Embed Size (px)
Citation preview
LWW/IYC lwwj111-03 June 4, 2005 3:52 Char Count= 0
Infants & Young ChildrenVol. 18, No. 3, pp. 186–199c© 2005 Lippincott Williams & Wilkins, Inc.
Exploring Mental HealthOutcomes for Low-incomeMothers of Children WithSpecial NeedsImplications for Policy and Practice
Chrishana M. Lloyd, PhD; Elisa Rosman, PhD
Research has indicated that there is a heightened risk for the occurrence of childhood disabilitiesin single-parent-female-headed households that are living at or below the poverty line. Researchalso demonstrates increased levels of parenting stress and parenting depression among motherswho have children with special needs. However, very little is currently known about mental healthoutcomes among women who are poor and raising children with disabilities. To work effectivelywith these caregivers, human service professionals must utilize multifaceted approaches based onan ecological framework to address the multitude of challenges that these families face. This articledraws upon ecological theory and a case study to examine the ways that having a child with spe-cial needs impacts women’s emotional well-being and their ability to function in roles they deemappropriate for their children. The case study highlights current policies and the ways in whichthey may exacerbate caretakers’ mental health issues. It also provides a framework to identify anddemonstrate the ways in which an ecological approach is useful in looking outside the individ-ual and the family to understand the processes through which other systems may interact withthe family to affect maternal mental health. Finally, specific links are drawn to both policies andpractice. Key words: early childhood special education, early intervention, maternal mentalhealth, poverty
POVERTY, CHILDREN WITH SPECIALNEEDS, AND MATERNAL MENTALHEALTH
In 2001, 16% of American children—almost12 million—were living in poverty (Lu, 2003).Poverty impacts children’s health in a myr-iad of ways. When families do not haveenough income, fundamental prerequisitesfor good health such as adequate shelterare often difficult to obtain. When shelter
From the School of Social Work, New York University.
This is a joint authored article, and the names of theauthors are not listed in any particular order.
Corresponding author: Chrishana M. Lloyd, PhD, NYUSchool of Social Work, 1 Washington Sq N, New York, NY10003 (e-mail: [email protected]).
is inadequate, basic hygiene is more difficultto maintain and infections can be easily con-tracted and spread. Moreover, the presence ofcockroaches, rodents, and other allergens, of-ten found in older, poorly maintained hous-ing (typically the type of housing that is foundin lower-income, minority, inner-city house-holds) can aggravate chronic conditions suchas asthma.
As a result of these multiple factors, child-hood disability is overrepresented among chil-dren living in poverty. Using the NationalHealth Interview Survey, Wise, Wampler,Chavkin, and Romero (2002) found thatamong children whose families were living inpoverty, there was a prevalence rate of 21.5%for chronic illness, and among those whosefamilies reported receiving Temporary Assis-tance to Needy Families (TANF), there was a
186

LWW/IYC lwwj111-03 June 4, 2005 3:52 Char Count= 0
Exploring Mental Health Outcomes 187
prevalence rate of 25.6% for chronic illness(defined here as asthma, mental retardation,cerebral palsy, autism, attention deficit disor-der, muscular dystrophy, cystic fibrosis, sickle-cell anemia, diabetes, arthritis, and congenitalheart disease). Looking specifically at fam-ilies receiving welfare, Meyers, Lukemeyer,and Smeeding (1996) found that 21% of thewomen in a sample of AFDC (Aid To Fami-lies With Dependent Children) recipients inCalifornia reported having at least one childwith a disability or chronic health problem.As a comparison, the American Academy ofPediatrics cites data finding that 12% to 16%of all children have some sort of developmen-tal or behavioral disorder (American Academyof Pediatrics, 2001). Finally, approaching theissue from the perspective of children diag-nosed with special needs, data from the Na-tional Early Intervention Longitudinal Studyshow that 42% of children entering early in-tervention were in families who were receiv-ing some form of public assistance (Hebbeleret al., 2001).
Both living in poverty and having a childwith special needs have been found to beassociated with negative mental health out-comes in women. Women living in povertyare approximately twice as likely as womenfrom higher income groups to be depressed(Lennon, Blome, & English, 2001), andwomen who have children with special needshave also been found to demonstrate higherlevels of both depression and parenting stressthan women with typically developing chil-dren (for a review, see Rosman, 2003).Women living in poverty who care for chil-dren with special needs often engage in a hostof healthcare activities related to their chil-dren, and this caretaking is often done in iso-lation (Lloyd, 2002). Because of this isolation,caregivers often feel high levels of emotionaland physical stress. These women often donot have periods of respite and relief that areimportant to maintaining mental and physicalhealth (Lloyd, 2002).
It is clear that poor women who havechildren with special needs are subject tosignificant demands. Parents must manage a
host of factors, including unexpected expen-ditures and medical appointments, and con-tinues worries about their children’s future(Meyers, Brady, & Seto, 2000). For familieswhose budget is already stretched to the limit,these demands can hit especially hard. Lack ofmoney for food, clothing, housing, and med-ical care leads to stress among family mem-bers. For example, a study conducted of 31low-income women—21 who cared for chil-dren with special needs and 10 who did not—found that the caregivers of children withspecial needs reported higher levels of psy-chological and physical distress. Depressionwas most prevalent; however, other mani-festations included high blood pressure, mi-graine headaches, anxiety, ulcers, and drugaddiction (Lloyd, 2002).
Scorgie, Wilgosh, and McDonald (1998)conducted an analysis of recent studies onfamilies who cared for children with specialneeds and found that higher income familieshad more choices available to assist with theirown coping. They also found that higher in-come families had increased levels of satisfac-tion in their role as parents. In addition tostress experienced from caring for children,interactions with systems outside of the homehad the ability to increase or decrease parentalstress and mental health outcomes. This focuson resources and systems outside of the familysuggests the importance of ecological theoryin examining the lives of women who are poorand have young children with disabilities.
The authors have chosen ecological theoryas a framework for this article, as it is systems-based and provides a useful mechanism forexploring various factors in and outside ofthe home that can impact mental healthfunctioning.
ECOLOGICAL SYSTEMS THEORY
Ecological theory suggests that there aremultiple facets both of being poor and hav-ing a child with special needs that can beexpected to impact maternal mental healthand well-being. Ecological theory, as originallyposited by Bronfenbrenner (1979), points to

LWW/IYC lwwj111-03 June 4, 2005 3:52 Char Count= 0
188 INFANTS & YOUNG CHILDREN/JULY–SEPTEMBER 2005
the importance of both relationships withinthe family as well as the family’s interac-tions with systems outside of the home.Bronfenbrenner’s theory is explicitly bidirec-tional, with the environment and individualsconcurrently affecting one another (Sontag,1996). Furthermore, while the family is oneimportant sphere of influence on individ-ual development and outcomes, systems out-side of the family also play important roles(Bronfenbrenners’ mesosystem, exosystem,and macrosystem).
Ecological theory has begun to play a rolein research examining children with specialneeds and their families. Glidden (2002) con-ceptualizes environment as a ladder of in-fluence, with parents directly shaping themicroenvironments that their children expe-rience by interacting with their children, aswell as choosing and changing the largermacroenvironment. As explained by Sontag(1996), special educators acknowledge theinfluence of multiple settings and systemson children and recognize the necessity ofexploring the multiple contexts that influ-ence children’s development. However, evenamong those studies that have turned toecological theory, the meaning and opera-tionalization of environment is still fairly lim-ited. Twenty years ago, Crnic, Friedrich, andGreenberg (1983) argued that “. . . the family’scoping resources and functioning are likely tobe mediated by the ecological systems withinwhich they must interact and be acted upon”(p. 126). In 2001, Hodapp (2001) stressed thatthe meaning of “environment” needs to bebroadened in future research.
ECOLOGICAL FACTORS THAT HAVE NOTBEEN FULLY EXAMINED IN THELITERATURE
Ecological theory suggests that there are awide range of factors that may influence ma-ternal mental health in families that are poorand have children with special needs that re-main largely untapped in the literature. Thereare multiple processes that still need to beexplored and that may be especially salient
for families who both have children with spe-cial needs and are living in poverty. These fac-tors also bear attention as they can be manip-ulated by policies and interventions. For thepurposes of this article, the authors have cho-sen to explore family resources, service uti-lization, and maternal employment.
Family resources
Families living in poverty are inherently lowon resources across multiple domains, includ-ing time, money, and supports (Yoshikawa& Hsueh, 2001). These resources may beeven more scarce as a result of the Per-sonal Responsibility and Work Opportunityand Reconciliation Act of 1996. This lack ofresources may be especially acute for familiesraising children with special needs. As Meyerset al. (2000) describe them, these are “expen-sive children in poor families.” For all fami-lies of children with special needs, there aretypically demands on the family’s time andresources that may not have been expectedand that are not encountered by typical fam-ilies. For example, families may have to payfor modifications to the home, in-home care,specialized medical equipment, out-of-pocket(ie, not reimbursed) medical expenses, trans-portation to and from appointments, baby-sitting for other siblings while attending treat-ments for the child, special clothing, food forchildren on specialized diets, and specializedday care (Hogan & Msall, 2002; Meyers, et al.,2000). For families whose budget is alreadystretched to the limit, these economic de-mands may hit especially hard, as these arefamilies for whom “there is relatively little inreserve” (Bernheimer, Weisner, and Lowe, inpress).
Some research has been conducted thatspecifically addresses the role of resourcesin predicting outcomes for families who arepoor and have children with special needs.For example, Supplemental Security Incomebenefits, which are offered to individuals inpoverty who are older than 65 years, blind, ordisabled, have been found to make the differ-ence for families between living above or be-low the poverty line (Kearney, Grundmann, &

LWW/IYC lwwj111-03 June 4, 2005 3:52 Char Count= 0
Exploring Mental Health Outcomes 189
Gallicchio, 1994; Meyers et al., 1996). How-ever, research is not available explicitly link-ing those resources to maternal mental healthand well-being. Furthermore, any researchthat does consider maternal mental healthtypically ignores the subgroup of familieswho have children with special needs. In theMinnesota Family Investment Program, a re-cent welfare-to-work experiment that em-braced the notion of “making work pay,” fi-nancial incentives reduced mothers’ risk ofdepression (Knox, Miller, & Genettian, 2000).However, this intervention did not specificallytarget or examine outcomes for families inpoverty who have children with disabilities(Rosman, 2003).
Service utilization and associated hassles
Another factor that has not been suffi-ciently explored in the literature is the roleof service utilization for families that are liv-ing in poverty and have children with spe-cial needs. These families live at the inter-section of both poverty- and disability-relatedservices and, therefore, may be interactingwith an unusually high number of serviceproviders and service systems. McDonald,Poertner, and Pierpont (1999) explored ser-vice utilization from an ecological perspec-tive. They counted the number of servicesused by families of children with serious emo-tional disorders and found a linear relation-ship between caregiver stress and total num-ber of services ever used. For families usingboth disability- and poverty-related services,this may translate to increased stress, simplyas a result of the large number of servicesbeing accessed. It is fairly easy to imaginethat the hassles involved with those interac-tions may stress mothers to a point wherepotential benefits are overshadowed by the“transaction costs” involved in obtaining them(Gibson & Weisner, 2002).
Rosman (2003) explored the effect thatservice-related hassles played in moderatingthe relationship between service utilizationand maternal mental health. She surveyed80 low-income mothers whose childrenwere receiving early intervention services in
Washington, DC, and Montgomery County,Md. Rosman found that the use of poverty-related services (eg, TANF, Food Stamps, Med-icaid) served a protective function on ma-ternal levels of child-related stress, but onlywhen the use of those services was accompa-nied with low levels of hassles. Similarly, theuse of child care was associated with lowerlevels of both child-related and parent-child-interaction-related stress, but only when ac-companied with low levels of hassles. Thesefindings suggest the need for increased at-tention to the hassles that these familiesencounter on a regular basis and the tollthey may be taking on maternal mentalhealth.
Maternal employment
The role of work in the lives of women whoare poor and have young children with dis-abilities has also not been sufficiently stud-ied. Most of the research that does exist ex-plores the impact that the child’s disabilitystatus may have on maternal employmentstatus. However, even in this area, thereare no clear-cut answers. Some researchersdocument lower levels of employment formothers whose children have special needs(Dodson, Manuel, & Bravo, 2002; Meyers,et al., 2000; Skinner, Slattery, Lachicotte,Cherlin, & Burton, 2002). However, othersfind inconsistent results, possibly due to dif-ferences in definition of childhood disability(Lee, Oh, Hartmann, & Gault, 2003). In a re-cent study using data from the 1996 panel ofthe Survey of Income and Program Participa-tion, Lee et al. (2003) found that childhooddisability had a significant negative impact onmaternal work, but not as great an effect asthe mother’s own disability status.
There is also a body of research that ex-plores that role of employment on maternalmental health for low-income women, reflect-ing a trend that suggests that maternal em-ployment may serve a protective function forlow-income women (Howard, 2003; Jackson& Huang, 2000; Rosman, 2003). However, thispattern is not typically explored specificallyfor families who have children with special

LWW/IYC lwwj111-03 June 4, 2005 3:52 Char Count= 0
190 INFANTS & YOUNG CHILDREN/JULY–SEPTEMBER 2005
needs. A qualitative study by Lloyd (2002)documented that low-income mothers whocared for children with special needs hadhigher levels of stress associated with employ-ment than low-income mothers who did nothave children with special needs. The stressoccurred as a result of difficulties in findingappropriate child care, as well as the difficultyof maintaining a consistent work schedule,particularly when children had chronic andunpredictable healthcare needs. While Lloyd(2002) was able to document the reportedstress that caretakers of special needs childrenfaced, the sample size was small and limitedto a specific geographic location. In addition,the study was exploratory so that one was notable to “measure” the differences betweenthe 2 groups of women and their reportedexperiences.
CASE STUDY
The following case study will be used tohelp explore some of the aforementioned is-sues. The family depicted in the case studyis a composite of various families that par-ticipated in a qualitative study that examinedthe transition from welfare to work for low-income women who cared for children withspecial needs (Lloyd, 2002). The women whoparticipated in the study were purposely sam-pled. That is, they were selected on the ba-sis of the fact that they could provide insightinto navigating welfare-to-work requirementswhile simultaneously caring for a child withspecial needs. The study also targeted care-takers on TANF who did not care for childrenwith special needs. This is especially impor-tant to note, as the comparison group allowedthe researcher to understand the differencesin the lives of low-income women who caredfor children with special needs and those whodid not. Thus, the distinction in sampling al-lows the case study to be presented in a man-ner that provides a snapshot of the contextualissues that a “typical” low-income urban care-taker who is attempting to meet TANF require-ments and care for a child with special needsfaces on a day-to-day basis.
The Darden family
Family structure
Deborah Darden is a 29-year-old never mar-ried mother of two: Davon, age 8, and David,age 4. Both children have the same father,Michael Jones. Although they never married,he was actively involved with the family un-til David was born. Ms Darden feels thatonce the father became aware that David hadmultiple health problems, he could not han-dle the stress and made a decision to “leavehis children.” Ms Darden’s mother lives in thearea and she is able to help out occasionallywith the children’s care. Ms Darden wishesher mother could do more, but she is in “poorhealth” and she does not want to “put a strainon her.”
Education and employment status
Ms Darden is a high school graduate andis currently employed part-time as a homehealth aid. Her job offers some flexibility withrespect to work hours, because she works forindividual clients in their homes.
Children’s health and school status
By all reports, Davon has no significantphysical health issues; however, his motherfeels that he is suffering emotionally becauseshe spends an inordinate amount of time car-ing for David. David has been diagnosed withasthma, attention deficit disorder, a behav-ioral disorder, developmental delays, encopre-sis, seizures, and a speech impairment. He at-tends a center-based early childhood specialeducation program. His teachers describe himas combative, noncompliant, difficult to keepon task, and unmotivated.
Child care
Both children are eligible for free daycarethrough welfare-to-work vouchers. Ms Dardentakes advantage of this benefit, and the chil-dren participate in after-school daycare pro-grams. Unfortunately, the daycare voucherthat is provided by the state does not coverthe costs of caring for a child with special

LWW/IYC lwwj111-03 June 4, 2005 3:52 Char Count= 0
Exploring Mental Health Outcomes 191
needs. In order for David to receive daycarewhile Ms Darden is at work, she pays an addi-tional $250 per month.
Community resources
Ms Darden is connected to a welfare-to-work program. She has a great relationshipwith her case manager, and the agency hasbeen helpful in assisting her develop a resumeand locate childcare. In addition, her casemanager has provided referrals for employ-ment, money for transportation, and emer-gency food. At one time, Ms Darden wasactively involved in the Agency’s training pro-gram; however, she had to stop attending be-cause she was missing too many days. Shefeels supported by her welfare-to-work casemanager; however, she does not feel sup-ported by her caseworker in the welfare of-fice. She states that the people at the welfareoffice are “nasty” and that they really do notwant to “see you succeed.” She reports havingto make numerous visits to the welfare officeto submit paperwork that “they already have.”
Housing
The family’s apartment is subsidized by theDepartment of Housing and Urban Develop-ment. It is located in a high-crime area, andthe unit is cramped, with minimal light, peel-ing paint, and leaky ceilings. There is also ev-idence of roaches and mice. The family livesnear a bus line, which enables them to travelto the children’s schools, the welfare-to-workoffice, church, grocery stores, the laundro-mat, and David’s medical appointments.
Income
Deborah is typical of many low-incomemothers in that she uses a combination ofearnings from work and welfare to make endsmeet. Her income includes monies from herpart-time job, a public assistance grant, foodstamps, and Supplemental Security Income.Her expenses include, but are not limited to,subsidized rent, utilities (gas, electric), a land-line phone and a cell phone, transportation,groceries, daycare, clothing, and laundry. Typ-ically, her expenses exceed her income.
Social supports
Ms Darden’s mother is able to assist occa-sionally with visits to David’s school to changehis diapers. Ms Darden feels supported byher welfare-to-work case manager and has astrong connection with a community church,although she does not attend regularly.
Mother’s health
Ms Darden expressed that it was extremelydifficult for her to care for her children, par-ticularly David, in addition to meeting the de-mands of her job. She feels like she “never getsa break from caretaking . . .” and expressedthat she often feels like she is on the vergeof having a breakdown. She has been di-agnosed with depression and sees a thera-pist who has recommended medication. MsDarden is resistant to taking the medicationeven though she stated at one point she “criedfor a week straight” and could not get outof bed to change her clothes, much less carefor her children. She also has been diagnosedwith anemia, asthma, and diabetes.
Strengths
The family is tight-knit, and all family mem-bers care about each other immensely. MsDarden has social supports who she feelsare reliable, although somewhat limited intheir ability to assist with her problems. MsDarden has a high school education and agood work history. She is interested in obtain-ing additional education and/or training, andshe has good parenting skills.
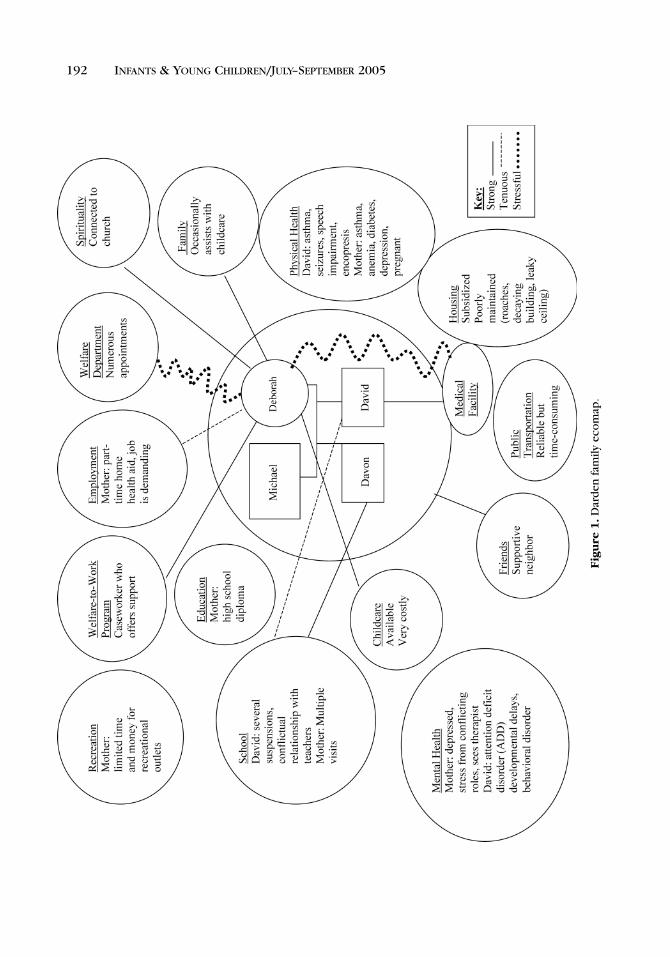
As the case study and ecomap (Fig 1) il-lustrate, the needs of the Darden family arevaried and complex. It is apparent that thereare several systems that affect their lives. Al-though Deborah Darden and her children areconnected to various human service agencieswithin their community, these agencies gen-erally do not coordinate with each other andoften have different expectations regardingMs Darden’s multiple roles, including mother,worker, and recipient of public assistance. Forexample, the preschool program has expecta-tions that Ms Darden should be available for
LWW/IYC lwwj111-03 June 4, 2005 3:52 Char Count= 0
192 INFANTS & YOUNG CHILDREN/JULY–SEPTEMBER 2005
Fig
ure
1.D
ard
enfa
mily
eco
map
.

LWW/IYC lwwj111-03 June 4, 2005 3:52 Char Count= 0
Exploring Mental Health Outcomes 193
meetings concerning her child’s care; how-ever, these meetings occur during businesshours when Ms Darden is expected to be atwork. Because she works with clients in theirhome, Ms Darden is able to occasionally ne-gotiate her schedule so that she can makemedical appointments during the day; how-ever, when this type of negotiation occurs,she often feels obligated to make up the timeby doing tasks outside of normal patient careduties, such grocery shopping and laundry.These tasks are typically time-consuming andher job offers no protection for her when sheis engaged in such activities since they do notcondone them and are unaware that this ne-gotiation is occurring. In addition, Ms Dardenis a part-time employee and is not eligible forbenefits such as paid time off and medicalinsurance.
Problems also develop when systems donot effectively communicate. For example,because the preschool nurse is part-time, shehas not been made aware of the treatment thatthe doctor has recommended for dealing withDavid’s encopresis. As a result, the center hasnot been able to actively reinforce the doctor’streatment recommendations and David is notreceiving consistent care. Ms Darden is alsoexpected to interface with multiple systems,and the differing expectations of these agen-cies and individuals cause great stress. As aresult, she becomes easily overwhelmed, andrequests like another medical appointment oran unpredictable asthma attack causes her al-ready fragile system to become unbalanced,and her physical and mental health to suffer.
DISCUSSION AND IMPLICATIONS FORPOLICY AND PRACTICE
The Darden case study highlights the 3main factors that are presented here as be-ing especially relevant to maternal health out-comes for women who are poor and havechildren with disabilities: resources, hassles,and maternal employment. These factors arevastly understudied, yet they are highly salientin the aforementioned ecological model. Im-
plications for policy and practice, on both mi-cro and macro levels, will be presented for all3 areas.
Family resources
David is clearly an example of an “expen-sive child in a poor family.” David’s encopre-sis means that his mother is constantly wash-ing sheets and pajamas. While Ms Darden’smother is occasionally available to visit theschool to change David’s diapers, this is aweak resource at best, as the grandmotherherself is in poor health. The potential ben-efits of increased resources for Ms Darden’smental health is suggested by the welfare-to-work interventions cited earlier and is alsomade clear by Ms Darden herself who said thatshe often feels on the verge of a breakdown asa result of so many demands on her. Six spe-cific recommendations for increasing this fam-ily’s resources are
1. Increased linkages with communityresources. Ms Darden could clearly benefitfrom an influx of additional resources fromthe community. For example, perhaps David’spreschool could participate in a foster grand-parent program, so Ms Darden and her motherwould need to go to the school less frequently.David’s service coordinator at school couldalso help connect them with community re-sources that provide diapers or help them ob-tain donated sheets or pajamas. Assistance inthis area would help to reduce the amount oflaundry that needs to be done on a daily basisin addition to decreasing the amount of timeand costs associated with washing clothes.
2. Increase knowledge and utilization ofrespite services. Ms Darden said that she“never gets a break from caretaking.” Both herwelfare-to-work case manager and her son’sservice coordinator should be able to connecther with respite care services. One resourcefor locating respite services is the ARCH Na-tional Respite Network and Resource Center,http://www.archrespite.org/. This is extremlyimportant as research clearly demonstratesthat use of respite care is associated withlower levels of caregiver stress and burnout(Cowen & Reed, 2002).
LWW/IYC lwwj111-03 June 4, 2005 3:52 Char Count= 0
194 INFANTS & YOUNG CHILDREN/JULY–SEPTEMBER 2005
3. Increase child care subsidies for fami-lies of children with special needs to reflectmarket rates for children with special needs(Rosman, Yoshikawa, & Knitzer, 2002). MsDarden paid an extra $250 per month aboveher subsidy for David’s child care. In theirfocus group study of welfare recipients withchildren with special needs, LeRoy andJohnson (2002) found that the averagehourly rate for specialized care was $4.80 inMichigan, while the subsidy was only $2.95per hour, regardless of whether or not achild had special needs. As research hasconsistently shown, financial hardship isa key indicator of poor mental health forindividuals in poverty (Chun-Chung Chow,Jaffee, & Snowden, 2003).
4. Education of early intervention special-ists. It is obvious from the case study thatthere are virtually no linkages between earlychildhood facilities and welfare agencies.Local welfare offices and welfare-to-work pro-grams should be in collaboration with agen-cies that service children with special needs.Once early childhood workers become fa-miliar with the goals and demands of pub-lic assistance offices, they will be in a betterposition to offer information to mothers or ad-vocate for them to receive exemptions basedon the mother’s or child’s physical and/ormental needs.
5. Mental health specialization of earlychildhood intervention specialists. Most earlychildhood facilities subscribe to the philoso-phy that children with special needs are bestserved when families are functioning at opti-mal capacity and are able to actively partici-pate in their children’s educational process.Making the family the focus of early childhoodcare ensures that the development of thesechildren is supported both in and outside ofthe home. Currently, early childhood agenciesare not equipped to address the needs of care-takers who are in need of substantial mentalhealth services.
For low-income mothers who are in need ofmental health services, the addition of case-workers who are skilled in the identificationand treatment of mental health issues can aid
in the early detection of the mental healthneeds of caretakers. As most developmentalliterature acknowledges, successful outcomesof children are in a large part dependent onthe context that parents are able to create(Ramey, 2002). To date, there are minimalwelfare-to-work agencies (Derr, Hill, & Pavetti,2000) or early childhood agencies that havea systematic approach to screening and as-sessing mental health needs of low-incomewomen. If early intervention workers can betrained to recognize the symptoms of com-mon mental health issues such as depression,improved family functioning, including bettercare for children, may be realized.
6. Provision of clinical case managementservices. Mothers who are identified as need-ing more support can be assigned a clinicalcase manager who is trained to work withwomen who are in need of more support.Issues such as time management, transporta-tion assistance, discharge planning, and navi-gation of multiple systems can be facilitatedby a specially trained clinical case managerwho is knowledgeable regarding issues thatimpact families in poverty and families whocare for children with special needs. Empha-sis should be on the development of an on-going relationship with the family. The clini-cal case manger can also help facilitate discus-sion among various agencies that work withthe family to ensure that all of the systems thatimpact the family are working collaboratively.Furthermore, any competing or conflictingagency ideologies can be discussed and treat-ment recommendations made that are satis-factory to all agencies involved in the care ofthe family unit.
Service utilization and associated hassles
Ms Darden was also very explicit about thelevel of hassles in her life. Not only is it com-mon sense that hassles are related to men-tal health but Rosman (2003) begins to sug-gest an empirical link as well. Hassles can bereduced both within individual systems andbetween systems. Three specific recommen-dations for reducing hassles are
LWW/IYC lwwj111-03 June 4, 2005 3:52 Char Count= 0
Exploring Mental Health Outcomes 195
1. Within individual services, ensuringthat the steps necessary to obtain or main-tain one particular service are not exces-sively cumbersome. Ms Darden’s statementthat she frequently makes visits to the wel-fare office to provide paperwork they “alreadyhave” demonstrates the importance of mak-ing poverty-related services easier to access.The hassles involved with poverty-related ser-vices need to be minimized so as not toovershadow the benefits. For example, intheir qualitative study of welfare recipientswho were part of the Project on Devolutionand Urban Change, Clampet-Lundquist, Edin,London, Scott, and Hunter (2003) discussthe differences between the Food Stampprograms in Cleveland and Philadelphia. InPhiladelphia, individuals had to provide ver-ification of their eligibility for Food Stampson a monthly basis, while in Cleveland,this paperwork had to be completed quar-terly. They found that this seemingly smalldifference had very real impacts on thelives of women in their study, with womenin Philadelphia reporting frequent prob-lems with the monthly reporting, stemmingfrom both their own difficulties keeping upwith the paperwork and from caseworkererror.
2. Create “one-stop shopping” for bothdisability- and poverty-related services. Mak-ing it possible for families to access multi-ple services in one location would better fa-cilitate families’ access to multiple services,as well as allowing for different types ofservices and service providers to commu-nicate with each other. A “one-stop shop-ping” model to services would mean thatfamilies could apply for benefits at early in-tervention or preschool centers, and programcaseworkers for antipoverty programs couldbe located at centers that provide disability-related services. Examples of these types ofapproaches already exist in the welfare litera-ture: in Oregon and Kentucky, mental healthservice providers are colocated in welfare of-fices; in California, CalWORKS offices housenot only welfare caseworkers but also pub-lic health nurses who are knowledgeable in
parenting and child development (Rosman,McCarthy, & Woolverton, 2001); and inMontgomery County, Ohio, more than 40agencies, nonprofits and businesses, are allhoused in a single job center to provideservices related to welfare, health, housing,children, employment, and veterans (Yates,1998). Richer, Kubo, & Frank (2003) discussthe potential of one-stop centers funded bythe Workforce Investment Act of 1998 to pro-vide information about a range of work sup-port programs, as well. Examples also ex-ist that follow the family resource centermodel. In the Orange County area of NorthCarolina, the Chapel Hill Training-OutreachProject manages 5 family resource centers.These are central locations in communitiesthat house a variety of programs and ser-vices ranging from children’s health servicesto preschool and literacy programs to ser-vices related to domestic issues, such as finan-cial planning, parenting education, and hous-ing assistance (Chapel Hill Training-OutreachProject, Inc., n.d.).
One-stop shopping should also include ser-vices for the adult caregiver. While early inter-vention staff members are competent in ad-dressing the needs of children, the parents’needs often go unidentified. In order to moreeffectively support the mental health needsof caregiving low-income women, early child-hood specialists must understand the types ofchallenges that low-income women face. Inaddition to understanding these needs, work-ers must be able to refer women out if theyare unable to provide services in their own fa-cilities. In light of the fact that the “typical”mother caring for a child with special needshas to interface with multiple systems, and isoften overburdened, it makes sense to limitthe amount of time and energy spent access-ing mental health services. To expedite thisprocess, the co-location of mental health facil-ities in early intervention agencies would behelpful. A realistic way that this could occurwould be for early childhood agencies to col-laborate with welfare offices, using welfare-to-work funding to expand their existingsystems.

LWW/IYC lwwj111-03 June 4, 2005 3:52 Char Count= 0
196 INFANTS & YOUNG CHILDREN/JULY–SEPTEMBER 2005
3. Communication and assistance be-tween disability- and poverty-related ser-vices. Ms Darden and her family received mul-tiple services, and there are many instances intheir story where it is clear that those serviceswere not communicating with each other.For example, the preschool serving David ex-pected Ms Darden to be able to attend meet-ings at times when her welfare-to-work casemanager expected her to be at work. AsRosman et al. (2002) explain, possible strate-gies for improving communication and col-laboration include sharing records betweenpoverty-related service providers and earlyintervention/special education systems (withparental consent) (Rosman & Knitzer, 2001;Rosman et al., 2001); allowing families tohave one service plan that would incorporategoals from multiple systems (Rosman et al.,2001; Woolverton, McCarthy, Schibanoff, &Schulzinger, 2000); and putting systems inplace for representatives of the multiple agen-cies that serve families on TANF to communi-cate on a regular basis (Derr et al., 2000).
Maternal employment
Ms Darden was somewhat fortunate in thatshe was able to create, to some extent, herown flexible work schedule. However, be-cause this flexibility was not condoned byher employer, she had no protection for her-self. For Ms Darden, it was a constant jugglingact between her children’s needs and her em-ployment that was mandated by her welfare-to-work program. This is in keeping withChase-Lansdale’s (1998) concerns about thepotential negative effect of employmentwhen it is not entered voluntarily. Three spe-cific recommendations for improving the roleof work in the lives of poor women with chil-dren with special needs are
1. For families receiving welfare, createbroader definitions of work, as well asbroader definitions of and application ofexemptions. Without adequate supports foremployment, physical and mental healthproblems are exacerbated and can lead to in-effectual care of children (Lloyd, 2002). Forfamilies who are attempting to meet wel-
fare work requirements, this may mean cre-ating broader definitions of what qualifies asemployment, such as allowing caregiving tosubstitute for work. Many states do allow care-giving as an alternative to work, although re-search has documented that mothers are of-ten unaware that the option exists (Lloyd,2002). This type of model recognizes thathelping families to maintain their carefullyconstructed routines and balances will help toreduce both parental stress and family levelsof risk. One example of a program model thatchallenges traditional notions of what quali-fies as work and instead meets the women“where they are” is Project Match, a pro-gram that began in the Cabrini-Green housingproject in Chicago. In Project Match, a “stepup” model is used in which women movethrough a ladder of economic independence,from things as basic as volunteering in theirchild’s Head Start classroom all the way upto work. This model provides women withattainable goals and a clear course to follow(Herr, Halpern, & Majeske, 1995; for moreinformation, see http://www.pmatch.org). Fi-nally, lengthening the amount of time thatwomen are eligible to receive TANF or stop-ping the TANF clock for women who are per-forming caretaking duties are also sensitiveand viable options that welfare-to-work agen-cies can employ.
While, as of 1999, 26 states offered exemp-tions to women “caring for a disabled house-hold member” (State Policy DocumentationProject, 2000), many women and their caseworkers are not aware that these exemptionsexist. When they do know that exemptionsare available, they are not clear regarding thetypes of conditions that enable them to qual-ify (Lloyd, 2002). In addition, because of thedisconnect between public assistance appli-cation sites and training sites, coordination ofexemptions, that is, who is eligible and howexemptions are documented, is inconsistentat best.
2. More education for employers concern-ing the specific needs of families who havechildren with special needs. Because low-income women are typically employed in jobs

LWW/IYC lwwj111-03 June 4, 2005 3:52 Char Count= 0
Exploring Mental Health Outcomes 197
that do not allow for much autonomy, it isimportant that employers receive training re-garding the inordinate number of demandswomen face when living in poverty and car-ing for a child with special needs. Chronichealth conditions and disabilities have uniquepresentations based on the individual, and acookie cutter, one-size-fits-all approach willprove to be ineffective for those who arejuggling the demands of work and caretak-ing. Linkages between welfare-to-work train-ing sites, agencies that employ women whoparticipate in these programs, and medical fa-cilities is one way to establish ongoing dia-logue regarding the individualized needs ofthese women and their children.
Collaborative models that are geared to-ward employer education and the develop-ment of proactive versus reactive responses tothe needs of families with special needs canhelp identify some of the overarching issuesthat families face. In addition, these collabo-rations will allow for advance planning whenemergencies do occur.
3. The creation of more flexible employ-ment that is supported. Lastly, considera-tions such as those identified by Bernheimer,Weisner, and Lowe (in press) and Lloyd (2002)point to the importance of making allowancesfor basic needs like time to make telephonecalls, leave for activities like attendance atmeetings outside of work such as school con-ferences, and the ability to attend medicaland welfare appointments. Policies that alloweducation and/or training or a reduction ofwork hours may also provide mothers withthe flexibility they need to meet their chil-
dren’s unique demands (Frieden, 2003; Ros-man et al., 2002).
CONCLUSION
As this article demonstrates, very little iscurrently known about the day-to-day needsof low-income caregivers of children with spe-cial needs and the way that a mother’s men-tal health is affected by and impacts children’sdevelopment. These families are not typicallythe focus of research in either the disabilityfield or the poverty field. However, a better,more sophisticated understanding of the waythat families develop and sustain caregiving inconjunction with the demands of the living inpoverty is critical if mothers are to be com-petent and skilled partners in their children’scare.
When making assessments, interventions,and/or developing polices, one must under-stand the functioning of all of the systems thata family must interact with on an everyday ba-sis. Each system has its own line of authority,norms, rules and expectations. This article be-gins to examine the ways in which systemsthat have not previously been studied may beplaying an important role in determining men-tal health outcomes for women who are poorand have young children with disabilities. Itis vital that exploration of these systems con-tinue, that is, how they help families, howtheir policies and practices can be improved,and how they can best serve to help—nothurt—families that are living with the con-founding challenges of poverty and childrenwith special needs.
REFERENCES
American Academy of Pediatrics, Committee on Childrenwith Disabilities. (2001). Developmental surveillanceand screening of infants and young children. Pedi-atrics, 108, 192–195.
Bernheimer, L. P., Weisner, T. S., & Lowe, E. D. (2003). Im-pacts of children with troubles on working poor fami-lies: Experimental and ethnographic evidence. MentalRetardation, 41, 403–419.
Bronfenbrenner, U. (1979). The ecology of human devel-opment. Cambridge, MA: Harvard University Press.
Chapel Hill Training-Outreach Project, Inc. (n.d.). OrangeCounty Family Resource Centers. Retrieved October9, 2003, from http://www.chtop.org/raising.htm
Chase-Lansdale, P. L. (1998). How Developmental Psy-chologists Think About Process and Child Develop-ment in Low Income Families. Paper presented at theFamily Process and Child Development in Low IncomeFamilies Pre-conference, Northwestern/University ofChicago Joint Poverty Research Center, Chicago,IL.
LWW/IYC lwwj111-03 June 4, 2005 3:52 Char Count= 0
198 INFANTS & YOUNG CHILDREN/JULY–SEPTEMBER 2005
Chun-Chung Chow, J. Jaffee, K., & Snowden, L. (2003).Racial/ethnic disparities in the use of mental healthservices in poverty areas. American Journal of PublicHealth, 93, 792–797.
Clampet-Lundquist, S., Edin, K., London, A. S., Scott, E.,& Hunter, V. (2003). “Making a way out of no way:”How mothers meet basic family needs while movingfrom welfare to work. Manpower Demonstration Re-search Corporation Work Paper Series, 14.
Cowen, P. S., & Reed, D. A. (2002). Effects of respitecare for children with developmental disabilities: Eval-uation of an intervention for at risk families. PublicHealth Nursing, 19, 272–283.
Crnic, K., Friedrich, W. N., & Greenberg, M. T. (1983).Adaptation of families with mentally retarded chil-dren: A model of stress, coping, and family ecology.American Journal of Mental Deficiency, 88, 125–138.
Derr, M. K., Hill, H., & Pavetti, L. (2000). Addressing men-tal health problems among TANF recipients: A guidefor program administrators. Washington, DC: Math-ematica Policy Research, Inc.
Dodson, L., Manuel, T., & Bravo, E. (2002). Keeping jobsand raising families in low-income America: It justdoesn’t work. Cambridge, MA: Radcliff Institute forAdvanced Study, Harvard University.
Frieden, L. (2003). TANF and disability: Importance ofsupports for families with disabilities in welfare re-form. Retrieved April 2, 2003, from http://www.ncd.gov/newsroom/publications/familysupports.html
Gibson, C. M., & Weisner, T.S. (2002). “Rational” and eco-cultural circumstances of program take-up among low-income working parents. Human Organization, 61,154–166.
Glidden, L. M. (2002). Parenting children with de-velopmental disabilities: A ladder of influence.In J. G. Borkowski, S. L. Ramey, & M. Bristol-Power (Eds.), Parenting and the child’s world:Influences on academic, intellectual, and social-emotional development (pp. 329–344). Mahwah, NJ:Erlbaum.
Hebbeler, K., Wagner, M., Spiker, D., Scarborough, A.,Simeonsson, R., & Collier, M. (2001). A first look atthe characteristics of children and families enter-ing early intervention services. Retrieved August 20,2003, from http://www.sri.com/neils/reports.html
Herr, T., Halpern, R., & Majeske, R. (1995). Bridg-ing the worlds of Head Start and welfare-to-work:Building a two-generation self-sufficiency programfrom the ground up. In S. Smith (Ed.), Two gen-eration programs for families in poverty: A newintervention strategy (pp. 161–197). Norwood, NJ:Ablex.
Hodapp, R. (2001). Commentary on “Children with dis-abilities.” Monograph of the Society for Research inChild Development, 66.
Hogan, D. P., & Msall, M. E. (2002). Family structure andresources and the parenting of children with disabil-
ities and functional limitations. In J. G. Borkowski,S. L. Ramey, & M. Bristol-Power (Eds.), Parenting andthe child’s world: Influences on academic, intellec-tual, and social-emotional development (pp. 311–327). Mahwah, NJ: Erlbaum.
Howard, E. C. (2003, April). Employment, social support,and well-being among low-income, minority moth-ers. Poster session presented at the biennial meetingof the Society for Research in Child Development,Tampa, FL.
Jackson, A. P., & Huang, C. C. (2000). Parenting stress andbehavior among single mothers of preschoolers: Themediating role of self-efficacy. Journal of Social Ser-vice Research, 26, 29–42.
Kearney, J. R., Grundmann, H. F., & Gallicchio, S. J. (1994).The influence of social security benefits and SSI pay-ments on the poverty status of children. Social Secu-rity Bulletin, 57, 27–43.
Knox, V., Miller, C., & Gennetian, L. A. (2000). Reformingwelfare and rewarding work: A summary of the fi-nal report on the Minnesota Family Investment Pro-gram. New York: Manpower Demonstration ResearchCorporation.
Lee, S., Oh, G., Hartmann, H., & Gault, B. (2003, Septem-ber). The impact of disabilities on mothers’ workparticipation: examining differences between singleand married mothers. Paper presented at the HHS-ASPE/Census Bureau Research Development GrantsConference, Washington, DC.
Lennon, M. C., Blome, J., & English, K. (2001). Depressionand low-income women: Challenges for TANF andwelfare-to-work policies and programs. New York:Research Forum on Children, Families and the NewFederalism.
LeRoy, B., & Johnson, D. M. (2002). Open road or blindalley? Welfare reform, mothers, and children with dis-abilities. Journal of Family and Economic Issues, 23,323–337.
Lloyd, C. (2002). A mother’s work is never done: A crit-ical analysis of low-income women’s roles as finan-cial provider and caretaker of children with specialneeds (Doctoral dissertation, University of Delaware,2002). Dissertation Abstracts International, 64 (01),298A.
Lu, H. (2003). Low-income children in the UnitedStates (2003). Retrieved November 11, 2003, fromhttp://www.nccp.org/pub cpf03.html
McDonald, T. P., Poertner, J., & Pierpont, J. (1999). Pre-dicting caregiver stress: An ecological perspective.American Journal of Orthopsychiatry, 69, 100–106.
Meyers, M. K., Brady, H. E., & Seto, E. Y. (2000). Expensivechildren in poor families: The intersection of child-hood disabilities and welfare. San Francisco, CA: Pub-lic Policy Institute of California.
Meyers, M. K., Lukemeyer, A., & Smeeding, T. M. (1996).Work, welfare, and the burden of disability: Caringfor special needs of children in poor families. IncomeSecurity Policy Series, Paper No. 12. Syracuse, NY:

LWW/IYC lwwj111-03 June 4, 2005 3:52 Char Count= 0
Exploring Mental Health Outcomes 199
Center for Policy Research, Maxwell School of Citizen-ship and Public Affairs, Syracuse University.
Ramey, S. L. (2002). The science and art of parenting.In J. G. Borkowski, S. L. Ramey, & M. Bristol-Power(Eds.), Parenting and the child’s world: Influences onacademic, intellectual, and social-emotional devel-opment (pp. 47–71). Mahwah, NJ: Erlbaum.
Richer, E., Kubo, H., & Frank, A. (2003). All in one stop?The accessibility of work support programs at one-stop centers. CLASP Policy Brief No. 3.
Rosman, E. A. (2003). At the crossroads of poverty anddisability: An ecological approach to predicting ma-ternal mental health outcomes in families who arepoor and have young children with disabilities [Doc-toral dissertation]. New York: New York University.
Rosman, E. A., & Knitzer, J. (2001). Welfare reform: Thespecial case of young children with disabilities andtheir families. Infants and Young Children, 13, 25–35.
Rosman, E. A., Yoshikawa, H., & Knitzer, J. (2002). To-wards an understanding of the impact of welfare re-form on children with disabilities and their families:Setting a research and policy agenda. Social Policy Re-port, XVI (IV).
Rosman, E. A., McCarthy, J., & Woolverton, M. (2001).Focusing on families in welfare reform reauthoriza-tion: Adults with mental health needs and childrenwith special needs. Washington, DC: GeorgetownUniversity.
Scorgie, K., Wilgosh, L., & McDonald, L. (1998). Stressand coping in families of children with disabilities: An
examination of recent literature. DevelopmentalDis-abilities Bulletin, 26(1), 22–42.
Skinner, D., Slattery, E., Lachicotte, W., Cherlin, A.,& Burton, L. (2002). Disability, health coverage, andwelfare reform. Washington, DC: The Kaiser Commis-sion on Medicaid and the Uninsured.
Sontag, J. (1996). Toward a comprehensive theoreticalframework for disability research: Bronfenbrenner re-visited. Journal of Special Education, 30, 319–344.
State Policy Documentation Project. (2000). Time limitexemptions (Part 1 of 2). Retrieved November 19,2003, from http://www.spdp.org
Wise, P. H., Wampler, N. S., Chavkin, W., & Romero, D.(2002). Chronic illness among poor children enrolledin the Temporary Assistance for Needy Families pro-gram. American Journal of Public Health, 92, 1458–1461.
Woolverton, M., McCarthy, J., Schibanoff, S., &Schulzinger, R. (2000). Welfare reform: Explor-ing opportunities for addressing children’s mentalhealth and child welfare issues. Washington, DC:National Technical Assistance Center for Children’sMental Health, Center for Child Health and Men-tal Health Policy, Georgetown University ChildDevelopment Center.
Yates, J. (1998). Delivering human services through “co-location” and “one-stop shopping.” Washington, DC:The Finance Project.
Yoshikawa, H., & Hsueh, J. (2001). Child developmentand public policy: Toward a dynamic systems perspec-tive. Child Development, 72, 1887–1903.
Lists of current articles: http://depts.washington.edu/isei/iyc/iyc_comments.html
Back to the list of previous articles: http://depts.washington.edu/isei/iyc/iyc_previous.html



![homelessness nyc - New York – São Paulo Exchange | The ... · 2/6/2010 · homelessness [nyc] homelessness ... ... 199 2 199 3 199 4 199 5 199 6 199 7 199 8 199 9 200 0 200 1 200](https://img.pdfslide.us/doc/110x75/5c622b0c09d3f2223c8b45ae/homelessness-nyc-new-york-sao-paulo-exchange-the-262010-homelessness.jpg)
















![[XLS]... Get Doc - Louisiana Department of Environmental Qualitydeq.louisiana.gov/assets/docs/Forms/Solid-Waste... · Web view11/28/1983 186 187 189 190 192 194 197 199 201 204 206](https://img.pdfslide.us/doc/110x75/5b0663eb7f8b9a93418cb749/xls-get-doc-louisiana-department-of-environmental-view11281983-186-187.jpg)








