Embed Size (px)
Citation preview

1
Paper for Health Economists' Study Group (HESG) Meeting
Glasgow Caledonian University 23rd
-25th
of June 2014
Increasing the personalisation of social
care in England: factors associated with
variations in local patterns12
Authors: Jose-Luis Fernandez, Valentina Zigante ©
PSSRU, London School of Economics and Political Science
Keywords: social care, personalisation, direct payments
Abstract
Personalisation has been a defining trend in English social care provision, exemplified
through the increasing focus on personal budgets and direct payments. This paper
explores the demand, supply and other factors associated with patterns of local
variability in coverage and intensity of direct payments in English local authorities.
We use local authority data on extensiveness of services, expenditure/cost and local
circumstances such as age structure, health and deprivation, for England from 2005 to
2012. Statistical analysis was conducted for four client groups; older people, people
with physical disabilities, people with learning disabilities and people with mental
health needs. We find a steady increase in the number direct payments relative to
other service types, however with considerable variation between local authorities,
partly explained by the local needs profile. Direct payments are further found to be
driven by the cost of alternative services and overall rationing of services.
1 Work in progress. Please do not quote, cite or distribute.
2 The work was funded by the Department of Health to the Policy Research Unit in the Economics of
Social and Health Care. The views expressed are those of the authors and not necessarily those of the
funders.

2
Introduction
Personalisation is a denoting feature across public services, exemplified by the
emphasis on individual decision making in aspects of health care such as choice of
hospital and treatment. More recently this has extended through the introduction of
personal health budgets (Forder et al. 2012). Social care is one of the public services
areas where personalisation is most relevant due to the importance of individual
preferences in the design of ideal care packages. Direct payments forms a key
component in the application of the broader ‘personalisation agenda’ governing the
reform of public services. This agenda has been promoted by successive governments
to encourage service users themselves to take greater control of commissioning
(Glendinning et al. 2008). Care services in England can be thought to have been
transformed by two phases of marketisation, with a shift in the provision of services
from local authorities to private organisations and, more recently, a shift from local
authority to individual purchasing of care through the allocation of personal budgets3
and direct payments instead of services in kind (Glendinning 2012).
Direct payments legislation was implemented in April 1997 in England, Wales and
Scotland and a year later in Northern Ireland. The policy framework enabled local
authorities4 and health and social service trusts to make cash payments to users to
purchase services on their own behalf rather than using those supplied and organised
by the local authority. The user has virtually full autonomy in what is purchased for
the direct payment; for example a hiring a personal assistant, paying an informal
caregiver (with restrictions) or purchasing food services. In order to qualify for a
direct payment, an individual has to be assessed as being eligible for community care
services (Department of Health 2000). Access was initially restricted to users between
the ages of 18 and 65 but was later extended to other client groups.5 The emphasis on
3 Direct payments are closely related to personal budgets, however while direct payments are monetary
payments made by local authorities directly to service users, in lieu of social service provisions, a
personal budget, on the other hand, is a notional amount of social care funding for an individual’s
support, some or all of which may be taken as a direct payment. 4 In England social care is organised at the local authority or council area level by Councils with Adult
Social Services Responsibilities (‘CASSR’). As is the common practice we refer to these as ‘local
authorities’ (LA) throughout this paper. 5 The government policy and guidance documents on Direct Payments have been continually amended
and altered over the past ten years in an attempt to widen the eligibility criteria for Direct Payments and
increase take up (see for example Department of Health 2000).

3
personalisation has continued since the implementation of the Direct Payments act –
in later years through the introduction of personal budgets.
Personalisation is valued for its benefits in terms of improved outcomes for users, a
more efficient market structure and an attractive way of managing services for local
authorities. For users the main advantages are the opportunity to have care
preferences met, gain autonomy and gain access to services which may not be
available through local authority provision. Similarly, more active and ‘mobile’ users
create impetus for more responsive and efficient behaviour among providers, in order
to remain competitive and attract users who are more able to ‘vote with their feet’.
The care market is further expanded, beyond the traditional conception of a mixed
economy of care – including outsourced provision and a strong role for voluntary
provision (Glendinning et al. 2008) – to include new types of care provision such as
friends and family and local pubs instead of meals on wheels. This can be particularly
beneficial in areas where formal supply is limited, such as in sparsely populated, or
expensive (e.g. in London) areas. The advantages for local authorities lie in the
prospective for rationing services – i.e. offering smaller care packages, compared to
market value, with the expectation that individuals are able to identify more cost-
efficient sources of care (for example paying an informal caregiver). This is facilitated
by the substantial discretion in the allocation of DPs on the part of care managers
(Ellis 2007; Ellis 2011).
Even though direct payments are generally seen as improving the user experience and
service outcomes, some concerns are worth noting. Individual users may struggle with
lacking information about the market in order to make appropriate commissioning
decisions. Similarly, individuals have less market power than local authorities which
implies a change in the balance of power between providers and purchasers (in this
case the individual). The hiring of personal assistants can place significant transaction
costs on service users due to the legal and administrative duties associated with
becoming an employer. The severity of these concerns is linked to the relative ability
among users to cope with the management and commissioning of their own care.
Partly as a result of differences in their motivations and abilities and the availability of
support for the management of care package from family and friends, research has

4
found substantial differences in take-up between client groups (Priestley et al. 2006;
Glendinning 2008).
At an individual level, a range of factors are likely to drive the success of the direct
payment model (for a general discussion see the Individual Budgets evaluation,
largely applicable also to DPs: Glendinning et al. 2008). Firstly, a larger care package
may be more attractive in terms of reducing the relative impact of the transaction
costs related to setting up and learning the system. Likewise, it is important that
market structures are in place which support the individuals as commissioners, in
dealing with care providers, and that the allocation and sign-off processes are not
overly long or bureaucratic (Holloway et al. 2011). As mentioned above, individual
ability to manage a payment matters (depending on informal support, cognitive
impairment etc.), but also the wishes and preferences of service users and their
families. Self-determination is unlikely to be equally attractive to all service users,
particularly in terms of being involved in the commissioning process. Different
individuals will also require different levels of support, which targeting of models will
be key to alleviate (Glendinning et al. 2008).
The use of direct payments has increased steadily across the country since the
introduction. The overall number of people who receive services on the other hand,
has contracted since 2005 and the rate of the fall increased after 2010 (Fernandez et
al. 2013). The proportion of the population covered by services dropped by just over
30% between 2005 and 2012 and it is clear that this is not due to decreasing need; in
fact, research indicates increasing need due to generally acknowledged demographic
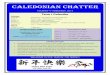
and social change (Wittenberg et al. 2011). Figure 1 illustrates the change in number
of users of community and nursing home services.

5
Figure 1 Number of community care clients and total number of clients 2005-2012, 1000s
Source: data from RAP collection from the health and social care information centre.
Direct payments on the other hand exhibit a rapid growth since 2005. DP’s as a
proportion of all services has increased from 3% of services to 17% between 2005 and
2012. It is important to remember that although DPs is the policy type increasing the
most; it only services a minority of users. This is particularly evident for certain user
groups; among older people and users with mental health needs on average around
10% of users receive a direct payment (see figure 2). Users in the group ‘Physical
disability’ on the other hand use DP to the highest extent. The difference between the
groups has remained fairly constant over the period, with no evidence of MH and OP
usage catching up. The growth in DP usage among older people has flattened out
somewhat between 2011 and 2012.
Previous work found distinct variation between local authorities in the extent to which
DP:s are utilised and also considerable variation between client groups; older people,
people with physical disabilities, people with mental health issues and finally, people
with learning disabilities (Fernandez et al. 2007; Leece & Leece 2006). The
differences between the user groups are also well known in the literature. For example
the particular role of the young disabled, in driving the introduction of DPs as
discussed above, resulted in the high usage rates also in our time period (Glasby &
Littlechild 2009).
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000
2005 2006 2007 2008 2009 2010 2011 2012
Community care clientsCommunity care, residential and nursing clients

6
Figure 2 Number of direct payments - proportion of community care users, by client group
Note: RAP data 2005-2012. Client groups: OP ‘older people’, MH ‘mental health’, PD ‘physical
disability’, LD ‘learning disability’.
This paper explores the factors associated with direct payments usage in the four
client groups between 2005 and 2012. The period is denoted by direct payment being
fairly well established (past the main implementation costs and early glitches) but also
by fiscal austerity being a key concern for the provision of social care in England. We
attempt to identify the role direct payments play as a part of the care offer of local
authorities, in relation to local need and economic and social characteristics, service
supply and rationing of services. We take into account how the allocation of services
takes place in a complex system of care provision, in which care managers play a key
gatekeeping role, with decisions constrained by local supply and commissioning
processes.
The paper is structured as follows; a brief background section first elaborates the
conceptual model of local care provision followed by a discussion of the data used,
the hypothesised relationships and econometric methods. The results are then outlined
followed by a discussion and conclusions.
Utilisation of direct payments – conceptual model
In the context of the general contraction of services we find an increase in DP
utilisation, however, there is as shown in figure 2, a wide disparity between client
groups, and as shown in figure 3, between local authorities. Each line in figure 3
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
2005 2006 2007 2008 2009 2010 2011 2012
OP MH PD LD

7
represents the 149 local authorities in terms of DP utilisation as a proportion of total
services. The local authorities are ranked by proportion for each client group, hence
the order varies accordingly. For example the client group ‘physical disability’ the
proportion varies from 10% to 90% of community services in 2012. The client group
‘older people’ has the least variation between local authorities, from 3 to 35%.
Figure 3 Variation in local authority utilisation of direct payments packages 2012
Note: Direct payments packages, as a proportion of community care services from RAP 2012/2013, by
client group.
The policy architecture underlying the distribution of DP clients relative to other
services as a whole is complex (see Fernandez et al. 2007) Given these complexities
and the remarkable difference is DP utilisation we now move to conceptually explore
the underlying structures and hypothesised influential variables which we will later
test empirically. By law, all users should be offered the option to receive their care
package as a direct payment (Glasby & Littlechild 2009). In practice however, the
process of deciding on a care package is likely to be a function of a wide range of
factors influencing both the user’s and the care manager’s preferences and constraints.
The decision making process can be likened to a bargaining process, in which the
negotiation between the user and the LA can result in a variety of care outcomes. In
figure 4 the decision making process is illustrated; from the initial contact to an
implemented care package. The various decisions come with a specific set of
considerations and negotiation between user and local authority representative
determines the final care allocation.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
OP MH PD LD

8
Figure 4 Model of care decision making – stages and options for individuals with care need
Source: author’s own
At the first stage: the initial contact between individual and the LA, the individual is
often in a situation where the need for (additional) care has become acute. This
contact often takes place at a time of crisis, for example after the individual suffering
from an adverse health event, such as a fall. Family and friends tend to be
instrumental in making this contact. Starting from the time of the user with care need
being assessed by the local authority, the first decision is whether the individual is
eligible – i.e. meeting the need and means tests.6 In many cases the individual him or
herself will fund all or part of the care needs (henceforth self-funded). This paper is
focused on the proportion of services being provided through the local authority;
hence excluding self-funded care for which to date little data is available. In terms of
the care choice, nursing or residential care will seem attractive if needs are substantial
or it is difficult for the user to stay at home for other reasons. This is commonly the
6 The specifics of the means-test is set at the national level (currently at £23,250 in capital for home
care) whereas the eligibility (needs test) varies significantly. The Fair Access to Care Services (FACS)
guidelines in 2003 set up a common framework against which to assess needs and set local eligibly
thresholds for the provision of care. Many authorities have however tightened eligibility thresholds
such that only those with critical or substantial levels of need are entitled to receive publicly-funded
care (Fernandez et al. 2013).

9
case for users with dementia or with extensive health care needs, possibly in
combination with a lack of informal support.
If the user is able to remain at home – which is the preferred option in line with the
‘ageing in place’ (Hillcoat-Nalletamby & Ogg 2013) discourse – numerous care
options become available; for example home care (directly provided), day care and
meals.7 The choice between direct payments and directly provided services (services
in kind) is at the focal point of this paper. Following this, we define our dependent
variable as the number of clients receiving their allocated care as a direct payment,
relative to the overall total number of clients receiving LA provided community care.
Through this we attempt to standardise for the needs profile of each LA, as we are
considering the care allocation for users who have already been deemed eligible for
care, and equally for DPs.
In terms of the choice between DP and directly provided services a few aspects
beyond those alluded to in the introduction are worth exploring further. In terms of
care users’ preference and abilities it has been found that relatively articulate and
‘forceful’ users, or those with a ‘champion’, such as a family member or engaged care
manager are more likely to use DPs. This may be reinforced by uncertainties held by
front line staff about the suitability of direct payments particularly impacting on users
with mental health needs, dementia or learning difficulties (Priestley et al. 2006).
Further, the implementation of direct payments involves numerous practical,
organisational and cultural challenges for staff at all levels in local authorities. The
care manager has a key role a gatekeeper (Ellis 2011) and makes an assessment of the
risk of relinquishing control to the user – whether the user has the adequate support
and ability to suitably manage his or her care (Milner & O’Byrne 1998). Foster et al.
found that practitioners’ awareness of the constraints and limitations of the resource
context influenced their assessment process and their decision-making. At times
constraints and limitations stood above the needs of service users and could be a
barrier to inclusive decision making and users receiving the appropriate care (2006).
7 Community-based services are services provided to people who live in their own homes (this includes
supported/sheltered accommodation and extra care housing). Clients living in a home setting can
receive a number of community-based services. Subsets of these services or components of service
include: Home care, Day care, Meals, Short-term residential – not respite, Direct payments and
personal budgets, Equipment and adaptations, Professional input and support, Other.

10
For our analysis this is especially relevant if there are systematic differences in
preferences and behaviour of care managers between local authorities.
Data and methods
This paper uses panel data from 2005 to 2012, obtained from official sources at local
authority level (n=147 2005-2008, n=149 2009-2012). Table 1 outlines the variables
used and sources of the data. These are discussed in detail below – outlining the
hypothesised relationships.
Table 1 Description of variables
Category Variable Source
Local need Health status Census
Limiting long-standing illness Census
Deprivations scores Census
Mortality ONS
Receipt of Social Security benefits DWP
Population profiles ONS
Informal support Census
Service provision Number of direct payments RAP forms, DoH
Number of clients of other services RAP forms, DoH
Residential care utilisation RS forms, DoH
Home care utilisation RS forms, DoH
Expenditure in social care services RS forms, DoH
Supply (Unit costs) Home care unit costs PAF forms, DoH
Local wages New Earnings Survey
House prices Land Registry
Area, Density ONS
Local performance Satisfaction with services
PAF forms, DoH/ASCS
survey 2011
Political control Electoral commission
The set of local need controls included in the models aim, in various ways, to control
for the characteristics of the user population and the way that they are likely to
interact with social care service provision.
We assume indicators of population health to be correlated with the need for social
care. This includes indicators of deprivation which is known to be closely related to
poor health among the population. On the other hand, DPs come with an expectation
of service users to manage their care. Users with poor health, beyond their disability,

11
may be less inclined to demand DPs, and likewise care managers may be less inclined
to offer. Our disability indicators, on the other hand, are population averaged limiting
long-standing illness and proportions receiving disability benefits (AA and DLA). We
expect a close link between service provision and indicators of disability. In terms of
the effect on DP utilisation, users with more extensive need may receive a larger care
packages. Theoretically this may cause care users to be more prone to accept a DP
instead of directly provided care due to the reduced impact of transaction costs
(economies of scale). Similarly, we expect care managers, facing budget pressures to
favour DPs for large care packages, which would otherwise be expensive to provide
directly.
It is also well known that provider supply and the broader care market conditions will
influence provision decisions. Unit costs for alternative care services, such as home
care, depending on local wages and population density, will influence the cost of
providing services. High costs are likely to shift utilisation in favour of DPs where it
is expected that the care user is able to source care in a more cost-effective manner,
potentially through paying informal care givers. Informal care is a cheap and efficient
way of utilising a DP – however subject to limitations: users are technically not
allowed to hire co-residential family members, but this regulation is implemented at
care managers’ discretion. Care managers may be reluctant to offer a DP when a well-
established informal caregiving arrangement is in place, but may in any case be able
to offer a smaller care package to allow respite for the caregiver. Particularly, for the
client group LD (learning disability) this may be a common practice as parents of LD
users provide informal care while also managing a DP.
Finally, we hypothesise that service provision variables are key for the relative
utilisation of DPs. One of the assumed key driving forces of the shift in provision
towards DPs, in the current economic climate, is rationing to meet shrinking budgets.
An LA which covers a relatively large proportion of its residents may face higher
need (which we can control for in models) but is likely to be wealthy and generous
and can provide services directly, instead of offering DP. This assuming that care
managers in wealthy LAs does not have a particular preference for DPs.
Our ability to draw conclusions from the analysis is hampered by the limitations of
the data. We estimate reduced form models, in which we are not able to disentangle

12
demand and supply. As the care utilisation is a result of a negotiation, taking into
account the preferences of both service user and LA, our control variables affect both
actors, potentially in contradictory ways. Similarly, as the data is collected at LA
level, what we are considering are the effects of population average of for example
health status or disability capturing need. This does not account for the severity of the
need, simply that a certain proportion of the population has self-rated as suffering
from a limiting long-standing illness or poor health. The strength of our interpretation
and precision of our estimates is affected.
Data is collected yearly from 2005 to 2012. 2005 covers the year 2005/2006 in terms
of the RAP (Referrals, Assessments and Packages of care) collection including
detailed data on social care provision. The majority or variables are proportions of the
relevant population – for example poor health status for older people is entered into
the regressions as the proportion of the total number of older people who have rated
their health as ‘poor’ in the Census questionnaire. The Census variables (2001 and
2011) as well as deprivation (2004, 2007 and 2010) are only available for a limited
number of years throughout the period these have been linearly intrapolated. The
dataset has 1,184 observations distributed over the 8 years of observation. The panel
is unbalanced due to the split of LA Cheshire into Cheshire East and Cheshire West &
Chester, and Bedfordshire into Bedford and Central Bedfordshire in 2009. The RAP
data collection has some missing values which have where possible been estimated.
The RAP recording of number of direct payments users changed in 2009/2010 –
essentially the direct payments were merged with the recording of personal budgets –
but reverted back to the old practice in 2010/2011. This means that the figures for
2009/2010 are not comparable with prior or later data (Health and Social Care
Information Centre 2012). The 2009 data was intrapolated and all models have been
run without the year included. Further, excluded categories are the substance misuse
client group which is generally not available for direct payments and similarly, three
small and atypical local authorities; City of London, Isles of Scilly and Isles of Wight
have also been excluded.
To account for the non-normality in the distributions of our key dependent
variable (the number of clients receiving their allocated care as a direct payment,
relative to the total number of clients receiving LA provided community care) we

13
employ generalised linear modelling (GLM) estimation methods taking into
account the panel structure of the data, with the appropriate variance function
chosen following the methodology proposed by Manning and Mullahy (2001).
We assume an AR1 correlation, i.e. that observations closer in time are more strongly
correlated. We observe collinearily between the aggregate area level indicators and
hence we approach the model building in steps by firstly focusing on need indicators,
followed by informal care and then social care variables. Particular attention is paid to
a range of LA level social care indicators of overall population coverage of care,
expenditure and cost of services (unit costs). The social care variables are closely
correlated and there are issues with endogeneity; the overall and variety of the care
offer is a function of the user demand, LA preferences and care supply as discussed
above.
Results
We initially consider a model controlling for need (demand) and supply exclusively –
the results are reported in table 2. Need is a key control variable as it will strongly
influence the coverage of the population each LA can afford (as the cost of care
packages will increase when needs are more severe). Moreover, the level of need
among the covered population will influence whether DPs are an appropriate care
option.
The proportion of limiting longstanding illness positively influences the usage of DPs
while the proportion reporting poor health status has a negative relation with DP
usage. These counterintuitive results – we would expect a higher proportion of poor
health would lead to a higher usage of DPs – may be explained by the historic role of
the disabled (PD client group) as the main usage group of DPs. It is not health status
that is driving DP usage – but rather disability. Similarly it is conceivable that self-
rated health status may differ qualitatively from (self-rated) limiting longstanding
illness. Life expectancy at age 65 is positive, which supports the idea that it is the
distinction between disability and health which is driving the need effect in the
models.

14
Table 2 Panel glm regressions, dependent variable DP as proportion of community care users, by
client group – need and supply
Client group Older people Physical
disability Mental health
Learning
disability
Poor health -10.585***
Poor health -33.331*** -53.012*** -42.575***
Life expectancy at age 65 0.324*** 0.060 0.249*** 0.179***
Limiting longst. illness 3.775***
Limiting longst. illness 1.430** 1.415 3.028***
AA 10.333***
DLA 23.513*** 50.015*** 49.150***
Weekly earnings (average) 0.001** 0.000 0.000 0.001***
Population density 0.068** 0.081*** 0.105*** 0.092***
Weekly cost, home care
provision 0.188** 0.100*** 0.262** 0.120**
Constant -12.884*** -3.201*** -9.490*** -7.395***
Number of observations 1147 1172 1148 1172
Notes: gamma, AR1 correlation structure a) Proportion of population age 65+
b) Proportion of population age 18-64
AA= attendance allowance (for individuals over age 65)
DLA = disability living allowance (for individuals under age 65)
Need is further captured through the proportion of the population receiving attendance
allowance (AA) and disability living allowance (DLA), which both have a positive
impact on DP usage. These variables are also closely linked to disability and need for
services rather than overall health. Other indicators of need with weaker relationship
with DP usage are social security benefits – here pension credit for OP and income
support for the other client groups (under age 65). These variables are related to
deprivation (also tested in the models) in that they capture the expected coverage of
social care services overall (the proportion of the population the LA is required to
serve based on the means-test). Including deprivation, the variables are also correlated
with need (health status and disability). These variables however tend to be
insignificant in models where need is controlled for through the variables discussed
above – with disability indicators having the strongest predictive power.
Moving to the supply side, also reported in table 2, our key indicators of the cost and
ease of provision are wages; population density and home care unit costs. Wages and
population density more broadly capture the price level in the local authority, and
implicitly the cost of providing various types of care. The positive sign on weekly
earnings and home care unit cost indicate that DPs are substituted when other types of
care are likely to be relatively expensive. Density on the other hand indicates that

15
there is a positive relation between DP utilisation and more urbanised areas. We
expect DPs to be common where the spread of care users implies that formal services
are relatively difficult to provide. On the other hand, this indicates that density
captures the cost of alternative services, which is higher in urban areas potentially
accounting for the positive effect of density.
Linked to the supply side and a key complement to formal social care provision is the
availability of informal care. Results from models incorporating informal care
variables are shown in table 3. Informal care is also (endogenously) related to demand
for formal care services and hence potentially DPs as a part of care services. We find
an overall negative effect when adding an indicator of informal care supply (as a
proportion of population) to our models – across the client groups.
Table 3 Panel glm regressions, dependent variable DP as proportion of community care users, by
client group – informal care
Client group Older people Physical
disability Mental health
Learning
disability
Poor health -15.648***
Poor health -30.152*** -50.005*** -40.299***
Life expectancy at age 65 0.236** 0.079** 0.272*** 0.154***
Limiting longst. illness 1.853**
Limiting longst. illness 1.662** 0.384 2.628**
AA 6.997**
DLA 14.708*** 19.993** 26.133***
Weekly earnings (average) 0.001*** 0.000 0.001 0.001***
Population density 0.036 0.017 0.058** -0.002
Weekly cost, home care
provision 0.046** 0.084** 0.271*** 0.108**
Informal care (1-19 hours) -35.334**
Informal care (20-49 hours) 153.763**
Informal care (50+ hours) -10.652
Informal care (1-19 hours) -13.954*** -14.760** -21.345***
Informal care (20-49 hours) 36.762** 27.221 83.319***
Informal care (50+ hours) 0.753 74.984** 14.648
Constant -7.578*** -2.518*** -9.690*** -5.594***
Number of observations 1147 1172 1148 1172
Notes: gamma, AR1 correlation structure a) Proportion of population age 65+
b) Proportion of population age 18-64
AA= attendance allowance (for individuals over age 65)
DLA = disability living allowance (for individuals under age 65)
As DP regulations prevent paying a co-residential informal caregiver this is the
expected outcome. The same results were found for client groups LD and MH in the
previous study (Fernandez et al. 2007). If informal care is already available, this is
taken into account in the care assessment, and DPs are less likely to be offered.

16
However, when considering intensity of informal care (number of hours per week) we
find that the 20-49 hour per week bracket has a positive effect on DP uptake while the
19 hours and below drives the overall negative effect identified. This is puzzling as
the higher the number of hours; the more likely is care is to be co-residential and
hence not generally covered by DPs. It is however possible that where directly
provided services are expensive; DPs are offered also where informal care is present
and potentially co-residential. For mental health users the positive effect is at the 50
hours and above bracket which may be explained by the potentially limited ability of
MH users to manage a DP without intensive support for an informal carer.
Finally, we directly consider indicators of spending and provision in LAs. Table 4
shows the results of the analysis, again across user groups.
Table 4 Panel glm regressions, dependent variable DP as proportion of community care users, by
client group – coverage and unit costs
Client group Older people Physical
disability Mental health
Learning
disability
Poor health -13.282***
Poor health -30.573*** -59.285*** -42.539***
Life expectancy at age 65 0.237** 0.083** 0.169* 0.086*
Limiting longst. illness 1.692*
Limiting longst. illness 1.341* 0.342 2.288**
AA 3.756
DLA 13.128*** 16.226* 22.625***
Weekly earnings (average) 0.001** 0.000 0.001 0.001***
Population density 0.015 0.022 0.082** 0.003
Weekly cost, home care
provision 0.083* 0.019* 0.201* 0.087**
Informal care (1-19 hours) -36.016**
Informal care (20-49 hours) 164.067***
Informal care (50+ hours) -17.192
Informal care (1-19 hours) -12.523*** -12.139* -21.827***
Informal care (20-49 hours) 32.770* 15.001 72.859***
Informal care (50+ hours) 8.431 88.724** 23.938
Change in coverage
(proportion of population
receiving services) -0.003** -0.006*** -0.006*** -0.002***
Constant -7.375** -2.415*** -7.159*** -3.866***
Number of observations 1147 1172 1148 1172
Notes: gamma, AR1 correlation structure a) Proportion of population age 65+
b) Proportion of population age 18-64
AA= attendance allowance (for individuals over age 65)
DLA = disability living allowance (for individuals under age 65

17
The variable year on year change in coverage is negative across the user groups –
indicating that DPs are more common in LAs which are contracting services and
providing to a smaller proportion of the population. The results are identical if
including the level of coverage or a lagged (one or more years) indicator of level of
coverage. These local authorities are thought to cut low-need users and focus on the
neediest as a method of reducing cost. This process may in itself incentivise more
direct payments as care packages are larger and therefore more attractive relative to
transaction costs. DP will further seem attractive when care managers are under
pressure to contain spending as the care packages are generally cheaper than the
equivalent value of direct services.
We note that population density is not significant when controlling for informal care,
which is linked to household size and in turn density. Further, the effect of unit costs
is weakened when introducing coverage, the positive sign is consistently maintained.
A range of variables, theoretically potentially related to DP usage, have been included
but found to be insignificant in the regressions. In particular, political party in power
and indicators of satisfaction with social care (albeit only cross-sectional data for this
variable) were found to be largely insignificant in models controlling for need and
supply effects. Adding year dummies causes most variables to go insignificant except
for the change in coverage indicator.
Discussion
The results indicate two main processes at play; DP utilisation being driven by
rationing of services and relatedly, by relative cost of directly provided services. This
is consistent across the four client groups, even though we find a certain variation in
relationships with need and supply between the groups. Compared to previous
research (see Fernandez et al. 2007) our set of predictors have evolved to match the
current policy environment. We find more uniform effects across the client groups,
indicating some convergence due to the increasing spread of DPs across the groups. In
the early years of the 2000s ‘physical disability’ users where still the only user group
where DPs were an inherent part to service provision. We are now also more
concerned with the effect of the current fiscal austerity impacting significantly on care
services. There is concern that the role of DPs as a tool for rationing services in the

18
current austere fiscal climate will lead to negative effects on quality. This particularly
due to the importance of information and support (Glendinning et al. 2008) in
managing DPs which may be rationalised in LAs attempting to contain costs.
A particularly puzzling result is the positive effect of population density on the
utilisation of DPs. However, when introducing informal care and coverage in the
models population density tends to be an insignificant – only for mental health users
does it remain significant. This implies that the care market effect of more densely
populated areas outweighs the potential challenges to direct service provision which
may lead more rural LAs to favour DPs. There may further be a demand effect in
cities where a DP seems more attractive due to the relative abundance of care staff
and other services which allows for a care package which meets the user’s
preferences. The ambiguity of this interpretation highlights the challenge of
disentangling the effect of the two utility functions underlying the negotiation
between the care manager and the service user. Population density clearly influences
both, potentially in contradictory directions, however the current data does not allow
us to separate the effect.
Further, the relationship identified between direct payments and the availability of
informal care is worth noting. Medium to high intensity (over 20 hours per week)
exhibits a positive relationship with DP utilisation indicating that informal care may
be complementary to DP usage. This may imply that pre-existent informal caregiving
relationships are being supplemented by DPs. If this is the case, this is likely to be a
positive development for informal caregivers, as the respite and support needed is
often sporadic and meeting (highly) specific needs, which direct service may struggle
to, or be unable to provide. We must however caution that the prevalence of informal
care is population averaged and intrapolated, leading to less precision in our
estimates.
Conclusions
This paper has empirically investigated the extent to which local patterns can help
explain the expansion of direct payments utilisation in English local authorities. A
causal interpretation is hampered by the inability to disentangle the care supply from
the demand or service users and the substitute/complement of informal care. The

19
reduced form modelling was necessary due to lack of data allowing us to instrument
at local authority level. However, our results still confirm that direct payments
utilisation is significantly shaped by attributes of local social care systems and both
supply and demand side influences.
The noticeable increase in direct payments utilisation across client groups, although
driven by a forceful lobby and consecutive governments, seems in later years to
correlate with issues of fiscal austerity and rationing of services. We find evidence of
direct payments being favoured by local authorities where coverage is shrinking and
where alternative methods of provision are relatively expensive. As direct payments
are broadening across the client groups it is crucial that investment in support
mechanisms is maintained. This is particularly important due to the fact that direct
payments are increasingly being used by service users with ‘less ability’. Individual
level data can beneficially explore this relationship further.
Finally, we have further shown that some influences are common across the user
groups while other have varying effects. Overall this indicates that the policy of direct
payments at the local level is shaped by broader policy drivers across user groups and
to some extend local authorities. The clear-cut variation between local authorities in
terms of direct payments utilisation, together with our findings on local patterns,
emphasises the importance for performance monitoring and further research taking
such factors into account, acknowledging the extent to which these influence the
policy choices of local authorities.

20
References Department of Health, 2000. Community Care (Direct Payments) Amendment
Regulations,
Ellis, K., 2007. Direct Payments and Social Work Practice: The Significance of
“Street-Level Bureaucracy” in Determining Eligibility. British Journal of Social
Work, 37(3), pp.405–422.
Ellis, K., 2011. “Street-level Bureaucracy” Revisited: The Changing Face of Frontline
Discretion in Adult Social Care in England. Social Policy & Administration,
45(3), pp.221–244.
Fernandez, J.-L. et al., 2007. Direct payments in England: factors linked to variations
in local provision. Journal of Social Policy, 36(01), pp.97–121.
Fernandez, J.-L. et al., 2013. Implications of setting eligibility criteria for adult social
care services in England at the moderate needs level,
Fernández, J.-L., Snell, T. & Wistow, G., 2013. Changes in the patterns of social care
provision in England: 2005/6 to 2012/13, PSSRU Discussion Paper 2867
Forder, J. et al., 2012. Evaluation of the personal health budget pilot
programme.PSSRU discucssion paper 2840_2
Foster, M. et al., 2006. Personalised social care for adults with disabilities: a
problematic concept for frontline practice. Health & social care in the
community, 14(2), pp.125–35.
Glasby, J. & Littlechild, R., 2009. Direct payments and personal budgets: Putting
personalisation into practice, Bristol: Policy Press.
Glendinning, C., Halliwell, S., Jacobs, S., Rummery, K., & Tyrer, J. (2000). Bridging
the gap: using direct payments to purchase integrated care. Health & Social Care
in the Community, 8(3), 192–200.
Glendinning, C. et al., 2008. Evaluation of the Individual Budgets Pilot Programme:
Final Report. Available at: http://kar.kent.ac.uk/13322/ [Accessed May 20,
2014].
Glendinning, C., 2012. Home care in England: markets in the context of under-
funding. Health & social care in the community, 20(3), pp.292–9.
Glendinning, C., 2008. Increasing Choice and Control for Older and Disabled People:
A Critical Review of New Developments in England. Social Policy &
Administration, 42(5), pp.451–469.
Health and Social Care Information Centre, 2012. Community Care Statistics 2010-
11: Social Services Activity Report, England,
Hillcoat-Nalletamby, S. & Ogg, J., Moving beyond “ageing in place”: older people’s
dislikes about their home and neighbourhood environments as a motive for
wishing to move. Ageing and Society.
Holloway, S., Neville, S. & Watts, R., 2011. Longitudinal Study of Cash Payments
for. Adult Social Care in Essex, London.
Leece, D. & Leece, J., 2006. Direct Payments: Creating a Two-Tiered System in
Social Care? British Journal of Social Work, 36(8), pp.1379–1393.
Manning, W.G. & Mullahy, J., 2001. Estimating log models: to transform or not to
transform? Journal of health economics, 20(4), pp.461–94.
Milner, J. & O’Byrne, P., 1998. Assessment in Social Work, Hampshire: Palgrave.
Priestley, M. et al., 2006. Direct Payments and Disabled People in the UK: Supply,
Demand and Devolution. British Journal of Social Work, 37(7), pp.1189–1204.
Wittenberg, R. et al., 2011. Projections of demand for and costs of social care for
older people in England, 2010 to 2030, under current and alternative funding
systems.