Embed Size (px)
Citation preview

INDICATIONS FOR HXMODIALYSIS IN ADVANCED UREMIC PROSTATIC OBSTRUCTION
By MILES Fox, Ch.M., F.R.C.S., and F. M. PARSONS, B.Sc., M.D., M.R.C.P.E. Renal Research Unit atzd Department of Urology, General Infirmary at Leeds
THE frequency of uramia complicating prostatic obstruction has decreased considerably in recent years, but it still presents a problem and demands attention. The most difficult patients to treat are those who do not regain sufficient renal function when adequate urinary drainage has been instituted. Weeks or even months may elapse before sufficient improvement occurs to allow safe prostatectomy (Badenoch, 1953 ; Edwards, 1956) and some patients succumb before adequate renal function has been regained (Rees, 1947). Wilson Hey (1949) recorded no recoveries when the blood urea exceeded 300 mg. per cent. on admission.
Malnutrition is often present, for uramia impairs appetite and may cause nausea and vomiting. This is difficult to counteract until the uramia has been corrected. The presence of an indwelling catheter in a uramic patient, who has a low resistance to infection, creates a further hazard. Tubular damage producing a “ salt-losing nephritis ” (Lapides, 1953 ; Parsons, 1954) is found frequently and requires careful electrolyte replacement until adequate renal tubular activity has returned.
It was decided to assess the value of hamodialysis in uramic patients when relief of obstruction was not followed by a rapid correction of the uramia. This report concerns the use of the artificial kidney in Leeds in the management of these patients during the past six years.
Materials and Methods-Hamodialysis was used pre-operatively in fifteen uramic subjects with bladder-neck obstruction during the six-year period, 1956-63. Five were referred from centres outside Leeds. Fourteen had prostatic obstruction from benign enlargement whilst the fifteenth, aged 24, had Marion’s disease of the bladder neck. No patient was refused treatment, even though the average age was 71 years. The blood urea levels on admission ranged between 100 and 627 mg. per cent., with a mean of 350 mg. per cent.
Initial investigation in the artificial kidney unit included urinalysis, blood urea, and electrolyte estimations, blood count, and X-ray examination of the chest and renal tract. Fluid and electrolyte imbalance when present was corrected by oral or intravenous therapy and closed bladder drainage was continued.
Hamodialysis was performed with a Kolff rotating drum machine (Parsons et al., 1961).
CLINICAL COURSE
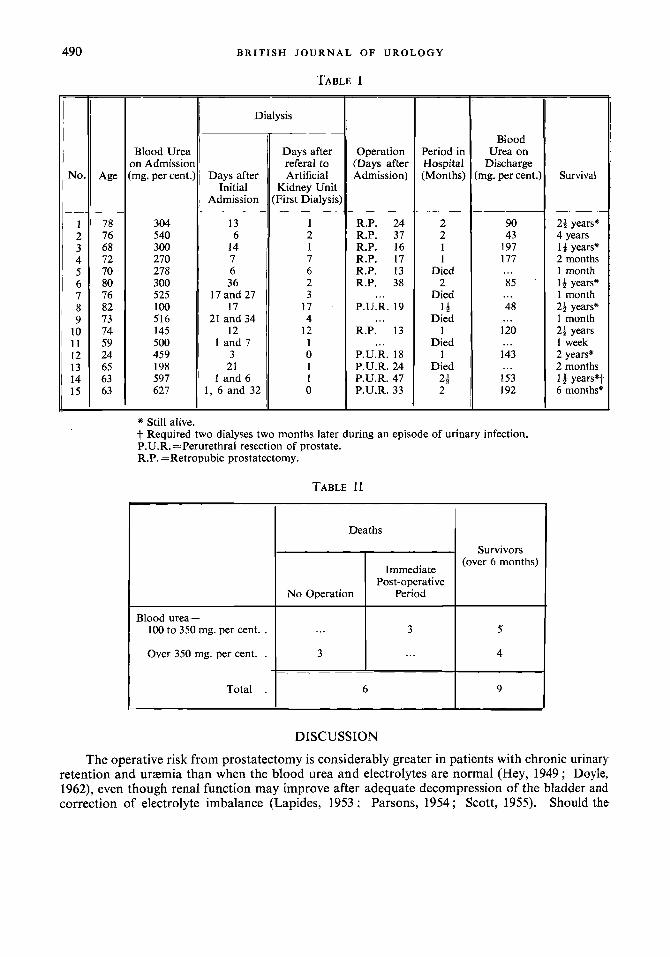
Table I summarises the course of the fifteen patients in chronological order. The patients could be divided into two main groups :-
1. Patients with gross uramia (blood urea> 350 mg. per cent.). 2. Patients with moderate uramia (blood urea 100 to 350 mg. per cent.).
1. Severe Uraemia (blood urea> 350 mg. per cent.)-Seven patients were referred with a blood urea in excess of 350 mg. per cent. Three died before operation could be carried out. The course of two is depicted in Figure 1 (Cases 7 and 9). In both, conservative management with fluid and electrolyte therapy and continuous urethral bladder drainage had been instituted from the day
487

488 BRITISH J O U R N A L OF UROLOGY
of admission. Case 7 was referred to the artificial kidney unit three weeks later as there was no improvement in the azotaemia and renal infection had supervened. Haemodialysis controlled the uraemia but the ascending urinary infection progressed and death occurred two weeks later. In Case 9 urinary infection developed even though there had been fairly rapid correction of the azotaemia. Following haemodialysis there was no improvement in the infection and death occurred one day after the second haemodialysis.
Four patients were treated successfully. Their blood ureas were 540, 459, 597, and 627 mg. per cent. These were our more recent cases in whom haemodialysis was carried out six, three, six, and two days respectively after admission to hospital and within eight hours after being referred to the artificial kidney unit. Figure 2 shows the course of three of the cases.
B.U.
400
200
0
400
200
0
CASE 7 B'u' DIALYSIS CASE 12
D\ALYSIS I DIALYSIS II t
600 mpIALYSIS I CASE 14
CASE 9
200
0 0 10 20 30 40 50 60
DAYS 10 20 30 40 50 60
DAYS FIG. 1 FIG. 2
Case 15 (aged 65 years) was semicomatose on admission. The bladder was distended to the umbilicus ; the prostate was small and soft. The blood urea was 627 mg. per cent., potassium 8.3 mEq./litre, the CO, combining power 7 3 mEq./litre, and the B.P. 130/65. There were signs of early basal pneumonia.
A urethral catheter was inserted. Immediate dialysis was carried out ; there were five urgent indications- semi-coma, pneumonia, severe azotaemia, acidosis, and hyperkalaemia. After four hours' haemodialysis, the serum potassium had fallen to 3 mEq./litre and the blood urea to 218 mg. per cent.
The following day the patient was fully conscious and demanded food. In spite of an adequate urine output the blood urea rose to 384 mg. per cent. over the next five days with some clinical deterioration. A second hiemodialysis reduced the blood urea to 92 mg. per cent. The patient was ambulant the next day and had an excellent appetite. The blood urea rose only slowly afterwards, even though a high protein diet (80 g. per day) was administered. He gained weight. Anabolic steroids were given (norethandrolone 30 mg. daily) and a urine output of over 3 litres was maintained. Renal loss of sodium was corrected by sodium chloride administration.
Thirty-one days following admission, a third haemodialysis was carried out and perurethral resection of the

INDICATIONS FOR HBMODIALYSIS IN ADVANCED UREMIC PROSTATIC OBSTRUCTION 489
prostate was performed two days afterwards. The patient was discharged from hospital one month later with a blood urea of 192 mg. per cent. He was ambulant, taking an interest in life and had a reasonable appetite. Six months later he was well.
Case 14 (aged 63 years).-The blood urea on admission was 597 mg. per cent. Two hzmodialyses were carried out, on the first and the sixth day. Haematemesis delayed a perurethral resection until the seventh week. He was discharged one month later with a blood urea of 130 mg. per cent. Two months later he was readmitted with a severe urinary tract infection and a blood urea of 504 mg. per cent. Two haemodialyses were performed and the infection responded to antibiotics. The blood urea settled to 170 mg. per cent. and he is alive and well eighteen months later,
Case 12 (aged 24 years).-The blood urea on admission was 459 mg. per cent. Hzmodialysis was carried out on the same day. This controlled the uraemia and renal function recovered rapidly. Perurethral resection (for 6.u.
nutritional state had been improved. He was discharged from hospital two weeks later with a blood urea of 140 mg. per cent. and he has remained well for over two years.
Marion’s disease) was delayed for two weeks until the ;;;L Dl ALY SIS CASE I
0 I
2. Moderate Uremia (blood urea 100 to 350
group. Four survived. The progress in three is 300 shown in Figure 3.
Case 1 (aged 78 years).-The blood urea was 304 mg. per cent. on admission. After five days’ bladder 0
mg. per cent.).-There were eight patients in this DIALYSIS CASE 3
d&ompression progress was halted and no further improve- ment of uraemia occurred during the following week. He 3oo DIALYSIS was referred for hzmodialysis and the blood urea was 1T.U.R.
CASE 8
reduced from 180 to 79 mg. per cent. Retropubic prosta- tectomy was carried out twelve days later. One year later he was well and the blood urea was 58 mg. per cent.
150
was the
- .
0 10 20 30 40 50 60
FIG. 3
Case 3 (aged 68 years).-The blood urea on admission 300 mg. per cent. Following bladder decompression ursemia did not regress satisfactorily and he was
Retropubic
DAYS
referred for haemodialysis two weeks later. prostatectomy was carried out two days afterwards. The patient was well two years after operation with a blood urea of 100 mg. per cent.
Case 8 (aged 82 years).-The blood urea was 100 mg. per cent. on admission. He was unco-operative and had a poor appetite. His general condition and ursemia did not improve after ten days’ bladder decompression. Hzmodialysis achieved a good clinical response and prostatectomy was performed safely two days later. After a post-operative rise, the blood urea level fell and has remained within normal limits for two and a half years.
Case 10 (aged 74 years).-The blood urea was 145 mg. per cent. on admission. Bladder drainage had been maintained for seven months, at first by urethral catheter and later by suprapubic cystostomy, with little effect o n his general condition and azotaemia. He was referred to the artificial kidney unit. After one hzmodialysis his general condition improved and prostatectomy was performed the following day. The post-operative period was uneventful and he was discharged from hospital two and a half weeks later. He lived for two and a half years with a blood urea in the region of 90 mg. per cent.
Results.-Results are shown in Tables I and 11. More than one dialysis was carried out in five patients and six deaths occurred. Three
patients never reached operation and three died in the immediate post-operative period. Uncontrollable urinary tract infection played a major part in the death of five of these patients. A further two have died from chronic renal failure two and a half and four years after operation. Seven are alive between six months and two years after treatment.
4 c
490
Blood urea- 100 to 350 mg. per cent. . Over 350 mg. per cent. .
Total .
BRITISH J O U R N A L O F U R O L O G Y
Deaths
Survivors (over 6 months)
Immediate Post-operative
No Operation Period
... 3 5
3 ... 4
6 9
TABLE I =
No.
- 1 2 3 4 5 6 7 8 9
10 11 12 13 14 15 -
78 76 68 72 70 80 76 82 73 74 59 24 65 63 63 -
Blood Urea )n Admissioi rng. per cent.
304 540 300 270 278 300 525 100 516 I45 500 459 198 597 627
Dialysis
Days after Initial
Admission
13 6
14 7 6 36
17 and 27 17
21 and 34 12
I and 7 3 21
1 and 6 1, 6 and 32
Days after referal to Artificial
Kidney Unit First Dialysis
1 2 1 7 6 2 3
17 4
12 1 0 1 I 0
Operation (Days after Admission)
R.P. 24 R.P. 37 R.P. 16 R.P. 17 R.P. 13 R.P. 38
P.U.R. 19
R.P. 13
P.U.R. 18 P.U.R. 24 P.U.R. 47 P.U.R. 33
...
...
...
Period in Hospital (Months)
2 2 I 1
Died 2
Died 1s
Died 1
Died 1
Died 2: 2
Blood Urea on
Discharge mg. per cent.)
90 43
197 177 ... 85 .
48
120
I43
153 I92
...
...
...
...
* Still alive. t Required two dialyses two months later during an episode of urinary infection. P.U.R. =Perurethral resection of prostate. R.P. =Retropubic prostatectomy.
TABLE I1
DISCUSSION
Survival
2: years" 4 years It years" 2 months 1 month 14 years" 1 month 23 years" 1 month 24 years 1 week 2 years' 2 months 14 years".t 6 months"
The operative risk from prostatectomy is considerably greater in patients with chronic urinary retention and uraemia than when the blood urea and electrolytes are normal (Hey, 1949 ; Doyle, 1962), even though renal function may improve after adequate decompression of the bladder and correction of electrolyte imbalance (Lapides, 1953 ; Parsons, 1954 ; Scott, 1955). Should the

INDICATIONS FOR HEMCDIALYSIS IN ADVANCED UREMIC PROSTATIC OBSTRUCTION 49 I
uraemia not be corrected rapidly, prolonged bladder drainage may be necessary and preliminary suprapubic cystostomy has been advised (Badenoch, 1953 ; Riches, 1954), and prostatectomy postponed until the patient’s condition improves. Suprapubic cystostomy carries a mortality in these ursemic subjects. Rolnick and Riskind (1937) reported 28.6 per cent. deaths after 598 cystostomies. Edwards (1956) had a 6 per cent. mortality, but only 69 per cent. of the survivors were ultimately able to undergo prostatectomy. Rees (1947) recorded a mortality of 28 per cent., most of the deaths being due to ascending renal infection.
Patients with chronic uraemia are unsuitable subjects for major operative procedures (Schreiner and Maher, 1963). They are undernourished, cerebration is often affected, wound healing is delayed (Stein and Wiersum, 1959), whilst anaemia and cardiac insufficiency allow little room for circulatory imbalances. Uramia impairs resistance to infection (Balch et al., 1955 ; Parsons and McCracken, 1959) and there is an increased risk of ascending urinary tract and systemic infection. Advanced uramia may cause an increase in protein catabolism thereby overloading an already diminished renal reserve (Parsons, 1960). The chances of improving the resilience of a uraemic subject without the help of dialysis within a reasonable time limit to allow a one-stage prostatectomy with safety are therefore greatly diminished.
Haemodialysis corrects most of the abnormalities encountered in chronic renal failure. Gastro- intestinal disturbances and abnormal cerebration are reversed within twenty-four to forty-eight hours, but improved resistance to infection and normal wound healing seem to be delayed until a positive nitrogen balance is achieved, which may take several weeks.
We have found that haemodialysis is tolerated well, even in the old age group, provided certain precautions are taken. Merrill (1952, 1957) reported that a rapid and drastic correction of an advanced uraemic state is inadvisable when an abnormal metabolic state has developed slowly over a period of months or years. This is particularly true when using a machine with a larger dialysing area (Parsons ef al., 1961). We have found that dialysis in advanced prostatic uraemia is safer and more effective if performed in two stages. In the first dialysis the blood urea level is reduced by about one half. A second and more complete dialysis is then carried out forty-eight to seventy-two hours later. Clinical improvement, as evidenced by a return to well- being, co-operation, and normal appetite is not necessarily related to a proportional improvement in the biochemical abnormalities (Merrill, 1952; Goldner el al., 1954). The more gradual correction of the biochemical abnormalities tends to guard against the development of convulsions during the haemodialysis. Should convulsions occur they can usually be controlled by the administration of 500 ml. of 62.5 per cent. laevulose (Kennedy et al., 1963), although it may be necessary to antesthetise the patient with thiopentone (Parsons et al., 1963).
As soon as the uramic symptoms are controlled by dialysis the patient should be mobilised. During this phase it is essential to correct malnutrition. Preliminary observations (Kenward et al., 1964) suggest that to achieve a positive nitrogen balance a minimum of 40 g. of protein and a total calorie intake of 2,500 must be given daily.
Careful attention to fluid and electrolyte balance is required pre-operatively and post- operatively. As the majority of these patients have a salt-losing renal lesion, correct sodium supplementation, according to the degree of renal loss, is most essential for not only does sodium depletion lower glomerular filtration rate (Nickel e l al., 1953) but it also increases protein catabolism (McCance, 1936 a, b).
Haemodialysis ensures a rapid control of the ursemic manifestations and allows the use of a one-stage prostatectomy to be performed not only earlier but also more safely. Unfortunately many of the patients in this series were referred very late and the prolonged use of an indwelling catheter in a uraemic subject resulted in a high mortality from ascending renal infection.
Indications for Dialysis.-In patients with uraemia from chronic prostatic obstruction we
1. Uramic Symptoms.-All patients with uraemic symptoms, regardless of the degree of advocate haemodialysis much earlier and more frequently in the presence of :-

492 B R I T I S H J O U R N A L OF U R O L O G Y
azotaemia, should have an immediate dialysis. Such symptoms would include lethargy, nausea, vomiting, and unco-operation.
If the blood urea “does not fall following catheterisation more than 50 mg. per cent. in the first twenty-four to forty-eight hours, dialysis should be performed forthwith.
3. Persistent Moderate Uramia.-A persistently elevated blood urea, say in the region of 150 mg. per cent., is not a contraindication to operation. As prostatectomy may cause an accelerated rate of protein catabolism (Merrill, 1952 ; Doyle et al., 1959), the diminished renal reserve may be further overloaded and a dangerous uraemic state may supervene. A pre-operative dialysis anticipating the possibility of these sequelae is to be preferred to a post-operative dialysis.
4. Infection.-Infection either in the urinary tract or elsewhere is the commonest cause of morbidity and mortality. It also increases protein breakdown which may overload already damaged kidneys. As the resistance to infection is decreased in uraemia we advocate using haemodialysis to keep the blood urea below 150 mg. per cent.
2. Advanced Uramia.-Blood urea<300 mg. per cent. on admission.
SUMMARY
Fifteen patients with severe uraemia from chronic prostatic obstruction have been treated .by liamodialysis pre-operatively. The value of dialysis in these subjects is discussed. Not only was dialysis a life-saving measure in some cases, it also allowed operation to be carried out safely in patients who would otherwise have been poor surgical risks. Moreover, one-stage prosta- tectomy was possible in all cases and the stay in hospital was shortened.
We should like to thank Professor L. N. Pyrah and Mr F. P. Raper for helpful advice and for allowing us to publish the case histories of those patients admitted under their care.
REFERENCES
BADENOCH, A. W. (1953). “ Manual of Urology.” (London : Wm. Heinemann.) BALCH, H. H., MERONE, W. H., and SAKO, Y. (1955). Surg. Gynee. Obstet., 100,439. DOYLE, J. E. (1962).
DOYLE, J. E., ANTHONE, R., ANTHONE, S., and MACNEILL, A. E. (1959). N.Y. Sf. J. Med., 59,4149. EDWARDS, P. D. (1956). Brit. J. Urol., 19, 83. GOLDNER, F., jun., GORDON, G. L., and DANZIG, L. E. (1954). Arch. intern. Med., 93, 61. HEY, W. H. (1949). Proc. Roy. SOC. Med., 42, 987. KENNEDY, A. C., LINTON, A. L., LUKE, R. G., and RENFREW, S. (1963). Lancet, 1,408. KENWARD, D. H., YOUNG, G. A., and PARSONS, F. M. (1964). Personal communication. LAPIDES, J. (1953). J . Urol., 70, 74. MCCANCE, R. A. (1936 a). Proc. roy. SOC. B., 119, 245. __ (1936 b). Lancet, 1, 823. MERRILL, J. P. (1952). New Engl. J. Med., 246, 17. - (1957). J. chon. Dis., 5 , 138. NICKEL, J. F., LOWRANCE, P. B., LEIFER, E., and BRADLEY, S. E. (1953). J. clin. Invest., 32, 68. PARSONS, F. M. (1954). Brit. J . Urol., 26, 7. - (1960). In ‘‘ Modern Trends in Urology.” Ed. Sir Eric Riches. (London : Butterworth.) PARSONS, F. M., BLAGG, C. R., and WILLIAMS, R. E. (1963). Biochemical Clinics, No. 2, “The
PARSONS, F. M., HOBSON, S. M., BLAGG, C. R., and MCCRACKEN, B. H. (1961). Lancet, 1 , 129. PARSONS, F. M., and MCCRACKEN, B. H. (1959). Brit. med. J . , 1 , 740. REES, W. S. (1947). Brit. J. Urol., 19, 83. RICHES, E. W. (1954). Ann. Roy. Coll. Surg. Engl., 15, 120. ROLNICK, H. C., and RISKIND, L. A. (1937). J. Urol., 37, 12. SCHREINER, G. E., and MAHER, J. F. (1963). Amer. J. Cardiol., 12, 317. Scorn, W. W. (1955). Editor’s note on Management of Enlarged Prostate, “ Year Book of Urology,”
1954-55, p. 240. (Chicago : Year Book Publishers.) STEIN, A. A., and WIERSUM, J. (1959). J. Urol., 82, 271.
“ Extracorporeal Hiemodialysis Therapy in Blood Chemistry Disorders.” (Springfield, Illinois : C. C. Thomas.)
Kidney,” p. 457.