Embed Size (px)
Citation preview

Independent Hospital Pricing Authority
Emergency care costing and classification
project
Costing methodology

Revision history
Version Date Modifications
0.1 15 June 2015 Initial draft
0.2 5 August 2015 Revisions following review by consortium members
0.3 13 August 2015 Revisions following review by IHPA
0.4 16 November 2015 Revisions following consultation.
0.5 27 January 2016 Revisions to align with update of data request specification.
0.6 14 March 2016 Minor edits, and modification of tables at Appendix C to match
Data request specification document.
1.0 4 April 2016 Version officially released for the study.
Health Policy Analysis consortium
The Emergency care costing and classification project is being undertaken by a consortium
led by Health Policy Analysis Pty Ltd. The consortium includes:
Health Policy Analysis Pty Ltd (Jim Pearse - Project Director, Deniza Mazevska - Project
Manager, Joel Tuccia, Akira Hachigo, Jane Elkington)
HealthConsult Pty Ltd (Joe Scuteri, Lisa Fodero, Cathy Hoadley)
Health Outcomes International Pty Ltd (Lilian Lazarevic, Darren Button)
Dr Sharon Wilcox (Health Policy Solutions Pty Ltd)
Dr Tim Smyth (timsmythconsulting Pty Ltd)
Dr Ralph Hanson
Professor Peter Sprivulis
Dr Sue Ieraci.
Suggested citation
Health Policy Analysis 2016, Emergency care costing and classification project – Costing
methodology, Independent Hospital Pricing Authority, Sydney.
Disclaimer
In accordance with Health Policy Analysis’ policy, we are obliged to advise that neither
Health Policy Analysis nor any employee nor sub-contractor undertakes responsibility in any
way whatsoever to any person or organisation (other than the Independent Hospital Pricing
Authority) in respect of information set out in this report, including any errors or omissions
therein, arising through negligence or otherwise however caused.
Health Policy Analysis Pty Ltd
Suite 102, 30 Atchison Street, St Leonards 2065
ABN: 54 105 830 920
Phone: +61 2 8065 6491

Table of contents 1 Introduction and purpose of this document ............................................................................. 1
Introduction .............................................................................................................................. 1
Purpose of this document ....................................................................................................... 2
2 Key features of the study ............................................................................................................. 3
Overview ................................................................................................................................... 3
Costing study scope ................................................................................................................ 6
Data collection components ................................................................................................. 6
Costing components of study ................................................................................................ 8
Study stages ............................................................................................................................ 10
3 Overview of methodology ......................................................................................................... 12
Local costing .......................................................................................................................... 12
Allocation of direct costs ...................................................................................................... 13
Final product categories ....................................................................................................... 17
4 Detailed description of each costing step .............................................................................. 20
Step 1: Final allocation statistics ........................................................................................... 20
Step 2: Alignment of costs to all product categories ........................................................ 23
Step 3: Overhead allocation ................................................................................................ 26
Step 4: Allocation to product categories ........................................................................... 26
Step 5: Allocation of costs to patients ................................................................................. 27
Step 6: Intermediate costs (pathology, imaging and pharmacy) .................................. 29
5 Reporting cost results and related data .................................................................................. 30
Appendix A – Approaches to developing RVUs ............................................................................. 31
A: Total clinician time method ............................................................................................. 31
B: Standard cost method ...................................................................................................... 37
Appendix B – Description of data submissions ................................................................................ 44
Appendix C – Cost data submissions – data elements .................................................................. 46
References ........................................................................................................................................... 48

Emergency care costing and classification project – Costing methodology Page 1
1 1 Introduction and purpose
of this document Introduction
The Independent Hospital Pricing Authority (IHPA) engaged Health Policy Analysis, as the
lead for a consortium, to develop a new classification system for emergency care services for
Australia, for the purposes of activity based funding. The project is referred to as the
Emergency care costing and classification project.
The objectives of the project are to:
1. Undertake a targeted costing study to further investigate the impact of particular
drivers in emergency department stay cost variation and thereby aid in the
development of a new emergency care classification system.
2. Develop a new classification system for emergency care services for activity based
funding purposes, based on a structure agreed by IHPA.
3. Undertake data development work to modify and enhance selected data items in
the emergency care data collections to support the implementation of a new
emergency care classification system.
The costing component of the study involves costing by a sample of emergency
departments and emergency services across Australia, and will be conducted between April
and June 2016. This component is referred to throughout this document as the Emergency
care costing study.
This document, the Costing methodology, is part of a suite of documents developed for the
study. Other documents in the suite are:
Sampling strategy, which provides an analysis of data already available from
previous round of the National Hospital Cost Data Collection and also sets out the
sampling strategy for the study.
Data request specification (DRS), which sets out the data to be provided by
participating sites and the timeframes around which these data are to be provided.
Site implementation plan, which provides guidance to participating sites on planning
for and implementing the study.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 2
Purpose of this document
This document provides guidance for hospitals participating in the costing component of the
Emergency care costing and classification study on the methods for costing activity in scope
of the study. The document:
Describes the key features of the study.
Provides an overview of the costing process for the study.
Summarises key dates related to the costing component of the study.
Provides guidance on the key steps in the costing process, namely:
Step1: Development of final allocation statistics for clinical staff and other resource
categories based on data on clinician time allocated to individual patients and/ or in
undertaking specific activities/ procedures over a two-week period.
Step 2: Assignment of cost centres in the general ledger to appropriate final cost
centre types (reflecting product categories wherever possible, including the specific
emergency care product categories) and indirect (overhead) cost centre types.
Mapping of cost line items to National Hospital Cost Data Collection line items.
Step 3: Allocation of costs from indirect (overhead) cost centres to direct cost
centres.
Step 4: Allocation of costs accumulated in final cost centres to product categories.
Step 5: Allocation of costs to patients within product categories.
Describes the cost data to be submitted for the study.
Emergency care costing and classification project – Costing methodology Page 3
2 2 Key features of the study
Overview
The primary objective of the Emergency care costing study is to achieve accurate patient
level costs that can be used to develop a classification system for emergency care for
funding purposes. To achieve this, the costing study has been designed with the following
key features:
● The study will include a representative sample of emergency departments and
emergency services from across Australia (i.e. including metropolitan, regional and
remote locations alongside other strata). The final data set will be weighted to reflect
the population of emergency departments and emergency services across Australia.
The data set will provide a means of exploring the cost differences for emergency
departments in metropolitan, regional and remote locations, and potentially
differences between emergency departments and emergency services, depending
on the number of emergency services participating.
● To explore the boundary between emergency care and admitted patient care, the
scope of the study includes the emergency care component of admitted hospital
episodes, plus the cost of any short stay units directly managed by or integrated with
the emergency department. Costs of other components of admitted patient care will
also be explored through data supplied to the National Hospital Cost Data
Collection.
● Hospitals participating in the study are required to comply with the Australian Hospital
Patient Costing Standards Version 3.1 (Independent Hospital Pricing Authority, 2014).
● Costs yielded by the study are required to be based on direct measures of resource
consumption from within the study rather than external reference information.
● A particular focus in the study is on good measures of resource consumption for:
o clinical staff inputs to care
o consumables used within the emergency department
o imaging ordered within the emergency department
o pathology ordered within the emergency department
o pharmacy ordered within the emergency department.
The levels of consultation and liaison services provided by staff from outside the
emergency department will be identified, and associated resources estimated and
assigned to a separate product.
● The study will be run over a minimum of one month within each participating site.
Patient characteristics and stay information identified as being important for the
study, and additional to that routinely collected by the hospital, will be required over
this one month period. In addition, two weeks within the month (with a two-day lead
in period, to settle data collection processes and maximise data quality), will be
dedicated to the collection of clinicians’ times associated with delivering care to

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 4
individual patients. This will require recording of clinicians’ time spent consulting with
each patient and/ or undertaking other specified activities, investigations and
procedures.
● In allocating emergency department/ service clinical staff resources to patients, two
broad strategies are available to sites. These are:
a. A total clinical time method: Under this method, all clinicians within the
emergency department participate in data collection and identify the
patient attributable time associated with each patient managed within the
emergency department during a two-week period. Data on activities and
procedures is also collected during this time. These data are then used to
quantify the total clinician time associated with each patient, and to
estimate the marginal impact on clinician time of specified patient
characteristics or the undertaking of specified procedures/activities. In the
costing process, relative value units (RVUs) can be applied that reflect (a)
directly measured clinician time (for the two-week period); (b) a standard
costing approach applied to utilisation indicators/measures derived from
data collected in the four week period of data collection; and (c) a
standard costing approach applied to utilisation indicators/measures
derived from data routinely collected for the rest of the financial year.
b. Standard cost method. Under this method, the sites undertakes data
collection related to specified activities/procedures undertaken within the
emergency department. This is then used to estimate the mean clinician
time associated with each activity/procedure, which is then used for
developing RVUs. In the costing process, RVUs are applied using (a) a
standard costing approach applied to utilisation indicators/ measures
derived from data collected in the four-week period; and (b) a standard
costing approach applied to utilisation indicators/measures derived from
data routinely collected throughout the rest of the financial year.
● Most emergency departments have several treatment areas. Examples are
resuscitation and fast track. Many patients are managed in only one treatment area,
but some move between areas. It is proposed to use data on the treatment areas
within the costing process, particularly for the allocation of nursing time. Each
treatment area has a specific number of nurses assigned reflecting the types of
patients managed within that area. Hence this information provides a good starting
point for the allocation of nursing costs. The standard cost method described above
can then be used to identify variations in costs for individual patients within a
treatment area (i.e. by identifying the types of consultations or interventions that they
received from other types of clinicians).
● RVUs will need to be developed separately for different types of clinicians, as follows:
● senior medical staff
● junior medical staff
● nurse practitioners
● nursing
● allied health.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 5
An alternative to developing RVUs for senior and junior medical doctors separately is
to have a single set for ‘medical staff’. The former is preferred for this study, but the
latter may be used if the seniority of medical staff cannot be distinguished in the data
collected.
● Each site will need to cost emergency care using a local costing application, and
submit the results of this for the study. Data on utilisation and staff-related RVUs
generated from the study should be used towards allocating costs to individual
patients. The principal reason that the costing needs to be undertaken locally is to
ensure indirect (overhead) costs are allocated appropriately to emergency care
products. This can only occur where the costing component of the study is
embedded within a whole-of-hospital costing study. A secondary objective of
requiring local costing to be undertaken is to create a capability within the
participating sites that results in improved emergency care costing in future years.
● Sites will be required to submit emergency care costs for the full 2015-16 financial
year.
● The data submission requirements for the study include the submission of key input
files for costing emergency care (i.e. those loaded into the costing application), in
addition to the costing results. This approach will assist the study in two ways:
● In some cases, sites may not have the flexibility to change RVUs within their
costing system. In this case the consortium will generate and apply the RVUs
instead.
● The input files will allow the consortium to reproduce local costing results as a
means of validating the results produced locally by the sites.
● The timing of when local costing is undertaken for the study has been aligned with
the period during which annual hospital costing is undertaken for the National
Hospital Cost Data Collection; draft costing results are due by 31 October 2016 and
final costing results by 16 December 2016. Subsequently, the costing approach used
in this study will be embedded within the National Hospital Cost Data Collection as
routine for emergency care costing.
● The costing study at each site will be supported by a field management team (FMT)
from the Health Policy Analysis consortium. FMTs will:
● Facilitate communication between study sites/ jurisdictions and the
consortium/ IHPA project management team.
● Train study site coordinators and other site project team staff (this will be on a
train-the-trainer basis; site co-ordinators will train clinicians).
● Assist site coordinators in setting up sites for data collection.
● Monitor site progress during data collection.
● Troubleshoot problems that arise.
● Feedback data to the site at the end of the study and collect information
about the site’s experiences with the study.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 6
Costing study scope
The study is designed to capture the clinical and stay characteristics of patients receiving
emergency care and related acute services (e.g. short stay units attached to the
emergency department), and costs. It will be conducted in a representative sample of
emergency departments and emergency services across Australia.
In Australia, emergency care units are classified into different levels according to a system
developed by IHPA in consultation with the Emergency Care Advisory Working Group (IHPA
2015). The levels reflect the nature and roles of the service and staffing of the units. Using this
classification:
Emergency departments are defined as emergency care services at levels 3B-6.
Emergency departments are usually located in medium to large hospitals.
Emergency services are defined as emergency care services at levels 1-3A.
Emergency services are usually located in small hospitals in rural and remote settings.
The classification is available at: www.ihpa.gov.au/internet/ihpa/publishing.nsf/Content/nep-
glossary-2015-16#attach.
Note that in this document the term ‘emergency department’ will be used to refer to both
emergency departments and emergency services, unless specific reference is being made
to one of these groups.
A Sampling strategy has been developed to ensure a representative spread of large, small,
regional, rural and metropolitan emergency departments/ services in the study. It is aimed to
include between 20 and 30 sites in the study from across Australia.
Emergency departments in larger hospitals often have one or several short stay units that are
managed as a part of the emergency department or closely coordinated with the
emergency department. Short stay units and models have a variety of names, such as short
stay units, medical assessment units, emergency management units, observation units.
Patients managed in short stay units are in scope of this study. The costing study component
has been designed to be broader than the current scope of emergency care classifications.
The reason for this is that the study will explore the implications of the boundaries between
emergency and acute care as defined under the current model of activity based funding.
Data collection components
The study has four data collection components, which are described below.
Part A: Service level descriptive and related data. This is service level data describing the
emergency care service and its relationships with other services within the hospital setting
(e.g. short stay units). These data are provided once at the start of the project (8 April 2016),
with an update of one component (annual staffing for 2015-16) later in the study (12 August
2016).
Part B: Clinician related time. This component of the study is to occur for a two-week period,
commencing between 1 April 2016 and 1 June 2016 (preceded by two days lead in, to settle

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 7
data collection processes and maximise data quality). During this two-week period data is to
be collected on clinical time associated with either:
patients and defined activities/procedures OR
defined activities/procedures.
The actual data collection approach adopted for a particular site will depend on the
capacity to collect the relevant clinical time data. Costing will be most accurate and
informative where clinical time associated with individual patients is collected. However, this
may not feasible for all sites. An alternative approach will be to collect clinical time
associated with a defined set of activities and procedures. This will yield an empirical basis for
assigning costs associated with clinical inputs.
The data from Part B is to be submitted by 12 August 2016.
Part C: Additional patient and emergency department stay characteristics. This component
of the study is to occur for a four-week period, overlapping with Part B, and commencing
between 1 April 2016 and 1 June 2016. A broad range of patient and emergency
department stay characteristics are already routinely collected by emergency department
staff. During this phase, additional data items will be collected, either prospectively or
through retrospective review of patient electronic and/or paper records. These additional
characteristics relate to:
Additional factors related to patients that potentially impact the cost of care
(referred to as diagnosis modifiers in this document).
Procedures and investigations undertaken on patients.
Patient movements between treatment areas within an emergency department.
Many of the data items above are already available in electronic form, in either emergency
department systems, patient administration systems, or imaging, pathology and pharmacy
systems. However, for most sites, this part of the study will involve collection of some
additional data on patient characteristics. Data on admitted patient episodes immediately
following an emergency department stay will also be required for the study.
In addition to data from the four-week period, data already routinely available for the full
2015-16 financial year is required to be submitted as part of the study. It should be
emphasised that there will be no additional data collection requirements outside the four-
week period.
The data from Part C is to be submitted by 12 August 2016.
Part D: Cost data: The final component of the study relates to costed emergency department
stays. The costing activities have been integrated with the annual National Hospital Cost
Data Collection process, and thus will occur in the period July-October 2016. Data from Parts
B and C will be used in the costing process, to generate more accurate costs for patient
emergency department stays. The costing results need to relate to the full 2015-16 financial
year, although analysis is likely to be focussed on data from the four-week period covered by
Part C.
In addition to the outputs of the costing process, key files that are inputs to the costing
process are required to be submitted for the study. Further information about costing is in the
Costing methodology document.
Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 8
Draft cost data is to be submitted by 31 October 2016, with final data submitted by 16
December 2016.
Costing components of study
For this study, costing is required to be undertaken for the full 2015-16 financial year. This is for
the following reasons:
Most sites cost either a six- or 12-month period. Many sites do not have the capacity
to cost shorter periods of time.
Requiring sites to submit input files to produce costs for one month (i.e. the length of
this study) would be onerous.
There is a capacity through this study to improve the costing results for the full 2015-16
financial year (this is described further below).
There is an interest in testing hypotheses over whether costs within emergency
departments vary across seasons, and this can be explored if the costing is done over
the full financial year.
All sites participating in the Emergency care costing study will be undertaking costing for the
full 2015-16 financial year for the National Hospital Cost Data Collection. (Participation in the
National Hospital Cost Data Collection is a prerequisite for participating in the Emergency
care costing study.) Given this, the additional requirements for this study are:
preparation of input files
development of RVUs based on data collected at the site during the study
application of the locally developed RVUs for the allocation of direct costs to
emergency care patients.
There is further discussion of the processes that can be used to develop RVUs in Chapter 3 of
this document.
The input files for costing are structured differently within different hospitals depending on the
costing system that a hospital uses. The systems in use include Power Performance
Management Version 2 (PPM2), Transition II, the Combo costing application (VisaSys) and
CostPro Plus (SyRis). Within these systems, a key file (known by various names, including
‘Emergency treatment data’, ‘Services table’) is used to identify whether there was utilisation
of a particular intermediate product during a patient episode or stay, and the amount of
utilisation of that product. The file includes data from a range of sources, including
emergency department stay data, admitted patient episode data, and extracts from
imaging, pathology and pharmacy systems. In this file, utilisation may be quantified (e.g. in
minutes or actual charges), or it may be flagged that there was use of a particular resource
(e.g. a value of 1 indicates that the service had been used during the stay or episode).
For this study, sites will be required to submit the overall results of the costing study and the
relevant input files used for costing. In addition to service level and activity data, there will be
four cost related submissions for the study. These are described in Table 1.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 9
Table 1 – Cost data submissions for the study
Submission File name File description
Submission D1 EDCost Patient and product cost file data elements: Costs of
emergency department patients, and admitted patient
episodes for patients subsequently admitted to hospital. This
file will be the output of a local costing application, structured
to reflect the standard output for the National Hospital Cost
Data Collection.
Submission D2 CostCentreExtract Final cost centre file: Extract from costing system to reflect the
direct cost centre costs for the emergency department cost
centre and associated short stay units. This will be extracted
from the local costing application and reflects the direct
costs after allocation to final emergency care cost centres,
and reflects any reclassification of costs that has been
applied through the costing process.
Submission D3 ServiceTreatment Service/ utilisation/ products file: This is the file within the
costing the application that reflects the indicators of
utilisation used in the costing process to allocate final cost
centre costs to patient stays.
Submission D4 RVU Relative value unit (RVU) file: The file will include details of all
RVUs used in the costing process for emergency care stays.
For this study, the RVUs for clinical staff costs are to be generated from data collected during
the study itself. The Health Policy Analysis consortium will be able to assist with this if sites are
not able to generate the RVUs themselves. The consortium will generate RVUs based on the
activity data collected by sites, which is to be submitted to IHPA (through the state/ territory
health authority) by 12 August 2016. The consortium will analyse the data to develop RVUs,
and provide the results back to sites through IHPA, in time for these to be used in the costing
phase of the project.
Staff related costs represent around three-quarters of emergency care costs. Improving the
allocation of staff costs to emergency care stays will be one of the key areas in which the
study will aim to improve cost estimation. Improvements will also be sought for the allocation
of other costs through greater attention to the processes that are generally in place for
routine costing for the National Hospital Cost Data Collection. These include the accurate
allocation of diagnostic imaging, pathology and pharmacy costs to emergency department
stays.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 10
Study stages
A sampling strategy for the study has been developed that identifies the numbers of sites
required to achieve representation of emergency care across metropolitan, regional, rural
and remote settings, and other relevant characteristics.
State and territory health authorities will coordinate the nomination of sites to participate in
the study. Sites that have been proposed to participate in the study will first be assessed to
determine the feasibility of their participation in the study. The feasibility assessment will
consider issues such as the sites’ existing capacity to collect relevant emergency care data
and undertake a patient costing process. Sites will complete a short feasibility survey form,
which will be analysed by the project team. Final decisions on site participation will be
undertaken by IHPA and state/territory health authorities.
The Table below describes the key stages of the project and timing.
Table 2 – Study stages
Project stage Project management tasks*:
Specific costing related tasks are in bold Target dates
Site selection Site nomination for participation in study 30 September 2015
Decision on sites selected for participation in study 31 December 2015
Study
preparation
Commencement of study coordinator February 2016
Establish arrangements for data collection of study
Identify mechanisms through which specified
data will be collected.
Take steps to ensure data collection/
extraction/ coding mechanisms are in place
and working prior to study commencement.
Coordinate training for clinical and other staff
on an additional data collection processes
required for the study.
Set up study database (to be provided by
consortium).
February to end of March
2016
Part A submissions due. Related to service level
characteristics, details of treatment areas,
medical and nursing staffing of shifts, allied health
arrangements, approach to setting RVUs for
clinical time for previous National Hospital Cost
Data Collection submissions.
8 April 2016
Data collection Commencement of collection of additional
patient characteristics.
Commencement of collection of clinician time.
Between 1 April 2016 and
1 June 2016
Part B and C submissions due. Relate to clinician
time, additional patient characteristics, and Non-
admitted patient emergency department care
and Admitted patient care national minimum
data sets.
12 August 2016
Costing Commence costing process. 1 July 2016
Develop process for partitioning emergency
department cost centres to address consultation/
liaison services, teaching training and research,
reception/triage, other product services.
July to August 2016
Clinical time RVUs to be prepared and finalised. 16 September 2016
Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 11
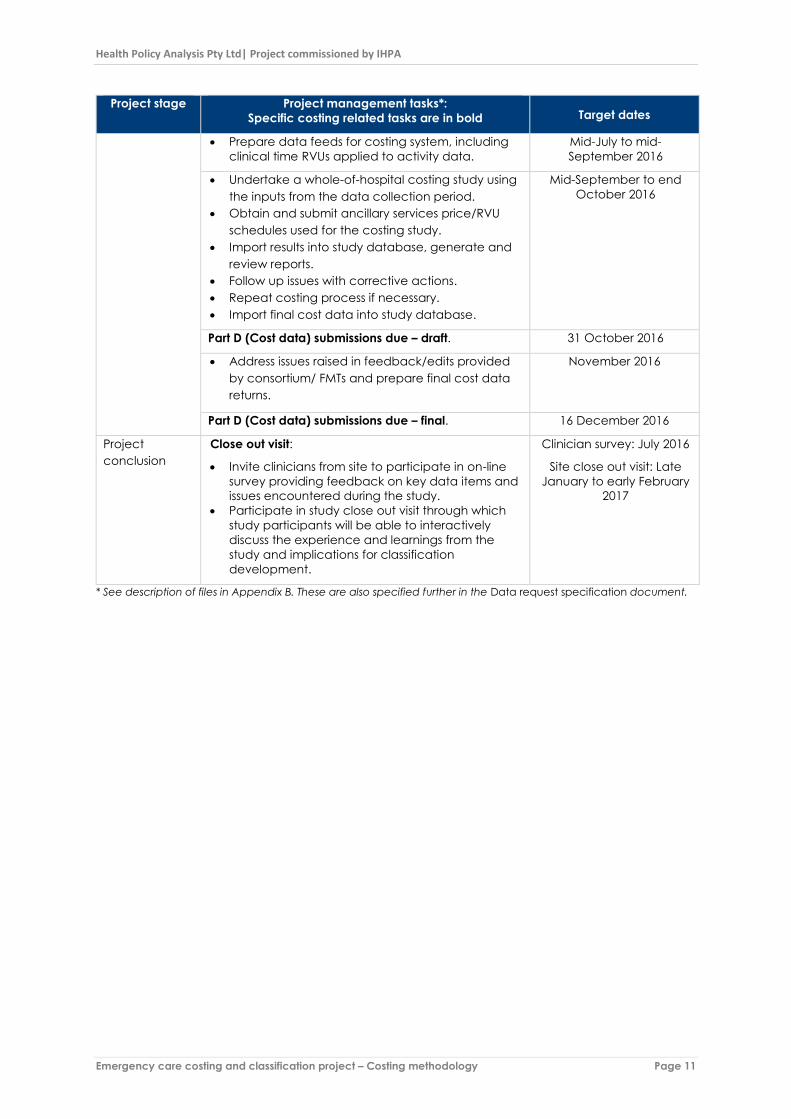
Project stage Project management tasks*:
Specific costing related tasks are in bold Target dates
Prepare data feeds for costing system, including
clinical time RVUs applied to activity data.
Mid-July to mid-
September 2016
Undertake a whole-of-hospital costing study using
the inputs from the data collection period.
Obtain and submit ancillary services price/RVU
schedules used for the costing study.
Import results into study database, generate and
review reports.
Follow up issues with corrective actions.
Repeat costing process if necessary.
Import final cost data into study database.
Mid-September to end
October 2016
Part D (Cost data) submissions due – draft. 31 October 2016
Address issues raised in feedback/edits provided
by consortium/ FMTs and prepare final cost data
returns.
November 2016
Part D (Cost data) submissions due – final. 16 December 2016
Project
conclusion
Close out visit:
Invite clinicians from site to participate in on-line
survey providing feedback on key data items and
issues encountered during the study.
Participate in study close out visit through which
study participants will be able to interactively
discuss the experience and learnings from the
study and implications for classification
development.
Clinician survey: July 2016
Site close out visit: Late
January to early February
2017
* See description of files in Appendix B. These are also specified further in the Data request specification document.

Emergency care costing and classification project – Costing methodology Page 12
3
3 Overview of methodology The Emergency care costing study involves several components designed to create the
necessary foundation for a rigorous costing process that is consistent with the Australian
Hospital Patient Costing Standards (Independent Hospital Pricing Authority, 2014).
The key features of the costing methodology are described below.
Local costing
A key design principle for this study is that patient level costing will be undertaken by study
sites. FMTs will provide support and advice to study site staff, but it is not intended that the
FMTs actually do the costing. As discussed above, the data submission requirements for the
study have been designed so that a costing process can be replicated by the Health Policy
Analysis consortium, and the sensitivity of results tested for variations in costing approaches.
However, local costing has been adopted as the appropriate strategy for the project for two
reasons:
By taking this approach, capacity and capability for improved patient level costing
of emergency care will be built within the participating sites. It is hoped that following
the completion of the study, sites will continue to apply the costing enhancements
implemented during the study and further refine these.
Certain aspects of any modelling of costs at the national level are best based on the
results of a local costing process. An example of this is the allocation of indirect costs
in the costing process. To meet the Australian Hospital Patient Costing Standards
Version 3.1 (Independent Hospital Pricing Authority, 2014), indirect cost allocations
should be based on a consistent process applied within the context of a whole-of-
hospital/health service costing study.
The study involves each site undertaking costing using a local costing application. This part
will be undertaken by local staff with costing expertise (e.g. those with experience with the
National Hospital Cost Data Collection).
Data submitted by sites will allow the costs generated at the local level to be analysed by
the Health Policy Analysis consortium. This will be for the purposes of understanding the
differences between sites in the approaches undertaken (which will be important for
classification development), as well as validating the local results.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 13
Allocation of direct costs
Emergency department clinical staff inputs
Staffing costs represent the most significant component of emergency department costs. In
this study, sites will be required to develop RVUs for clinical staff inputs, separately for senior
medical staff, junior medical staff, nurse practitioners, other nursing staff, and allied health.
(There is an option to develop ‘medical staff’ RVUs if the costs of senior and junior doctors
cannot be differentiated.) These RVUs will be based on data collected locally for the study,
supplemented, where appropriate, by other information generated from the study. In
addition, other data will also be collected through the study to allow a better basis for
allocating clinical staff inputs to emergency patients.
Table 3 gives an overview of the allocation methods for clinician time that are possible for
the Emergency care costing study based on data collected during the study.
Table 3 – Description of final allocation statistic methods to be applied in the Emergency
care costing study for clinician time
Allocation method
for clinician time
Description Use in Emergency care costing
study
Actual time
The actual time spent by a clinician to
provide services to an individual patient.
For allocating the costs of clinician time,
this number will be multiplied by the
average hourly rate of the clinician type.
This option is available for those
sites collecting actual clinician
time for all clinicians and across all
patients. This approach can only
be applied for the two-week
period during which clinician time
will be collected.
Actual utilisation
with internally
derived RVUs
The actual number of units consumed
(from the feeder system), with RVUs
developed from internal data
(preferably with local clinical
involvement) applied to reflect the
relative cost of each product/service
consumed in the end-product class.
These RVUs may be calculated on
several bases depending on the service
setting, including occupied bed days,
theatre sessions, emergency
department and non-admitted patient
products.
This is the ‘standard’ costing
method described earlier. RVUs
will be more specific for the weeks
in which data on additional
patient characteristics have been
collected. The study will also
develop RVUs that can be applied
to data routinely collected by
each site, which will be used in
costing the remainder of the
financial year.
This study also intends to address the issue that staffing varies across shifts during the day and
also potentially across days of the week, as well as the impact of public holidays on staffing.
It is also recognised that the seniority of staff, staffing levels by shift, penalty rates and call
back arrangements all have an impact on cost, and will be explored in the analysis.
An analysis of the National Hospital Cost Data Collection shows that many sites are using
externally derived RVUs to allocate costs. In addition, these are frequently applied to
measures of utilisation such as treatment time in the emergency department, triage
category, or emergency department class (i.e. using Urgency Related Groups or Urgency
Disposition Groups). Without appropriate adjustment, treatment time is problematic for
allocating costs in that it assumes that more resources were allocated to a patient due to the

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 14
fact that they stayed longer in the emergency department. This is not necessarily the case.
Also, the use of triage category or emergency department class results in circularity in the
costing, as these variables are reinforced as cost drivers rather than reflecting actual
variation in costs between patients based on other characteristics.
Another issue identified within the current approaches to costing emergency care is possible
over-allocation of costs to patients who do not wait to be treated. It is suspected that this is a
result of treatment costs being allocated to this group of patients, and/or the use of
measures of treatment time that including a waiting time component. For the purposes of this
study, sites will be requested to separate out costs associated with the pre-treatment/ triage
stage from those associated with treatment. This will allow only the pre-treatment/ triage-
related costs to be allocated to patients who do not wait for treatment.
In summary, the study will capture information on actual clinician time. This will be used to
generate local RVUs to apply to other components of the study. By collecting additional
utilisation measures and paying close attention to factors known to impact costs, the study
will yield cost estimates which will be significantly more accurate than those routinely
generated from costing processes currently contributing data to the National Hospital Cost
Data Collection. The study will avoid the inherent circularity in using external RVUs based
on triage and existing classification systems.
Short stay units
Costs of short stay units managed within the emergency department are in scope of the
current study. One of the aims of the study is to explore the boundaries between emergency
departments and short stay units. It is also possible that the type of patients managed in a
short stay unit by some hospitals are managed in the emergency department by others; and
thus these differences in classification of these patients will be important to explore in the
study. The approach to costing this component of the stay will be based on the usual
National Hospital Cost Data Collection approach.
Mental health services/units located in emergency care settings
Mental health services/units located in emergency care settings will be in-scope for the
study. The main reason for this is to understand the crossover between the emergency
department and these units in care provision, and the types of patients referred to these units
where they exist.
Diagnostic imaging
Diagnostic imaging costs are an important component of emergency care costs. For most
sites participating in the National Hospital Cost Data Collection, these are usually costed
separately as an intermediate product and then allocated to patients actually receiving
imaging. This provides an accurate measure of resource utilisation of diagnostic imaging.
The additional insights that will be provided by the Emergency care costing study are:
Diagnostic imaging data will be captured for each patient, as part of the
investigations submission (Submission C4).
Diagnostic imaging utilisation data used in costing will be collected as part of the
study.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 15
Additional information will be obtained from each site on the RVU/cost schedule used
for diagnostic imaging, together with relevant descriptors.
Analysis will be undertaken nationally to determine whether differences in RVU/cost
schedules for diagnostic imaging items has a material effect on cost estimates. If
there is evidence of material and systematic effects, then adjustments to address
these may be considered.
Pathology costs
The approach proposed for pathology costs is the same as that for diagnostic imaging.
Pharmacy costs
The approach proposed for pharmacy costs is similar to that for diagnostic imaging. An issue
to be considered for the study will be the impact of pharmacy imprest. There are a few
relatively higher cost drugs used within emergency departments, such a thrombolytics. These
may or may not be recorded as individually prescribed drugs and allocated to patients
based on the relevant pharmacy data extracts used for costing. This issue should be
investigated by site costing coordinators. If higher costs drugs prescribed and administered
within the emergency department are not included in pharmacy extracts (e.g. they are
available as imprest), site costing co-ordinators should consider whether there are alternative
means of identifying the emergency department patients being administered these drugs
and incorporating this into the costing process.
Medical and surgical supplies
The approach to medical and surgical supplies will align with the approaches for the
National Hospital Cost Data Collection.
Consultation liaison services
Clinical liaison is a significant activity for some emergency departments, and thus will be
captured in this study. There are two types of consultation liaison services that are relevant to
the current study:
a. Emergency department outreach: Consultation liaison services provided by
emergency department staff for patients who are not currently patients of the
emergency department. This can occur where a general practitioner or clinician at
another emergency department calls and requests advice about a patient. In some
instances, the patient may be subsequently referred to the emergency department,
but in many cases, this may be avoided. In this study:
Aggregate counts of these contacts will be captured (Submission B4).
Costs for these contacts should be allocated to a separate final product (NE2
- Non-admitted care provided by an emergency department clinician to a
patient who is not currently a patient of the emergency department, through
consultation and liaison, telemedicine or other means).
b. Emergency department in-reach: Consultation liaison services provided by other
clinical staff in the hospital (who are not paid for under the emergency department
cost centres) for patients currently in the emergency department. This type of care
might involve, for example:

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 16
A specialist assessment of a patient, which helps inform the treatment course
(including whether the patient should be admitted). In a substantial
proportion of these instances the patient may not be subsequently admitted.
A specialist assessment of a patient where the treatment course is generally
known, but that early assessment will facilitate the next stages of treatment
(e.g. a surgical advanced trainee’s and/ or an anaesthetist’s assessment of a
patient who will need surgery, an assessment of a patient with hip fracture by
an orthogeriatrician or geriatric advanced trainee).
Provision of an intervention by a nurse from a specialised team (e.g. pain
management).
A count of these services has been included in study (Submission B5). However, it is
not expected that separate adjustments will be made for these services within the
costing component of the study.
Costing study steps
The costing component of the study has five broad steps, which align with the steps involved
in the conduct of any hospital costing study. As mentioned previously, the costing should be
conducted as part of a whole-of-hospital costing study. The key steps are:
Step1: Development of final allocation statistics for clinical staff and other resource
categories based on data collected during the study.
Step 2: Assignment of cost centres in the general ledger to appropriate final cost
centre types (reflecting product categories wherever possible, including the specific
emergency care product categories) and indirect (overhead) cost centre types.
Mapping of cost line items to National Hospital Cost Data Collection line type item
categories.
Step 3: Allocation of costs from indirect (overhead) cost centres to direct cost
centres.
Step 4: Allocation of costs accumulated in final cost centres to product categories.
Step 5: Allocation of costs to patients within product categories.
These five steps are shown in Figure 1. The Figure references the most relevant standards from
the Australian Hospital Patient Costing Standards that need to be applied at each step. The
chapters following this one provide additional guidance on each of these steps, highlighting
the issues that are likely to be specific to the Emergency care costing study. In each of the
sections, specific Australian Hospital Patient Costing Standards that will be important for the
study are highlighted. However, the published version of Australian Hospital Patient Costing
Standards Version 3.1 should be references for detail on the standards and related material.
This is available at:
http://www.ihpa.gov.au/internet/ihpa/publishing.nsf/content/Australia-Hospital-Patient-
Costing-Standards.htm

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 17
Final product categories
In an activity based costing exercise, all products generated by a health service should be
costed (i.e. including both patient and non-patient products). It is only through the costing of
all products that one can be reasonably confident that there will be reconciliation between
the costs incurred by a health service and the costs reflected in the patient level costing
results.
The final product categories defined for this study are shown in Table 4 below. These align
with the National Hospital Cost Data Collection product classes, except for Non-admitted
emergency care (NE), where for the purposes of this study, the product is to be split into:
NE1 Non-admitted emergency care for patients currently within emergency
department.
NE2 Non-admitted care – external consultation and liaison - patient not currently
within the emergency department.
The study will capture the cost of admitted patient episodes that immediately follow an
emergency department stay. These will principally be acute episodes (product class AC).
This will capture the cost of the short stay unit(s) plus, the cost of any additional components
of the acute care episode that follows the short stay unit.
This data may include some sub-acute episodes that follow emergency department stay
(reflected in products RH, PC, GM, PG, MA, OA). Non-admitted services following an
emergency department stay (products OP, OC and MH) are not in scope of the study.
Table 4 – Final product categories for the Emergency care costing study
Code Product class Comment
AC Acute As defined for the National Hospital Cost Data
Collection. Will include the cost of patient stay within
short stay units. This may be followed by a transfer to
another ward or discharge
RH Rehab As defined for the National Hospital Cost Data
Collection PC Palcare
GM GEM
PG PsychGer
MA Maint
OA OthAdmPatCar
OG OrganProc
BD Boarder
NB Newborn
AE AdmED The costs of the emergency department component
of care prior to transfer to a short stay unit, ward,
operating theatre or intensive care, coronary care
unit or other admitted patient service.
NE1 Non-admitted emergency care for
patient currently within emergency
department.
The costs of emergency department care provided
to patients who are treated in the emergency
department but not admitted to the hospital in which
the emergency department is located. This will
include the costs of patients who did not wait.
NE2 Non-admitted care – external
consultation and liaison - patient
not currently within emergency
department.
Non-admitted care provided by an emergency
department clinician to a non-admitted patient who
is not currently within the emergency department,
through consultation and liaison, telemedicine or
other means.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 18
Code Product class Comment
OP Outpat Not relevant for the study
OC OutComm
RS Research As defined for the National Hospital Cost Data
Collection TC Teaching
OT Other
MH Mental Health (Community)

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 19
Figure 1 – Schematic representation of emergency care costing process and related Australian Hospital Patient Costing Standards (AHPCS)

Emergency care costing and classification project – Costing methodology Page 20
4
4 Detailed description of
each costing step This Chapter details the steps for costing for the Emergency care costing study. The costing
component of the study can proceed once the activity data collection has been
completed.
Step 1: Final allocation statistics
Final allocation statistics are required for:
medical staff
nursing staff
allied health staff
other staff
medical and surgical supplies.
In most sites intermediate or ancillary services (diagnostic imaging, pathology and
pharmacy) are represented separately, with costs allocated to individual patient episodes or
stays. Within many hospitals and health services, there are cross-charging arrangements in
place for ancillary services. Alternatively, standard approaches to developing RVUs for
ancillary services are in place, with data that allow allocation of costs to individual patients.
Existing data sources which indicate clinical inputs at the patient
level
Many sites have data collection systems for some clinical categories that provide an
indication of clinical input (either time or other service) associated with an individual patient.
In the initial establishment stage for the study, each site should investigate and assess local
data systems that can be used for identifying clinical inputs to emergency care for individual
patients. Examples include:
In small hospitals, medical services are sometimes provided by a local general
practitioner, and in some instances these general practitioners are paid on a fee-for-
service basis. In this case the fee-for-service charge reflects the actual cost allocation
statistic for medical services at the patient level.
In many hospitals, allied health departments or specific allied health disciplines have
implemented data capture systems for clinician time associated with individual
patients. These data collection systems can be used to generate actual time
allocation statistics for all (or some components) of allied health services.
In some hospitals nurse dependency systems are in place that classify patients
according to the level of nursing required. These systems give an indication of the
relative nursing input for patients at different levels of dependency on average, but
do not necessarily reflect the actual nursing input an individual patient receives.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 21
These systems can be used to generate RVUs for allocating nursing costs. The RVU
depends on whether estimates of the relative levels of nursing input for different levels
of nursing might have been generated from a local study (internally-derived RVUs),
an external study (externally-derived RVUs), or a judgment about the levels of nursing
implied for different types of patients.
The assessment of existing collections should consider whether these systems are sufficient to
meet the requirements for the Emergency care costing study. The following points should be
considered:
How complete is the data collection? That is, is the data collected for all patients by
all relevant clinicians? If not, gaps will need to be filled.
Are some elements of the data based on sources external to the site? In this case it
would be important to consider a local study to validate the RVUs.
Does the relativity need to be adjusted to reflect a different denominator? For
example, the RVUs may be applied to time a patient spends in a unit. However, if it
has been calculated to reflect relativities for patients as a whole, it may need to be
re-weighted.
For this study, RVUs based on triage, Urgency Related Group or Urgency Disposition Group
will not be accepted.
Approaches to developing RVUs
As outlined in earlier in this document, there are two broad strategies are available to sites for
developing clinician time RVUs based on data collected through this study. These are:
A: Total clinician time method: Under this method all clinicians within the emergency
department participate in data collection. They collect their time associated with
providing care to individual patients within the emergency department during a two-
week period. RVUs are developed by analysing the relationships between patient
and stay characteristics (including the provision of procedures) and clinician time. For
this method the focus of the clinician time data collection will be on total clinician
time for a patient.
B: Standard cost method: Under this method a standard set of activities/ procedures
that are undertaken on patients in the emergency department is specified. Data
collection is focussed on estimating the time associated with these activities/
procedures, and how this is impacted by patient characteristics. For this method the
focus of the clinician time data collection will be on activities and procedures, and it
is not necessary to consider the total clinician time associated with a patient.
These approaches are described in detail in Appendix A.
Definition of treatment, waiting and other periods
In local systems and the Non-admitted patient emergency department care national
minimum data set, the following date/time variables are recorded:
Presentation date/time (when the patient first presented to the emergency
department).
Triage date/time (when the patient was assessed by a triage nurse).

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 22
Clinical care commencement date/time.
Episode end date/time.
Physical departure time.
(Some local systems also report the time first seen by a nurse and the time first seen by a
doctor.)
With the exception of resuscitation patients, patients attending an emergency department
usually present to the emergency department reception where they are registered and then
seen and assessed by a triage nurse. The patient then usually waits for a period of time prior
to commencement of treatment. This waiting period may be extended. Some patients do
not wait for treatment, and for these patients, there will be an episode end date/time but no
clinical care commencement date/time. These patients have an episode end status of ‘did
not wait’. Some patients may also not be assessed by a triage nurse.
The treatment phase of a patient emergency care stay will end when treatment has been
completed. In most cases patients depart the emergency department at this time. In other
instances there may be delay before the patient physically leaves the emergency
department.
These date/time stamps and associated periods are described in Figure 2 below. For the
costing study it will be important that:
Treatment time is measured on a consistent basis. This should be the time between
the commencement of clinical care and the episode end time.
Waiting time is not included in treatment time and the costs of the triage process are
appropriately allocated. For this study, the costs of triage and waiting times are to be
separately identified. Where the site does not have an actual separate cost centre
for this service, a virtual cost centre should be created, based on the usual staffing for
the triage function. Through Step 2 of the costing process described in Figure 1 (p. 19),
study sites should allocate the costs of triage to this separate cost centre. Costs from
this cost centre should then be allocated to patients based on an indicator that the
patient was triaged. This will be able to be derived from the emergency department
stay data. This should exclude all visit types (including patients that are dead on
arrival) other than ‘emergency presentation’1.
Adjustments are made for patients where the stay has ended, but the patient has not
yet physically departed the emergency department. This time should be excluded
from the treatment time calculations. However, some consideration should be given
to appropriate means to address costs that may occur in these circumstances.
Arrangements are likely to vary across sites.
1 See ‘Type of visit to emergency department’, METeOR identifier 495958,
http://meteor.aihw.gov.au/content/index.phtml/itemId/495958.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 23
Figure 2 – Components of an emergency department stay
Source: Australian Institute of Health and Welfare 2014. Australian hospital statistics 2013–14: emergency
department care. Health services series no. 58. Cat. no. HSE 153. Canberra: AIHW, Figure 1.1 page 5.
Dead on arrival
Dead on arrival may have different meanings at different sites, and between states and
territories. A common definition is that the patient was attended to by an ambulance, but
died at the scene or prior to their arrival to the emergency department. However, in other
cases the category is also used to register people that die outside of hospital without being
attended to as an emergency, prior to transferring the body to the mortuary. An appropriate
approach to costing dead on arrival patients needs to be developed by sites reflecting the
local meaning of this category.
Step 2: Alignment of costs to all product categories
The emergency care costing for this project will be undertaken as part of a whole-of-hospital
costing study. This will ensure that all relevant costs are considered, that emergency care
services are allocated appropriate overhead costs, and that costs of the subsequent hospital
stay for patients in short stay units associated with emergency departments can also be
estimated.
Step 2 of the costing process described in Figure 1 (p. 19) involves working with the general
ledger for a hospital to ensure the data is in a structure that can be most effectively used for
costing. As discussed previously, the product categories for this study align with the product
categories for the National Hospital Cost Data Collection. The one enhancement in this study
is that the product category of NE Non-admitted emergency care has been split into two
sub-categories:
NE1 Non-admitted emergency care for patient currently within emergency
department: The costs of emergency department care provided to patients who are
treated in the emergency department but not admitted to the hospital in which the
emergency department is located. This will include the costs of patients who did not
wait.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 24
NE2 Non-admitted care – external consultation and liaison - patient not currently
within emergency department: Non-admitted care provided by an emergency
department clinician to a patient who is not currently a patient of the emergency
department, through consultation and liaison, telemedicine or other means.
The key elements of this step are well described in the Australian Hospital Patient Costing
Standards. Standards that have a particular relevance to the current study are listed below.
SCP 1.004 Hospital Products in Scope: Which defines the broad set of products that should be
in scope for any hospital costing study, specifically:
admitted patient products
non-admitted patient products
emergency department patient products
teaching, training and research products
non-patient products.
For this study, these broader categories have been split into the categories specified in Table
4 above.
SCP 3B.001 Costing all Products: This standard requires that all costs should be accounted for
in the costing process and allocated, as appropriate, across all patient and non-patient
products generated by the hospital in the costing period.
SCP 3G.001 Reconciliation to Source Data: This standard requires that there be a statement
that reconciles the activity and cost data outputs of the product costing process to the
activity and costs that were captured in the source data. For this study, this requirement
would be met through exactly the same processes adopted for the National Hospital Cost
Data Collection.
SCP 3.001 – Matching Production and Cost: This standard is important for several stages in the
costing study. The following points are particularly important to note for Step 2 of the costing
process described in Figure 1:
Matching starts at the level of the whole hospital by determining the manipulations
required to the general ledger entries to align the costs to be used in product costing
with the quantities of products produced (application of SCP 1.004, SCP 2.003., SCP
3E.001, GL 1.003, GL 1.003, GL 2.004, GL 4.004).
This manipulation process should generally occur within the product costing systems
(not the general ledger), and should be done in such a way that there is a clear
reconciliation of the costs reported in the product costing system to the hospital’s
general ledger.
…it may be necessary to partition final cost centres into product categories
(application of SCP 2A.003, SCP 2B.002, SCP 3B.001, SCP 3C.001, GL 4A.002, GL 4B.003,
GL 4C.002).
In the current study the following issues may need specific attention by sites:
Partitioning costs related to management of emergency department
reception/triage and waiting times. A clear basis and rationale for partitioning costs

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 25
related to these functions should be developed and documented as part of the
study.
Partitioning costs related to short stay units managed within an emergency care unit
cost centre. A clear basis and rationale for partitioning costs related to these
functions should be developed and documented as part of the study.
Ensuring cost centres/costs associated with TTR that are directly managed within the
emergency care department are allocated to separate TTR cost centres.
Determining whether costs for the consultation liaison services provided by
emergency department clinicians are to be identified as a separate “cost centre” at
Step 2 or partitioned in an allocation process at Step 3 of the costing process
described in Figure 1. A clear basis and rationale for partitioning costs related to
these functions should be developed and documented as part of the study. This
should reflect the results of the clinician time allocation study undertaken as part of
the study.
Partitioning costs related to any other services/non-patient costs. These might
include, for example, costs of emergency care staff involved in retrieval services.
Sometimes retrieval relates to patient admitted to another hospital and this also
needs to be factored into the costing study. A clear basis and rationale for
partitioning costs related to these functions should be developed and documented
as part of the study.
GL 4B.003 ED definition: This standard provides a definition of an emergency department as
follows:
A department that provides initial, typically unscheduled, treatment to patients with a
broad spectrum of illnesses and injuries, some of which may be life threatening and
require immediate attention.
The guidelines for the standard go on to state:
Any discrete areas of the hospital that may be attached to, or associated with, the
emergency department in which admitted patients are managed are considered to
be general ward areas for product costing purposes…Such services include Short
Stay Admitted Units, Clinical Decision Units, Short Stay Medical Assessment Units, and
Emergency Management Units. The key defining attribute is admission to a bed in a
discrete area that is used only for admitted patients, in contrast to admitting a patient
while he/she is occupying a trolley or examination bay in the emergency department
that is also used to provide care to patients who are not admitted.
This study will be consistent with this standard, but the scope of the study will include costing
patients managed by or closely associated with emergency departments, such as short stay
admitted units, clinical decision units, medical assessment units, and emergency
management units. This will allow the study to yield data that will assist in examining issues
associated with the boundaries between emergency department and these units.
The guidelines for this standard also state that:

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 26
For the purpose of product costing, the emergency department service event is
considered to comprise all the services provided in the period from a patient’s
presentation to his/her departure from the emergency department including all
ancillary services ordered for the patient during that period.
This guideline will also be applied during the study. As a consequence, ancillary services
ordered for the patient during the emergency department stay are to be attached to the
emergency care stay.
The standard is silent with respect to Emergency Services. These will be in-scope for this study.
GL 2.004 – Account Code Mapping to Line Items: This standard requires hospitals to map all
in-scope costs to the list of line items specified in the GL 2.004 standard. This standard will also
apply for this study.
Some states and territories have adopted standard that split a range of other line items into
more detailed categories. For this study data reported using the more detailed line
categories will be accepted, as long as these can be mapped without ambiguity to the
standard list of line items specified in the Australian Hospital Patient Costing Standards.
Step 3: Overhead allocation
The process of allocating indirect costs (overheads) to direct cost centres is an important
stage of any product costing process. The Australian Hospital Patient Costing Standards have
several standards that address these issues, including:
COST 1.002 – Overhead Allocation Method
COST 1A.002 – Overhead Allocation – Hotel Services
COST 1B.002 – Overhead Allocation – Overhead Depreciation Costs
COST 2.004 – Overhead Allocation Statistics.
Study sites participating in the Emergency care costing study should apply these standards. It
is anticipated that this involves no specific additional efforts over and above those
undertaken for rounds of the National Hospital Cost Data Collection.
Step 4: Allocation to product categories
Ideally many of the issues associated with the allocation of costs to product categories will
have been resolved in Step 2 of the costing process described in Figure 1. Final costs centres
should be aligned with final products. As discussed above, the product categories for this
study align with the product categories for the National Hospital Cost Data Collection. The
one enhancement is that the product category of NE Non-admitted emergency care, has
been split into two sub-categories:
NE1 Non-admitted emergency care for patient currently within emergency
department: The costs of emergency department care provided to patients who are
treated in the emergency department but not admitted to the hospital in which the
emergency department is located. This will include the costs of patients who did not
wait.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 27
NE2 Non-admitted care – external consultation and liaison - patient not currently
within emergency department: Non-admitted care provided by an emergency
department clinician to a patient who is not currently a patient of the emergency
department, through consultation and liaison, telemedicine or other means.
Step 5: Allocation of costs to patients
The allocation of costs within final cost centres to patients is at the centre of costing
processes. Costing application typically process several files including:
Data allocated to the final cost centres (with overheads) split into cost components.
(In this study, this is Submission D2: Final cost centre file).
Data identifying and describing the patient stay/ episode to which costs will be
allocated. (In this study, this is Submission C1: Emergency department stay and C6:
The Admitted patient care NMDS).
Data inputs indicating the utilisation/level of services provided to the patient during
their stay. These may include, for example, variables related to the length of stay in a
ward, the treatment time in an emergency department and other indicators related
to the service level involved. In many instances these variables are flags that indicate
that a particular service was accessed (1) or not (0), rather than the level of service
used. There may be several records for a single patient episode, reflecting indicators
of the service level for different types of input (e.g. medical staff inputs, nursing inputs,
medical and surgical supplies). (In this study, this is Submission D3: Service/ utilisation/
products file).
RVU or weights files, which provide an indication of the relative weights that should be
applied against the utilisation/services data in C above. For example in current
costing for emergency care it is not uncommon for the Urgency Related Groups or
Urgency Disposition weights to be specified in the RVU/weights file (reflecting
estimates of the time input or indeed the national cost weights). A specification of
how the weights are to be applied may also be included. For example, it is not
uncommon for the specification to be that the treatment time in the emergency
department should be multiplied by the weights based on the Urgency Related
Group of the episode. Weights associated with particular indicator variables (such as
related to a particular procedure) may also be specified, reflecting the addition
resource (or time) input that may be required when that procedure is performed. (In
this study, this is Submission D4: RVU).
The costing process will involve merging the data from the utilisation/services file with the RVU
file to identify an indication of the relative utilisation of particular intermediate product (e.g.
medical salaries), for each emergency care stay or episode. The result is then merged with
the final costs data (A) so that all final costs for an intermediate product are allocated to
across patient stays/ episodes reflect the measure of utilisation.
The allocation of costs to stays/episodes is driven by the data in the Service/ utilisation/
products file and the RVU files. For the Emergency care costing study, RVUs for staff related
costs will be generated through the processes described in Step 1 of the costing process
described in Figure 1 (p. 19), and further described in Appendix A.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 28
The standard from the Australian Hospital Patient Costing Standards which has particular
relevance to this stage of the study is: Cost 3.004 Final Cost Allocation to patients and other
products. This standard requires that “all final costs will be allocated to patients and other
products using methods prescribed in this standard”. The standards include an Appendix
(Table E.2) which includes suggested allocation methods. The sections of this Table related to
emergency departments are shown in Table 5.
A key objective if this study is to allocate clinical staff costs to patients based on either data
collected on total clinician time (Alternative 1 in Table 5), or based on RVUs generated from
the study (Alternative 3 in Table 5). These RVUs will be applied to indicators of services/
utilisation generated from the study and also services/utilisation that can be generated from
routinely available data. The study aims to provide a sound empirical basis on which these
internally derived RVUs are developed.
Table 5 – Allocation methods for final costs suggested in
the Australian Hospital Patient Costing Standards
Cost type Alternative 1 Alternative 2 Alternative 3 Alternative 4
Medical Salaries &
Wages Actual time
Planned/ rostered
time
Internally derived
RVUs by patient
service event
Externally derived
RVUs by patient
service event
Nurse Salaries &
Wages Actual time
Planned/ rostered
time
Internally derived
RVUs by patient
service event
Externally derived
RVUs by patient
service event
Allied Health
Salaries & Wages Actual time
Planned/ rostered
time
Internally derived
RVUs by patient
service event
Externally derived
RVUs by patient
service event
Other Salaries &
Wages
Actual time Planned/ rostered
time
Internally derived
RVUs by patient
service event
Externally derived
RVUs by patient
service event
Prosthetics
Actual cost
Actual utilisation
with internally
derived RVUs
Actual utilisation
with externally
derived RVUs
Externally derived
RVUs
Other Goods and
Services Actual cost
Actual utilisation
with internally
derived RVUs
Actual utilisation
with externally
derived RVUs
Externally derived
RVUs
Pharmacy Actual cost
Actual utilisation
with internally
derived RVUs
Actual utilisation
with externally
derived RVUs
Externally derived
RVUs
Pathology Actual cost
Actual utilisation
with internally
derived RVUs
Actual utilisation
with externally
derived RVUs
Externally derived
RVUs
Imaging Actual cost
Actual utilisation
with internally
derived RVUs
Actual utilisation
with externally
derived RVUs
Externally derived
RVUs
On-costs As per relevant Salaries & Wages line item.
Hotel Services Actual cost
Actual utilisation
with internally
derived RVUs
Actual utilisation
with externally
derived RVUs
Externally derived
RVUs
Depreciation
Actual utilisation
with internally
derived RVUs
Actual utilisation
with externally
derived RVUs
Externally derived
RVUs

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 29
Step 6: Intermediate costs (pathology, imaging and
pharmacy)
Intermediate/ancillary costs such as diagnostic imaging, pathology and pharmacy are
important components of the costs of emergency care. In most costing studies, these are
costed in a separate intermediate product costing process and then allocated to individual
patients. Allocation to individual patient is often possible because systems for managing
orders for imaging and pathology are electronic as is the case for most pharmacy systems.
The costing of intermediate products generally involves determining average costs for items
in hospital or services specific schedule that specifies the type of diagnostic imaging
procedures, pathology tests or drugs. Sometimes external reference schedules are used to
estimate relativities (e.g. the Medical Benefits Schedule) and sometimes relativities for items
have been generated through a local costing process.
For this study, sites should use the costing processes already established for ancillary services
with respect to the National Hospital Cost Data Collection. Through the study, however,
information is to be gathered from each participating site on the schedules and the
prices/relativities that will be used for costing. This information will be used to test the
sensitivity of final results to differences in prices/RVUs for ancillary services.
One of the important processes in costing is the attribution of ancillary costs. This study will
adopt the approach stated in the standard GL 4B.003 ED definition:
For the purpose of product costing, the emergency department service event is
considered to comprise all the services provided in the period from a patient’s
presentation to his/her departure from the emergency department including all
ancillary services ordered for the patient during that period.
The standard COST 6.001 – Intermediate Product/Service Matching Method also has
relevance to this stage of the study. The purpose of this standard is to “ensure that the cost of
all intermediate products/services prescribed or ordered during an admitted patient,
emergency department or non-admitted patient service event are captured and attributed
to that service event”. The standard states that:
Intermediate products/services will be costed to the patient service event in which
they are ordered or prescribed. Where there are multiple possibilities for cost
attribution, the point of referral or an explicit preference order encounter matching
method must be used.

Emergency care costing and classification project – Costing
methodology
Page 30
5 5 Reporting cost results and
related data Cost results and related data are to be submitted initially in draft form by 31 October 2016.
Final data are required by 16 December 2016.
The cost results for the study will be submitted as Submission D1 Patient and product cost file
data. This submission is structured in the same way as outputs for the National Hospital Cost
Data Collection. Three other files are also required:
Submission D2: Final cost centre file: An extract from the costing system related to the
emergency department cost centre and associated short stay units. This needs to
include the allocations of direct and indirect costs for emergency care, and the
allocation of within these costs centres to non-patient products such as teaching,
research and other products.
Submission D3: The service/ utilisation/ products file, which is also an extract
from/input to the costing system costing emergency department stays and
associated inpatient episodes.
Submission D4: Relative value unit file: Through which details of RVUs used in the
costing process for emergency department stays are provided.
These files were described in Table 1, and further details of the data elements are shown in
Appendix C. Detailed specifications for each of these files are provided in the Data Request
Specification document.
The provision of these files will allow analysis to be undertaken by the Health Policy Analysis
consortium to understand the local costing allocation approaches, and validate the costing
results. In some instances, local sites will not have the flexibility to change RVUs and related
files to reflect the results of the study. In these cases the consortium will reconstruct the input
files reflecting the utilisation and RVUs, and undertake the costing on behalf of the site. This
also requires the input files described above to be submitted.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 31
Appendix A – Approaches to
developing RVUs Two broad strategies for developing clinician time RVUs based on data collected through
this study were identified in this document:
A: Total clinician time method
B: Standard cost method.
These are described in detail here.
A: Total clinician time method
Under this method all clinicians within the emergency department participate in data
collection and identify the patient attributable time associated with each patient managed
within the emergency department during a two-week period. Depending on the assessment
of the adequacy of existing systems (as discussed above), the scope of this data might be
limited to a certain group of clinicians (e.g. medical staff only), or collected for all clinicians.
Table 6 below illustrates the structure of data that would be collected under the total
clinician time method. The data reflects Submission B3 (Cliniciantime), with the value of the
professions/discipline derived by reference to Submission B1 (StaffStudy), which includes a
de-identified list of all staff contributing to the study and their professions/disciplines. Within
the data collected procedures/activities undertaken will also be recorded. There may be
more than one procedure/activity recorded for each entry.
Table 6 – Structure of patient related clinician time data
Staff ID
(studyStaffID)
Profession/
discipline
(staffProf)
Emergency
department stay
ID (studyStayID)
Procedure/activity
undertaken
(ProcActivity)
Patient related
time
(ClinStafftime)
101 253112a 100000001 xxx 20
101 253112a 100000001 xxx 10
102 253112c 100000001 xxx 15
301 254499 100000001 xxx 20
302 254499a 100000001 xxx 40
401 252511 100000001 Xxx 30 (Profession/ discipline code have the following meanings: 253112a Staff specialist emergency medicine; 253112c =
Advanced trainee (registrar); 254499 = Registered Nurse other; 254499a = Enrolled nurse/Endorsed enrolled nurse;
252511= Physiotherapist.)
This data can be summarised into the total time per patient for each discipline group
representing an intermediate product in the costing system (and which RVUs will be
required). In the summary process, relativities could be introduced to reflect the average
difference in base salary costs between different categories within a discipline group (e.g.
weighting the time of a specialist emergency doctor relative to the time of an advanced
trainee to reflect the difference in in salary levels on average). Total emergency department
treatment time (that is elapsed time between when clinical care commences and when the
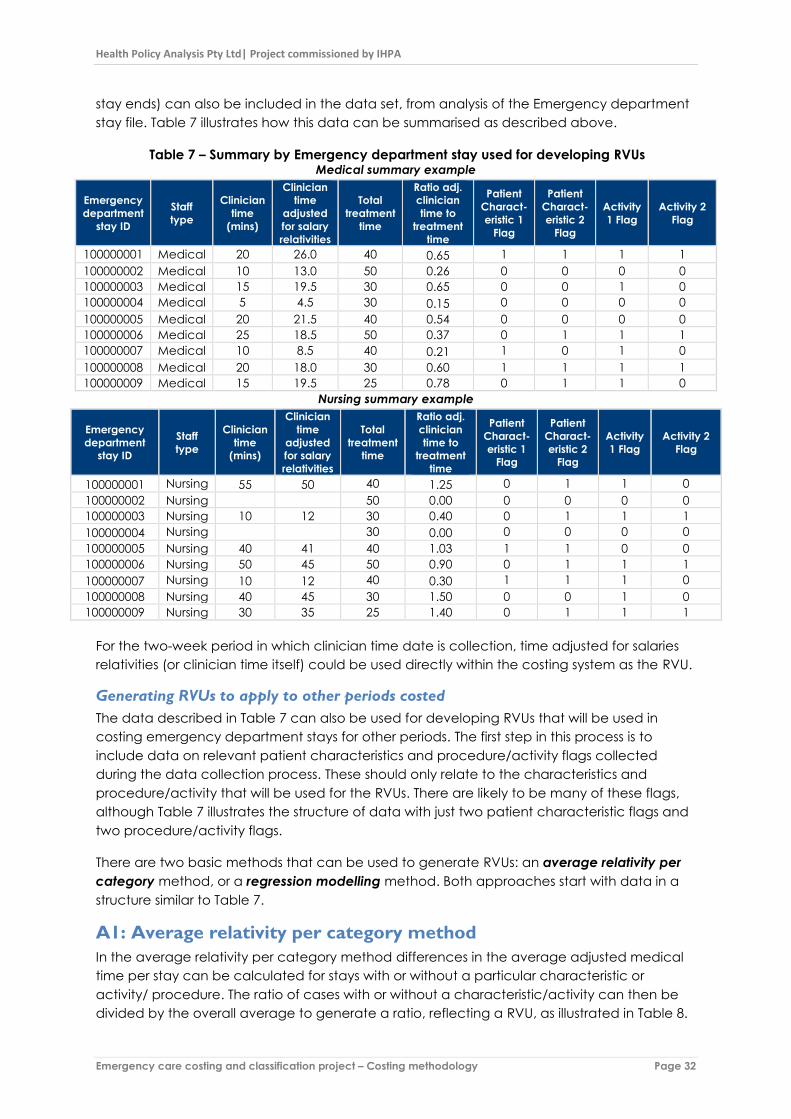
Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 32
stay ends) can also be included in the data set, from analysis of the Emergency department
stay file. Table 7 illustrates how this data can be summarised as described above.
Table 7 – Summary by Emergency department stay used for developing RVUs Medical summary example
Emergency
department
stay ID
Staff
type
Clinician
time
(mins)
Clinician
time
adjusted
for salary
relativities
Total
treatment
time
Ratio adj.
clinician
time to
treatment
time
Patient
Charact-
eristic 1
Flag
Patient
Charact-
eristic 2
Flag
Activity
1 Flag
Activity 2
Flag
100000001 Medical 20 26.0 40 0.65 1 1 1 1
100000002 Medical 10 13.0 50 0.26 0 0 0 0
100000003 Medical 15 19.5 30 0.65 0 0 1 0
100000004 Medical 5 4.5 30 0.15 0 0 0 0
100000005 Medical 20 21.5 40 0.54 0 0 0 0
100000006 Medical 25 18.5 50 0.37 0 1 1 1
100000007 Medical 10 8.5 40 0.21 1 0 1 0
100000008 Medical 20 18.0 30 0.60 1 1 1 1
100000009 Medical 15 19.5 25 0.78 0 1 1 0
Nursing summary example
Emergency
department
stay ID
Staff
type
Clinician
time
(mins)
Clinician
time
adjusted
for salary
relativities
Total
treatment
time
Ratio adj.
clinician
time to
treatment
time
Patient
Charact-
eristic 1
Flag
Patient
Charact-
eristic 2
Flag
Activity
1 Flag
Activity 2
Flag
100000001 Nursing 55 50 40 1.25 0 1 1 0
100000002 Nursing 50 0.00 0 0 0 0
100000003 Nursing 10 12 30 0.40 0 1 1 1
100000004 Nursing 30 0.00 0 0 0 0
100000005 Nursing 40 41 40 1.03 1 1 0 0
100000006 Nursing 50 45 50 0.90 0 1 1 1
100000007 Nursing 10 12 40 0.30 1 1 1 0
100000008 Nursing 40 45 30 1.50 0 0 1 0
100000009 Nursing 30 35 25 1.40 0 1 1 1
For the two-week period in which clinician time date is collection, time adjusted for salaries
relativities (or clinician time itself) could be used directly within the costing system as the RVU.
Generating RVUs to apply to other periods costed
The data described in Table 7 can also be used for developing RVUs that will be used in
costing emergency department stays for other periods. The first step in this process is to
include data on relevant patient characteristics and procedure/activity flags collected
during the data collection process. These should only relate to the characteristics and
procedure/activity that will be used for the RVUs. There are likely to be many of these flags,
although Table 7 illustrates the structure of data with just two patient characteristic flags and
two procedure/activity flags.
There are two basic methods that can be used to generate RVUs: an average relativity per
category method, or a regression modelling method. Both approaches start with data in a
structure similar to Table 7.
A1: Average relativity per category method
In the average relativity per category method differences in the average adjusted medical
time per stay can be calculated for stays with or without a particular characteristic or
activity/ procedure. The ratio of cases with or without a characteristic/activity can then be
divided by the overall average to generate a ratio, reflecting a RVU, as illustrated in Table 8.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 33
Table 8 – Illustration of development of RVUs
(using the data illustrative medical clinician time data from Table 7)
Character-
istic 1
Character-
istic 2 Activity 1 Activity 2
Mean adjusted clinician time
Without characteristic/activity 16.08 13.40 13.00 14.42
With characteristic/activity 17.50 20.50 18.33 20.83
Overall mean 16.56 16.56 16.56 16.56
RVUs
Without characteristic/activity 0.97 0.81 0.79 0.87
With characteristic/activity 1.06 1.24 1.11 1.26
Mean 1.00 1.00 1.00 1.00
The resulting RVUs can be applied in the costing processes to emergency care stays outside
the two-week period in which clinician time data was collected, using data that indicates
whether or not the specified patient characteristics are present or activities/procedures have
occurred for a patient.
The approach described above is simplified in that the tables above show only two patient
characteristics and two activities. In the study there will likely be a much wider range of
characteristics and activities.
The disadvantages of average relativity per category method include:
At its simplest level of implementation, as illustrated above, the method does not
control for the impact of other characteristics/activities that may be present. This can
be partly addressed by considering the combined effects of two characteristics
together. However, this becomes unwieldly if there are too many patient
characteristics to consider in the analysis.
It is possible that there will be some combinations of patient characteristics that were
not observed during the period in which clinician time was collected.
A2: Regression modelling method
An alternative is to generate estimates of the impact of the presence of patient
characteristics through a multiple regression model. In the model, adjusted clinician time
could be specified as the response or dependent variable, with the characteristics and
activities included as predictor or independent variables. For example, using the example
above, the model could be specified as:
Adjusted Clinician time = Intercept + β1*Characteristic1 + β2*Characteristic2 +
β3*Activity1 + β4*Activity2
Table 9 and Table 10 illustrate the results of regression modelling applied to the illustrative
data from Table 7. Table 9 shows the estimated coefficients for the model. These include an
intercept (the average predicted level of adjusted clinician time when none of the
characteristics or activities are present) and coefficients for each characteristics and activity,
representing the increase (or decrease) in adjusted clinician time associated with the
presence of absence of the characteristic/activity. Table 9 shows how these coefficient can
be combined to estimate all combinations of characteristics and activities. In this simple

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 34
example there are ten unique combinations, but with the addition of other
characteristics/activities possible combinations increase significantly.
Table 9 – Illustration of estimation of a multiple regression model using the
medical clinician time data from Table 7: Estimated coefficients
Estimate Std. Error t value Pr(>|t|)
(Intercept) 13.00 4.44 2.9280 0.0429*
Characteristic1 -2.71 7.12 -0.3810 0.7224
Characteristic2 4.14 10.07 0.4110 0.7018
Activity1 2.36 7.87 0.2990 0.7795
Activity2 3.14 10.07 0.3120 0.7705
Table 10 – Illustration of results from a multiple regression model used to generate RVUs for
combinations of characteristics and activities
Combinations of characteristics Predicted adj.
clinician time RVU
Mean all observations 16.56 1.00
Characteristic 1 alone 10.29 0.62
Characteristic 1+2 14.43 0.87
Characteristic 1+2 + Activity 1 16.79 1.01
Characteristic 1+2 + Activity 1+2 19.93 1.20
Characteristic 2 alone 17.14 1.04
Characteristic 2 + Activity 1 19.50 1.18
Characteristic 2 + Activity 1+2 22.64 1.37
Activity 1 alone 15.36 0.93
Activity 1+2 18.50 1.12
Activity 2 alone 16.14 0.98
The model described in above can be extended by including a treatment time variable in
the specification as follows:
Adjusted Clinician time = Intercept + β1*Treatmenttime + β2*Characteristic1 +
β3*Characteristic2 + β4*Activity1 + β5*Activity2 + β6*Activity2
This model, yields the results shown in Table 11. The results of this specification are similar to
the interpretation of the previous model, except now there is an additional coefficient for
Treatmenttime. This coefficient can be interpreted as the additional amount of adjusted
clinician time for each additional minute of treatment time (i.e. the elapsed time the patient
spends within the emergency department from when clinical treatment starts). The model still
includes an intercept, which reflects the minimum amount of adjusted clinician time for any
patient. However, as treatment time increases, this approach would also allow for an
increase in the adjusted clinician time estimated for a patient.
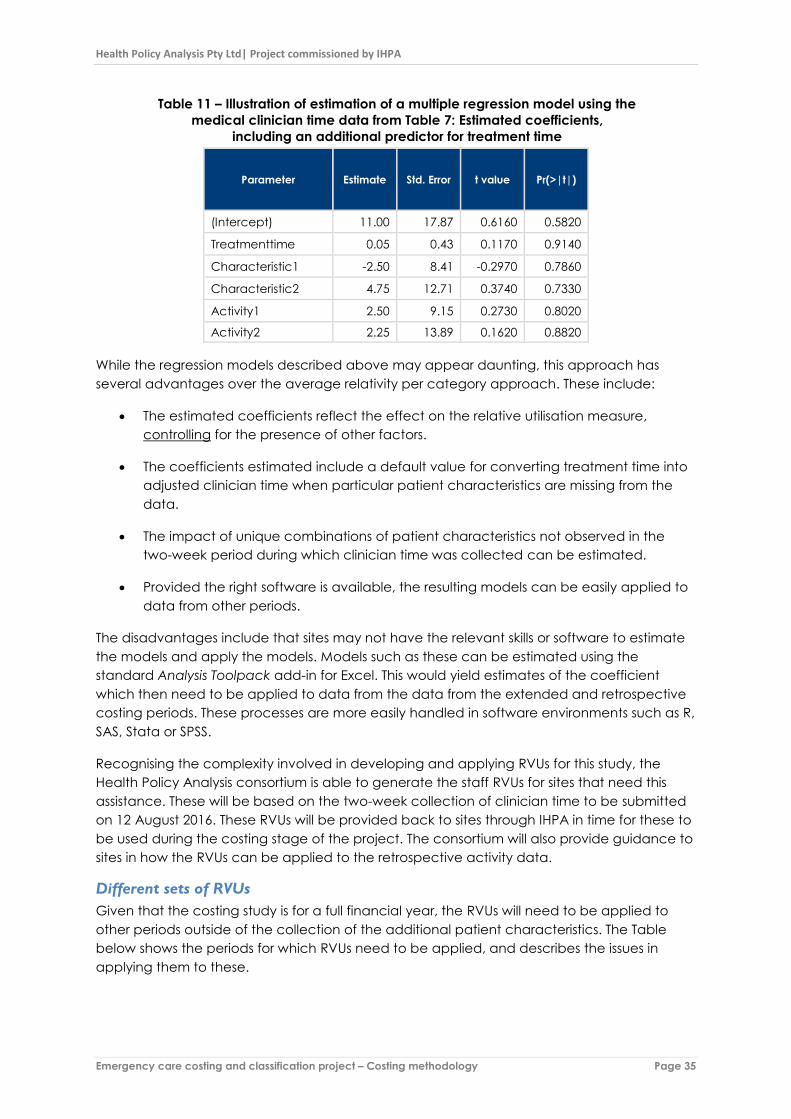
Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 35
Table 11 – Illustration of estimation of a multiple regression model using the
medical clinician time data from Table 7: Estimated coefficients,
including an additional predictor for treatment time
Parameter Estimate Std. Error t value Pr(>|t|)
(Intercept) 11.00 17.87 0.6160 0.5820
Treatmenttime 0.05 0.43 0.1170 0.9140
Characteristic1 -2.50 8.41 -0.2970 0.7860
Characteristic2 4.75 12.71 0.3740 0.7330
Activity1 2.50 9.15 0.2730 0.8020
Activity2 2.25 13.89 0.1620 0.8820
While the regression models described above may appear daunting, this approach has
several advantages over the average relativity per category approach. These include:
The estimated coefficients reflect the effect on the relative utilisation measure,
controlling for the presence of other factors.
The coefficients estimated include a default value for converting treatment time into
adjusted clinician time when particular patient characteristics are missing from the
data.
The impact of unique combinations of patient characteristics not observed in the
two-week period during which clinician time was collected can be estimated.
Provided the right software is available, the resulting models can be easily applied to
data from other periods.
The disadvantages include that sites may not have the relevant skills or software to estimate
the models and apply the models. Models such as these can be estimated using the
standard Analysis Toolpack add-in for Excel. This would yield estimates of the coefficient
which then need to be applied to data from the data from the extended and retrospective
costing periods. These processes are more easily handled in software environments such as R,
SAS, Stata or SPSS.
Recognising the complexity involved in developing and applying RVUs for this study, the
Health Policy Analysis consortium is able to generate the staff RVUs for sites that need this
assistance. These will be based on the two-week collection of clinician time to be submitted
on 12 August 2016. These RVUs will be provided back to sites through IHPA in time for these to
be used during the costing stage of the project. The consortium will also provide guidance to
sites in how the RVUs can be applied to the retrospective activity data.
Different sets of RVUs
Given that the costing study is for a full financial year, the RVUs will need to be applied to
other periods outside of the collection of the additional patient characteristics. The Table
below shows the periods for which RVUs need to be applied, and describes the issues in
applying them to these.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 36
Table 12 – Periods to be costed during the study and
the issues in applying RVUs to these periods
Periods included in the costing study Issues in applying RVUs generated
from the study
The period prior to the start of data collection for
the study.
RVUs need to be applied to data that is routinely
available.
The period during which clinician time has been
collected (a 2 week period). During this time
additional data on patient characteristics and
activities/procedure will also be collected.
The costing process could use the results clinician
time component of the study (i.e. allocate costs
to patients based on actual clinician time), or
use the RVUs generated from this process,
applied to the extended set of patient
characteristics/ activities collected during this
period.
The period during which additional data on
patient characteristics and activities/procedure
is collected, but collection of clinician time has
ceased (a one-month period all up, with two
weeks overlapping with the collection of the
clinician time collection).
The costing process will use the RVUs generated
from this process, applied to the extended set of
patient characteristics/ activities collected
through the study.
The period following the end of the data
collection for the study (unless the study finishes
on 30 June 2016).
RVUs need to be applied to data that is routinely
available.
One implication is that at least two sets of RVUs need to be generated for the costing
process:
1. RVUs limited to data on patients characteristics and activities/procedures which are
routinely available.
2. RVUs related to the full set of patient characteristics and activities/procedures
collected during the study.
These can be easily estimated using the clinician time data using the methods described
above. For the regression modelling approach, models can be estimated including and
excluding the variables that are not available for certain periods to be costed. This will ensure
the resulting RVUs are calibrated between periods (although additional checks should be
applied).
For practical reasons in the costing process, these resulting RVUs will need to be combined
into one comprehensive set of RVUs that can apply across both periods. As mentioned
above, in doing this it is extremely important to calibrate the overall effect of the RVUs so that
they do not result in over- or under-allocation of resources between the study period and the
rest of the financial year.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 37
B: Standard cost method
The approach starts with the development of a standard set of activities/ procedures that
are undertaken on patients in the emergency department. Table 13 provides examples of
these activities. They include:
Activities that are associated with the usual flow of patients through an emergency
department (e.g. triage assessment, initial nursing assessment, initial treating clinician
bedside evaluation).
Activities related to discrete procedures undertaken for specific patients (e.g. IV
medication dispensing and administration, chest tube/catheter insertion).
Figure 3 illustrates the types of activities that might occur within a particular emergency
department stay.
For each of these activities an estimate of the average clinician time associated with the
activity is developed. The estimates of average clinician time is used to develop RVUs
associated with each activity. The process for the development of estimates of average
clinician time per activity and RVUs is described further below.
The next step in the process is to analyse data collected routinely and data collected
throughout the study on activities/procedures to flag in which emergency department stays
specific activities/procedures occurred. Many activities/procedures can be inferred through
routinely collected data. For example, for each patient with a triage assessment date and
time and a valid triage value, it can be inferred that a triage assessment was undertaken. For
patients where there is a clinical care commencement date and time recorded, it can be
inferred that an initial nursing assessment and an initial treating clinician bedside evaluation
occurred. For patients where a diagnostic imaging investigation is recorded, it can be
assumed that a clinician ordered the test (and also interpreted the results).

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 38
Table 13 – Examples of activities used for standard costing approach Activity examples Description How the activity can be flagged
Nursing activities – standard workflow
Triage assessment All actions undertaken at initial contact by triaging
clinician until triage process completed.
All emergency department stays in which a
triage assessment date and time is recorded.
Exceptions include where the visit type is a
planned visit, or the patient is dead on arrival.
Initial nursing assessment All actions undertaken during initial assessment and
documentation of initial assessment. This may include an
initial set of observations and actions to prepare a
patient for treating clinician assessment (e.g. positioning
patient, cleaning patient, changing patient etc.).
All emergency department stays in which the
patient is moved to treatment areas in which an
initial nursing assessment is routinely undertaken
for patients.
Clinical observations Acquisition of a set of clinical observations relevant to
the attendance including explanation of process, actual
measurements and documentation of observations -
when done as a distinct activity rather than part of an
initial nursing assessment
For most patients within particular treatment
areas observations will be undertaken regularly
during the patients stay in that area. The time in
the treatment area can be used to estimate the
number of times observations will be taken.
Nursing summation and disposition Activities undertaken to complete the episode of care
including dispensing of discharge medications,
discussion of discharge instructions, finalisation of
documentation, liaison or assistance to facilitate patient
physically leaving emergency department, finalisation of
data entry into emergency care system.
End of emergency department stay within
treatment area.
Nursing activities – other activities/procedures
IV medication dispensing and
administration
All actions from preparation, checking out medications
from stores, administration at bedside, documenting
administration and any post administration actions –
(e.g. dispensing packaging/sharps, other than additional
observations undertaken post administration (which are
counted separately)
Procedure code recorded for Peripheral IV
insertion.
Blood specimen collection Pathology test code reported in Investigation
data return

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 39
Table 13 continued Activity examples Description How the activity can be flagged
Treating clinician activities – standard workflow
Initial treating clinician
bedside evaluation
All actions from first assigning self to patient on emergency
department tracking system until detailed patient assessment at
bedside completed. This may include an initial perusal of referral
information, results or imaging or viewing of clinical documentation
from prior clinical record before actually moving to the bedside.
All emergency department stays in which
clinical care commences. Estimated times
may vary between different types of patients
which can be inferred from patient data and
treatment area.
Initial treating clinician
synthesis & documentation
All actions undertaken in preparing and completing the initial
documentation of the patient assessment and plan of management
in the clinical record. This may include perusal of referral information,
results or imaging or viewing of clinical documentation from prior
clinical record and discussion with other clinicians in the emergency
department or external to the emergency department, conversations
with GPs, residential care facilities and next of kin not present in
emergency department prior to completing the initial entry in the
clinical record.
All emergency department stays in which
clinical care commences. Estimated times will
vary between different types of patients based
on analysis of patient data and treatment
area.
Additional treating clinician
bedside evaluation:
Additional discrete periods of time the treating clinician spends at the
bedside irrespective of activity undertaken (e.g. could include re-
evaluation, discussion with relatives present, updates on progress,
addressing concerns)
Involvement of an additional clinician may
need to be inferred by the nature of the
patient, based on analysis of patient data and
treatment area.
Additional treating clinician
synthesis and documentation
Discrete periods of time a clinician spends on one patient perusing
results or imaging or in discussion with other clinicians in the
emergency department or external to the emergency department or
reading and editing the clinical record of the patient or
communicating with external individuals like GPs, residential care
facilities and next of kin not present in the hospital.
Involvement of an additional clinician may
need to be inferred by the nature of the
patient, based on analysis of patient data and
treatment area.
Treating clinician activities – other activities/procedures
Place diagnostic imaging
order
Diagnostic imaging order code reported in
Investigation data return
Interpret diagnostic imaging
order
Diagnostic imaging order code reported in
Investigation data return
Chest tube/catheter insertion Procedure code recorded for Chest
tube/catheter

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 40
Figure 3 – Illustration of possible activities to be used within a standard costing approach

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 41
Estimation of average clinician time per activity
Estimation of the average clinician time per activity can be based on empirical data
collection and/or clinician estimation. This study will primarily rely on empirical data collection
occurring during the study. However, a clinician estimation process will also be undertaken to
provide a means of triangulating and supplementing the empirical results from data
collection at a site. This may be important, as the local data collection processes may not
fully capture all types of activities required for costing.
Prior to the study’s commencement a clinical estimation process will be undertaken by the
study consortium. This will yield estimates of the average clinician time associated with the list
of activities and how these vary across a high level categorisation of patient types as follows:
Table 14 – Patient type grouping for estimate variation in clinician time by
activity/procedure related to the usual flow of patients
Patient
type
Description Possible criteria for assigning patients
1 Simple case No more than one each of an investigations,
procedures or external consultations.
2 Complex case - medical Medical diagnosis (excluding mental health
diagnosis) with more than one of either investigations,
procedures or external consultations.
3 Complex case – injury Injury diagnosis with more than one of either
investigations, procedures or external consultations.
4 Resuscitation case Resuscitation triage or relevant procedure recorded
5 Cooperative mental health
case
Mental health diagnosis, without presence of
diagnosis modifier – Distress/ confusion/ agitation
requiring one-to-one nursing
6 Aroused/ aggressive case
requiring sedation
Presence of diagnosis modifier – Distress/ confusion/
agitation requiring one-to-one nursing
Within the study data on clinician time for each activity is to be collected in the format
specified for Submission B2 Clinician time allocated to patients and procedures/activities,
which has been illustrated Table 6. The principal difference with the total clinician time
approach, is that data on all clinical interactions with each patient need not be collected
for the standard costing approach. Rather data needs to be collected on a sufficient
number of activities to enable the mean clinician time associated with the activity to be
estimated and analysis of how that varies across different patient categories undertaken.
Once data is collected it will need to be summarised by activity/procedure. This will yield the
total clinician time per activity/procedure. Using data on the type of clinician involved in the
activity/procedure it is also possible to calculate clinician time adjusted for salary relativities
as described earlier. Information on patient characteristics and other factors will also be used
to categorise the patient for which the activity is undertaken into one of the patient types
described in Table 14. Table 15 illustrates how this summarises data would appear for
selected nurse interventions.
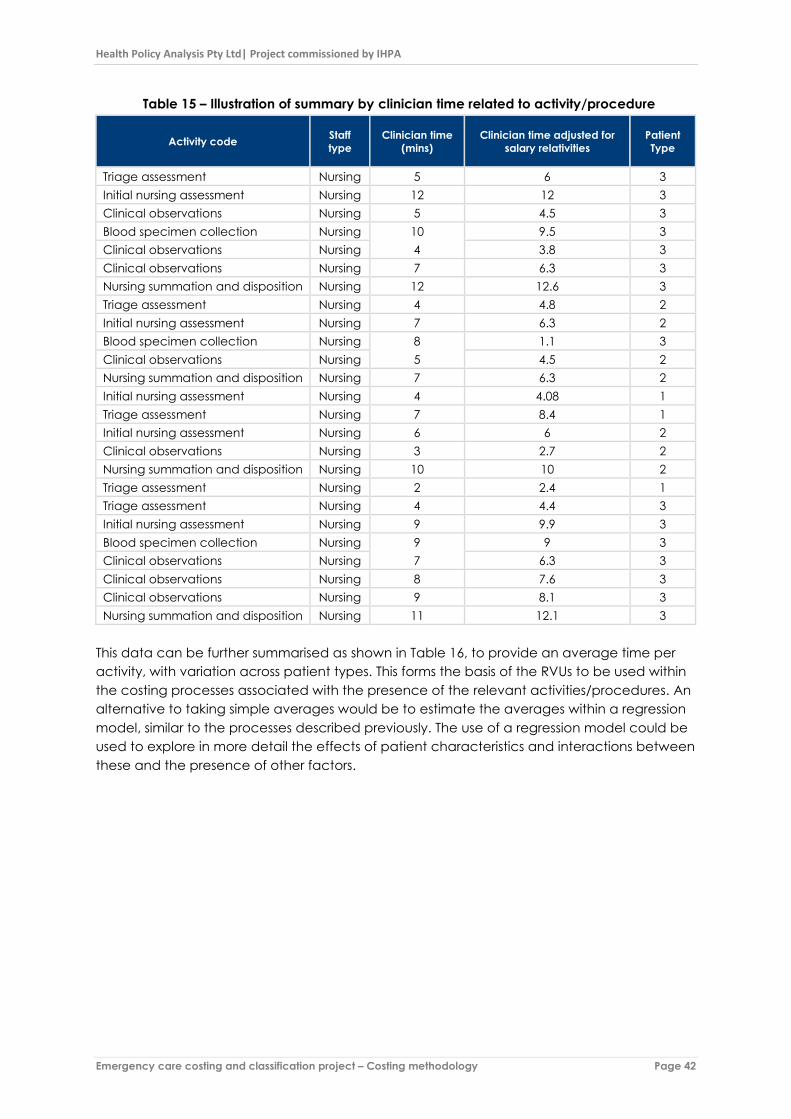
Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 42
Table 15 – Illustration of summary by clinician time related to activity/procedure
Activity code Staff
type
Clinician time
(mins)
Clinician time adjusted for
salary relativities
Patient
Type
Triage assessment Nursing 5 6 3
Initial nursing assessment Nursing 12 12 3
Clinical observations Nursing 5 4.5 3
Blood specimen collection Nursing 10 9.5 3
Clinical observations Nursing 4 3.8 3
Clinical observations Nursing 7 6.3 3
Nursing summation and disposition Nursing 12 12.6 3
Triage assessment Nursing 4 4.8 2
Initial nursing assessment Nursing 7 6.3 2
Blood specimen collection Nursing 8 1.1 3
Clinical observations Nursing 5 4.5 2
Nursing summation and disposition Nursing 7 6.3 2
Initial nursing assessment Nursing 4 4.08 1
Triage assessment Nursing 7 8.4 1
Initial nursing assessment Nursing 6 6 2
Clinical observations Nursing 3 2.7 2
Nursing summation and disposition Nursing 10 10 2
Triage assessment Nursing 2 2.4 1
Triage assessment Nursing 4 4.4 3
Initial nursing assessment Nursing 9 9.9 3
Blood specimen collection Nursing 9 9 3
Clinical observations Nursing 7 6.3 3
Clinical observations Nursing 8 7.6 3
Clinical observations Nursing 9 8.1 3
Nursing summation and disposition Nursing 11 12.1 3
This data can be further summarised as shown in Table 16, to provide an average time per
activity, with variation across patient types. This forms the basis of the RVUs to be used within
the costing processes associated with the presence of the relevant activities/procedures. An
alternative to taking simple averages would be to estimate the averages within a regression
model, similar to the processes described previously. The use of a regression model could be
used to explore in more detail the effects of patient characteristics and interactions between
these and the presence of other factors.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 43
Table 16 – Illustration of average clinician time per activity/procedure
Activity Patient types
1 2 3 All types
Average of Clinician time (mins)
Triage assessment 4.5 4.0 4.5 4.4
Initial nursing assessment 4.0 6.5 10.5 7.6
Clinical observations (per set of observations) 4.0 6.7 6.0
Nursing summation and disposition 8.5 12.0 9.7
Blood specimen collection 9.0
Average of Clinician time adjusted for salary relativities
Triage assessment 5.4 4.8 5.2 5.2
Initial nursing assessment 4.1 6.2 11.0 7.7
Clinical observations 3.6 6.1 5.5
Nursing summation and disposition 8.5 12.0 9.7
Blood specimen collection 6.5
Different sets of RVUs
The standard costing method described will require RVUs that are applicable outside the
period of the data collection. As discussed above, it will be possible to infer that certain types
of activity occur, using routinely available data. However, for periods outside the four weeks
of the data collection, data on additional procedures may not be available.
One consequence of this is that the RVUs for the periods outside the data collection need to
calibrated, so that one average, they end up allocating an appropriate proportion of
resources to stays within and outside the data collection period. Unless this occurs, the
costing process will over allocated resources to the data collection period, and under
allocate resources to the rest of the financial year.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 44
Appendix B – Description of
data submissions See Data request specification for detailed specifications of files.
Table 17 – Description of data files
Submission File name File description
Submission A1 ServiceReturn Service level return: Characteristics of the emergency
department (e.g. annual volume, role delineation,
location).
Submission A2 TreatmentArea Treatment areas: A listing of treatment areas within the
emergency department, characteristics and usual nursing
staffing across shifts.
Submission A3 MedTeam Medical teams: A listing of medical teams within the
emergency department.
Submission A4 MedTeamStaff Medical team staff: A listing of medical staff types within the
team and usual shift start and end times.
Submission A5 AlliedStaff Allied health staff: A listing of allied health staff types and
usual shift start and end times.
Submission A6 StaffProfile Staff profile: Full time equivalent staff directly employed in
the emergency department by type of staff for 2014-15 and
2015-16.
Submission A7 LocalCodesDis Local disposition codes: The list of emergency department
disposition codes recorded in local system with mapping to
national and study values.
Submission A8 LocalCodesPP Local presenting problem codes: The list of emergency
department presenting problem (complaint) codes
recorded in local system (if these exist) with mapping to
study values.
Submission A9 LocalCodesProc Local procedures codes: The list of emergency department
procedure codes used for the study. For most hospitals,
these will be those listed on barcodes for clinicians and/ or
coders to collect during the study. For some they might be
those contained in the local emergency department
information system.
Submission B1 StaffStudy Staff in study: A de-identified list of clinical staff of the
emergency department employed during the data
collection period of the study, including their discipline and
the cost centre from which they are paid.
Submission B2 StaffStudyShifts Staff shifts: Days and shifts worked by staff of the emergency
department during data collection period for the study.
Submission B3 ClinicalTime Staff time allocated to individual patients and/or
procedures/activities: Clinical staff time allocated to
individual patients and the associated procedure/activity.
Submission B4 ExternalConsults External consultations: Consultations provided by
emergency department clinicians related to patients who
are not currently patients of the emergency department.
Submission B5 InternalConsults Internal consultations: Consultations provided by clinicians
not part of the usual staffing of the emergency department.
These are in relation to patients of the emergency
department, and may be to clinicians, or directly to the
patient.
Submission C1 EDStay
Emergency department stay: All of the data elements of the
Non-admitted patient emergency department care NMDS
2015-16 (METeOR identifier 588932) together with additional
study-specific items.
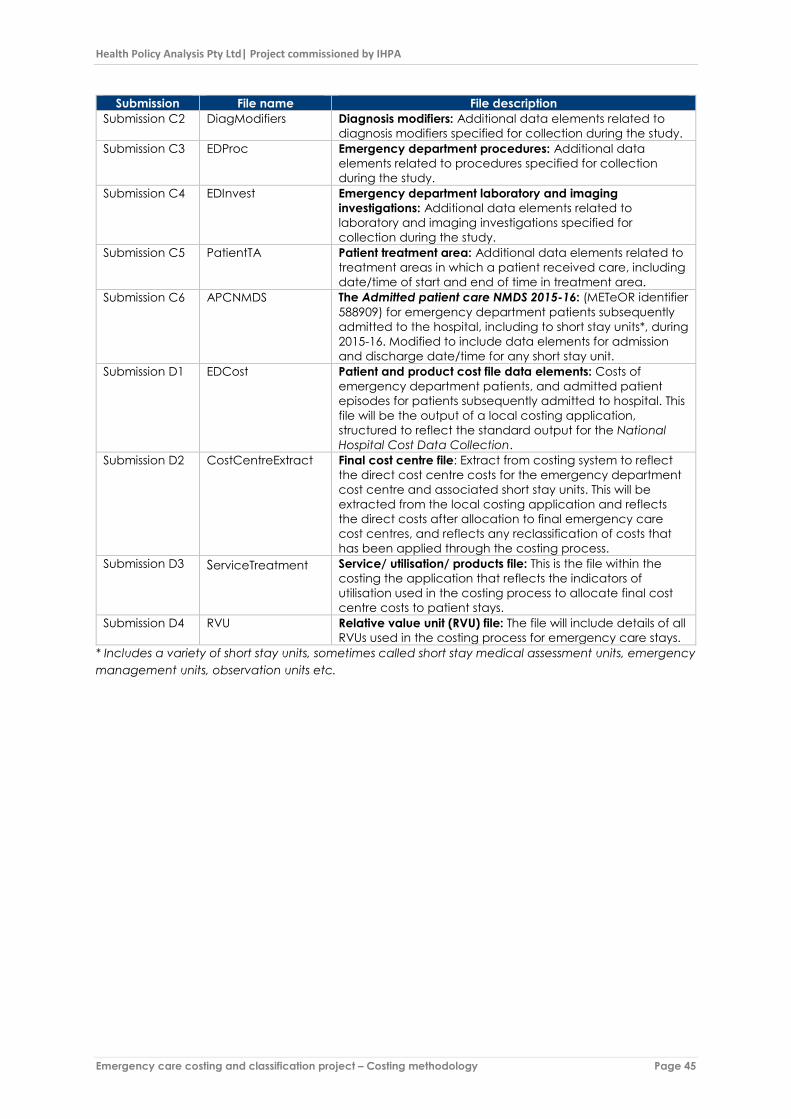
Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 45
Submission File name File description
Submission C2 DiagModifiers Diagnosis modifiers: Additional data elements related to
diagnosis modifiers specified for collection during the study.
Submission C3 EDProc Emergency department procedures: Additional data
elements related to procedures specified for collection
during the study.
Submission C4 EDInvest Emergency department laboratory and imaging
investigations: Additional data elements related to
laboratory and imaging investigations specified for
collection during the study.
Submission C5 PatientTA Patient treatment area: Additional data elements related to
treatment areas in which a patient received care, including
date/time of start and end of time in treatment area.
Submission C6 APCNMDS The Admitted patient care NMDS 2015-16: (METeOR identifier
588909) for emergency department patients subsequently
admitted to the hospital, including to short stay units*, during
2015-16. Modified to include data elements for admission
and discharge date/time for any short stay unit.
Submission D1 EDCost Patient and product cost file data elements: Costs of
emergency department patients, and admitted patient
episodes for patients subsequently admitted to hospital. This
file will be the output of a local costing application,
structured to reflect the standard output for the National
Hospital Cost Data Collection.
Submission D2 CostCentreExtract Final cost centre file: Extract from costing system to reflect
the direct cost centre costs for the emergency department
cost centre and associated short stay units. This will be
extracted from the local costing application and reflects
the direct costs after allocation to final emergency care
cost centres, and reflects any reclassification of costs that
has been applied through the costing process.
Submission D3 ServiceTreatment Service/ utilisation/ products file: This is the file within the
costing the application that reflects the indicators of
utilisation used in the costing process to allocate final cost
centre costs to patient stays.
Submission D4 RVU Relative value unit (RVU) file: The file will include details of all
RVUs used in the costing process for emergency care stays.
* Includes a variety of short stay units, sometimes called short stay medical assessment units, emergency
management units, observation units etc.

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 46
Appendix C – Cost data
submissions – data elements Table 18 – Submission D1 Patient and product cost file (EDCost) - data elements
Data element ID Data element name METeOR
identifier Type
estid Establishment—organisation identifier 269973 Char[9]
EDCostRowNo Table row identifier – patients and products n.a. Num
studyPersonID Person – Emergency department costing study
patient ID (encrypted ID)
n.a. Char[20]
studyStayID
Emergency department stay – Emergency
department costing study episode ID (encrypted
Episode ID)
n.a.
Char[20]
studyadmitepID Admitted patient episode ID (encrypted Episode
ID)
n.a. Char[20]
ProdType Product type n.a. Char[2]
StudyProduct Study product subtype n.a. Char[3]
ORP Order Request Point n.a. Char[9]
NhcdcCC NHCDC Final Cost Centre n.a. Char[15]
NhcdcItem NHCDC line item n.a. Char[15]
CostDir Direct cost n.a. Num[7]
CostOH Indirect cost n.a. Num[7]
TotalCost Total cost of episode n.a. Num[7]
The following items are maintained in the local study site management system, but not included in
the data submitted for the study:
hospPersonID Person—person identifier (local) 290046 Char[20]
hospEDstayID Emergency department stay identifier (local) n.a.
hospadmitepID Admitted patient episode identifier (local) n.a.
Note: The National Hospital Cost Data Collection involves reporting of cost data at the phase
level for admitted subacute patient care. Phase level reporting will not be required for this
study.
Table 19 – Submission D2 Final cost centre file (CostCentreExtract) – data elements
Data element ID Data element name METeOR identifier Type
estid Establishment—organisation identifier 269973 Char[9]
CCExtractRowNo Table row identifier – final cost centre extract n.a. Num
CCCode Cost Centre code n.a. Char[20]
CCName Cost Centre name n.a. Char[20]
ProdType Product type n.a. Char[2]
StudyProduct Study product subtype n.a. Char[3]
NhcdcCC NHCDC FINAL Cost Centre n.a. Char[15]
NhcdcItem NHCDC line item n.a. Char[15]
Amount Direct costs for this cost centre 2015-16 n.a. Num[9]
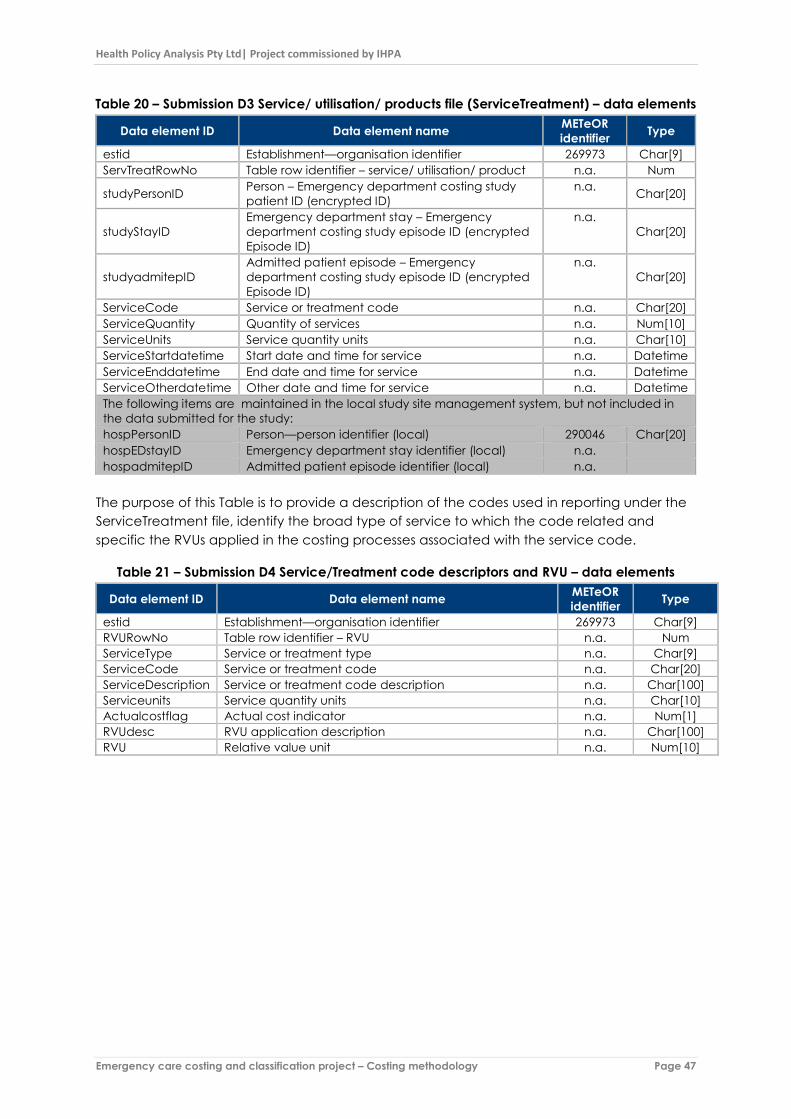
Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 47
Table 20 – Submission D3 Service/ utilisation/ products file (ServiceTreatment) – data elements
Data element ID Data element name METeOR
identifier Type
estid Establishment—organisation identifier 269973 Char[9]
ServTreatRowNo Table row identifier – service/ utilisation/ product n.a. Num
studyPersonID Person – Emergency department costing study
patient ID (encrypted ID)
n.a. Char[20]
studyStayID
Emergency department stay – Emergency
department costing study episode ID (encrypted
Episode ID)
n.a.
Char[20]
studyadmitepID
Admitted patient episode – Emergency
department costing study episode ID (encrypted
Episode ID)
n.a.
Char[20]
ServiceCode Service or treatment code n.a. Char[20]
ServiceQuantity Quantity of services n.a. Num[10]
ServiceUnits Service quantity units n.a. Char[10]
ServiceStartdatetime Start date and time for service n.a. Datetime
ServiceEnddatetime End date and time for service n.a. Datetime
ServiceOtherdatetime Other date and time for service n.a. Datetime
The following items are maintained in the local study site management system, but not included in
the data submitted for the study:
hospPersonID Person—person identifier (local) 290046 Char[20]
hospEDstayID Emergency department stay identifier (local) n.a.
hospadmitepID Admitted patient episode identifier (local) n.a.
The purpose of this Table is to provide a description of the codes used in reporting under the
ServiceTreatment file, identify the broad type of service to which the code related and
specific the RVUs applied in the costing processes associated with the service code.
Table 21 – Submission D4 Service/Treatment code descriptors and RVU – data elements
Data element ID Data element name METeOR
identifier Type
estid Establishment—organisation identifier 269973 Char[9]
RVURowNo Table row identifier – RVU n.a. Num
ServiceType Service or treatment type n.a. Char[9]
ServiceCode Service or treatment code n.a. Char[20]
ServiceDescription Service or treatment code description n.a. Char[100]
Serviceunits Service quantity units n.a. Char[10]
Actualcostflag Actual cost indicator n.a. Num[1]
RVUdesc RVU application description n.a. Char[100]
RVU Relative value unit n.a. Num[10]

Health Policy Analysis Pty Ltd| Project commissioned by IHPA
Emergency care costing and classification project – Costing methodology Page 48
References Independent Hospital Pricing Authority. (2014). Hospital Patient Costing Standards Version 3.1.
Sydney: IHPA. Available at:
http://www.ihpa.gov.au/internet/ihpa/publishing.nsf/content/Australia-Hospital-Patient-
Costing-Standards.htm
Independent Hospital Pricing Authority (2015). Three Year Data Plan 2015-16 to 2017-18.
Canberra: Sydney: IHPA. Available at:
http://ihpa.gov.au/internet/ihpa/publishing.nsf/Content/ihpa-three-year-
plan.html~appendix-A