Embed Size (px)
Citation preview

LWW/IYC AS237-02 December 4, 2003 11:47 Char Count= 0
Infants and Young ChildrenVol. 17, No. 1, pp. 17–31c© 2004 Lippincott Williams & Wilkins, Inc.
Self-Directed Learning ofChild-Care Skills by ParentsWith Intellectual Disabilities
Maurice A. Feldman, PhD
Children of parents with intellectual disabilities (ID) are at risk for neglectful care due to parent-ing skill deficiencies. This article describes the development, use, and evaluation of self-directedlearning (via self-instructional audiovisual child-care materials) to teach basic child-care, health,and safety skills to parents with ID. We developed the materials based on input from pediatrichealth care professionals and research on how to present visual materials to persons with lowliteracy skills. The parents quickly learned how to use the pictorial manuals and accompanyingaudiocassette. Controlled field studies with 33 parents with ID (30 mothers, 3 fathers) found that96% of the self-trained skills rapidly reached the same level seen in competent parents and main-tained as long as 3.5 years. Consumer satisfaction ratings were uniformly high. Percentage correctperformance was significantly related to the parents’ reading abilities and initial acceptance of thematerials. Overall, the results of these studies indicate that many parents with ID may improvetheir parenting skills with low cost, low tech, self-directed learning. Future research should eval-uate the effects of mass dissemination of the self-instructional materials on the incidence of childneglect related to parental incompetence. Key words: parenting, parent training, parents withintellectual disabilities, self-directed learning
CHILDREN of parents with intellectual dis-abilities (ID)∗ are at risk for neglect-
ful care that leads to health, developmental,and behavioural problems (Feldman, 1997,2002a; Feldman & Walton-Allen, 1997). Mostof these problems can be traced to parent-ing skill deficiencies, rather than purposeful
From the Department of Child and Youth Studies,Brock University, St Catharines, Ontario, Canada.
The research described herein was supported by grantsfrom the Ontario Ministry of Community, Family, andChildren Services and the Ontario Mental Health Foun-dation. I would like to thank the staff and clients ofthe Parent Education Program, Toronto; and Lake RidgeCommunity Support Services, Oshawa, Ontario.
Corresponding author: Maurice A. Feldman, PhD, De-partment of Child and Youth Studies, Brock University,500 Glenridge Ave, St Catharines, Ontario, Canada L2S3A1 (e-mail: [email protected]).
∗In this article, intellectual disability is synonymous withthe DSM-IV definition of mental retardation (AmericanPsychiatric Association, 1994).
abuse or neglect. Many of these parents (whocome to the attention of social service andchild protection agencies) lack critical knowl-edge and skills in providing adequate instru-mental child-care (Feldman, 1998b; Feldman,Case, & Sparks, 1992), a safe home envi-ronment (Barone, Greene, & Lutzker, 1986;Feldman & Case, 1999; Tymchuk, Hamada,Andron, & Anderson, 1990b; Watson-Perczel,Lutzker, Greene, & McGimpsey, 1988), propernutrition (Feldman, Garrick, & Case, 1997;Sarber, Halasz, Messmer, Bickett, & Lutzker,1983), and nurturing interactions (Feldman,Sparks, & Case, 1993; Slater, 1986; Tymchuk &Andron, l992). Parents with ID also have diffi-culties in problem-solving (Tymchuk, Yokota,& Rahbar, 1990), recognizing and treatingmedical emergencies (Feldman & Case, 1999;Tymchuk, Hamada, Andron, & Anderson,1990a), and understanding basic child devel-opment information (Tymchuk, Andron, &Tymchuk, 1990).
Fortunately, many of these problems canbe rectified through parent education and
17

LWW/IYC AS237-02 December 4, 2003 11:47 Char Count= 0
18 INFANTS AND YOUNG CHILDREN/JANUARY–MARCH 2004
supports (Feldman, 1994). Effective parenttraining typically involves frequent (eg,weekly) instruction in the home (or a home-like setting) by specially trained parenteducators. Skills are trained individually bydirect instruction methods including taskanalysis, illustrations, prompting, modelling,feedback, and reinforcement (Feldman,1998b). This training enhances child healthand development and dramatically decreasesthe need for child custody intervention(Feldman et al., 1992, 1993, 1997).
Despite the existence of an evidence-basedparent educational technology for this popu-lation, few specialized programs exist. Manyfamily support and early intervention pro-grams are not equipped to commit to the in-tensive and long-lasting supports these fami-lies require. Workers often do not have theunique (broad) set of knowledge and skillsneeded to effectively function as parent edu-cators. These competencies comprise knowl-edge of child development, health, safety, andnutrition, as well as effective teaching meth-ods for adults with cognitive and literacy limi-tations. In addition, a parent educator shouldbe unbiased, nonjudgmental, empathic, andoffer competency-enhancing support (Espe-Scherwindt & Kerlin, 1990; Feldman, 2002b;Tucker & Johnson, 1989).
COST-EFFECTIVE INTERVENTIONS
More cost-effective and disseminable par-ent education approaches are needed to reachas many of these families as possible to re-duce the incidence of child neglect due toparenting skill deficits. A promising efficientapproach is self-directed learning using spe-cially designed audiovisual materials. Severalstudies have added illustrations to full train-ing packages to function as memory aides inbetween training sessions and after trainingwas completed (Feldman, Case, Garrick, et al.,1992; Feldman et al., 1992, 1997; Sarber et al.,1983; Tymchuk et al., 1990a, 1990b). It oc-curred to us that perhaps inexpensive, easilydistributed audiovisual materials could be de-
signed for independent self-instruction of par-enting skills, thereby eliminating the need forintensive training by specially trained parenteducators (at least for some parents). The ma-terials could remain with the parents, servingas permanent prompts to encourage gener-alization and maintenance of child-care skills(Wacker, Berg, Berrie, & Swatta, 1985). Suc-cessful experiences in self-directed learningmay have the added benefit of promotingparental empowerment, self-confidence, andself-esteem (Christensen & Jacobson, 1994).Before describing the development, use, andevaluation of self-directed child-care trainingfor parents with ID, I will briefly summarizethe literature on self-directed parent trainingfor parents without ID and the use of self-instructional audiovisual materials to teachskills to persons with ID.
Self-directed parent education forparents without ID
Many more people read self-help booksthan seek professional counselling for psycho-logical problems (Christensen & Jacobson,1994) and parenting is no exception; self-help parenting books abound and manybookstores have a dedicated section. Meta-analysis supports the effectiveness of self-administered parent training (Scogin, Bynum,Stephens, & Calhoon, 1990). Instructionalparenting manuals and videotapes have beenshown to be more effective than wait listcontrols, and as effective (and more cost-effective) than therapist-led training for par-ents of children with a variety of issues in-cluding behaviour problems at home and inthe community (Bauman, Reiss, Rogers, &Bailey, 1983, Clark et al., 1977; Connell,Sanders, & Markie-Dadds, 1997; Ergon-Rowe,Ichinose, & Clark, 1991; Sanders, Markie-Dadds, Tully, & Bor, 2000; Webster-Stratton,Kolpacoff, & Hollingsworth, 1988), sleepproblems (Seymour, Brock, During, & Poole,1989), fears (Giebenhain & O’Dell, 1984),enuresis (Besalal, Azrin, Thienes-Hontos, &McMorrow, 1980), and self-care skill deficits(Kashima, Baker, & Landen, 1988).

LWW/IYC AS237-02 December 4, 2003 11:47 Char Count= 0
Self-Directed Learning of Child-Care Skills 19
Self-directed learning for personswith ID
While the use of self-directed approachesfor parents without ID is supported, it isnot clear whether parents with cognitivelimitations would respond as well. Researchshows that persons with ID can learn rela-tively complex repertoires, such as domes-tic (Alberto, Sharpton, Briggs, & Stight, 1986;Wacker et al., 1985), cooking (Johnson &Cuvo, 1981; Robinson-Wilson, 1977), com-puter use (Frank, Wacker, Berg, & McMahon,1985), Internet access (Davies, Stock, &Wehmeyer, 2001), academic (Van Luit &Naglieri, 1999), self-care (Stephan, 1987;Thinesen & Bryan, 1981), and vocational skills(Agran & Moore, 1994; Alberto et al., 1986;Connis, 1979; Davies, Stock, & Wehmeyer,2002; Davis, Brady, Williams, & Burta, 1992;Sowers, Verdi, Bourbeau, & Sheehan, 1985;Wacker & Berg, 1983; Wacker et al., 1985) viaself-instruction involving audio or visual cues.Thus, there is reason to believe that parentswith ID could learn a set of specific parentingskills via self-learning.
SELF-DIRECTED PARENTINGEDUCATION FOR PARENTS WITH ID
Context
The parent education assessment and inter-vention model that includes the self-directedapproaches described herein was developedin 1981 at Surrey Place Centre, Toronto,Canada. Surrey Place Centre is funded by theprovincial government to provide a variety ofcommunity outreach professional services topersons with ID. The Parent Education Pro-gram (PEP) started as a demonstration projectand was funded by internal service and ex-ternal research grants until 1987 when theprogram became part of the center’s inter-nal operating budget. Over the years, PEPhas provided services to hundreds of fami-lies. From 1982 to 1994, I was director of theprogram and principal investigator on all re-search grants (totalling over Can $300,000).PEP therapists have had undergraduate and
graduate degrees in psychology, nursing, andearly childhood education. PEP works closelywith other agencies in Toronto providingservices to families headed by parents withID, including child protection, public healthnurses, adult support workers, case coordina-tors, and daycares. Today, PEP (now called theParent Enhancement Program) remains one ofthe few services in the world dedicated exclu-sively to these families.
Child-care checklists
We designed child-care checklists that aretask analyses of important basic child-care,health, safety, and interactional skills (partic-ularly for newborn to preschool age range),based on current validated source materials.Pediatric health care professionals (eg, pedi-atricians, public health nurses, nutritionists)reviewed the content of the checklists andrecommended changes that we incorporatedinto the final versions. We have used thesechecklists in numerous studies to evaluatefull training (Feldman, Case, Garrick, et al.,1992; Feldman et al., 1992, 1997, self-learning(Feldman & Case, 1997, 1999; Feldman,Ducharme, & Case, 1999), and skills of par-ents without ID (Feldman, 1998a). The check-lists have good content validity, baseline stabil-ity, and high interobserver agreement (meanpercentage agreement was 90.8%, 91.5%, and95%, respectively, in the 3 published self-learning studies). The checklists differenti-ate the (pretraining) child-care performanceof parents with and without ID (Feldman,1998a) and detect short-term and long-termchanges in parenting skills due to training.Table 1 illustrates the preparing the bath child-care checklist used in our work
Development of manuals and audiotapes
Manuals
The self-instructional materials cover thecontents of the child-care checklists. The pic-torial manuals illustrate each checklist itemfor 25 basic parenting skills relevant for chil-dren aged 0 to 5 years old. We have compiledthe checklists and manuals (and additional ma-terials) into a 230 page, parenting handbook

LWW/IYC AS237-02 December 4, 2003 11:47 Char Count= 0
20 INFANTS AND YOUNG CHILDREN/JANUARY–MARCH 2004
Table 1. Example of a child-care checklist
Preparing a tub bath
1. (Parent) closes the window to warm upthe room.
2. Puts the bath supplies next to the tub(see “Supplies for the Bath” manual).
3. Puts the bathmat in the tub and pushes itdown so that it sticks.
4. Runs warm water into the tub up toparent’s wrist (when thumb is touchingtub bottom).
5. Tests the temperature of the water bypouring some on wrist and makesadjustments to water temperature asnecessary.
6. Undresses the baby and cleans bottom ifdirty.
(Proceed to “Giving a Bath in the Tub”Manual)
(Case & Feldman, 1993) available from the au-thor at cost. Table 2 presents the list of skillsfor which manuals are available.
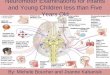
The pictures in the manuals are line draw-ings traced from photographs, ranging in sizefrom 7.3 cm × 9.6 cm to 10 cm × 12.5 cm.As seen in Fig 1, each picture depicts a stepof the task analysis (no more than 2 pictures
Table 2. Parenting skills for which pictorial manuals are available
First aid & medicalHome safety and prevention Cribs and bedtime emergencies
Objects out of reach∗ Crib safety∗ Diaper rash treatment∗
Kitchen safety∗ Bedtime safety∗ When to call the doctor∗
Cuts, burns, & bruises∗ Choosing a crib When to call 911∗
Suffocation∗ Getting the crib ready BathingElectric shock∗ Bedtime routine Preparing the bath∗
Cosmetic poisoning∗ Feeding Bathing an infant∗
Household poisoning∗ Cleaning baby bottles∗ Washing baby’s hair∗
Choking Sterilizing baby bottles∗ Bathing suppliesMedicinal poisoning Nutrition∗ OtherPoisonous plants Burping baby∗ Diapering∗
Serious falls and wandering away Preventing spitting up formula Giving clear instructions∗
∗Training for these items was given in the 3 published studies.
per page). We experimented with differentimages (actual photos, cartoon drawings), butwe found that parents with low literacy skillspreferred and best understood the line draw-ings. The line drawings are easy to reproduce;they allow us to control how much infor-mation is illustrated and emphasize the mostimportant elements in the picture. We rec-ognized that most of the pictures were notself-explanatory; hence, we added short titlesabove, and brief descriptions, beside, eachpicture. The text and format of all the man-uals were guided by research with personswho have below average literacy skills (Doak,Doak, & Root, 1995). The reading level of themanuals average grade 3, and is no higher thangrade 6 (based on Fry formula, in Doak et al.,1995). Pediatric health care professionals re-viewed and approved the manuals prior to ex-tensive field-testing by parents with and with-out ID
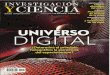
Not all skills lent themselves to task analy-sis, so some manuals were set up as discrim-ination tasks. For instance, as seen in Fig 2,the home safety manuals have 2 pictures side-by-side on each page. The one on the left (ti-tled, “Find”) illustrates a safety hazard (eg, aplastic bag within reach of the child) and thepicture on the right (titled, “Fix”) shows the“parent”putting the hazard out of reach of the

LWW/IYC AS237-02 December 4, 2003 11:47 Char Count= 0
Self-Directed Learning of Child-Care Skills 21
Fig 1. Page 1 from the Getting Ready for a Tub Bath manual.
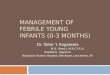
child (eg, putting the bag on the top shelf ofa cupboard). Below these 2 pictures are illus-trations of generalization items (ie, differenttypes of bags). As seen in Fig 3, the medicalemergencies manuals consists of illustrationsof various childhood ailments and accidents,
one to a page (or card) for “When to Call theDoctor” or “When to Call 911.” After review-ing the manuals, the parents sort a shuffleddeck of these pictures into 2 piles—whetherthe condition is serious enough to call 911(eg, child was unconscious) or calling the

LWW/IYC AS237-02 December 4, 2003 11:47 Char Count= 0
22 INFANTS AND YOUNG CHILDREN/JANUARY–MARCH 2004
Fig 2. Page 2 from the Prevention of Falls and Wandering safety manual.
family physician (or telemedicine informa-tion) is sufficient (eg, mild diaper rash).
Audiotapes
Some of the parents were unable to readeven the simple text in the manuals, so werecorded supplementary audiotapes. The au-diotapes consist of a woman with a clear voiceslowly reading the written contents of eachmanual. The voice provides instructions onwhere to look on the page and when to turnthe page. The audiotapes are standard size cas-settes suitable for portable cassette players.
We provided players and batteries to the par-ents involved in our studies.
Procedure
Skills assessment
After obtaining informed consent, and mak-ing several home visits to develop rapport andmake informal observations, we observe theparent caring for the child on a typical day orat different times over several days. We ask theparent to “do what you usually would do.”Asthe parent performs a particular task (eg, di-apering), we fill out the relevant child-care

LWW/IYC AS237-02 December 4, 2003 11:47 Char Count= 0
Self-Directed Learning of Child-Care Skills 23
Fig 3. Page 2 from the When to Call 911 manual.
checklist. If toward the end of the visit, theparent has not performed a skill that we wishto observe, then we ask them to do so (if it isnot too disruptive to the child or family rou-tine). To check home safety, we inspect thehome for hazards, along with the parent (todetermine the parent’s ability to identifyhousehold hazards). We also orally administerseveral checklists of knowledge and skills thatcannot be readily observed during a homevisit (eg, responding to medical emergen-cies; treatment of common childhood ail-ments) and we document the parent’s verbalresponses.
Correct and incorrect responses are notedon each step of the checklist. A correct scoremeans that the step is performed as specified,without trainer instruction, prompting, or as-sistance while the parent attempts the task.Not performing the step independently (or atall) is scored as incorrect. Steps can be com-pleted in a different sequence than in the taskanalysis as long as this order does not compro-mise the otherwise correct (and safe) task per-formance. We calculate the percentage cor-rect score on the whole task as the number ofsteps performed correctly divided by the totalnumber of steps times 100%. Unless we need

LWW/IYC AS237-02 December 4, 2003 11:47 Char Count= 0
24 INFANTS AND YOUNG CHILDREN/JANUARY–MARCH 2004
to fix something immediately (eg, the bath wa-ter is too hot), we offer no instruction dur-ing the assessment, baseline or subsequentself-learning phase. Following the assessment,we inform the parents which skills they per-formed adequately—same as the mean per-formance of a group of known competentparents (Feldman, 1998a)—and which skillscould be improved. If the parent needs train-ing on more than 1 skill, we give them achoice of which one they want to try first.This skill assessment is the same whether weplan to use self-directed learning or full train-ing (Feldman, 1998a, 1998b).
Baseline
After completing the parenting skills as-sessment, we schedule several home visits tomonitor baseline performance. To ensure thatskill performance is consistently below crite-ria, we prefer to obtain approximately 3 base-line points over several weeks before startingtraining (if a skill needs to be trained quickly—eg, diaper rash treatment—we usually starttraining immediately after 1 baseline session).We ask the parent to perform the to-be trainedskill usually at a time when the parent wouldnaturally be performing the skill (eg, when thebaby’s diaper needs changing). We provide nofurther instructions, training, or feedback. Anindividual baseline session lasts as long as ittakes the parent to demonstrate the skill be-ing observed (eg, 5–10 min). We also monitorbaseline performance on other skills that alsoneed training.
Training the use of the manuals
Most parents with whom we have workedquickly learn how to use the self-instructionalmanuals and audiotapes. First, we read themanual together. We ask the parent to de-scribe each picture and read the accompa-nying text to the best of her/his ability. Werecord oral reading errors and immediatelycorrect them. We then ask some comprehen-sion questions to determine if the parent fullyunderstands the contents of the manual (eg,“What do you do after you finish changingthe baby’s diaper?” Answer: “Put the diaper
in the garbage and wash my hands.”). If theparent did not answer a comprehension ques-tion correctly, we would review the relevantsection of the manual and provide further re-mediation as needed. This instruction takesabout half hour. Note that this training isonly done once, when the manual is intro-duced for each skill needing training.
Training the use of the audiotapes
We routinely offer the parents audiotapesthat orally present the manual text. We showthem how to install the tape, plug in and wearthe headphones, operate the tape player, andchange the batteries (most parents alreadyknew how to operate a cassette player). Wethen ask them to listen to the tape while read-ing along (silently), and pointing to the pic-ture being described on the tape. Using a dualheadphone jack, we listen on a second set ofheadphones to be sure that the parent is fol-lowing the directions on the tape (eg, whento turn the page). We originally suggested thatthe parent use the manual (and listen to thetape) while they performed the task. Parentsinformed us, however, that they found it cum-bersome to do so. Now we recommend thatthey review the materials just before needingto do the task.
Monitoring use of the manual
Several days after leaving the materials withthe parent (and sometimes in between sub-sequent home visits), we call to ask whether(and how often) the parent used the materi-als during the interim period. Regardless ofthe response, we do not say anything specifi-cally about the skills or using the manual. Weschedule weekly home visits to observe theparent performing the designated child-careskills (ones that have or would receive the self-instructional materials). As in the assessment,we again use the child-care checklists to mon-itor performance and we (initially) do not pro-vide any prompting or feedback.
Prompting
If the parent does not make substantialprogress after about 3 or 4 visits, we institute a

LWW/IYC AS237-02 December 4, 2003 11:47 Char Count= 0
Self-Directed Learning of Child-Care Skills 25
2-level least-to-most prompting procedureover several weeks. In the first level, we gen-tly remind the parent to use the materials. Ifno improvement is noted on the next visit, wemay repeat the level 1 prompt or give a level 2prompt in which we ask the parent to read themanual out loud in our presence (we alwaysbring extra copies of the manual and tapesin case the parent claims that he/she lost thematerials); with level 2 prompts, the trainermore assertively recommends that the parentreview the materials each time he/she needsto perform the task.
Follow-up
We continue weekly monitoring visits untilthe parent meets criterion on that skill (80%over 2 consecutive visits); we then graduallyfade observations of that skill from once aweek to once a month, every 3-months, to ev-ery 6-months. If the parent needs training onanother skill, we offer another set of materi-als, usually on the same visit when the parentmet criterion on the first skill.
Full training
If the parent fails to meet criterion by aboutthe seventh monitoring visit and did not re-spond to the prompts, then we offer fulltraining. Full training consists of supplement-ing the self-directed learning with trainer-directed teaching including verbal prompting,modelling (of the specific steps the parentis performing incorrectly), praise for cor-rect responses, and corrective feedback (seeFeldman, 1998a, 1998b, for more details).
EVALUATION OF SELF-DIRECTEDLEARNING FOR PARENTS WITH ID
We have conducted a series of controlledfield-tests of our self-directed parenting train-ing protocols using multiple baseline acrossskills and participants and alternating treat-ment designs Barlow & Hersen, 1984). Thealternating treatments study compared self-directed instruction on different skills (of sim-ilar difficulty) with the manual plus audiotapeto that with the manual alone or to no train-
ing within the same participant (Feldman &Case, 1997). The no training skills were subse-quently trained using either the manual aloneor the manual plus audiotape, but monitoringsessions were conducted monthly rather thanweekly. Here, I summarize the results acrossthe 3 published studies involving 30 mothersand 3 fathers with ID (Feldman & Case, 1997,1999; Feldman et al., 1999).
Participants
Details of the 33 families who participatedare found within the respective publications.Briefly, the parents were all considered tohave ID, based on recent eligibility assess-ments for government funding and servicesreserved for persons with ID. In Ontario, thedefinition of ID is synonymous with the DSM-IV definition of mental retardation (AmericanPsychiatric Association, 1994). Most partici-pants received this diagnosis when they werein school, but we were aware that some of theparents had adult IQ scores between 70 and80. Nonetheless, they continued to receive IDservices, including ours; we found that these“borderline” IQ participants in fact demon-strated parenting skill deficits similar to thatof parents with IQs <70. In addition to theparent education service described herein,many of the parents received additional ser-vices such as a support worker (who helpedwith aspects of daily living such as budgeting,finding accommodations, and employment),public health nurse (available to all high-riskfamilies), and a visiting homemaker (to keepthe home clean and teach domestic skills).All parents were able to give their own in-formed consent to (voluntarily) participate(we read the program information and con-sent forms to them and the parents signedthe consent form in front of a witness of theirchoice).
Child protection services were supervising79% of the families and some children hadbeen placed in care at different times. All ofthe families were living independently in thecommunity below the poverty line (30% wereliving in subsidized housing), 82% receivedwelfare or disability allowance or both. The

LWW/IYC AS237-02 December 4, 2003 11:47 Char Count= 0
26 INFANTS AND YOUNG CHILDREN/JANUARY–MARCH 2004
mean age of the parents was 26.3 years, range:19 to 40 years, and 73% were married. Al-though up-to-date IQ scores were unavailablefor most of the parents, their mean readinggrade level was 4.1, range: 1.25 to 8.25, basedon the Wide Range Achievement Test (Jastak& Wilkinson, 1984). The mean age of the tar-get children (17 females, 16 males) was 9.9months, range: 2 to 51 months.
Skill performance
The starred items in Table 2 are the 21 skillsfor which training was given across the 33 par-ticipants. Table 3 summarizes pertinent find-ings from each study. Note that in Feldmanand Case (1997) there were 4 within-subjecttraining conditions with different skills: man-ual and audiotape (weekly or monthly moni-toring) and manual alone (weekly or monthlymonitoring); in total, 50 of 61 skills (82%)reached criterion in a mean of 3.5 trials.These results are comparable to our full train-ing outcomes with similar parents and skills(Feldman, Case, Garrick, et al., 1992; Feldmanet al., 1992, 1997; Tymchuk et al., 1990a,1990b). Figure 4 illustrates the combined re-sults across the 3 studies. Note that perfor-mance continued to increase in the follow-upperiod (mean = 7 months; range: 0.4 to 43.4months).
Across all studies, 96% of the skills thatmet criteria via self-learning maintained above80% in follow-up without further training.Skills were maintained despite monitoring be-ing reduced to once every 6-months and mostof the parents telling us that they no longerneeded to refer to the manual to rememberto perform the tasks correctly. Of the 33 par-ents, only 2 failed to reach criterion on at least1 skill via self-learning and another parent re-quired full training in follow-up to regain cri-terion levels.
We gave level 1 and level 2 prompts to9 and 3 parents, respectively. These parentswere prompted because they informed us thatthey had not been using the materials (usuallysaying that they had misplaced them) and/ortheir performance remained low or droppedback to baseline levels. Only 2 parents did
not improve to criterion with prompting(they subsequently met criterion with fulltraining).
We detected no meaningful differences inresponse to the self-directed approach: (a) be-tween mothers and fathers (although havingonly 3 fathers limits conclusions), (b) whenvisits were monthly rather than weekly (forthe original no training skill) (Feldman & Case,1997), or (c) when another agency used ourself-directed parent training protocols and ma-terials for 2 parents (Feldman & Case, 1999).Although there were no significant differ-ences between the manual plus audiotape andthe manual alone conditions in Feldman andCase (1997), 3 of 4 skills that failed to meetcriterion in the manual alone condition did sowhen an audiotape was added (see Table 3).Finally, consumer satisfaction was uniformlyhigh across studies. Interestingly, in the studyusing an alternating treatment design, parentswho had experienced both the manuals aloneand the manuals plus audiotape (for differentskills) tended to have no preference or pre-ferred the manuals alone (Feldman & Case,1997).
Predictors of success
We examined (a) baseline measure of read-ing and (b) acceptance of the self-learning ma-terials as 2 potential predictors of successfulself-directed parent training. The trainer (whorecorded and corrected oral reading and com-prehension errors) rated the parent’s readingof the first manual presented to the parent.Reading ratings ranged from 1 (read and un-derstood the manual very poorly) to 5 (readand understood manual very well). To mea-sure acceptance of the manual, the trainerfilled out a Likert-type scale based on the par-ent’s response to being offered the first man-ual. Scores ranged from 1 (parent acceptedthe materials very poorly) (ie, parent was re-luctant, or refused, to accept the materials) to5 (parent accepted the materials very well)(ie, parent enthusiastically accepted the ma-terials, and used them at the first opportu-nity). Across the 3 studies, we found a signi-ficant correlation between the trainer’s rating

LWW/IYC AS237-02 December 4, 2003 11:47 Char Count= 0
Self-Directed Learning of Child-Care Skills 27
Tab
le3
.Su
mm
ary
of
the
resu
lts
of
3se
lf-le
arn
ing
stu
die
sfo
rp
aren
tsw
ith
inte
llect
ual
dis
abili
ties
Mea
n%
corr
ect
inM
ean
%fo
llo
w-u
pM
ean
corr
ect
in(m
ean
no
.o
fN
o.o
fN
o.o
fM
ean
%se
lf-
no
.o
fse
ssio
ns
skil
lsn
ot
skil
lsco
rrec
tin
inst
ruct
ion
alm
on
ths
into
reac
hin
gSt
ud
yN
trai
ned
bas
elin
ep
has
efo
llo
w-u
p)
crit
erio
n∗
crit
erio
n
Feld
man
etal
.(19
99)—
man
ual
alo
ne
1013
5679
%90
%(1
1.9)
3.8
1Fe
ldm
an&
Cas
e(1
999)
—au
dio
tap
e+
man
ual
†10
1239
7286
(4)
2.5
1Fe
ldm
anan
dC
ase
(199
7)—
man
ual
alo
ne†
1313
5481
82(6
.1)
3.6
4‡
Feld
man
and
Cas
e(1
997)
—au
dio
tap
e+
man
ual
†13
1348
8291
(6.1
)6.
02
Feld
man
and
Cas
e(1
997)
—m
anu
alal
on
e3
345
78..
.2
1(m
on
thly
mo
nit
ori
ng)
†
Feld
man
and
Cas
e(1
997)
—au
dio
tap
e+
man
ual
77
4573
...
3.4
2(m
on
thly
mo
nit
ori
ng)
†
∗ Cri
teri
on
:≥80
%o
ver
2co
nse
cuti
vese
ssio
ns.
† Sam
e13
par
tici
pan
tsw
ho
wer
ein
aal
tern
atin
gtr
eatm
ents
des
ign
inFe
ldm
anan
dC
ase
(199
7),b
ut
each
con
dit
ion
use
dd
iffe
ren
tsk
ills.
‡ Th
ree
of
thes
e4
skill
ssu
bse
qu
entl
yre
ach
edcr
iter
ion
wh
enth
ep
aren
tsw
ere
give
nau
dio
tap
esto
acco
mp
any
the
man
ual
s.

LWW/IYC AS237-02 December 4, 2003 11:47 Char Count= 0
28 INFANTS AND YOUNG CHILDREN/JANUARY–MARCH 2004
of reading (mean = 1.59) and mean percent-age score during training (mean = 83.1%),r = 0.42, p < .03. There were no significantcorrelations between reading scores and base-line or follow-up percentage correct, or trialsto criterion. These results suggest that read-ing abilities may affect overall scores duringtraining; perhaps using supplemental audioor video aides may allow those parents withlow literacy skills to benefit from self-directedlearning. Indeed, 3 parents who failed toreach criterion with the manual alone, did so,after receiving the complementary audiotape(although the research design did not allow usto conclude with certainty that the improve-ment was due to the addition of the audio-tape) (Feldman & Case, 1997). We also founda significant correlation between the accep-tance score (mean = 3.3) and the follow-upscore (mean = 87.8%), r = 0.34, p = .05; noother correlations were significant. Only oneparent (Katherine in Feldman & Case, 1999)initially refused to accept the manual (sayingit reminded her of school work), but withsome encouragement, she did agree to give ita try (and failed). The relationship betweenthe acceptance ratings and follow-up scoressuggests that (although most of the parentswillingly accepted the materials) parents whoare initially enthusiastic about using the ma-terials may maintain their skills better. These
Fig 4. Mean percentage correct in baseline, training, and follow-up for the 33 parents in the 3 publishedself-learning studies.
correlational findings should be interpretedcautiously because of the small sample sizeand different skills taught.
CONCLUSION
Self-directed learning appears to be a feasi-ble and easily disseminable way of providing,low-cost, low-tech, highly satisfying child-caretraining to parents with cognitive limitations.Almost all the parents rapidly met criterion onthe trained skills (based on the performanceof known competent parents) that were main-tained over many months. The results ob-tained closely resemble those achieved withfull training packages provided by speciallytrained parent educators (Feldman, 1994).Many parents improved their skills using justthe visual materials, although some parentsdid not benefit until an audiotape was added.Several parents needed prompting to remindthem to use the materials, but these promptswere quite simple and could easily be issuedby anyone involved in supporting the family(eg, support worker, family member).
Future research is needed to clarify the con-tent validity, efficacy, and clinical utility ofself-directed learning for parents with ID. Al-though we found comparable results to fulltraining, a multisite, randomized clinical trialthat directly compares different instructional

LWW/IYC AS237-02 December 4, 2003 11:47 Char Count= 0
Self-Directed Learning of Child-Care Skills 29
strategies (and control groups) with a largesample is still needed. The effects of self-learning of child-care skills on the parent’sself-esteem and confidence as well as on thechild’s health and development require closerexamination. Does the use of the treating di-aper rash manual result in elimination of therash in the child (we have one affirmative casein Feldman et al., 1999)? Would use of nutri-tion and feeding pictorial prompts alone in-crease rate of weight gain in low-weight in-fants as when they are combined with fulltraining (Feldman et al., 1997)?
The clinical utility of the materials needs tobe systematically studied. Two parents whoreceived the materials and monitoring fromanother agency did just as well as our partic-ipants. Anecdotally, we have sent the manu-als to hundreds of services around the world
supporting parents with ID, and some ofthese agencies have provided unsolicited tes-timonials of success with the materials. Itwould be worthwhile to evaluate audiovisualmaterials (particularly videotapes) designedto teach positive parent-child interactions be-cause many parents with ID have difficultyin this area (Feldman et al., 1993). Impor-tantly, more field-testing is needed to evaluatethe effectiveness of routine distribution ofself-instructional parenting materials, prena-tally or postnatally (eg, at prenatal classes,hospital discharge, newborn check-ups) byhome visitors, nurses, family physicians,and pediatricians. Ultimately, mass dissemi-nation of self-learning child-care guides mayhave a significant impact on the incidenceof child neglect due to parenting skilldeficiencies.
REFERENCES
Agran, M., & Moore, S. C. (1994). How to teach self-instruction of job skills. Washington, DC: AmericanAssociation on Mental Retardation.
Alberto, P. A., Sharpton, W. R., Briggs, A., & Stright, M. H.(1986). Facilitating task acquisition through the use ofa self-operated auditory prompting system. Journal ofthe Association for Persons with Severe Handicaps,11, 85–91.
American Psychiatric Association. (1994). Diagnosticand Statistical Manual. (4th ed.). Washington, DC:APA.
Barlow, D. H., & Hersen, M. (1984). Single-case exper-imental designs. Strategies for studying behaviorchange. New York: Pergamon Press.
Barone, V. J., Greene, B. F., & Lutzker, J. R. (1986).Home safety with families being treated for childabuse and neglect. Behavior Modification, 10, 93–114.
Bauman, K. E., Reiss, M. L., Rogers, R. W., & Bailey, J. S.(1983). Dining out with children: Effectiveness of aparent advice package on pre-meal inappropriate be-havior. Journal of Applied Behavior Analysis, 16, 55–68.
Besalal, V. A., Azrin, N. H., Thienes-Hontos, P., & McMor-row, M. (1980). Evaluation of a parent’s manual fortraining enuretic children. Behaviour Research andTherapy, 18, 358–360.
Case, L., & Feldman, M. A. (1993). Step-by-step child-care:A pictorial manual for parents, child-care workers,and babysitters. Toronto: Authors.
Christensen, A., & Jacobson, N. S. (1994). Who (or what)
can do psychotherapy: The status and challenge ofnonprofessional therapies. Psychological Science, 5,8–14.
Clark, H. B., Greene, B. F., Macrae, J. W., McNees, M. P.,Davis, J. L., & Risley, T. R. (1977). A family advice pack-age for family shopping trips: Development and evalu-ation. Journal of Applied Behavior Analysis, 10, 605–624.
Connell, S., Sanders, M. R., & Markie-Dadds, C. (1997).Self-directed behavioural family intervention for par-ents of oppositional children in rural and remote ar-eas. Behavior Modification, 21, 379–408.
Connis, R. T. (1979). The effects of sequential pictorialcues, self-recording, and praise on the job task se-quencing of retarded adults. Journal of Applied Be-havior Analysis, 12, 355–361.
Davies, D. K., Stock, S. E., & Wehmeyer, M. L. (2001).Enhancing independent Internet access for individu-als with mental retardation through the use of a spe-cialized web browser: A pilot study. Education andTraining in Mental Relardation and DevelopmentalDisabilities, 36, 107–113.
Davies, D. K., Stock, S. E., & Wehmeyer, M. L. (2002). En-hancing independent task performance for individu-als with mental retardation through use of a handheldself-directed visual and audio prompting system. Edu-cation and Training in Mental Retardation and De-velopmental Disabilities, 37, 209–218.
Davis, C. A., Brady, M. P., Williams, R. E., & Burta, M.(1992). The effects of self-operated auditory prompt-ing tapes on the performance fluency of persons with

LWW/IYC AS237-02 December 4, 2003 11:47 Char Count= 0
30 INFANTS AND YOUNG CHILDREN/JANUARY–MARCH 2004
severe mental retardation. Education and Training inMental Retardation, 27, 39–50.
Doak, C. G., Doak, L. G., & Root, J. H. (1995). Teachingpatients with low literacy skills. Philadelphia: Lippin-cott.
Ergon-Rowe, E., Ichinose, C. K., & Clark, H. B. (1991). Re-ducing child whining through self-instructional parenttraining materials. Child and Family Behavior Ther-apy, 13, 41–57.
Espe-Scherwindt, M., & Kerlin, S. (1990). Early interven-tion with parents with mental retardation: Do we em-power or impair? Infants and Young Children, 2, 21–28.
Feldman, M. A. (1994). Parenting education for parentswith intellectual disabilities: A review of outcomestudies. Research in Developmental Disabilities, 15,299–332.
Feldman, M. A. (1997). The effectiveness of early in-tervention for children whose mothers are mentallyretarded. In M. J. Guralnick (Ed.), The effectivenessof early intervention: Directions for second genera-tion research (pp. 171–191). Baltimore, MD: Paul H.Brookes.
Feldman, M. A. (1998a). Parents with intellectual disabil-ities: Implications and interventions. In J. R. Lutzker(Ed.), Handbook of child abuse and neglect research(pp. 401–419). New York: Plenum.
Feldman, M. A. (1998b). Preventing child neglect: Child-care training for parents with intellectual disabilities.Infants & Young Children, 11, 1–11.
Feldman, M. A. (2002a). Children of parents with intel-lectual disabilities. In R. McMahon & R. DeV. Peters(Eds.), The effects of parental dysfunction on chil-dren (pp. 205–223). New York: Kluwer Academic.
Feldman, M. A. (2002b). Parents with intellectual disabil-ities and their children: Impediments and supports.In D. Griffiths & P. Federoff (Eds.), Ethical dilemmas:Sexuality and developmental disability (pp. 255–292). Kingston, NY: NADD Press.
Feldman, M. A, & Case, L. (1997). Effectiveness of self-instructional audiovisual materials in teaching child-care skills to parents with intellectual disabilities. Jour-nal of Behavioral Education, 7, 235–257.
Feldman, M. A., & Case, L. (1999). Teaching child-careand safety skills to parents with intellectual disabilitiesvia self-learning. Journal of Intellectual and Develop-mental Disability, 24, 27–44.
Feldman, M. A., Case, L., Garrick, M., MacIntyre-Grande,W., Carnwell, J., & Sparks, B. (1992). Teaching child-care skills to parents with developmental disabili-ties. Journal of Applied Behavior Analysis, 25, 205–215.
Feldman, M. A., Case, L., & Sparks, B. (1992). Effective-ness of a child-care training program for parents at-riskfor child neglect. Canadian Journal of BehaviouralScience, 24, 14–28.
Feldman, M. A., Ducharme, J. M., & Case, L. (1999). Usingself-instructional pictorial manuals to teach child-care
skills to mothers with intellectual disabilities. Behav-ior Modification, 23, 480–497.
Feldman, M. A., Garrick, M., & Case, L. (1997). The ef-fects of parent training on weight gain of nonorganic-failure-to-thrive children of parents with intellectualdisabilities. Journal on Developmental Disabilities, 5,47–61.
Feldman, M. A., Sparks, B., & Case, L. (1993). Effective-ness of home-based early intervention on the languagedevelopment of children of parents with mental retar-dation. Research in Developmental Disabilities, 14,387–408.
Feldman, M. A., & Walton-Allen, N. (1997). Effects of ma-ternal mental retardation and poverty on intellectual,academic, and behavioral status of school-age chil-dren. American Journal on Mental Retardation, 101,352–264.
Frank, A. R., Wacker, D. P., Berg, W. K., & McMahon, C. M.(1985). Teaching selected microcomputer skills to re-tarded students via picture prompts. Journal of Ap-plied Behavior Analysis, 18, 179–185.
Giebenhain, J. E., & O’Dell, S. L. (1984). Evaluation of aparent-training manula for reducing children’s fear ofthe dark. Journal of Applied Behavior Analysis, 17,121–125.
Jastak, S., & Wilkinson, G. S. (1984). WRAT-R manual.Toronto: Brace, Jovanovich.
Johnson, B. F., & Cuvo, A. J. (1981). Teaching mentally re-tarded adults to cook. Behavior Modification, 5, 187–202.
Kashima, K. J., Baker, B. L., & Landen, S. J. (1988). Media-based versus professionally led training for parentsof mentally retarded children. American Journal onMental Retardation, 93, 209–217.
Robinson-Wilson, M. A. (1977). Picture recipe cards as anapproach to teach severely and profoundly retardedadults to cook. Education and Training of the Men-tally Retarded, 12, 69–73.
Sanders, M. R., Markie-Dadds, C., Tully, L. A., & Bor, W.(2000). The Triple P Positive Parenting Program: Acomparison of enhanced, standard, and self-directedbehavioural family intervention for parents of childrenwith early onset conduct problems. Journal of Con-sulting and Clinical Psychology, 68, 624–640.
Sarber, R. E., Halasz, M. M., Messmer, M. C., Bickett, A. D.,& Lutzker, J. R. (1983). Teaching menu planning andgrocery shopping skills to a mentally retarded mother.Mental Retardation, 21, 101–106.
Scogin, F., Bynum, J., Stephens, G., & Calhoon, S.(1990). Efficacy of self-administered treatment pro-grams: Meta-analytic review. Professional Psychology:Research and Practice, 21, 41–47.
Seymour, F. W., Brock, P., During, M., & Poole, G. (1989).Reducing sleep distruptions in young children: Evalu-ation of therapist-guided and written information ap-proaches. A brief report. Journal of Child Psychologyand Psychiatry, 30, 913–918.
Slater, M. A. (1986). Modification of mother-child

LWW/IYC AS237-02 December 4, 2003 11:47 Char Count= 0
Self-Directed Learning of Child-Care Skills 31
interaction processes in families with children at-riskfor mental retardation. American Journal of MentalDeficiency, 91, 257–267.
Sowers, J-A., Verdi, M., Bourbeau, P., & Sheehan, M.(1985). Teaching job independence and flexibility tomentally retarded students through the use of a self-control package. Journal of Applied Behavior Analy-sis, 18, 81–85.
Stephan, R. A. (1987). Audiotape instruction of face-washing for an adult with mental retardation. Amer-ican Journal of Occupational Therapy, 41, 184–185.
Thinesen, P., & Bryan, A. (1981). The use of sequen-tial picture cues in the initiation and maintenanceof grooming behaviors with mentally retarded adults.Mental Retardation, 19, 246–250.
Tucker, M. B., & Johnson, O. (1989). Competence pro-moting versus competence inhibiting social supportfor mentally retarded mothers. Human Organization,48, 95–107.
Tymchuk, A. J., & Andron, L. (1992). Project parenting:Child interactional training with mothers who arementally handicapped. Mental Handicap Research, 5,4–32.
Tymchuk, A. J., Andron, L., & Tymchuk, M. (1990). Train-ing mothers with mental handicaps to understand be-havioral and developmental principles. Mental Hand-icap Research, 3, 51–59.
Tymchuk, A. J., Hamada, D., Andron, L. & Anderson, S.(1990a). Emergency training for mothers with mentalretardation. Child and Family Behavior Therapy, 12,31–47.
Tymchuk, A. J., Hamada, D., Andron, L., & Anderson, S.(1990b). Home safety training with mothers who arementally retarded. Education and Training in MentalRetardation, 25, 142–149.
Tymchuk, A. J., Yokota, A., & Rahbar, B. (1990). Decision-making abilities of mothers with mental retardation.Research in Developmental Disabilities, 11, 97–109.
Van Luit, J. E. H., & Naglieri, J. A. (1999). Effectivenessof the MASTER program for teaching special childrenmultiplication and division. Journal of Learning Dis-abilities, 32, 98–107.
Wacker, D. P., & Berg, W. K. (1983). Effects of pictureprompts on the acquisition of complex vocationaltasks by mentally retarded adolescents. Journal of Ap-plied Behavior Analysis, 16, 417–433.
Wacker, D. P., Berg, W. K., Berrie, P., & Swatta, P. (1985).Generalization and maintenance of complex skills byseverely handicapped adolescents following pictureprompt training. Journal of Applied Behavior Anal-ysis, 18, 329–336.
Watson-Perczel, M., Lutzker, J. R., Greene, B. F., &McGimpsey, B. J. (1988). Assessment and modifica-tion of home cleanliness among families adjudicatedfor child neglect. Behavior Modification, 12, 57–81.
Webster-Stratton, C., Kolpacoff, M., & Hollinsworth, T.(1988). Self-administered videotape therapy for fami-lies with conduct-problem children: Comparison withtwo cost-effective treatments and a control group.Journal of Consulting and Clinical Psychology, 56,558–566.
Lists of current articles: http://depts.washington.edu/isei/iyc/iyc_comments.html
To view previous articles: http://depts.washington.edu/isei/iyc/iyc_previous.html