Embed Size (px)
Citation preview
Independent risk factors associated with Candida auris candidaemia in
South Africa – an analysis of national surveillance data, 2016-2017
E van Schalkwyk1, L Shuping1, H Ismail1, J Thomas1 and NP Govender1,2
1. Centre for Healthcare-Associated Infections, Antimicrobial Resistance and Mycoses, National Institute for Communicable Diseases
2. Faculty of Health Sciences, University of the Witwatersrand, Johannesburg

Candida is a common cause of healthcare-associated infections
• #1 pathogen implicated in bloodstream infections in the US (22%)
• Candidaemia associated with high in-hospital mortality, prolonged hospitalisation and increased healthcare costs
Magill SS, et al. N Engl J Med, 2014

Known patient risk factors for candidaemia
• Underlying co-morbidities
• Immunosuppression e.g. neutropaenia
• Prior or prolonged broad-spectrum antibiotic use
• Medical interventions
– Surgery
– Parenteral nutrition
– Invasive medical devices
• ICU admission

What we are yet to learn about C. auris
Environment MicrobeThe infectious disease triad
Human host

Host
• Which host factors predispose patients to develop C. auris invasive infections?
• Are these host factors different from patients with other invasive infections and/or other Candidaspecies?

Case reports and case series from 16 countries
• Most common underlying conditions and predisposing factors*:• Diabetes mellitus
• Chronic renal disease
• Peripheral vascular disease
• Prior healthcare exposure
• Broad-spectrum antibiotics
• Surgery (esp. abdominal surgery)
• CVC
• TPN
• ICU care
• Urinary catheterization
• Mechanical ventilation*Arauz et al. Mycoses 2017, Lockhart et al. CID 2017, Tsay et al. MMWR 2017, Schwartz et al. CCDR 2017, Ben-Ami et al. EID 2017, Morales-Lopez et al. EID 2017, Vallabhaneni et al. MMWR 2016, Chowdhary et al. EID 2013, Chowdhary et al. Eur J Clin Microbiol Infect Dis 2013, Kim et al. CID 2009
• 27 ICUs across India
• 1161 patients
• April 2011 to Sept 2012
• Risk factors for C. auris candidaemia v. non-C. auris species• Prior antifungal exposure (OR: 2.8; 95% CI: 1.64-4.86)
• Vascular surgery
• Underlying respiratory illness
• Admission to North-Indian ICUs
• Admission to public-sector hospitals
• Urinary catheter in-situ
• Low APACHE II score
Rudramurthy et al. J Antimicrob Chemother 2017

Aim and objectives
Aim: To advise on appropriate changes to diagnostic, clinical management and infection prevention and control algorithms and to inform future study design
Objective of this analysis:
To determine risk factors for candidaemia caused by C. auris versus other Candida species

Methods
• Active national laboratory-based surveillance for candidaemia (GERMS-SA) – Public- and private-sector facilities
– Across SA
• Jan 2016 – Sept 2017
• Clinical and demographic data collected on a subset of cases at enhanced surveillance sites– 22 public-sector sites
– 3 private-sector sites (one private hospital group)

GERMS-SA candidaemia surveillance
• Case definition:
• Any patient
• Blood culture yielding Candida species at an NHLS or private-sector diagnostic laboratory
• Multiple isolates cultured within 30 days of the first positive specimen included within a single case
• For C. auris: any isolate referred to NICD (incl. Candida haemulonii, Saccharomyces cerevisiae, Rhodotorula glutinis etc.) and confirmed as C. auris

• Cases classified according to final confirmed ID at NICD
– C. auris candidaemia
– Non-C. auris candidaemia =
• Candida albicans
• Candida parapsilosis
• Candida glabrata
• other Candida species
• Statistical analysis
– Descriptive analysis of possible risk factors
– Multivariable logistic regression model

Results
• 21 cases had candidaemia caused by C. auris and another Candida species concurrently (mostly C. parapsilosis, n=16)
2414 cases of candidaemia
Non-C. aurisn=2151 (89%)
C. aurisn=262 (11%)
C. auris with clinical data
n=52
Non-C. auriswith clinical data
n=857

At least one case of C. auris candidaemia was diagnosed at 9 public-sector and 43 private-
sector hospitals
Public-sector hospitals
Private-sector hospitals

Public-sector hospitals
Private-sector hospitals
First neonatal C. auris cases identified in August 2017 (incl. 2 clusters at one public-sector and one private-
sector facility)

Demographic characteristics of cases (n=2414)
Patient characteristics, n/N (%)C. auris candidaemia
(N=262)Non-C. auris candidaemia
(N=2152)
Age in years, median (IQR) 53 (34-65) 28 (0-57)
Male 163/260 (63) 1135/2109 (54)
Province
Gauteng 245/260 (94.2) 1314/2139 (61.4)
Mpumalanga 7/260 (2.7) 40/2139 (1.9)
Limpopo 2/260 (0.8) 37/2139 (1.7)
Western Cape 2/260 (0.8) 264/2139 (12.3)
Kwa Zulu Natal 3/260 (1.2) 212/2139 (9.9)
Free State 1/260 (0.4) 141/2139 (6.6)
Eastern Cape 0/260 (0) 79/2139 (3.7)
Northern Cape 0/260 (0) 22/2139 (12.3)
North West 0/260 (0) 30/2139 (1.4)
Healthcare sector
Private 198/262 (75.6) 792/2152 (36.8)
Public 64/262 (24.4) 1360/2152 (63.2)
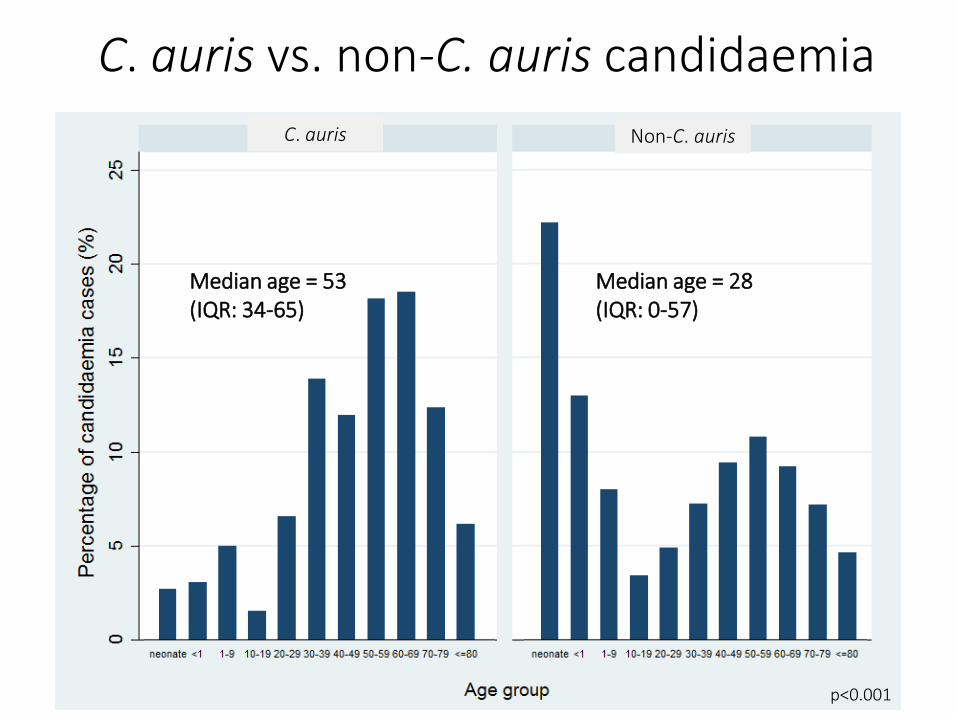
C. auris vs. non-C. auris candidaemia
Non-C. aurisC. auris
Median age = 28 (IQR: 0-57)
Median age = 53 (IQR: 34-65)
p<0.001

C. auris vs. non-C. auris candidaemia
Patient characteristics, n/N (%)C. auris
n=52Non-C. auris
n=857C. albicans
n=307C. parapsilosis
n=320C. glabrata
n=122
Length of stay to first positive blood culture in days, median (IQR)
28 (15-42) 12 (5-23) 10 (4-20) 17 (9-30) 5 (1-15)
Prior hospital admission 28/47 (60) 535/812 (66) 185/288 (64) 195/305 (64) 78/116 (67)
ICU admission 36/47 (77) 524/790 (66) 176/283 (62) 232/296 (78) 68/112 (61)
Mechanical ventilation 24/42 (57) 238/753 (32) 77/261 (30) 97/277 (35) 41/113 (36)
Central venous catheter 31/43 (72) 383/761 (50) 122/264 (46) 157/283 (55) 60/113 (53)
Prior systemic antimicrobialtherapy
36/43 (84) 479/755 (63) 156/260 (60) 200/283 (71) 66/112 (59)
Prior antifungal therapy 12/43 (28) 96/758 (13) 17/261 (7) 61/281 (22) 6/114 (5)
Crude in-hospital mortality 23/49 (47) 347/827 (42) 142/295 (48) 107/308 (35) 54/119 (45)
Independent risk factors for C. auriscandidaemia
• Admission to a private-sector facility increased the odds four-fold (aOR 4.1; 95% CI 1.8-8.7)
• Increased age (aOR 1.01 for every year; 95%CI: 1.01-1.03)
• Increased length of hospital stay before first positive blood culture (aOR 1.01 for every day admitted; 95% CI: 1.01-1.03).
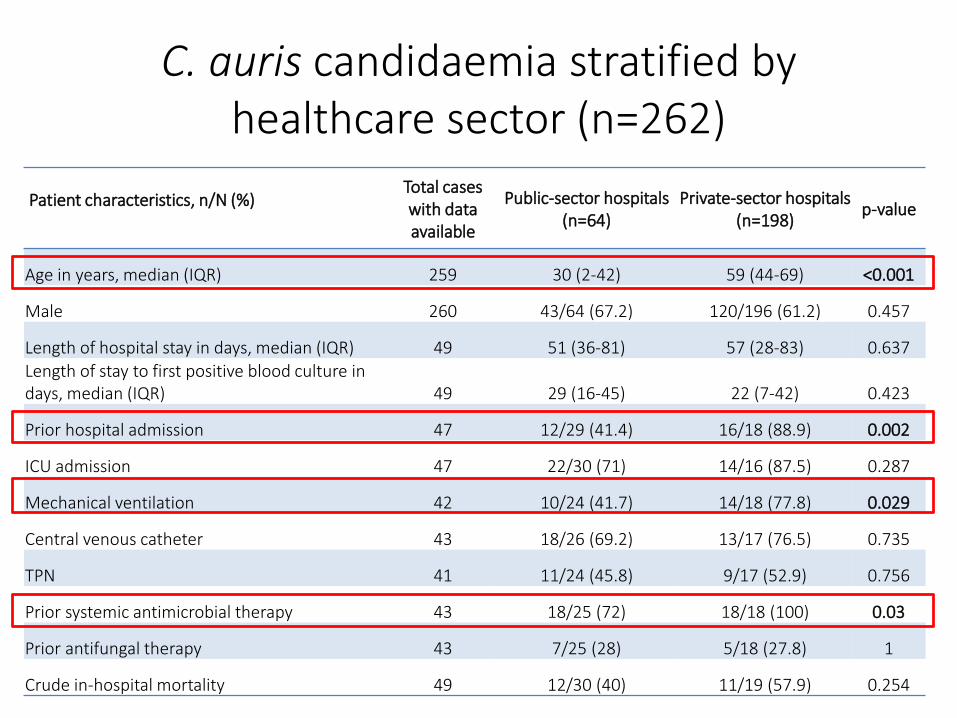
C. auris candidaemia stratified by healthcare sector (n=262)
Patient characteristics, n/N (%)Total cases with data available
Public-sector hospitals (n=64)
Private-sector hospitals (n=198)
p-value
Age in years, median (IQR) 259 30 (2-42) 59 (44-69) <0.001
Male 260 43/64 (67.2) 120/196 (61.2) 0.457
Length of hospital stay in days, median (IQR) 49 51 (36-81) 57 (28-83) 0.637Length of stay to first positive blood culture in days, median (IQR) 49 29 (16-45) 22 (7-42) 0.423
Prior hospital admission 47 12/29 (41.4) 16/18 (88.9) 0.002
ICU admission 47 22/30 (71) 14/16 (87.5) 0.287
Mechanical ventilation 42 10/24 (41.7) 14/18 (77.8) 0.029
Central venous catheter 43 18/26 (69.2) 13/17 (76.5) 0.735
TPN 41 11/24 (45.8) 9/17 (52.9) 0.756
Prior systemic antimicrobial therapy 43 18/25 (72) 18/18 (100) 0.03
Prior antifungal therapy 43 7/25 (28) 5/18 (27.8) 1
Crude in-hospital mortality 49 12/30 (40) 11/19 (57.9) 0.254

Discussion
• Patients with C. auris candidaemia have similar risk factors to patients with non-C. auriscandidaemia but more likely to:
– Be admitted to private facilities
– Be older
– Spend a longer time in hospital before developing candidaemia

• Inherent differences between private- and public-sector facilities– Differences in patient populations - older patients?
– More patients mechanically ventilated?
– Differences in prior antimicrobial exposure?
– Differences in prior healthcare exposure?
– Differences in IPC practices?
• Longer hospital stay might be a proxy for prolonged exposure to the healthcare environment and/or prolonged colonisation before infection

Limitations
• Risk factor analysis limited to secondary data
– Unable to assess duration of exposure to risk factors, e.g. TPN
– Unable to assess type of prior antimicrobial exposure
• Appropriate comparison group - non-C. auriscases
– Perhaps rather use patients with other types of BSI or non-BSI patients?

Conclusion
• 3 independent risk factors for C. auris vs. non-C. auris candidaemia identified – however, further characterisation is needed
• At-risk patients should be carefully managed with regards to existing co-morbidities
• Duration of hospital admission should be minimised as far as possible
• South African consensus recommendations are being drafted

Acknowledgements• NICD
– Mycology team, CHARM– GERMS-SA team
• GERMS-SA enhanced surveillance sites, incl. Netcare hospital group
Thank you to all participating patients,
laboratory, clinical and administrative staff
for submitting case reports and isolates
NICD Centre staff:CED: Bolele Disenyeng, Elias Khomane, Emily Dloboyi, Jack Kekana, MandileThobela, Mimmy Ngomane, MunyadziwaMuvhali, Mzikazi Dickmolo, Nomsa Tau, Portia Mogale, Shannon Smouse, ThinaDuze, Tshegofatso Ntshabela,VishaniLukmanCOTHI: Ernest Tsotetsi, Boniwe Makwakwa, Crystal Viljoen, Gloria Molaba, Mbali Dube, Mabatho Mhlanga, Mpho Thankjekwayo, Naseema Bulbulia, Rosah Kganakga, Rubeina Badat, Ruth Mohlabeng, Serisha Naicker, Thokozile Zulu, Tsidiso Maphanga, Sydney Mogokotleng.CRDM: Dineo Mogale, Fahima Moosa, Happy Skosana, Karistha Ganesh, Kedibone Ndlangisa,, Maimuna Carrim, Malefu Moleleke, Mignon du Plessis, Nicole Wolter, Noluthando Duma, Olga Hattingh, Prabha Naidoo, Thabo Mohale, Judith Tshabalala, Thembi Mthembu.CTB: Cecilia de Abreu, Danny Lathane, Halima Said, George Ngconjana, LavaniaJoseph, Linsay Blows, Lwazi Danisa, Minty van der Meulen, Ronny Kaapu, Trisha Munsamy, Shaheed Vally Omar, ThabisileGwala, Tracy Arendse, Vancy Letsoalo, Yasmin Gardee, Zacharia Mabena, ZahedaBhyatCEZD: Chantel le Roux, Venessa Patharoo, Naazneen Moolla , Sindi Virasamy, Natasha Trataris-Rebisz, Malodi SethediDPHSR: Emily Sikanyika, Tsakane Nkuna, Yoliswa Bacela
GERMS-SA: John Black, Vanessa Pearce (EC); Anwar Hoosen, Vicky Kleinhans (FS); Alan Karstaedt, Caroline Maluleka, Charl Verwey, CharlesFeldman, David Moore, Gary Reubenson, Khine Swe Swe Han, Jeannette Wadula, Jeremy Nel, Kathy Lindeque, Maphoshane Nchabeleng, NazleeSamodien, Nicolette du Plessis, Norma Bosman, Ranmini Kularatne, Sharona Seetharam, Teena Thomas, Theunis Avenant, Trusha Nana,Vindana Chibabhai (GA); Adhil Maharj, Asmeeta Burra, Fathima Naby, Halima Dawood, Jade Mogamberry, Koleka Mlisana, Lisha Sookan,Praksha Ramjathan, Prasha Mahabeer, Romola Naidoo, Sumayya Haffejee, Yacoob Coovadia (KZN); Ken Hamese, Ngoaka Sibiya, RuthLekalakala (LP); Greta Hoyland, Jacob Lebudi (MP); Pieter Jooste (NC); Ebrahim Variava, Erna du Plessis (NW); Andrew Whitelaw, KessendriReddy, Mark Nicol, Preneshni Naicker (WC); Adrian Brink, Elizabeth Prentice, Inge Zietsman, Maria Botha, Peter Smith, Xoliswa Poswa(AMPATH); Chetna Govind, Keshree Pillay, Suzy Budavari (LANCET); Carel Haumann, Catherine Samuel, Marthinus Senekal (PathCare); AndriesDreyer, Khatija Ahmed, Louis Marcus, Warren Lowman (Vermaak and Vennote); Angeliki Messina, Dena van den Bergh, Karin Swart (Netcare);Cynthia Whitney (CDC); Keith Klugman (Emory); Ananta Nanoo, Andries Dreyer, Anne von Gottberg, Anthony Smith, Arvinda Sooka, CeciliaMiller, Charlotte Sriruttan, Cheryl Cohen, Chikwe Ihekweazu, Claire von Mollendorf, Desiree du Plessis, Erika Britz, Frans Radebe, GenevieNtshoe, Gillian Hunt, Hlengain Mathema, Jacqueline Weyer, Jenny Rossouw, John Frean, Karen Keddy, Kerrigan McCarthy, Linda de Gouveia,Linda Erasmus, Lucille Blumberg, Marshagne Smith, Martha Makgoba, Motshabi Modise, Nazir Ismail, Nelesh Govender, Neo Legare, NicolaPage, Ntsieni Ramalwa, Nuraan Paulse, Phumeza Vazi, Olga Perovic, Penny Crowther-Gibson, Portia Mutevedzi, Riyadh Manesen, RuthMpembe, Sarona Lengana, Shabir Madhi, Sibongile Walaza, Sonwabo Lindani, Sunnieboy Njikho, Susan Meiring, Thejane Motladiile, TiisetsoLebaka, Vanessa Quan, Verushka Chetty (NICD).
Provincial surveillance teams: Badikazi Matiwana, Bongiwe Cetywayo, Noluthando Mveni, Sandisiwe Joyi, Ntombizanele Dyonase, Zukiswa Langeni, (EC); Khasiane Mawasha, Thandeka Kosana (FS); Anna Motsi, Dikeledi Leshaba, Fiona Timber, Hazel Mzolo, John Mothlasi, Molly Morapeli, Nthabiseng Motati, Ophtia Kaoho, Phindile Ngema, Rachel Nare, Thandi Mdima, Thami Ntuli, VenesaKok, Vusi Ndlovu, Zodwa Kgaphola (GA) Beverly Hewitt, Elana Pavkovich, Roshanara Saloojee (Netcare GA); Indran Naidoo, Nelisiwe Buthelezi, Nkosinathi Mbhele, Nokuthula Nzuza, NompumeleoShezi, Thobeka Simelani, (KZN); Tebogo Modiba (LP); Ennica Ntlemo, Kgashane Rapaledi, Lesley Ingle, Nqobile Ntshali, Tumelo Thlomelang, Sanelisiwe Mtetwa (MP); Matsheko Siyaka (NC); Bekiwe Ncwana, Busisiwe Zungu, Joyce Tsotsotso, Louisa Phalatse, Myra Motemi, Sessing Tsebane, Sibongile Rasmeni-Quariva (NW); Cheryl Mentor, Elizabeth Jerome, Katherine Bishop, Nazila Shalabi, Priscilla Mouton, (WC).
NICD GERMS-SA Annual Surveillance Review, 27 October 2015





























