Embed Size (px)
Citation preview
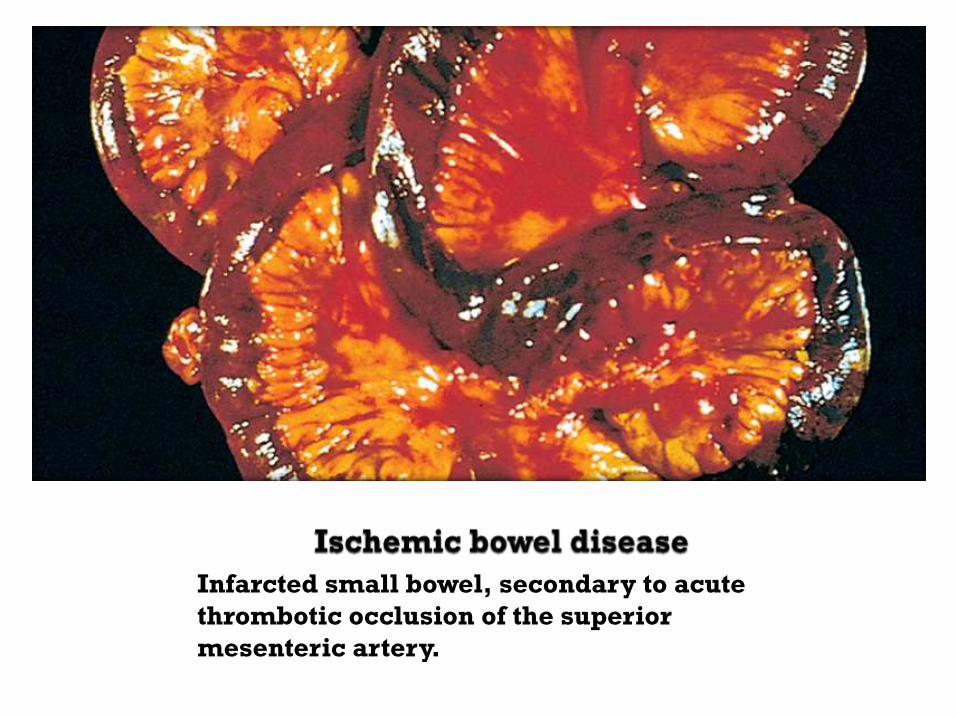
Infarcted small bowel, secondary to acute
thrombotic occlusion of the superior
mesenteric artery.
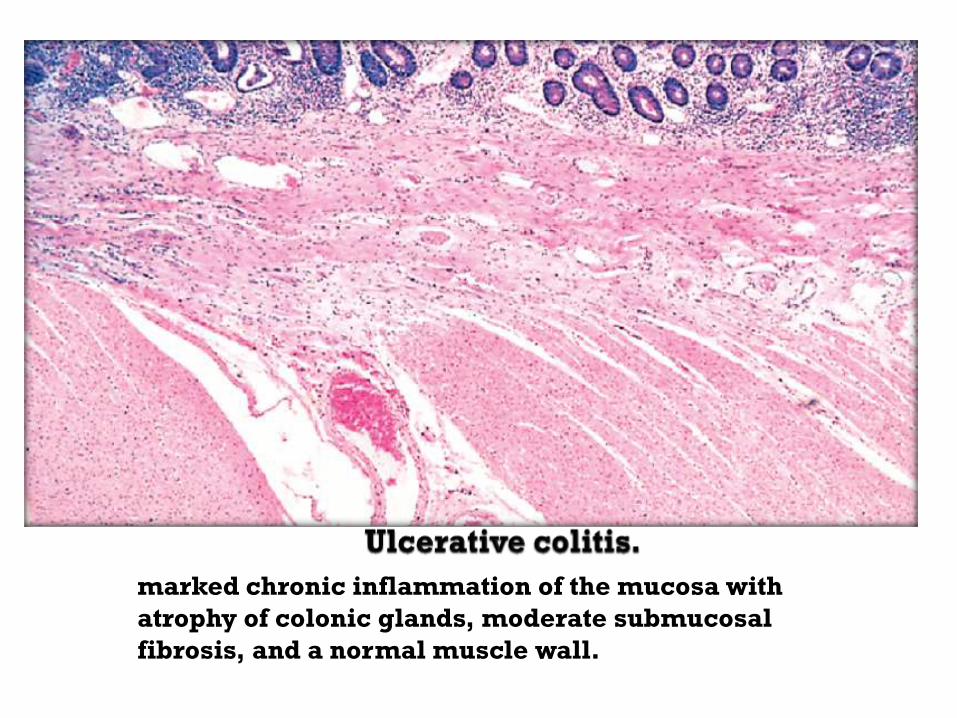
marked chronic inflammation of the mucosa with
atrophy of colonic glands, moderate submucosal
fibrosis, and a normal muscle wall.
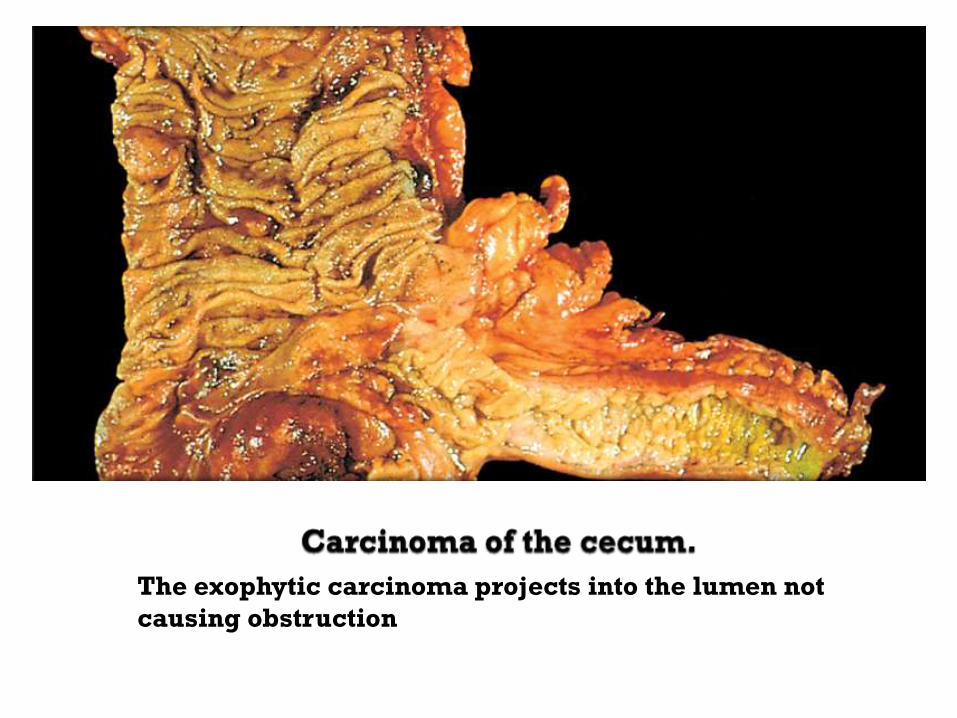
The exophytic carcinoma projects into the lumen not
causing obstruction
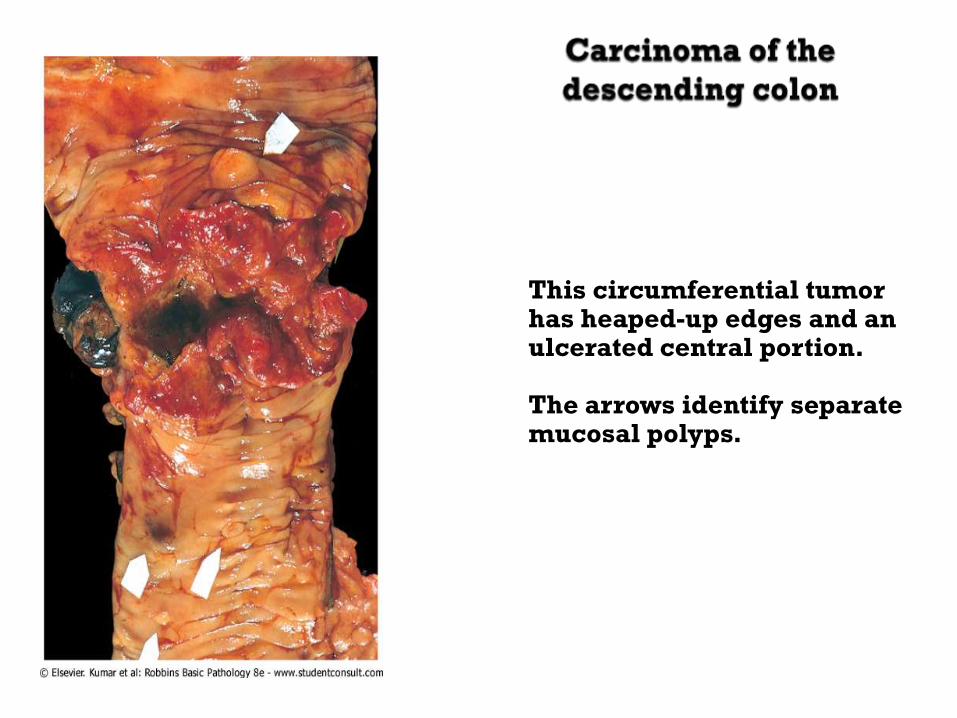
This circumferential tumor has heaped-up edges and an ulcerated central portion. The arrows identify separate mucosal polyps.
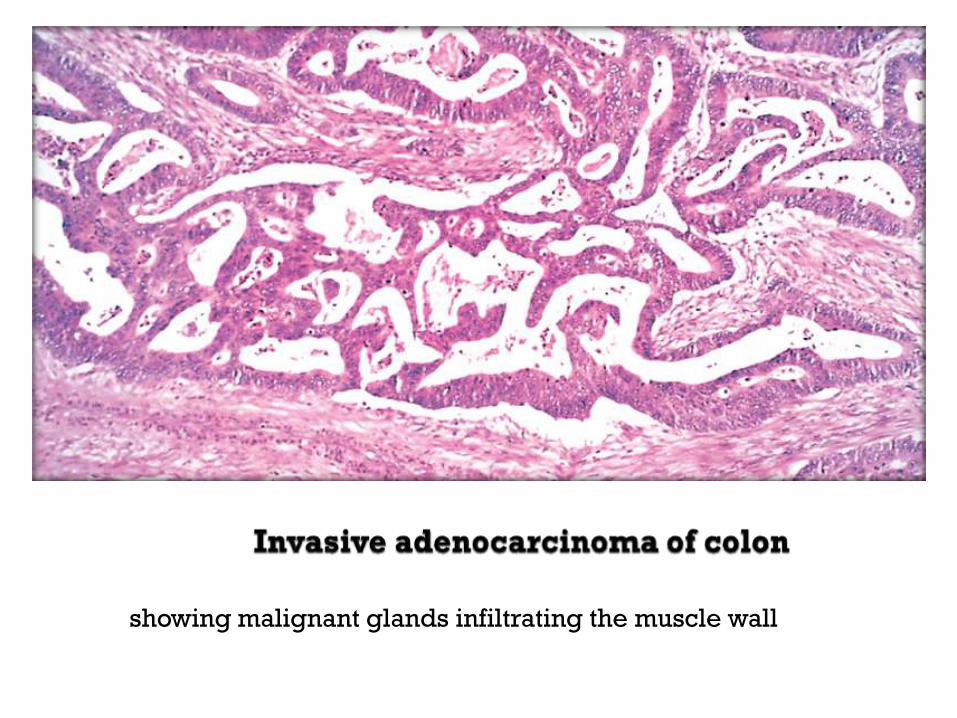
showing malignant glands infiltrating the muscle wall
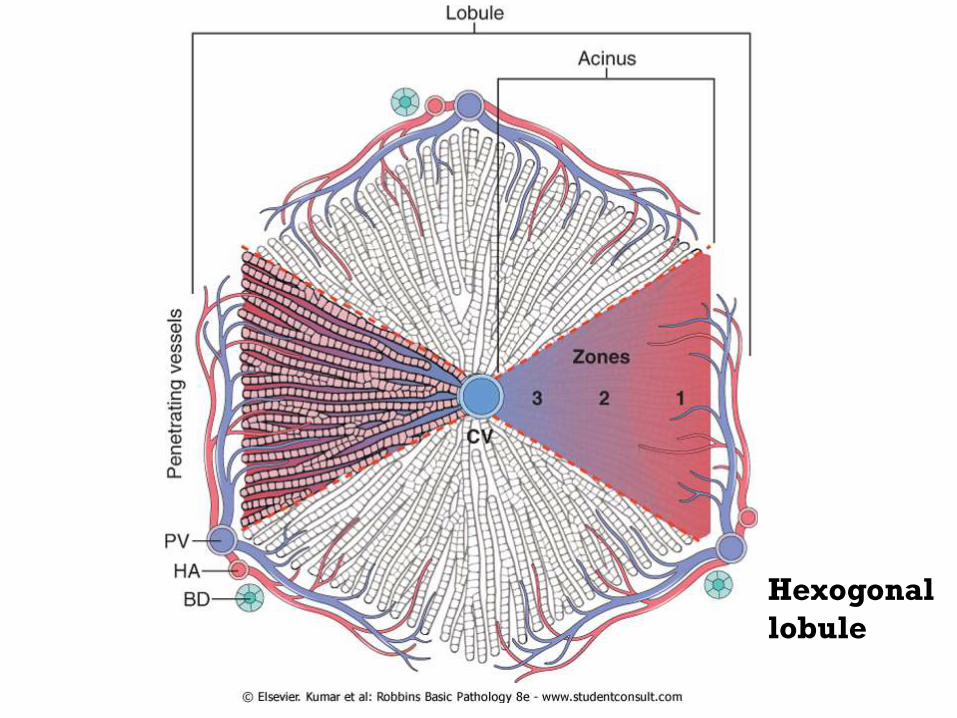
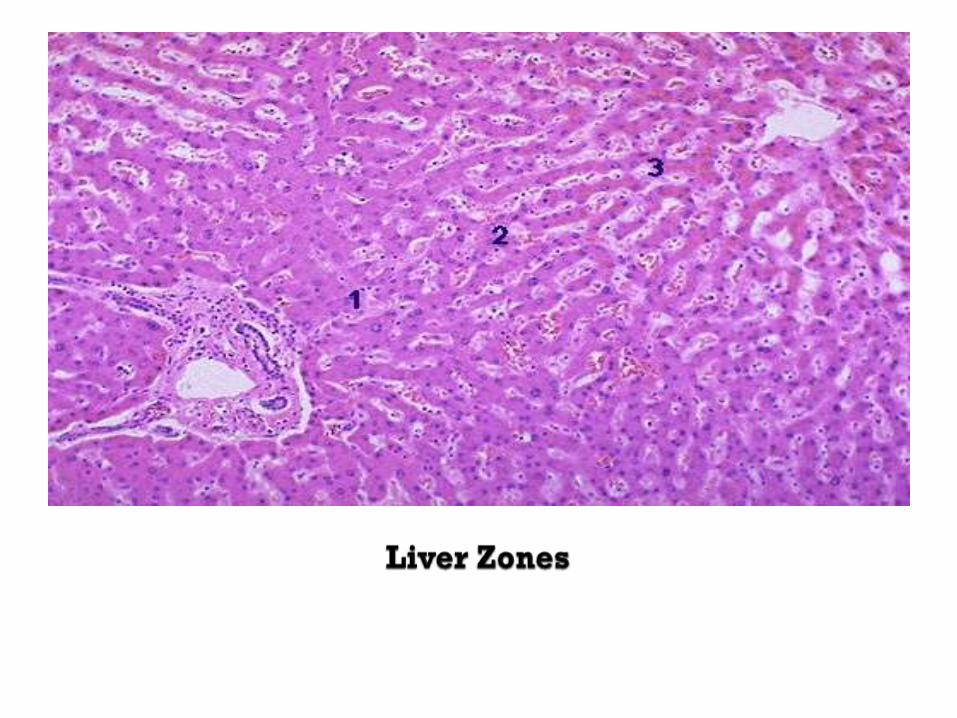
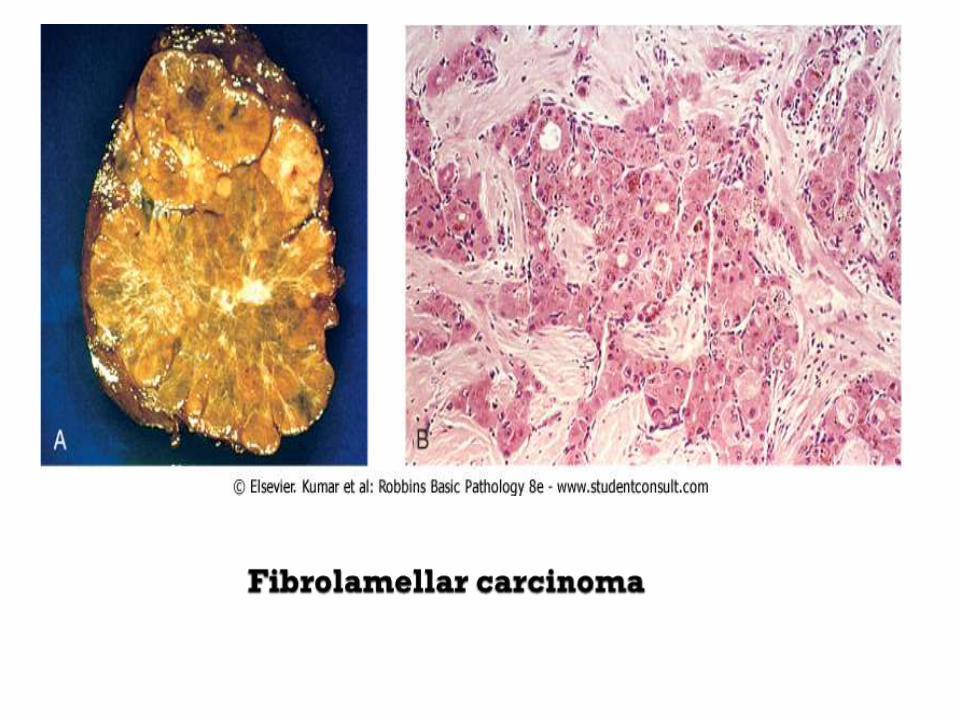
Hexogonal
lobule

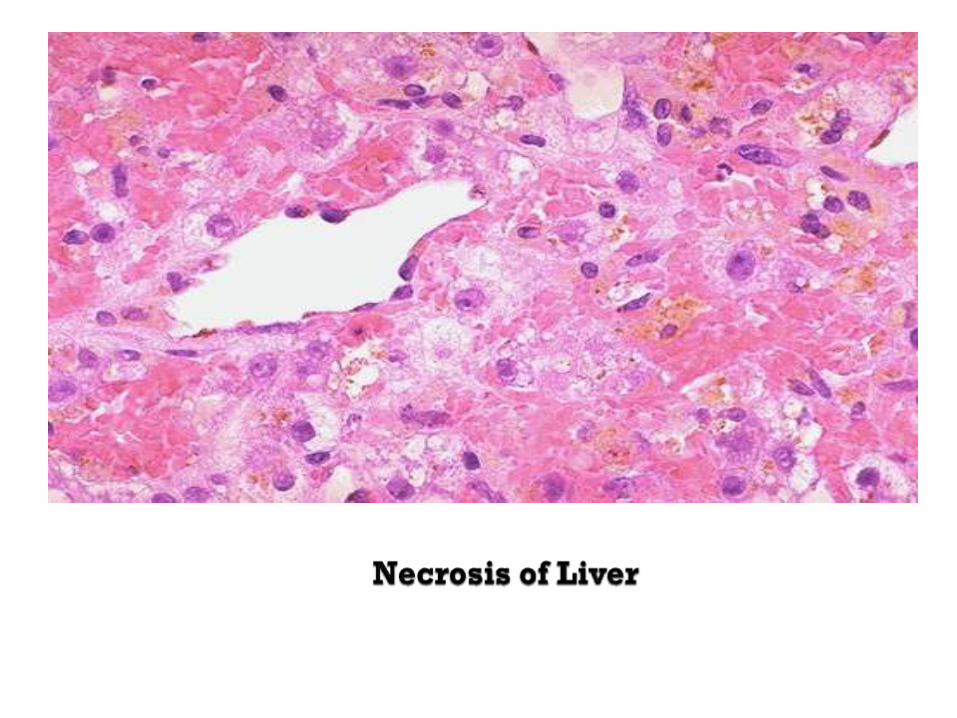

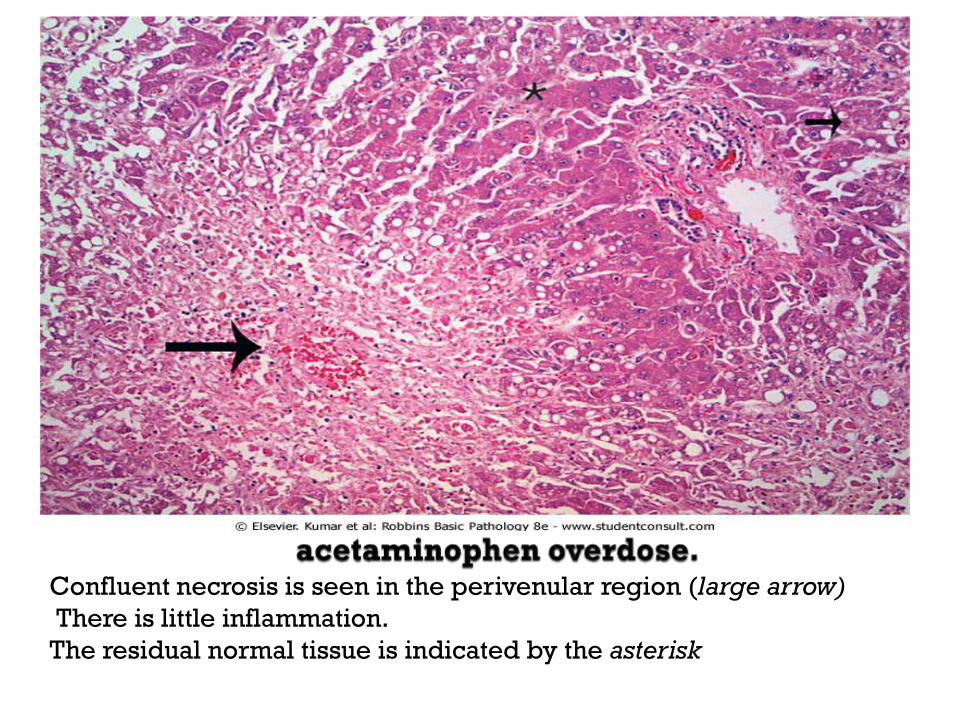
Confluent necrosis is seen in the perivenular region (large arrow)
There is little inflammation.
The residual normal tissue is indicated by the asterisk
Infections of the Liver
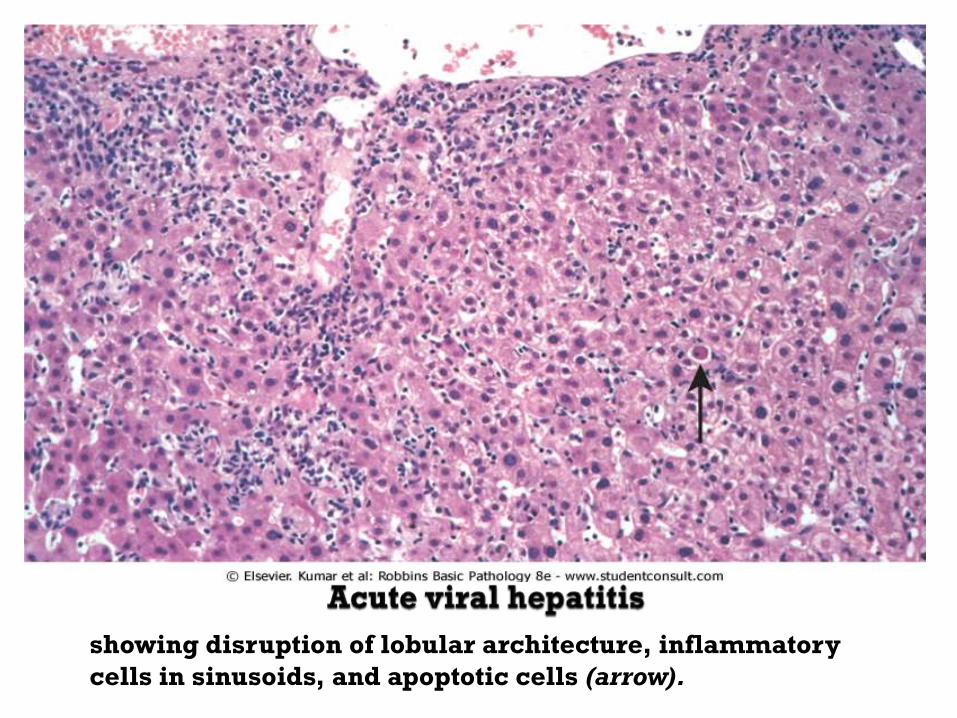
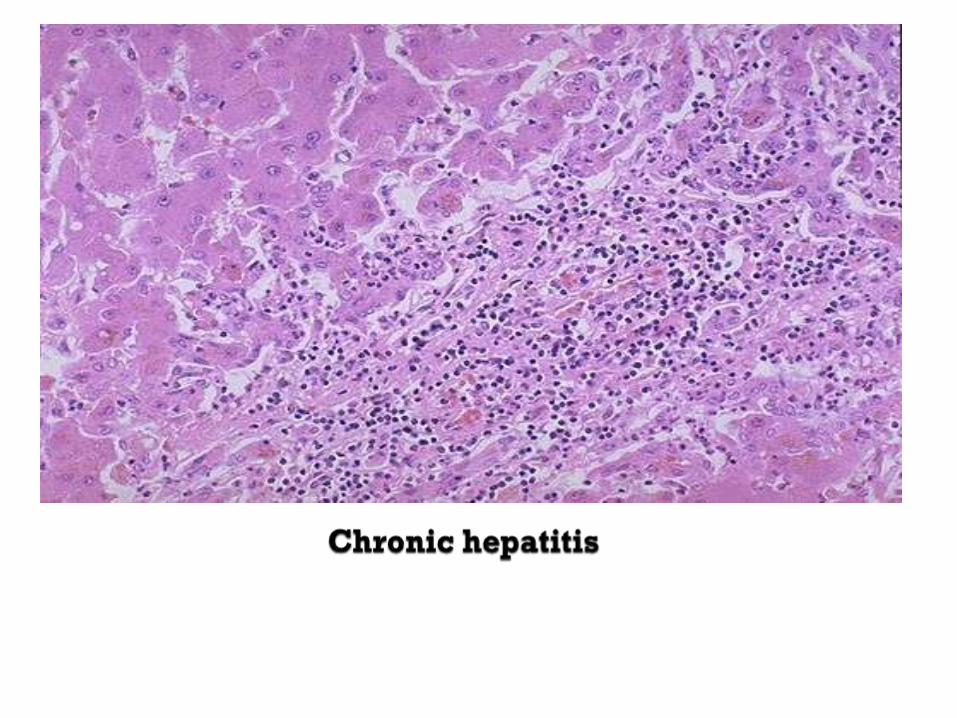
showing disruption of lobular architecture, inflammatory
cells in sinusoids, and apoptotic cells (arrow).
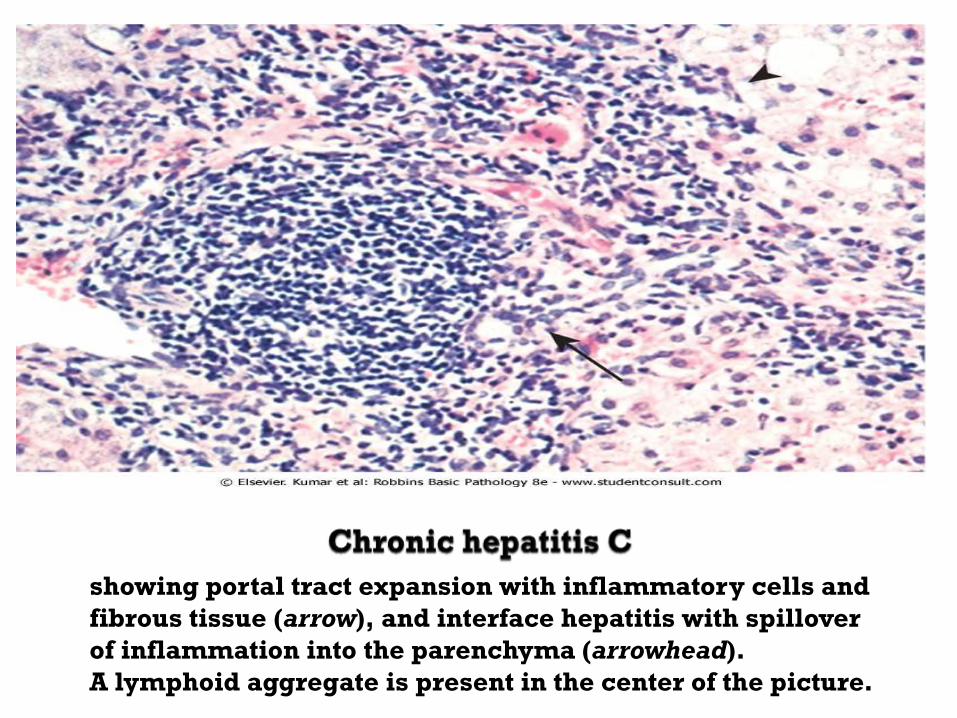
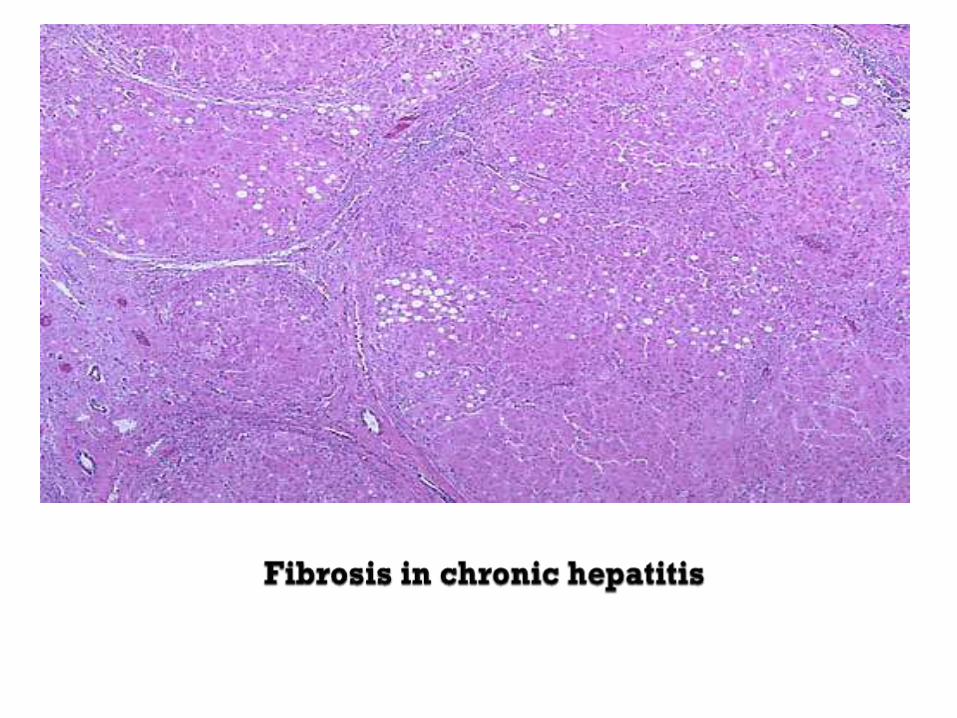
showing portal tract expansion with inflammatory cells and
fibrous tissue (arrow), and interface hepatitis with spillover
of inflammation into the parenchyma (arrowhead).
A lymphoid aggregate is present in the center of the picture.
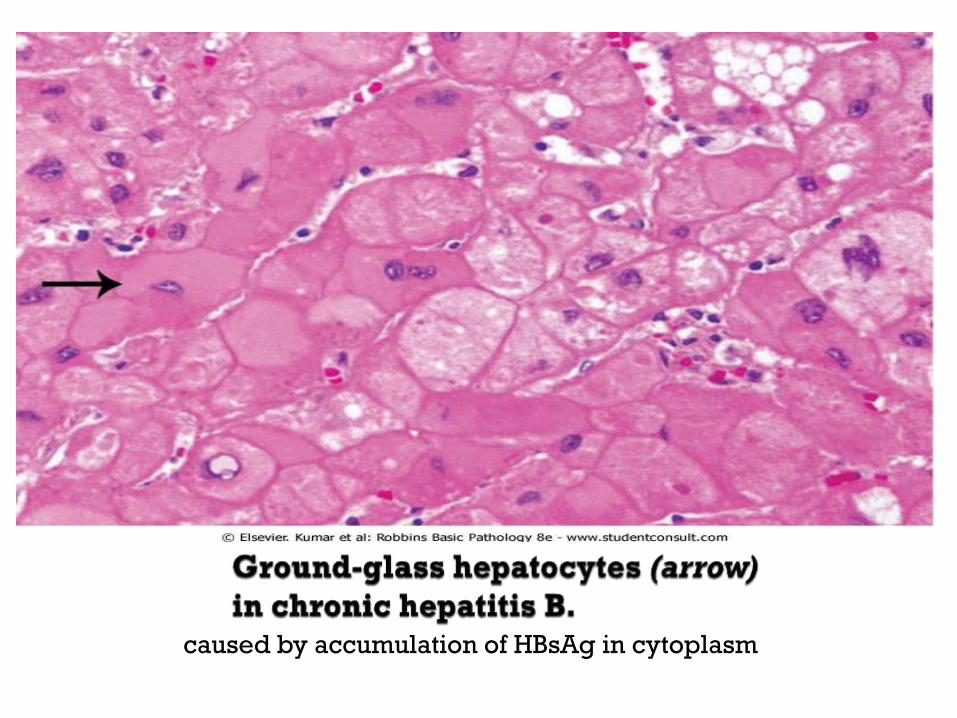
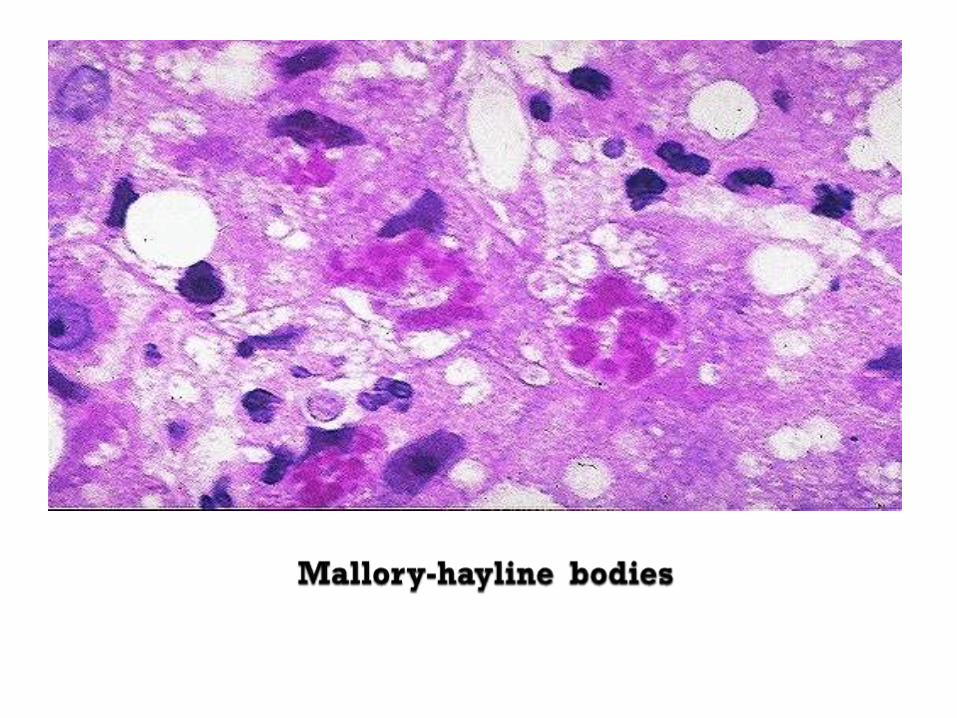
caused by accumulation of HBsAg in cytoplasm
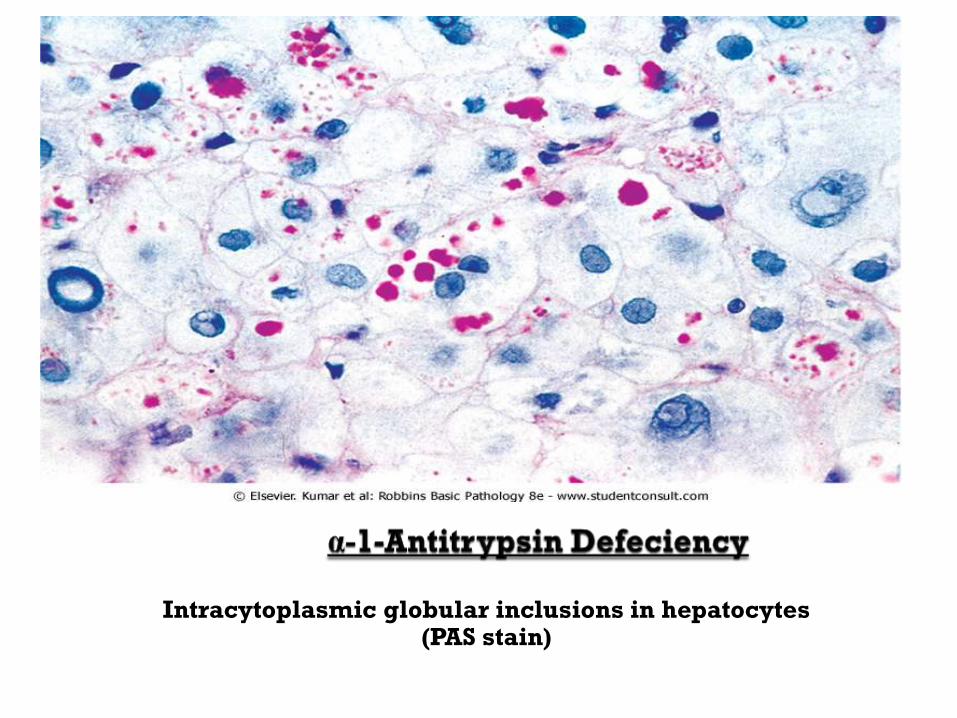
Intracytoplasmic globular inclusions in hepatocytes
(PAS stain)
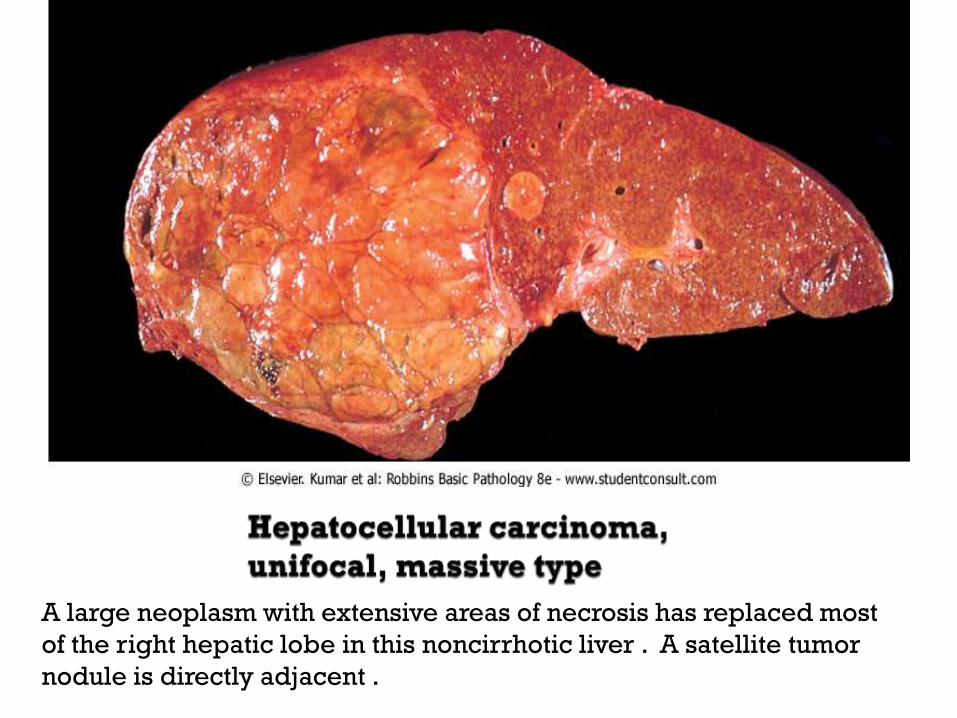
A large neoplasm with extensive areas of necrosis has replaced most
of the right hepatic lobe in this noncirrhotic liver . A satellite tumor
nodule is directly adjacent .
Your colleague :-
Lutfi Sowan .




![Bowel Elimination Si.ppt [Read-Only] - ocw.usu.ac.idocw.usu.ac.id/.../kdm_slide_bowel_elimination.pdfPrimary organ of bowel elimination ... Small bowel series Barium enema. ... Sigmoid](https://img.pdfslide.us/doc/110x75/5adf17e77f8b9ac0428bbfc8/bowel-elimination-sippt-read-only-ocwusuacidocwusuacidkdmslidebowel.jpg)

![Small bowel intussusception secondary from …...[2, 3]. The pathophysiology of intussusception secondary to tumor (either intraluminal or extraluminal lesion) is associated with alteration](https://img.pdfslide.us/doc/110x75/5fa74c53d9fad058eb45178c/small-bowel-intussusception-secondary-from-2-3-the-pathophysiology-of-intussusception.jpg)






![Small bowel metastasis from pulmonary rhabdomyosarcoma causing intussusception… · 2019. 5. 10. · about intussusception secondary to small bowel metasta-ses [15, 16]. The incidence](https://img.pdfslide.us/doc/110x75/60b78e3a5ed00d2e7a4d273e/small-bowel-metastasis-from-pulmonary-rhabdomyosarcoma-causing-intussusception-2019.jpg)














