Embed Size (px)
Citation preview

1257
tubules never exceeded the normal length for an age ofsix months.The very short proximal convoluted tubules of cystinosis
and nephrogenic diabetes insipidus may be unable toreabsorb enough water to prevent the distal convolutedtubule from becoming overburdened with hypotonicfiltrate, particularly if the intact ascending limb of Henlepreferentially excretes sodium. This would account forcertain characteristics of the two diseases, notably theapparent inactivity of antidiuretic hormone.
This work was supported by research grants no. HE-05254 andHE-08208-01 from the National Institutes of Health, United StatesPublic Health Service.We are also grateful to those who sent us kidneys as mentioned in
tables 11 and III, but particularly to Dr. A. Rich, Dr. B. Childs ofJohns Hopkins Hospital, Baltimore; Dr. M. A. Holliday and Dr. G.Fetterman, of Children’s Hospital of Pittsburgh; Dr. B. E. Schlesinger,Dr. R. C. B. Pugh, and Dr. W. W. Payne, formerly of the Hospitalfor Sick Children, Great Ormond Street, London; and to Prof. C. E.Dent of University College Hospital, London, for encouraging othersto send us material.
REFERENCES
Bialestock, D., quoted by MacDonald, W. B. (1955) Pædiatrics, 15, 298.Biber, Th. U. L., Mytle, M., Gottschalk, C. W. (1963) Excerpta Medica
International Congress series no. 78. Proceedings of the 2nd Inter-national Congress of Nephrology, Prague. Amsterdam.
Bruck, E., Rapoport, M., Rubin, I. M. (1954) J. clin. Invest. 33, 699.Clay, R. D., Darmady, E. M., Hawkins, M. (1953) J. Path. Bact. 65, 551.Darmady, E. M., Stranack, F. (1954) quoted by Kirkman et al. (1956).- - (1957) Brit. med. Bull. 13, 21.
Dicker, S. E., Eggleton, M. G. (1960) J. Physiol. 154, 378.de Wardener, H. (1962) in Renal Disease (edited by D. A. K. Black).
Oxford.Fetterman, G., Holliday, M. A. (1962) Personal communication.Gottschalk, C. W. (1964) Personal communication.Kirkman, B. H., Black, J. A., Wilkinson, R. H., Evans, P. R. (1956) Arch.
Dis. Childh. 31, 59.Metcoff, J., Nakasone, N., Rance, C. P. (1954) J. clin. Invest. 33, 665.Osathanondh, V., Potter, E. L. (1963) Arch. Path. 76, 271.Schedl, H. P., Bartter, F. C. (1958) J. clin. Invest. 37, 928.Stanbury, S. W. (1958) Advanc. intern. Med. 3, 231.Williams, R. H., Henry, C. (1947) Ann. intern. Med. 27, 84.
INFECTION WITH
STRONGYLOIDES STERCORALIS IN JAMAICAG. BRAS
M.D. Batavia, F.C.Path.PROFESSOR OF PATHOLOGY
R. A. IRVINEM.B. Leeds, M.R.C.P.LECTURER IN MEDICINE
R. C. RICHARDSM.B. Durh., M.R.C.P.LECTURER IN MEDICINE
P. F. A. MILNERM.B. N.U.I., D.C.P.
LECTURER IN HÆMATOLOGY
M. M. S. RAGBEERM.B. Lond.
REGISTRAR IN PATHOLOGY
UNIVERSITY OF THE WEST INDIES, KINGSTON, JAMAICA
Strongyloides stercoralis is a helminthic parasite enteringthe body by the skin and passing through the lung on itsway to the duodenal/jejunal region, where the femalesrapidly mature. While symptoms may occur in the skin(pruritus) or in the lung (small haemorrhages, pneumonicareas, cough), the common complaints are understandablylinked with the gastrointestinal tract (diarrhoea).Many people, however, suffer very little from the
infection (de Langen and Lichtenstein 1936). Lie KianJoe (1940) found an incidence of 13-1 % among Indonesiansand 4-8% among Chinese who were attending a municipalhospital in Indonesia for some other complaint and had nospecific symptoms.
<
Paralytic ileus as the result of massive invasion of thebowel wall is considered uncommon (Nolasco and Africa1936, Pinheiro et al. 1959). Recently Wilson and Thomp-son (1964) described this complication in a West Indianfemale immigrant in London. Also uncommon is hyper-infestation due to autoinfection-i.e., invasion of thebowel wall by large numbers of larva: which normally
should be evacuated with the stools (see Faust 1957).Galliard (1949, 1951) maintained that such hyper-infestation resulted not from different biological charac-teristics of the parasite but from an unusual susceptibilityof the patient due to severe undernutrition or other
debilitating states.The incidence of infestation with Strongyloides stercoralis
is not known in Jamaica. A pilot survey in. a small hillcommunity showed a 1% prevalence in 900 stoolsexamined (Chen 1964).
In this paper the clinical and pathological findings in6 fatal cases and 4 other cases of severe infestation arereviewed.
Case-reportsThe patients were all observed in the University College
Hospital which serves a combined urban and rural popula-tion of low social economic status. In Jamaica severemalnutrition is rare in adults, although it occurs in chil-dren under two years of age. Severe infestation withintestinal worms is again rare, presumably because the soilis relatively dry and, except in some areas in the hills,unsuitable for the development of larvx or ova.The clinical findings are summarised in the table. All
patients were severely undernourished and all but onehad malabsorption syndrome. 3 case-histories have beenselected as representative of the series.
Case 5 .
A 14-year-old schoolboy developed nausea and copiousvomiting three weeks before admission. The vomiting was notrelated to meals. About a week later he began to have diarrhoea(6-8 watery, brownish stools daily with neither mucus norblood) and colicky periumbilical and general muscle pain. His
legs became gradually swollen. He had had a rash since earlychildhood. He had had one meal a day, usually with animalprotein in some form once or twice a week; but occasionally hehad had no meat for as long as a month at a time. He was
intelligent, alert, thin, tall, and almost bald, with oedema offace and legs but no jaundice or clubbing. His weight was82 lb. (39 kg.) and his height 5 ft. 11/2 in. (155 cm.). There wasextensive scabies with numerous small discrete lymph-nodes inall areas, roughly 1-1-5 cm. in diameter. His abdomen was
grossly distended and he had ascites. The liver was enlargedto 4 cm. below the costal margin; the edge was soft and smooth.The spleen was not felt. Rectal examination was normal. Therewere scattered rhonchi and coarse crepitations in the lowerlobes of both lungs. The cardiovascular system was normal.
Haemoglobin 9-0 g. per 100 ml.; packed-cell volume 30%;mean corpuscular haemoglobin concentration (M.C.H.C.) 30;white-cell count 12,000 per c.mm. (neuthrophils 92%lymphocytes 6%, monocytes 2%; serum-albumin 1-2 g.and blood-urea 17 mg. per 100 ml.).Hookworm ova and strongyloides larvae in stools, and
strongyloides larvae in the duodenal aspirate and sputum. Hewas treated with dithiazine iodide (’ Telmid ’), 100 mg. threetimes daily for seven days, repeated a fortnight later. In
addition, ’ Alcopar’ was given on three successive occasions.He responded well to a high-protein diet, and at the end of eightweeks his hxmoglobin was 12-6 g. and his serum-albumin3-5 g. per 100 ml. On discharge his stools were free from wormsand his weight had increased to 94 lb. (45 kg.).He was readmitted six months later, having relapsed again,
presenting with duodenal ileus. He remains desperately ill.
Case 6
Another 14-year-old schoolboy gave a two-month historyof intermittent right-sided chest pain, never severe, aggravatedby breathing. About the same time he began to notice pro-gressive swelling of his feet and legs and distension of hisabdomen. Appetite was poor for some weeks. He had 3-4bowel actions a day, consisting of loose, brownish stools. His
protein intake was less than 100 g. per week. He was a puffy,

1258
SUMMARY OF CLINICAL MANIFESTATIONS
pale boy, with swelling of the abdomen and feet and thinbrownish hair. He was tender in the right iliac fossa and overthe liver which was enlarged 4-5 cm. below the right costalmargin. There was no splenomegaly. There were crepitationsat both lung bases. The cardiovascular system was normal.Haemoglobin 10-1 g. per 100 ml.; white-cell count 10,300 perc.mm. (band forms 70%, neutrophils 9%, lymphocytes 3%,monocytes 8%, eosinophils 1%, metamyelocytes 9%). Hisurine contained no albumin or sugar and culture was negative.Blood-sugar, 108 mg. per 100 ml.; serum Na+ 144, K+ 3-6,Cl- 9-7 mEq. per litre; C02 15 c.cm. per litre. Albumin 2-4 g.globulin 4-1 g. per 100 ml.Hookworm and strongyloides larvx in stools. Twelve hours
after admission he developed symptoms of acute appendicitiswith early peritonitis. This was confirmed at laparotomy. Hewas treated with dithiazine iodide and alcopar and a high-protein intake. His general condition improved: serum-
albumin 3 g. per 100 ml. and weight 78 lb. (37-5 kg.) ondischarge.He was seen two years later with a three-month history of
recurrence of symptoms with copious vomiting for two weeks.He was cachectic. There was generalised lymphadenopathy,epigastric distension, and hepatotomegaly. Haemoglobin 7-7 g.per 100 ml., packed-cell volume 27%; white-cell count 8100per c.mm. (neutrophils 92%, lymphocytes 7%, monocytes 1 %).Serum Na 137, K- 3-2, Cl- 96 mEq. per litre. C02 18 c.cm.
per litre. Blood-urea 39 mg. per 100 ml. A flat X-ray ofabdomen showed dilation of the stomach and duodenum.Strongyloides larva in the stomach aspirate. In spite ofintravenous fluids and blood-transfusions the patient’s condi-tion deteriorated and he died in hypovolsmic shock fifty-sevenhours after admission.
Case 7
A cultivator, aged 58, gave a six-week history of vague upperabdominal pain. A week later he began to vomit about 1/2-1 1pint altered food ten to thirty minutes after meals three or fourtimes a day. The vomitus contained bile on one occasion butwas never blood-stained. He lost about 40 lb. in six weeks. Hebecame constipated with hard brown stools at infrequentintervals. His protein intake was low. On examination he wasemaciated and thin; weight 92 lb. (44 kg.) and height 5 ft. 8 in.(172 cm.). The tongue was furred and dry and the mucosa’were pale, but no abnormality was found in any system. Adiagnosis of cachexia, possibly the result of malignant disease ofthe stomach or pancreas was made. Haemoglobin 11-7 g. per100 ml.; packed-cell volume 39%; M.C.H.C. 30; leucocytes
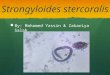
Fig. 1-Duodenal biopsy in case 10. Adult strongyloides worms (A),ova (0), and rhabditiform larva: (L). The villi are blunted andthere is a dense inflammatory infiltrate. (Hxmatoxylin and eosin:< 220, reduced by a third.)
Fig. 2-Duodenal biopsy in case 10. Ova excavating the epitheliallining of a crypt. (Haematoxylin and eosin: >e550, reduced by athird.)

1259
Fig. 3-Duodenal biopsy in case 10. An adult female strongyloideshas " wormed itself " into 2 adjacent crypts. Note ova (0) inpregnant uterus and blunted villus (V). (Hasmatoxylin and eosin:x 550, reduced by a third.)
7400 per c.mm. (neutrophils 91%, lymphocytes 6%, mono-cytes 2%, eosinophils 1%); blood-sugar 185 mg. per 100 ml.Total proteins 5-9 g., albumin 3 g., globulin 2-9 g. per 100 ml.No occult blood in stools on three occasions. A flat X-ray ofabdomen showed distension of the upper gastrointestinal tract.A barium meal showed the very irregular mucosal foldings inthe antrum and at the pylorus, but no evidence of stenosis.
He was treated with parenteral fluids, but continued to lookill. Five days after admission his haemoglobin had fallen to8-9 g. per 100 ml. and the white-cell count was 16,300. He wasgiven 2 pints of whole blood and again his condition improved.When he began to develop crepitations at the lung bases,crystalline penicillin, 1 million units six-hourly, was given. Hisweight increased to 98 lb. (47 kg.) at the end of one week.However, his haemoglobin subsequently fell to 6-6 g. per100 ml. with a packed-cell volume of 23% and a M.C.H.C. of 25.Large volumes of fluid were aspirated from his stomach dailyand he continued to deteriorate. He then developed acuterespiratory obstruction from inhaled gastric contents and died.Necropsy revealed strongyloides superinfestation.Duodenal Biopsies
Peroral duodenal and jejunal biopsies were performed in3 cases with a Crosby biopsy capsule (Crosby and Kugler1957). The mucosa showed severe inflammatory changesand blunting of villi (fig. 1). Adult worms were seen toenter the crypts where females apparently deposit ova(figs. 1, 3). Ova had excavated the mucosa and were eithercovered by mucus or buried inside the epithelium (figs.2, 4). Newly hatched rhabditiform larvae were seen in asimilar excavated position (fig. 4). After treatment theinflammation disappeared and the villi reformed normally.Post-mortem Findings
All patients showed severe malnutrition with someoedema and a varying amount of fluid in abdominal andpleural cavities. Fatty change in the liver was also common.The following findings refer mainly to the gastrointestinaltracts:
Case l.-Superficial ulcers (1-2 per sq. cm.), up to 5 mm.in diameter, in the entire colon. Strongyloides stercoralis wormsin the duodenal/jejunal region. Histologically strongyloideslarvae in all levels of the bowel wall and in the lungs.
Case 2.-Hypereemic gastric and duodenal mucosa. Patchy,granular, hyperxmic jejunum and upper ileum. Diffuselyreddened lower ileum and colon with tiny superficial ulcers,approximately 1-2 per sq. cm. Inflamed mesenteric lymph-nodes up to 2 cm. in diameter. Strongyloides in vast numbersin the duodenal/jejunal region: no other worms. Histologically
Fig. 4-Duodenal biopsy in case 10. Ova (a) and hatching larva (b)in the epithelial layer of a crypt. (Haernatoxylin and eosin: x 550.)
Fig. 5-Larva (L) in myocardium in case 2. (Hsematoxylm andeosin: x770.)

1260
Fig. 6-Larva in sinusoid of liver in case 3.(Haematoxytin and eosin: / 770, reducedby a third.)
AW
,
Fig. 7-Group of larvae (L) in alveolus oflung in case 2. (Haematoxylin and eosin:x 770, reduced by a third.)
strongyloides larva= in all levels of the bowel wall, the lungs,heart, liver, and kidney.
Case 3.-Fibrous stricture in the jejunum approximately 1metre from the duodeno/jejunal flexure. The colon, especiallythe csecum, hasmorrhagic and obviously inflamed but notdefinitely ulcerated. Strongyloides in the duodenal/jejunalregion. Histologically many larva: in the glands of the pylorusand jejunum, in lymphatics of the pylorus, in the colonicmucosa and submucosa, and in the kidneys, liver, and lungs.
Case 4.-Atrophic gastritis and atrophy of the small bowel.Thickened caecum and rectum. Enlarged mesenteric lymph-nodes. No other worms besides strongyloides in the duodenal/jejunal region. Histologically strongyloides larvae in all levelsof the bowel wall, in the lungs, and in the liver.
Case 6.-Distended small intestines. Hundreds of strongy-loides adults and larvae, 27 Necator americanus, and 1 Trichuristrichiuria, in the duodenal/jejunal region. Histologicallystrongyloides larvas in the muscle layer of the gallbladder, in thewall of the jejunum, and in the lungs. Granulomata in someareas.
Case 7.-Congested and dilated intestines. (There may havebeen a terminal volvulus of most of the ileum as this wasdiscoloured.) Colon and rectum normal. Evidence of aspira-tion of gastric contents in the lungs. Strongyloides worms inthe duodenal/jejunal region. Histologically strongyloides in alllevels of the bowel wall and in the lungs.
Fig. 8-Adult female strongyloides from case 6. Note ova inside worm(0) and 3 ova embedded in adjacent piece of duodenal mucosa.
Discussion
Strongyloides stercoralis infesta-tion should be borne in mind with
any undernourished patient whocomplains of abdominal symptoms,particularly intractable diarrhoea.Van Lavieren (1959) and Sibthorpe(1961) quote cases of ex-Service-men who had remained undiag-nosed after a multitude of medicalexaminations by several doctors.Of our ten patients, nine were
cachectic because of under-nutri-tion or chronic diarrhoea or both.Normand (1876) first recognisedsteatorrhoea as a result of strongy-loides infection. De Paola (1961,1962) ascribed to these worms
changes in the villi of the duodenal/jejunal region, and Alcorn andKotcher (1961) reported two fatalcases of malabsorption.
In some of our patients hundredsof adult worms and their larvae
...... -.,
were seen; and duodenal biopsiesdemonstrated the mucosal invasion by parasites and ovaand the resulting inflammation and blunting of the villi.This is in keeping with the malabsorption syndromeobserved clinically (table). Normal villi reappeared aftertreatment.
The invasion of the bowel wall by strongyloides in largenumbers presumably caused the paralytic ileus observedin 5 cases (table). There was remarkably little tissuereaction to the larvae in the deeper layers of the bowel, butoccasional granulomata had developed. Larvae in the
heart, lungs, liver, and kidney also produced few
histological changes.Ulceration of the colon (cases 1 and 2) seems to be rare
but has been reported from Brazil by De Paola (1961,1962).The prevalence of strongyloides infestation in the general
population of Jamaica seems to be low: a thorough searchfor strongyloides in the duodenal/jejunal region in 50 con-secutive necropsies proved negative. It appears extra-
ordinary that, nevertheless, we should have seen so manysevere and even fatal cases, and new incidence studies are
obviously overdue.In the clinical management of these cases the differential
diagnosis from hookworm larvx is important. Interestingwas the absence of significant eosinophilia in six patients,and the relatively short history in some.We are grateful to Prof. J. J. C. Buckley, of the London School
of Hygiene and Tropical Medicine, for his advice on the morphologyof the parasite.
REFERENCES
Alcorn, M. O., Jr., Kotcher, E. (1961) Sth. med. J. 54, 193.Chen, W. (1964) Personal communication.Crosby, W. H., Kugler, H. W. (1957) Amer.J. dig. Dis. 2, 236.de Langen, C. D., Lichtenstein, A. (1936) Clinical Textbook of Tropical
Medicine. Batavia and Amsterdam.de Paola, D. (1961) Trop. Dis. Bull. 1962, 59, 281.
— (1962) ibid. 1963, 60, 348.Faust, E. C., Russel, P. F. (1957) Clinical Parasitology, London.Galliard, H. (1949) C.R. Soc. Biol. 68, 686.
— (1951) Ann. Parasit. 26, 67, 201.Lie, Kian Joe (1940) Geneesk, Tijdschr. Ned. Ind. 80, 2020.Nolasco, J. O., Africa, C. M. (1936) J. Phil. Is. med. Ass. 16, 275.Normand, A. (1876) quoted by De Paola (1961).Pinheiro, G. C., Pinheiro, R. M. V. D. R. C., Filho, P. D. (1959) Med.
Cirurg. Farm. 280, 311.Sibthorpe, G. (1961) Med. J. Aust. 2, 599.Van Lavieren, G. H. (1959) Ned. milit.-Geneesk. Arch. 12, 230.Wilson, S., Thompson, A. E. (1964) J. Path. Bact. 87, 169.










![Prevalence and risk factors of Strongyloides stercoralis ...Strongyloides stercoralis, a soil-transmitted nematode, is ar-guably the most neglected tropical disease [1], yet an esti-mated](https://img.pdfslide.us/doc/110x75/603910f33d86085b0845e0dd/prevalence-and-risk-factors-of-strongyloides-stercoralis-strongyloides-stercoralis.jpg)