Embed Size (px)
Citation preview
Indicators of universal healthcare in Ireland
Sara BurkeProject Co-ordinator: Mapping the Pathways to Universal Healthcare Centre for Health Policy and Management, Trinity College Dublin
22 September 2015
Trinity College Dublin, The University of Dublin
Indicators of universal healthcare in Ireland
– Full package• Community, Acute, Long Term Care• Needs based
– Quality• Timely• Integrated – Continuity• Appropriate, Best Practice Clinical
– Coverage for all• Universal means everyone
– Resources • Sufficiency (threshold) • Efficiency (Allocative, Technical – Right
mix)
– Financial protection • Free Care (at point of contact)• Affordable care (progressive, avoid
catastrophic payment and risk of impoverishment)
Developing a suite of indicators to reflect dimensions of UHC
Indicators of Universal healthcare:Package of care
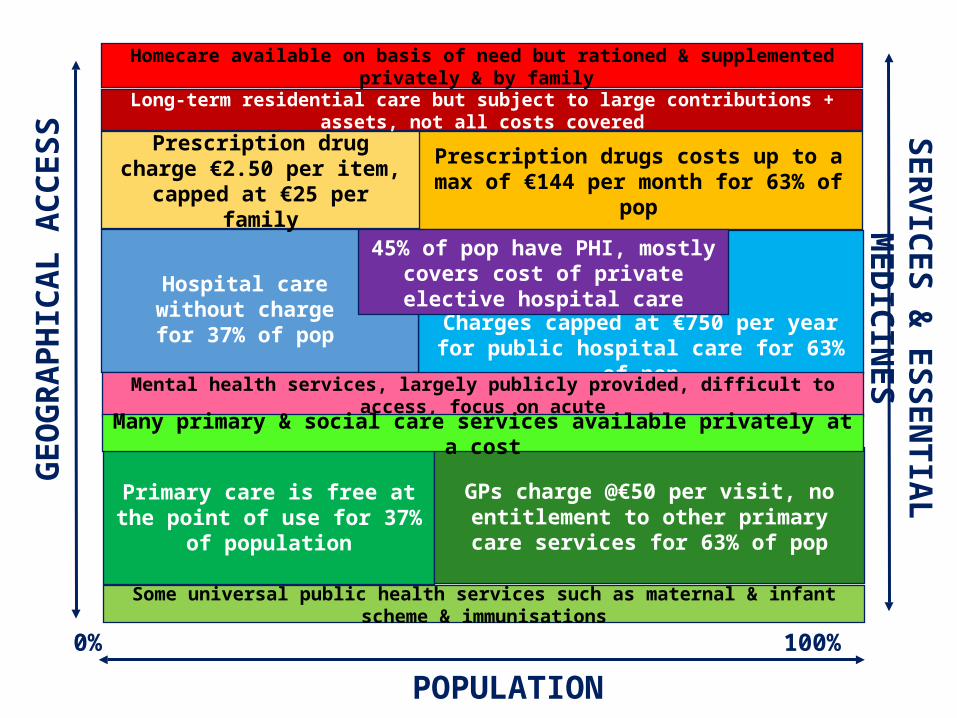
Charges capped at €750 per year for public hospital care for 63% of pop
Primary care is free at the point of use for 37% of population
Homecare available on basis of need but rationed & supplemented privately & by family
POPULATION
SER
VIC
ES
& E
SS
EN
TIA
L
MED
ICIN
ES
0% 100%
Hospital care without charge for 37% of pop
GPs charge @€50 per visit, no entitlement to other primary care services for 63% of pop
Prescription drugs costs up to a max of €144 per month for 63% of pop
Prescription drug charge €2.50 per item, capped at €25 per
family
Some universal public health services such as maternal & infant scheme & immunisations
45% of pop have PHI, mostly covers cost of private elective hospital care
Long-term residential care but subject to large contributions + assets, not all costs covered
Mental health services, largely publicly provided, difficult to access, focus on acute
Many primary & social care services available privately at a cost
GEO
GR
AP
HIC
AL A
CC
ESS

Trinity College Dublin, The University of Dublin
• Subtitle — Source Sans Pro Regular 20pt
2001: Medical cards for all over 70s
2011: Promise of free GP care for all
2008: Universal medical cards for over 70s
withdrawn
2015: free GP care for u’6s & o’70s
2013: tightening up of rules on discretionary medical cads
2011: Promise
of Universal
Health Insurance
2015: UHI costings remain unpublished
Indicators of Universal healthcare:Quality of care
Trinity College Dublin, The University of Dublin
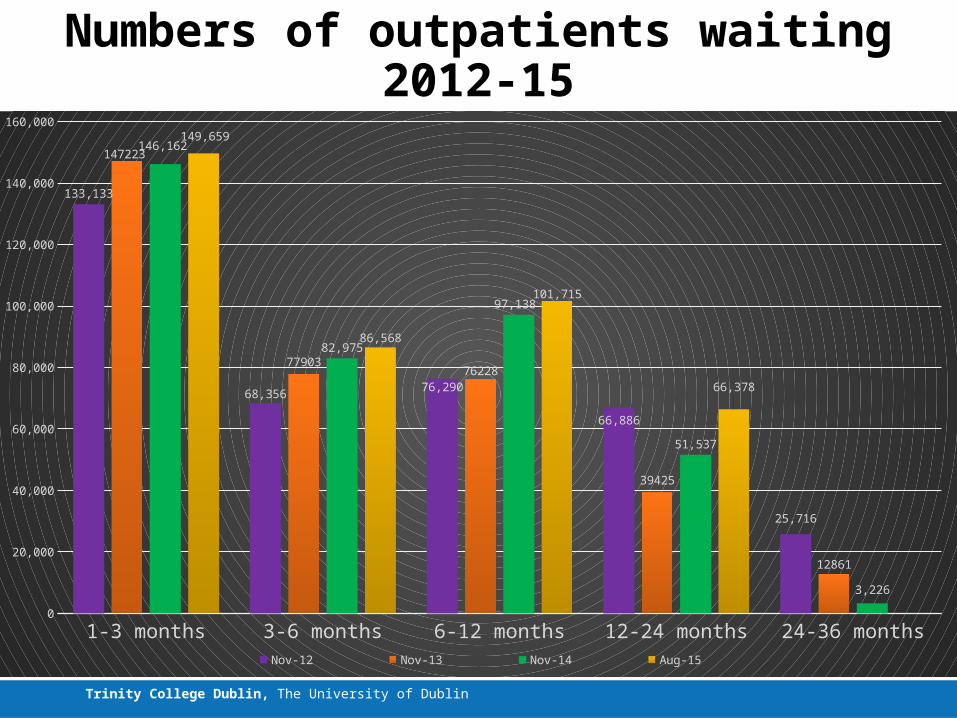
Numbers of outpatients waiting 2012-15
1-3 months 3-6 months 6-12 months 12-24 months 24-36 months0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
133,133
68,356 76,290
66,886
25,716
147223
7790376228
39425
12861
146,162
82,975
97,138
51,537
3,226
149,659
86,568
101,715
66,378
Nov-12 Nov-13 Nov-14 Aug-15
Trinity College Dublin, The University of Dublin
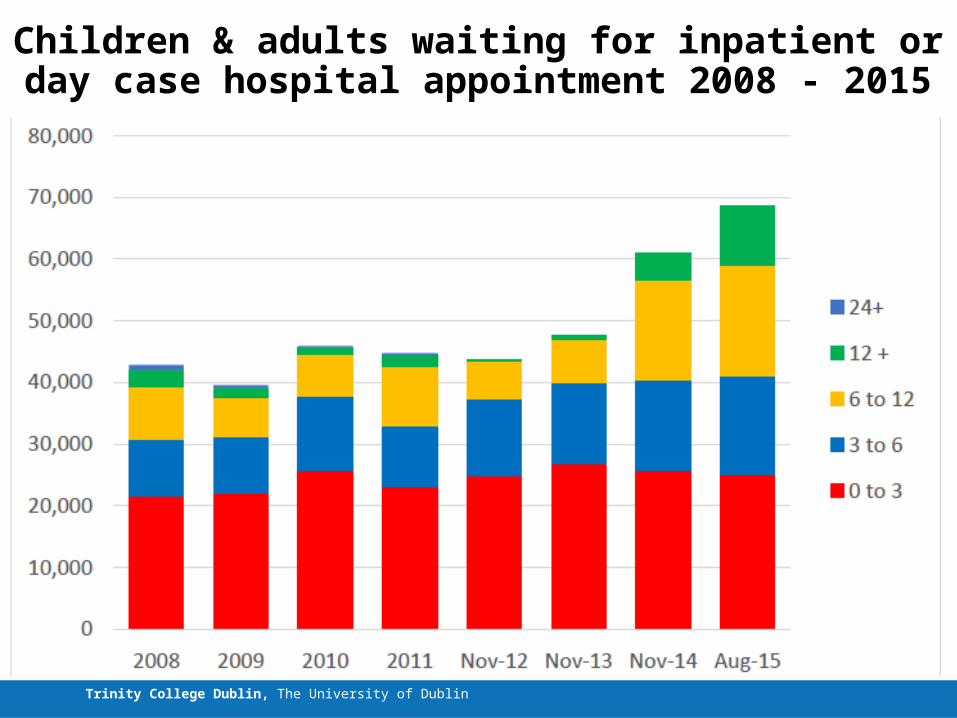
Children & adults waiting for inpatient or day case hospital appointment 2008 - 2015
Trinity College Dublin, The University of Dublin
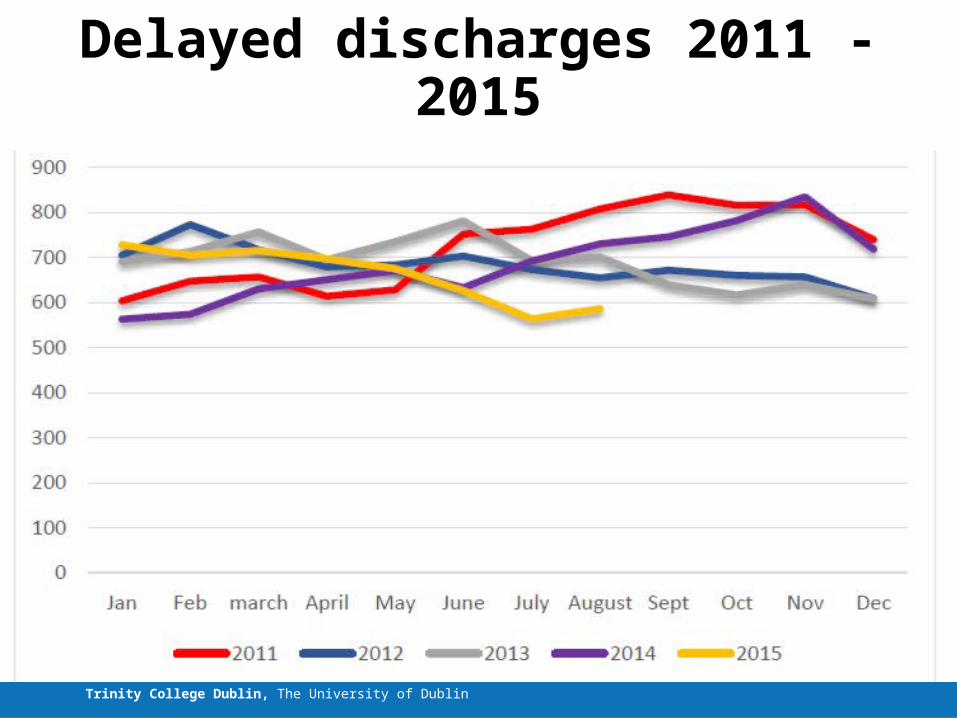
Delayed discharges 2011 - 2015
Trinity College Dublin, The University of Dublin
IMAGE
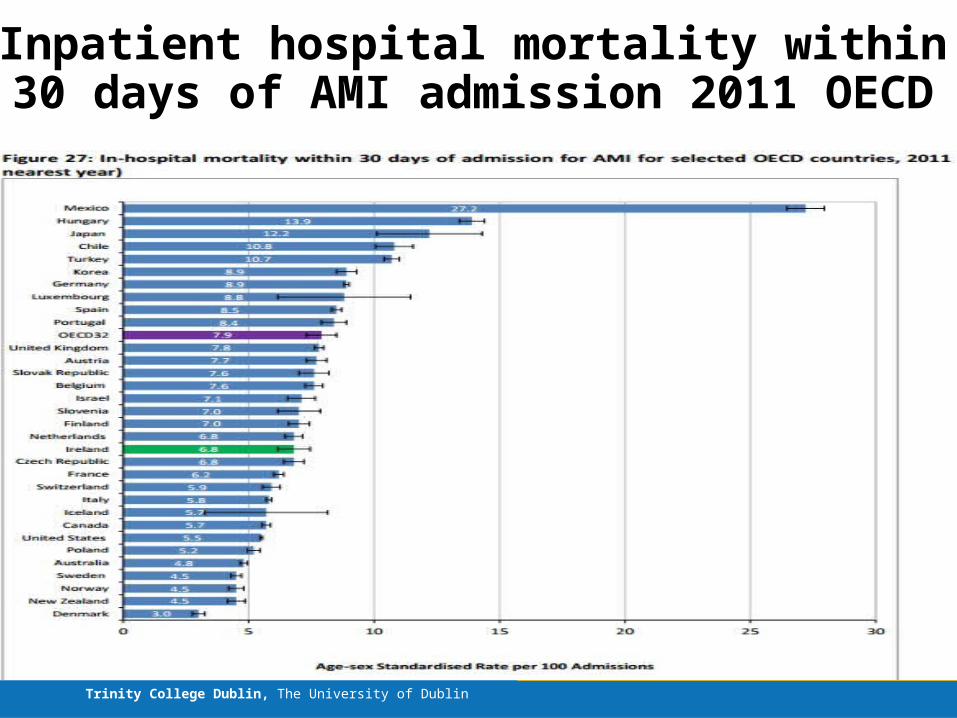
Inpatient hospital mortality within 30 days of AMI admission 2011 OECD
Trinity College Dublin, The University of Dublin
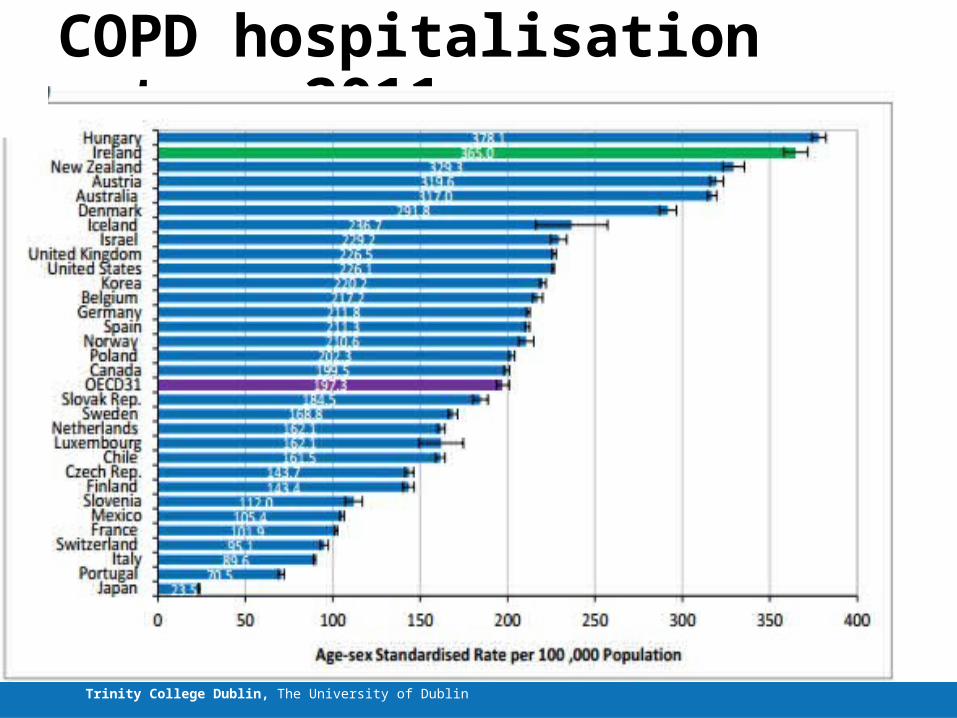
COPD hospitalisation rates, 2011

Indicators of Universal healthcare:Coverage
Trinity College Dublin, The University of Dublin
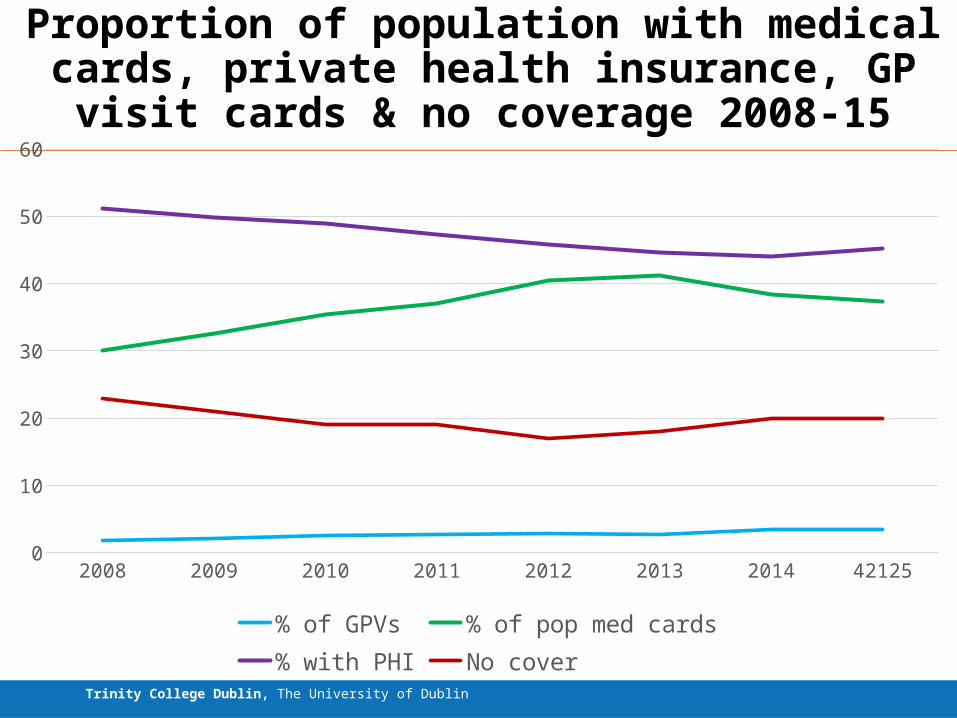
Proportion of population with medical cards, private health insurance, GP visit cards & no coverage 2008-15
2008 2009 2010 2011 2012 2013 2014 421250
10
20
30
40
50
60
% of GPVs % of pop med cards% with PHI No cover
Indicators of Universal healthcare:Resources
Trinity College Dublin, The University of Dublin
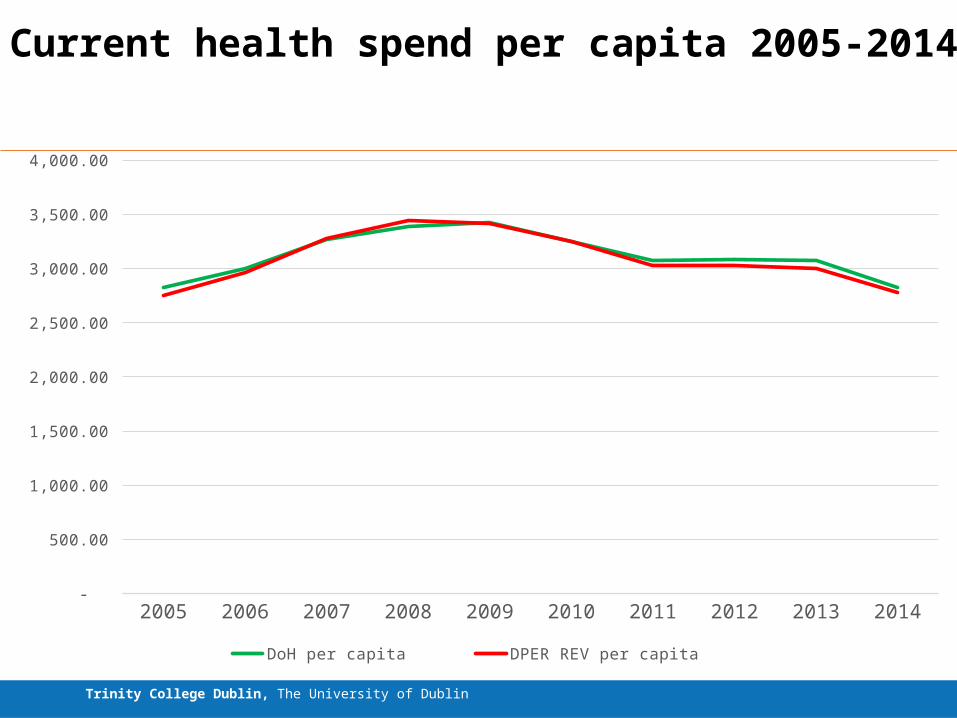
Current health spend per capita 2005-2014
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 -
500.00
1,000.00
1,500.00
2,000.00
2,500.00
3,000.00
3,500.00
4,000.00
DoH per capita DPER REV per capita
Trinity College Dublin, The University of Dublin
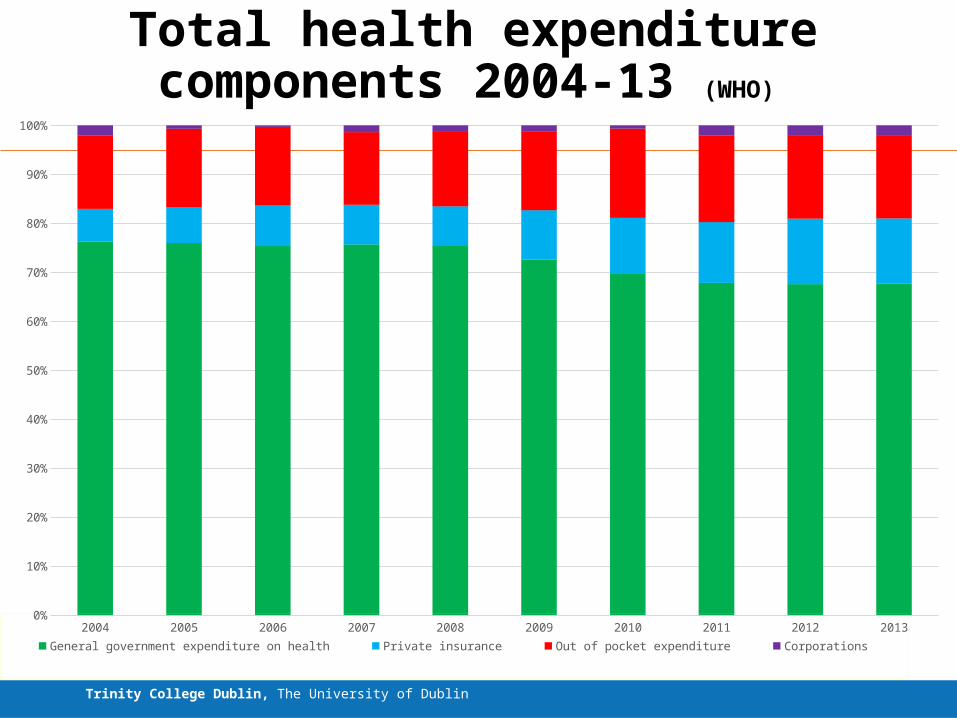
Total health expenditure components 2004-13 (WHO)
2004 2005 2006 2007 2008 2009 2010 2011 2012 20130%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
General government expenditure on health Private insurance Out of pocket expenditure Corporations
Indicators of Universal healthcare:Financial protection
Trinity College Dublin, The University of Dublin
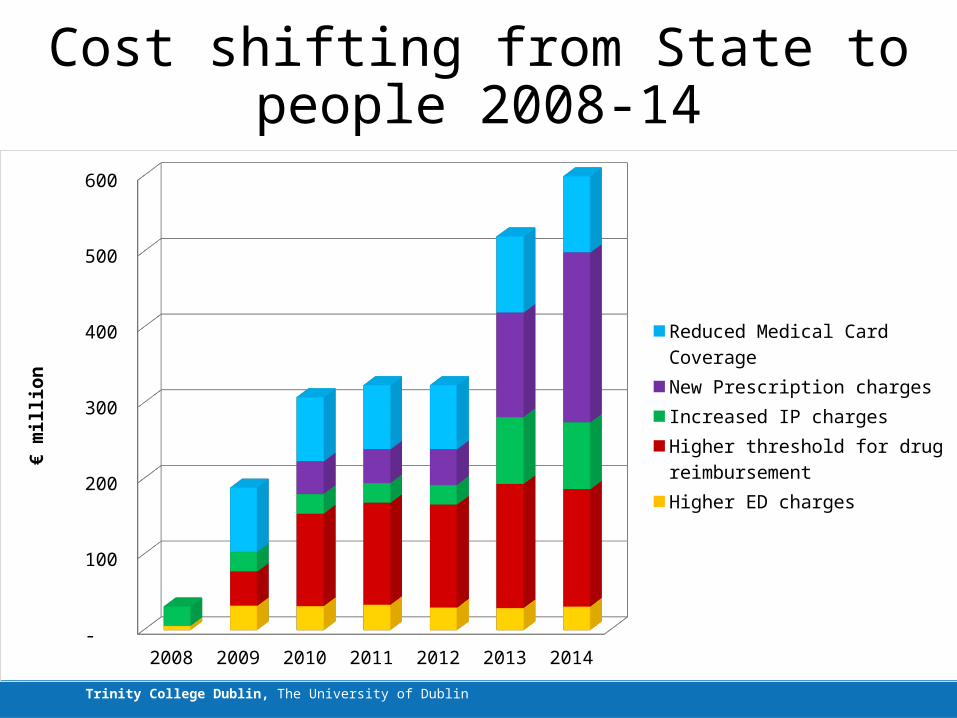
Cost shifting from State to people 2008-14
2008 2009 2010 2011 2012 2013 2014 -
100
200
300
400
500
600
Reduced Medical Card CoverageNew Prescription chargesIncreased IP chargesHigher threshold for drug re-imbursementHigher ED charges
€ m
illio
n
Trinity College Dublin, The University of Dublin
Indicators of universal healthcare in Ireland
– Full package• Complicated, have to pay for it, geography?
– Quality• Timely – Deteriorating access • Integrated – Difficult to measure• Appropriate, best practice, clinical: Pockets of
good practice, not mainstreamed, largely hospital based, hard to quantify progress
– Coverage for all• NOT UNIVERSAL
– Resources • Sufficiency (threshold) - Declining• Efficiency (Allocative, Technical – Right mix) –
Shift out of hospital - difficult to measure
– Financial protection • Free Care (at point of contact) – NOT• Affordable care (progressive, avoid
catastrophic payment and risk of impoverishment) – ???
Reflecting the five dimensions of UHC
Trinity College Dublin, The University of Dublin
Progress on universal healthcare?
– Little change in breadth of coverage except for Free GP Care
– No change in scope except increased waiting lists, getting worse?
– Decline in depth of coverage due to new & increasing charges (except for free GP care)
– More snakes than ladders
Thank you, any questions?





























