-
Psychopharmacology (2005) 181: 4859DOI
10.1007/s00213-005-2219-1
ORIGINAL INVESTIGATION
Douglas S. Ramsay . Karl J. Kaiyala .Brian G. Leroux . Stephen
C. Woods
Individual differences in initial sensitivity and acutetolerance
predict patterns of chronic drug toleranceto nitrous-oxide-induced
hypothermia in rats
Received: 4 August 2004 / Accepted: 20 January 2005 / Published
online: 19 March 2005# Springer-Verlag 2005
Abstract Rationale: A preventive strategy for drug addic-tion
would benefit from being able to identify vulnerableindividuals.
Understanding how an individual responds dur-ing an initial drug
exposure may be useful for predictinghow that individual will
respond to repeated drug admin-istrations. Objectives: This study
investigated whetherindividual differences in initial drug
sensitivity and acutetolerance can predict how chronic tolerance
develops.Methods: During an initial 3-h administration of 60%
ni-trous oxide (N2O), male LongEvans rats were screenedfor N2Os
hypothermic effect into subsets based on beinginitially insensitive
(II), sensitive with acute tolerance (AT),or sensitive with no
intrasessional recovery (NR). Animalsin each individual difference
category were randomly as-signed to receive six 90-min exposures of
either 60% N2Oor placebo gas. Core temperature was measured
telemet-rically. Results: Rats that exhibited a comparable
degree
of hypothermia during an initial N2O exposure, but dif-fered in
acute tolerance development, developed differentpatterns of chronic
tolerance. Specifically, the NR groupdid not become fully tolerant
over repeated N2O expo-sures while the AT group developed an
initial hyperther-mia followed by a return of core temperature to
controllevels indicative of full tolerance development. By the
sec-ond N2O exposure, the II group breathing N2O becamehyperthermic
relative to the placebo control group andthis hyperthermia
persisted throughout the multiple N2Oexposures. Conclusions:
Individual differences in initialdrug sensitivity and acute
tolerance development predictdifferent patterns of chronic
tolerance. The hypothesis issuggested that individual differences
in opponent-adaptiveresponses may mediate this relationship.
Keywords Inhalant . Addictive vulnerability . Addiction .Drug
dependence . Intrasessional tolerance . Allostasis .Homeostasis .
Regulation
Introduction
Drug abuse is a major public health and economic
problemworldwide (McGinnis and Foege 1999; Single et al.
1999;Fenoglio et al. 2003). While advances are being made
tounderstand the neurobiology of addictions for devisingnovel
pharmacological therapies (OBrien 1997), an alter-native approach
is to identify especially vulnerable indi-viduals to utilize
preventive strategies (Piazza and LeMoal1996). Individual
differences in key characteristics couldthen be used to identify
at-risk individuals before they be-come addicted to abusable drugs
(Crabbe et al. 1999;Schuckit et al. 2001). The adaptations an
individual makesduring an initial drug exposure may indicate how
that in-dividual will respond to future drug exposures.Adaptation
models of drug addiction are popular be-
cause they account for central features of the drug
addictionprocess, including tolerance, dependence, and
withdrawal(Jaffe 1985; Peper 2004). These phenomena are thought
tobe manifestations of a common underlying adaptive re-
D. S. Ramsay (*) . K. J. Kaiyala . B. G. LerouxDepartment of
Dental Public Health Sciences,University of Washington,P.O. Box
357475 Seattle, WA, 98195-7475, USAe-mail:
[email protected].: +1-206-5432034Fax: +1-206-6854258
D. S. RamsayDepartment of Orthodontics,University of
Washington,Seattle, WA, USA
D. S. RamsayDepartment of Pediatric Dentistry,University of
Washington,Seattle, WA, USA
B. G. LerouxDepartment of Biostatistics,University of
Washington,Seattle, WA, USA
S. C. WoodsDepartment of Psychiatry,University of Cincinnati
Medical Center,Cincinnati, OH, USA
-
sponse that develops with repeated drug use. In brief, thedrug
initially perturbs a biologically regulated system,eliciting
adaptive changes that reduce the perturbation (i.e.,tolerance
develops). Over repeated drug administrations,the individual comes
to function in a drug-adapted or-dependent state wherein
drug-induced perturbations areeffectively countered by acquired
neutralizing or compen-satory adaptations. If the drug effect is
removed, the com-pensatory effects caused by these adaptations
becomeunopposed and result in withdrawal. A premise of adap-tation
models is that addiction results from adaptive re-sponses made when
confronted with repeated drug-inducedregulatory disturbances.
Presumably, individuals who donot become addicted despite repeated
drug exposures arenot making those same adaptations. This suggests
the hy-pothesis that individuals differ quantitatively or
qualitativelyin terms of the adaptive responses elicited by
comparabledrug exposures. Individuals could differ in the
magnitudeof the disturbance required to initiate adaptive
responses,or vulnerable individuals may react to a drug-induced
per-turbation with rigorous adaptive responses while individ-uals
with sluggish or weak adaptive responses would beless susceptible
to becoming addicted. Investigating thishypothesis requires
identifying how individuals differ inthe adaptive responses that
are elicited during the initialadministration of a drug.Identifying
the response(s) an individual makes during
an initial drug administration is not obvious. When a de-pendent
measure is assessed before and after a drug ad-ministration, the
resulting change in the measure is casuallyreferred to as either
the drug effect or the individualsresponse to the drug. Yet,
neither description is accurate.What is typically being measured
represents an integral ofmany ongoing processes that include both
the direct phar-macological effect of the drug as well as the
adaptive re-sponses that are elicited by the drug-induced
regulatorydisturbance (Dworkin 1993; Ramsay and Woods 1997;Kaiyala
and Ramsay 2005). The challenge is to distinguishthe individuals
response from the direct effect of the drugand from the effects of
other cooccurring processes (e.g.,handling, circadian rhythms) that
influence that same mea-sure (Brick et al. 1984; Peris and
Cunningham 1986). Pro-posed methods for evaluating the response an
individualmakes during an initial drug exposure include
assessinginitial drug sensitivity, acute tolerance, and
precipitatedwithdrawal (Ramsay and Woods 1997). Human and
animaldata suggest that these processes have predictive value
forunderstanding how an individual will react to chronic
drugexposure. Humans who appear initially insensitive to al-cohol
are at greater risk of becoming addicted than aremore
drug-sensitive individuals (Schuckit and Smith 1996;Heath et al.
1999). Schuckit (1994) has described initialinsensitivity to
alcohol as ... a potent predictor of futurealcohol abuse or
dependence (p. 341). McBride and Li(1998) reported that initial
sensitivity and acute (within-session) tolerance are by far the
most generalizable and ro-bust responses to ethanol found in
association with ethanolpreference in rodents (p. 346). Kest and
colleagues (2002)quantified naloxone-precipitated withdrawal during
an ini-
tial administration of morphine in 11 inbred mouse strainsand
found that .... the differential genetic liability to mor-phine
physical dependence begins with, and is predictedby, the first
morphine exposure (p. 463).The goal of the present study was to
investigate the
relationship between individual differences in acute toler-ance
and sensitivity during an initial drug administrationand the
development of chronic tolerance. Core body tem-perature was
selected as the dependent variable because itcan be measured
accurately, continuously, and noninva-sively and because it
reflects the operation of a well-stud-ied, centrally regulated
control system. This is importantbecause regulatory principles are
at the foundation of nu-merous influential theories relevant to
drug addiction(e.g., Solomon 1980; Poulos and Cappell 1991; Koob
andLeMoal 1997; Siegel et al. 2000). Our drug choice wasinfluenced
by the ease, speed, and accuracy with whichsteady-state drug
concentrations could be achieved andmaintained. The
pharmacologically active gas, nitrous oxide(N2O), is well suited
for this purpose. N2O reaches steady-state concentrations quickly
(Eger 1985) and its concen-tration can be measured accurately and
continuously usinginfrared spectroscopy. N2O causes a pronounced
hypo-thermia at typical ambient temperatures (Quock et al.
1987;Pertwee et al. 1990). Outbred LongEvans rats exhibit
widebetween-subject variation in initial sensitivity and
acutetolerance to N2O-induced hypothermia (Ramsay et al. 1999)and
these differences are reliable characteristics of an in-dividual
(Kaiyala et al. 2001). Chronic tolerance also de-velops to N2O
hypothermia (Ramsay et al. 1999).This research addresses a
long-standing question con-
cerning the relationship between acute and chronic toler-ance
(Kalant et al. 1971; Tabakoff and Rothstein 1983; Wuet al. 2001).
Based on the premise that adaptive responsesplay a role in
tolerance development, two primary hypoth-eses were evaluated. The
first was that sensitive indi-viduals who have significant acute
tolerance developmentare likely to develop chronic tolerance more
quickly and toa greater degree than sensitive individuals who
developlittle acute tolerance. The second was that initially
insen-sitive individuals will quickly become fully tolerant to
asmall initial hypothermic effect and then remain
insensitive/tolerant over repeated drug administrations. This
hypoth-esis is consistent with contemporary explanations for
ini-tial insensitivity. If individuals are insensitive because
thedrug has little or no pharmacological effect on their tis-sues,
it seems unlikely that repeated drug exposure wouldcause a drug
effect to develop. Alternatively, if some indi-viduals are
insensitive because of an effective or powerfuladaptive response
that effectively counters the drugs hy-pothermic effect within an
initial exposure, effective reg-ulation of core temperature should
continue over repeateddrug exposures.
Methods
Subjects Male LongEvans rats (ten squads of 40 ratseach,
Simonsen Laboratory, Gilroy, CA) weighing 200
49
-
250 g were housed in groups of two to three per tub withfree
access to pelleted chow and water. The housing roomhad a 12 h:12 h
light/dark cycle (07001900 h) and anambient temperature of 221C.
The animal proceduresused in this research were approved by the
University ofWashingtons IACUC and were conducted in accordancewith
the Guidelines for the Care and Use of Mammals inNeuroscience and
Behavioral Research (National Re-search Council 2003).
Surgery for core temperature measures At least 7 daysafter
arriving in the lab, each rat was anesthetized (0.5 ml/kg of a
solution containing 90.9mg/ml ketamine and 1.8 mg/ml xylazine,
i.p.) and a telemetric temperature sensor (E-mitters from
Mini-Mitter Co., Bend, OR) was implantedinto the peritoneal cavity.
Rats recovered for 7 days be-fore the experiment.
N2O delivery/temperature data acquisition system Acustom-built,
automated system controlled gas deliveryand data acquisition.
Medical grade oxygen (O2), nitrogen(N2), and N2O were blended to
produce an outflow of 30%O2, 10% N2, and 60% N2O (referred to as
60% N2O). N2and O2 were blended to produce an outflow consisting
of30% O2 and 70% N2 (referred to as placebo gas). Twolines affixed
to outlets in each chambers lid provided alow-resistance path by
which exhaust gas flowed to a fumehood. Effluent gas sampling [N2O,
O2, and CO2 by aninfrared gas analyzer (Normocapoxy, Datex
InstrumentsCorp., Helsinki, Finland)] and data acquisition were
con-trolled by a program written in LabView 5.0
(NationalInstruments, Austin, TX) installed on a Macintosh
IIcicomputer. This system is described fully elsewhere (Kaiyalaet
al. 2001).Each exposure chamber (Columbus Instruments, Colum-
bus, OH) was made of clear Lexan and had a removable lidsecured
with four latches and sealed with a closed-cell sil-icone foam
rubber gasket. The floor of the chamber wascovered with a layer of
wood shavings. The chambers in-ternal dimensions were 181831 cm,
yielding a volume of10 l. With a gas inflow (and outflow) rate of
3.0 l/min, thetheoretical half-time by which the 10-l chamber
achievesthe target gas composition is 2.3 min (Lewis et al.
1987).The chambers gas environment is calculated to reach 97%of the
administered gas concentration in 11.6 min. Infraredgas analyses
confirmed this figure and indicated that 60%N2O steady-state gas
concentrations were achieved in thisstudy. Each test chamber was
placed on a platform thatenergized the implanted temperature sensor
and receivedits signal. Temperature data were acquired using
VitalViewsoftware (Mini-Mitter Co.). During all sessions, a
blackvinyl drape visually isolated each chamber. All gas
admin-istrations occurred in the light part of the cycle and
com-menced at least 2 h after lights on and ended at least 2 h
priorto lights off.
Experimental design and procedures During the initialscreening
session, each rat received a 2-h administration ofplacebo gas
followed immediately by a 3-h administration
of 60% N2O. A squad of 40 rats was screened over a periodof 11
days after which ten rats (25%) were retained thatexhibited: (1)
minimal hypothermia while receiving N2O(designated as initially
insensitive, II); (2) a large hypo-thermic effect that persisted
throughout the N2O adminis-tration (designated sensitive with no
recovery, NR); or (3) alarge hypothermic effect followed by a
robust return oftemperature toward baseline (designated as
sensitive withacute tolerance, AT). These categorizations were
based onZ-scores of the regression residuals (Kaiyala et al.
2001)for: (1) the size of the drug effect (degree of
sensitivity)adjusted for baseline temperature, and (2) the degree
ofrecovery from the drug effect (acute tolerance) adjusted
forbaseline temperature and drug effect.Each of the ten retained
rats was randomly assigned to
receive either placebo gas or 60% N2O for six
additionalexposures on an every-other-day schedule beginning 4 or5
days after screening. Rats assigned to the 60% N2Ogroup received 2
h of placebo gas followed by 1.5 h of60% N2O at each gas exposure
session while rats assignedto the placebo group received 3.5 h of
placebo gas.
Individual difference group assignment Categorization ofrats
into the three individual difference groups was doneusing methods
described previously (Kaiyala et al. 2001).Temperature values were
recorded at 30-s intervals over the5-h screening session. These
were smoothed using naturalsmoothing splines with 10 df (Hastie
1992) to minimizethe influence of occasional aberrant temperature
values.The smoothed temperature values were used to calculatethe
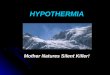
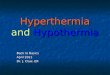
following three parameters (see Fig. 1 for illustration):(1)
baseline core temperature, equal to the average of thesmoothed
temperature values for the 3-min period prior todrug
administration; (2) drug effect, equal to the differencebetween
baseline temperature and the minimum smoothedtemperature value
after drug onset; and (3) acute tolerance
Fig. 1 Core temperature data (dashed line) from a single rat
aresmoothed (solid line) and calculations of baseline
temperature,minimum temperature after drug onset, and the final
temperature aremade using the smoothed data. The drug effect equals
1.07C (i.e.,37.24 minus 36.17), the drug effect regression residual
equals0.01637, and the drug effect Z-score equals 0.0308. Acute
toleranceequals 0.73C (i.e., 36.90 minus 36.17), the acute
tolerance re-gression residual equals 0.01099, and the acute
tolerance Z-scoreequals 0.0399. This rat is depicted in the
scatterplot of Fig. 2a asthe most average rat
50
-
(i.e., intrasessional recovery), equal to the difference
be-tween the mean of the smoothed values over the final 15 minof
drug administration minus the minimum smoothed tem-perature. After
a squad of rats completed screening, regres-sion residuals were
calculated for each rats drug effect andacute tolerance scores
(Nagoshi et al. 1986; Kaiyala et al.2001). The drug effect
regression residual is an adjusted drugeffect score that is not
confounded by baseline core tem-perature; this adjustment is
important because on aver-age, rats with higher baseline
temperatures can exhibitsignificantly greater N2O-induced
hypothermia (Kaiyalaet al. 2001). The drug effect regression
residual was calcu-lated by subtracting from the drug effect score
the regression-predicted mean drug effect score given the rats
observedbaseline core temperature (T):
Drug Effect RegressionResidual
Drug Effect Score 1 T
Based on the 387 rats that completed the screeningsession, the
values of the beta coefficients for the drug effectregression
residual calculation were: (intercept)=1.698and 1 (coefficient for
baseline temperature)=0.07391. Ap-plying this formula to the data
in Fig. 1 yields a drug effectregression residual of
0.01637=1.071(1.698+0.0739137.243).The acute tolerance regression
residual is an adjusted
acute tolerance score that is not confounded by baselinecore
temperature or the drug effect score; this adjustment isimportant
because mean acute tolerance magnitude variesdirectly with the drug
effect which is influenced by baselinetemperature. The acute
tolerance regression residual wascalculated by subtracting from the
acute tolerance score theregression-predicted mean acute tolerance
score given therats observed baseline core temperature (T) and drug
effect:
Acute Tolerance Regression Residual Acute Tolerance Score 1 T 2
Drug Effect Score
Based on the 387 rats that completed the screening ses-sion, the
values of the beta coefficients for the acute tol-erance regression
residual calculation were: (intercept)=1.790, 1 (coefficient for
baseline temperature)=0.03887and 2 (coefficient for drug
effect)=0.03750. Applyingthis formula to the data provided in Fig.
1 yields an acutetolerance regression residual of
0.01099=0.733[1.79+(0.03887)37.243+0.37501.071].To operationally
define which rats were exemplars of
high/low initial sensitivity and which rats exemplifiedinitial
sensitivity with high/low acute tolerance develop-ment, Z-scores
were used to identify where each rat waslocated within the
distribution of drug effect regressionresiduals (i.e., initial
sensitivity) and the distribution ofacute tolerance regression
residuals (i.e., acute tolerancedevelopment). Selection criteria
for group assignment werebased on critical values for independent
normal distribu-
tions for drug effect and acute tolerance Z-scores and
weredesigned to assign 25% of the screened population into oneof
the three groups. Z-scores were calculated by dividingeach rats
drug effect and acute tolerance regression re-siduals by the
corresponding standard deviation for thoseregression residuals.
Based on the 387 rats that completedthe screening session, the
standard deviation of the drugeffect regression residuals was
0.5316 and the standarddeviation of the acute tolerance regression
residuals was0.2755. The individual rats data provided in Fig. 1
can beconverted to Z-scores as follows: the drug effect
Z-scoreequals 0.0308 (i.e., 0.01637/0.5316) and the acute
toler-ance Z-score equals 0.0399 (i.e., 0.01099/0.2755). Be-cause
both Z-score values are close to zero, this rat was quiteaverage in
both the magnitude of the hypothermic drugeffect and the amount of
acute tolerance that developed.Thus, this rat would not be a good
exemplar of high or lowinitial sensitivity, nor of high or low
acute tolerance de-velopment (and it was not considered
further).
Data analysis Temperatures for each of the six test ses-sions
were summarized by the baseline temperature (meanof temperature
values over the 15-min interval prior todrug administration) and
the change from baseline to themean temperature over three
intervals: (1) 030 min afterdrug onset, (2) 3060 min after drug
onset, and (3) 6090min after drug onset. Baseline temperature
values andchanges from baseline temperature were analyzed by
fit-ting linear models using Generalized Estimating Equations(GEEs;
Liang and Zeger 1986) to account for the cor-relation between
repeated measures on the same animal.The individual difference
group (II, AT, or NR) and thedrug condition (N2O or placebo) were
factors and session(27) was used as a continuous independent
variable. Alltwo-way interactions and the three-way interaction
werealso included in the models. Statistical significance was
de-termined using empiricalWald tests (Liang and Zeger 1986).One
GEE analysis was performed for baseline tempera-tures and three
separate GEE analyses were performed forchanges from baseline over
each of the three time intervals(030, 3060, and 6090 min). The
analysis of temper-ature changes included the baseline temperature
as a pre-caution to protect against spurious associations due
todifferences between groups in baseline temperature.
Results
Of the 400 rats (ten squads) initially screened, 13 had
un-usable data resulting from E-mitter failure. Of the 387remaining
rats, 96 were categorized into the three indi-vidual difference
groupings as follows: II=34, AT=37,NR=25. These 96 rats had extreme
values for the combi-nation of drug effect and acute tolerance
Z-scores (Fig. 2a).The mean temperature curves during the initial
screeningsession with 60% N2O for each of the three groups
dem-onstrate that the groups fit the intended profiles (Fig.
2b).The average Z-scores for each of the selected groups of
ratswere: 1.48 (drug effect) and 0.18 (acute tolerance) for the
51
-
II group, 0.96 (drug effect) and 1.36 (acute tolerance) forthe
AT group, and 1.13 (drug effect) and 1.70 (acutetolerance) for the
NR group. These mean Z-scores reflecthighly selected subgroups of
animals; the probability ofrandomly selecting three groups with
these characteristicsis vanishingly small. The mean (SD) baseline
core temper-ature for each individual difference group was:
37.23C(0.45) for the II group, 37.11C (0.48) for the AT group,
and37.27C (0.31) for the NR group. After the onset of N2O,the mean
(SD) maximal hypothermia (i.e., lowest coretemperature) for each
individual difference group was:37.00C (0.48) for the II group,
35.58C (0.44) for the ATgroup, and 35.61C (0.60) for the NR group.
Since rats ineach individual difference group were assigned
randomlyto receive placebo gas or 60% N2O during the subsequentsix
test sessions, there was a similar distribution of the drugeffect
and acute tolerance regression residual Z-scores forthe placebo and
N2O conditions, within each individualdifference grouping (Fig.
2a).Figure 3 depicts how core temperature changed over six
additional N2O exposures as a function of an individualsinitial
(in)sensitivity and acute tolerance development toN2O. GEE analysis
provided no evidence for differencesin baseline temperature by
individual difference group (p=0.68), by drug condition (p=0.39),
or by session (p= 0.44)(see Table 1). The two-way interactions
(GroupSession,GroupDrug, DrugSession) and the three-way
interaction(GroupDrugSession) were also nonsignificant
(p=0.32,0.17, 0.55, and 0.45, respectively). Results from GEE
anal-ysis of temperature change from baseline over repeatedN2O or
placebo exposures demonstrated distinct patternsfor the three
individual difference groups. Results are pre-sented separately
below for each of the three 30-min post-baseline time
intervals.
For the 0- to 30-min time interval (Fig. 4), there
weresignificant differences among individual difference groupsin
the effect of N2O at Session 2 (p
- the effect in the 0- to 30-min interval, namely, a
hyper-thermia of 0.18C (compare with 0.22C for 030 min),and there
was no evidence for a change in core tempera-ture across sessions
(p=0.44). For the AT group, there wasa significant (p
- with 0.22 and 0.18C for the other two time intervals), andthere
was no evidence for a change in core temperatureacross sessions
(p=0.99). For the AT group, there wasa significant (p
-
tial N2O administration, the AT group exhibited
significanthyperthermia during the initial 30 min of N2O
inhalationfor each of the final three sessions (Fig. 4, 030 min).
Thedirect observation of hyperthermia argues that a warmingadaptive
response is recruited during the development ofchronic tolerance.
This adaptive response occurs shortlyafter N2O onset in
anticipation of the upcoming drug ef-fect. Furthermore, the
hyperthermia is of sufficient magni-tude to counter N2Os
hypothermic drug effect and bringscore temperature to control
levels during the final hourof the last three sessions. Presumably,
the NR rats alsoactivate a warming adaptive response during chronic
tol-erance development. However, the less robust/effectiveadaptive
responses made by the NR group are not suffi-cient to create a
statistically significant hyperthermia andare thus insufficient to
fully counter the hypothermic ef-fects of N2O. Based on adaptation
models of addiction,individuals with a weaker adaptive response may
be ex-pected to be less vulnerable to developing addiction.The
second hypothesis tested was whether rats that are
initially insensitive to N2O hypothermia (II) would devel-op
altered core temperature during repeated N2O admin-istrations. We
expected the II group to rejoin its controlgroup rapidly and to
remain that way over the remainderof the exposure sessions.
However, by the second N2Oadministration, the II group surpassed
the temperature ofthe placebo control group (i.e., moved in the
hyperthermicdirection) and this prolonged hyperthermic effect
persistedacross the remainder of the sessions (Figs. 3, 4). Based
onthese differences between the N2O group and placebocontrol group,
it is inaccurate to view N2O as being rela-tively inert (i.e.,
having little impact on temperature regu-latory mechanisms) in rats
that appear initially insensitiveto N2Os hypothermic effects.A
provocative implication of these findings has to do
with the nature of regulatory control systems in
initiallyinsensitive individuals. During the initial N2O
adminis-tration, II rats may rapidly activate adaptive
regulatorymechanisms that minimize the hypothermic drug
perturba-tion such that core temperature is defended (i.e., little
drugeffect is observed). However, during subsequent drug
ad-ministrations, these warming responses are so robust thatthey
cause core temperature to overshoot control valuesand the rat
becomes hyperthermic. Indeed, the II rat ex-periences a
withdrawal-like effect in the presence of thedrug. This type of
dysregulation could contribute to a rapidescalation of drug taking.
As can occur for drug-dependentindividuals who take a drug to
ameliorate withdrawal ef-fects (Baker et al. 2004), II rats could
attempt to restorenormothermia by countering the withdrawal-like
hyperther-mia caused by their own dysregulated warming response
byincreasing the hypothermic drug effect through increaseddrug
consumption. It may be this adaptive over-responsive-ness of the
regulatory system in initially insensitive individ-uals that puts
them at increased vulnerability for addiction.Future research will
need to assess whether the hyperther-mia observed in II rats during
repeated N2O administrationsreflects a perturbation away from the
defended core tem-perature or, alternatively, represents a
drug-induced allo-
static (Koob and LeMoal 2001) increase in the defendedcore
temperature. It is important to distinguish betweendrug-induced
changes in body temperature that result frombeing forced away from
the set point versus those that resultfrom a change in set point
temperature because these dif-ferent scenarios activate quite
different regulatory responses(Gordon 2001).Direct observation of
hyperthermia in the II group during
subsequent N2O exposures (Sessions 27) suggests that anopponent
regulatory response is present during those ses-sions. The II rats
may also make an adaptive opponent re-sponse within minutes of the
initial N2O exposure that issufficiently robust to prevent
significant hypothermia fromdeveloping and thereby cause the
appearance of initial in-sensitivity. However, without direct
evidence of hyperther-mia during the initial exposure, this
hypothesis dependsupon an unobserved underlying process. To
investigatepossible underlying processes, our lab has begun to
mea-sure metabolic heat production and heat loss, the two prox-imal
determinants of core temperature. We simultaneouslyquantify heat
production using indirect calorimetry, heatloss using direct
calorimetry, and core temperature viatelemetry. On average, rats
become hypothermic to asteady-state administration of 60% N2O
because of arapid reduction in heat production and an increase in
heatloss (Kaiyala and Ramsay 2005). Unpublished
individualdifference data from our lab indicate that it is possible
fora rat to appear initially insensitive to N2Os hypothermiceffects
despite exhibiting an N2O-induced increase in heatloss that is
comparable to what is observed in rats thatexhibit a significant
hypothermia to N2O. In this case, therat appears initially
insensitive at the level of core tem-perature because the typical
increase in heat loss is largelyoffset by an increase in heat
production. This observationsupports the hypothesis that although a
drug can exert itspharmacological effect in an initially
insensitive individ-ual, little or no change is evident in the
dependent mea-sure because the individuals adaptive response
effectivelycounters the drug-induced regulatory disturbance
(Dworkin1993; Ramsay and Woods 1997). If effective opponentadaptive
responses are occurring in the II group duringtheir initial N2O
exposure, it is unclear why these re-sponses become excessive
(i.e., dysregulated) and resultin a persistent hyperthermia with
repeated exposure. Re-search that identifies the specific
unconditioned responsesthat are triggered by a drugs initial effect
is likely toprovide insight into the nature of the conditioned
re-sponses that develop with repeated drug exposures andmodify the
measured variable (Dworkin 1993; Ramsayand Woods 1997; Siegel et
al. 2000). The developmentof hyperthermia in the II group is
consistent with thepossibility that increased heat production is
the uncon-ditioned response and that the ... conditioned
reflexresembles the unconditioned reflex, and as it develops,
itaugments the effect of the unconditioned reflex (Dworkin1993, p.
38).The findings of this study prompt a discussion about
the interpretation and measurement of chronic tolerance.Chronic
tolerance is a reduction in the magnitude of drug-
55
-
induced change in a dependent measure that develops overrepeated
drug exposures. This can be seen as a shift to theright in the
doseeffect curve indicating that a larger drugdose is required to
elicit the same magnitude of effect in atolerant individual as is
observed in a drug-nave controlsubject (L et al. 1992). Chronic
tolerance can also be mea-sured as the degree of reduction in a
drug-induced changein a dependent measure that develops when a
constantdrug dose is administered repeatedly. The present studyused
the latter method by repeatedly administering a 60%N2O
concentration to evaluate chronic tolerance develop-ment. In the
case of chronic tolerance development, thelargest drug-induced
deviation from baseline (or a controlgroup defined baseline)
typically occurs during an initialdrug administration and then the
magnitude of this dis-crepancy diminishes over repeated
administrations as tol-erance develops. Conceptually, there would
be no tolerancedevelopment if the initial degree of drug-induced
devia-tion did not change over repeated drug administrationswhile
full/complete tolerance development would occurif the amount of
drug-induced change in the dependentvariable diminishes to the
extent that it is indistinguishablefrom baseline or control
values.Common methods to quantify chronic tolerance devel-
opment include measuring the change over sessions ineither the
maximum deviation from baseline (i.e., sensi-tivity) or the area
under the curve (i.e., the total or inte-grated effect). The
different patterns of chronic tolerancedata collected for the three
individual difference groupsillustrate shortcomings of this
analytical approach (Fig. 3).During the first 30 min of the final
three drug adminis-tration sessions, the NR group is considered the
most tol-erant of the three groups because its core temperature
ismost similar to that of its control group (Fig. 4). Yet,
theinability of the NR group to mount a more powerful hy-perthermic
response during this initial 30-min period mayexplain why these
rats are the least tolerant during the finalhour of the drug
administration (Fig. 4). During the finalthree drug administration
sessions, the AT group is the mostchronically tolerant of the
groups when considering thefinal hour of the drug exposure (Fig.
4). The AT groupshyperthermic deviation away from control values
duringthe first 30 min of the final drug exposure sessions maybe
responsible for the full chronic tolerance that resultsduring the
following hour. How then should the II groupbe described in terms
of tolerance development consider-ing that they began with a high
degree of initial insensi-tivity or innate tolerance (Kalant et al.
1971)? Relativeto their initial exposure to N2O, the II group moved
fur-ther away from their control values during subsequent
ex-posures (i.e., Sessions 27) that could be described asdeveloping
more than 100% tolerance (Fig. 4). Should theII group be described
as being hypertolerant or overlytolerant? The point is that if
there are different patterns ofchronic tolerance development (see
Fig. 3), then simplesummary measures such as area under the curve
or maxi-mum drug effect serve to mask these patterns. Further,
theexistence of these distinct patterns of change over re-
peated drug administrations illustrate the limitations ofour
current use of the term tolerance.
Perspectives There is a wealth of human and animal liter-ature,
primarily from research on ethanol, that investigateswhether
characteristics measured during an initial drugadministration
predict chronic tolerance or the magnitudeof subsequent drug
consumption. For example, early workindicated that young men with a
family history of alco-holism report being less sensitive to
ethanols effects thando control subjects (Schuckit 1980). Schuckit
and col-leagues (2001) estimate that 40% of children of alco-holics
are relatively insensitive to ethanol while only 10%of children of
nonalcoholics have this characteristic. Ani-mal research has
investigated whether these initial intra-sessional factors are
associated with subsequent chronictolerance development or drug
consumption by using ro-dents from outbred and inbred strains, as
well as knock-out mice and selectively bred lines for drug
consumption,drug sensitivity, and acute tolerance [e.g., outbred
strains(Tabakoff and Culp 1984; San-Marina et al. 1989; Khannaet
al. 1990b, 1991); inbred strains (Crabbe et al. 1982,1994; Tabakoff
and Culp 1984; Khanna et al. 1990a;Gehle and Erwin 2000); knock-out
mice (Naassila et al.2002); lines selectively bred for consumption
(Tampierand Mardones 1999; Tampier et al. 2000; Bell et al.2001);
lines selectively bred for sensitivity (Khanna et al.1985; Crabbe
et al. 1989; Limm and Crabbe 1992; Crabbe1994; Browman et al. 2000;
Deitrich et al. 2000; Draskiet al. 2001; Palmer et al. 2002); lines
selectively bred foracute tolerance (Deitrich et al. 2000; Rustay
et al. 2001;Wu et al. 2001)]. While the scientific literature is in
generalagreement that initial sensitivity and acute tolerance
arerelevant to the subsequent development of chronic toler-ance and
drug consumption, a coherent description of thisrelationship has
not emerged. Newlin and Thomson (1990)describe the human literature
on whether offspring of al-coholics are more or less sensitive to
alcohol as beingremarkably inconsistent (p. 385). Khanna and
colleagues(1990b) describe the animal literature on the
relationshipbetween sensitivity and tolerance to alcohol
consumptionas being inconclusive, because of contradictory
results(p. 429). More recently, Ponomarev and Crabbe (2002)state
that It is not clear how initial sensitivity and acutetolerance
individually contribute to alcohol abuse (p. 257)and they suggest a
novel method to improve animal re-search on the topic. Much of this
literature discusses thefactors that contribute to this lack of
clarity. Describingsome of these factors places our current study
in propercontext.Too few intermittent measurements of a dependent
var-
iable can make it difficult to assess initial sensitivity
(i.e.,observe the maximal drug effect) and to measure acute
tol-erance (Khanna et al. 1985; San-Marina et al. 1989). Like-wise,
too few measurements of the drug concentration alsocomplicate this
assessment especially when drug concen-trations are rapidly
changing (L et al. 1992; Deitrich et al.2000; Gehle and Erwin 2000;
Rustay et al. 2001). Fur-
56
-
thermore, venous blood measurements of the drug con-centration
often do not reflect the drug concentration in thebrain (Wu et al.
2001; L et al. 1992). To circumvent thesemethodological problems, a
compelling rationale has beenmade for measuring acute tolerance at
steady-state drug con-centrations for ethanol (Ramchandani et al.
1999; Froehlichet al. 2001) and for other drugs as well (Kissin et
al. 1996;Kaiyala et al. 2001). Measuring a dependent variable
con-tinuously at steady-state drug concentrations facilitates
themeasurement of initial sensitivity and acute tolerance.Many
dependent variables have been used to measure
drug effects (L et al. 1992). Estimates of drug sensitivityand
tolerance often do not generalize across dependentmeasures but
instead are task-specific (San-Marina et al.1989; Deitrich et al.
2000). Interpreting the relationship be-tween initial sensitivity,
acute tolerance, and chronic toler-ance is facilitated when they
are investigated in the samestudy with a consistent dependent
measure. Some depen-dent variables are affected by the measurement
procedureitself and associated handling. A good example is
coretemperature measurement in rodents where the act of tak-ing a
rectal temperature changes core temperature and canalter the
apparent magnitude of the drug effect (Peris andCunningham 1986).
Dependent measures assessing drugeffects can also be influenced by
intoxicated practice (Wengeret al. 1981; L and Kalant 1992; L et
al. 1992; Zack andVogel-Sprott 1995). These are but examples of the
factorsthat make it difficult to draw general conclusions from
stud-ies that use different methods and dependent measures.There is
often both a conceptual and an analytical con-
founding of initial sensitivity and acute and chronic
tolerance.Numerous investigators have recognized that measures
ofinitial sensitivity often represent a mixture of sensitivityand
acute tolerance development (San-Marina et al. 1989;Khanna et al.
1990a, b, 1991; Ramsay and Woods 1997;Deitrich et al. 2000; Gehle
and Erwin 2000; Ponomarev andCrabbe 2002). Research investigating
how initial drugsensitivity, acute tolerance, and chronic tolerance
are re-lated is susceptible to finding spurious associations
be-cause a baseline value can influence the size of the drugeffect
(sensitivity) that in turn can influence the amount ofacute and
chronic tolerance that can develop. For example,the absence of a
large initial drug effect (i.e., as seen in aninitially insensitive
individual) prevents a large amount ofacute or chronic tolerance
from developing because there islittle deviation to recover from
when a drug effect is small(Khanna et al. 1985; San-Marina et al.
1989). The recom-mended strategy for testing these relationships is
to useresidual scores from regression analyses to quantify
indi-vidual differences in initial sensitivity and tolerance
ratherthan difference or ratio scores (Nagoshi et al. 1986; Grantet
al. 1989). Unfortunately, the improper use of differencescores to
relate initial sensitivity and tolerance can com-plicate
interpretation of the literature (e.g., see Fig.1 ofSan-Marina et
al. 1989).The experimental paradigm selected for our current
study has numerous strengths. N2O is a hypothermic drugthat
equilibrates quickly throughout the body and is wellsuited for
steady-state administrations (Eger 1985). N2O is
inhaled and thus there are no surgical procedures neededto
enable drug administration. This made it feasible to in-vestigate
individual differences using a large number ofsubjects because of
the ease with which prolonged steady-state drug concentrations
could be achieved over multiplesessions. Pharmacokinetic
explanations for changes in thedependent variable during a
steady-state N2O administra-tion are eliminated because there are
no significant meta-bolic pathways for N2O (Trudell 1985). Core
temperaturedata are collected continuously and noninvasively at
aknown steady-state N2O concentration. This facilitates
themeasurement of initial sensitivity and acute and
chronictolerance. Using core temperature as the primary depen-dent
variable also builds on an extensive body of drugtolerance
research. The experimental design incorporatesmeasures of initial
sensitivity, acute tolerance, and chronictolerance in the same
study. The data analytical proceduresemploy regression residual
scores to avoid spurious find-ings that could result from using
simple difference scores.Outbred rats were used to study individual
differences sothat the predictive utility of any associations could
be rel-evant to a heterogeneous population (San-Marina et al.1989).
The ability to screen large numbers of rats effi-ciently permitted
the use of a selective screening process tocreate distinct
individual difference groups that enhancedour ability to visualize
the effect that these differences hadon chronic tolerance
development. Thus, this experimen-tal paradigm was able to address
and circumvent many ofthe problematic factors common to this type
of research.Of course, the present study also has its limitations.
It is
not known whether the relationships found in the presentstudy
apply to other drugs, species, or dependent variables.It is
possible to evaluate whether these findings generalizeto
ethanol-induced hypothermia in rats by using the steady-state
ethanol infusion method described by Froehlich andcolleagues
(2001). It is also important to determine whetherthe relationships
observed in this study reflect a processthat is common to other
regulated physiological systems orif the findings are specific to
the temperature regulatorysystem. If unusually adaptive control
systems exist in someindividuals for psychophysiologically
regulated variablesthat motivate drug taking (e.g., hedonic or
affective state),then being initially insensitive in regard to such
variablescould be the result of a relatively prompt and
excessiveactivation of adaptive responses causing
withdrawal-likesymptoms that could motivate an escalation of drug
use.Our observation of a withdrawal-like shift at the level ofcore
temperature in the II rats (Fig. 3) suggests a novelhypothesis to
explain the documented association betweeninitial drug (alcohol)
insensitivity and addictive vulnera-bility. However, extending our
present research paradigmto investigate the effect of individual
differences in sen-sitivity and tolerance on drug consumption is
hampered bythe minimal work on N2O self-administration methods.N2O
is a drug of abuse (Layzer 1985) and although self-administration
methods exist for monkeys (Grubman andWoods 1982; Nemeth and Woods
1982; Wood et al. 1977),there is only a single published study
investigating N2Oself-administration methods in the rat (Ramsay et
al. 2003).
57
-
Finally, chronic tolerance development was evaluated overseven
N2O exposure sessions. It is possible that the ob-served individual
differences in chronic tolerance devel-opment could change with
additional exposure sessions.
Conclusion The present data provide new insight into
thephenomenon of chronic drug tolerance. As chronic
tolerancedevelops over repeated drug administrations, the
prevailingbelief has been that the perturbed variable is returning
to-ward a baseline or control value. The among-subject var-iability
in the speed and magnitude of chronic tolerancedevelopment
typically has been viewed as error variabilitythat obscures a
single common underlying trajectory. Inthe present study, stringent
criteria were used to select in-dividual outbred rats for further
study based on reliable in-dividual difference characteristics in
sensitivity and acutetolerance (i.e., NR, AT, and II) that were
assessed during aninitial drug exposure. Importantly, these
individual differ-ences predict qualitatively different patterns of
chronictolerance development. We believe the effect of these
in-dividual differences on chronic tolerance has gone unno-ticed
because research often emphasizes group means thatcan obscure
meaningful individual differences. The causesof these individual
differences in chronic tolerance de-velopment may be relevant to
understanding individualdifferences in addictive vulnerability and
warrant furtherinvestigation.
Acknowledgements This investigation was supported by theNational
Institute on Drug Abuse (DA010611 and DA016047). Wealso acknowledge
Chris Prall and Chae Watson for their technicalcontributions to
this study.
References
Baker TB, Piper ME, McCarthy DE, Majeskie MR, Fiore MC(2004)
Addiction motivation reformulated: an affective process-ing model
of negative reinforcement. Psychol Rev 111:3351
Bell RL, Stewart RB, Woods JE II, Lumeng L, Li TK, Murphy
JM,McBride WJ (2001) Responsivity and development of toler-ance to
the motor impairing effects of moderate doses ofethanol in
alcohol-preferring (P) and-nonpreferring (NP) ratlines. Alcohol
Clin Exp Res 25:644650
Brick J, Pohorecky LA, Faulkner W, Adams MN (1984)
Circadianvariations in behavioral and biological sensitivity to
ethanol.Alcohol Clin Exp Res 8:204211
Browman KE, Rustay NR, Nikolaidis N, Crawshaw L, Crabbe JC(2000)
Sensitivity and tolerance to ethanol in mouse linesselected for
ethanol-induced hypothermia. Pharmacol BiochemBehav 67:821829
Crabbe JC (1994) Tolerance to ethanol hypothermia in HOT andCOLD
mice. Alcohol Clin Exp Res 18:4246
Crabbe JC, Janowsky TS, Young ER, Kosobud A, Stack J, Rigter
H(1982) Tolerance to ethanol hypothermia in inbred mice: geno-typic
correlations with behavioral responses. Alcohol Clin ExpRes
6:446458
Crabbe JC, Feller DJ, Dorow JS (1989) Sensitivity and tolerance
toethanol-induced hypothermia in genetically selected mice.
JPharmacol Exp Ther 249:456461
Crabbe JC, Belknap JK, Mitchell SR, Crawshaw LI
(1994)Quantitative trait loci mpping genes that influence the
sensi-tivity and tolerance to ethanol-induced hypothermia in
BXDrecombinant inbred mice. J Pharmacol Exp Ther 269:184192
Crabbe JC, Phillips TJ, Buck KJ, Cunningham CL, Belknap JK(1999)
Identifying genes for alcohol and drug sensitivity: recentprogress
and future directions. Trends Neurosci 22:173179
Deitrich RA, Bludeau P, Erwin VG (2000) Phenotypic andgenotypic
relationships between ethanol tolerance and sensi-tivity in mice
selectively bred for initial sensitivity to ethanol(SS and LS) or
development of acute tolerance (HAFT andLAFT). Alcohol Clin Exp Res
24:595604
Draski LJ, Bice PJ, Deitrich RA (2001) Developmental
alterationsof ethanol sensitivity in selectively bred high and low
alcoholsensitive rats. Pharmacol Biochem Behav 70:387396
Dworkin BR (1993) Learning and physiological regulation.
TheUniversity of Chicago Press, Chicago
Eger EI II (1985) MAC. In: Eger EI II (ed) Nitrous
oxide/N2O.Elsevier Science Publishing Company, New York, pp
5767
Fenoglio P, Parel V, Kopp P (2003) The social cost of
alcohol,tobacco and illicit drugs in France. Eur Addict Res
9:1828
Froehlich JC, Janowsky RB, Li TK, Mosemiller AK, McCulloughDE,
Ho MC, Kisner JM (2001) Induction of steady-state bloodalcohol
levels: application to the study of within-session alco-hol
tolerance in rats. Alcohol Clin Exp Res 25:370376
Gehle VM, Erwin VG (2000) The genetics of acute
functionaltolerance and initial sensitivity to ethanol for an
ataxia test inthe LsxSS RI strains. Alcohol Clin Exp Res
24:579587
Gordon CJ (2001) The therapeutic potential of regulated
hypother-mia. J Emerg Med 18:8189
Grant KA, Werner R, Hoffman PL, Tabakoff B (1989)
Chronictolerance to ethanol in the N: NIH rat. Alcohol Clin Exp
Res13:402406
Grubman J, Woods JH (1982) Effects of morphine and cocaine
onresponding under a multiple schedule of food or nitrous
oxidepresentation. In: Saito S, Yanagita T (eds) Learning and
memorydrugs as reinforcers. Excerpta medica: international
congressseries 620, pp 259274
Hastie TJ (1992) Generalized additive models. In: Chambers
JM,Hastie TJ (eds) Statistical models. S. Wadsworth &
Brooks/Cole Advanced Books & Software, Pacific Grove, CA, pp
249307
Heath AC, Madden PA, Bucholz KK, Dinwiddie SH, Slutske WS,Bierut
LJ, Rohrbaugh JW, Statham DJ, Dunne MP, WhitfieldJB, Martin NG
(1999) Genetic differences in alcohol sensitivityand the
inheritance of alcoholism risk. Psychol Med 29:10691081
Jaffe JH (1985) Drug addiction and drug abuse. In: Gilman
AG,Goodman LS, Rall TW, Murad F (eds) Goodman and Gillmansthe
pharmacological basis of therapeutics, 7th edn.
MacMillanPublishing, New York, pp 532581
Kaiyala KJ, Ramsay DS (2005) Assessment of heat production,
heatloss, and core temperature during nitrous oxide exposure: a
newparadigm for studying drug effects and opponent responses.Am J
Physiol Regul Integr Comp Physiol 288:692701
Kaiyala KJ, Leroux BG, Watson CH, Prall CW, Coldwell SE,
WoodsSC, Ramsay DS (2001) Reliability of individual differences
ininitial sensitivity and acute tolerance to nitrous oxide
hypother-mia. Pharmacol Biochem Behav 68:691699
Kalant H, LeBlanc AE, Gibbins RJ (1971) Tolerance to, and
de-pendence on, some non-opiate psychotropic drugs. PharmacolRev
23:135191
Kest B, Palmese CA, Hopkins E, Adler M, Juni A, Mogil JS
(2002)Naloxone-precipitated withdrawal jumping in 11 inbred
mousestrains: evidence for common genetic mechanisms in acute
andchronic morphine physical dependence. Neuroscience
115:463469
Khanna JM, L AD, LeBlanc AE, Shah G (1985) Initial
sensitivityversus acquired tolerance to ethanol in rats selectively
bred forethanol sensitivity. Psychopharmacology 86:302306
Khanna JM, Kalant H, Chau AK, Sharma H (1990a) Initial
sen-sitivity, acute tolerance and alcohol consumption in four
inbredstrains of rats. Psychopharmacology 101:390395
Khanna JM, Kalant H, Shah G, Sharma H (1990b) Comparison
ofsensitivity and alcohol consumption in four outbred strains
ofrats. Alcohol 7:429434
58
-
Khanna JM, Kalant H, Sharma H, Chau AK (1991) Initial
sensi-tivity, acute tolerance and alcohol consumption in Fischer
344and Long Evans rats. Psychopharmacology 105:175180
Kissin I, Lee SS, Arthur GR, Bradley EL Jr (1996) Time
coursecharacteristics of acute tolerance development to
continuouslyinfused alfentanil in rats. Anesth Analg 83:600605
Koob GF, LeMoal M (1997) Drug abuse: hedonic
homeostaticdysregulation. Science 278:5258
Koob GF, LeMoal M (2001) Drug addiction, dysregulation ofreward,
and allostasis. Neuropsychopharmacology 24:97129
Layzer RB (1985) Nitrous oxide abuse. In: Eger EI II (ed)
Nitrousoxide/N2O. Elsevier Science Publishing Company, New York,pp
249257
L AD, Kalant H (1992) Influence of intoxicated practice on
thedevelopment of acute tolerance to the motor impairment effectof
ethanol. Psychopharmacology 106:572576
L AD, Mihic SJ, Wu PH (1992) Alcohol tolerance:
methodologicaland experimental issues. In: Boulton A, Baker G, Wu
PH (eds)Neuromethods, vol 24: animal models of drug
addiction.Humana Press, Totowa, NJ, pp 95124
Lewis JL, Pruhs RJ, Quock RM (1987) Modification of an
infantincubator for exposure of experimental animals to
nitrousoxide. J Pharmacol Methods 18:143150
Liang KY, Zeger SL (1986) Longitudinal data analysis
usinggeneralized linear models. Biometrika 73:1322
Limm M, Crabbe JC (1992) Ethanol tolerance in a genetically
insen-sitive selected mouse line. Alcohol Clin Exp Res
16:800805
McBride WJ, Li T-K (1998) Animal models of
alcoholism:neurobiology of high alcohol-drinking behavior in
rodents.Crit Rev Neurobiol 12:339369
McGinnis JM, Foege WH (1999) Mortality and morbidityattributable
to use of addictive substances in the United States.Proc Assoc Am
Physicians 111:109118
Naassila M, Ledent C, Daoust M (2002) Low ethanol sensitivity
andincreased ethanol consumption in mice lacking adenosine
A2Areceptors. J Neurosci 22:1048710493
Nagoshi CT, Wilson JR, Plomin R (1986) Use of
regressionresiduals to quantify individual differences in acute
sensitivityand tolerance to alcohol. Alcohol Clin Exp Res
10:343349
Nemeth MA, Woods JH (1982) Effects of morphine and cocaine
onresponding under a multiple schedule of food or nitrous
oxidepresentation. In: Saito S, Yanagita T (eds) Learning and
mem-ory drugs as reinforcers. Excerpta medica: international
con-gress series, vol. 620, pp 275285
Newlin DB, Thomson JB (1990) Alcohol challenge with sons
ofalcoholics: a critical review and analysis. Psychol Bull
108:383402
OBrien CP (1997) A range of research-based pharmacotherapiesfor
addiction. Science 278:6670
Palmer AA, Moyer MR, Crabbe JC, Phillips TJ (2002)
Initialsensitivity, tolerance and cross-tolerance to
allopregnanolone-and ethanol-induced hypothermia in selected mouse
lines.Psychopharmacology 162:313322
Peper A (2004) A theory of drug tolerance and dependence I:
aconceptual analysis. J Theor Biol 229:477490
Peris J, Cunningham CL (1986) Handling-induced enhancement
ofalcohols acute physiological effects. Life Sci 38:273279
Pertwee RG, Marshall NR, MacDonald AG (1990)
Behaviouralthermoregulation in mice: effects of low doses of
generalanaesthetics of different potency. Exp Physiol 75:629637
Piazza PV, LeMoal M (1996) Pathophysiological basis of
vulner-ability to drug abuse: role of an interaction between
stress,glucocorticoids, and dopaminergic neurons. Annu Rev
Phar-macol Toxicol 36:359378
Ponomarev I, Crabbe JC (2002) A novel method to assess
initialsensitivity and acute tolerance to hypnotic effects of
ethanol. JPharmacol Exp Ther 302:257263
Poulos CX, Cappell H (1991) Homeostatic theory of drug
tolerance:a general model of physiological adaptation. Psychol
Rev98:390408
Quock RM, Panek RW, Kouchich FJ, Rosenthal MA (1987)
Nitrousoxide-induced hypothermia in the rat. Life Sci 41:683690
Ramchandani VA, OConnor S, Blekher T, Kareken D, Morzorati
S,Nurnberger J Jr, Li TK (1999) A preliminary study of
acuteresponses to clamped alcohol concentration and family
historyof alcoholism. Alcohol Clin Exp Res 23:13201330
Ramsay DS, Woods SC (1997) Biological consequences of a
drugadministration: implications for acute and chronic
tolerance.Psychol Rev 104:170193
Ramsay DS, Omachi K, Leroux BG, Seeley RJ, Prall C, Woods
SC(1999) Nitrous oxide-induced hypothemia in the rat: acute
andchronic tolerance. Pharmacol Biochem Behav 62:189196
Ramsay DS, Watson C, Leroux BG, Prall CW, Kaiyala KJ
(2003)Conditioned place aversion and self-administration of
nitrousoxide in rats. Pharmacol Biochem Behav 74:623633
Rustay NR, Boehm SL II, Schafer GL, Browman KE, Erwin VG,Crabbe
JC (2001) Sensitivity and tolerance to
ethanol-inducedincoordination and hypothermia in HAFT and LAFT
mice.Pharmacol Biochem Behav 70:167174
San-Marina A, Khanna JM, Kalant H (1989) Relationship
betweeninitial sensitivity, acute tolerance and chronic tolerance
toethanol in a heterogeneous population of Swiss mice.
Psycho-pharmacology 99:450457
Schuckit MA (1980) Self-rating of alcohol intoxication by
youngmen with and without family histories of alcoholism. J
StudAlcohol Toxicol 41:242249
Schuckit MA (1994) Alcohol sensitivity and dependence.
In:Jansson B, Jrnvall H, Rydberg U, Terenius L, Vallee BL(eds)
Toward a molecular basis of alcohol use and abuse.Birkhuser Verlag,
Basel, Switzerland, pp 341348
Schuckit MA, Smith TL (1996) An 8-year follow-up of 450 sons
ofalcoholic and control subjects. Arch Gen Psychiatry 53:202210
Schuckit MA, Edenberg HJ, Kalmijn J, Flury L, Smith TL, Reich
T,Bierut L, Goate A, Foroud T (2001) A genome-wide search forgenes
that relate to a low level of response to alcohol. AlcoholClin Exp
Res 25:323329
Siegel S, Baptista MA, Kim JA, McDonald RV, Weise-Kelly L(2000)
Pavlovian psychopharmacology: the associative basis oftolerance.
Exp Clin Psychopharmacol 8:276293
Single E, Robson L, Rehm J, Xie X, Xi X (1999) Morbidity
andmortality attributable to alcohol, tobacco, and illicit drug use
inCanada. Am J Public Health 89:385390
Solomon RL (1980) The opponent-process theory of
acquiredmotivation: the costs of pleasure and the benefits of pain.
AmPsychol 35:691712
Tabakoff B, Culp SG (1984) Studies on tolerance development
ininbred and heterogeneous stock National Institutes of Healthrats.
Alcohol Clin Exp Res 8:495499
Tabakoff B, Rothstein JD (1983) Biology of tolerance and
de-pendence. In: Tabakoff B, Sutker PB, Randall CL (eds) Medicaland
social aspects of alcohol abuse. Plenum Press, New York,pp
187220
Tampier L, Mardones J (1999) Differences in ethanol sensitivity
andacute tolerance between UChA and UChB rats. J Stud
Alcohol60:168171
Tampier L, Quintanilla ME, Mardones J (2000) Acute
tolerance,ethanol sensitivity and drinking pattern in the F2
generation ofUChA and UChB rats. J Stud Alcohol 61:647651
Trudell JR (1985) Metabolism of nitrous oxide. In: Eger EI II
(ed)Nitrous oxide/N2O. Elsevier Science Publishing Company,New
York, pp 203210
Wenger JR, Tiffany TM, Bombardier C, Nicholls K, Woods SC(1981)
Ethanol tolerance in the rat is learned. Science 213:575577
Wood RW, Grubman J, Weiss B (1977) Nitrous oxide
self-ad-ministration in the squirrel monkey. J Pharmacol Exp
Ther202:491499
Wu PH, Tabakoff B, Szab G, Hoffman PL (2001) Chronic
ethanolexposure results in increased acute functional tolerance
inselected lines of HAFT and LAFT mice.
Psychopharmacology155:405412
Zack M, Vogel-Sprott M (1995) Behavioral tolerance and
sensiti-zation to alcohol in humans: the contribution of learning.
ExpClin Psychopharmacol 3:396401
59
Individual differences in initial sensitivity and acute
tolerance predict patterns of chronic drug tolerance to
nitrous-oxide-induced hypothermia in
ratsAbstractAbstractAbstractAbstractAbstractAbstractIntroductionMethodsSubjectsSurgery
for core temperature measuresN2O delivery/temperature data
acquisition systemExperimental design and proceduresIndividual
difference group assignmentData analysis
ResultsDiscussionPerspectivesConclusion
References
/ColorImageDict > /JPEG2000ColorACSImageDict >
/JPEG2000ColorImageDict > /AntiAliasGrayImages false
/DownsampleGrayImages true /GrayImageDownsampleType /Bicubic
/GrayImageResolution 150 /GrayImageDepth -1
/GrayImageDownsampleThreshold 1.50000 /EncodeGrayImages true
/GrayImageFilter /DCTEncode /AutoFilterGrayImages true
/GrayImageAutoFilterStrategy /JPEG /GrayACSImageDict >
/GrayImageDict > /JPEG2000GrayACSImageDict >
/JPEG2000GrayImageDict > /AntiAliasMonoImages false
/DownsampleMonoImages true /MonoImageDownsampleType /Bicubic
/MonoImageResolution 600 /MonoImageDepth -1
/MonoImageDownsampleThreshold 1.50000 /EncodeMonoImages true
/MonoImageFilter /CCITTFaxEncode /MonoImageDict >
/AllowPSXObjects false /PDFX1aCheck false /PDFX3Check false
/PDFXCompliantPDFOnly false /PDFXNoTrimBoxError true
/PDFXTrimBoxToMediaBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ]
/PDFXSetBleedBoxToMediaBox true /PDFXBleedBoxToTrimBoxOffset [
0.00000 0.00000 0.00000 0.00000 ] /PDFXOutputIntentProfile (None)
/PDFXOutputCondition () /PDFXRegistryName (http://www.color.org?)
/PDFXTrapped /False
/SyntheticBoldness 1.000000 /Description >>>
setdistillerparams> setpagedevice

![Therapeutic Hypothermia in Traumatic Brain Injurycdn.intechopen.com/pdfs/42406/InTech-Therapeutic... · 80 Therapeutic Hypothermia in Brain Injury hypothermia [13-50]. In addition,](https://img.pdfslide.us/doc/110x75/5e902d36c9c187069d5dbc10/therapeutic-hypothermia-in-traumatic-brain-80-therapeutic-hypothermia-in-brain-injury.jpg)