Embed Size (px)
Citation preview
LWW/IYC AS292-03 May 28, 2004 18:49 Char Count= 0
Infants and Young ChildrenVol. 17, No. 3, pp. 223–235c© 2004 Lippincott Williams & Wilkins, Inc.
Understanding the Emergenceof Behavior Problems in YoungChildren With DevelopmentalDelays
Keith Crnic, PhD; Casey Hoffman, PhD; Catherine Gaze, PhD;Craig Edelbrock, PhD
Children with developmental delays have a much higher incidence of behavior problems than dochildren who are typically developing. This article reviews the current research on the occurrenceand nature of behavior problems in these children, with particular attention to issues relevant toyoung children and the type and severity of problems that have been observed at ages as youngas 2 years. Evidence in support of a conceptual framework for understanding how such behaviorproblems may develop is presented, with a particular focus on early biological or constitutionalfactors, family stress, and children’s developing self-regulatory capacities. Implications for practiceare discussed. Key words: behavior problems, developmental delay, families, self-regulation
IN RECENT YEARS, there has been a gooddeal of attention focused on the occurrence
of behavior problems in older children andadolescents with developmental disabilities,including those with mental retardation. Fromthis work, there have emerged strong indica-tions that children with developmental prob-lems may have up to 4 times the likelihood ofhaving a concurrent mental health diagnosiscompared with children who are typically de-veloping (Baker, Blacher, Crnic, & Edelbrock,2002; Pfeiffer & Baker, 1994). Despite this ac-cruing knowledge in older children, there isvery little known about the presence of be-havior problems in young children with devel-
From the Penn State University, University Park, Pa.
This work was supported in part by grant #HD34879from the National Institute of Child Health and HumanDevelopment, and addresses efforts of the CollaborativeFamily Study (Keith Crnic, principal investigator; andDrs Bruce Baker, Jan Blacher, and Craig Edelbrock, coin-vestigators).
Corresponding author: Keith Crnic, PhD, Departmentof Psychology, 417 Moore Bldg, Penn State University,University Park, PA 16802 (e-mail: [email protected]).
opmental (cognitive) delays, and how theseproblems emerge during the early childhoodperiod.
The co-occurrence of mental retardationand mental health problems is often referredto as “dual diagnosis,” and it is only withinthe past 2 decades that concerns associatedwith dual diagnosis have developed withinthe field (Borthwick-Duffy, 1994; Matson &Frame, 1986). For many years, clinicians didnot specifically attend to the variety of symp-toms of psychopathology in persons withmental retardation or in young children withdevelopmental delays. In all likelihood, thislack of attention was the result of “diagnosticovershadowing,” a process in which deficitsrelated primarily to intellectual limitationsdominated clinical concerns, and the symp-toms consistent with criteria for psychologi-cal disorders were often considered to be afunction of the intellectual deficit rather thanindicative of another diagnosis (Borthwick-Duffy, 1994). The concept of dual diagnosis,however, avoids labeling either the develop-mental disability or the psychological disor-der as primary, and reflects the belief that thediagnoses are distinct and equally important
223
LWW/IYC AS292-03 May 28, 2004 18:49 Char Count= 0
224 INFANTS AND YOUNG CHILDREN/JULY–SEPTEMBER 2004
to recognize for treatment (Pfeiffer & Baker,1994).
In this article, we review the current statusof research on behavior problems in childrenwith early developmental delays or disabili-ties. We then consider a model that attemptsto explain the emergence of behavior prob-lems in these children, and discuss evidencein support of the major constructs involved.Finally, we consider the implications of theseissues for practice.
BEHAVIOR PROBLEMS AND EARLYDEVELOPMENTAL DELAY
General considerations in dual diagnosis
Before addressing how behavior problemsmay develop in young children with devel-opmental delays, it is useful to provide somebackground on the key issues associated withbehavior problems in children and adoles-cents with developmental delays that set thestage for understanding how such problemsmay develop. Prevalence in the population aswell as the descriptive data on the types ofbehavior disorders typically associated withdevelopmental delay are especially importantconcerns for clinicians with interests in thispopulation of children. The prevalence ofpsychopathology reported in the literaturevaries considerably, ranging from low esti-mates of less than 10% to high estimates ofmore than 80% across age groups (Borthwick-Duffy, 1994; Nezu, Nezu, & Gill-Weiss, 1992).Not only is there a wide range in the estimatesof the numbers of individuals who might bedually diagnosed, but research also indicatesthat there is a wide range in the types ofpsychological disorders that may be present(Dykens, 2000; Jacobson, 1990).
The disparate prevalence estimates re-ported in the literature can be traced to sev-eral factors (for review see Borthwick-Duffy,1994). Perhaps the most important consid-eration is that the classification of mentalretardation or developmental delay across re-search studies varies widely. Typically, defi-nitions of mental retardation or meaningful
developmental delay include scores on stan-dardized cognitive assessments that reflect 2or more standard deviations below the meanas well as deficits in adaptive behavior. Al-though more recent research studies use bothcriteria, some studies use only the standard-ized cognitive criterion. To further compli-cate matters, basic definitions of mental retar-dation and developmental delay have changedover time, as have definitions or classificationsystems for psychopathology.
Across the childhood period, research indi-cates that the presence of behavior problemsin children with developmental problems issubstantial. For example, Jacobson (1990) re-ported a prevalence of 40% in children aged 5to 17 years, with a wide range of diagnosesapparent. In a study of children with men-tal retardation and epilepsy, Steffenburg, Gill-berg, and Steffenburg (1996) also found highrates of psychiatric diagnoses. Within the pop-ulation of children diagnosed with mild men-tal retardation, the most common diagnoseswere autism and autism-like disorders. Eigh-teen percent of the children with mild men-tal retardation were diagnosed with attention-deficit hyperactivity disorder (ADHD).
A recent epidemiological study of psy-chopathology in children with cognitive de-lays (Stromme & Diseth, 2000) identified allof the children born within a 5-year periodin a county in Norway who met criteria formental retardation. The presence of a psy-chiatric diagnosis was evaluated based on asemi-structured interview with the parentsand a clinical child interview, both of whichwere modeled on the International Statisti-cal Classification of Diseases, 10th Revisionclassification system. Psychiatric diagnosiswas then classified as either comorbid fea-tures of the developmental disorder or a pre-dominant psychiatric disorder. Stromme andDiseth found that overall 37% of the samplemet criteria for psychiatric disorders. The vastmajority of these diagnoses (74%) were con-sidered comorbid to the syndrome, while theremaining were considered predominantlypsychiatric in origin. Of those that werepsychiatric, the problems were evenly split

LWW/IYC AS292-03 May 28, 2004 18:49 Char Count= 0
Behavior Problems in Young Children With Developmental Delays 225
between autism and hyperkinesis (ADHD),corroborating the findings of Steffenburget al. (1996). It seems apparent from thesegeneral studies across childhood that behav-ior problems in this population are a majorconcern. Yet, few of these studies specificallyaddressed the issues with young children, andit is likely that behavior problems may emergeearlier than school age.
Young children with developmentaldelays
Given the rate of psychopathology in olderpopulations of people with mental retarda-tion, research has begun to explore the riskand protective factors associated with thedevelopment of dual diagnosis. To this end,young children identified as developmentallydelayed or at risk for developmental delayhave been studied. In one such study, Bakeret al. (2002) reported an increased rate ofbehavior problems in children with develop-mental delays as compared to typically de-veloping children at 3 years of age. Childrenwere classified as having a developmental de-lay based on a score of less than 70 on the Bay-ley Scales of Infant Development. Twenty-sixpercent of the developmentally delayed chil-dren in this sample were reported by their par-ents to be in the clinical range for externaliz-ing problems on the Child Behavior Checklist(CBCL). In contrast, only 8% of the typicallydeveloping children scored in this range, in-dicating that children with developmental de-lays were 3 times as likely to be in the clini-cal range for problem behaviors as early as age3 years. When problem behaviors were againassessed 1 year later, children with devel-opmental delays showed significantly moreproblem behaviors at age 4 years, and greaterstability of problem behaviors than did typi-cally developing children (Baker et al., 2003).
Studying even younger children, Feldman,Hancock, Rielly, Minnes, and Cairns (2000) as-sessed problem behaviors in 2-year-olds iden-tified as developmentally delayed or at risk fordevelopmental delays. Not all of these chil-dren had been formally diagnosed, but allwere referred by agencies working with chil-
dren with delays. Forty-two percent of par-ents reported some problem behaviors and25% of the parents rated their children withinthe clinical range for behavior problems. Ofinterest, however, was the fact that this per-centage was not significantly different thanthat reported in the normative sample of typ-ically developing children. Although the per-centage of children rated in the clinical rangefor broadband externalizing and internalizingproblems was not elevated for the develop-mentally delayed sample, the 6 narrowbandsubscales of the CBCL were elevated. Theauthors suggested that children with devel-opmental delays may show elevated risk forproblem behaviors as young as 2 years, butthat these problems are not sufficient to cre-ate more generalized externalizing or inter-nalizing disorder. Nonetheless, Feldman et al.(2000) concluded that the relationship be-tween delay and problem behaviors mightdevelop over time as the child’s interactionsbecome more dependent on communicationwith others.
Preschool-age children identified as devel-opmentally delayed have also been foundto evidence greater problem behaviors andgreater social skills deficits than their typi-cally developing peers as rated by either a par-ent or teacher (Merrell & Holland, 1997). Itis important to note, however, that develop-mental delay in this study was a broad cate-gory that was not based on a formal assess-ment and included social-emotional delaysas well as cognitive delays. Despite the prob-lematic heterogeneity in the sample, thisstudy adds to the growing base of evidencethat suggests that children with early de-velopmental delays show indications of sig-nificant behavior and social skill problemsas early as the preschool years. Guralnick(1999) further presents a cogent discussionof the difficulties often found in peer-relatedsocial competencies of children with earlydevelopmental delays. Across multiple stud-ies, Guralnick has shown that children withdevelopmental delays engage in less inter-active and more solitary play (Guralnick &Groom, 1987), are more negative and difficult

LWW/IYC AS292-03 May 28, 2004 18:49 Char Count= 0
226 INFANTS AND YOUNG CHILDREN/JULY–SEPTEMBER 2004
when conflicts with peers arise (Guralnicket al., 1998), and are less successful in gainingpositive peer response (Guralnick, Connor,Hammond, Gottman, & Kinnish, 1996). Suchproblems in peer social competencies are as-sociated with adjustment difficulties for thesechildren (Guralnick, 1999).
It seems apparent that the degree of de-velopmental delay is also an important con-sideration in the types of behavior problemsthat children have. In a review of preschool-ers’ records from an inpatient unit (Johnson,Lubetsky, & Sacco, 1995), child diagnoseswere compared across a range of intellec-tual functioning. Sixty percent of the totalsample met criteria for mental retardation.Comparing children across a range of intel-lectual functioning, those children classifiedin the borderline and mild mental retardationgroup were more likely to be diagnosed withADHD or oppositional defiant disorder, whilechildren in the lower range of intellectualfunctioning were most likely to be diagnosedwith stereotypies. The authors attribute someof the difference in diagnosis rates to thenature of oppositional behavior, which re-quires a higher degree of cognitive function-ing. Stereotypic behavior, in contrast, requiresno higher order cognitive planning and there-fore is more likely to be associated withmore severe cognitive deficit in younger chil-dren. Other studies as well offer support thathigher rates of behavior problems are foundin children with more mild than severe de-lays, and the most typical behavior problemsfound are conduct disorders, anxiety disor-ders, and ADHD (Borthwick-Duffy & Eyman,1990; Grizenko, Cvejic, Vida, & Sayegh, 1991;Jacobson, 1990). Despite this evidence, find-ings that greater behavior problems are associ-ated with milder rather than more severe de-velopmental deficits are not uniform (Koller,Richardson, Katz, & McLaren, 1983; Myers,1987). However, the research that suggeststhat behavior problems increase with more se-vere developmental deficits typically includedata from adults with mental retardation and,therefore, are less directly relevant to consid-erations with young children.
Related to issues of specificity in degree ofdelay, questions are beginning to be raised re-garding the specificity of type of developmen-tal delay, particularly when the type involvessome biopathological origin. As discussed ear-lier, Stromme and Diseth (2000) addressedthis distinction when they differentiated psy-chopathology that was considered comorbidto the child’s developmental delay from thatwhich reflected a dominant psychopathology.Chadwick, Piroth, Walker, Bernard, and Taylor(2000) recently reported on risk factors for be-havior problems in children with low intellec-tual functioning assessed using the Vinelandscreener. They found that both age and am-bulation were important correlates. Youngerdelayed children had somewhat more severeproblems, whereas ambulation was related tothe types, but not severity of behavior prob-lems reported. Children with lower levels offunctioning (more organic in origin) weremore likely to show destructive behavior,overactivity, self-injury, and sleeping difficul-ties, whereas physical aggression, attention-seeking behavior, and temper tantrums werenot related to level of functioning. Generalself-help skills deficits were found to be as re-lated to the development of behavior prob-lems as were communication deficits in thesechildren. What is intriguing is that neither sexof child nor socioeconomic status proved tobe significant risk factors, leading Chadwicket al. (2000) to conclude that for childrenwith intellectual delay, the neurological dam-age and severity of basic skills deficits maywell override the effects of other risk factorstypically found children with no developmen-tal delays. It is difficult to discount the biolog-ical component in the emergence of behav-ior problems in young children, and it shouldnot be discounted. However, it is interestingthat those children with less delay, and there-fore less clear organicity, are often the chil-dren with more behavior problems.
Behavioral phenotypes
Recently, Dykens and Hodapp have sug-gested that the risk of psychopathology forchildren with developmental delays is best

LWW/IYC AS292-03 May 28, 2004 18:49 Char Count= 0
Behavior Problems in Young Children With Developmental Delays 227
understood by distinguishing among specificsyndromes, rather than by treating childrenwith developmental delay as a heterogeneousgroup (Dykens, 2000; Dykens & Hodapp,1997). Their research has shown that dif-ferent psychiatric disorders are more preva-lent with certain syndromes. For example,boys with fragile X syndrome are at increasedrisk for social anxiety, autism/pervasive de-velopmental disorder, hyperactivity, and inat-tention, whereas girls with this disorder ap-pear to be at increased risk for depression.In contrast, children with Down syndromehave a lower rate of comorbid psychopathol-ogy relative to children with undifferentiateddevelopmental delays. Chadwick et al. (2000)likewise found that children with Down syn-drome showed less severe behavior problems.Although the rates are lower, children withDown syndrome who do meet criteria fora psychiatric disorder are most often diag-nosed with ADHD, oppositional, and anxi-ety disorders—problems which are similar tothose in the population of young delayed chil-dren overall. Although the behavior problemsfor children with specific syndromes oftenoverlap, suggesting that the behavioral phe-notypes lack specificity, Dykens and Hodapp(1997) do note that distinguishing among thesyndromes can be an important guide to treat-ment interventions that are tailored to specificchildren and their disability, and that clini-cians need to take note of specific syndromes.
Summary of behavior problems status
It seems clear that children with devel-opmental disabilities have a greater risk forbehavior problems than do children who aretypically developing, and children with milddelays are at somewhat greater risk over-all. The full range of behavior disorders maybe found in these children, and even youngchildren show an array of difficulties thatinclude oppositionality, anxiety, ADHD, andpoor peer-related social competencies. Chil-dren with mild delays appear to be at great-est risk, as these children have the cognitiveabilities to avail themselves of wider behaviorchoices, and individual differences in children
remain important in determining the degreeand extent of the behavior problems that sur-face. Although behavioral patterns character-istic of children with specific syndromes aregrowing in their popularity as explanations ofproblematic behavior, there are still a num-ber of exogenous and endogenous factors thatmay be critical to the emergence of behav-ior problems early in children’s lives. Chiefamong these factors are family functioningand newly emerging notions regarding chil-dren’s regulatory competencies.
FAMILY PROCESSES AND THEEMERGENCE OF BEHAVIOR PROBLEMS
Given the significance of dual diagnosis as aclinical problem, the identification of risk fac-tors for the emergence of behavior problemsin children with developmental delays is ofclear importance. In delineating these risk fac-tors, both endogenous and exogenous factorswould appear to be crucial considerations. En-dogenous factors are those that reflect char-acteristics of the child and the developmentaldisorder itself (eg, temperament, neurobiolog-ical deficits associated with cognitive delay).Exogenous factors are those that represent in-fluences external to the child, such as relatedfamily stress and constrained social networksand support systems. Despite the fact that re-search has continued to focus on single factorexplanations of primary causal significance,current conceptualizations of dual diagnosisare beginning to acknowledge the complexinteractive role that both exogenous and en-dogenous factors are likely to play.
The emergence of behavior problems inyoung children with developmental delays re-flects an intricate transaction of factors merg-ing across time. These factors likely includethe endogenous indices of children’s bio-logic condition that creates the developmen-tal disability itself, and the child’s tempera-mental reactivity. Exogenous factors of familyfunctioning and parent-child relationships arealso key determinants across time. Endoge-nous and exogenous factors combine to affect
LWW/IYC AS292-03 May 28, 2004 18:49 Char Count= 0
228 INFANTS AND YOUNG CHILDREN/JULY–SEPTEMBER 2004
children’s ability to regulate their behaviorin the face of social and emotional chal-lenge or ambiguity. Given decreased cogni-tive capacities, these young children strug-gle to adapt to the demands of emotionallyand behaviorally challenging events, and therisk for behavior problems increases. Thesecritical self-regulatory abilities include bothemotional and behavioral facets (Eisenberg &Fabes, 1992). Emotion regulation involves ex-trinsic and intrinsic management of the inten-sive and temporal features of emotional ex-pressiveness and arousal, whereas behaviorregulation refers to the adoption and internal-ization of a set of standards to manage one’sbehavior (Kopp, 1992).
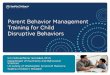
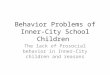
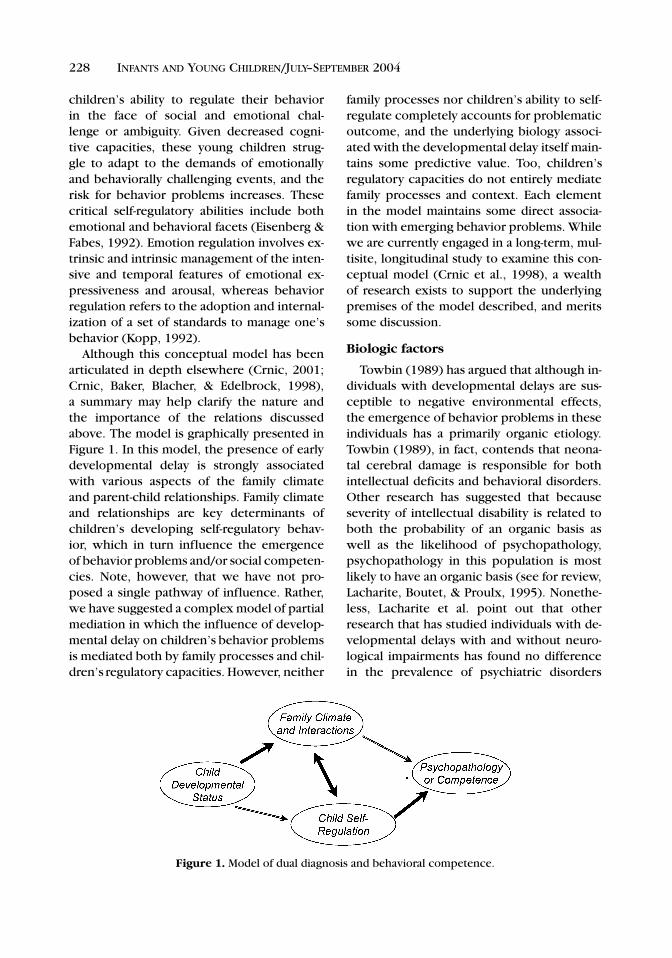
Although this conceptual model has beenarticulated in depth elsewhere (Crnic, 2001;Crnic, Baker, Blacher, & Edelbrock, 1998),a summary may help clarify the nature andthe importance of the relations discussedabove. The model is graphically presented inFigure 1. In this model, the presence of earlydevelopmental delay is strongly associatedwith various aspects of the family climateand parent-child relationships. Family climateand relationships are key determinants ofchildren’s developing self-regulatory behav-ior, which in turn influence the emergenceof behavior problems and/or social competen-cies. Note, however, that we have not pro-posed a single pathway of influence. Rather,we have suggested a complex model of partialmediation in which the influence of develop-mental delay on children’s behavior problemsis mediated both by family processes and chil-dren’s regulatory capacities. However, neither
Figure 1. Model of dual diagnosis and behavioral competence.
family processes nor children’s ability to self-regulate completely accounts for problematicoutcome, and the underlying biology associ-ated with the developmental delay itself main-tains some predictive value. Too, children’sregulatory capacities do not entirely mediatefamily processes and context. Each elementin the model maintains some direct associa-tion with emerging behavior problems. Whilewe are currently engaged in a long-term, mul-tisite, longitudinal study to examine this con-ceptual model (Crnic et al., 1998), a wealthof research exists to support the underlyingpremises of the model described, and meritssome discussion.
Biologic factors
Towbin (1989) has argued that although in-dividuals with developmental delays are sus-ceptible to negative environmental effects,the emergence of behavior problems in theseindividuals has a primarily organic etiology.Towbin (1989), in fact, contends that neona-tal cerebral damage is responsible for bothintellectual deficits and behavioral disorders.Other research has suggested that becauseseverity of intellectual disability is related toboth the probability of an organic basis aswell as the likelihood of psychopathology,psychopathology in this population is mostlikely to have an organic basis (see for review,Lacharite, Boutet, & Proulx, 1995). Nonethe-less, Lacharite et al. point out that otherresearch that has studied individuals with de-velopmental delays with and without neuro-logical impairments has found no differencein the prevalence of psychiatric disorders

LWW/IYC AS292-03 May 28, 2004 18:49 Char Count= 0
Behavior Problems in Young Children With Developmental Delays 229
between the two groups. At this point, the fullcontribution of expressly biological explana-tions is unclear. Certainly, the work of Dykensand Hodapp (1997), identifying specific be-havioral phenotypes of specific syndromes,suggests that underlying biological factors areimportant, but they do not tell the full story.
Beyond the expressly biologic factors,other endogenous factors have received at-tention as potential risk factors for the emer-gence of psychopathology, including childtemperament. Although the vast majority ofresearch on temperament has focused on chil-dren without developmental delays, Chessand Korn (1970) found that children with de-velopmental delays who had certain temper-ament profiles characteristic of a more “diffi-cult” temperament were much more likely toexhibit behavior problems than those with an“easy” temperament. Difficult temperaments,for example, might reflect characteristics inwhich children are less adaptive, more emo-tionally intense, and less sociable. However,in studies where temperament is thought toplay a key role in the emergence of psy-chopathology, temperament is not generallythought to exert its influence directly. Rather,temperament is thought to affect behaviorproblems indirectly through its influence onother exogenous factors, such as the interac-tions between the child and his environment.Specifically, temperamental styles during earlychildhood are thought to help shape interac-tions within the family system, such that chil-dren with more difficult temperamental stylespose greater challenges to parenting. In casesfor which parenting is already compromised,as is sometimes the case for young childrenwith developmental delays, interactions be-tween a child with a difficult temperamentand parents who lack effective parenting skillsare more likely to be characterized by acoercive pattern that can contribute to the de-velopment of childhood aggression and psy-chopathology (Patterson, 1986).
Parent-child interactions
Research examining parent-child interac-tions in families with children with devel-
opmental delays has noted that these chil-dren pose unique parenting challenges thatinclude intensified behavioral management is-sues (Baker, Blacher, Kopp, & Kraemer, 1997).Given that these increased demands on par-enting may overtax parenting resources andleave parents feeling ineffective, one mightexpect that, over time, coercive exchangeslike those described above might ensue.These exchanges might then predispose chil-dren with developmental delays to developbehavioral disorders, resulting in the greaterprevalence of behavioral disorders among thisgroup of children than in the general popu-lation. Floyd and Phillippe (1993) tested thisassumption, noting that children with devel-opmental delays have been shown to be lesscompliant and, therefore, pose a greater chal-lenge to parents’ behavior management skillsthan do children without these delays. Theyfound that, although the children with devel-opmental delays had significantly higher be-havior problem scores than children withoutdelays, there were no significant differencesin the rate of coercive exchanges in the twogroups of families. Parents of children withdelays were found to issue more commandsduring behavior management; however, theseparents were also more likely than parents ofchildren without delays to deliver a clear di-rective rather than a vague request. Floyd andPhillippe interpret these results as indicatingthat although children with mental retarda-tion pose greater challenges to parents’ behav-ior management skills, these parents are ableto provide needed directives without fallinginto a coercive pattern of interaction. A laterstudy of family problem solving again foundthat although parents had to make use of agreater number of directives to manage thebehavior of children with delays, they did notfall into greater aversive behaviors than didparents in the comparison group (Costigan,Floyd, Harter, & McClintock, 1997).
One possible explanation for the absenceof coercive processes, despite the presence ofincreased behavior problems in families ofchildren with delays, may be taken from theresults of a study by Floyd and Zmich (1991).

LWW/IYC AS292-03 May 28, 2004 18:49 Char Count= 0
230 INFANTS AND YOUNG CHILDREN/JULY–SEPTEMBER 2004
These investigators found a relation betweenpoor perceived parenting skill and increasedbehavior problems among the comparisonfamilies, but not among those with a childwith developmental delays. Floyd and Zmich(1991) subsequently reason that parents ofchildren with developmental delays may bemore likely to view behavior problems as re-lated to endogenous child factors than parent-ing failures because they expect their childrento display negative behaviors related to theirdisability. On the other hand, they also ex-plain that parents of the nondelayed childrenmay view these behaviors as unexpected andabnormal, and, therefore, may be more likelyto attribute them to failures in parenting skillthan to child factors.
Family stress
Despite the apparent resiliency in avoid-ing coercive behavior exchanges in the faceof greater behavior management challenges,families of young children with developmen-tal delay evidence other potential risk fac-tors. For example, research has consistentlydemonstrated that families of children withdevelopmental delays experience heightenedlevels of stress, particularly related to childrearing, which is not surprising consideringthe unique challenges these children presentto parents (Crnic, Friedrich, & Greenberg,1983). Certainly, it has been well establishedthat stress is related to behavior problemsin both developmentally delayed and nonde-layed samples of young preschool children(Baker & Heller, 1996). Research has also in-dicated that parenting stress is an importantpredictor of children’s behavior problems re-gardless of cognitive functioning (Crnic &Greenberg, 1990; Heller, Baker, Henker, &Hinshaw, 1996). However, given the typicallyhigher levels of stress in families of childrenwith developmental delays, stress can be ex-pected to play an especially significant rolein emerging behavior problems. For exam-ple, Baker et al. (2002) reported corroborat-ing evidence that parents of children with de-velopmental delays were more stressed thanparents of children without delays. But Baker
et al. also reported that in predicting parentstress in parents of children with developmen-tal delays, child behavior problems accountedfor significantly more of the variance than thechildren’s level of cognitive functioning. Fur-ther, cognitive functioning contributed non-meaningfully when behavior problems wereentered first in regression analyses, implyingthat behavior problems rather than cognitivelevel per se play the key role in parents’ stresslevels. A second study by Baker et al. (2003)examined the relations between parentingstress and behavior problems over time in fam-ilies with children with developmental delays.This study attempted to delineate the direc-tion of effect in the relations between behav-ior problems and parenting stress in familiesof children with early developmental delays.They found that behavior problems were bothpredictive of and predicted by parents’ stress,indicating that the higher instance of behav-ior problems in children with early develop-mental delays may be functionally related toearly family stress and subsequently be associ-ated with higher levels of family stress at laterperiods. This suggests that the developmentof behavior problems in children with earlydevelopmental delays is likely the result of acomplex transactional process that includeschild characteristics that challenge parents aswell as factors that can compromise parent-ing, thereby adversely affecting children’s be-havior (Crnic, 2001).
Child regulatory ability
Given that both child and family character-istics are likely to influence the emergence ofpsychopathology in children with and with-out developmental delays, a crucial questionarises: How do these various endogenous andexogenous factors together affect the devel-opment of disordered behavior? One possi-ble connector involves the important role thatself-regulation, and especially emotion regula-tion processes, plays in relation to the emer-gence of psychopathology or competence inchildren (Cole, Michel, & Teti, 1994). Bothchild and family factors play key roles in thedevelopment of children’s emotion regulation
LWW/IYC AS292-03 May 28, 2004 18:49 Char Count= 0
Behavior Problems in Young Children With Developmental Delays 231
abilities (Brenner & Salovey, 1997; Calkins,1994). Although there are multiple perspec-tives on emotion regulation, and the constructis somewhat controversial, Cole et al. (1994)define emotion regulation as an individual’sability to respond to the ongoing demands ofdaily experiences with a range of emotionsthat are socially tolerable and sufficiently flex-ible to allow or inhibit spontaneous reactions.Cole et al. note that these abilities are im-portant to success in a wide range of devel-opmental tasks, such as being able to copewith frustration, maintain interest in learn-ing, and adaptively engage in social relationswith others. By contrast, emotion dysregula-tion would occur when established emotionalpatterns interfere with adaptive functioningacross these domains. Cole et al. describedysregulated emotional patterns as providingthe basis for the development of disorder interms of overregulated or underregulated be-havior. Effective, as opposed to deficient, reg-ulatory abilities are likely to have importantconsequences for psychological functioning,especially given the consistency of an indi-vidual’s patterns of emotion regulation overtime (Murphy, Eisenberg, Fabes, Shepard, &Guthrie, 1999).
The ability to regulate one’s own emotionsdevelops as a function of both an infant’s ownabilities to self-regulate, as well as the abili-ties of the caregiver to recognize the infant’sneeds for assistance with regulatory func-tions (Brenner & Salovey, 1997; Calkins, 1994;Shaw, Keenan, Vondra, Delliquadri, & Giovan-nelli, 1997). Calkins (1994) points out thatopposing parenting styles, such as responsiveversus insensitive and accepting versus ne-glecting parenting, are likely to interact withchildren’s behavior traits, such as adaptabilityversus reactivity, in order to promote or inter-fere with the development of emotion regula-tion abilities. When a caregiver is insensitiveor unresponsive to an infant’s needs, the in-fant’s emotional state is likely to become dys-regulated. Under these circumstances, the in-fant is obligated to devote coping resources toregulating negative affect, which limits the re-sources available to support the achievement
of important developmental goals (Weinberg& Tronick, 1998). In addition, infants may beso reactive to their environments that theircaregivers are unable to be responsive to allof their distress, creating a greater regulationchallenge for parents (Calkins, 1994).
Given the importance of both child andfamily factors in the development of emotionregulation competencies, children with de-velopmental delays may be particularly sus-ceptible to emotion regulation deficits for avariety of reasons. First, parents of childrenwith developmental delays who are experi-encing heightened levels of stress may be lessavailable to aid in regulatory concerns. Sec-ond, intellectual deficits are likely to interferewith the acquisition of emotion regulationabilities. For example, Brenner and Salovey(1997) point out that children use emotionalknowledge to help them with emotion reg-ulation, including the ability to talk aboutemotions, determine others’ emotional states,describe the experience of simultaneous emo-tions, and internalize cultural rules aboutemotional expressiveness. Clearly, childrenwith compromised cognitive abilities wouldbe more likely to experience difficulties withthese tasks. Calkins (1994) also lists cogni-tive components such as the development ofinternal working models, the awareness ofthe need for regulation, and the ability to ap-ply strategies as important sources of individ-ual differences in emotion regulation abilities.Further, Brenner and Salovey (1997) describethe progression of emotion regulation strate-gies as moving from reliance on purely behav-ioral strategies toward the use of more cogni-tive strategies, such as cognitive distraction,which may not be as readily available to in-dividuals with developmental delays. Brennerand Salovey also point out that children’s abil-ity to regulate emotions without assistance im-proves with age, which may be a much slowerprocess for young children with developmen-tal delays who may acquire these abilities atmuch slower rates or rely on different strate-gies altogether.
Few studies have examined emotion regula-tion difficulty in children with developmental

LWW/IYC AS292-03 May 28, 2004 18:49 Char Count= 0
232 INFANTS AND YOUNG CHILDREN/JULY–SEPTEMBER 2004
delays, and its potential role in the emergenceof dual diagnosis. In the only study to date,Wilson (1999) examined social entry behav-iors in children with and without develop-mental delays and found that the delayed chil-dren utilized less effective emotion regulationstrategies to cope with entry failure. This im-portant, yet limited study is suggestive; how-ever, more research is needed to assess therole that emotion regulation plays in the de-velopment of behavior problems in childrenwith developmental delays. Further, researchneeds to address how specific child and par-ent characteristics in families of children withdevelopmental delays interact to support orinhibit the development of effective emotionregulation abilities.
Summary of factors affecting emergingbehavior problems
A wealth of data has established that fam-ilies are affected by and affect their youngchildren with developmental delays. Thesefamilies are more stressed as a rule, and mayengage in interactions that can place theirchild at further risk for developmental prob-lems. Both stress and less positive interactionshave been found to be correlates of behaviorproblems in children regardless of cognitivefunctioning, but clearly create increased riskin children that do have cognitive deficits. Butfamily factors alone do not offer a completeexplanation for the behavior problems, be-cause child characteristics, such as tempera-ment and self-regulatory ability, are likely key,and may in fact mediate the relations betweendevelopmental delay, family functioning, andthe emergence of behavior problems duringearly childhood.
It is critical to note that the presence ofearly developmental delay is not a sentence topoorer outcomes across the various domainsthat have been discussed. Many children andfamilies have resiliencies that have been welldocumented in the literature and the fieldhas thankfully moved beyond the pathologi-cal models that so dominated thinking priorto the 1980s. However, it is important to beaware that the greater risk for behavior prob-
lems in children with developmental delaysis real and substantial. These behavior prob-lems are not first apparent in adolescenceor adulthood for persons with developmen-tal disabilities, or even during middle child-hood. Rather, problems are apparent as youngas age 2 and 3, and the factors associated withthe emergence of these problems must be ad-dressed at this early childhood period. Why isthis critical? Because these behavior problemshave important clinical costs. In the extreme,Blacher, Hanneman, and Rousey (1992) havenoted that behavior problems are the majorreason that families place their children withdevelopmental disabilities out of home.
IMPLICATIONS FOR PRACTICE
The review and discussion provided abovesuggests that there is a need for practitionersto be aware that behavior problems are rela-tively common in young children with earlydevelopmental delays, even though suchproblems are not ubiquitous. When childrenwith early developmental delays are identi-fied, the potential for dual conditions (devel-opmental delay and behavior disorder) shouldbe a priority concern of professionals, and at-tention to children’s behavioral status as wellas their specific developmental/cognitivefunctioning should be the key foci ofassessment.
Attention to the emergence of behaviorproblems in children with early developmen-tal delays requires that professionals specif-ically address issues of family functioning,parent-child interactions, as well as chil-dren’s temperamental functioning and emerg-ing self-regulatory capacities. Each of thesefactors appears to represent important factorsthat contribute to mental health outcomes forthese children, especially during the criticalinfancy and preschool period. In particular,the degree to which families are stressed re-quires attention, as stress is more common infamilies in which there is a child with a devel-opmental delay. Family and parenting stressesare major predictors of subsequent adjust-ment difficulties for children (Crnic & Low,

LWW/IYC AS292-03 May 28, 2004 18:49 Char Count= 0
Behavior Problems in Young Children With Developmental Delays 233
2002), and stress typically serves as a changeagent within families creating problematic cir-cumstance. Families under stress require cop-ing resources, such as social supports andfacilitated access to appropriate services, tohelp prevent the kinds of changes that leadto adjustment problems in the children. Like-wise, helping parents focus on the major in-teraction qualities that promote healthy ad-justment is key. Sensitivity and positivity ininteractions facilitate adjustment, whereas in-trusiveness and negativity tend to be rou-tinely associated with more problematicdevelopment. Parental directiveness is some-times considered detrimental for typically de-veloping children, but may be helpful for chil-dren with developmental delays and may not
reflect an insensitive approach to buildingrelationships (Marfo, 1992). Further, facilitat-ing appropriate parent-child interaction willhelp support the emergence of stronger self-regulatory skills in young children with de-velopmental delays, which should prove espe-cially helpful in minimizing problem behaviorin these children. It is critical to again cautionthat risk is not reality, and many children withearly developmental delays do not evidencethe kinds of behavior problems that have beendiscussed above. Nonetheless, it is imperativefor professionals to be aware of the risks, at-tend to the various family and child consider-ations raised, and make appropriate referralsfor specialized psychological services whenconcerns are present.
REFERENCES
Baker, B. L., Blacher, J., Crnic, K., & Edelbrock, C. (2002).Behavior problems and parenting stress in families ofthree-year old children with and without developmen-tal delays. American Journal on Mental Retardation,107, 433–444.
Baker, B. L., Blacher, J., Kopp, C. B., & Kraemer, B. (1997).Parenting children with mental retardation. Interna-tional Review of Research in Mental Retardation,20, 1–45.
Baker, B. L., & Heller, T. L. (1996). Preschool childrenwith externalizing behaviors: Experience of fathersand mothers. Journal of Abnormal Child Psychology,24, 513–532.
Baker, B. L., McIntyre, L. L., Blacher, J. B., Crnic, K., Edel-brock, C., & Low, C. (2003). Preschool children withand without developmental delay: Behavior problemsand parenting stress over time. Journal of IntellectualDisability Research, 47, 217–230.
Blacher, J., Hanneman, R., & Rousey, A. M. (1992). Out-of-home placement of children with severe handicaps:A comparison of approaches. American Journal onMental Retardation, 96, 607–616.
Borthwick-Duffy, S. (1994). Epidemiology and prevalenceof psychopathology in people with mental retarda-tion. Journal of Consulting and Clinical Psychology,62(1), 17–27.
Borthwick-Duffy, S. A., & Eyman, R. K. (1990). Who arethe dually diagnosed? American Journal on MentalRetardation, 94, 586–595.
Brenner, E. M., & Salovey, P. (1997). Emotion regulationduring childhood: Developmental, interpersonal, andindividual considerations. In P. Salovey & D. J. Sluyter(Eds.), Emotional development and emotional in-
telligence: Educational implications (pp. 168–195).New York: BasicBooks.
Calkins, S. D. (1994). Origins and outcomes of individualdifferences in emotion regulation. Monographs of theSociety for Research in Child Development, 59, 53–72.
Chadwick, O., Piroth, N., Walker, J., Bernard, S., & Tay-lor, E. (2000). Factors affecting the risk of behaviorproblems in children with severe intellectual disabil-ity. Journal of Intellectual Disability Research, 44(2),108–123.
Chess, S., & Korn, S. (1970). Temperament and behaviordisorders in mentally retarded children. Archives ofGeneral Psychiatry, 23, 122–130.
Cole, P. M., Michel, M. K., & Teti, L. O. (1994). The de-velopment of emotion regulation and dysregulation:A clinical perspective. Monographs of the Society for-Research in Child Development, 59, 73–100.
Costigan, C. L., Floyd, F. J., Harter, K. S. M., & McClintock,J. C. (1997). Family process and adaptation to childrenwith mental retardation: Disruption and resilience infamily problem-solving interactions. Journal of Fam-ily Psychology, 11, 515–529.
Crnic, K. (2001, March). Family, emotion, and regu-lation: Process in the emergence of dual diagno-sis. Invited address at the Gatlinburg Conference onMental Retardation and Developmental Disabilities,Charleston, SC.
Crnic, K., Baker, B., Blacher, J., & Edelbrock, C. (1998).Children with MR: Families, processes, and dualdiagnosis. Research Grant (HD34879) funded byNICHD, NIH.
Crnic, K. A., Friedrich, W. N., & Greenberg, M. T. (1983).
LWW/IYC AS292-03 May 28, 2004 18:49 Char Count= 0
234 INFANTS AND YOUNG CHILDREN/JULY–SEPTEMBER 2004
The adaptation of families of mentally retarded chil-dren: A model of stress, coping, and family ecology.American Journal of Mental Deficiency, 88, 125–138.
Crnic, K. A., & Greenberg, M. T. (1990). Minor parentingstresses with young children. Child Development, 61,1628–1637.
Crnic, K. A., & Low, C. (2002). Everyday stresses and par-enting. In M. Bornstein (Ed.), Handbook of parenting(Vol. 4, 2nd ed, pp. 243–268). Hillsdale, NJ: Erlbaum.
Dykens, E. (2000). Psychopathology in children with in-tellectual disability. Journal of Child Psychology andPsychiatry, 41, 407–417.
Dykens, E. M., & Hodapp, R. M. (1997). Treatment is-sues in genetic mental retardation syndromes. Profes-sional Psychology Research and Practice, 28, 263–270.
Eisenberg, N., & Fabes, R. (1992). Emotion, regulation,and the development of social competence. In M. S.Clark (Ed.), Emotion and social behavior: Review ofpersonality and social psychology (Vol. 14, pp. 119–150). Newbury Park, CA: Sage.
Feldman, M., Hancock, C., Rielly, N., Minnes, P., & Cairns,C. (2000). Behavior problems in young children withor at risk for developmental delay. Journal of Childand Family Studies, 9(2), 247–261.
Floyd, F. J., & Phillippe, K. A. (1993). Parental interactionswith children with and without mental retardation:Behavior management, coerciveness, and positive ex-change. American Journal on Mental Retardation,97, 673–684.
Floyd, F. J., & Zmich, D. E. (1991). Marriage and parent-ing partnership: Perceptions and interactions of par-ents with mentally retarded and typically developingchildren. Child Development, 62, 1434–1448.
Grizenko, N., Cvejic, H., Vida, S., & Sayegh, L. (1991). Be-haviour problems in the mentally retarded. CanadianJournal of Psychiatry, 36, 712–717.
Guralnick, M. J. (1999). Family and child influences onthe peer-related social competence of young childrenwith developmental delays. Mental Retardation andDevelopmental Disabilities Research Reviews, 5, 21–29.
Guralnick, M. J., Connor, R., Hammond, M., Gottman,J. M., & Kinnish, K. (1996). Immediate effects of main-stream settings on the social interactions and social in-tegration of preschool children. American Journal ofmental Retardation, 100, 359–377.
Guralnick, M. J., & Groom, J. M. (1987). Dyadic peerinteractions of mildly delayed and non-handicappedpreschool children. American Journal of Mental De-ficiency, 92, 178–193.
Guralnick, M. J., Paul-Brown, D., Groom, J. M., Booth, C.L., Hammond, M. A., Tupper, D. B., et al. (1998). Con-flict resolution patterns of preschool children withand without developmental delays in heterogeneousplaygroups. Early Education and Development, 9,49–77.
Heller, T. L., Baker, B. L., Henker, B., & Hinshaw, S. P.(1996). Externalizing behavior and cognitive function-ing from preschool to first grade: Stability and predic-tors. Journal of Clinical Child Psychology, 25, 376–387.
Jacobson, J. (1990). Do some mental disorders occur lessfrequently among persons with mental retardation?American Journal on Mental Retardation, 94(6),596–602.
Johnson, C., Lubetsy, M., & Sacco, K. (1995). Psy-chiatric and behavioral disorders in hospitalizedpreschoolers with developmental disabilities. Journalof Autism and Developmental Disorders, 25(2), 169–182.
Koller, H., Richardson, S. A., Katz, M., & McLaren, J.(1983). Behavior disturbance since childhood amonga 5-year birth cohort of all mentally retarded youngadults in a city. American Journal on Mental Defi-ciency, 87, 386–395.
Kopp, C. B. (1992). Emotion and its regulation in early de-velopment. New Directions for Child Development,55, 41–56.
Lacharite, C., Boutet, M., & Proulx, R. (1995). Intellectualdisability and psychopathology: Developmental per-spective. Canada’s Mental Health, 43, 2–8.
Marfo, K. (1992). Correlates of maternal directivenesswith children who are developmentally delayed.American Journal of Orthopsychiatry, 62, 219–233.
Matson, J., & Frame, C. (1986). Psychopathology amongmentally retarded children and adolescents. BeverlyHills, CA: Sage.
Merrell, K., & Holland, M. (1997). Social-emotional behav-ior of preschool children with and without develop-mental delays. Research in Developmental Disabili-ties, 18(6), 393–405.
Murphy, B. C., Eisenberg, N., Fabes, R. A., Shepard,S., & Guthrie, I. K. (1999). Consistency and changein children’s emotionality and regulation: A longi-tudinal study. Merrill-Palmer Quarterly, 45, 413–444.
Myers, B. A. (1987). Psychiatric problems in adolescentswith developmental disabilities. Journal of the Amer-ican Academy of Child and Adolescent Psychiatry,26, 74–79.
Nezu, C., Nezu, A., Gill-Weiss, M. (1992). Psychopathol-ogy in persons with mental retardation: Clinicalguidelines for assessment and treatment. Cham-paign, IL: Research Press.
Patterson, G. R. (1986). Performance models for antisocialboys. American Psychologist, 41, 432–444.
Pfeiffer, S., & Baker, B. (1994). Residential treatment forchildren with dual diagnoses of mental retardation andmental disorder. In J. Blacher (Ed.), When there’s noplace like home: Options for children living apartfrom their natural families. Baltimore, MD: Paul H.Brookes.
Shaw, D. S., Keenan, K., Vondra, J. I., Delliquadri, E.,

LWW/IYC AS292-03 May 28, 2004 18:49 Char Count= 0
Behavior Problems in Young Children With Developmental Delays 235
& Giovannelli, J. (1997). Antecedents of preschoolchildren’s internalizing problems: A longitudinal studyof low-income families. Journal of the AmericanAcademy of Child & Adolescent Psychiatry, 36,1760–1767.
Steffenburg, S., Gillberg, C., & Steffenburg, U. (1996).Psychiatric disorders in children and adolescents withmental retardation and active epilepsy. Archives ofNeurology, 53, 904–912.
Stromme, P., & Diseth, T. (2000). Prevalence of psychi-atric diagnoses in children with mental retardation:
Data from a population-based study. DevelopmentalMedicine and Child Neurology, 42, 266–270.
Towbin, A. (1989). Behavior disorders in mentally re-tarded persons, the dually diagnosed: Factors of patho-genesis. Journal of Clinical Psychology, 45, 910–918.
Weinberg, M. K., & Tronick, E. Z. (1998). The impactof maternal psychiatric illness on infant development.Journal of Clinical Psychiatry, 59, 53–61.
Wilson, B. J. (1999). Entry behavior and emotion regula-tion abilities of developmentally delayed boys. Devel-opmental Psychology, 35, 214–222.
Lists of current articles: http://depts.washington.edu/isei/iyc/iyc_comments.html
To view previous articles: http://depts.washington.edu/isei/iyc/iyc_previous.html