Embed Size (px)
Citation preview

AEP Course 06/10/2016
1
Infection Control in
Optometric Practice
William D. Townsend, O.D., FAAO
Advanced Eye Care - Canyon, TX
Adjunct Professor, UHCO - Houston, TX
Why Infection Control in Optometry?
Changes in national standards
Changes in legal climate
Changes in disease entitiesHIV
Hepatitis C
Tuberculosis
MRSA
Changes in OptometryCL ushered in a new era
Procedures, instruments, sharps
Body fluids; tears, blood
Hospital privileges
Guide to Infection Prevention for
Outpatient Settings: Minimum
Expectations for Safe Care
“All healthcare settings, regardless of the
level of
care provided, must make infection
prevention a priority and must be equipped
to observe Standard Precautions. The 2007
CDC and HICPAC Guideline for Isolation
Precautions was a first attempt to provide
recommendations that can be applied in all

AEP Course 06/10/2016
2
Realistic Goals for Infection
Control: How Far Do We Go?
Optometrists practice in a non-sterile environment, not an
operating room!1. Protect the patient from clinic-acquired
infection
2. Protect the staff and doctors from infectious agents
3. Meet infection control standards established by government and healthcare industry
4. Avoid unnecessary cost, effort
Know Your Enemies-
MicroorganismsFree living, capable of respiration, reproductionBacteria
No cell nucleus
No cell organelles
Cell wall
Genetic info- single DNA strand
FungiTrue cell nucleus
True cell organelles
Cell wall
Non-motile
Protozoa (Acanthamoeba)True cell nucleus
True cell organelles
Cell membrane
Bacteria
Shape-important for
classification
Cocci- round, so less affected
by drying
Diplo- pairs
Strepto- chains
Staphylo- clusters
Bacillus- rods
Spiral- improved motility
Helix- elongated spirals

AEP Course 06/10/2016
3
nucleoid
cytoplasm
flagella
pili
ribosomes
cell wall
capsule
cytoplasmic
membrane
Bacterial StructureCapsule- coating for protection
Cell wall- structural Absent in animal cells
Targeted by some antibioticsGives staining characteristics
CytoplasmChromatin material (nucleoid)
Ribosomes for protein synthesis
Lipids for energy
Flagella- motility
Microbial Survival Tactics:
Endospores, Cysts, EnzymesConversion from vegetative to encapsulated forms
Bacteria- spores
Amoeba- cysts
Fungi- alter form depending on environment
Encapsulated forms MUCH more difficult to kill
Boiling- NO, Alcohol- NO
�The ability to kill spores is the “gold standard” in infection control!
Endospore Formation
Clostridial Species
Clostridium botulinum- botulism
Clostridium tetani –tetanus
Clostridium perfringens- gangrene
Bacillus Species
Bacillus anthrasis- anthrax
Bacillus cereus- diarrheal syndrome
Viruses
Are they living?
Incapable of respiration, reproduction
Rely on host cell to replicate
Genetic elements- not cells
Structure
Core of genetic material; DNA or RNA
Covering of protein
Viability outside host cell varies with species
Basically, not really a living organism!

AEP Course 06/10/2016
4
Size of Protozoa, Bacteria,
VirusesViral Replication
Viruses incapable of independent
reproduction
Virus attaches to host cell
Virus injects genetic material into host cell
Host cell replicates thousands of viral
particles
Viruses released into environment
Infect adjacent cells
The infection spreads exponentially
Viral Infection & Replication Important Viruses In Eye Care
Herpes simplex- cold sore, keratitis, uveitis, retina
Herpes zoster- shingles, HZ ophthalmicus
Adenoviruses Epidemic keratoconjunctivitis- EKC
Pharyngoconjunctival fever- PCF
Pox viruses- molluscum contagiosum
Transmission: “asymptomatic viral shedding.”

AEP Course 06/10/2016
5
Important Viruses In Eye Care
Hepatitis B
Hepatitis C
Papova viruses- lid warts
Enterovirus- hemorrhagic conjunctivitis
Human immunodeficiency virus- HIV & AIDS
Increased risk for :
Fungal infection
Bacterial infection
Fungal infection
Cytomegalovirus (CMV) retinitis
Protozoa (Example:
Acanthamoeba)
Vegetative (normal) form
Capable of forming cysts
Increased resistance to hostile conditions
Cause severe corneal infection that are
highly resistant to treatment
Present in distilled, tap water in virtually
all communities
Present in soil, hot tubs, HVAC units
Federal Register, June 2002
“EPA's preliminary determination is that
no regulatory action is appropriate for
the contaminants Acanthamoeba,
aldrin, dieldrin, hexachlorobutadiene,
manganese, metribuzin, naphthalene,
sodium, and sulfate.”Suddenly it is OK to have amoebae in our water
supply!
Confused about terminology?

AEP Course 06/10/2016
6
Antiseptics
“..a substance that inhibits
the growth and
development of
microorganisms without
necessarily killing them.”
For use on skin, tissue
Not for inanimate objects
Disinfectant
“substances that are
applied to non-living
objects to destroy
microorganisms”
Used to destroy
microorganisms on
surfaces, i.e.
countertops, face
shields
Disinfection Versus
Sterilization
The “golden standard” in infection
control
Spores more difficult to kill than
vegetative forms.
Spore destruction is the pivotal criteria in
IC
“Can any given method kill spores?”
If no, disinfection
If yes, sterilization
Infection Control Terminology
Sterilization- all life forms killed
Spores
Cysts
Vegetative forms
Viruses
Fungi
Politicians
Disinfection- all life forms killed except
spores & cysts

AEP Course 06/10/2016
7
Infection Control Terminology
…cidal
Indicates death of specific life form
Virucidal- kills viruses
Sporicidal- kills spores
Tuberculocidal- kills bacteria that cause
tuberculosis
Fungicidal- kills fungi
Spaulding Classification
Based on type of tissue object will enter.
Critical- enters sterile tissue or vascular
tissue
Example
Spud, burr, spatula, scalpel, scissors
Spaulding Classification
Semicritical- touches mucous
membranes
Example: forceps, lacrimal dilators, lacrimal
cannulas, tonometer probes
Noncritical- touches skin
Example: cilia forceps, stethoscopes,
occluders, face shields, head rests
Infection Control: Basic Procedures
Hand washing- #1 form of infection
control
Gloving
Solution/drug sterility
Surface disinfection
Tonometer disinfection
Sharps disposal
Basic Procedures are Important Procedures!

AEP Course 06/10/2016
8
Hand Washing in Health Care Workers:
The cornerstone of infection control
English
Spanish
French
Hand Washing in Health Care
Workers:
The cornerstone of infection controlDuration of hand scrubbing by HCW
1989- 24 seconds � 1997- 5 seconds
Negative factors
Dr. vs. nurse
Male vs. female
Working during week vs. weekend shift
Lack of role model, encouragement
Hold each other accountable!
Hand Washing
#1 means of preventing nosocomial
infection
Use a liquid disinfectant soap
Never use bar soaps
Rinse well
Shake off hands w/ fingers pointing
down
NO cloth towels, only paper towels
Turn off water w/ paper towel & dispose
Hands must be dry prior to patient
Hand Washing
Sing “Happy Birthday” (to yourself)
approximately 15 seconds

AEP Course 06/10/2016
9
Pathogen Survival on
SurfacesViruses
Adenoviruses: 3-8 weeks at room temperature
Hepatitis A: 4 hours
Hepatitis B: 7 days
Herpes simplex: 8 weeks
HIV: 4-5 days (numbers very reduced in hours)
Influenza virus: 2-4 days
Bacteria
Pseudomonas aeruginosa: 7 hours
Methicillin-resistant Staph aureus (MRSA): 2 days
Surface Disinfection
When?
After every patient
Always after red eyes
At the end of every day
Which agent?
Alcohol pads for face shields
Let the patient see you do it!
Use cotton balls and bottled alcohol-Save
$$!
Disinfectant spray for counters
Isopropyl alcohol (60%) all surfaces
Hypochlorite (1/1000 concentration)
995 ml distilled water, 5 ml bleach
Frugality in Infection ControlGloving
Non-sterile gloves in red eyes
Sterile gloves in invasive procedures
Keep gloves in all treatment areas
Proper sizing important, so make
various sizes available if needed
Wash hands after de-gloving
Glove while cleaning

AEP Course 06/10/2016
10
Solution/Drug SterilityOnce opened, it isn’t sterile
Never touch dropper to eye
Do “expiration date” inspections
Small bottles of CL solution in exam rooms
Date CL solutions when put in each room
Replace all CL solution bottles each month
Tonometer Probe Disinfection
After every patient
Alcohol swabs- degrades plastic tonometer
probe
Hydrogen peroxide (3%) 10 minutes- wipe
off
Sodium hypochlorite 500 ppm (0.0005%)
Within 10 minutes of application, destroys
herpes simplex virus, adenovirus 8, and
enterovirus 70
Soaking units for disinfection
Tonometer Probe
Disinfection
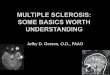
Disinfection of Tonometer Tips
Contaminated With Adenovirus 8Wiped With
dry wipe
wipe w/ water
wipe w/ isopropyl
alcohol
wipe w/ hydrogen
peroxide
wipe w/ povidone-iodine
Soaked 5 Minutes In
water
isopropyl alcohol
hydrogen peroxide
povidone-iodine
Threlkeld AB.et al Efficacy of a disinfectant wipe method for the removal of
adenovirus 8 from tonometer tips. Ophthalmology. Dec 1993
ResultsDry wiped tips positive for active virus
Tips soaked in water positive for active virus
No viable virus recovered from tips wiped w/ water or any of the
disinfectants

AEP Course 06/10/2016
11
TonopenCompares favorably with Goldmann
Disposable tip covers- great for infection control
Does not reqire patient be seated at slit lamp
Technique easily mastered by techs
More costly than Goldmann
Breaks when you (your tech) drops them
Disposable, protects from contamination, small
STDs
Sharps Disposal
Biohazard disposal companies easy to
find; just ask your dentist or PCP
Never recap needles
Micropuncture needles
Cannulas
Scalpels
Spuds
CPR Microshield:
Are you & your staff CPR certified?
Considerations in Infection Control:
Instrument Maintenance
Disinfection or Sterilization?
Which would you want for your eye?
Heat or Chemical?
Long-term effects of chemical disinfection-sterilization on stainless steel
Corrosion
Dulling
Storage of instruments after disinfection or sterilization?

AEP Course 06/10/2016
12
Non-disposable Instruments
Disinfection / Sterilization
Use disposable whenever possible
Soaking & cleaning of instruments
Disinfection / sterilization
Storage
Monitoring stored instruments
Who is responsible for maintaining the
system?
Soaking & Cleaning Instruments
Reduces bacteria on instrument surfaces
Loosens, removes protein, blood
Presoak 3% H2O
2for minimum 10 minutes
Ultrasound vs. scrubbing
Scrub w/ heavy gloves
Rinse w/ saline
Chemical Disinfection/Sterilization
Systems
Relatively inexpensive
Ideal for plastics, rubber
Chemicals must be rinsed off instruments
after cycle is complete- with what?
Storage after disinfection or sterilization?
Chemical Systems
Alcohols- do not sterilize
Chlorines- do not sterilize
Phenols- do not sterilize
Quaternary alcohols- do not sterilize
Hydrogen peroxide- sterilizes in very
high concentration
Glutaraldehyde- sterilizes @ high
concentrations, temperature dependent
Stinks!

AEP Course 06/10/2016
13
Gluteraldehyde
Activated by alkalinizing agent
Alters bacterial, viral RNA & DNA
Unpleasant odor @ 2%
Sterilant- 2% @ 37o for 6 hrs.
Disinfectant- 2% @ 37o for 2 hrs.
Examples
Cidex Plus 28-day Solution (Johnson & Johnson)
Metricide 28 (Metrex Research Corp.)
MaxiCide (Henry Schein Inc.)
Replace every month
Chemical Disinfection/ Sterilization
Gluteraldehyde systems
Phenols
The original disinfecting agent
Disrupt cell wall and precipitate proteins
Some viruses, spores unaffected by
phenols
Commonly combined with
glutaraldehyde
Quaternary Ammonium /Alcohol Compounds
Safest, fastest products on the
market today
Higher concentration of alcohol =
faster kill time
Available delivery forms
Traditional ready-to-use liquid
Convenient pre-saturated towelettes
Disinfect but DO NOT STERILIZE

AEP Course 06/10/2016
14
Chemical Disinfection/Sterilization
OK for many applications in
Optometry, but………….
Issues to consider
How do you store after disinfection or
disinfection?
How often do you re-treat instruments?
Heat Sterilization
Kills by coagulating enzymes and
proteins
Dry heat
Becoming the standard with many dentists
Old systems were slow
New heat sterilizers very fast
Autoclaving
Heat/Chemical combination
Dry Heat
Conventional
Heat instruments at 320° for 60 -120 minutes
Inefficient
Inexpensive
Rapid heat transfer
Very popular in dentistry
Expensive but very efficient
Source- contact a dental supply for prices
and information
Dry Heat
Disinfection
& Sterilization

AEP Course 06/10/2016
15
Autoclaving
Saturated steam under pressure
Boiling water does not kill spores
270° F for 4 minutes at 150 psi
Total cycle time @ 35 minutes
Storage
Instruments wrapped prior to sterilization
Instruments dated, stored in “see-through”
packages
Expense moderate to high
Newer office units smaller, less expensive
Autoclaves: Cost $600 to $3000
Refurbished autoclaves
available from dental
suppliers
Two Reasons Why It's So Hard To
Solve An Arkansas Murder:
1. All the DNA is the same.
2. There are no dental records.
Heat/Chemical (Chemiclave)
Unsaturated chemical vapor under low
pressure, high heat
270° at 20-40 psi for 20-40 minutes
Chemicals (Vaposterile) include water,
ethyl alcohol, and formaldehyde
Moderate cost
Instruments can be pre-packaged
Disadvantages; unpleasant odor and
incompatible with some plastics

AEP Course 06/10/2016
16
Chemiclaves
Unsaturated chemical
vapor method is a low-
humidity process
No time-consuming drying
phase is needed
Use a solution containing
alcohol, tend to be much
less corrosive to
instruments.
Not-so-pleasant odor
Used, refurbished
chemiclaves available
from dental suppliers
Instrument Storage
69
Diagnostic Contact
Lens DisinfectionLargely a non-issue due to disposables
Non-disposables require disinfection
Appropriate method depends on water
content
Diagnostic Contact
Lens Disinfection
Cleaning diagnostic lenses
Proper cleaning reduces bacterial load on
lenses by 99.99%
Best accomplished by manual cleaning with
bactericidal cleaner (Miraflow)
Leach et al found that after cleaning with
Miraflow, no bacteria were present on
lenses

AEP Course 06/10/2016
17
Diagnostic Contact Lens
DisinfectionLow water content lenses
Always use heat when possible
Contamination rate
Heat 5%
Chemical 67%
Does not damage low water content lenses
With time, heat treated lenses become
contaminated in vials (Callendar et al)
Re-treat with heat every month if possible
Diagnostic Contact Lens
Disinfection
High water content lenses
Heat reduces life of lens
Meticulous cleaning with bactericidal
cleaner
Use system with maximum kill
(Hydrogen peroxide, Optifree
PureMoist, Biofinity)
Re-treatment of lenses monthly
Who Will Be King (Queen)
Designate an “infection
control commissioner”
Must be self starter
Must be consistent &
persistent
Everyone in the office is
answerable including
doctors
Implementing Infection Control
In Your Office Tomorrow
Doctors, educate yourself first
Educate a key infection control “person”
Educate your entire staff
Write a “plan of action” for each facet of infection control
Basic procedures
Instrument sterilization
Contact lens disinfection
Conduct staff training sessions
Initiate and maintain a system

AEP Course 06/10/2016
18
Implementation Of Infection
Control In Your OfficeDesignate an infection control person
Dependable, meticulous, self-starter
What level of disinfection / sterilization you
want?
Which system you want to use?
Heat vs. Chemical
Purchase the required materials
Train and model- be a role model
Maintain the system!
Develop quality assurance controls
Conclusion
Optometry is becoming more involved in
procedures that require infection control
We are held to the same standard as other
health care professionals
If optometry fails to implement infection
control we may be “discovered” - Ask any
dentist
The time to start an infection control
program in your office is now!
Let me know if I can help!