Embed Size (px)
Citation preview

Prepared for the Health Statistics and Evaluation Branch and the State Tobacco Education and Prevention Partnership,
Colorado Department of Public Health and Environment
Community Epidemiology & Program Evaluation Group
Independent Evaluation:
Hospital systems change to improve inpatient tobacco dependence treatment
Final Results
June 2015

Prepared for Prepared for the Health Statistics and Evaluation Branch and the State Tobacco Education and Prevention Partnership,
Colorado Department of Public Health and Environment
Community Epidemiology & Program Evaluation Group
cepeg-ucdenver.org
Faculty and staff
Arnold H. Levinson, PhD MJ, Director Erin Martinez, MPH
Michele Kimminau, General Manager Carol-Ann Demaio Goheen, MSPH
Katherine James, PhD MSPH MSCE (School of Medicine)
Shannon Pray, MSPH
Whitney Jones, PhD MSPA Hillary Anderson, MPH
Yaqiang Li, PhD MPH Korrine J. Thomas, MPH
Kim McFann, PhD Alice Franco, MA
Sara L. Cooper, PhD MSPH Kathleen Moreira
Ming Ma, MD MPH Ali Billings
Patricia Alvarez Valverde, PhD MPH Vicki Weister
Kathleen Garrett, MA NCC MINT Erin McKay
Affiliates
Ashley Brooks-Russell, PHD MPH Adam Atherly, PhD
Yvonne Kellar-Guenther, PhD Eline Van Den Broek, PhD
William Betts, PhD Mark Gritz, PhD
Ernesto A. Moralez, MPH Tessa L. Crume, PhD MSPH
Edie Bridge Kristin Kidd, MA
The current report was prepared by Sara Cooper and Shannon Pray.
Disclosure: Arnold Levinson is Director of the University Health Smoking Cessation Service and provides scientific direction to the Colorado Model of Inpatient Tobacco Treatment (COMITT) program.

Prepared for Prepared for the Health Statistics and Evaluation Branch and the State Tobacco Education and Prevention Partnership,
Colorado Department of Public Health and Environment
Contents
Background………………….…………………………………………………………………………………………………………….1
Methods………………………………………………………………………………………………………………….…………………4
Results…………….….…………………………………………………………………………………………………..…………………9
Baseline Measures…………………………………………………………………………………….…………………..9
Adherence to OMSC and implementation challenges………………………………………………..….9
Reach and program uptake………………………………………………………………………………………….15
Tobacco cessation outcomes …………………………………………………………….………………………..19
Interactive Voice Response (IVR) follow-up………………………………………………………………….21
Conclusions……………………………………………………………………………………………………………………………..23
Appendices
Appendix A: Tobacco Treatment Specialist consultation tracking worksheet ………………………..24
Appendix B: Pre-implementation Key Informant Interview Guide …………………………………………26
Appendix C: Six-month follow-up survey (Version 1, Enrolled)……………………………………………….30

Page 1
Background
In November 2004, Colorado voters approved constitutional Amendment 35 (A35) to increase tobacco taxes by $0.64 per pack and use the revenue for health-related purposes. A portion of the revenue is distributed through competitive awards for programs to prevent and reduce tobacco use throughout the state. The awards are administered by the State Tobacco Education and Prevention Partnership (STEPP) upon approval by the Colorado Board of Health. As part of STEPP’s goal to help Colorado smokers quit, University of Colorado Hospital Authority (UCHA) and Penrose-St. Francis Health Services (PSF) each received a 33-month award, effective Oct. 1, 2012, to develop procedures for ensuring that every tobacco-using inpatient is identified and offered evidence-based tobacco cessation treatment. The grants were funded with state tobacco tax revenues administered by the Colorado Department of Public Health and Environment (CDPHE) and provide for phased program development across each hospital’s parent system (UCHealth and PSF), starting with University of Colorado Hospital (UCH) and Penrose Hospital (PH). The grant-funded programs are based on the Ottawa Model of Smoking Cessation (OMSC), adapted to operate within available resources and align with existing hospital policies and procedures. The OMSC uses evidence-based clinical protocols for the organized treatment of hospitalized smokers. The approaches help smoking patients manage withdrawal while in the hospital and support cessation attempts for patients interested in quitting. The principal goal is to reach large numbers of hospitalized smokers with best-practice tobacco dependence treatment, resulting in increased long-term cessation. The OMSC has three main components:
1. Identification and documentation: Ascertain smoking status of all patients at admission, and record the status on all registration forms, admitting orders, and health history documents.
2. Treatment: Offer counseling and pharmacotherapy to all tobacco-dependent patients, including users who have recently quit, are ready to try, or are not ready to try quitting.
3. Follow-up: Provide support after discharge via interactive voice response (IVR) or similar technology, and refer patients to specialists or other available cessation resources.
Before the grants began, UCH and PH had modest programs for inpatient smoking cessation. UCH’s year-old pilot program served inpatients that were referred by a hospital staff member and did not include routine orders for nicotine replacement therapy (NRT) for tobacco users while they were hospitalized. At PH, respiratory therapists delivered tobacco cessation education consultations to inpatient tobacco users; NRT was not a component of the program.

Page 2
The Community Epidemiology and Program Evaluation Group (CEPEG), University of Colorado Denver, was asked by CDPHE to conduct an independent evaluation of the two hospitals’ grant-funded initiatives. The evaluation addresses four questions:
How do UCH and PH identify tobacco-use status and treat inpatient tobacco users? How closely do the programs adhere to the OMSC; what explains departures from the
model, and what were challenges to model implementation? What are the new programs’ reach? To what extent do the new programs affect patients’ smoking behavior after discharge?
This final report describes the process of model adoption, characteristics of the hospitals’ inpatient smokers, treatment completeness under the new programs, and treatment outcomes. The economic assessment of program impact on hospital readmissions rates and length of stay authored by Eline van den Broek-Altenburg, Adam Atherley and Arnold Levinson is available as a separate, stand-alone report. Program Overview UCH’s Colorado Model of Inpatient Tobacco Treatment (COMITT) UCH change processes took about 10 months and new procedures began operating July 13, 2013. The Colorado Model of Inpatient Tobacco Treatment (COMITT) offers nicotine replacement therapy (NRT) in the hospital and free tobacco cessation consultation for active tobacco users admitted to any UCH department. COMITT also provides a free, two-week supply of NRT at discharge and six months of free follow-up counseling support for patients who choose to enroll. Follow-up counseling is offered by interactive voice response (IVR) telephone technology that includes (a) pre-recorded advice keyed to individual patient needs, (b) a warm-transfer option to speak with a live tobacco treatment specialist (during the first 18 months of program operations), and (c) collection of patient smoking and cessation treatment measures. In January, 2015, COMITT was incorporated into UCHealth’s permanent budget and became an in-house program. During this transition period, the warm-transfer option was discontinued. Instead, program enrollees seeking additional support are encouraged to leave a voicemail for a return call from a Tobacco Treatment Specialist (TTS). COMITT was launched at affiliate hospitals in the UCHealth system beginning in February, 2015, and preliminary enrollment data from Memorial Hospital are included in this evaluation.

Page 3
Penrose-St Francis Tobacco Cessation Program (PSF-TCP) PSF launched its inpatient smoking cessation program at Penrose Hospital on October 28, 2013. The PSF Tobacco Cessation Program (PSF-TCP) provides free tobacco cessation counseling for active tobacco users admitted to the hospital. At the tobacco treatment specialist’s discretion and with a doctor’s consent, NRT is offered to patients during their hospital stay. Patients interested in quitting tobacco can enroll in a follow-up counseling program and receive a discount voucher for a two-week supply of NRT at discharge. Smokers discharged before being seen by a PSF-TCP counselor receive a post-discharge telephone call to offer program enrollment. Follow-up counseling is delivered through IVR and includes pre-recorded advice keyed to individual needs, and collection of patient smoking and cessation treatment measures. PH uses a separate IVR vendor from COMITT and the PSF_TCP IVR calls do not include a warm-transfer option to speak with a live tobacco treatment specialist. IVR follow-up was initiated approximately six months after program launch; before IVR launch, the PST-TCP program manager conducted follow-up calls by telephone. Program managers anticipate expanding the PSF-TCP to St. Francis Hospital during 2015.

Page 4
Methods Summary For the purposes of this evaluation, data were collected from a variety of sources to compare and contrast program integration, assess program reach, and evaluate program impact on tobacco-related behaviors. Data sources include primary data collection (baseline assessment, six-month follow-up survey, and tobacco treatment specialist (TTS) tracking worksheet), key informant interviews, and secondary data collection (electronic health records and other program management software, and program-specific tracking databases). Detail on specific evaluation and data collection methods is provided below. Establishing baseline data At UCH, smoking prevalence and cessation rates were collected during fiscal year 2012-13, before any systems changes had occurred, to determine baseline tobacco dependence treatment practices. The primary measures, (a) pre-program accuracy of smoking status data in UCH’s electronic health records (EHR; Epic Systems Corp., Verona, WI), and (b) the “natural” pre-program smoking cessation rate among smoker inpatients, were measured by interviewing a random sample (n=819) of UCH inpatients who had been admitted during fiscal year 2012-2013, before COMITT was launched. Baseline data for PSF-TCP were unavailable. OMSC adoption process evaluation System change data were obtained through interviews with key informants at each site (n=5 at UCH and n=7 at Penrose). Interview topics included challenges in developing and launching the programs; how and why programs differed from the OMSC, and recommendations for future implementation of similar programs. Informants included program managers, and high-level hospital administrators. The interview guide (Appendix B) was designed to encourage open-ended discussion about the topics that were most relevant to the interviewee’s direct experience with program adoption. Interviews were audio-recorded and transcribed, and interviewer field notes were integrated with the transcripts to provide additional context. Transcripts were analyzed in MS-Word and Atlas TI to facilitate coding, text retrieval, data management and content analysis. The lead analyst coded the transcripts using Pattern, Theme and Content Analysis1 with the interview guide as an organizing structure. Two other analysts independently applied the initial code list and generated additional codes as needed. Inter-rater reliability was good (Fleiss' Κ=0.79), and coding differences were resolved through discussion. The three analysts
1 Patton ML. Qualitative Research and Evaluation Methods, 3rd Edition. Sage Publications, February 1990.

Page 5
then independently aggregated codes into emergent themes, and results were compared and reconciled by discussion among the analysts. During the evaluation period, additional key informant interviews were conducted with tobacco treatment specialists and program managers to identify emergent challenges and adaptations as the COMITT and PSF_TCP programs evolved, and to monitor the progress of program expansion to hospital affiliates. Program reach and implementation COMITT Initial program reach and accuracy of post-change smoking status were assess using extracted EHR data for all UCH inpatients admitted during program operations from July, 2013 - March, 2014. Measures included demographic information (age, gender, race/ ethnicity), smoking-related items (current status, packs per day), and program-related measures (admitting department, whether best-practices advisory was triggered to order tobacco treatment consultation, NRT approved by physician). As a result of CEPEG concerns over data quality issues related to IVR services (which are described in more detail in the Methods: Treatment outcomes section of this report), COMITT contracted with a new IVR system vendor in October, 2014 (TelASK Quit Manager, www.telask.com). The IVR software includes a program management component and is fully integrated into all aspects of program operations: it identifies inpatient smokers and refers them to the COMITT program for consultation; it collects patient demographics, tobacco use and program operations data (i.e., consultation fulfillment), and manages the IVR process including treatment and tobacco cessation outcomes. Data were extracted from the Quit Manager system for October, 2014 - March, 2015. Prior to launch of the Quit Manager system, COMITT did not track consultation fulfillment. In addition, despite several modifications to support COMITT operations, the EHR system was not designed to capture program-level data. Key components of program implementation such as Tobacco Treatment Specialists’ (TTS) interactions with enrollees, inpatients’ use of NRT in the hospital, or reasons for non-enrollment in the follow-up program were not systematically collected by program staff. To study these, evaluators and program staff collaboratively created a consultation tracking worksheet (Appendix A). These worksheets were used to provide evaluators with a “snapshot” of program operations: they would track consultation fulfillment, inpatient NRT use, and patient interactions. The form was implemented during six randomly selected weeks in February- April, 2014, which included 35 days when consults were made.

Page 6
Currently the TelASK Quit Manager software routinely tracks many of these program components. PSF-TCP At PH, program staff tracks program reach, implementation metrics, and IVR outcomes data in a stand-alone excel database. Continuous program data were provided by the PSF-TCP program coordinator for program operations during the evaluation period (October 28, 2013 – March 31, 2015). Measures included demographic characteristics of inpatient smokers, delivery mode of tobacco consultation, and certain program-related measures such as IVR follow-up and tobacco cessation outcomes. Measures requested by evaluators but unavailable from the hospital include overall inpatient characteristics, smoking consumption levels (i.e., packs-per-day), and the pre-program quit rate. Treatment outcomes Although COMITT and PSF-TCP use different IVR vendors, the systems used in both programs provide similar post-discharge follow-up support, and collect tobacco use and cessation data. The systems represent substantial departures from both pre-existing tobacco treatment programs: before grant-funded systems changes, UCH tobacco treatment specialists provided live follow-up counseling by telephone, while Penrose hospital provided no follow-up. CEPEG evaluators audited the initial phase of the IVR fulfillment process at UCH and found substantial data management and quality issues. After the issues were reportedly addressed, a second audit found continuing concerns with data quality and management. Ultimately, evaluators were unable to determine:
whether the IVR system made all prescribed calls; whether the correct enrollees were contacted at the prescribed time periods; whether the IVR system used the appropriate questionnaire at each time period; whether the IVR system accepted and recorded all enrollee responses.
As a result of these limitations, CEPEG did not analyze UCH IVR data during the initial evaluation period. Although PH contracted with a separate IVR vendor, initial analysis of PSF_TCP IVR data collected during this same period revealed a response rate below 10% at six months post-discharge. Evaluators determined that additional data collection was necessary for both COMITT and PSF-TCP to capture tobacco treatment outcomes; these data would supplement or replace the IVR

Page 7
response data. A six-month follow-up multi-modal survey was designed and implemented beginning in April, 2014 to capture the six-month abstinence rate and the seven-day point prevalence abstinence rate at six months post-discharge. Evaluators were also able to compare the effectiveness of the inpatient tobacco treatment consultation plus six-months of IVR follow-up support to consultation alone. In advance of instrument development, a detailed survey administration protocol was written outlining patient outreach and data management policies and procedures, and appropriate IRB protocols were followed. Evaluators contacted Colorado Multiple Institutions Review Board (COMIRB) to determine the level of review necessary to implement the six-month follow-up survey. COMIRB informed evaluators via telephone conversation that no review was necessary because the primary purpose of the survey was program evaluation and the secondary purpose was participant satisfaction, both of which are exempt activities. COMITT and PSF-TCP staff then provided CEPEG with: 1) contact information for all program enrollees; and 2) an equal number of randomly selected inpatient smokers who received a consultation but did not enroll in the program. Survey topics for all respondents included tobacco use, quit attempts, use of NRT or other quit strategies, and acceptance of the program. For enrollees, the survey was expanded to include additional topics which focused on participants’ level of satisfaction with the IVR support, and extent of program engagement (Appendix C). Reliability testing for the survey instruments was high using both test-retest and alternate form reliability assessment methods (r=0.82).2 Survey participants received a postcard notification approximately six months after discharge, and the written survey instrument along with cash incentive one week later. Non-responders received a second survey two weeks after the initial mailing, and then were transferred to the CEPEG call-center for additional telephone follow-up. A maximum of seven call attempts were made to non-responders before the contact was retired. Telephone responders received an additional cash incentive for completing the survey. COMITT surveys were hand-entered into the survey database using double-data-entry techniques to maintain data integrity. The PSF-TCP survey used Scantron technology (standardized assessment forms; Scantron, Eagan, MN); paper surveys were scanned by CEPEG staff into the survey database. Telephone responses were entered directly into the database during the interview. A 5% quality check was performed on the Scantron surveys to assess bubble completeness and a 10% quality check was performed on the final dataset prior to analysis.
2Litwin, Mark. How to Measure Survey Reliability and Validity. Sage Publications. 1995.

Page 8
COMITT IVR data collected since October, 2014 were extracted from the TelASK Quit Manager system and analyzed to determine IVR acceptance and tobacco abstinence rates at selected time-points during the follow-up period. PSF-TCP IVR data were aggregated across the evaluation period for analysis. Analysis Standard descriptive statistics (frequencies, means, proportions, t-tests and chi-squared tests) were used to estimate program reach and impact, and to determine significant differences between groups. Comparisons between programs are provided where possible.

Page 9
Results Baseline Measures Among pre-program UCH inpatients contacted six months after discharge, 94% of respondents confirmed the accuracy of the hospital’s smoking status at admission. During the follow-up interview, about one in five smokers-at-admission (21%) reported that they had not smoked during the previous seven days. Evaluators used this rate to represent the “natural” (pre-COMITT) cessation rate among UCH in patients after hospital discharge and compared it to corresponding measures during COMITT operation. PH did not provide data on the accuracy of smoking status recorded at admission or the natural (pre-program) quit rate after discharge. Program Adoption and Adaptation Processes Adherence to OMSC and implementation challenges Both COMITT and PSF-TCP reflect all major OMSC components. The following adaptations were made to align the program with existing hospital systems:
Two OMSC pharmacotherapy cessation options included in the OMSC (bupropion and varenicline) are not offered by COMITT or PSF-TCP; patients who are taking one of these drugs at admission are able to continue taking them while in the hospital.
COMITT established standard orders for a tobacco cessation consultation and NRT for all admitted current smokers in compliance with OSMC guidelines. PSF-TCP does not routinely provide inpatient NRT.
COMITT and PSF-TCP provide participants with a two-week supply of NRT at discharge; OMSC does not.
OSMC offers treatment to recent former smokers; neither COMITT nor PSF-TCP includes former smokers.
COMITT sends reminder postcards to program participants in advance of telephone calls; OMSC does not.
PSF-TCP manager described the pursuit of OMSC adherence this way:
“We started off wanting to stay very, very close to [the OMSC]. But, as we got up on the floors and talked to the respiratory therapists and the nursing staff, it became apparent that we were going to have to work within some systems that were already there. In order to get buy-in, we traded off a little bit. [Many mechanisms] already existed [that were] slightly different that the way Ottawa Model wants… but it works.”
Page 10
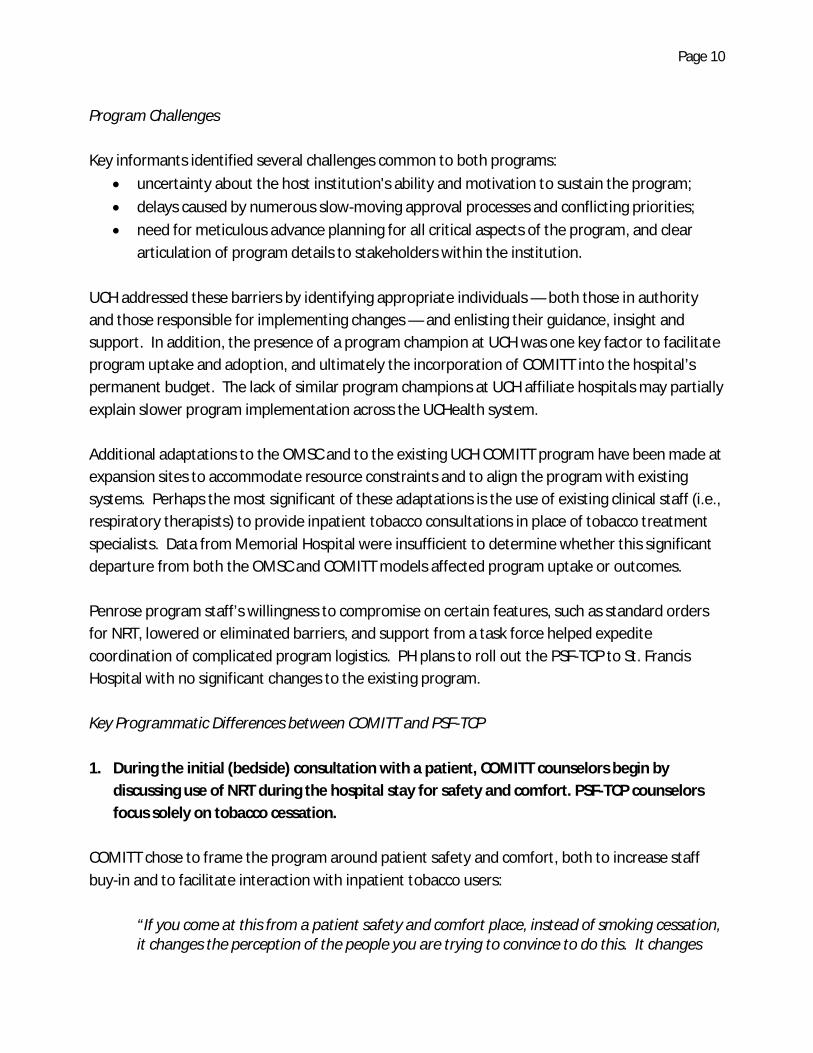
Program Challenges Key informants identified several challenges common to both programs:
uncertainty about the host institution's ability and motivation to sustain the program; delays caused by numerous slow-moving approval processes and conflicting priorities; need for meticulous advance planning for all critical aspects of the program, and clear
articulation of program details to stakeholders within the institution. UCH addressed these barriers by identifying appropriate individuals — both those in authority and those responsible for implementing changes — and enlisting their guidance, insight and support. In addition, the presence of a program champion at UCH was one key factor to facilitate program uptake and adoption, and ultimately the incorporation of COMITT into the hospital’s permanent budget. The lack of similar program champions at UCH affiliate hospitals may partially explain slower program implementation across the UCHealth system. Additional adaptations to the OMSC and to the existing UCH COMITT program have been made at expansion sites to accommodate resource constraints and to align the program with existing systems. Perhaps the most significant of these adaptations is the use of existing clinical staff (i.e., respiratory therapists) to provide inpatient tobacco consultations in place of tobacco treatment specialists. Data from Memorial Hospital were insufficient to determine whether this significant departure from both the OMSC and COMITT models affected program uptake or outcomes. Penrose program staff’s willingness to compromise on certain features, such as standard orders for NRT, lowered or eliminated barriers, and support from a task force helped expedite coordination of complicated program logistics. PH plans to roll out the PSF-TCP to St. Francis Hospital with no significant changes to the existing program. Key Programmatic Differences between COMITT and PSF-TCP 1. During the initial (bedside) consultation with a patient, COMITT counselors begin by
discussing use of NRT during the hospital stay for safety and comfort. PSF-TCP counselors focus solely on tobacco cessation.
COMITT chose to frame the program around patient safety and comfort, both to increase staff buy-in and to facilitate interaction with inpatient tobacco users:
“If you come at this from a patient safety and comfort place, instead of smoking cessation, it changes the perception of the people you are trying to convince to do this. It changes

Page 11
the argument. If you tell a nurse who smokes, ‘We’re coming in and we’re going to tell people to quit smoking,’ they aren’t on board. But, if you say, ‘This is about the patient and their safety and comfort, and gosh, isn’t he grouchy?’ it’s a totally different conversation.” (COMITT Manager)
PH interviewees uniformly agreed that the purpose of the PSF-TCP is to increase tobacco quit rates among inpatients. There was no discussion of patient comfort or withdrawal symptom management as a component of the program. When asked about providing NRT so inpatients are more comfortable during their hospital stay, the program manager said, “You know, I really don’t even know about that.” 2. COMITT created standard orders for NRT and tobacco cessation consultation, and
integrated them into the EHR system. COMITT’s integration into routine patient care involved substantial institutional changes. Perhaps the most critical change involved the EHR. The system was modified using a best practices advisory (BPA) to alert every provider viewing a tobacco user's medical record that orders are recommended for a consult with a Tobacco Treatment Specialist and a prescription for inpatient NRT. In October 2014, COMITT program management launched integrated operations management and IVR software (TelASK Quit Manager, www.telask.com). Implementation of this new data management system changed the way inpatient smokers were identified and referred to COMITT for consultation, bypassing the BPA built into the EHR. Consult orders no longer rely on physician approval, instead they are triggered automatically by the quit manager system. NRT orders still rely on the BPA for physician approval and its administration is not tracked in the new program management system. PSF-TCP does not make the provision of inpatient NRT to all current smokers a part of routine care. NRT may be preordered by the admitting physician, requested by the patient, or recommended by the tobacco treatment specialist. The manager said that NRT is offered:
“Where appropriate… part of [the] intervention [is] really evaluating how ready [patients] are to quit. I think [the tobacco treatment specialist is] being very judicious with when it is offered. It’s not just offered to everybody. I think when it’s appropriate and when [the specialist] feels like it’s really going to help that person and that they’re serious about quitting, I think [the specialist] will continue to consistently offer it.”
As part of the Centura Health national healthcare system, PH was not able to implement standard orders for tobacco cessation consults or NRT, nor was it able to change its EHR system (Meditech,

Page 12
Westwood, MA). Instead, the program relies on existing reporting systems: current smokers are identified at admissions, and an automated report is sent to respiratory therapy where it is picked up by the PSF-TCP counselor. The program developed an Excel database and paper-based tracking tools to monitor reach, implementation, and tobacco related health and behavior outcomes. Figures 1 and 2 illustrate COMITT and PSF-TCP program operations. Figure 1: UCH COMITT Program Diagram

Page 13
Figure 2: PSF-TCP Program Diagram
3. UCH supports a larger staff of tobacco treatment specialists (TTSs).
During the first 18 months of program operations, COMITT staffing was sufficient to provide consistent bedside consults six days per week throughout the year (patients admitted on Saturday evening or Sunday typically receive TTS consultations Monday morning). COMITT consultations typically follow a similar format and include standardized content so that all inpatients receive a consistent intervention. COMITT staffing was also sufficient to provide “warm transfers,” from the IVR system to a live tobacco treatment counselor during post-discharge follow-up calls. Since its inception, PSF-TCP supports a single tobacco treatment specialist at Penrose Hospital. Respiratory Therapists provide tobacco cessation education during weekends and when the TTS is unavailable. PH patients admitted after hours or over the weekend received tobacco education from respiratory therapy and ideally, either an in-person or telephone consultation from the TTS. The program manager said, “On the weekends, the respiratory therapists are doing the intervention, [but] it’s not really a full intervention because [the respiratory therapists] have other things they have to do. They are providing some patient education on the weekends.” PSF-TCP does not offer a warm-transfer option during follow-up IVR counseling. Participants who want to speak with a counselor are encouraged to call the QuitLine or to leave a message with

Page 14
the program office for a call back from the TTS. Evaluators worked with the PSF-TCS Program Manager to track the specific intervention components each patient received to determine whether these differences in program delivery affected subsequent tobacco use. In January 2015, COMITT became a UCHealth System-funded program. Current funding supports TTS staff five days per week at UCH instead of six days. Patients admitted after Friday afternoon and during the weekend receive TTS consultations on Monday morning or a follow-up telephone consultation if they have been discharged. Program leadership is working to secure additional funding from UCHealth System to provide weekend coverage again. In addition, the warm transfer option is no longer available. Instead participants seeking additional support are encouraged to contact the QuitLine or leave a message for a call back from the TTS. 4. Penrose program leadership established a task force to support program development and
decision-making. The PSF-TCP task force is composed of hospital leadership from key departments and represents a variety of specialties committed to supporting the tobacco cessation program. The task force was initially convened to establish a broad base of support within PH and to help identify critical changes needed to implement the program. It continued to meet regularly to evaluate program reach and implementation and review emergent issues. COMITT program leaders acknowledge that the lack of an oversight body was a weakness in program development and implementation. 5. COMITT provides a prescription voucher at discharge for one free two-week supply of NRT
to all patients enrolled in the six-month follow-up counseling program. PSF-TCP provides NRT with a small copay at discharge.
The PSF-TCP chooses to charge program participants for NRT on the basis that participants who pay for NRT are more likely to be committed to their quit attempt.
“The reason we have a co-pay is we wanted to offer the product to the patients at a very economical price. We did not want word to get out that we were just giving away nicotine replacement items for free. We wanted a little skin in the game from patients.”
About twice as many COMITT enrollees as PSF-TCP enrollees fill their NRT prescriptions at discharge (61% vs. 36%). Nevertheless, the PH manager expressed surprise at the fulfillment volume, saying “We’re seeing very quickly [that NRT] is going to be a much larger percentage of the budget than we had originally planned on. [Patients] are actually picking up [the NRT] on their way out the door. We’re surprised at the level of pick-ups.”

Page 15
6. The two programs collect different data. Programmatic differences and barriers to obtaining certain inpatient data account for the differences in data collection. For example, the PSF-TCP began tracking the number of times inpatient NRT is prescribed in response to an evaluation inquiry, while PSF-TCP routinely collects consultation fulfillment and program follow-up data but COMITT does not. The current report compares program reach and specific outcomes between sites where possible, however evaluators were only somewhat successful in working with each program to standardize data collection measures and methods. Reach and treatment uptake: COMITT During the first nine months of program operations, UCH admitted 13,567 patients, of whom 95% had a smoking status entered in their EHR. A total of 2,289 inpatients (18%) were current smokers, with a higher rate among male inpatients (23%). More than half of current smokers were admitted to any of five hospital departments: medical specialties (12%), progressive care (10%), neurosciences (10%), oncology (10%) or pulmonary (8%). Former smokers were significantly older than inpatients with other smoking statuses.
Orders for bedside tobacco consultation were entered for nearly three-fourths (73.7%) of inpatient current smokers. Consult orders were more common among women and non-Hispanic whites. During the evaluation process, program staff and evaluators jointly identified an EHR system glitch that kept some inpatient smokers from having tobacco consults automatically ordered. The problem involved response options in the “packs-per-day” field: only a few drop-down menu options were triggering as intended. The problem was resolved in January 2014 but the automatic order rate did not improve during the following two months. Since October, 2014, 12,244 patients were admitted to UCH. The quit manager system identified 1,181 (10%) inpatients as active current smokers and referred them to the TTS. The number of inpatient smokers identified through the Quit Manager program is lower than those identified through the EHR system. One reason may be that Quit Manger uses a different methodology to identify current active smokers than Epic. The software uses a proprietary algorithm to triangulate smoking data based on admissions records downloaded from the EHR system three times per day. This process allows the software to compile “a more accurate real-time list of active current smokers (presumably) reducing the number of ‘wasted’ consult attempts with patients who are ineligible, have already quit, or never smoked.”3
3 Telephone conversations with Vince Talbot, UCH Account Manager for TelASK, TelASK Systems, Ottowa Canada; February, 2015 with follow-up conversations in March, April and May, 2015.)

Page 16
Of the 1,181 active smokers, 802 confirmed that they had used tobacco in the past 30 days and were eligible for a consult. Eligible inpatient smokers were likely to be male (55%) between the ages of 55 and 64; 88% consented to the consult. During this period, consults were completed with 92.5% (n=652) of the eligible inpatient smokers who consented to participate. Almost half of these inpatients (47.6%) indicated they were in either the “pre-contemplation” or “contemplation” stages of readiness to quit tobacco. 38% (n=261) felt they were “ready to quit” tobacco, and over 40% (n=281) said that they had the highest level of confidence in their ability to do so. Almost one-third (27%) of inpatients who received a consult reported smoking at least one pack of cigarettes per day. During the initial nine-month evaluation period, inpatient NRT was ordered for 39% of current smokers, more commonly among older smokers and men. The NRT ordering level remained relatively constant during that period. Among the 61% of cases where NRT was not ordered, no reason was given in four out of five instances. The NRT order rate may indicate a need for provider education. Nearly one-third of inpatient current smokers (32.5%) had orders for both bedside cessation consultation and NRT. No data are available through the Quit Manger program on inpatient NRT use. The observed rates of both consult and NRT orders established during the initial nine-month evaluation period are consistent with those seen at other OMSC sites,4 although COMITT staff believe the inpatient NRT order rate (39%) leaves a majority of inpatient smokers uncomfortable while hospitalized and without proper medical management of nicotine withdrawal. COMITT staff is considering other ways to work with physicians to increase the NRT prescription rate. One TTS noted that “It seems like as the floor staff—the nurses and the docs— get used to seeing us, they remember the program and they think about NRT for their patients who are smokers. It feels like it comes up a little bit more than it used to.” COMITT tobacco treatment specialists received referrals for approximately six consults per day during the first nine months of program operations. An average of 17.8% of inpatient smokers – 24% of those with tobacco-consult orders – enrolled in the cessation treatment program, with no significant change over that period. Since October, 2014, 21.3% of inpatient smokers –38.7% of those who received a consult – enrolled in the follow-up. In the past five months, 88% of inpatients who enrolled in the follow-up program received a voucher for a single two-week supply of NRT to be filled at discharge. No data were available on
4 Reid RD, Mullen K-A, Slovinec ME et al. Smoking Cessation for Hospitalized Smokers: An Evaluation of the “Ottawa
Model.” Nicotine & Tobacco Research 2010; 12(1): 11-18.

Page 17
the number of prescriptions filled since October, 2014, but, 61% of NRT vouchers were filled at discharge during the first nine months of program operations. COMITT Consultation Tracking Worksheet The consultation tracking worksheet was implemented at the tail end of the initial nine-month evaluation period (February, 2014- April, 2104) to provide supplemental program data on activities not otherwise measured during this phase. The worksheets were used to track consultations for 229 current smokers (~6 per day) eligible for tobacco cessation consultation and NRT; 90% of those eligible (n=198) received consultations. The results discussed here are based on this subset of inpatients identified through the TTS worksheet. It took an average of two attempts per patient to conclude a consult. Among patients receiving a consult, 95% were receptive to discussing NRT patches and their level of comfort level during their hospital stay, and 88% were receptive to a discussion about quitting tobacco. Ten patients receiving a consult had quit tobacco use prior to hospital admission. Three patients declined a consult. The tracking data show that more than half (55%) of patients received an NRT patch prior to the COMITT consult, 14% of patients were not offered NRT, and 31% declined offers of NRT while hospitalized. 13% of inpatients not patched at the consult requested NRT after their consult. The observed patch rate is higher than might be expected given an overall NRT order rate of 39% and could indicate that physicians who order bedside tobacco treatment consultations may be more likely to order NRT. Patients who were patched before the consult were more than four times as likely to enroll in the tobacco treatment program as those who weren’t patched. This association may indicate that inpatients who are predisposed toward quitting tobacco ask for or accept NRT before they have any program contact, or, alternatively, that in-hospital experience with NRT tends to motivate inpatients toward quitting. The consult tracking form also showed that 64 patients (36%) who received a consult subsequently enrolled in the program, 62 (31%) were not ready to make a quit attempt, 24 (12%) said they could quit on their own, and 17 (8%) adopted harm reduction strategies such as smoking less, only smoking outside, or not relighting cigarettes. Five percent of patients were ineligible for the program.

Page 18
Reach and treatment uptake: PSF-TCP PH provided data about all current smokers (n=2,881) identified from the EHR between October 28, 2013 and April 30, 2015. PH inpatient smokers were more often male (58.0%), non-Hispanic white (78.7%) with an average age of 53 years. Smoking prevalence among PH inpatients was not provided, and data were not provided to assess accuracy and completeness of smoking status ascertainment. PSF-TCP consults are conducted in-person by the TTS during the work-week (Monday-Friday). Patients admitted on a weekend receive a brief educational consult with a respiratory therapist, and a follow-up TTS consult the following week either in person if the patient is still in the hospital or over the phone if the patient has been discharged. Of the 2,881 smokers admitted to Penrose, 90% received a tobacco cessation consultation. This rate has been consistent across the evaluation period with little variation. Among patients admitted on a weekend (n=177), 163 (92.1%) received a follow-up consult with the TTS, while 14 received only the educational consult with a respiratory therapist; TTS follow-up for these patients was not completed because they had been discharged and were unavailable by telephone. The average consult lasted 10 minutes. About three-quarters of PH inpatient smokers identified in the EHR were admitted to any of four hospital departments: Cardiovascular Unit (26.7%), Medical/Renal/Diabetic (17.6%), Medical/Surgery/TB/Ventilators (15.8%), and Observation Unit (14.4%). As of April, 2014, Penrose began tracking number of smokers offered NRT during their hospital stay. Based on available data, 51% of admitted smokers were offered NRT, of whom over one-third accepted the prescription (37%) and half declined (52%); approximately 11% were contraindicated for NRT. Current data revealed no differences in patient demographic characteristics between those offered NRT and those who were not, or between those who accepted versus those who refused NRT while in hospital. More than one-fourth (27.2%) of PH inpatient smokers enrolled in the follow-up program. Almost 95% of PH enrollees reported they were in the “action” stage of readiness to quit tobacco. In contrast, only one-third of non-enrollees were in the “action” stage. Instead, 53% reported they were in either the “pre-contemplation” or “contemplation stage.” Of those inpatients that enrolled in the follow-up program, 58% received a voucher for a single discounted two-week supple of NRT and 36% filled the prescription at discharge.

Page 19
Reach and treatment uptake: UC Health expansion sites Preliminary data were available through the TelASK Quit Manager software to evaluate program reach at one expansion site: Memorial Hospital (MH). Since October, 2014, 101 inpatient smokers were identified at MH. Inpatients smokers were predominantly female (n=55) between the ages of 50-64 years, and smoked a half pack of cigarettes per day on average. 86% consented to a tobacco consultation (n=87). Of those who received a consult, 39% believed they were in the “pre-contemplation” or “contemplation” stage of readiness to quit tobacco, while less than one third were in action “action” stage (27%). Inpatient smokers were about evenly split between low confidence and high confidence in their ability to quit tobacco (46% “low” or “very low” confidence vs. 45% “high” or “very high” confidence). Almost 40% of inpatient smokers enrolled in the follow-up program after consult at MH (n=34). No additional data were available for this site. Tobacco cessation outcomes Six-month follow-up survey: Response Rates The overall response rates for the six-month follow-up survey were 74.6% for UCH (n=535) and 28.3% for PH (n=160) across all survey waves. In general, respondents who enrolled in the follow-up were less likely to respond to the survey compared to non-enrollees, although this difference was not significant at either hospital. Almost 80% of PH respondents returned the paper survey, while UCH respondents were more likely to respond to the telephone survey (59%). At both sites, respondents had similar distributions of key demographic characteristics in the enrolled versus non-enrolled groups. Six-month follow-up survey: COMITT tobacco cessation outcomes and participant satisfaction Seven-day point prevalence abstinence at six-month post-discharge for respondents enrolled in the UCH follow-up program was 35.8% compared to 29.2% for non-enrolled, and 21% pre-program or “natural” 7-day abstinence rate at baseline. 22% of program enrollees reported remaining tobacco free six months after hospital discharge compared to 16% of non-enrollees. Three out of four enrollees (75.3%) reported at least one quit attempt during the previous six months and 68% reported using some form of NRT to help them quit tobacco. 57% of non-enrollees also reported at least one quit attempt, but fewer than 20% reported using NRT during their quit.

Page 20
Enrollees at UCH were almost two and a half times more likely to report that the TTS consultation made them more interested in quitting tobacco compared to non-enrollees (72.0% versus 29.0%). About 45% of non-enrollees did not recall meeting with a TTS during their hospital stay compared to less than 4% of enrollees (3.85%). Over 60% of respondents enrolled in the follow-up recalled using NRT during their hospital stay, two out of three who reported using NRT in the hospital believed it made them feel more comfortable during their stay. Overall, COMITT respondents who enrolled in the follow-up program were ambivalent about the support provided by the IVR, but two-thirds (65.0%) did respond to at least one IVR call, and over half stated that the IVR system provided the “right number of calls.” In general, enrollees at UCH were not interested in more free or discounted NRT after discharge or in receiving live support calls from a person instead of IVR. Six-month follow-up survey: PSF-TCP tobacco cessation outcomes and participant satisfaction Seven-day point prevalence abstinence at six-months post-discharge for PH respondents enrolled in the follow-up program was 39.4% compared to 27.6% for non-enrolled. The baseline quit rate was not available at PH. 30% of program enrollees and 27% of non-enrollees reported remaining tobacco free six months after hospital discharge. About three-quarters of enrollees (72.2%) reported at least one quit attempt during the previous six months and 51% reported using some form of NRT to help them quit tobacco. 53% of non-enrollees also reported at least one quit attempt, but only 22% reported using NRT during their quit. Almost half (48%) of all respondents said that the TTS consultation made them more interested in quitting tobacco (60% enrollees vs. 30% non-enrollees), but almost two-thirds did not think the consultation had any effect on their level of comfort during their hospital stay (50% enrollees vs. 77% non-enrollees). 37% of non-enrollees and 13 % of enrollees did not recall meeting with a TTS in the hospital. About half of all survey respondents who recalled using NRT in the hospital believed it made them feel more comfortable (54.1% of enrollees and 47.1% of non-enrollees), and 35.6% of enrollees who received a prescription for NRT at discharge filled it. These data are consistent with PH program data from other sources. PH respondents enrolled in the follow-up program were also ambivalent about the IVR support: 38.4% believed the calls were either “somewhat” or “very helpful,” while 37.0% believed they were “not very helpful.” In general, enrollees at PH were interested in getting access to more discounted NRT after discharge (30.4%), referral to an outpatient support group (28.3%), and a least one live call during the follow-up period from a person in addition to the IVR (23.9%).
Page 21
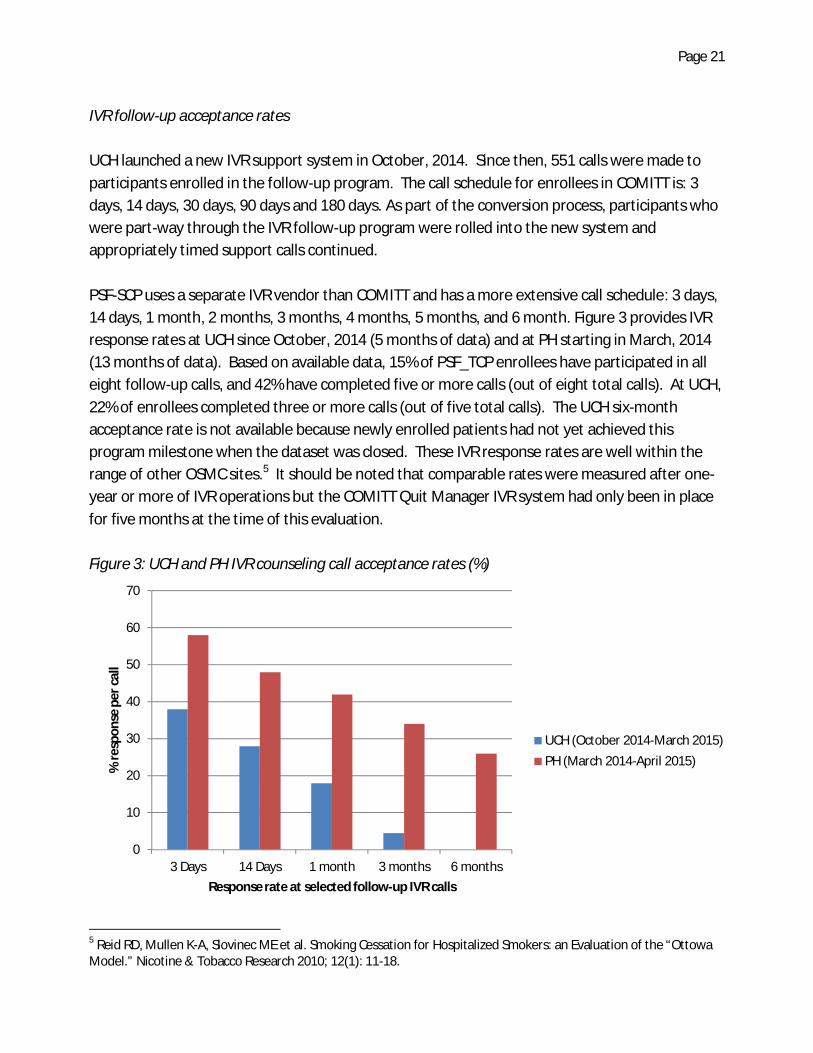
IVR follow-up acceptance rates UCH launched a new IVR support system in October, 2014. Since then, 551 calls were made to participants enrolled in the follow-up program. The call schedule for enrollees in COMITT is: 3 days, 14 days, 30 days, 90 days and 180 days. As part of the conversion process, participants who were part-way through the IVR follow-up program were rolled into the new system and appropriately timed support calls continued. PSF-SCP uses a separate IVR vendor than COMITT and has a more extensive call schedule: 3 days, 14 days, 1 month, 2 months, 3 months, 4 months, 5 months, and 6 month. Figure 3 provides IVR response rates at UCH since October, 2014 (5 months of data) and at PH starting in March, 2014 (13 months of data). Based on available data, 15% of PSF_TCP enrollees have participated in all eight follow-up calls, and 42% have completed five or more calls (out of eight total calls). At UCH, 22% of enrollees completed three or more calls (out of five total calls). The UCH six-month acceptance rate is not available because newly enrolled patients had not yet achieved this program milestone when the dataset was closed. These IVR response rates are well within the range of other OSMC sites.5 It should be noted that comparable rates were measured after one-year or more of IVR operations but the COMITT Quit Manager IVR system had only been in place for five months at the time of this evaluation. Figure 3: UCH and PH IVR counseling call acceptance rates (%)
5 Reid RD, Mullen K-A, Slovinec ME et al. Smoking Cessation for Hospitalized Smokers: an Evaluation of the “Ottowa Model.” Nicotine & Tobacco Research 2010; 12(1): 11-18.
0
10
20
30
40
50
60
70
3 Days 14 Days 1 month 3 months 6 months
% re
spon
se p
er c
all
Response rate at selected follow-up IVR calls
UCH (October 2014-March 2015)PH (March 2014-April 2015)

Page 22
Of note, the UCH IVR acceptance rate through their previous vendor averaged about 18% per call with a range of 29% at three days post-discharge to 8% at 6 months. The PSF-TCP IVR system was implemented on March 12, 2014. Their system was rolled out later than planned due primarily to vendor programming issues; before IVR launch, the program manager conducted live follow-up calls. The delayed IVR startup provided a natural quasi-experiment for evaluators to compare contact-acceptance when enrollees were called by a live counselor (call n=717) vs. IVR (call n=277) for the first three outreach sessions (figure 4). Call completion declined over time at similar rates for both modes, and IVR acceptance was consistently 60% of the rate with live calling. During this early period, the IVR acceptance rate was also lower than rates reported at other OMSC hospitals.6 Figure 4: Counseling call acceptance rates (%) among PSF-TCP enrollees, live counselors vs. IVR
IVR data: tobacco cessation outcomes The IVR follow-up systems at both sites ask respondents two questions about their recent tobacco use: 1) has the respondent used any form of tobacco in the past seven days; and 2) has the respondent used any form of tobacco since the previous call. Based on UCH IVR follow-up data, 39% of enrollees were abstinent (no smoking in the past seven days) at one week follow-up, 6 Reid, RD, Mullen K-A, Slovinec ME et al. Smoking Cessation for Hospitalized Smokers: and Evaluation of the “Ottowa Model.” Nicotine & Tobacco Research 2010; 12(1): 11-18.
0
10
20
30
40
50
60
70
80
3 days 14 days 1 month
Live
IVR

Page 23
36% at one month, and 38% at three months post discharge. UCH six month data were not available. At PH, 25% of enrollees reported seven-day abstinence one week after discharge, 21% at one month, 19% at 3 months, and 12% at 6 months. No IVR comparison data is available from non-enrollees. At six months post-discharge, the PH IVR seven-day point prevalence abstinence and the six-month abstinence rates are both lower than those reported in the six-month follow-up survey. PH is currently implementing a texting option to provide tobacco cessation support during the follow-up period. Program leadership anticipates that offering multiple opportunities and modalities to offer support will increase participant engagement in the program and potentially improve treatment outcomes. The program cessation specialist said, “The hope is that this option [texting] will allow the participant to engage with the program in a different and potentially more convenient way.” Conclusions University of Colorado Hospital and Penrose Hospital have implemented smoking cessation programs for inpatients that adhere to all major OMSC components and are adapted to fit within their respective healthcare systems. Implementation and process issues identified by program staff were resolved in a timely manner. Both UCH and PH continue to identify opportunities to improve and enhance their respective programs despite budgetary and other challenges. Process changes to the programs have generally resulted in improved outcomes moving forward. Inpatient cessation consultation, NRT, and program enrollment have reached levels similar to those reported at other OMSC sites. At UCH, where data were available, tobacco cessation efforts demonstrate improved seven day point prevalence abstinence and six-month abstinence rates compared to baseline measures.

Page 24
Appendix A: COMITT Tobacco Treatment Specialist Consultation tracking worksheet

Page 25
Tobacco Treatment Program Consultation Assessment
Date:________________________________ Patient already discharged Patient sleeping/not in room Patient MRN:______________________________ Patient refused consult Patient unconscious/intubated
1. Patient was receptive to discussion about NRT and comfort level.
Yes No
2. Patient was receptive to discussion about quitting smoking. Yes No
3. Patient was patched at consult
Yes No Patient declined Patch not offered
4. I made request of Nurse No a. Administer patch
b. Changed patient’s mind about NRT and now patient wants patch
c. Requested increased patch dose
d. Requested gum
5. Patient enrolled in the program?
Yes No
6. Reason for not enrolling:
a. Patient not eligible
b. Patient not ready to quit Agreed to harm reduction strategies
c. Patient already enrolled in program
d. Patient involved in other quit program
e. Patient could quit on his/her own
f. Other: ____________________________________________________

Page 26
Appendix B: Hospital System Change Pre-Implementation Key Informant Interview Guide

Page 27
Pre-Implementation Interview Guide
Good (morning/afternoon). Thank you for meeting with me to discuss the expansion of the inpatient tobacco cessation program here at __________. My name is __________ and I am the __________ for CEPEG, the external evaluation team contracted by The Colorado Department of Public Health to review inpatient tobacco cessation programs.
Through these interviews we hope to get a sense of how the cessation program evolved into its current format. We are particularly interested in:
The challenges you identified in the implementation process, and how these were resolved,
The lessons you learned during program implementation Any recommendations you may have for other organizations wishing to adopt similar
inpatient tobacco cessation initiatives in their own facilities
We want the inpatient tobacco cessation program at ____________ to be a successful model. With your help, we will work to identify ways to improve the current program, and ensure the sustainability of smoking cessation programs at this facility and others.
This interview should take 20-40 minutes. With your permission, I will record our discussion using a digital voice recorder. At the conclusion of all of the key informant interviews, the evaluation team will generate a summary report describing the pre-implementation system change process at ____________ along with lessons learned. Any specific quotes used in the report will be de-identified unless we explicitly ask your permission to use your words.
Do you have any questions before we get started?
1. First, would you please tell me your name and your job title?
2. How did you get involved with the inpatient smoking cessation program?
3. Can you provide a brief overview of how the program works at your site? a. Who is conducting the intervention? b. How are you identifying smokers? c. Weekend/evening coverage?
4. How similar is this program to the one at UCH?
a. Can you provide us with some examples of how the programs differ? How they are the same?
5. How have plans for implementing the program evolved since you first came on board?
Page 28
a. Were there any significant challenges that had to be resolved before you could move forward? How were they resolved?
6. Were you familiar with the Ottowa Model for Smoking Cessation before you became involved with this project? How familiar are you now?
a. Did the fact that this program was based on the OMSC influence your willingness to become involved?
b. How important was it to you to rigorously follow the OMSC? c. How closely does your program follow the original OMSC? Would you give us some
examples of how it differs? i. Why do you think the program was modified from the OSMC model? ii. Who ultimately made the final decision to make those changes?
7. Overall, how receptive do you think hospital staff is to this program?
a. Is it a priority?
8. Does ________________ have a task force or leadership committee to oversee the program?
a. What is your position on the task force? b. Who else is on the task force? How were they selected? c. How does the task force function? How are challenges or controversies resolved? d. Is there a particular are of the program that you have been most involved it?
9. Now let’s talk about the staff members who will participate in the program at your
hospital. a. What is their job title? b. How much/what type of training is required? c. What did they do previously? (i.e., were they hired specifically to provide this
program or were they recruited from other positions?) How have their jobs changed?
i. How much will this program add to their workload? ii. How receptive have they been to these changes?
d. How will your program interact with hospital staff (i.e., doctors, charge nurses, etc.)?
10. How involved are you in the program’s day-to-day operations? a. Will your patient care responsibilities and/or overall workload change as a result of
launching the program?

Page 29
b. Will the staff you oversee experience changes to their workload as a result of the program? How do you plan to manage that? (Foresee any difficulties?)
11. Do you think that launching this program will improve how accurately and consistently a patient’s smoking status is documented?
a. What changes were made to insure this?
12. How do you think this program will affect a patient’s overall experience at your hospital?
13. What role you do think pharmacotherapy such as nicotine replacement therapy (NRT) will play in this program?
a. How has it been integrated it into the program? b. Do you think it is a critical part of the program? c. Do you think it will be consistently offered to tobacco users— where appropriate—
during their stay? d. How did you decide what forms of NRT to stock? Who decides what type and
appropriate dosage?
14. Are there policies and procedures in place to evaluate the program? Who is responsible for overseeing this?
a. Accuracy of smoking status documentation? b. Responsiveness to requests for NRT? c. Adequacy of tobacco cessation consults? d. Methods for providing timely feedback?
15. What lessons have you learned that would make implementing a similar program at
another hospital system easier?
16. What do you think still needs to be done with this project in order for it to be successful?

Page 30
Appendix C: Hospital System Change Six-month post-discharge follow-up survey

Page 31
Hello! We are writing to you because you were admitted to University of Colorado Hospital about 6 months ago, and during your hospital stay you enrolled in the Smoking Cessation Program. We are contacting all program participants to find out about your experience with the program, how the program was helpful to you, and what areas can be improved. Your participation in this survey is voluntary and your cooperation is very important to our understanding of how well the program worked and how we can improve it to help people like you quit smoking. All of your answers will be kept strictly confidential and will only be used to improve this program. We won’t share your answers with your doctor or with anyone else. You may choose not to answer any of the questions at any time. This survey takes about 5 minutes to complete. Once you have completed it, please return it to us in the enclosed pre-paid envelope. Thank you for completing the survey. Instructions: These questions are about your tobacco use since you were discharged from University of Colorado Hospital approximately 6 months ago. Please answer them to the best of your recollection. Date Completed: _____ / ______ / ______
1. Have you used any form of tobacco since leaving the hospital approximately 6 months
ago? o Yes o No
2. Have you used any form of tobacco in the past 7 days?
o Yes If yes, how often are you using tobacco?
o Every day o Some days o Rarely
o No

Page 32
3. Since you left the hospital approximately 6 months ago, how many times have you
stopped using tobacco for at least 24 hours because you were trying to quit? o 0-1 o 2-3 o 4 o 5 or more times
4. In your quit attempt(s) since you left the hospital approximately 6 months ago, what
was the longest time you went without using any tobacco, even a puff of a cigarette? o 1 day o Several days o 1 week o Several weeks o 1 month o More than 1 month
5. Did you use Nicotine Replacement Therapy such as patches and/or gum or lozenges in
any of your quit attempts? o Yes o No
6. Did you use Nicotine Replacement Therapy such as patches and/or lozenges when you
were in the hospital? o Yes o No o I don’t remember
7. Being in the hospital can be uncomfortable. Thinking about your time in the hospital
approximately 6 months ago, did nicotine replacement therapy make you more comfortable, less comfortable or made no difference?
o More comfortable o Less comfortable o No difference o I did not use NRT in the hospital

Page 33
8. Thinking about your time in the hospital approximately 6 months ago, did meeting with the tobacco counselor during your stay make you more comfortable, less comfortable or made no difference?
o More comfortable o Less comfortable o No difference o I did not meet with a counselor
9. If you met with a tobacco counselor in the hospital, did your meeting cause you to feel
more interested in quitting, less interested in quitting or no different about quitting tobacco use?
o More interested o Less interested o No different o I did not meet with a counselor
As part of your participation in the Tobacco Cessation Program you received a number of follow-up calls about your tobacco use after you were discharged from University Hospital. These calls involved an automated telephone survey and several encouraging messages about your efforts to quit tobacco use. These next questions are about your experiences with the automated telephone survey since you were discharged from University Hospital approximately 6 months ago.
10. Did you respond to at least 1 follow- up call from the tobacco cessation program about your tobacco use?
o Yes o No
If no, what is the main reason you did not respond to any follow-up calls? o I did not realize calls came from program o The calls came at bad times o The automated system was too hard or too confusing to use o I joined another quit program o I wasn’t ready to quit o Other:_____________________________________________________

Page 34
11. Do you think there were too many calls, too few calls or the right number of calls? o Too many calls o Too few calls o Right number o I did not respond to any calls
12. How helpful were the calls in supporting your efforts to quit tobacco?
o Very helpful o Somewhat helpful o Not very helpful o I did not respond to any calls
13. What else would you like the hospital program to do to help you quit using tobacco?
o Provide more NRT after hospital discharge o Provide at least 1 personal call from a tobacco counselor after hospital discharge o Other:____________________________________________________________
14. If you responded to 1 or more automated calls, what one thing did you like the most
about using the automated telephone survey? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
15. What one thing did you like least about the automated telephone survey? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
16. The automated telephone survey lets you transfer to a tobacco counselor or leave a message for a counselor to call you back. How often did you use this feature?
o 1 time o Several times o Every call o Never
Page 35
17. If you requested to be transferred, were you able to speak with a tobacco counselor? o Transferred directly to a counselor o Left message and received call back o Left message but did not receive call back o Did not use this feature
18. What prompted you to ask to be transferred to a tobacco counselor? Please select all
that apply. o Requested more NRT o Struggling with urges o Needed coping strategies to manage smoking triggers o Wanted stress management techniques o Wanted coping strategies to manage living with a smoker while trying to quit o Other:____________________________________________________________
19. Is there anything else you would like to share about this program or your experiences
quitting tobacco? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Thank you very much for your time!