Embed Size (px)
Citation preview

Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/7071545
InfantswithPerinatalHypoxicIschemia:FeasibilityofFiberTrackingatBirthand3Months1
ArticleinRadiology·August2006
DOI:10.1148/radiol.2393041523·Source:PubMed
CITATIONS
19
READS
28
5authors,including:
Someoftheauthorsofthispublicationarealsoworkingontheserelatedprojects:
High-DimensionalSingle-CellAnalysisByMassCytometry(CyTOF)OfTheMucosalIntestinalImmune
SystemInHealthAndDisease.Viewproject
VisualAnalysisinPopulationImagingResearch(VAnPIRe)Viewproject
CarolavanPul
MaximaMedicalCenter
39PUBLICATIONS371CITATIONS
SEEPROFILE
JanBuijs
MaximaMedicalCenter
12PUBLICATIONS147CITATIONS
SEEPROFILE
AnnaVilanova
DelftUniversityofTechnology
141PUBLICATIONS1,353CITATIONS
SEEPROFILE
P.F.F.Wijn
MaximaMedicalCenter
93PUBLICATIONS1,044CITATIONS
SEEPROFILE
AllcontentfollowingthispagewasuploadedbyCarolavanPulon30September2014.
Theuserhasrequestedenhancementofthedownloadedfile.Allin-textreferencesunderlinedinblueareaddedtotheoriginaldocument
andarelinkedtopublicationsonResearchGate,lettingyouaccessandreadthemimmediately.

Infants with Perinatal HypoxicIschemia: Feasibility of FiberTracking at Birth and 3 Months1
Carola van Pul, PhDJan Buijs, MDAnna Vilanova, PhDF. George Roos, MDPieter F. F. Wijn, PhD
The purpose of this study was to retrospectively investi-gate the feasibility of fiber tracking at birth and 3 months ininfants with hypoxic ischemia to detect disturbances inwhite matter development. This retrospective study didnot require institutional review board approval. All par-ents gave informed consent. Diffusion-tensor magneticresonance (MR) images were obtained in full-term new-borns: seven with standard MR imaging findings and 10with perinatal hypoxic ischemia–related abnormalities. Vi-sualization of white matter tracts was investigated by usinga volume-tracing and quantification technique. Fiber track-ing was useful for studying the neonatal brain. Abnormali-ties resulted in fiber patterns that were different from thefiber patterns of normal brain tissue. The corona radiatafibers were frequently affected.
� RSNA, 2006
1 From the Departments of Clinical Physics (C.v.P.,P.F.F.W.), Neonatology (J.B.), and Radiology (F.G.R.), Max-ima Medical Center Veldhoven, De Run 4600, PO Box7777, 5500 MB Veldhoven, the Netherlands; and Depart-ments of Applied Physics (C.v.P., P.F.F.W.) and Biomedi-cal Engineering (A.V.), Eindhoven University of Technol-ogy, Eindhoven, the Netherlands. Received September 3,2004; revision requested November 11; revision receivedFebruary 3, 2005; accepted March 11; final version ac-cepted August 1. Address correspondence to C.v.P.(e-mail: [email protected] ).
� RSNA, 2006
ORIGINALRESEARCH
�TECHNICAL
DEVELOPMENTS
Radiology: Volume 240: Number 1—July 2006 203

Cerebral white matter myelinationis known to start in utero and tocontinue during the first year of
life (1). At birth, myelination is ob-served in only a few cerebral white mat-ter structures; among these are the pos-terior limb of the internal capsule(PLIC) and the central part of the co-rona radiata (CR). During the firstmonths of life, the optic radiation andthe splenium of the corpus callosum(CC) become myelinated; the anteriorlimb of the internal capsule and thegenu of the CC become myelinated at3–6 months (1–3).
The process of myelination can befollowed by using conventional magneticresonance (MR) imaging techniques,such as T1- and T2-weighted imaging(4), or by using the relatively recentlyintroduced technique, diffusion-tensorimaging (5–7). A preference of watermolecules for diffusion in a particulardirection (ie, anisotropic diffusion) re-flects the underlying tissue structure.Diffusion-tensor imaging is based on theacquisition of a tensor to describe diffu-sion. The main eigenvector of the diffu-sion tensor defines the preferred direc-tion when the underlying tissue struc-ture (eg, white matter) is linear (8,9).Various methods for visualization of thediffusion anisotropy and the preferreddirection are available and include an-isotropy maps that display the anisot-ropy index (10) and color maps thatdepict the diffusion direction with color-coded pixels (11–13). Fiber tracking, arelatively recently introduced technol-ogy, is a three-dimensional visualizationtechnique in which the underlying linearstructure defined by the diffusion tensoris reconstructed (9,14–16).
White matter in the adult brain ishighly myelinated, and visualization ofthe main direction of diffusion corre-sponds to known white matter path-ways on anatomy atlases, as outlined indetail on a recently published brain fiberatlas (13). In neonates, the white matteris still developing. Diffusion anisotropyhas been reported to occur before my-elination occurs and to increase withincreasing myelination (5–7,17).
The preliminary results of fibertracking with 3.0-T MR imaging in new-
borns obtained by Zhai et al (18) showthat this technique is feasible in the neo-natal brain, although only the majorwhite matter tracts could be traced. In acase report of one neonate and two chil-dren aged approximately 2 years, fibertracking was shown to yield additionalinformation about the white matter con-figuration during dysgenesis of the CC(19). Furthermore, asymmetry in thepyramidal tracts has been observed inchildren with congenital hemiparesis(20).
A high incidence of severe motorproblems in newborns with hypoxic-is-chemic injury in the white matterand/or injury in the basal ganglia hasbeen reported (1,21,22). Thus, the pur-pose of our study was to retrospectivelyinvestigate the feasibility of fiber track-ing at birth and 3 months in infants withhypoxic ischemia to detect disturbancesin white matter development.
Materials and Methods
At our medical center (Maxima MedicalCenter Veldhoven), an MR imaging pro-tocol, including diffusion-tensor imag-ing, has been approved by the board ofthe neonatal department to be part ofour normal clinical routine. All parentsgave informed consent for the inclusionof their babies’ imaging and clinical datain this study. We consulted our institu-tional review board, which did not re-quire its approval for this retrospectivestudy. All infants with abnormalities ob-served on MR images obtained duringthe first month after the onset of symp-toms were reexamined at ages 3–4months for determination of either thefinal extent of the possible injury or nor-mal brain development. We retrospec-tively selected all neonatal patients inwhom diffusion-tensor images that weresuitable for fiber tracking had been ob-tained.
Infant Patient GroupThe study group was recruited from agroup of neonates who were born atterm with perinatal hypoxic ischemiaand were treated in our neonatal inten-sive care unit. Perinatal hypoxic ische-mia was diagnosed when clinical symp-
toms of neonatal encephalopathy werepresent with two or more of the follow-ing risk factors during the first days oflife: fetal heart rate abnormality, umbil-ical artery pH level lower than 7.10,meconium-stained fluid, and Apgarscore 5 minutes after birth lower than7. Included in our study group were allinfants from this group in whom a diffu-sion-tensor image suitable for fibertracking at birth and at 3 months wasobtained. All babies with congenital ab-normalities, neurometabolic disease,and/or perinatal infection were ex-cluded.
The data from a total of 10 full-terminfants were included between Novem-ber 2002 and June 2004. All includedbabies were born after an uneventfulpregnancy. The onset of symptomscould be timed to the day of birth. Thenewborns (nine male, one female) had amean gestational age of 40.2 weeks �1.6 (standard deviation � in the group)and were imaged at ages 1–9 days (n �9); one baby was imaged 17 days afterbirth. Follow-up MR imaging was per-formed a mean of 3.4 months � 0.5later. Neurodevelopmental evaluationswere performed when the infants werebetween 6 and 12 months of age, ac-cording to the protocol of Amiel-Tisonet al (23). The Bayley Scales of Infant
Published online before print10.1148/radiol.2393041523
Radiology 2006; 240:203–214
Abbreviations:ADC � apparent diffusion coefficientCC � corpus callosumCl � linear anisotropy indexCR � corona radiataIFO/OR � inferior fronto-occipital fasciculus and/or optic
radiationPLIC � posterior limb of internal capsuleROI � region of interest
Author contributions:Guarantor of integrity of entire study, P.F.F.W.; study con-cepts/study design or data acquisition or data analysis/interpretation, all authors; manuscript drafting or manu-script revision for important intellectual content, all au-thors; manuscript final version approval, all authors;literature research, C.v.P., J.B., A.V.; clinical studies,C.v.P., J.B., A.V., F.G.R.; statistical analysis, C.v.P.,P.F.F.W.; and manuscript editing, C.v.P., J.B., A.V.
Authors stated no financial relationship to disclose.
TECHNICAL DEVELOPMENTS: Fiber Tracking in Infants van Pul et al
204 Radiology: Volume 240: Number 1—July 2006

Development (edition 2, Dutch version)were used to test the psychomotor de-velopment of the infants when theywere aged 1 year or older. According tothe Bayley classification system, a psy-chomotor development score lowerthan �2� indicates severe delay and ascore between �2� and �1� indicatesmoderate delay. Neurodevelopmentalexaminations were performed in the in-fants at ages 6 months (n � 5) and 1year (n � 5).
Reference ValuesBecause we did not have a control groupof healthy newborns, we obtained refer-ence values from seven full-term new-borns in whom MR imaging was per-formed for clinical purposes during thesame period that the newborns in thepatient group were imaged. The refer-ence values were obtained from full-term newborns who had various clinicalsymptoms; the values were not chosenby using the criteria used to select thehypoxic-ischemic encephalopathy group.The newborns in this reference group hadclinical symptoms of Sarnat stage 1 or 2perinatal hypoxic ischemia (five babies),perinatal infection (one baby), and mildpersistent neonatal pulmonary hyperten-sion (one baby, who needed endotrachealventilation for 3 days and nitric oxidetherapy for 1 day and had a normal clini-cal short- and long-term follow-up). All ofthese newborns were imaged 4–13 daysafter birth. MR imaging revealed normalfindings (n � 4), minor signal intensityabnormalities in the cortex (ie, high signalintensity on the T1-weighted image [22])with no signal intensity abnormalities inthe white matter (n � 2), or a minorabnormality in the cerebellum (n � 1).This reference group consisted of one fe-male and six male neonates with a meangestational age of 39.0 weeks � 1.6. Theirbrain development and myelination wereassessed at T1- and T2-weighted imagingand found to be normal. It was verifiedthat no abnormalities were visible on thediffusion-weighted images, all of whichwere acquired within the first week afterbirth (by J.B., F.G.R.). The same neuro-developmental examinations that wereperformed in the patient group were per-formed in these children at ages 6 months
(two babies) and 1 year (five babies). Allof these babies were deemed to be devel-opmentally healthy. Two babies in thisgroup were examined at follow-up MRimaging, including diffusion-tensor imag-ing, at age 31⁄2 months.
MR Imaging ProtocolA 1.0-T MR imaging unit (Gyroscan;Philips Medical Systems, Best, theNetherlands) was used. The imagingprotocol included the acquisition of T1-weighted spin-echo (568/18 [repetitiontime msec/echo time msec]), T2-weighted fast spin-echo (4381/120),and inversion-recovery (3436/18/400[repetition time msec/echo time msec/inversion time msec]) MR images. Theneonatal patients were sedated withchloral hydrate and fixated by using avacuum pillow. For all brain imaging, astandard birdcage head coil was used.
The imaging protocol also includeddiffusion-tensor imaging, which wasperformed by using pulsed field gradi-ents in six directions with single-shotecho-planar MR imaging. In the neona-tal brain, 20 adjacent sections were re-corded within 3 minutes with 3595/82and a voxel size of 1.56 � 1.56 � 3 mm.Two signals were acquired. Three b val-ues (0, 400, and 800 sec/mm2) wereused to calculate the apparent diffusioncoefficient (ADC). A duration of onegradient lobe of the pulsed field gradi-ents of 20.06 msec, a time between theonset of the first gradient lobe and theonset of the second gradient lobe of40.5 msec, and a gradient lobe strengthof 19.6 mT/m were used with a b of 400sec/mm2, and a gradient lobe strengthof 27.8 mT/m (by combining the x, y,and z gradients) was used with a b of800 sec/mm2. We chose to use b valueslower than those used in the adult brain(typically 1000 sec/mm2) because theADC in the white matter of neonates ishigher than that in the white matter ofadults. The optimal b value was calcu-lated by using the method of Jones et al(24).
Postprocessing and Image AnalysisADC maps were constructed by usingsoftware on the MR imaging unit. Thediffusion-tensor images were converted
into the file format used in the fiber-tracking program by using Mathematica4.2 software (Wolfram Research, Ur-bana, Ill). For display of global informa-tion, color mapping and fiber trackingwere implemented. Color mapping wasperformed by mapping the first eigen-vector of the diffusion tensor directly tothe red-green-blue channel and therebycolor coding the diffusion direction. Fi-ber tracking is based on the line propa-gation technique (9), which involves theuse of the second-order Runge-Kuttamethod for numerical integration. Stop-ping criteria, which are used in the fi-ber-tracking procedure to determinewhen the tracking is to be stopped,could be defined by the user. Examplesof user-defined stopping criteria wouldbe an anisotropy value smaller than thethreshold value and an � angle (maximalangle between connected vectors duringfiber tracking) larger than the thresholdangle. For visualization, the user couldalso choose to display only fibers of acertain length. The stopping criteriathat were used in this study are listed inTable 1.
A problem with fiber tracking is thatof selecting the seed points from whichthe fiber tracking will be started. Usu-ally, the seed points are defined by theuser—for example, by defining an ROI,which requires prior knowledge aboutthe structures in the data set. The disad-vantage of using this seed point selec-tion method is that information can beeasily missed when abnormalities arepresent in the data set. For example,when fibers are disrupted, ROI-basedtracing will be stopped in the disruptedarea, and the other part of the fiber—ifit is intact—will not be detected. Fur-thermore, the fact that it is unknownwhich tracts in the brain of a newborncan be visualized complicates fibertracking.
We have implemented a volume-tracing method of fiber tracking inwhich all voxels are considered as possi-ble seed points. This approach yieldslong and evenly spaced fibers. The userdefines how dense the visualized fibersmust be by choosing values for the min-imal distance between the seed pointsand the fibers and for the minimal dis-
TECHNICAL DEVELOPMENTS: Fiber Tracking in Infants van Pul et al
Radiology: Volume 240: Number 1—July 2006 205

tance allowed between the fibers oncetracking has started. Tracking of a givenfiber stops if the tracking starts to occurtoo close to other fibers—that is, withina distance that is less than the minimaldistance allowed between the fibersduring tracking. This algorithm hasbeen described in detail previously (25).
For detailed visualization of a partic-ular white matter structure, multipleROIs for seed point selection can bedefined. ROIs that are sampled uni-formly to generate seed points arecalled “Or ROIs” derived by using the“Or” criterion. ROIs defined to show thefibers that pass through it are called“And ROIs” derived by using the “And”criterion. If no ROI derived with the“Or” criterion is defined, then the entirevolume is seeded and just the fibers thatpass through the “And” ROI are shown.This method prevents structures frombeing missed owing to undersampling ofthe ROI. It must be noted that, in con-trast to conventionally displayed radio-logic images, fiber-tracking images can-not always be displayed from the feet tothe head. Therefore, for all images, theviewpoint has been indicated.
The color maps were used to evalu-ate the directionality and anisotropy ofseveral white matter structures bymeans of visual inspection. The struc-tural information observed on the colormaps was compared with the structuresobserved on the color maps used by
Makris et al (11), Wakana et al (13),and Jellison et al (26). Quantitative an-isotropy maps were used to determinewhether anisotropy was increased in af-fected regions and thus to determinewhether this increased anisotropy couldinfluence the fiber tracking. Volumetracing was used to determine, in auser-independent way, which fiberstructures were visible. The obtainedfiber-tracking images were comparedwith the fiber-tracking atlases definedby Wakana et al (13) and Jellison et al(26). The color maps, anisotropy maps,and fiber-tracking images were evalu-ated and interpreted in consensus bythree authors (C.v.P., J.B., and F.G.R.,all with 5 years experience in pediatricbrain MR imaging and/or diffusion-tensor imaging). The fiber structuresobserved in the babies with standardMR imaging findings served as a refer-ence.
The fiber structures observed inthe babies at 3 months were comparedwith the structures observed in thesame babies at birth. Some tracts, likethe inferior fronto-occipital fasciculusand the optic radiation, have been re-ported to course close together and tobe oriented in a similar direction (26–28). These tracts could not be de-tected separately by using color map-ping or volume tracing and weretherefore considered to be a combinedtract (ie, fronto-occipital fasciculus
and/or optic radiation [IFO/OR] tract);thus, “IFO/OR” indicated that the fiberpath detected could have correspondedto either or both tracts. These tractscan be separated by using ROIs with the“And” criterion; however, this processwas not performed in this study. Weused the term fiber pathology to de-scribe an abnormality in which a visibleasymmetry in the fiber pattern betweenthe left and right hemispheres or a largedeviation in the fiber pattern, as com-pared with the fiber pattern in the refer-ence infant group, was observed. Afterdetermining which structures were visi-ble, with use of an ROI-based tracingmethod, we defined multiple ROIs tovisualize the structures observed at vol-ume tracing in more detail.
We chose the anisotropy index Cl—not fractional anisotropy or relative an-isotropy—as a stopping criterion be-cause it is more sensitive to linear an-isotropy and less sensitive to planaranisotropy, as determined by using nor-malized eigenvalue space plots (29).The values for Cl were based on thevalues measured in neonatal white mat-ter and CC (30). To avoid fiber informa-tion cluttering, the chosen value atwhich fiber volume tracing was stoppedwas larger than that at which ROI-basedtracing was stopped (Table 1).
With both volume tracing and ROI-based tracing, fibers were displayedonly if they were longer than a user-defined length, because visualization ofthe smaller fibers could have resulted inadditional information cluttering. Forneonates at birth, a minimal length ofgreater than 3 mm was used, and forbabies at 3 months of age, a minimallength of greater than 5 mm was used(Table 1).
Quantification of PLIC FibersThe motor and somatosensory path-ways in the CR pass perpendicular tothe transversal plane through the PLIC(31). Herein, these fibers are referredto as PLIC fibers. To determine thelength and volume of the PLIC fibers,two ROIs were drawn roughly aroundthe PLIC in two adjacent transversalsections. We used the “And” criterion:Fiber tracking was initiated from all
Table 1
Criteria Used to Stop Fiber Tracking in Patient Groups and Evaluation Methods
Patient GroupCriteria to StopVolume Tracing
Criteria to StopROI-based Tracing
Criteria to Stop PLICFiber Measurements
Neonates at birth Cl � 0.12 Cl � 0.08 Cl � 0.12� � 10° � � 10° � � 10°L � 3 mm L � 3 mm L � 0 mm
Infants aged 3 mo Cl � 0.14 Cl � 0.10 Cl � 0.12� � 10° � � 10° � � 10°L � 5 mm L � 5 mm L � 0 mm
Note.—With volume tracing, the minimal distance between the seed points and the fibers (dl) was 1.0 mm and the minimaldistance allowed between the fibers was 0.5 � dl. The region-of-interest (ROI)-based method involved the use of four to six ROIsobtained with the “Or” criterion. To determine the length and volume of the PLIC fibers, two ROIs were drawn around the PLICin two adjacent transversal sections and the “And” criterion was used. Different stopping criteria were used in babies at birthand in those aged 3 months, because the structures were more developed at 3 months and using the same stopping criteriacould have led to information cluttering. With use of more stringent stopping criteria at 3 months, cluttering was prevented andno fiber information was lost. Cl � linear anisotropy index (ie, index sensitive to linear diffusion), L � length of the displayedfibers, � � maximal angle between connected vectors during fiber tracking.
TECHNICAL DEVELOPMENTS: Fiber Tracking in Infants van Pul et al
206 Radiology: Volume 240: Number 1—July 2006

points in the volume, and only thosefibers passing through both ROIs weredisplayed. This technique was similarto the method used by Mori et al (31).If an abnormality was suspected to bedisturbing fiber tracking, the patternof disturbance was checked by usingvolume tracing. The detected distur-bance pattern would be used to deter-mine whether normal ROI selectionshould be used or the ROI selectionshould be defined in other nearbytransversal sections to prevent fibersfrom being missed owing to ROI mis-placement. Analysis of the PLIC fiberswas performed in consensus by threeauthors (C.v.P., J.B., F.G.R.). Aftervisualization of the PLIC fibers, themean length of all the fibers was calcu-lated. It must be noted that not thetrue length of the white matter fibers,but rather an indication of the lengthof the linear diffusion path of diffusingwater molecules, was determined.The fiber volume was the volume of allpixels through which one or more fi-bers passed. In all infants, the meanfiber lengths and volumes calculatedwith three Cl values (0.08, 0.10, and0.12) were determined at birth and at3 months.
Statistical AnalysesTo compare the PLIC fiber lengths mea-sured in the left and right hemispheres,a Student t test was used. A paired Stu-dent t test was used to compare thePLIC fiber lengths measured in neonatesat birth with those measured in thesame babies at 3 months. P � .05 wasconsidered to indicate significance (32).Statistical analyses were performed byusing Mathematica 4.2 software. Theseanalyses were performed by two au-thors (C.v.P., P.F.F.W.).
Results
Color MapsIn the seven infants with standard MRimaging findings (reference group),the structures that were visible onthe color maps at birth were evalu-ated. In this group, the followingstructures were clearly visible at
birth: the PLIC in all seven infants; theanterior limb of the internal capsule insix; the posterior, middle, and frontalregions of the IFO/OR in all seven in-fants, six infants, and one infant, re-spectively; the fornix in six; the cingu-
lum (directly above the CC) in six; andthe superior region of the CR in allseven. Two infants in the referencegroup were examined with MR imag-ing at 3 months. A clear differencebetween the color maps obtained at
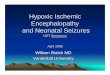
Figure 1
Figure 1: Left: Fiber-tracking images obtained at various angles in full-term newborn with standard MRimaging findings 6 days after birth. Right: Corresponding fiber-tracking images obtained in the same infant at3 months. These three-dimensional fiber-tracking images are superimposed on two-dimensional ADC maps,which were constructed by using diffusion-tensor images acquired with pulsed field gradients in six direc-tions with single-shot echo-planar MR imaging (3595/82, two signals acquired, 1.56 � 1.56 � 3-mm voxelsize, b values of 0, 400, and 800 sec/mm2). The main white matter structures are shown and closely matchstructures on the fiber-tracking atlas introduced by Wakana et al (13). The stopping criteria for ROI-basedtracing summarized in Table 1 were used. CG � cingulum, FX � fornix, spl � splenium.
TECHNICAL DEVELOPMENTS: Fiber Tracking in Infants van Pul et al
Radiology: Volume 240: Number 1—July 2006 207

birth and those obtained at 3 monthsin these babies was observed. The an-terior and posterior regions of theCR, as well as the superior fronto-occipital fasciculus and the superiorlongitudinal fasciculus, were visual-ized better at 3 months. Also, the IFO/
OR, CC, and cingulum were more ap-parent. Most structures were less pro-nounced compared with the samestructures in adults observed on thecolor maps described in several stud-ies (11,13,26).
In the infant group with fiber abnor-
malities, the color maps showed a dis-turbed pattern compared with the fiberpattern observed in the reference infantgroup. In the affected areas, there wasincreased anisotropy, which was appar-ent in white matter areas and in thegyri.
Table 2
Abnormalities and Outcomes in Infant Patients
Patient No. Main Abnormality at Birth Fiber Abnormality at Birth Main Abnormality at 3 mo Fiber Abnormality at 3 mo Outcome
1 Multifocal WM lesions,anisotropy stronglyhigher in R than in Lhemisphere
None remarkable Mildly delayedmyelination, anisotropynearly equal in R and Lhemispheres
None remarkable Normal findingsat 6 mo
2 Multifocal WM lesions,anisotropy stronglyhigher in R than in Lhemisphere
Anisotropy lower in R thanin L CR
Local tissue loss,anisotropy stronglyhigher in R than in Lhemisphere
None remarkable Normal findingsat 1 y
3 Multifocal WM lesions,anisotropy nearly equalin R and L hemispheres
Anisotropy strongly lower inR than in L IFO/OR
Normal MR findings None remarkable Normal findingsat 1 y
4 Bilateral basal gangliainjury, anisotropynearly equal in R and Lhemispheres
Anisotropy in CR stronglylower than normal,anisotropy lower in Rthan in L IFO/OR
Low myelination in ALIC,anisotropy nearlyequal in R and L partsof splenium of CC
Anisotropy lower in R thanin L CR
Moderateneuromotordelay at 1 y
5 Minor basal ganglia injury,edema in R spleniumof CC
Anisotropy strongly lower inR than in L splenium ofCC and lower in L than inR IFO/OR
Delayed myelination inALIC, anisotropy nearlyequal in R and Lhemispheres
Anisotropy lower in L thanin R IFO/OR
Normal findingsat 6 mo
6 Bilateral basal gangliainjury, diffuse WMinjury, anisotropynearly equal in R and Lhemispheres
Anisotropy low, no fibersvisible
WM and basal gangliaatrophy, anisotropynearly equal in R and Lhemispheres
Anisotropy in CR stronglylower than normal; CC,CG, and fornix notvisible
Severepsychomotorretardation at6 mo, death
7 Large infarct in territory ofMCA and basal gangliainjury, all in Lhemisphere
Anisotropy strongly lower inL than in R CR, spleniumof CC, and IFO/OR
Severe tissue loss ininfarct in L hemisphere
Anisotropy strongly lowerin L than in R CR andIFO/OR, splenium of CCand cingulum notvisible
R hemiplegia at1 y
8 Large infarct and basalganglia injury in Lhemisphere
Anisotropy strongly lower inL than in R CR, stronglyhigher in L than in Rsplenium of CC, andstrongly lower in L thanin R IFO/OR*
Severe tissue loss in Lhemisphere infarct
Anisotropy strongly lowerin L than in R CR, lowerin L than in R spleniumof CC, and stronglylower in L than in RIFO/OR
R hemiplegia at1 y
9 Occipital infarct affectingsplenium of CC in Lhemisphere
Anisotropy strongly higherin L than in R spleniumof CC, strongly lower in Lthan in R IFO/OR*
Delayed myelination ininternal capsule,anisotropy nearlyequal in R and Lhemispheres
Anisotropy strongly lowerin R than in L spleniumof CC
Hypertonia ofarms and legsat 6 mo
10 Mild WM delay None remarkable Widened ventricles None remarkable Normal findingsat 6 mo
Note.—ALIC � anterior limb of internal capsule, CG � cingulum, L � left, MCA � middle cerebral artery, R � right, WM � white matter.
* There was prolongation of splenium of CC tract owing to high anisotropy.
TECHNICAL DEVELOPMENTS: Fiber Tracking in Infants van Pul et al
208 Radiology: Volume 240: Number 1—July 2006

Fiber TrackingIn the infants with standard MR imagingfindings, several white matter tractscould be appreciated on fiber-trackingimages at birth and at 3 months (Fig 1).No differences between the right andleft hemispheres were observed in thisgroup. The following main white matterstructures could be visualized with fibertracking in these infants at birth: the CRin all seven babies, the genu and sple-nium of the CC in all seven; the entireCC in two; the posterior, middle, andfrontal regions of the IFO/OR in allseven, six, and two babies, respectively;the fornix in all seven; and the cingulum(directly above the CC) in five. All otherfibers defined on published fiber-track-ing atlases (13,26) could not yet be de-tected at birth. It must be noted that insome newborns in the reference group,structures that were not well visualizedon the color maps were visible on thefiber-tracking images. On the otherhand, not all structures that were visibleon the color maps were traceable atbirth—for example, usually only a smallpart of the cingulum could be traced. Inthe two infants with standard MR imag-ing results available at 3 months, thestructures observed at birth were moredeveloped at 3 months, although newlydeveloped structures could not be de-tected.
In the infants with abnormalities re-lated to perinatal hypoxic ischemia, de-viations in the expected pattern of fiberswere observed in the regions of the ab-normalities. A detailed overview ofthese findings is given in Table 2; thepatients are grouped according to ab-normality. In the patient group of 10infants, the following fiber structureswere frequently affected at birth: theCR in five babies, the IFO/OR in seven,and the CC in five. When these infantswere aged 3 months, disturbed fiberpatterns were still visible in the CR infour of them, in the IFO/OR in three,and in the CC in four. All of the infantswho had disturbed patterns in the CR at3 months demonstrated major motorproblems.
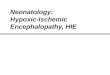
Figure 2 shows examples of fibertracking at birth and at 3 months in twoinfants with perinatal hypoxic ischemia–
related abnormalities (patients 8 and 9[Table 2]). Both infants had an infarct inthe left hemisphere, but in patient 8 alarger area was affected. In patient 8,fibers were not traced in the CR (blue)
at birth owing to the large infarct, whichaffected the basal ganglia also (Fig 2,top left). In the infarcted region, theanisotropy was inhomogeneously in-creased, and, thus, some fibers were
Figure 2
Figure 2: Fiber-tracking images obtained in (a) a newborn (patient 8, Table 2) at term and (b) the sameinfant at 3 months. Arrow points to region in which the CR fibers cannot be traced. (c) Fiber-tracking imageobtained in patient 9 (Table 2) at term. Left arrow (pointing downward) indicates the infarct, which has a lowADC. Right arrow (pointing upward) indicates the splenium of the CC in the affected hemisphere, in which thesplenium fibers are longer than those in the nonaffected hemisphere—probably owing to the abnormality.(d) Fiber-tracking image obtained in the same infant (patient 9) at 3 months. The splenium can be traced betterin the affected hemisphere than in the nonaffected hemisphere. All images shown are three-dimensional fiber-tracking images superimposed on two-dimensional ADC maps, which were constructed from diffusion-tensorimages acquired by using pulsed field gradients in six directions with single-shot echo-planar MR imaging(3595/82, two signals acquired, 1.56 � 1.56 � 3-mm voxel size, b values of 0, 400, and 800 sec/mm2).
TECHNICAL DEVELOPMENTS: Fiber Tracking in Infants van Pul et al
Radiology: Volume 240: Number 1—July 2006 209

traced in this area and were consideredfiber artifacts. Also, it is apparent thatthe IFO/OR was not traced in the af-fected hemisphere. At 3 months, the CRand IFO/OR in this infant still were nottraceable (Fig 2, top right).
In patient 9 at birth, the splenium ofthe CC had an area of low ADC and highanisotropy (Fig 2, bottom left). The an-isotropy was more increased in the leftpart of the CC than in the right, and,thus, longer fibers were traced in theleft part compared with the fiberstraced in the right part. The IFO/ORwas less visible in the affected hemi-sphere than in the nonaffected hemi-sphere. At 3 months, a widened ventri-cle was observed in the affected hemi-sphere in this infant. Development ofthe posterior forceps of the CC wasmore pronounced in the affected hemi-sphere than in the nonaffected hemi-sphere.
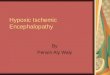
One of the problems with usingvolume tracing is that informationcluttering can occur during the tracing
owing to artifacts on the MR images(Fig 3a), which do not occur when theROI-based tracing method is used (Fig3b). The data set displayed in Figure 3is one of our worst examples. In gen-eral, the artifacts appeared as lessdense lines. They could be easily dis-tinguished from real fibers becausethey occurred only at the air-tissueboundaries. With our fiber-trackingprotocol, it is possible to rotate thestructures, use thick or thin fibers,and “look through” the cluttering.
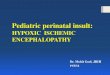
Quantification of PLIC FibersIn the infants with standard MR imagingfindings, no remarkable differences be-tween the left and right hemisphereswere observed (Fig 4, two top rows). Inpatient 8, however, a clear difference inPLIC fiber length and volume betweenthe left and right hemispheres was ob-served (Fig 4, two bottom rows). Fur-thermore, the fiber structures observedin the nonaffected hemispheres ap-peared to be smaller than normal.
At Cl values of between 0.08 and0.16, the fiber lengths in the infants withstandard MR imaging findings were ob-served to have a linear dependency onthe choice of the Cl as the stopping cri-terion. More important, the mean fiberlengths and volumes determined in theleft and right hemispheres were compa-rable. Comparing values among theseinfants was possible as long as the samestopping criteria were used. At a Cl of0.12, the mean PLIC fiber length in thereference infant group was 25 mm � 4(standard deviation � in the group) forboth hemispheres and the mean volumewas 3.0 cm3 � 1.0 for both hemi-spheres.
Of the infants with fiber abnormali-ties, four had significantly reduced PLICfiber lengths compared with the fiberlengths measured in the reference in-fant group (Fig 5a; values outside theshaded area indicate P � .05). In fivepatients, the measured fiber volumeswere reduced significantly comparedwith the reference values (P � .05) (Fig5b). The mean fiber length and volumein the patient group at 3 months weresignificantly increased compared withthe values at birth (P � .01). For threeinfants (patients 6–8), the mean fibervolume (in one or both hemispheres) at3 months deviated largely from themean value for the other patients (Fig5c, 5d). However, no comparable nor-mal values were available because onlytwo infants from the reference groupwere imaged at 3 months (Fig 5).
Discussion
Interpretation of Color Maps andFiber-tracking ImagesColor maps appear to be useful for de-termining whether the brain develop-ment in general is normal. However,interpretations of these images for theassessment of fiber structures are notstraightforward. Fiber tracking is moresuitable for these applications. How-ever, because some parts of the inferiorfronto-occipital fasciculus are close tothe optic radiation (26–28), the separa-tion of these tracts with volume tracingwas not possible in our study. To visual-
Figure 3
Figure 3: (a) Fiber-tracking image (top view) shows volume tracing in newborn with standard MR imagingfindings. The typical artifacts that result from using single-shot diffusion-tensor echo-planar imaging areseen. (b) Fiber-tracking image (top view) obtained in the same infant by using five ROIs for seed point selec-tion. Both of these three-dimensional fiber-tracking images are superimposed on two-dimensional ADCmaps, which were converted by using edge detection to display the difference between fibers and backgroundtissue more clearly. The ADC maps were calculated from diffusion-tensor images acquired by using pulsedfield gradients in six directions with single-shot echo-planar MR imaging (3595/82, two signals acquired,1.56 � 1.56 � 3-mm voxel size, b values of 0, 400, and 800 sec/mm2).
TECHNICAL DEVELOPMENTS: Fiber Tracking in Infants van Pul et al
210 Radiology: Volume 240: Number 1—July 2006

ize white matter tracts in the neonatalbrain, stopping criteria different fromthose used in the adult brain have to beused, because the anisotropy in thewhite matter of infants is lower.
Diffusion anisotropy has been ob-served before myelination occurred(5,6). Neil et al (5) divided the whitematter regions visualized at birth intothree types: (a) those packed into my-elinated parallel bundles (type 1),(b) those with mostly nonmyelinatedparallel bundles (type 2), and (c) thosethat are neither closely packed nor my-elinated (type 3). Type 1 white mattertracts—for example, the central part ofthe CR that is myelinated in infants atbirth—can be easily traced (2,6,33).The splenium of the CC and the opticradiation become myelinated in infantswithin the first 3 months and are type 2tracts. These tracts can be visualized ininfants at birth by using fiber trackingowing to the parallel orientation of thecell membranes. Type 3 white mattertracts cannot be visualized.
In the infants with fiber abnormali-ties, we observed disturbed fiber pat-terns. We must remark that when fibersare missed during fiber tracking, it doesnot mean that the white matter fibersare disconnected. This is, however, anindication that processes that have dis-turbed the diffusion have occurred.
It appears that the minor white mat-ter abnormalities seen with fiber track-ing (ie, asymmetry between hemi-spheres in a part of a traced fiber struc-ture, the IFO/OR in particular) in ourstudy tended to resolve at 3 months,while marked changes such as large fi-ber asymmetry persisted. All four pa-tients who had large fiber abnormalitiesin the CR at 3 months had a poor out-come (ie, moderate to severe motorproblems).
Several study investigators have re-ported that patients with hemiparesishave decreased anisotropy in the CRand the pyramidal tracts, which hasbeen associated with loss of myelinationand wallerian degeneration (20,34). Inour study, the loss of fibers in the CR atbirth was also visible at 3 months in fourof the five patients in whom disturbedCR fibers were visible on the fiber-
tracking images. In two of these infants,this fiber loss was associated with walle-rian degeneration.
In a previous study, ischemia wasobserved to result in increased anisot-ropy in lesions in newborns (34). In twoinfants with ischemia in the splenium ofthe CC in our study, the increased an-
isotropy resulted in longer fibers beingtraced. The implications of these obser-vations are not clear.
One of the limitations of our studywas related to the criteria used to selectthe reference group. Although all of theinfants in this group had standard MRimaging findings and normal short-term
Figure 4
Figure 4: Traced fibers of the CR (viewpoint from the left in the left column and from the right in the rightcolumn). Top four images show fibers traced in an infant with standard MR imaging findings at birth and at 3months. The difference in length and volume can be appreciated. Lower four images show fibers traced in aninfant (patient 8) with fiber abnormality; asymmetry between the left and right hemispheres is immediatelyclear. The stopping criteria used for PLIC fiber tracking summarized in Table 1 were used. These three-dimen-sional fiber-tracking images are superimposed on two-dimensional ADC maps, which were converted byusing edge detection to display the difference between fibers and background tissue more clearly. The ADCmaps were constructed from diffusion-tensor images acquired by using pulsed field gradients in six direc-tions with single-shot echo-planar MR imaging (3595/82, two signals acquired, 1.56 � 1.56 � 3-mm voxelsize, b values of 0, 400, and 800 sec/mm2).
TECHNICAL DEVELOPMENTS: Fiber Tracking in Infants van Pul et al
Radiology: Volume 240: Number 1—July 2006 211

follow-up results, we realize that thewhite matter in these babies could havebeen affected because they all were ex-amined with MR imaging because ofclinical indications. However, the gen-eral fiber pattern observed in these in-fants was similar, with no asymmetry;therefore, we assumed that this groupcould be used to obtain reference val-ues.
Quantification of PLIC FibersBecause the PLIC is myelinated at birth(2,6,20), ROI selection in this area re-sults in a clear pattern of fibers, whichinclude the motor and somatosensorytracts (31). Quantification of the lengthsand volumes of PLIC fibers appears tobe useful for detecting abnormalities,although the results must be carefullyinterpreted because they depend on thestopping criteria used. In most cases,the abnormality is directly visible owing
to the asymmetry seen on the fiber-tracking images; however, in some pa-tients the abnormality is less clear. Fur-thermore, quantification could be usefulfor identifying patients with global my-elination delays in both hemispheres.The implications of detecting this typeof abnormality for further neurologicdevelopment of the infant are not yetclear and require further study.
Fiber-tracking Methods andStudy LimitationsVolume tracing enables user-indepen-dent fiber tracking. The advantages ofusing this method are that all fibers aretraced and no fibers are missed as aresult of ROI misplacement. Further-more, if fibers appear to be disrupted,tracking from a single ROI will result inonly part of the fibers being traced. Incontrast, with use of volume tracing, allfibers, if present, will be detected as
long as they display anisotropic diffu-sion. The main problem with the vol-ume-tracing method is that typical diffu-sion-tensor and echo-planar imaging ar-tifacts, such as image distortions due toeddy currents and air-tissue susceptibil-ity effects, can result in erroneouslylarge anisotropy values. The large an-isotropy values result in what we callfiber artifacts, which can clutter the im-age. ROI-based tracing results in imageswith fewer artifacts, but it requiresprior knowledge about the structures inthe data set for correct ROI placement.By first using volume tracing to deter-mine the presence of fiber structuresand then performing ROI placement onthe basis of the knowledge obtainedwith volume tracing, the best aspects ofboth techniques can be used.
One of the main limitations of allcurrently available fiber-tracking meth-ods—this limitation was reported notonly in our current study but also inother investigations (13)—is that thetracking is stopped in regions with pla-nar anisotropy because no main direc-tion of diffusion can be determined inthese regions. With ROI-based tracingin particular, fibers might be missed ow-ing to this limitation.
It must be noted that the fiber-tracking results reported herein shouldbe carefully interpreted. First, the tech-nique is not yet validated; however, inthe myocardium, a good correlation be-tween the direction of the first eigenvec-tor and the histologic findings has beenshown (35–37). In terms of white mat-ter, good correspondence between thefiber-tracking results and the findings onanatomy atlases and/or in dissected an-atomic sections has been observed(13,26,38).
Second, the fiber-tracking techniqueis susceptible to several errors, as ex-tensively discussed in the articles ofBasser et al (39), Tournier et al (40),and Mori and van Zijl (9). In our clinicalpractice, we use a 1.0-T MR system andrelatively large voxels, in which partialvolume effects occur. Furthermore, an-isotropy is lower in the neonatal brainthan in the adult brain. The inherentlylower signal-to-noise ratio and loweranisotropy affect the accuracy of fiber
Figure 5
Figure 5: (a, b) Graphs show PLIC fiber lengths and volumes in two infants from the reference group (N1and N2) and the 10 infants from the patient group (abnormalities summarized in Table 2) at birth. Error barsindicate standard deviations of the mean fiber lengths. Shaded areas indicate 95% confidence intervals forvalues measured in the seven infants in the reference group. (a) The mean fiber length for four patients and(b) the mean fiber volume for five patients are outside the confidence intervals. The values in these patientswere significantly (P � .05) different from normal. (c, d) Graphs show fiber lengths and volumes in the sametwo infants and 10 patients whose values are illustrated in a and b, at 3 months. The mean fiber lengths andvolumes are greatly increased compared with the values at birth. (d) For three infants with abnormalities (pa-tients 6 – 8), the mean fiber volume deviated largely from the other patients’ values, in one or both hemi-spheres. In all four graphs, ‚ � left hemisphere, ■ � right hemisphere.
TECHNICAL DEVELOPMENTS: Fiber Tracking in Infants van Pul et al
212 Radiology: Volume 240: Number 1—July 2006

tracking. One problem that can occurowing to the low signal-to-noise ratio istract jumping, in which the fiber path isdetermined erroneously (39). Further-more, the anisotropy in a voxel can beobscured owing to partial volume ef-fects. Tournier et al, by using simula-tions on synthetic data, showed that toidentify small fibers, the signal-to-noiseratio needs to be high (40). This is prob-ably the reason that we cannot distin-guish small fiber tracts that are close toeach other, like the fornix and the ante-rior commissure. Although several opti-mization steps still have to be taken, themain fiber tracts in the neonatal braincan be identified by using fiber tracking.Furthermore, the topologic features ofthe identified fibers correspond to ex-pected white matter structures.
In conclusion, we have demon-strated the feasibility of fiber track-ing—a user-independent volume-trac-ing method in particular—to study theneonatal brain. Abnormalities related toperinatal hypoxic ischemia resulted infiber patterns that were different fromthe fiber structures detected in infantswith standard MR imaging findings. Fi-ber tract abnormalities occurred fre-quently in the CR; this was expectedbecause a high incidence of severe mo-tor problems in asphyxiated newbornshas been reported (1,21,22). With use ofa quantification fiber-tracking method, anabnormality could be clearly seen as adifference between the hemispheres.Furthermore, significant differences infiber lengths and volumes were ob-served between the infants with abnor-malities in the basal ganglia and thosewith standard MR imaging findings. Fur-ther investigations are necessary to de-termine whether fiber abnormalitiescorrelate with neonatal patient out-comes; our patient group was too smallfor us to make such conclusions.
References1. Volpe JJ. Neurology of the newborn. 3rd ed.
Philadelphia, Pa: Saunders, 1995.
2. Sie LT, van der Knaap MS, van Wezel-Meijler G, Valk J. MRI assessment of myeli-nation of motor and sensory pathways in thebrain of preterm and term-born infants.Neuropediatrics 1997;28:97–105.
3. Paus T, Collins DL, Evans AC, Leonard G,Pike B, Zijdenbos A. Maturation of whitematter in the human brain: a review of mag-netic resonance studies. Brain Res Bull 2001;54:255–266.
4. van der Knaap MS, Valk J. MR imaging ofthe various stages of normal myelinationduring the first year of life. Neuroradiology1990;31:459–470.
5. Neil JJ, Shiran SI, McKinstry RC, et al. Nor-mal brain in human newborns: apparent dif-fusion coefficient and diffusion anisotropymeasured by using diffusion tensor MR imag-ing. Radiology 1998;209:57–66.
6. Huppi PS, Maier SE, Peled S, et al. Micro-structural development of human newborncerebral white matter assessed in vivo bydiffusion tensor magnetic resonance imag-ing. Pediatr Res 1998;44:584–590.
7. Neil J, Miller J, Mukherjee P, Huppi PS.Diffusion tensor imaging of normal and in-jured developing human brain: a technicalreview. NMR Biomed 2002;15:543–552.
8. Basser PJ, Mattiello J, LeBihan D. Estima-tion of the effective self-diffusion tensor fromthe NMR spin echo. J Magn Reson B 1994;103:247–254.
9. Mori S, van Zijl PC. Fiber tracking: princi-ples and strategies. NMR Biomed 2002;15:468–480.
10. Basser PJ, Pierpaoli C. Microstructural andphysiological features of tissues elucidatedby quantitative-diffusion-tensor MRI. J MagnReson B 1996;111:209–219.
11. Makris N, Worth AJ, Sorensen AG, et al.Morphometry of in vivo human white matterassociation pathways with diffusion-weightedmagnetic resonance imaging. Ann Neurol1997;42:951–962.
12. Pajevic S, Pierpaoli C. Color schemes to rep-resent the orientation of anisotropic tissuesfrom diffusion tensor data: application towhite matter fiber tract mapping in the hu-man brain. Magn Reson Med 1999;42:526–540.
13. Wakana S, Jiang H, Nagae-Poetscher LM,van Zijl PC, Mori S. Fiber tract-based atlas ofhuman white matter anatomy. Radiology2004;230:77–87.
14. Xue R, van Zijl PC, Crain BJ, Solaiyappan M,Mori S. In vivo three-dimensional recon-struction of rat brain axonal projections bydiffusion tensor imaging. Magn Reson Med1999;42:1123–1127.
15. Conturo TE, Lori NF, Cull TS, et al. Trackingneuronal fiber pathways in the living humanbrain. Proc Natl Acad Sci U S A 1999;96:10422–10427.
16. Jones DK, Simmons A, Williams SC, Hors-field MA. Non-invasive assessment of axonalfiber connectivity in the human brain via dif-fusion tensor MRI. Magn Reson Med 1999;42:37–41.
17. Mukherjee P, Miller JH, Shimony JS, et al.Normal brain maturation during childhood:developmental trends characterized with dif-fusion-tensor MR imaging. Radiology 2001;221:349–358.
18. Zhai G, Lin W, Wilber KP, Gerig G, GilmoreJH. Comparisons of regional white matterdiffusion in healthy neonates and adults per-formed with a 3.0-T head-only MR imagingunit. Radiology 2003;229:673–681.
19. Lee SK, Mori S, Kim DJ, Kim SY, Kim SY,Kim DI. Diffusion tensor MR imaging visual-izes the altered hemispheric fiber connectionin callosal dysgenesis. AJNR Am J Neurora-diol 2004;25:25–28.
20. Glenn OA, Henry RG, Berman JI, et al. DTI-based three-dimensional tractography de-tects differences in the pyramidal tracts ofinfants and children with congenital hemipa-resis. J Magn Reson Imaging 2003;18:641–648.
21. Cowan F. Outcome after intrapartum as-phyxia in term infants. Semin Neonatol2000;5:127–140.
22. Barnett A, Mercuri E, Rutherford M, et al.Neurological and perceptual-motor outcomeat 5–6 years of age in children with neonatalencephalopathy: relationship with neonatalbrain MRI. Neuropediatrics 2002;33:242–248.
23. Amiel-Tison C, Maillard F, Lebrun F, et al.Neurological and physical maturation in nor-mal growth singletons from 37 to 41 weeks’gestation. Early Hum Dev 1999;54:145–156.
24. Jones DK, Horsfield MA, Simmons A. Opti-mal strategies for measuring diffusion inanisotropic systems by magnetic resonanceimaging. Magn Reson Med 1999;42:515–525.
25. Vilanova A, Berenschot G, van Pul C. DTIVisualization with stream surfaces andevenly-spaced volume seeding. Eurograph-ics/IEEE TCVG VisSym 2004; 173–182.
26. Jellison BJ, Field AS, Medow J, Lazar M,Salamat MS, Alexander AL. Diffusion tensorimaging of cerebral white matter: a pictorialreview of physics, fiber tract anatomy, andtumor imaging patterns. AJNR Am J Neuro-radiol 2004;25:356–369.
27. Kier EL, Staib LH, Davis LM, Bronen RA.Anatomic dissection tractography: a newmethod for precise MR localization of whitematter tracts. AJNR Am J Neuroradiol 2004;25:670–676.
TECHNICAL DEVELOPMENTS: Fiber Tracking in Infants van Pul et al
Radiology: Volume 240: Number 1—July 2006 213

28. Kier EL, Staib LH, Davis LM, Bronen RA.MR imaging of the temporal stem: anatomicdissection tractography of the uncinate fas-ciculus, inferior occipitofrontal fasciculus,and Meyer’s loop of the optic radiation.AJNR Am J Neuroradiol 2004;25:677–691.
29. Bahn MM. Comparison of scalar measuresused in magnetic resonance diffusion tensorimaging. J Magn Reson 1999;139:1–7.
30. Talairach J, Tournoux P. Referentially ori-ented cerebral MRI anatomy. Stuttgart,Germany: Thieme Verlag, 1993.
31. Mori S, Kaufmann WE, Davatzikos C, et al.Imaging cortical association tracts in the hu-man brain using diffusion-tensor-based ax-onal tracking. Magn Reson Med 2002;47:215–223.
32. Counsell SJ, Maalouf EF, Fletcher AM, et al.MR imaging assessment of myelination in the
very preterm brain. AJNR Am J Neuroradiol2002;23:872–881.
33. Wieshmann UC, Clark CA, Symms MR,Franconi F, Barker GJ, Shorvon SD. Anisot-ropy of water diffusion in corona radiata andcerebral peduncle in patients with hemipare-sis. Neuroimage 1999;10:225–230.
34. van Pul C, Buijs J, Janssen MJ, Roos GF,Vlaardingerbroek MT, Wijn PF. Selectingthe best index for following the temporalevolution of apparent diffusion coefficientand diffusion anisotropy after hypoxic-ische-mic white matter injury in neonates. AJNRAm J Neuroradiol 2005;26(3):469–481.
35. Scollan DF, Holmes A, Winslow R, ForderJ. Histological validation of myocardial mi-crostructure obtained from diffusion tensormagnetic resonance imaging. Am J Physiol1998;275(6 pt 2):H2308–H2318.
36. Holmes AA, Scollan DF, Winslow RL. Direct
histological validation of diffusion tensorMRI in formaldehyde-fixed myocardium.Magn Reson Med 2000;44:157–161.
37. Tseng WY, Wedeen VJ, Reese TG, SmithRN, Halpern EF. Diffusion tensor MRI ofmyocardial fibers and sheets: correspon-dence with visible cut-face texture. J MagnReson Imaging 2003;17:31–42.
38. Douglas C, Montgomery G. Applied statisticsand probability for engineers. New York,NY: Wiley, 1999.
39. Basser PJ, Pajevic S, Pierpaoli C, Duda J,Aldroubi A. In vivo fiber tractography usingDT-MRI data. Magn Reson Med 2000;44:625–632.
40. Tournier JD, Calamante F, King MD, GadianDG, Connelly A. Limitations and require-ments of diffusion tensor fiber tracking: anassessment using simulations. Magn ResonMed 2002;47:701–708.
TECHNICAL DEVELOPMENTS: Fiber Tracking in Infants van Pul et al
214 Radiology: Volume 240: Number 1—July 2006
View publication statsView publication stats