Embed Size (px)
Citation preview

Confidential: For Review O
nly
Inequalities in Access to Total Hip Arthroplasty for Hip
Fracture: Population Based Study
Journal: BMJ
Manuscript ID: BMJ.2015.028371
Article Type: Research
BMJ Journal: BMJ
Date Submitted by the Author: 28-Jul-2015
Complete List of Authors: Perry, Daniel; University of Liverpool, Institute of Translational Medicine Metcalfe, David; Harvard Medical School, Center for Surgery and Public Health Griffin, Xavier; Warwick Medical School, Warwick Orthopaedics Costa, Matthew; University of Oxford, Nuffield Department of
Orthopaedics, Rheumatology and Musculoskeletal Sciences (NDORMS)
Keywords: Hip Fracture, Inequalities, Total Hip Replacement, Arthroplasty, Fracture, Osteoporosis, Surgery, Orthopaedics
https://mc.manuscriptcentral.com/bmj
BMJ

Confidential: For Review O
nlyInequalities in Access to Total Hip Arthroplasty for Hip Fracture:
Population Based Study
Daniel C Perry, David Metcalfe, Matthew L Costa.
Warwick Clinical Trials Unit, University of Warwick, Coventry, CV4 7AL, UK.
Daniel C Perry NIHR clinician scientist in orthopaedic surgery Institute of
Translational Medicine, University of Liverpool, Liverpool, L12 2AP, UK.
David Metcalfe research fellow Center for Surgery and Public Health, Harvard
Medical School, Boston, MA 02115, USA.
Xavier Griffin NIHR clinical lecturer Warwick Clinical Trials Unit, University of
Warwick, CV4 7AL
Matthew Costa professor of orthopaedic trauma surgery Nuffield Department of
Orthopaedics, Rheumatology, and Musculoskeletal Sciences, University of Oxford,
Oxford, OX3 7HE, UK.
Correspondence to: DC Perry
Daniel Perry designed the study, performed the analysis and drafted the paper.
David Metcalfe contributed to the data analysis, interpretation of results, and
draft manuscript. Matthew Costa and Xavier Griffin contributed to the design of
the study, interpretation of results and critically appraised the paper. All authors
have approved the final manuscript. Daniel Perry is guarantor.
No external funding was received for this work.
Data sharing: Pursuant to the terms of our data sharing agreement with the
National Hip Fracture Database we regret that no additional data can be made
available by the authors.
Page 1 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyAbstract
Objectives To determine whether the decision to offer total hip arthroplasty
(THA) to individuals with a displaced intracapsular fracture of the femoral neck
is based on national guidelines, or if there are systematic inequalities in access to
THA.
Design Observational cohort study using the UK National Hip Fracture Database
(NHFD).
Setting All hospitals that treat adults with hip fractures in England, Wales, and
Northern Ireland.
Main outcome measures Provision of THA to patients considered eligible under
criteria published by the National Institute for Health and Care Excellence (NICE).
Participants All patients within the NHFD that were aged >60 and received
operative treatment for a non-pathological displaced intracapsular hip fracture
between 1st July 2011 and 31st April 2015.
Results 114,119 hip fracture patients were included, 11,683 (10.2%) of which
underwent THA. 32.0% that appeared to satisfy the NICE criteria received a THA,
and only 42.0% of patients that underwent THA actually satisfied the criteria. A
recursive-partitioning algorithm found that the NICE eligibility criteria did not
optimally explain which patients underwent THA. A model with superior
explanatory power drew distinctions that are not supported by NICE: age >77
years and use of a stick for ambulation. Amongst patients satisfying the NICE
eligibility criteria for THA, logistic regression demonstrated that access to THA
was limited based on higher age (OR 0.88, 95% CI 0.87 to 0.88), lower
Abbreviated Mental Test Score (OR 1.44, 95% CI 1.34 to 1.54), higher American
Society of Anesthesiologists (ASA) score (OR 0.74, 95% CI 0.66 to 0.84), male sex
(OR 0.85, 95% CI 0.77 to 0.93), walking with a stick (0.32, 95% CI 0.28 to 0.35),
and quintiles of increasing socioeconomic area deprivation (1.0 (ref) lowest
quintile vs. highest quintile 1.30, 95% CI 1.13 to 1.51). Patients receiving
treatment during the working week were more likely to receive THA than those
at the weekend (OR 1.12, 95% CI 1.04 to 1.21).
Conclusions There are wide disparities in access to THA amongst individuals
with hip fractures and compliance with NICE guidance is poor. Patients with
higher levels of socioeconomic deprivation and requiring surgery at the weekend
Page 2 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyare less likely to receive THA. Inconsistent compliance with NICE
recommendations means that the optimal treatment for older adults with hip
fractures can depend on where and when they present to hospital.
Page 3 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyIntroduction
There are over 70,000 hip fractures in the United Kingdom every year, with a
combined health and social cost of £2 billion.1 Demographic projections estimate
that the annual incidence will increase to over 100,000 by 2020.2 Mortality is
high, with 8.5% of patients deceased within 30 days of hip fracture.3
A number of initiatives have been credited with improving hip fracture outcomes
in the UK.3 The National Hip Fracture Database (NHFD) was established in 2004,
by the British Orthopaedic Association (BOA) and the British Geriatrics Society
(BGS), with the aim of improving hip fracture outcomes through continuous
national clinical audit.4 The NHFD was supported by combined BOA/BGS clinical
guidance5 and later by the Best Practice Tariff for Hip Fracture which rewards
NHS organisations for meeting defined quality standards, including surgery
within 36 hours of arrival at hospital.6 These initiatives have been associated
with improved hip fracture outcomes, including a fall in 30-day mortality from
10.9% in 2007 to 8.5% in 2011.3
Displaced intracapsular hip fractures are at high risk of painful non-union and so
the recommended treatment is either hemiarthroplasty (HA) or total hip
arthroplasty (THA).7-9 In HA, the femoral head is replaced but, in THA, both the
femoral head and acetabulum are replaced. Although the risk-benefit profiles
vary between these two operations, it has been shown that hip fracture patients
undergoing THA have better function and less need for revision surgery than
HA.7 9-11 In June 2011, the National Institute for Health and Care Excellence
(NICE) recommended that THA should be offered to patients with a displaced
intracapsular hip fracture who are “(a) able to walk independently out of doors
with no more than the use of a stick (b) not cognitively impaired and (c)
medically fit for anaesthesia and the procedure”.8 The provision of THA to hip
fracture patients is not explicitly included as a quality indicator within the NHFD
and so the extent to which surgeons comply with this guideline is unknown.
Page 4 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyThis study sought to identify whether the decision to offer THA is based on
factors that are consistent with national recommendations, or if systematic
inequalities exist with regards access to THA for hip fracture.
Methods
An observational cohort study was performed using the NHFD. The study
protocol was approved by the Healthcare Quality Improvement Partnership
(HQIP) but research ethics committee approval was not sought for secondary
analysis of administrative data in line with Governance Arrangements for
Research Ethics Committee (GAfREC) guidelines.12
Data source
The NHFD is commissioned by the HQIP and captures over 95% of hip fractures
treated in England, Wales, Northern Ireland and the Channel Islands. Data
include patient characteristics, fracture pattern, surgical interventions, and
outcomes. These details are typically collected by specialist nurses within each
hospital that provide continuity of care to patients with hip fractures and
manage submissions to the NHFD.
Inclusion criteria
This study included all patients aged >60 years that presented to hospital
between 1st July 2011 and 31st April 2015 with a displaced intracapsular hip
fracture. 1st July 2011 was selected as one month following publication of NICE
Clinical Guideline 124.8 Patients were excluded if their fracture was coded as
“pathological”.
Variables and outcomes
Data cleaning involved several steps. Two patients had ages recorded as >115
years (both >1000 years) which were recoded to exclude this variable. In 27
(0.01%) cases, the Abbreviated Mental Test Score (AMTS) was not recorded as
an integer and so scores were rounded to the nearest integer. On 1st April 2014
the NHFD data collection tool was updated to record mobility differently within
Page 5 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlythe revised database. Earlier data were therefore mapped onto the new version
using an algorithm presented as Appendix A. In the event of hospital trust
reconfiguration (closure/merger), the hospital code at the time of data entry was
used. As a consequence, some hospitals only contributed data for a few months
prior to reconfiguration.
Variables extracted from the NHFD were age (whole years), sex, lower level
super output area (LSOA), date of admission, treating hospital, pre-morbid
mobility, American Society of Anesthesiologists (ASA) physical status
classification score, and AMTS. The ASA score ranges between 1 (healthy
patient) and 5 (moribund patient not expected to survive for 24 hours with or
without surgery). The AMTS is a test of ten questions (e.g. “what is your age?”),
which gives a score from 0 (zero answers correct) to 10 (all correct).
Deprivation scores for patients living in England were determined using the
Index of Multiple Deprivation (IMD) 2007. These scores reflect deprivation
related to income, health and disability, employment, barriers to housing and
services, living environment, education, and crime.13 IMD scores were generated
from LSOAs, which were then categorised into quintiles of deprivation based on
the population of the UK.
Day of the week was determined from the date of admission. In the UK, hip
fracture surgery usually takes place on the next available trauma operating list
which is the day following admission for most patients in the NHFD (>65%).
“Weekend” surgery was therefore identified by admission on a Friday or
Saturday.
Hospital case volume was analysed by decile and defined by the number of
displaced intracapsular fractures admitted to each centre over the study period.
Date of surgery was analysed as seven 6-month periods (1st July 2011 – 31st
December 2015) and one 4-month period (1st Jan 2015 – 31st April 2015).
Page 6 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyStatistical analysis
Guideline compliance was determined using a decision tree ordered to mirror
the NICE recommendations, i.e. based on mobility (mobile outdoors with or
without the use of a stick), cognition (defined as AMTS >8), and fitness for
anaesthesia (defined as ASA 1 or 2).
Recursive partitioning (RP) was used to determine the optimal decision tree that
explains current practice, i.e. to illustrate how the guidelines are being
interpreted. RP is a statistical technique for multivariable analysis that models
how variables are best organised to predict a given outcome (e.g. THA). In RP,
decision trees are built by identifying a variable that best splits the data into two
groups. RP defines a cut-off (split) for continuous or ordinal variables, to enable
the decision tree to correctly classify the maximum members of the population.
Categorical variables are similarly grouped in RP, to build a tree with the least
error. This process is then applied separately to each sub-group and continues
recursively until either a maximum number of steps are reached or no further
improvement is possible.14
RP was undertaken using the “rpart” function in R. The tree was built using 10-
fold cross validation and a negative complexity parameter to ensure that the
maximum tree was built. Predictors included in the model were age, sex,
mobility, AMTS, ASA, IMD quintile, and day-of-the-week of admission. The tree
was pruned using the complexity (“cp”) function of the smallest tree within one
standard error of the best functioning tree, i.e. the tree with the smallest xerror,
which was confirmed graphically. A pragmatic approach was also used to
consider the tree complexity and efficiency related to clinical practice.
Individuals that fulfilled the NICE criteria were further analysed to explore
factors associated with undergoing THA. An RP decision tree was constructed to
model differentiating between THA and no-THA in this subgroup. The treating
hospital was included as a factor variable, which allowed the partitioning
algorithm to select optimal cut-off points for best fit within the model.
Page 7 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyA mixed effects logistic regression model was constructed to explore factors
associated with access to THA amongst patients that fulfilled the NICE criteria.
Age, sex, date of surgery, AMTS, and ASA were included as continuous
predictors; and IMD quintile and weekend surgery as categorical predictors.
Weekend admission was then substituted for day of the week to explore this
predictor further in a second analysis. Hospital case volume was included as a
centre level fixed effect and the unique hospital identifier as a centre level
random effect.
Statistical analyses were performed using R and Stata v.10.0. p<0.05 was
adopted as the threshold for statistical significance.
Results
In the 46-month period between 1st July 2011 and 31st April 2015, 248,013 hip
fracture patients were recorded within the NHFD. 114,119 (46.0%) satisfied the
study criteria as they were aged >60 years and sustained a non-pathological
displaced intracapsular hip fracture. Within this group, 11,683 (10.2%)
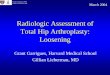
underwent THA. However, only 32.0% of the 21,193 that satisfied the NICE
criteria received a THA (Figure 1) and, of the 11,683 patients that did undergo
THA, only 4,903 (42.0%) satisfied the criteria.
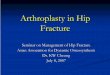
The RP algorithm identified ten terminal nodes (nine splits) as the most
predictive model, although this offered little improvement over five terminal
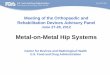
nodes (four splits) (Figure 2). The variable with the greatest importance was
patient age, with a cut-off of at 77 years defining the initial split (Figure 3). The
mobility split occurred between patients that ambulate independently and those
that required the use of a stick. The other important predictive variables were as
recommended by NICE, with splits occurring as predicted at ASA>3 and AMTS>8.
Using the decision tree, the unexplained variation in practice across the whole
dataset reduced from 12.9% (NICE guidelines) to 9.4% (recursive model).
Page 8 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
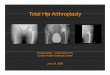
nlyAmongst the 21,193 patients fulfilling the NICE eligibility criteria, the RP
algorithm identified 20 terminal nodes (19 splits) to be the most efficient, though
after three splits (four terminal nodes) the complexity of the tree increased
markedly with little associated gain in efficiency (Figure 4). Age was again the
most significant predictor, with 79 years identifying the splitting point (Figure 5).
For patients aged 79 years and above, the treating hospital was the next most
important predictor (further details in Appendix B), followed by mobility (with
or without the use of a stick). Hospital variation amongst individuals fulfilling the
NICE guidelines was considerable (Figure 6). 77% of the variation in practice
could be explained using this RP algorithm.
Date of surgery demonstrated that there was a progressive increase in the
provision of THA for eligible individuals over the study period (Table 1).
Table 1: The proportion of eligible patients undergoing THA by time period.
Period Total number of individuals
undergoing THA / Total number of
individuals fulfilling NICE criteria.
Percentage
undergoing
THA
1st July 2011 – 31st Dec 2011 453/ 2,020 22%
1st Jan 2012 – 30th June 2012 649/ 2,409 27%
1st July 2012 – 31st Dec 2012 804/ 2,703 30%
1st Jan 2013 – 30th June 2013 942/ 3,041 31%
1st July 2013 – 31st Dec 2013 1,007/ 3,099 32%
1st Jan 2014 – 30th June 2014 1,104/ 3,077 36%
1st July 2014 – 31st Dec 2014 1,160/ 3,094 37%
1st Jan 2015 – 30th April 2015 661/ 1,089 38%
The logistic model (Table 2) showed that hospital volume declines did not effect
THA provision (OR 1.02, 95% CI 0.97 to 1.08). However, increasing age (0.88,
0.87 to 0.88), AMTS (1.41, 1.31 to 1.54), and ASA (0.74, 0.66 to 0.84) were
associated with fewer THAs, as was male sex (0.85, 0.77 to 0.93). Admissions
during the working week (Sunday-Thursday) had the highest rates of THA
provision (1.12, 1.04 to 1.21). There was a stepwise decrease in THA surgery
Page 9 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlywith increasing area level deprivation so that the most deprived quintile had
least access to THA (1.30, 1.13 to 1.51).
Table 2: Mixed effects logistic model to demonstrate those receiving a THA
amongst those deemed eligible using the NICE guidelines.
Variable OR (95% CI) P-value
Age (Years) 0.88 (0.87 to 0.88) <0.001
AMTS 1.44 (1.34 to 1.54) <0.001
ASA 0.74 (0.66 to 0.84) <0.001
Mobility
Walk independently without aids
Walk with the aid of 1 stick
1.0 (ref)
0.32 (0.28 to 0.35)
-
<0.001
Sex
Female
Male
1.0 (Ref)
0.85 (0.77 to 0.93)
-
0.002
Fracture Volume (Deciles) 1.02 (0.97 to 1.08) 0.46
Day of Admission
Friday
Saturday
Sunday
Monday
Tuesday
Wednesday
Thursday
1.0 (ref)
1.01 (0.88 to 1.16)
1.03 (0.89 to 1.19)
1.09 (0.95 to 1.26)
1.11 (0.96 to 1.27)
1.17 (1.02 to 1.35)
1.17 (1.02 to 1.34)
-
0.92
0.66
0.21
0.16
0.03
0.03
Weekday Admission* 1.12 (1.04 to 1.21) 0.01
Deprivation Quintile
1 – Most deprived
2 -
3 -
4 -
5 – Least deprived
1.0 (ref)
1.07 (0.932to 1.24)
1.20 (1.04 to 1.38)
1.28 (1.11 to 1.47)
1.30 (1.13 to 1.51)
-
0.39
0.01
<0.001
<0.001
Date of surgery (6-months) 1.13 (1.10 to 1.15) <0.001
Page 10 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
* “Weekend” was defined as a Friday or Saturday admission, as surgery most
commonly occurs on the day following admission. ‘Weekday’ was therefore defined
as Sunday-Thursday. “Weekend” was included in the logistic model as a
dichotomous variable and day-of-the-week excluded as collinear.
Discussion
This observational study used a large national dataset and has demonstrated
unexplained variation in access to THA following hip fracture. Access to THA is
influenced by a number of patient characteristics, including age, sex, AMTS, ASA,
socioeconomic status, and pre-fracture mobility. Other key determinants were
the treating hospital and the day-of-the week of admission. Access to THA
amongst eligible patients improved over the study period but remains both low
and variable.
Compliance with NICE recommendations
NICE was established in 1999 to promote evidence-based treatments and reduce
unexplained variation in care across the NHS, the so-called “postcode lottery”.15
In June 2011, NICE recommended that THA should be offered to patients with a
displaced intracapsular hip fracture who can walk independently outdoors (with
no more than a single mobility aid), are cognitively intact, and are medically fit to
undergo the operation. This guideline is consistent with a developing evidence
base, which suggests that THA leads to better functional outcomes than HA
following hip fracture7 9-11. However, our study found that variation in access to
THA persists across the NHS because of poor compliance with NICE guidelines.
There was substantial variation in compliance (0.1 to 60.0%) between hospitals.
As patient-level predictors were unable to account for this variation, it is likely to
reflect systematic differences in practice between centres.
The optimal recursive partitioning model suggested that surgeons might
consider factors that could be relevant even if not strictly included within the
NICE guidelines. For example, older patients were less likely to undergo THA, as
were those that mobilised using a stick compared to those mobilising
Page 11 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyindependently without aids. Although there is strong evidence that some hip
fracture patients benefit from THA7 9-11, its precise indications are not well
defined. Our model offers a glimpse into the collective judgment of orthopaedic
surgeons and could be used to help inform the development of future NICE
guidelines in the absence of higher-level evidence. It is nevertheless concerning
that deprivation quintile was inversely associated with access to THA. There are
many potential explanations for this observation, including patient preferences
and confounding factors. However, it is also possible that heuristic judgments
about which patients are sufficiently “independent” to benefit from THA could be
influenced by implicit surgeon bias. Social class biases have been shown to
influence treatment decisions across a range of settings16-18 and could raise a
barrier for patients that are otherwise eligible to undergo THA. This inverse
association risks exacerbating health inequalities and is a further reason to
promote clear, evidence-based, national guidelines.
Barriers to increased THA provision
One potential obstacle to delivering THA for all eligible hip fracture patients is
the availability of experienced hip surgeons. It is widely accepted that patients
undergoing elective THA by a low-volume surgeon have greater risks of
dislocation, need for revision surgery, post-operative complications, and death19-
23. For this reason, many orthopaedic surgeons do not perform THA for hip
fracture if this operation is not part of their routine elective practice. The limited
availability of suitably experienced hip surgeons might account for the reduced
THA access observed at weekends. This finding is important in the context of
recent proposals to introduce seven-day services across the NHS24. Although this
discussion is principally framed around increased weekend mortality25 26, timely
access to THA for fracture may also need to be addressed. Regionalisation of hip
fracture services is one possible means of ensuring equal access to THA
throughout the week. High hospital case volume was not however associated
with improved access to THA.
Strengths and limitations of study
Page 12 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyThe main strength of this study was its use of a dataset that captures almost
every (>95%) hip fracture treated in England, Wales, and Northern Ireland.
There were variables that aligned closely with the NICE eligibility criteria, which
permitted the recommended treatment algorithm to be mapped over the
administrative data recorded within the NHFD.
The principal limitation was that the NHFD does not record individual patient
comorbidities. Some of the variables in our analysis (e.g. age and deprivation)
could simply represent a tendency towards a greater comorbidity burden.
However, ASA score has been shown to have equivalent or even greater
predictive value for mortality and complications than standard comorbidity
measures, such as the Charlson Comorbidity Index)27-29. It is unlikely that
patients assigned an ASA score <2 (2 = “mild systemic disease”) were medically
unfit to undergo THA. The NHFD also does not include sufficient detail to
understand clinical decision-making at the individual patient level. For example,
it is possible that THA was discussed with some patients and HA chosen
following a balanced risk-benefit discussion. However, the inter-hospital
variation in compliance with NICE guidelines suggests the existence of
systematic problems with THA provision.
Conclusion
Compliance with NICE guidance on THA for hip fracture is poor, with many
eligible patients failing to undergo THA. There continues to be substantial inter-
hospital variation in practice, which is not readily explained by patient-level
differences. The limited provision of THA to patients from deprived areas and
those requiring treatment at the weekend are particular concerns as it is
unacceptable for such decisions to depend on when and where a patient seeks
treatment for their hip fracture. There have been substantial improvements in all
of the quality indicators measured by the NHFD since its creation in 2004.3 The
NHFD should consider reporting data on THA provision at the hospital-level to
help achieve greater consistency across the NHS.
Page 13 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyCompeting interests
All authors have completed the ICMJE uniform disclosure form at
www.icmje.org/coi_disclosure.pdf and declare: no support from any
organisation for the submitted work; no financial relationships with any
organisations that might have an interest in the submitted work in the previous
three years; no other relationships or activities that could appear to have
influenced the submitted work.
Licence
The Corresponding Author has the right to grant on behalf of all authors and
does grant on behalf of all authors, a worldwide licence
(http://www.bmj.com/sites/default/files/BMJ%20Author%20Licence%20Marc
h%202013.doc) to the Publishers and its licensees in perpetuity, in all forms,
formats and media (whether known now or created in the future), to i) publish,
reproduce, distribute, display and store the Contribution, ii) translate the
Contribution into other languages, create adaptations, reprints, include within
collections and create summaries, extracts and/or, abstracts of the Contribution
and convert or allow conversion into any format including without limitation
audio, iii) create any other derivative work(s) based in whole or part on the on
the Contribution, iv) to exploit all subsidiary rights to exploit all subsidiary rights
that currently exist or as may exist in the future in the Contribution, v) the
inclusion of electronic links from the Contribution to third party material where-
ever it may be located; and, vi) licence any third party to do any or all of the
above. All research articles will be made available on an Open Access basis (with
authors being asked to pay an open access fee—see
http://www.bmj.com/about-bmj/resources-authors/forms-policies-and-
checklists/copyright-open-access-and-permission-reuse). The terms of such
Open Access shall be governed by a Creative Commons licence—details as to
which Creative Commons licence will apply to the research article are set out in
our worldwide licence referred to above.
Page 14 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyTransparency Declaration
Daniel Perry (the manuscript’s guarantor) affirms that the manuscript is an
honest, accurate, and transparent account of the study being reported; that no
important aspects of the study have been omitted; and that any discrepancies
from the study as planned (and, if relevant, registered) have been explained.
What this paper adds
1. What is already known on this subject
A defined subset of hip fracture patients achieve better functional outcomes from
total hip arthroplasty (THA) than hemiarthroplasty. Guidelines published by the
National Institute for Health and Care Excellence (NICE) clearly indicate which
hip fracture patients should be offered THA.
2. What this study adds
Compliance with NICE guidelines is poor and there is considerable variation
between hospitals. Surgeons appear to apply different eligibility criteria for THA
than NICE. Socioeconomic deprivation and need for hip fracture surgery at the
weekend are particular barriers to accessing THA. Further efforts are necessary
to improve access to THA for eligible patients and reduce unexplained variation
in care for older adults with hip fractures.
Page 15 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyFigure legends
Figure 1 – Decision tree for THA in displaced intracapsular fractures as per NICE
guidelines. Parentheses indicate the number of people within each leaf and the
percentage of people within the leaf that underwent THA.
Figure 2 – Graph illustrating limited improvement in the model using the optimal
tree size of ten terminal nodes (lowest error), and a more pragmatic tree with
five nodes. cp = complexity function.
Figure 3 – Decision tree for THA in displaced intracapsular fractures using a
recursive partitioning algorithm. Parentheses indicate the number of people
within each leaf and the percentage of people within the leaf that underwent
THA.
Figure 4 – Graph illustrating limited improvement in the model using the optimal
tree size of 20 terminal nodes, and a simplified tree with four nodes.
Figure 5 - Decision tree using a recursive partitioning algorithm to indicate the
important predictors for THA amongst individuals fulfilling the NICE criteria for
consideration of THA. Parentheses indicate the number of people within each
leaf and the percentage of people within the leaf that underwent THA.
Figure 6 – Variation in the number of THAs performed within each hospital, as a
proportion of the total number of individuals fulfilling the NICE guidelines. Only
hospitals that contributed >100 NICE eligible patients are included to minimise
spurious data (n=96). Each bar represents a hospital.
Page 16 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyReferences
1. Royal College of Physicians. National Hip Fracture Database annual report
2014. London, UK: RCP 2014.
2. Burge RT, Worley D, Johansen A, et al. The cost of osteoporotic fractures in the
UK: projections for 2000-2020. J Med Econ 2001;4:51-62.
3. Neuburger J, Currie C, Wakeman R, et al. The impact of a national clinician-led
auditinitiative on care and mortality after hip fracture in England: an
external evaluation using time trends in ton-audit tata. Med Care
2015;53(8):686-91.
4. Sahota O, Currie C. Hip fracture care: all change. Age Ageing 2008;37(2):128-9.
5. British Orthopaedic Association, British Geriatrics Society. The Care of Patients
with Fragility Fracture. London: BOA 2007.
6. Department of Health. Payment by Results Guidance for 2013-14. London:
DoH 2013.
7. Hopley C, Stengel D, Ekkernkamp A, et al. Primary total hip arthroplasty versus
hemiarthroplasty for displaced intracapsular hip fractures in older
patients: systematic review. BMJ 2010;340:c2332.
8. National Institute for Health and Care Excellence. Hip fracture: the
management of hip fracture in adults. NICE clinical guideline 124. London,
NICE 2011.
9. Parker MJ, Gurusamy KS, Azegami S. Arthroplasties (with and without bone
cement) for proximal femoral fractures in adults. The Cochrane Database
of Systematic Reviews 2010(6):CD001706.
10. Avery PP, Baker RP, Walton MJ, et al. Total hip replacement and
hemiarthroplasty in mobile, independent patients with a displaced
intracapsular fracture of the femoral neck: a seven- to ten-year follow-up
report of a prospective randomised controlled trial. J Bone Joint Surg Br
2011;93(8):1045-8.
11. Yu L, Wang Y, Chen J. Total hip arthroplasty versus hemiarthroplasty for
displaced femoral neck fractures: meta-analysis of randomized trials. Clin
Orthop Relat Res 2012;470(8):2235-43.
12. Department of Health. Governance arrangements for research ethics
committees. London: DoH 2011.
13. McLennan D, Barnes H, Noble M, et al. The English Indices of Deprivation
2010. London: Department for Communities and Local Government 2011.
14. Therneau TM, Atkinson EJ. An introduction to recursive partitioning using
rpart routines: The Comprehensive R Archive Network (CRAN), 2015.
15. Vyawahare B, Hallas N, Brookes M, et al. Impact of the National Institute for
Health and Care Excellence (NICE) guidance on medical technology
uptake: analysis of the uptake of spinal cord stimulation in England 2008-
2012. BMJ Open 2014;4(1):e004182.
16. Haider AH, Schneider EB, Sriram N, et al. Unconscious race and social class
bias among acute care surgical clinicians and clinical treatment decisions.
JAMA Surg 2015;150(5):457-64.
17. Tamayo-Sarver JH, Dawson NV, Hinze SW, et al. The effect of race/ethnicity
and desirable social characteristics on physicians' decisions to prescribe
opioid analgesics. Acad Emerg Med 2003;10(11):1239-48.
Page 17 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly18. Street RL, Jr., O'Malley KJ, Cooper LA, et al. Understanding concordance in
patient-physician relationships: personal and ethnic dimensions of shared
identity. Ann Fam Med 2008;6(3):198-205.
19. Hedlundh U, Ahnfelt L, Hybbinette CH, et al. Surgical experience related to
dislocations after total hip arthroplasty. J Bone Joint Surg Br
1996;78(2):206-9.
20. Lavernia CJ, Guzman JF. Relationship of surgical volume to short-term
mortality, morbidity, and hospital charges in arthroplasty. J Arthroplasty
1995;10(2):133-40.
21. Katz JN, Losina E, Barrett J, et al. Association between hospital and surgeon
procedure volume and outcomes of total hip replacement in the United
States medicare population. J Bone Joint Surg Am 2001;83-A(11):1622-9.
22. Losina E, Barrett J, Mahomed NN, et al. Early failures of total hip replacement:
effect of surgeon volume. Arthritis Rheum 2004;50(4):1338-43.
23. Katz JN, Phillips CB, Baron JA, et al. Association of hospital and surgeon
volume of total hip replacement with functional status and satisfaction
three years following surgery. Arthritis Rheum 2003;48(2):560-8.
24. Kleebauer A, Comerford C. Government commits to seven-day NHS. Nurs
Manage 2015;22(3):6.
25. Freemantle N, Richardson M, Wood J, et al. Weekend hospitalization and
additional risk of death: an analysis of inpatient data. J R Soc Med
2012;105(2):74-84.
26. Keogh B. Should the NHS work at weekends as it does in the week? Yes. BMJ
2013;346:f621.
27. Whitmore RG, Stephen JH, Vernick C, et al. ASA grade and Charlson
Comorbidity Index of spinal surgery patients: correlation with
complications and societal costs. Spine J 2014;14(1):31-8.
28. Tan WP, Talbott VA, Leong QQ, et al. American Society of Anesthesiologists
class and Charlson's comorbidity index as predictors of postoperative
colorectal anastomotic leak: a single-institution experience. J Surg Res
2013;184(1):115-9.
29. Dekker JW, Gooiker GA, van der Geest LG, et al. Use of different comorbidity
scores for risk-adjustment in the evaluation of quality of colorectal cancer
surgery: does it matter? Eur J Surg Oncol 2012;38(11):1071-8.
Page 18 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
Figure 1
240x128mm (72 x 72 DPI)
Page 19 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
Figure 2
278x153mm (72 x 72 DPI)
Page 20 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
Figure 3
240x128mm (72 x 72 DPI)
Page 21 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
Figure 4
228x125mm (72 x 72 DPI)
Page 22 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
Figure 5
240x128mm (72 x 72 DPI)
Page 23 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
Figure 6
289x420mm (72 x 72 DPI)
Page 24 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyMobility Scores
Version 7 and 8 of NHFD have different mobility scores
V7 therefore tracked onto V8
MOBILITY (VERSION 7 ONLY)
WalkInside Walking Ability Indoors (V7 only)
0 Regulary walked without aids
1 Regularly walked with one aid
2 Regularly walked with two aids or frame
3 Wheelchair or bedbound
4 Unknown
. Missing
WalkOutside Walking ability outside (V7 only)
0 Regulary walked without aids
1 Regularly walked with one aid
2 Regularly walked with two aids or frame
3 Wheelchair or bedbound
4 Never goes outdoors
5 Electric buggy
6 Unknown
. Missing
AccompOutside Accompanied to Walk Ouside (V7 only)
0 No
1 Yes
2 Wheelchair or bedbound
3 Unknown
4 Never goes outdoors
. Missing
AccompInside Accompanied to Walk Inside (V7 only)
0 No
1 Yes
2 Wheelchair or bedbound
3 Unknown
. Missing
MOBILITY VERSION 8 ONLY
Mobility Pre-Fracture Walking Ability (VERSION 8 ONLY)
1 Freely mobile without aids
2 Mobile outdoors with one aid
3 Mobile outdoors with two aids or frame
Page 25 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly4 Some indoor mobility but never goes outside without help
5 Unknown
6 No functional mobility
V7 TRACKED ONTO V8 (variable name = mob)
1 Freely mobile without aids (walkoutside 0) 2 Mobile outdoors with one aid (walkoutside 1) 3 Mobile outdoors with two aids or frame (walkoutside 2)
4
Some indoor mobility but never goes outside without help
ANY WALKING INSIDE(0-2) AND ACCOMPANIEDOUTSIDE (1,2 and 4) OR ANYWALKING INSIDE(0-2) AND WALKINGOUTDOORS WHEEL/ BUGGY (3, 4,5)
5 No functional ability Wheelchair or bedbound inside (walkinside 3) 6 Unknown
STATA CODE
replace mob=mobility
replace mob=5 if walkinside==3
replace mob=4 if (walkinside==0 & accompoutside==1)
replace mob=4 if (walkinside==1 & accompoutside==1)
replace mob=4 if (walkinside==2 & accompoutside==1)
replace mob=4 if (walkinside==0 & accompoutside==2)
replace mob=4 if (walkinside==1 & accompoutside==2)
replace mob=4 if (walkinside==2 & accompoutside==2)
replace mob=4 if (walkinside==0 & accompoutside==4)
replace mob=4 if (walkinside==1 & accompoutside==4)
replace mob=4 if (walkinside==2 & accompoutside==4)
replace mob=4 if (walkinside==0 & walkoutside==3)
replace mob=4 if (walkinside==1 & walkoutside==3)
replace mob=4 if (walkinside==2 & walkoutside==3)
replace mob=4 if (walkinside==0 & walkoutside==4)
Page 26 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyreplace mob=4 if (walkinside==1 & walkoutside==4)
replace mob=4 if (walkinside==2 & walkoutside==4)
replace mob=4 if (walkinside==0 & walkoutside==5)
replace mob=4 if (walkinside==1 & walkoutside==5)
replace mob=4 if (walkinside==2 & walkoutside==5)
replace mob=3 if walkoutside==2
replace mob=2 if walkoutside==1
replace mob=1 if walkoutside==0
Page 27 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyGroup ‘X’ Hospitals
ADD. Addenbrookes Hospital
AEI. Royal Albert Edward Infirmary
AIR. Airedale General Hospital
ASH. Wansbeck General Hospital
BAR. Barnsley District General Hospital
BAS. Basildon Hospital
BAT. Royal United Hospital Bath
BFH. Broomfield Chelmsford
BOL. Royal Bolton Hospital
BRD. Bradford Royal Infirmary
BRG. Bronglais General Hospital
BRI. Bristol Royal Infirmary
CCH. Charing Cross Hospital
CHE. Chesterfield Royal
CHG. Cheltenham General Hospital
COC. Countess of Chester Hospital
CRG. Craigavon Area Hospital
DAR. Darlington Memorial Hospital
DGE. Eastbourne DGH
DVH. Darent Valley Hospital
EAL. Ealing Hospital
EBH. Birmingham Heartlands Hospital
ESU. East Surrey Hospital
FAZ. University Hospital Aintree
FGH. Furness General
FRM. Frimley Park Hospital
FRY. Frenchay Hospital
GGH. Diana Princess of Wales Hospital
GHS. Good Hope General Hospital
GLO. Gloucestershire Royal Hospital
GRA. Grantham And District General Hospital
GWY. Ysbyty Gwynedd Hospital
HAR. Harrogate District Hospital
HCH. County Hospital Hereford
HIN. Hinchingbrooke Hospital
HOM. Homerton Hospital
HRI. Hull Royal Infirmary
IOW. St Marys Hospital Newport
JPH. James Paget Hospital
LDH. Luton & Dunstable Hospital
LGH. Leighton Hospital
LGI. Leeds General Infirmary
LIN. Lincoln County Hospital
LON. Royal London Hospital
Page 28 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyMAC. Macclesfield District General Hospital
MKH. Milton Keynes General Hospital
MOR. Morriston Hospital
MPH. Taunton & Somerset Hospital
NCR. New Cross Hospital
NEV. Nevill Hall Hospital
NGS. Northern General Hospital
NHH. North Hampshire Hospital
NMG. North Manchester General Hospital
NMH. North Middlesex Hospital
NTG. University Hospital of North Tees
NTH. Northampton General Hospital
NUH. Ulster Hospital
OHM. Royal Oldham Hospital
PAH. Princess Alexandra Hospital
PIN. Pinderfields General Hospital
PLY. Derriford Hospital
PMS. The Great Western Hospital
QAP. Queen Alexandra Hospital
QEB. Queen Elizabeth Hospital Edgbaston
QEG. Queen Elizabeth Hospital Gateshead
QKL. Queen Elizabeth Hospital (Kings Lynn)
RAD. John Radcliffe Hospital
RBE. Royal Berkshire Hospital
RCH. Royal Cornwall Hospital
RDE. Royal Devon & Exeter Hospital
RED. The Alexandra Hospital
RFH. Royal Free Hospital
RGH. Royal Glamorgan
RHC. Royal Hampshire County Hospital
RLI. Royal Lancaster Infirmary
RLU. Royal Liverpool University Hospital
ROT. Rotherham General Hospital
RPH. Royal Preston Hospital
RSC. Royal Sussex County Hospital
RSS. Royal Shrewsbury Hospital
RSU. Royal Surrey County Hospital
RVB. Royal Victoria Hospital
RVN. Royal Victoria Infirmary
SAL. Salisbury District Hospital
SAN. Sandwell District Hospital
SCA. Scarborough General Hospital
SCM. James Cook University Hospital
SDG. Staffordshire General Hospital
SEH. Southend Hospital
SGH. Southampton General Hospital
Page 29 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlySHH. Stepping Hill Hospital
SLF. Hope Hospital
SMV. Stoke Mandeville Hospital
SOU. Southport and Formby District General
SPH. St Peters Hospital
STD. South Tyneside District Hospital
STH. St Thomas Hospital
STM. St Marys Hospital Paddington
STO. University Hospital of North Staffordshire
STR. St Richards Hospital
SUN. Sunderland Royal Hospital
TOR. Torbay Hospital
TRA. Trafford General Hospital
TUN. Tunbridge Wells Hospital
UCL. University College Hospital
UHC. University Hospital Coventry
UHW. University Hospital of Wales
WAR. Warwick Hospital
WDG. Warrington District General Hospital
WES. Chelsea & Westminister Hospital
WEX. Wexham Park Hospital
WGH. Weston General Hospital
WHC. Whipps Cross Hospital
WHH. William Harvey Hospital
WHI. Whiston Hospital
WIR. Arrowe Park Hospital
WRG. Worthing Hospital
WRX. Maelor Hospital
WSH. West Suffolk Hospital
WWG. West Wales General
YDH. York District Hospital
YEO. Yeovil District Hospital
ENH. East and North Herts Hospital
QEW. Queen Elizabeth II Hospital (Welwyn)
Page 30 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyGroup ‘Y’ Hospitals
ALT. Altnagelvin Hospital
BED. Bedford Hospital
BLA. Royal Blackburn Hospital
BNT. Barnet General Hospital
BRO. Princess Royal University Hospital
(Bromley)
BRT. Queens Hospital
BRY. Fairfield General Hospital
BSL. Bassetlaw District General Hospital
CHS. Chase Farm Hospital
CLW. Glan Clwyd DGH Trust
CMI. Cumberland Infirmary
COL. Colchester General Hospital
DER. Royal Derby Hospital
DID. Doncaster Royal Infirmary
DRY. University Hospital of North Durham
GEO. St Georges Hospital
GWE. Royal Gwent Hospital
GWH. Queen Elizabeth Hospital Woolwich
HIL. Hillingdon Hospital
HOR. Horton General Hospital
HUD. Huddersfield Royal Infirmary
IPS. The Ipswich Hospital
KCH. Kings College Hospital
KGH. Kettering General Hospital
KMH. Kings Mill Hospital
KTH. Kingston Hospital
LER. Leicester Royal Infirmary
LEW. University Hospital Lewisham
MAY. Mayday University Hospital
MDW. Medway Maritime Hospital
MRI. Manchester Royal Infirmary
NDD. North Devon District Hospital
NOB. Nobles Hospital
NOR. Norfolk and Norwich Hospital
NPH. Northwick Park Hospital
NTY. North Tyneside Hospital
NUN. George Eliot Hospital
NWG. Newham General Hospital
OLD. Queens Hospital Romford
PCH. Prince Charles Hospital
PET. Peterborough City Hospital
PGH. Poole General Hospital
PIL. Pilgrim Hospital
Page 31 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyPOW. Princess Of Wales Hospital
QEQ. Queen Elizabeth the Queen Mother
Hospital
RUS. Russells Hall Hospital
SCU. Scunthorpe General Hospital
SHC. St Helier Hospital
TGA. Tameside General Hospital
TLF. Princess Royal Hospital Telford
UHN. University Hospital Queens Medical
Centre
VIC. Victoria Hospital
WAT. Watford General Hospital
WDH. Dorset County Hospital
WHT. Whittington Hospital
WMH. Manor Hospital
WMU. West Middlesex University Hospital
WRC. Worcestershire Royal Hospital
WYB. Withybush General Hospital
WYT. Wythenshawe Hospital
MAI. Maidstone General Hospital
Hospitals not contributing to analysis owing to absent
or insufficient data
KSX. Kent & Sussex Hospital
CGH. Conquest Hospital
CMH. Central Middlesex Hospital
DMO. Demonstration Medical Centre
PEH. Princess Elizabeth Hospital
SHJ. Jersey General Hospital
WCI. West Cumberland Infirmary
LIS. Lister Hospital
Page 32 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Inequalities in Access to Total Hip Arthroplasty for Hip Fracture: Population Based Study
Item
No Recommendation
Title and abstract
Y (a) Indicate the study's design with a commonly used term in the title or the abstract
(b) Provide in the abstract an informative and balanced summary of what was done and what was found
Introduction
Background/rationale Y Explain the scientific background and rationale for the investigation being reported
Objectives Y State specific objectives, including any prespecified hypotheses
Methods
Study design Y Present key elements of study design early in the paper
Setting Y Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data
collection
Participants Y
(a) Cohort study?Give the eligibility criteria, and the sources and methods of selection of participants. Describe
methods of follow-upCase-control study?Give the eligibility criteria, and the sources and methods of case
ascertainment and control selection. Give the rationale for the choice of cases and controlsCross sectional study?Give
the eligibility criteria, and the sources and methods of selection of participants
(b) Cohort study?For matched studies, give matching criteria and number of exposed and unexposedCase-control
study?For matched studies, give matching criteria and the number of controls per case
Variables Y Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria,
if applicable
Data sources/ measurement Y For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe
comparability of assessment methods if there is more than one group
Bias Y Describe any efforts to address potential sources of bias
Study size Y Explain how the study size was arrived at
Quantitative variables Y Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen
and why
Statistical methods Y
(a) Describe all statistical methods, including those used to control for confounding
(b) Describe any methods used to examine subgroups and interactions
(c) Explain how missing data were addressed
(d) Cohort study?If applicable, explain how loss to follow-up was addressedCase-control study?If applicable, explain
how matching of cases and controls was addressedCross sectional study?If applicable, describe analytical methods
Page 33 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
taking account of sampling strategy
(e) Describe any sensitivity analyses
Results
Participants Y
(a) Report numbers of individuals at each stage of study?eg numbers potentially eligible, examined for eligibility,
confirmed eligible, included in the study, completing follow-up, and analysed
(b) Give reasons for non-participation at each stage
(c) Consider use of a flow diagram
Descriptive data Y
(a)Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and
potential confounders
(b) Indicate number of participants with missing data for each variable of interest
(c) Cohort study?Summarise follow-up time (eg average and total amount)
Outcome data Y
Cohort study?Report numbers of outcome events or summary measures over time
Case-control study?Report numbers in each exposure category, or summary measures of exposure
Cross sectional study?Report numbers of outcome events or summary measures
Main results Y
(a) Report the numbers of individuals at each stage of the study?eg numbers potentially eligible, examined for
eligibility, confirmed eligible, included in the study, completing follow-up, and analysed
(b) Give reasons for non-participation at each stage
(c) Consider use of a flow diagram
Other analyses Y Report other analyses done?eg analyses of subgroups and interactions, and sensitivity analyses
Discussion
Key results Y Summarise key results with reference to study objectives
Limitations Y Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and
magnitude of any potential bias
Interpretation Y Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from
similar studies, and other relevant evidence
Generalisability Y Discuss the generalisability (external validity) of the study results
Other information
Funding Y Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on
which the present article is based
Page 34 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960