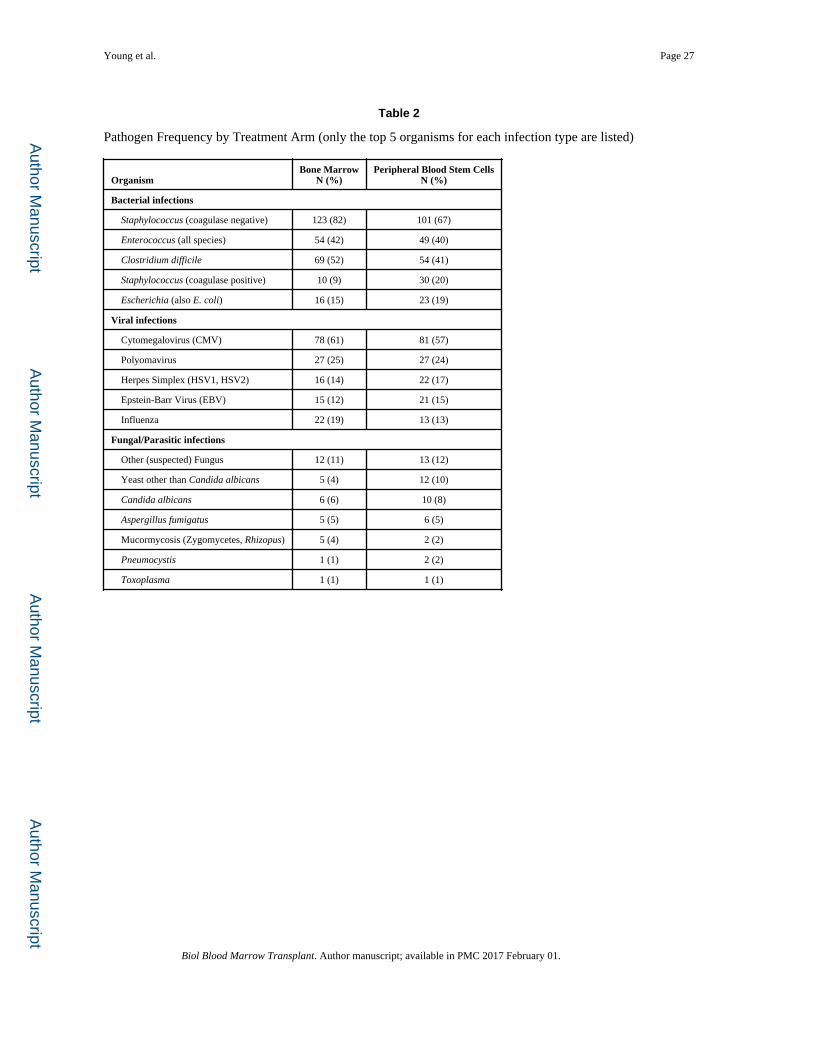
respectively (Figure 3a, P = .003). Among Gram-positive organisms, coagulase negative
Staphylococcus accounted for 224 infection episodes in 149 patients, Staphylococcus aureus
for 40 infections in 29 patients, and Enterococcus (all species) for 103 infections in 82
patients (Table 2). Among Gram-negative infections, Escherichia coli accounted for 39
infection episodes in 34 patients, Klebsiella species for 36 infections in 29 patients,
Pseudomonas species for 32 infections in 25 patients, Enterobacter for 14 infections in 12
patients, and Stenotrophomonas for 13 infections in 12 patients. There were 123 Clostridium
difficile, 5 Nocardia, and 2 non-tuberculous mycobacterial infections. No cases of
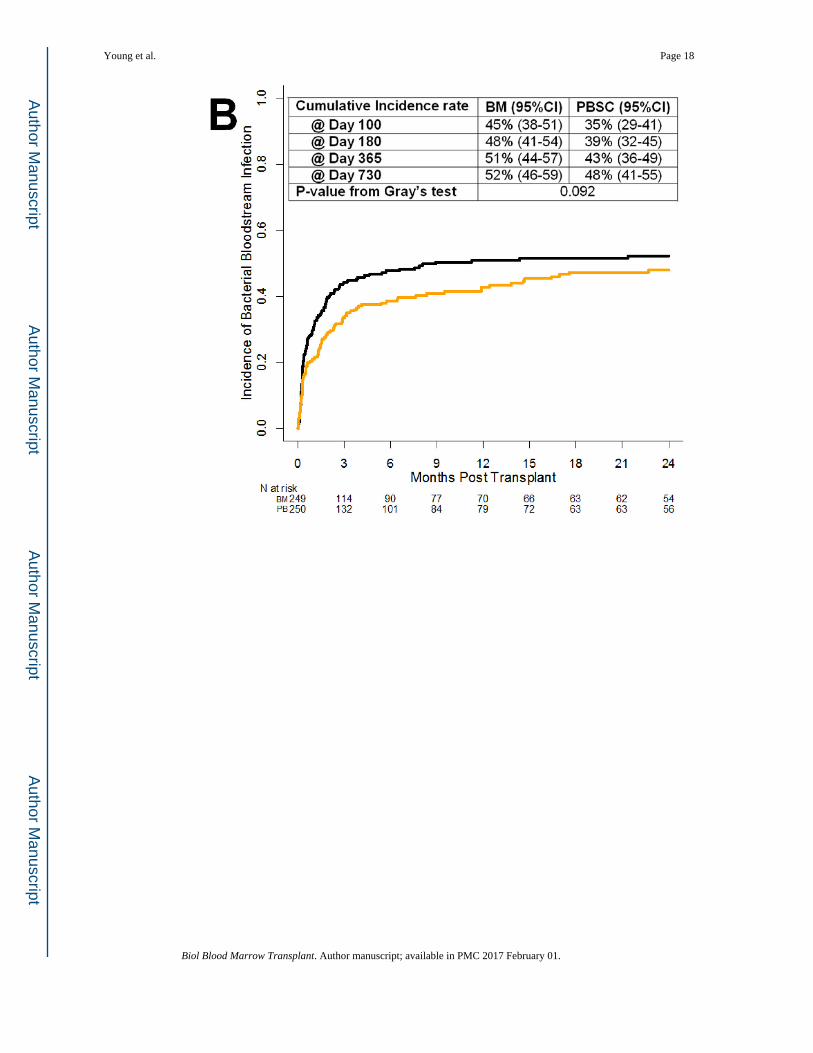
tuberculosis were reported. Of the bacterial infections, 413 were recovered from the
bloodstream. The cumulative incidence of bloodstream bacterial infections during the first
100 days following transplantation was 44.8% (95%CI, 38.5–51.1) for the BM arm vs.
35.0% (95%CI, 28.9–41.1) for the PBSC arm (Figure 3b, P = .092), possibly related to
quicker neutrophil engraftment using PBSC.
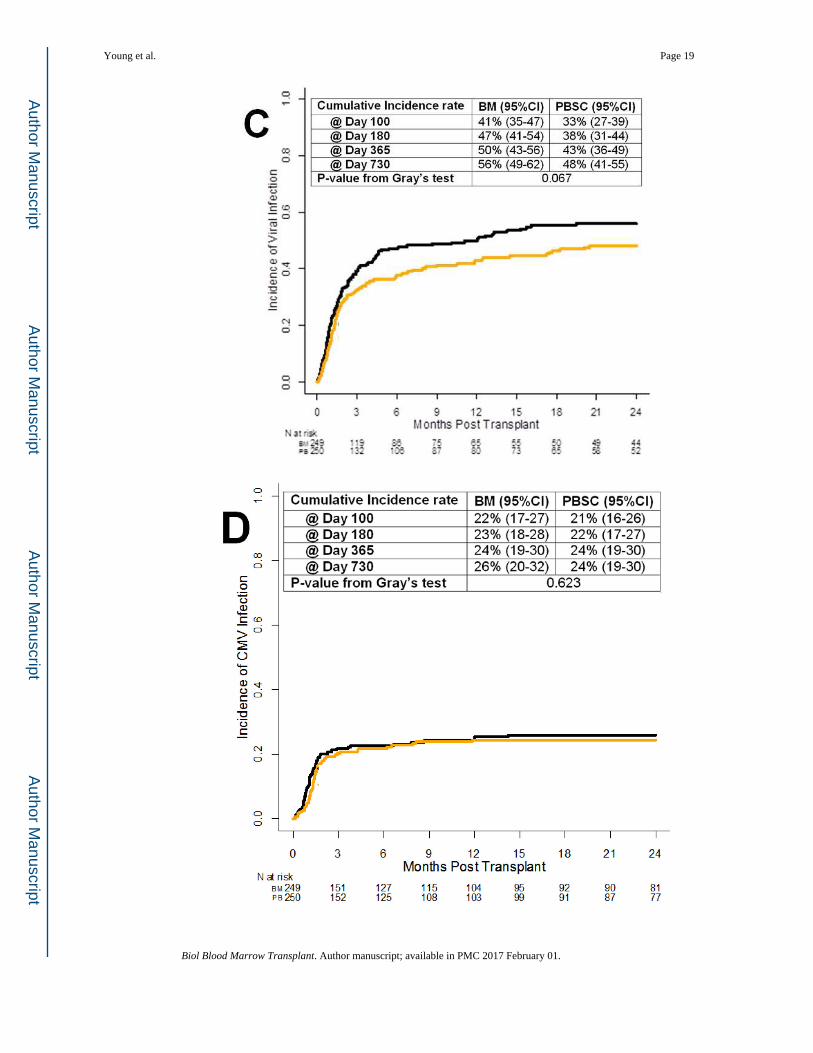
Among 438 viral infection episodes (136 severe and 48 life-threatening and/or fatal), 234
were on the BM arm and 204 on the PBSC arm (Figure 3c). Herpesvirus infections
accounted for the majority of infections. CMV accounted for 159 infection episodes in 118
patients, herpes simplex for 38 infections in 31 patients, Epstein-Barr virus for 36 infections
in 27 patients (none of these 27 patients had anti-thymocyte globulin use reported in the
graft versus host disease treatment form), and varicella for 22 infections in 20 patients.
Respiratory viruses accounted for 93 infection episodes including 35 for influenza, 23
respiratory syncytial virus, 17 parainfluenza virus, 14 adenovirus, and 4 rhinovirus.
Additional clinically significant viral infections included a total of 54 infection episodes
among 49 patients due to polyomavirus (BK virus); 10 due to human herpes virus-6; 2 due
to enterovirus; and 2 due to rotavirus. The 2-year cumulative incidence of CMV infection
was 25.9% (95%CI, 20.2–31.6) for the BM arm, vs. 24.4% (95%CI, 18.8–30.0) for the
PBSC arm (Figure 3d, P = .62). Among 248 CMV-seropositive recipients, the cumulative
incidence of CMV infection was 40.6% (95%CI, 31.8–49.2) in the BM arm compared with
36.9% (95%CI, 27.9–46.0) in the PBSC arm (P = .47). CMV infection episodes occurred in
the bloodstream only in 78.6% of CMV-infected patients, versus progression to non-
bloodstream sites in 21.4%. Among the CMV-infected patients, a later episode of infection
occurred beyond two months from the first infection in 20.3%, although further detail
regarding whether these were recurrent, refractory, or resistant infections is not within the
scope of data collected by this trial. CMV seropositivity did not impact survival in the
models.
Young et al. Page 6
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
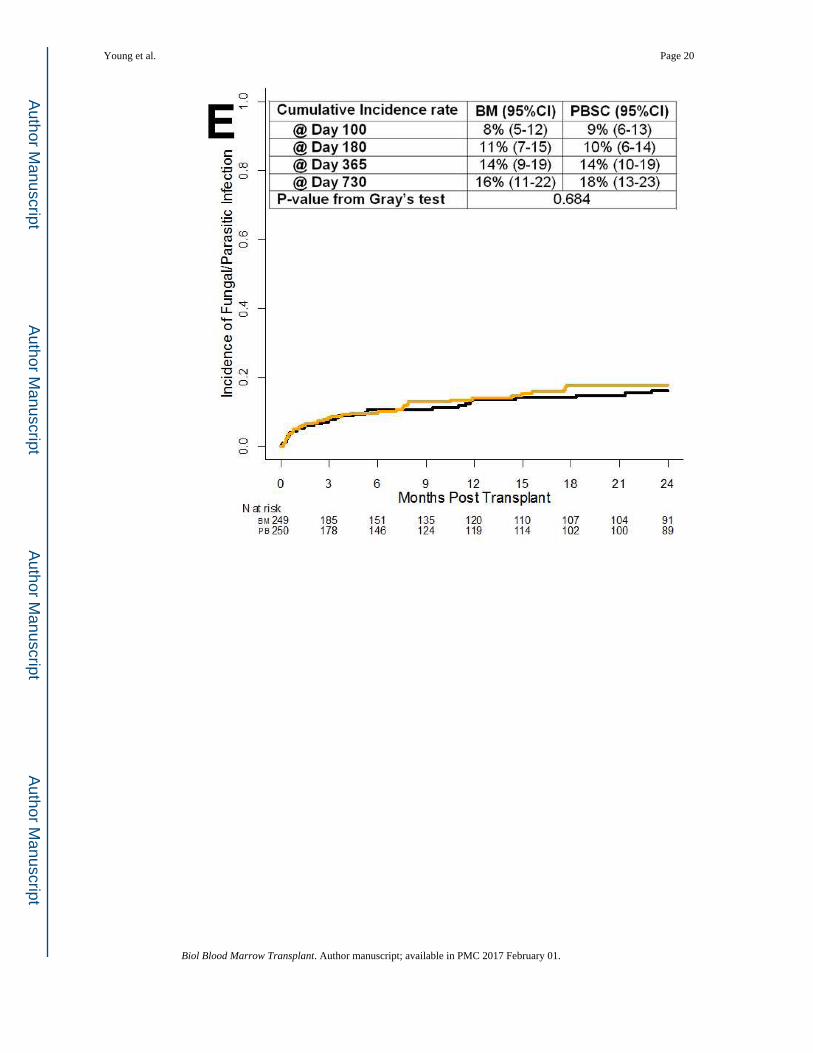
Among 89 fungal infections (Figure 3e), there were 37 due to yeast (including 1 case of
Saccharomyces cerevisiae in the bloodstream), 31 due to mold (20 cases of aspergillosis, 7
of mucormycosis, 2 cases of penicilliosis, 1 case of cavitary pulmonary Microascus, and 1
of fusariosis), and 1 case of coccidioidomycosis. Twenty infection episodes classified as
fungal were cases of infection that were assessed to be responsive to antifungal therapy.
Thirty-one of the fungal infection episodes were severe and 25 were life-threatening and/or
fatal, distributed among 34 patients (13 severe and 9 life-threatening and/or fatal) on the BM
arm and 37 (13 and 9) on the PBSC arm. There were 3 Pneumocystis infections and 1 case
of toxoplasmosis. The Aspergillus species included 11 A. fumigatus, 2 A. niger, and 1 A.
flavus. Six cases of aspergillosis were not speciated. The 2-year cumulative incidence of
invasive aspergillosis was 3.9% (95%CI, 1.2–6.6) for the BM arm, vs. 3.6% (95%CI, 1.0–
6.2) for the PBSC arm (Figure 3f, P = .81).
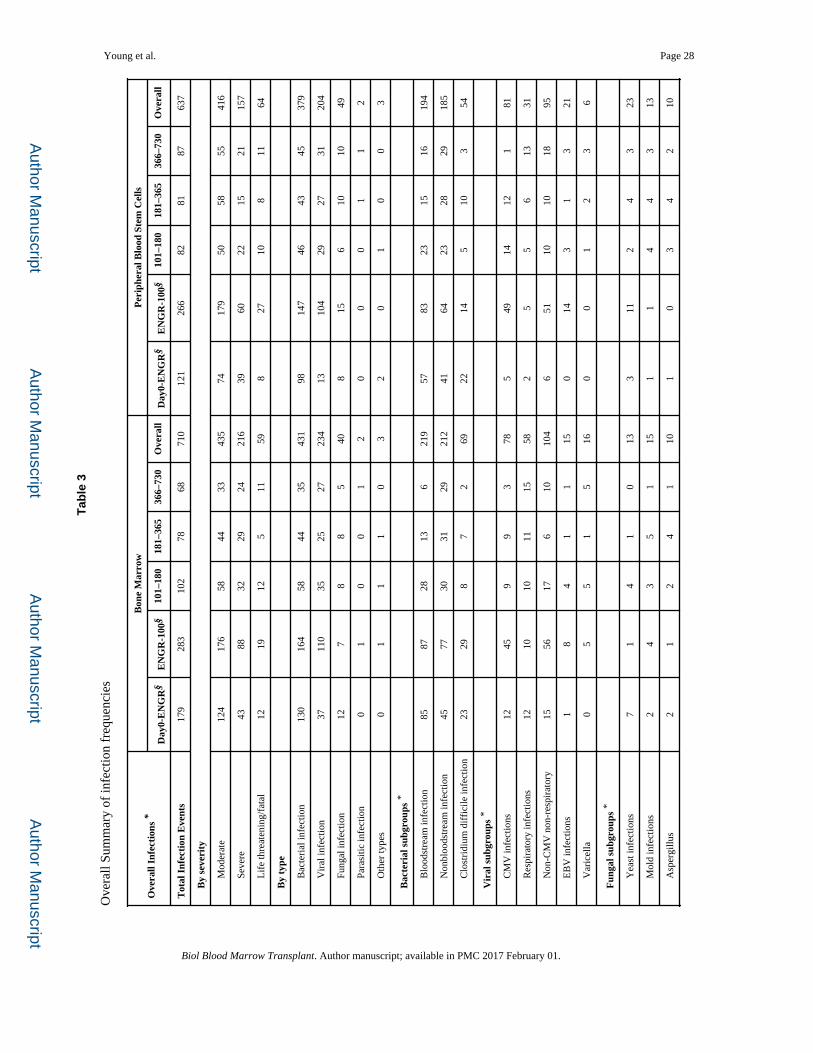
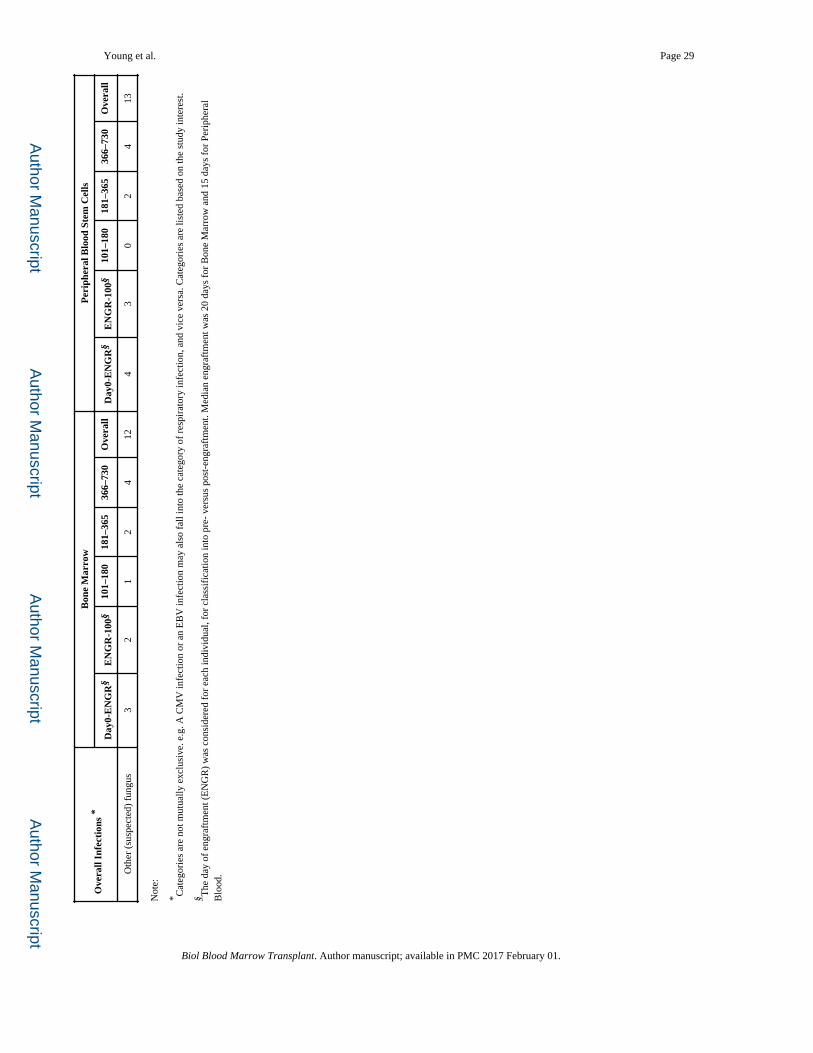
Infection Density
The overall infection density for the study was 0.63 events per 100 patient days at risk; 0.67
for BM and 0.60 for PBSC (Figure 4a). The infection density of bacterial infections was 0.4
for both arms (Figure 4b). The infection density for viral infections was 0.2 in both arms
(Figure 4c). The infection density for fungal/parasitic infections was 0.04 and 0.05 for the
BM and the PBSC arm, respectively (Figure 4d). Infection density for each assessment
period was computed by looking into the infections reported during this period over the risk
days during this period. For example, bacterial bloodstream and non-bloodstream infections
had their highest density during the Day 0 to Day 100 interval (Figure 4e and 4f), and
decreased over time (Table 3). The infection density for infections of moderate, severe, and
life-threatening and/or fatal severity followed a similar trend with regard to infection density
over time (Figures 4g, 4h, and 4i).
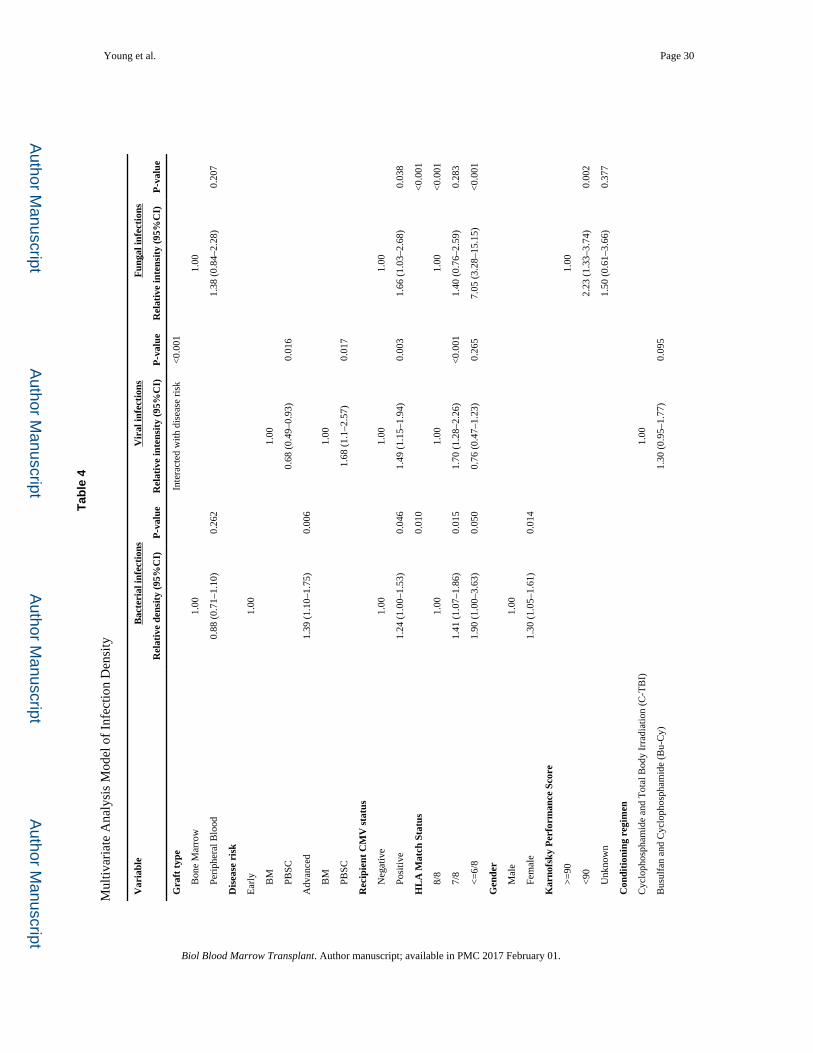
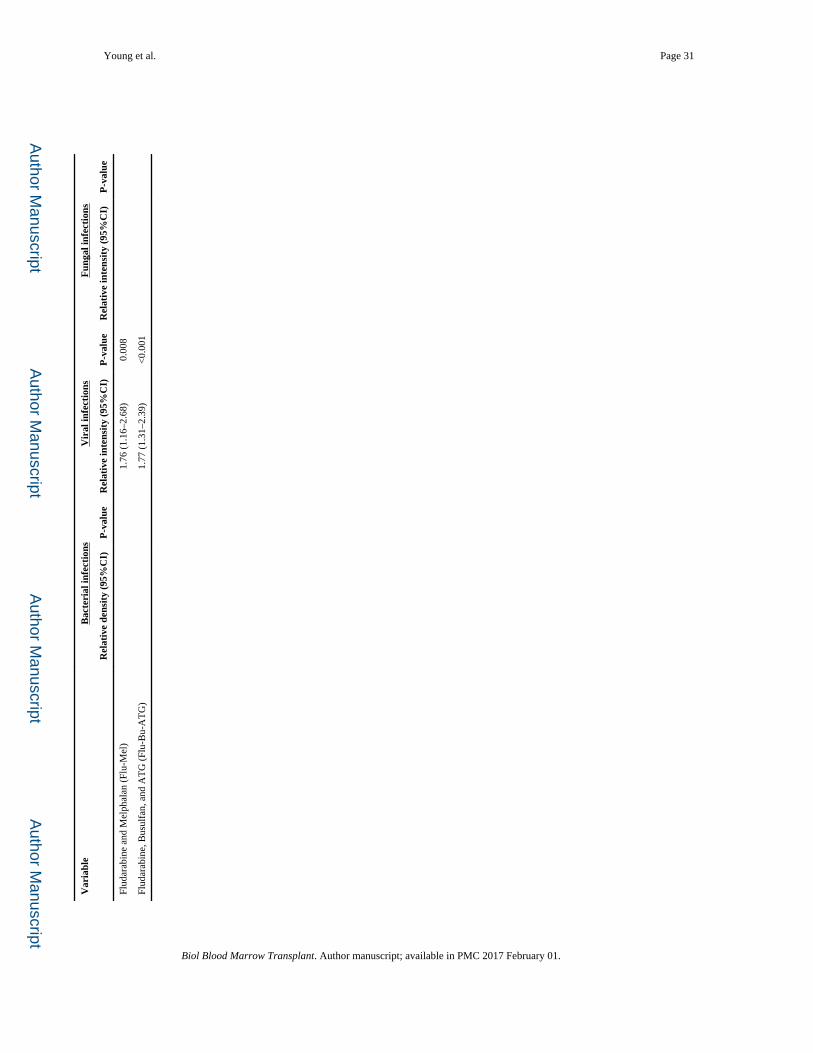
Relationship of Infection to GVHD: Multivariate Analyses
The baseline covariates in Table 1 were considered in the multivariate analyses. In
multivariate analyses of infection density, there were no significant differences between
PBSC and BM for density of bacterial or fungal infections (Table 4). For viral infections, a
significant interaction was detected between graft type and disease risk (P < 0.001), so that
for early disease the risk of viral infections was lower with PBSC compared to BM, while
for advanced / late disease, risks of viral infection were higher with PBSC. However, there
was no overall significant effect of graft type on viral infections if this interaction was
ignored.
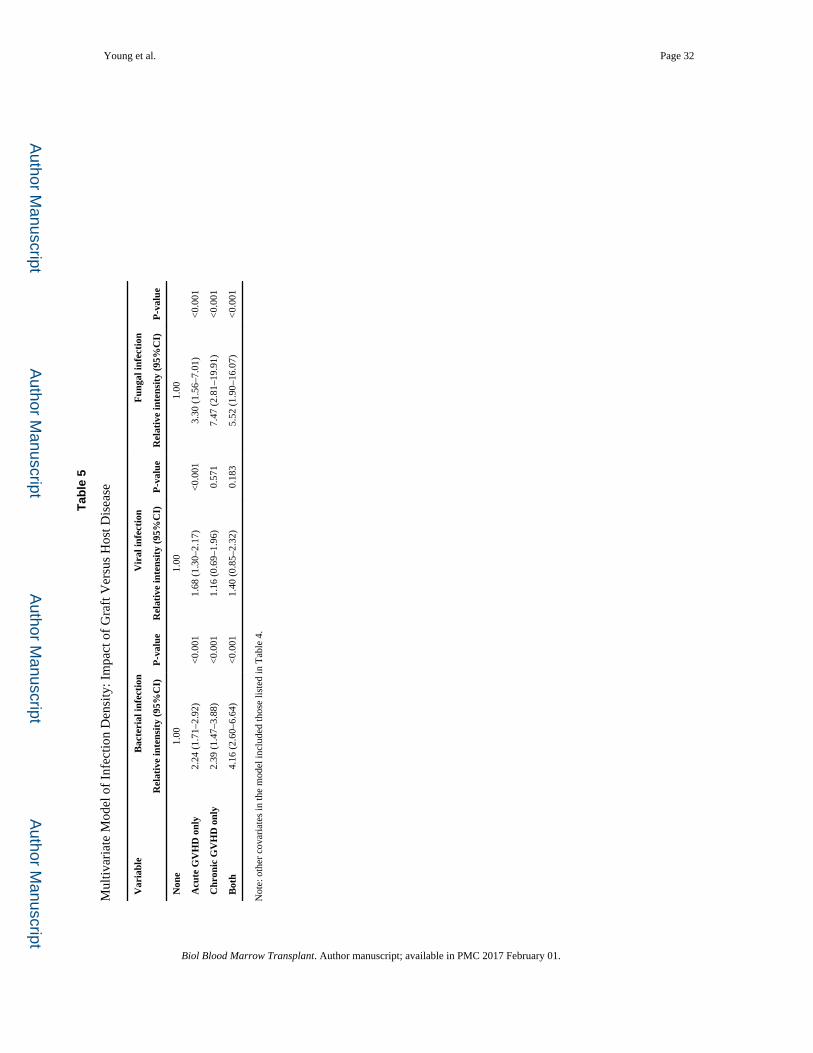
Both acute and chronic GVHD were associated with increased rates of bacterial and fungal
infections in both the BM and PBSC arms (Table 5). Only acute (but not chronic) GVHD
was associated with increased rates of viral infections.
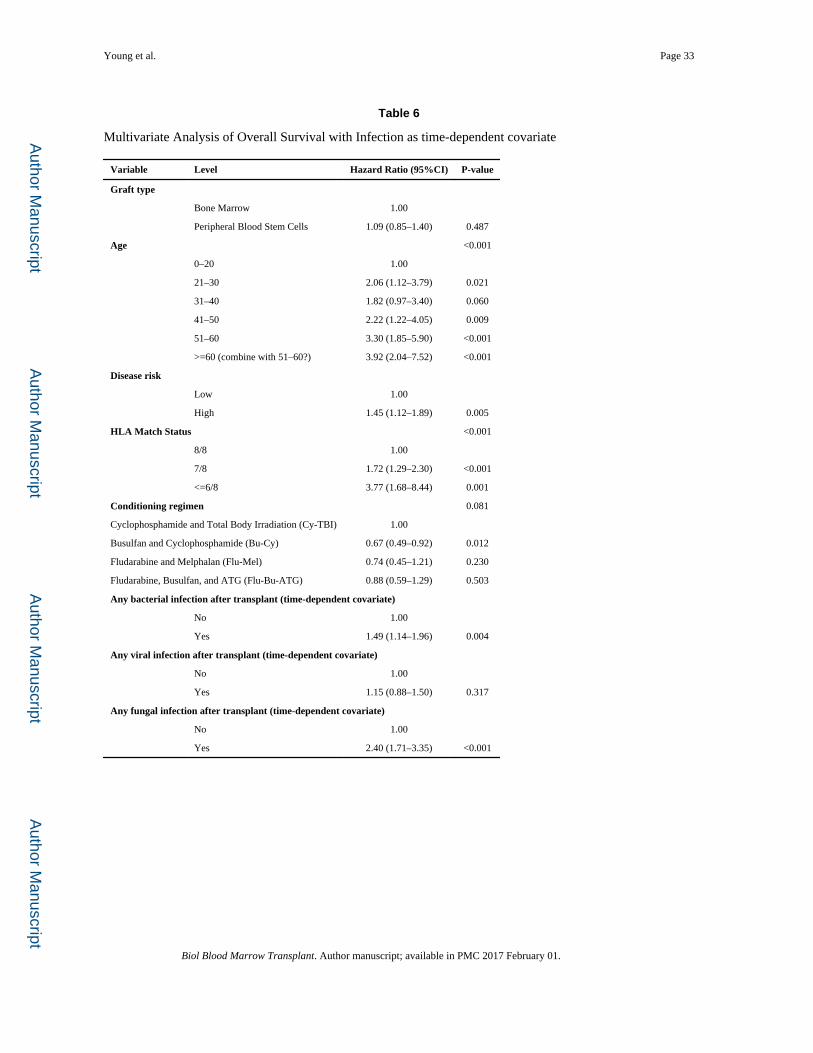
After adjustment for significant covariates including age, conditioning regimen, HLA
matching, and disease risk, bacterial and fungal, but not viral or even specifically CMV,
infections were associated with worse survival in both BM and PBSC recipient groups
(Table 6).
Young et al. Page 7
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Infections within 30 days prior to Death
Infection was reported as a primary cause of death for 11 of 133 deceased patients on the
BM arm and for 9 of 139 on the PBSC arm. Patients where infection was a de novo cause of
death included 2 viral infections (2/11 = 18% of BM, and 22% of PBSC, or ~ 20%) and 1
fungal infection (9% of BM, and 11% of PBSC, or ~ 10%) on each arm, with the remainder
being bacterial infections generally associated with multiorgan failure (73% of BM, and
67% of PBSC, or ~ 70%). We reviewed infections within 30 days of death to examine the
proximate relationship of any infections to death. On the BM arm, 111 infections were
reported on 50 patients within 30 days prior to death; on the PBSC arm, 96 infections were
reported on 39 patients. Of these 207 infections reported within 30 days of death, bacteria
accounted for 138, viruses for 38, and fungi/parasites for 30. Patients with acute or chronic
GVHD reported as the cause of death, and an infection noted as being the most severe
within 30 days of death, had a high percentage of fungal infections (20/52 or ~ 38%), with
fewer viral (~ 14%), bacterial (~44%), or protozoal infections (~ 4%).
Relationship of Infection to Engraftment
The cumulative incidence of infections that occurred among engrafted patients, 1 year
following engraftment, was 71.1% (95%CI, 64.4–76.9) for the BM arm vs. 67.2% (95%CI,
60.1–73.2) for the PBSC arm (P = .23) (Figure 5a). The cumulative incidence of pre-
engraftment infections (occurring before Day 30) was 47.9% (95%CI, 41.5–53.9) for the
BM arm vs. 32.8% (95%CI, 27.1–38.7) for the PBSC arm (P = .002) (Figure 5b).
DISCUSSION
We analyzed all infection events during two years of follow-up for two randomly assigned
graft source treatment arms for unrelated donor myeloablative hematopoietic cell
transplantation patients who participated in BMT CTN 0201 (a minority were not
myeloablative). When the trial was designed, we hypothesized that infection may play a
major role in augmenting morbidity and mortality in this randomized trial, so infection
events were collected prospectively as a prespecified secondary outcome. This multicenter,
randomized phase 3 trial demonstrated that infections remain common and occurred for 85%
of BM recipients and 80% of PBSC recipients. Strengths of this prospective study are the
large sample size, as well as the detailed and audited data capture on all infections during
extended follow-up. No previous comparison of these 2 graft sources for use in
transplantation has such a rich and detailed infection database with which to examine
infectious complications for this important question of PBSC or BM as the graft source for
allogeneic hematopoietic cell transplantation.
In this large randomized study of allogeneic hematopoietic cell transplantation, we observed
a cumulative incidence of bacterial infections that is higher among patients who received
BM rather than PBSC grafts for transplantation. The cumulative incidence of infections was
driven by bacterial infections occurring before Day 100. Since the median time to neutrophil
engraftment was 5 days longer for BM recipients than for those randomly assigned to
receive PBSC, it is not surprising to see many bacterial infections early after transplant.
These bacterial infections were more common prior to engraftment and over the two years
Young et al. Page 8
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
following transplantation, but speed of engraftment or graft failure alone did not wholly
account for this finding. Bacterial bloodstream infections accounted for 30% of all
infections, a finding similar to an earlier prospective study of T cell depletion to limit
GVHD after unrelated donor hematopoietic cell transplantation [17].
There are no data regarding pre- or peri-transplant prophylaxis agents used, especially
relevant for quinolones with the 123 cases of Clostridium difficile infection during this time
prior to use of toxin-based PCR assays. As a result, antibacterial prophylaxis is a baseline
characteristic that probably modulates the events seen but cannot otherwise be assessed.
During the analysis of transplant-related endpoints for this study, recipients of PBSC grafts
had a higher rate of chronic GVHD, so infections that occurred after Day 100 were of
particular interest, especially viral and fungal infections. CMV infections were not more
frequent using BM or PBSC, even in the setting of GVHD. This study is the first
comparative, long-term follow-up trial with infection data and does not support late CMV
disease as a common event. Our database was not structured to capture self-limited (i.e.,
untreated) CMV viremia. Our database did not capture recurrent, refractory, or resistant
CMV.
The probability of developing a clinically important CMV infection was less than 30% in
each arm, a rate consistent with other studies published in the last 10 years, and lower than
studies published earlier [17,24–26]. In our study, there were 61 CMV infection episodes on
the BM arm and 57 infections for patients transplanted using PBSC. The infection density
for CMV infections was 0.25 for BM and 0.24 for PBSC during the Day 0 to Day 100
interval, declining to 0.06 for BM and to 0.10 for PBSC during the Day 100 to Day 180
interval, and to 0.03 for BM and to 0.05 for PBSC during the Day 181 to Day 365 interval.
Survival among patients who developed a CMV infection was 41% for the BM arm and
49% for the PBSC arm. Regardless of study arm, this overall improved rate of any CMV
infection, in comparison to studies published over the last 20 years, likely reflects changes in
CMV monitoring/preemptive schemas, anti-CMV prophylaxis, the stem cell product itself,
and in conditioning regimens over time. The rapid turnaround time in the newest generation
of CMV diagnostic testing, and the availability of oral antiviral agents (e.g., valganciclovir),
may have contributed to the low and comparable rates of CMV between the study arms.
By 2 years after transplant, the cumulative incidence of Aspergillus infection was 4% in
each study arm, much lower than previously reported rates of 10–15% [17,27]. The 4% rate
(20 cases) represents some form of culture and/or histopathologic documentation, so these
are cases of proven or probable infection but not possible infection. This is the lowest
estimate of invasive aspergillosis in any allogeneic hematopoietic stem cell transplant series.
The low rates of invasive aspergillosis may be related to ascertainment bias. Centers
participating in this Clinical Trials Network perform bronchoscopies with various levels of
aggressiveness, and when a bronchoscopy is performed, may have variable testing for
Aspergillus galactomannan using lavage fluid. Thus, there is an undercount of probable and
proven invasive aspergillosis since many of these pneumonias end up being “possible”
invasive fungal infections or merely are treated empirically as fungal infection; in fact, there
Young et al. Page 9
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
were 20 infection episodes classified as fungal that were cases of infection that were
assessed to be responsive to antifungal therapy.
Diagnostic testing for fungal infections was in a state of evolution during the years that this
study was conducted. While the improvement in cumulative incidence is likely related to
advances in antifungal agents that can be successfully employed with less toxicity and with
prophylactic intent over the last 15 years, there was still a nontrivial rate of invasive fungal
infections for the patients on this study. The 2-year cumulative incidence of invasive fungal
infections was 16% for BM patients and 18% for PBSC patients. This includes 7 cases of
mucormycosis, a fungal organism that is not within the spectrum of activity of either
voriconazole or echinocandins, as well as 25 cases of “other fungus”, some of which were
clinical cases of pulmonary nodules responsive to antifungal therapy.
This detailed review of prospectively reported infectious disease events speaks to the
challenges to infection data completeness and accuracy, even in this prospective and
carefully monitored randomized trial. Despite prospective reporting, the initial audit of 15%
of the patients (583 infections for 78 patients) identified frequent minor errors among one or
more of the different data points associated with each infection (date, organism, body site,
clinical severity). While these disagreements were not entirely correct as originally entered,
most of these disagreements were minor did not affect the final results.
Accuracy of infection reporting goes down markedly after Day 100, when most patients
leave the transplant center. When the accumulated list of all the infections was compared to
the primary source documents, 65 previously unreported infections were identified. More
than half of these infections occurred after Day 100. Twenty-two infections occurred after
engraftment but before Day 100, of which two thirds were bacterial often coagulase negative
Staphylococcus and one third were viral often CMV. The follow-up site self-audit used for
this study indicates the importance of data accuracy, and argues for this type of approach in
future studies evaluating complex, multiple endpoint infectious disease data, even if
prospectively collected.
The data coordinating center has submitted all study data from this clinical trial, including
these infection data, to the National Heart, Lung, and Blood Institute (NHLBI) data
repository, so that future users should be able to access the data from a public end.
There are several limitations to interpreting a complex infection database when collected
from hospitals across the study. There are differences in diagnostic testing at the various
sites, and incidence rates may be altered based on current testing strategies (particularly for
respiratory viruses and fungal infections). Additionally, with the detailed and complete
retrospective audit of the protocol prescribed monitoring of infections, it is unlikely that
many major infections were unrecognized.
This study noted a tremendous burden of infection among transplanted patients. Fortunately,
infection was an uncommon cause of death. The incidence and severity of infection is lower
than historical cohorts. The greatest differences were seen in the pre-engraftment time
period. We need ways to continue to drive down the burden of infection for all patients.
Morbidity and mortality from infection following transplantation was frequent using either
Young et al. Page 10
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
graft source, with no observed differences in fungal or viral infection rates. Among those
who died, few had infection reported as the primary cause of death although many infections
occurred in the final month of life. The higher observed risks of bacterial infections using
BM grafts may suggest either augmented prophylaxis or heightened surveillance after these
transplants.
Supplementary Material
Refer to Web version on PubMed Central for supplementary material.
Acknowledgments
Supported by a grant from the National Heart, Lung, and Blood Institute and the National Cancer Institute (U10HL069294), by the Office of Naval Research, and by the National Marrow Donor Program. Disclosure forms were provided by the authors. We thank the transplantation-center teams in the United States and Canada for enrolling patients in this trial; the donor-center teams in the United States, Canada, and Germany for recruiting the donors for the trial; and the National Marrow Donor Program coordinating center for facilitating the transplantations.
We thank the infectious disease auditors at each center: Nathalie Lachapelle and Jean Roy (Hôpital Maisonneuve-Rosemont), Susan Durham (Cohen Children’s Medical Center), Karen Parrott (University of Iowa Hospitals and Clinics), Andrea Ortega (Hackensack University Medical Center), Mindy Shuster (University of Pennsylvania Cancer Center), Jessica Piggee (Vanderbilt University Medical Center), Margaret Shea and Francisco Marty (Dana-Farber Cancer Institute and Brigham and Women’s Hospital), Erik Dubberke (Washington University: Barnes-Jewish), Juliana Ongley (University of California, San Diego), Lisa Malick (University of Maryland Cancer Center), Stanley Martin (Ohio State: Arthur G. James Cancer Hospital), Valerie Dorcas (Queen Elizabeth II Health Sciences Centre), JoDell McCracken (Texas Transplant Institute), Lisa Dutton (Mayo Clinic, Rochester), Lynne Strasfeld (Oregon Health & Science University), Daniel Kaul (University of Michigan Health System), Ginger Butterworth (Baylor University Medical Center), Lisa Williams (University of Alabama at Birmingham), Michael Pulsipher (Primary Children’s Hospital/Utah BMT), David Hurd (Wake Forest University), Tia Thomas (Washington University: St. Louis Children’s Hospital), Melissa Moynihan (Vancouver General Hospital), Amy O’Sullivan, Brittni Prosdocimo, and Mounzer Agha (University of Pittsburgh Cancer Institute), Janice (Wes) Brown (Stanford Hospital and Clinics), Greg McFadden (University of Nebraska Medical Center), Lynn Savoie (Tom Baker Cancer Centre), Patti Cunningham (Oklahoma University Medical Center), Adina Londrc (City of Hope National Medical Center), John Wingard (University of Florida: College of Medicine), Rebecca Gerkin (Emory University Hospital), Tammy DeGelder (McMaster University Medical Centre: Hamilton Health Sciences), Shaun DeJarnette and Abhyankar (University of Kansas Medical Center), Carol Cutrone (Loyola University Medical Center), Sofia Qureshi (MD Anderson Cancer Center), Jueleah Expose’-Spencer (University of California, San Francisco), Isabel Belen (University of Toronto: Princess Margaret), Jessica Greene (Roswell Park Cancer Institute), Mitch Horwitz (Duke University Medical Center), and Steven Pergam (Fred Hutchinson Cancer Research Center).
References
1. Anasetti C, Logan BR, Lee SJ, et al. Peripheral-blood stem cells versus bone marrow from unrelated donors. N Engl J Med. 2012; 367:1487–1496. [PubMed: 23075175]
2. Holtick U, Albrecht M, Chemnitz JM, et al. Comparison of bone marrow versus peripheral blood allogeneic hematopoietic stem cell transplantation for hematological malignancies in adults-a systematic review and meta-analysis. Crit Rev Oncol Hematol. 2014
3. Holtick U, Albrecht M, Chemnitz JM, et al. Bone marrow versus peripheral blood allogeneic haematopoietic stem cell transplantation for haematological malignancies in adults. Cochrane Database Syst Rev. 2014; 4:CD010189. [PubMed: 24748537]
4. Stamatovic D, Balint B, Tukic L, et al. Impact of stem cell source on allogeneic stem cell transplantation outcome in hematological malignancies. Vojnosanit Pregl. 2011; 68:1026–1032. [PubMed: 22352263]
5. Korbling M. Peripheral Blood Stem Cells: A Novel Source for Allogeneic Transplantation. Oncologist. 1997; 2:104–113. [PubMed: 10388037]
Young et al. Page 11
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
6. Appelbaum FR. Choosing the source of stem cells for allogeneic transplantation: no longer a peripheral issue. Blood. 1999; 94:381–383. [PubMed: 10397703]
7. Campregher PV, Hamerschlak N, Colturato VA, et al. Survival and graft-versus-host disease in patients receiving peripheral stem cell compared to bone marrow transplantation from HLA-matched related donor: retrospective analysis of 334 consecutive patients. Eur J Haematol. 2015
8. Serody JS, Sparks SD, Lin Y, et al. Comparison of granulocyte colony-stimulating factor (G-CSF)--mobilized peripheral blood progenitor cells and G-CSF--stimulated bone marrow as a source of stem cells in HLA-matched sibling transplantation. Biol Blood Marrow Transplant. 2000; 6:434–440. [PubMed: 10975512]
9. Champlin RE, Schmitz N, Horowitz MM, et al. Blood stem cells compared with bone marrow as a source of hematopoietic cells for allogeneic transplantation. IBMTR Histocompatibility and Stem Cell Sources Working Committee and the European Group for Blood and Marrow Transplantation (EBMT). Blood. 2000; 95:3702–3709. [PubMed: 10845900]
10. Barge RM, Brouwer RE, Beersma MF, et al. Comparison of allogeneic T cell-depleted peripheral blood stem cell and bone marrow transplantation: effect of stem cell source on short- and long-term outcome. Bone Marrow Transplant. 2001; 27:1053–1058. [PubMed: 11438820]
11. Tomblyn M, Chiller T, Einsele H, et al. Guidelines for preventing infectious complications among hematopoietic cell transplantation recipients: a global perspective. Biol Blood Marrow Transplant. 2009; 15:1143–1238. [PubMed: 19747629]
12. Sherertz RJ, Belani A, Kramer BS, et al. Impact of air filtration on nosocomial Aspergillus infections. Unique risk of bone marrow transplant recipients. American Journal of Medicine. 1987; 83:709–718. [PubMed: 3314494]
13. Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of america. Clin Infect Dis. 2011; 52:e56–93. [PubMed: 21258094]
14. Pollack M, Heugel J, Xie H, et al. An international comparison of current strategies to prevent herpesvirus and fungal infections in hematopoietic cell transplant recipients. Biol Blood Marrow Transplant. 2011; 17:664–673. [PubMed: 20699126]
15. Tuan IZ, Dennison D, Weisdorf DJ. Pneumocystis carinii pneumonitis following bone marrow transplantation. Bone Marrow Transplant. 1992; 10:267–272. [PubMed: 1422481]
16. Boeckh M, Boivin G. Quantitation of cytomegalovirus: methodologic aspects and clinical applications. Clin Microbiol Rev. 1998; 11:533–554. [PubMed: 9665982]
17. van Burik J-AH, Carter SL, Freifeld AG, et al. Higher-risk of cytomegalovirus and aspergillus infections in recipients of T cell depleted unrelated bone marrow: Analysis of infectious complications in patients treated with T cell depletion versus immune suppressive therapy to prevent graft-versus-host disease. Biology of Blood and Marrow Transplant. 2007; 13:1487–1498.
18. Copelan E, Casper JT, Carter SL, et al. A scheme for defining cause of death and its application in the T cell depletion trial. Biol Blood Marrow Transplant. 2007; 13:1469–1476. [PubMed: 18022577]
19. Kurtzberg J, Prasad VK, Carter SL, et al. Results of the Cord Blood Transplantation Study (COBLT): clinical outcomes of unrelated donor umbilical cord blood transplantation in pediatric patients with hematologic malignancies. Blood. 2008; 112:4318–4327. [PubMed: 18723429]
20. Tomblyn M, Young JA, Haagenson MD, et al. Decreased infections in recipients of unrelated donor hematopoietic cell transplantation from donors with an activating KIR genotype. Biol Blood Marrow Transplant. 2010; 16:1155–1161. [PubMed: 20197104]
21. Barker JN, Hough RE, van Burik JA, et al. Serious infections after unrelated donor transplantation in 136 children: impact of stem cell source. Biol Blood Marrow Transplant. 2005; 11:362–370. [PubMed: 15846290]
22. Bachanova V, Brunstein CG, Burns LJ, et al. Fewer infections and lower infection-related mortality following non-myeloablative versus myeloablative conditioning for allotransplantation of patients with lymphoma. Bone Marrow Transplant. 2009; 43:237–244. [PubMed: 18806838]
23. Lin D, Wei L, Yang I, Ying Z. Semiparametric Regression for the Mean and Rate Functions of Recurrent Events. Journal of the Royal Statistical Society. 2000; 62:711–730.
Young et al. Page 12
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
24. Boeckh M, Gooley TA, Myerson D, Cunningham T, Schoch G, Bowden RA. Cytomegalovirus pp65 antigenemia-guided early treatment with ganciclovir versus ganciclovir at engraftment after allogeneic marrow transplantation: a randomized double-blind study. Blood. 1996; 88:4063–4071. [PubMed: 8916975]
25. Qayed M, Khurana M, Hilinski J, et al. Risk for CMV reactivation in children undergoing allogeneic hematopoietic stem cell transplantation. Pediatr Blood Cancer. 2014
26. Walker CM, van Burik JA, De For TE, Weisdorf DJ. Cytomegalovirus infection after allogeneic transplantation: comparison of cord blood with peripheral blood and marrow graft sources. Biol Blood Marrow Transplant. 2007; 13:1106–1115. [PubMed: 17697973]
27. Wald A, Leisenring W, van Burik JA, Bowden RA. Epidemiology of Aspergillus infections in a large cohort of patients undergoing bone marrow transplantation. J Infect Dis. 1997; 175:1459–1466. [PubMed: 9180187]
Young et al. Page 13
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Highlights
• Infections following unrelated donor transplantation remain frequent using
either graft source, with no difference in fungal or viral rates
• Bone marrow graft recipients had higher rates of bacterial and pre-engraftment
infections
Young et al. Page 14
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
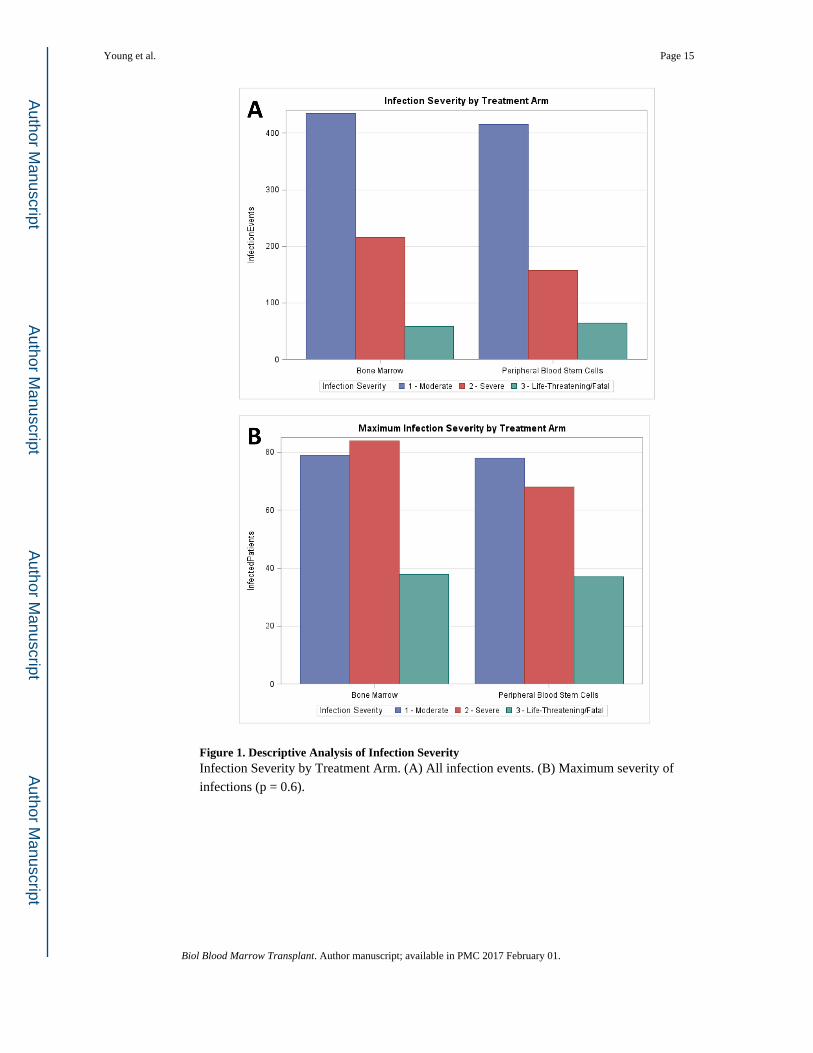
Figure 1. Descriptive Analysis of Infection SeverityInfection Severity by Treatment Arm. (A) All infection events. (B) Maximum severity of
infections (p = 0.6).
Young et al. Page 15
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
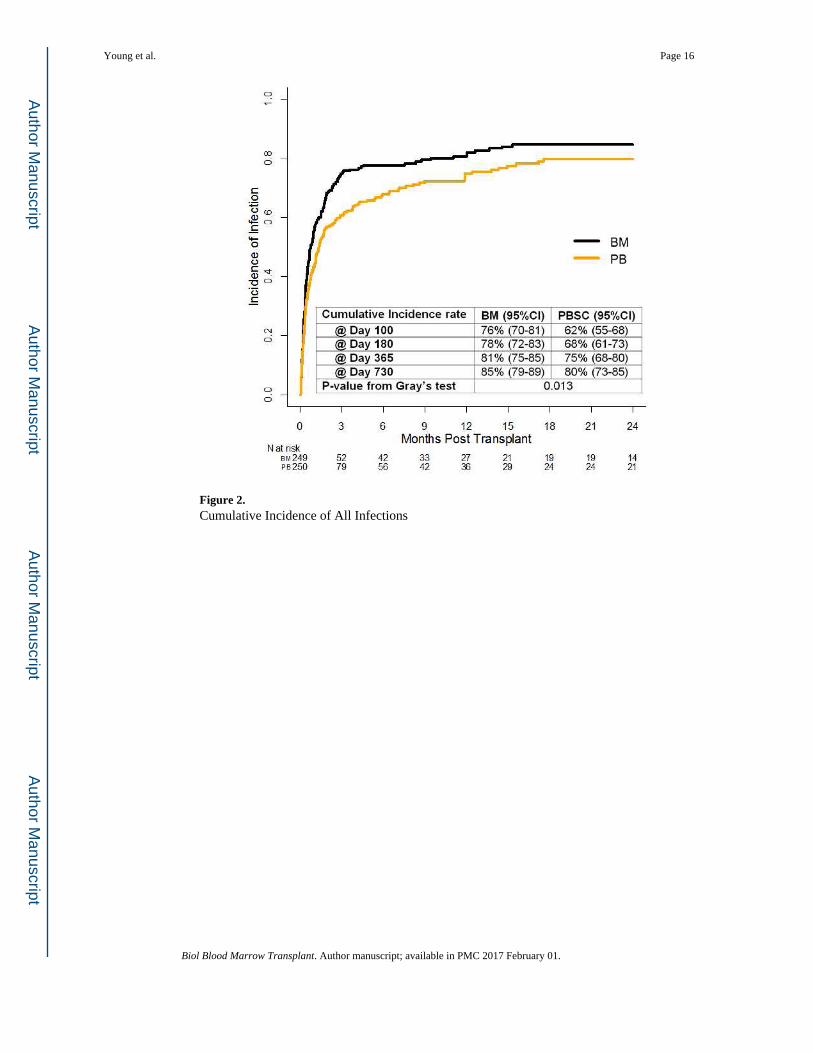
Figure 2. Cumulative Incidence of All Infections
Young et al. Page 16
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Young et al. Page 17
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Young et al. Page 18
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Young et al. Page 19
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Young et al. Page 20
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
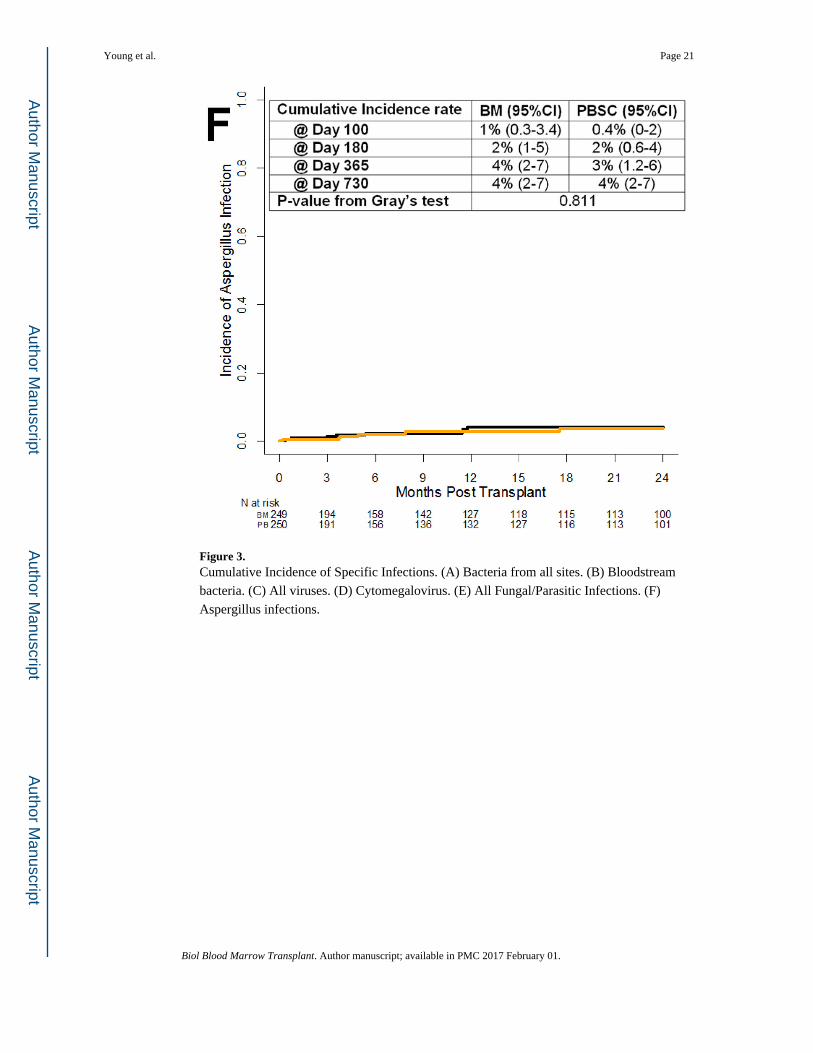
Figure 3. Cumulative Incidence of Specific Infections. (A) Bacteria from all sites. (B) Bloodstream
bacteria. (C) All viruses. (D) Cytomegalovirus. (E) All Fungal/Parasitic Infections. (F)
Aspergillus infections.
Young et al. Page 21
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
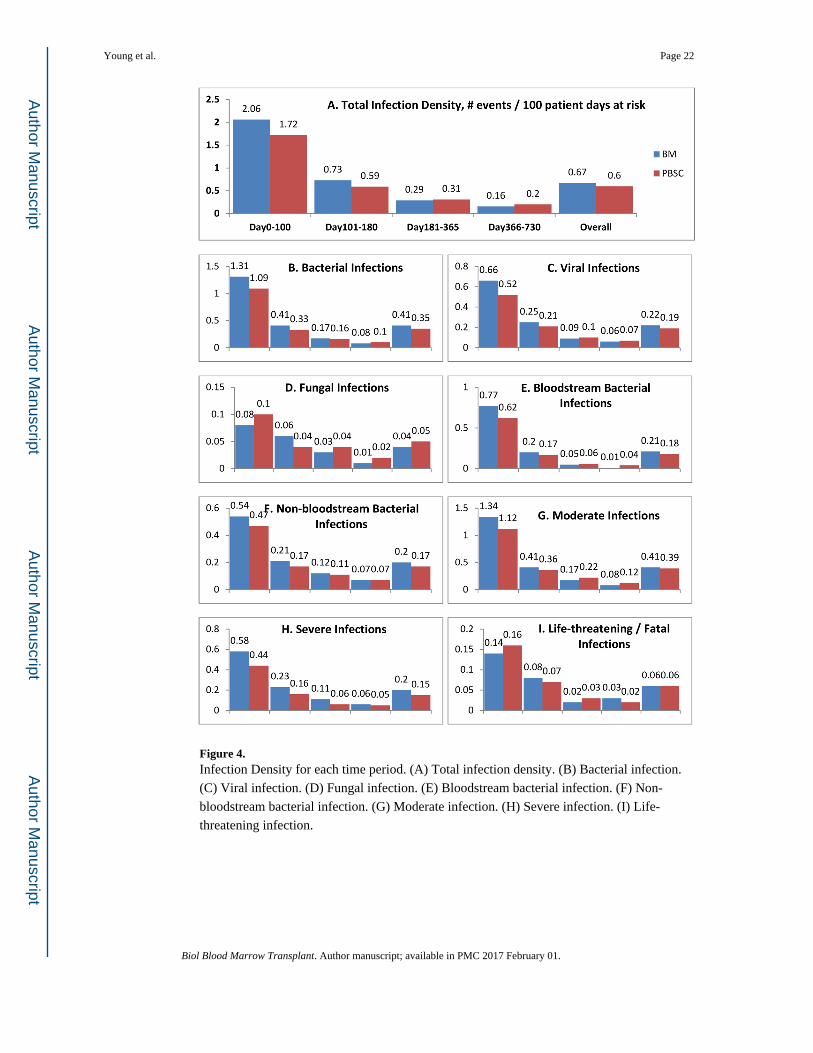
Figure 4. Infection Density for each time period. (A) Total infection density. (B) Bacterial infection.
(C) Viral infection. (D) Fungal infection. (E) Bloodstream bacterial infection. (F) Non-
bloodstream bacterial infection. (G) Moderate infection. (H) Severe infection. (I) Life-
threatening infection.
Young et al. Page 22
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
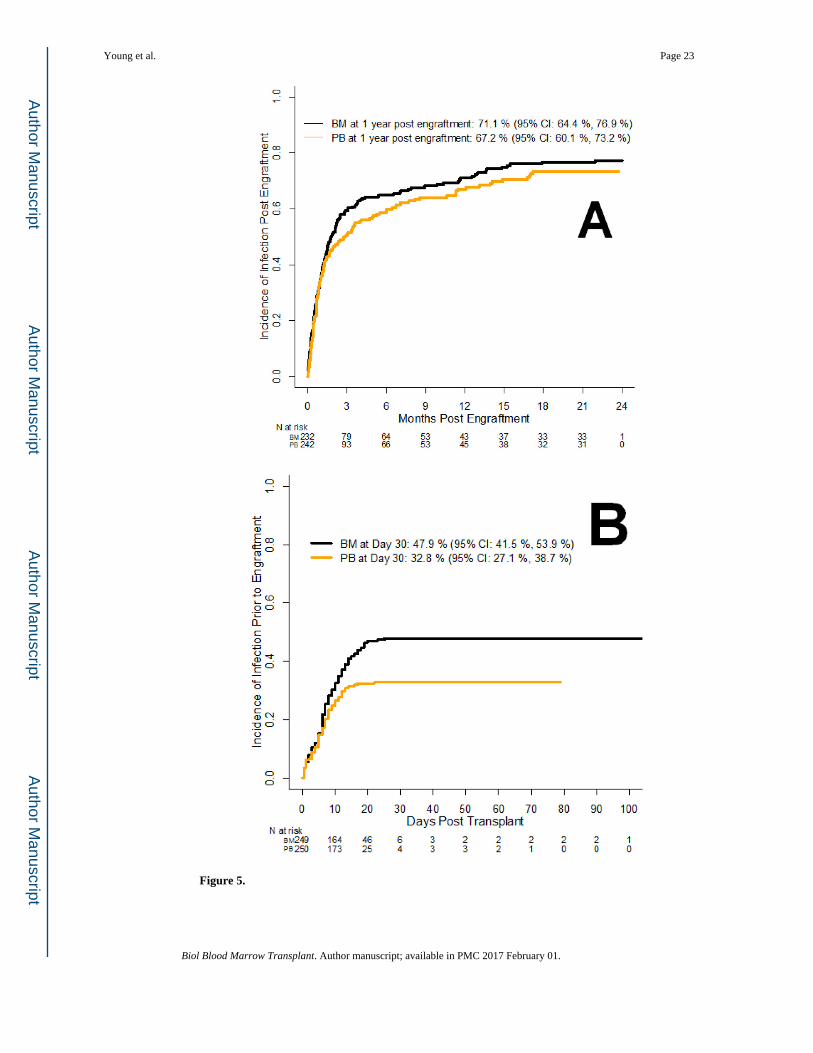
Figure 5.
Young et al. Page 23
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
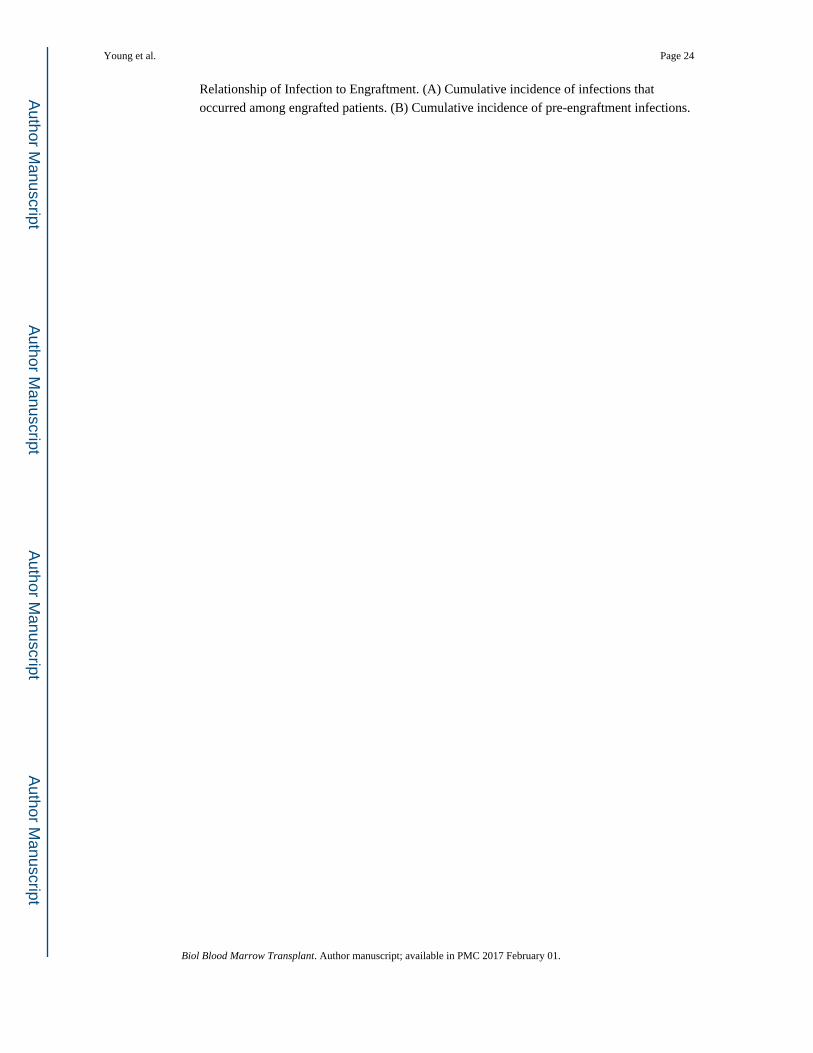
Relationship of Infection to Engraftment. (A) Cumulative incidence of infections that
occurred among engrafted patients. (B) Cumulative incidence of pre-engraftment infections.
Young et al. Page 24
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Young et al. Page 25
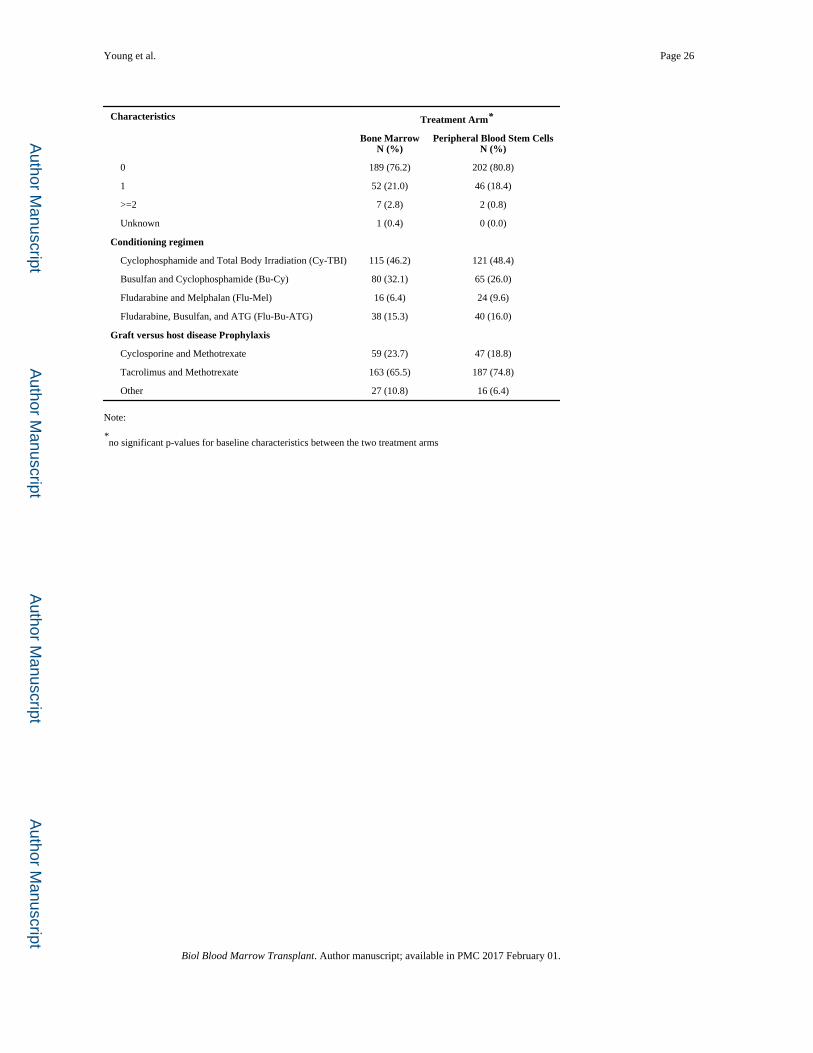
Table 1
Baseline Characteristics
Characteristics Treatment Arm*
Bone MarrowN (%)
Peripheral Blood Stem CellsN (%)
Total (N=499) 249 (100.0) 250 (100.0)
Age (years)
Median 44.1 43.8
<40 105 (42.2) 103 (41.2)
>=40 144 (57.8) 147 (58.8)
Recipient Gender
Male 147 (59.0) 135 (54.0)
Race
White 226 (90.8) 227 (90.8)
Others 23 (9.2) 23 (9.2)
Ethnicity
Hispanic or Latino 9 (3.6) 12 (4.8)
Others 240 (96.4) 238 (95.2)
Karnofsky Performance Score
90–100 165 (66.3) 150 (60.0)
<90 64 (25.7) 71 (28.4)
Unknown 20 (8.0) 29 (11.6)
Primary Disease at Enrollment
Acute Myelogenous Leukemia 116 (46.6) 122 (48.8)
Acute Lymphoblastic Leukemia 54 (21.7) 52 (20.8)
Chronic Myelogenous Leukemia 27 (10.8) 32 (12.8)
Myelodysplastic Syndrome 46 (18.5) 37 (14.8)
Chronic Myelomonocytic Leukemia 4 (1.6) 3 (1.2)
Disease risk
Early 182 (73.1) 181 (72.4)
Advanced 67 (26.9) 69 (27.6)
Donor/Recipient Gender
Female/Female 33 (13.3) 50 (20.0)
Male/Male 115 (46.2) 102 (40.8)
Female/Male 32 (12.8) 33 (13.2)
Male/Female 69 (27.7) 65 (26.0)
Donor/Recipient CMV Status
Positive/Positive 42 (16.9) 52 (20.8)
Negative/Negative 87 (34.9) 102 (40.8)
Positive/Negative 30 (12.0) 30 (12.0)
Negative/Positive 89 (35.7) 65 (26.0)
Unknown/Negative 1 (0.4) 1 (0.4)
Number of allele level HLA mismatches at HLA-A,-B,-C,-DRB1
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Young et al. Page 26
Characteristics Treatment Arm*
Bone MarrowN (%)
Peripheral Blood Stem CellsN (%)
0 189 (76.2) 202 (80.8)
1 52 (21.0) 46 (18.4)
>=2 7 (2.8) 2 (0.8)
Unknown 1 (0.4) 0 (0.0)
Conditioning regimen
Cyclophosphamide and Total Body Irradiation (Cy-TBI) 115 (46.2) 121 (48.4)
Busulfan and Cyclophosphamide (Bu-Cy) 80 (32.1) 65 (26.0)
Fludarabine and Melphalan (Flu-Mel) 16 (6.4) 24 (9.6)
Fludarabine, Busulfan, and ATG (Flu-Bu-ATG) 38 (15.3) 40 (16.0)
Graft versus host disease Prophylaxis
Cyclosporine and Methotrexate 59 (23.7) 47 (18.8)
Tacrolimus and Methotrexate 163 (65.5) 187 (74.8)
Other 27 (10.8) 16 (6.4)
Note:
*no significant p-values for baseline characteristics between the two treatment arms
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Young et al. Page 27
Table 2
Pathogen Frequency by Treatment Arm (only the top 5 organisms for each infection type are listed)
OrganismBone Marrow
N (%)Peripheral Blood Stem Cells
N (%)
Bacterial infections
Staphylococcus (coagulase negative) 123 (82) 101 (67)
Enterococcus (all species) 54 (42) 49 (40)
Clostridium difficile 69 (52) 54 (41)
Staphylococcus (coagulase positive) 10 (9) 30 (20)
Escherichia (also E. coli) 16 (15) 23 (19)
Viral infections
Cytomegalovirus (CMV) 78 (61) 81 (57)
Polyomavirus 27 (25) 27 (24)
Herpes Simplex (HSV1, HSV2) 16 (14) 22 (17)
Epstein-Barr Virus (EBV) 15 (12) 21 (15)
Influenza 22 (19) 13 (13)
Fungal/Parasitic infections
Other (suspected) Fungus 12 (11) 13 (12)
Yeast other than Candida albicans 5 (4) 12 (10)
Candida albicans 6 (6) 10 (8)
Aspergillus fumigatus 5 (5) 6 (5)
Mucormycosis (Zygomycetes, Rhizopus) 5 (4) 2 (2)
Pneumocystis 1 (1) 2 (2)
Toxoplasma 1 (1) 1 (1)
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Young et al. Page 28
Tab
le 3
Ove
rall
Sum
mar
y of
infe
ctio
n fr
eque
ncie
s
Ove
rall
Infe
ctio
ns *
Bon
e M
arro
wP
erip
hera
l Blo
od S
tem
Cel
ls
Day
0-E
NG
R§
EN
GR
-100
§10
1–18
018
1–36
536
6–73
0O
vera
llD
ay0-
EN
GR
§E
NG
R-1
00§
101–
180
181–
365
366–
730
Ove
rall
Tot
al I
nfec
tion
Eve
nts
179
283
102
7868
710
121
266
8281
8763
7
B
y se
veri
ty
Mod
erat
e12
417
658
4433
435
7417
950
5855
416
Seve
re43
8832
2924
216
3960
2215
2115
7
Lif
e th
reat
enin
g/fa
tal
1219
125
1159
827
108
1164
B
y ty
pe
Bac
teri
al in
fect
ion
130
164
5844
3543
198
147
4643
4537
9
Vir
al in
fect
ion
3711
035
2527
234
1310
429
2731
204
Fung
al in
fect
ion
127
88
540
815
610
1049
Para
sitic
infe
ctio
n0
10
01
20
00
11
2
Oth
er ty
pes
01
11
03
20
10
03
B
acte
rial
sub
grou
ps *
Blo
odst
ream
infe
ctio
n85
8728
136
219
5783
2315
1619
4
Non
bloo
dstr
eam
infe
ctio
n45
7730
3129
212
4164
2328
2918
5
Clo
stri
dium
dif
fici
le in
fect
ion
2329
87
269
2214
510
354
V
iral
sub
grou
ps *
CM
V in
fect
ions
1245
99
378
549
1412
181
Res
pira
tory
infe
ctio
ns12
1010
1115
582
55
613
31
Non
-CM
V n
on-r
espi
rato
ry15
5617
610
104
651
1010
1895
EB
V in
fect
ions
18
41
115
014
31
321
Var
icel
la0
55
15
160
01
23
6
F
unga
l sub
grou
ps *
Yea
st in
fect
ions
71
41
013
311
24
323
Mol
d in
fect
ions
24
35
115
11
44
313
Asp
ergi
llus
21
24
110
10
34
210
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Young et al. Page 29
Ove
rall
Infe
ctio
ns *
Bon
e M
arro
wP
erip
hera
l Blo
od S
tem
Cel
ls
Day
0-E
NG
R§
EN
GR
-100
§10
1–18
018
1–36
536
6–73
0O
vera
llD
ay0-
EN
GR
§E
NG
R-1
00§
101–
180
181–
365
366–
730
Ove
rall
Oth
er (
susp
ecte
d) f
ungu
s3
21
24
124
30
24
13
Not
e:
* Cat
egor
ies
are
not m
utua
lly e
xclu
sive
. e.g
. A C
MV
infe
ctio
n or
an
EB
V in
fect
ion
may
als
o fa
ll in
to th
e ca
tego
ry o
f re
spir
ator
y in
fect
ion,
and
vic
e ve
rsa.
Cat
egor
ies
are
liste
d ba
sed
on th
e st
udy
inte
rest
.
§ The
day
of
engr
aftm
ent (
EN
GR
) w
as c
onsi
dere
d fo
r ea
ch in
divi
dual
, for
cla
ssif
icat
ion
into
pre
- ve
rsus
pos
t-en
graf
tmen
t. M
edia
n en
graf
tmen
t was
20
days
for
Bon
e M
arro
w a
nd 1
5 da
ys f
or P
erip
hera
l B
lood
.
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Young et al. Page 30
Tab
le 4
Mul
tivar
iate
Ana
lysi
s M
odel
of
Infe
ctio
n D
ensi
ty
Var
iabl
eB
acte
rial
infe
ctio
nsV
iral
infe
ctio
nsF
unga
l inf
ecti
ons
Rel
ativ
e de
nsit
y (9
5%C
I)P
-val
ueR
elat
ive
inte
nsit
y (9
5%C
I)P
-val
ueR
elat
ive
inte
nsit
y (9
5%C
I)P
-val
ue
Gra
ft t
ype
Inte
ract
ed w
ith d
isea
se r
isk
<0.
001
B
one
Mar
row
1.00
1.00
Pe
riph
eral
Blo
od0.
88 (
0.71
–1.1
0)0.
262
1.38
(0.
84–2
.28)
0.20
7
Dis
ease
ris
k
Ear
ly1.
00
B
M1.
00
PB
SC0.
68 (
0.49
–0.9
3)0.
016
Adv
ance
d1.
39 (
1.10
–1.7
5)0.
006
B
M1.
00
PB
SC1.
68 (
1.1–
2.57
)0.
017
Rec
ipie
nt C
MV
sta
tus
N
egat
ive
1.00
1.00
1.00
Po
sitiv
e1.
24 (
1.00
–1.5
3)0.
046
1.49
(1.
15–1
.94)
0.00
31.
66 (
1.03
–2.6
8)0.
038
HL
A M
atch
Sta
tus
0.01
0<
0.00
1
8/
81.
001.
001.
00<
0.00
1
7/
81.
41 (
1.07
–1.8
6)0.
015
1.70
(1.
28–2
.26)
<0.
001
1.40
(0.
76–2
.59)
0.28
3
<
=6/
81.
90 (
1.00
–3.6
3)0.
050
0.76
(0.
47–1
.23)
0.26
57.
05 (
3.28
–15.
15)
<0.
001
Gen
der
M
ale
1.00
Fe
mal
e1.
30 (
1.05
–1.6
1)0.
014
Kar
nofs
ky P
erfo
rman
ce S
core
>
=90
1.00
<
902.
23 (
1.33
–3.7
4)0.
002
U
nkno
wn
1.50
(0.
61–3
.66)
0.37
7
Con
diti
onin
g re
gim
en
Cyc
loph
osph
amid
e an
d T
otal
Bod
y Ir
radi
atio
n (C
-TB
I)1.
00
Bus
ulfa
n an
d C
yclo
phos
pham
ide
(Bu-
Cy)
1.30
(0.
95–1
.77)
0.09
5
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Young et al. Page 31
Var
iabl
eB
acte
rial
infe
ctio
nsV
iral
infe
ctio
nsF
unga
l inf
ecti
ons
Rel
ativ
e de
nsit
y (9
5%C
I)P
-val
ueR
elat
ive
inte
nsit
y (9
5%C
I)P
-val
ueR
elat
ive
inte
nsit
y (9
5%C
I)P
-val
ue
Flud
arab
ine
and
Mel
phal
an (
Flu-
Mel
)1.
76 (
1.16
–2.6
8)0.
008
Flud
arab
ine,
Bus
ulfa
n, a
nd A
TG
(Fl
u-B
u-A
TG
)1.
77 (
1.31
–2.3
9)<
0.00
1
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Young et al. Page 32
Tab
le 5
Mul
tivar
iate
Mod
el o
f In
fect
ion
Den
sity
: Im
pact
of
Gra
ft V
ersu
s H
ost D
isea
se
Var
iabl
eB
acte
rial
infe
ctio
nV
iral
infe
ctio
nF
unga
l inf
ecti
on
Rel
ativ
e in
tens
ity
(95%
CI)
P-v
alue
Rel
ativ
e in
tens
ity
(95%
CI)
P-v
alue
Rel
ativ
e in
tens
ity
(95%
CI)
P-v
alue
Non
e1.
001.
001.
00
Acu
te G
VH
D o
nly
2.24
(1.
71–2
.92)
<0.
001
1.68
(1.
30–2
.17)
<0.
001
3.30
(1.
56–7
.01)
<0.
001
Chr
onic
GV
HD
onl
y2.
39 (
1.47
–3.8
8)<
0.00
11.
16 (
0.69
–1.9
6)0.
571
7.47
(2.
81–1
9.91
)<
0.00
1
Bot
h4.
16 (
2.60
–6.6
4)<
0.00
11.
40 (
0.85
–2.3
2)0.
183
5.52
(1.
90–1
6.07
)<
0.00
1
Not
e: o
ther
cov
aria
tes
in th
e m
odel
incl
uded
thos
e lis
ted
in T
able
4.
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Young et al. Page 33
Table 6
Multivariate Analysis of Overall Survival with Infection as time-dependent covariate
Variable Level Hazard Ratio (95%CI) P-value
Graft type
Bone Marrow 1.00
Peripheral Blood Stem Cells 1.09 (0.85–1.40) 0.487
Age <0.001
0–20 1.00
21–30 2.06 (1.12–3.79) 0.021
31–40 1.82 (0.97–3.40) 0.060
41–50 2.22 (1.22–4.05) 0.009
51–60 3.30 (1.85–5.90) <0.001
>=60 (combine with 51–60?) 3.92 (2.04–7.52) <0.001
Disease risk
Low 1.00
High 1.45 (1.12–1.89) 0.005
HLA Match Status <0.001
8/8 1.00
7/8 1.72 (1.29–2.30) <0.001
<=6/8 3.77 (1.68–8.44) 0.001
Conditioning regimen 0.081
Cyclophosphamide and Total Body Irradiation (Cy-TBI) 1.00
Busulfan and Cyclophosphamide (Bu-Cy) 0.67 (0.49–0.92) 0.012
Fludarabine and Melphalan (Flu-Mel) 0.74 (0.45–1.21) 0.230
Fludarabine, Busulfan, and ATG (Flu-Bu-ATG) 0.88 (0.59–1.29) 0.503
Any bacterial infection after transplant (time-dependent covariate)
No 1.00
Yes 1.49 (1.14–1.96) 0.004
Any viral infection after transplant (time-dependent covariate)
No 1.00
Yes 1.15 (0.88–1.50) 0.317
Any fungal infection after transplant (time-dependent covariate)
No 1.00
Yes 2.40 (1.71–3.35) <0.001
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2017 February 01.