Embed Size (px)
Citation preview

Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle
Change Program - A CASE STUDY ON CLINICAL
IMPLEMENTATION

Theviewsexpressedinthispresentationaretheauthors’anddonotreflecttheofficialpolicyorpositionoftheCentersforDiseaseControlandPreventionortheU.S.government.

Table of Contents
Executive Summary 6
The National Diabetes DPP Lifestyle Change Program 8
The American College of Preventive Medicine Demonstration Projects 11
Case Study 1: Federally Qualified Health Center: Northeast Missouri Health Council 15
Pre-Demonstration Project Approach 15
Demonstration Project 16
Success, Challenges, and Lessons Learned 20
Scalability and Next Steps 20
Case Study 2: Independent Practice Association: Accent on Health 21
Pre-Demonstration Project Approach 21
Demonstration Project 21
Successes, Challenges, and Lessons Learned 24
Scalability and Next Steps 25
Case Study 3: Independent Practice Association: Griffin Faculty Physicians 26
Pre-Demonstration Project Approach 26
Demonstration Project 27
Summary of Challenges 33
Summary of Successes 34
Challenges 37
Conclusion 38
Resources 40

Acknowledgements
AbouttheCentersforDiseaseControlandPrevention(CDC),DivisionofDiabetesTranslationTheCDCDivisionofDiabetesTranslation(DDT)workstoreducethepreventableburdenofdiabetesthroughpublichealthleadership,partnership,research,programs,andpoliciesthattranslatescienceintopractice.Strategicgoalsfocuson:
• Preventingtype2diabetes;• Preventingcomplications,disabilities,andburdenassociatedwithdiabetes;and• Eliminatingdiabetes-relatedhealthdisparities.
AbouttheAmericanCollegeofPreventiveMedicineTheAmericanCollegeofPreventiveMedicine(ACPM)isaprofessionalmedicalsocietyofmorethan2,700preventivemedicineandpublichealthphysicianswhomanage,research,andinfluencepopulationhealth.Preventivemedicinephysiciansareemployedinawiderangeofsectorsandsettings,andACPMFellowsaresoughtafterleadersinlocal,national,andinternationalhealthsectors.Tothesespecialists,ACPMprovidesadynamicforumfortheexchangeofknowledgeandoffershigh-qualityeducationalprogramsaswellasprofessionaldevelopmentresourcesandnetworkingopportunities.
KeyProjectContributors:
• LianaLianov,MD,MPH,FACPM,FACLM,HealthTypeLLC• HeatherTindallReadhead,MD,MPH,UniversityofCaliforniaBerkeley• ShannonM.Haworth,MA,AmericanCollegeofPreventiveMedicine• DaniellePere,MPM,AmericanCollegeofPreventiveMedicine• MarissaHudson,BS,AmericanCollegeofPreventiveMedicine
ProjectFunding:TheAmericanCollegeofPreventiveMedicineissupportedbyafive-yearcooperativeagreement(#6NU38OT000130-05-01)fromtheCDCOfficeofState,Tribal,Local,andTerritorialSupport(OSTLTS).ForMoreInformationontheProject:
PleasecontactDaniellePere,VicePresidentofPrograms&Education,ACPM,[email protected]
AmericanCollegeofPreventiveMedicine455MassachusettsAvenueNW,Suite200
Washington,[email protected]
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 5

Executive Summary
PrediabetesandType2diabetesareserioushealthconcernsthataffectalargeportionoftheUnitedStatespopulation.TheAmericanCollegeofPreventiveMedicine(ACPM)in2016undertookatwo-yearprojecttoraiseawarenessoftheseconditionsanddevelopprotocolsforscreening,testing,andreferringpatientswithprediabetestoCDC-recognizedorganizationsofferingtheNationalDiabetesPreventionProgram(NationalDPP)lifestylechangeprogram.
Inthetwo-yearproject,ACPMoversawninedemonstrationprojectstohelpclinicsandhealthcareorganizationsinterestedindevelopingandimplementingprediabetesscreening,testing,andreferralmodels.
Thiscasestudyreviewstheapproaches,barriers,scalabilityplans,andrelatedlessonslearnedofthreeofthesehealthcareorganizations:
• NortheastMissouriHealthCenter–Kirksville,Missouri(FQHC)• AccentonHealth–Washington,DC(IPA)• GriffinFacultyAssociates–Derby,Connecticut(IPA)
The focusof theprojectwas to increasephysicians’/health careprofessionals’ awarenessofprediabetes as aserious health condition; develop and implement protocols for screening, testing, and referring patientswithprediabetestoaCDC-recognizedorganizationofferingtheNationalDPPlifestylechangeprogram;andincreasethe number of physicians/health care professionals taking action to screen, test, and refer patients withprediabetestoCDC-recognizedorganizations(organizationswithpending,preliminary,orfullrecognition).
Promisingpracticesidentifiedinthecasestudyspeaktothesimilaritiesinhealthcaredeliverydespitevariationsingeographiclocation,patientpopulations,orinsurancecoverage.
Thiscasestudyisaresourcethatwillhelpclinicsandhealthcareorganizationsinterestedinimprovingordevelopingandimplementingprediabetesscreening,testing,andreferralmodels.

Keyareasforlessonslearnedwereorganizedby:• ProviderConcerns• Delays• Communication/Awareness• Technology• Processes/Workflow
Keytakeaways:
• Type2diabetesriskassessmentsshouldbeincorporatedintostandard,easilyrepeatableworkflowproceduresforprovidersandstaff.Oncethatworkflowisestablishedandimplemented,itshouldbecomeroutine,muchliketakingapatient’sweightorbloodpressure.
• Addinganothersteptoanestablishedpracticeworkflowcantakephysicians/providerstimetorevisetheworkflow.
• Communicationandeducationforpatientsandprovidersalikeiscriticaltosuccess.Systems,processes,andtechnologycanbeputtocoordinatedusetoovercomesomeofthesechallenges.Educationcancomeintheformofautomatedtechnology,emailand/orotherdigitalplatforms,andtraining.
• Using technology to conduct quality assurance reviews of data, and minimizing delays by using bulkmessaging functions within an EHR, are additional ways to improve the process for providers andpatients.
Thiscasestudyshowsclearbenefitsofacoordinatedapproachtodevelopingandimplementingprediabetesscreening,testing,andreferralmodels.Identifyingkeypointsofcontactforpatientsandprovidershelpsfacilitatebuy-inacrossthefullspectrumofpatientcare.
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 7

IncreasingPhysicianScreening,TestingandReferralofPatientswithPrediabetestotheNationalDPPLifestyleChangeProgram 8
1NationalInstitutesofHealth.DiabetesPreventionProgramFactSheet.Retrievedfrom:https://www.niddk.nih.gov/about-niddk/research-areas/diabetes/diabetes-prevention-program-dpp2Long-termeffectsoflifestyleinterventionormetforminondiabetesdevelopmentandmicrovascularcomplicationsover15-yearfollow-up:theDiabetesPreventionProgramOutcomesStudy.Retrievedfrom:https://www.thelancet.com/journals/landia/article/PIIS2213-8587(15)00291-0/fulltext
The National Diabetes Prevention Program: TheCDC-ledNationalDiabetesPreventionProgram(NationalDPP)isapartnershipofpublicandprivateorganizationsworkingtogethertobuildanationwidedeliverysystemforalifestylechangeprogramproventopreventordelayonsetoftype2diabetesinadultswithprediabetes.TheNationalDPPprovidesaframeworkfortype2diabetespreventioneffortsintheU.S.foundedonfourkeypillars:1)atrainedworkforceoflifestylecoaches;2)nationalqualitystandardssupportedbytheCDCDiabetesPreventionRecognitionProgram;3)anetworkofprogramdeliveryorganizationssustainedthroughcoverage;and4)participantuptakeandreferral.1ThesepillarslinkcloselytotheCDC’sstrategicgoalsfortheNationalDPP:increasethesupplyofqualityprograms;increasedemandfortheprogramamongpeopleatrisk;increasereferralsfromhealthcareproviders;andincreasecoverageamongpublicandprivatepayers.1
AkeycomponentoftheNationalDPPisastructured,evidence-based,year-longlifestylechangeprogramtopreventordelayonsetoftype2diabetesinadultswithprediabetesoratriskofdevelopingtype2diabetes.1TheNationalDPPlifestylechangeprogramisfoundedonthescienceoftheDiabetesPreventionProgramresearchstudy,andsubsequenttranslationstudies,whichshowedthatmakingrealisticbehaviorchangeshelpedpeoplewithprediabeteslose5%to7%oftheirbodyweightandreducetheirriskofdevelopingtype2diabetesby58%(71%forpeopleover60yearsold).1ThegroundbreakingDPPstudyenrolled3,324overweightparticipantswithelevatedfastingandpost-loadplasmaglucoseconcentrations.Participantswererandomlyassignedtothreegroupsinthestudy:lifestyle,metformin,andplacebo.Theprimaryoutcomemeasurewasdevelopmentoftype2diabetes,diagnosedonthebasisofanannualoralglucose-tolerancetestorasemiannualfastingplasmaglucosetest.1Resultsshowedthatbothlifestylechangeandtreatmentwithmetforminreducedtheincidenceoftype2diabetesinpersonsathighriskcomparedwithaplacebo,butthelifestyleinterventionprovedmoreeffectivethanmetformininpreventingtheonsetoftype2diabetes(Diagram1).1TheDPP’sresultsalsoindicatedthatmillionsofhigh-riskadultscanpreventordelayonsetoftype2diabetesbylosingweightthroughastructuredlifestyleinterventionemphasizingregularphysicalactivityandadietlowinfatandcalories.After15yearsofstudy,participantsinthelifestyleinterventiongroupcontinuetohavea27%reducedriskofdevelopingtype2diabetescomparedtoan18%reducedriskinthemetformingroup.2

The National Diabetes Prevention Program:
Theprogramisgroup-based,facilitatedbyatrainedlifestylecoach,andusesaCDC-approvedcurriculum.Thecurriculumsupportsregularinteractionbetweenthelifestylecoachandparticipants;buildspeersupport;andfocusesonbehaviormodificationthroughhealthyeating,increasingphysicalactivity,andmanagingstress.Theprogrammaybedeliveredin-person,online,viadistancelearning,orthroughacombinationofthesedeliverymodesandconsistsof:
• Aninitialsix-monthphaseofferingaminimumof16sessionsover16to24weeks.• Asecondsix-monthphaseofferingaminimumofonesessionamonth(atleastsixsessions).• Facilitationbyatrainedlifestylecoach.• ACDC-approvedcurriculum.• Regularopportunitiesfordirectinteractionbetweenthelifestylecoachandparticipants.• Afocusonbehaviormodificationthroughhealthyeating,increasingphysicalactivity,managing
stress,andpeersupport.
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 9

CDC’sDiabetesPreventionRecognitionProgram(DPRP)isthequalityassurancearmoftheNationalDPP.ThroughtheDPRP,CDCawardsrecognitiontoprogramdeliveryorganizationsthatmeetnationalstandardsandachievetheoutcomesproventopreventordelayonsetoftype2diabetes.
AsofJuly2018,thereweremorethan1,700in-personandvirtualorganizationsintheDPRPregistrythathadenrolledmorethan230,000participants.CoveragefortheNationalDPPlifestylechangeprogramasahealthbenefitisexpanding.3AsofJuly2018,over3.4millionpublicemployeesanddependentsin19stateshadtheNationalDPPlifestylechangeprogramasacoveredbenefit,andmorethan100employersandinsurerswerecoveringtheprograminvariousmarkets.4
OnNovember2,2017,theCentersforMedicare&MedicaidServices(CMS)issuedthe2018PhysicianFeeSchedule(PFS)finalrule,whichfinalizedpoliciestoimplementtheMedicareDiabetesPreventionProgram(MDPP)expandedmodel,whichtookeffectonApril1,2018.4TheMDPPexpandedmodelallowsMedicarebeneficiarieswithprediabetestoaccesstheNationalDPPlifestylechangeprogramasacoveredservice.AnMDPPsupplierisanorganizationthatisenrolledinMedicareandcanbillforMDPPservicesprovidedtoeligiblebeneficiaries.5InordertoapplytobecomeanMDPPsupplier,anorganizationmusthavepreliminaryorfullrecognitionfromCDC’sDPRP.
3IncreasingCoveragefortheNationalDPPthroughPublicandPrivateEmployers,CommercialHealthPlans,andMedicaid.Retrievedfrom:https://www.cdc.gov/diabetes/programs/stateandlocal/resources/increasing-coverage.html4CentersforMedicare&MedicaidServices.FactSheet:FinalPoliciesfortheMedicareDiabetesPreventionProgramExpandedModelintheCalendarYear2018PhysicianFeeScheduleFinalRule.Retrievedfrom:https://innovation.cms.gov/Files/fact-sheet/mdpp-cy2018fr-fs.pdf5MedicareDiabetesPreventionProgram(MDPP):MDPPSupplierRoadMap.Retrievedfrom:https://innovation.cms.gov/Files/x/mdpp-orientation_roadmap.pdf
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 10

TostartMDPPservices,beneficiariesmusthave:• MedicarePartBcoveragethroughMedicareFee-for-ServiceoraMedicare
Advantage(MA)Plan.• Resultsfromoneofthreebloodtestsconductedwithinoneyearbeforethefirstcore
session:
--HemoglobinA1C:5.7--6.4%or--Fastingplasmaglucose:110--125mg/dLor--Oralglucosetolerancetestwithavalueof140--199mg/dl
• BodyMassIndex(BMI)ofatleast25,oratleast23ifself-identifiedasAsian• Nohistoryoftype1or2diabetes,withtheexceptionofgestationaldiabetes• NoEndStageRenalDisease(ESRD)• NotreceivedMDPPservicespreviously
Diagram 2. Requirements to Start MDPP Services
Source:https://innovation.cms.gov/initiatives/medicare-diabetes-prevention-program/)andtheMDPPoverviewfactsheet(https://innovation.cms.gov/Files/x/MDPP_Overview_Fact_Sheet.pdf)
The American College of Preventive Medicine Demonstration Projects
Infall2016,TheAmericanCollegeofPreventiveMedicine(ACPM)wasfundedbytheCDCDivisionofDiabetesTranslationtoincreasescreening,testing,andreferralofpeoplewithprediabetestoorganizationsofferingtheNationalDPPlifestylechangeprogramandparticipatingintheCDCDiabetesPreventionRecognitionProgram(CDC-recognizedorganizations).

Fortwoyears,ACPMoversawninedemonstrationprojectsforhealthcareorganizations/practiceswiththegoalsof:
1. Increasingphysicians’/healthcareprofessionals’awarenessofprediabetesasaserioushealthcondition.2. Developingandimplementingprotocolsforscreening,testing,andreferringpatientswithprediabetestoa
CDC-recognizedorganization,eitherthroughtheEHRorbyusinganothernon-electronicapproach.3. Increasingthenumberofphysicians/healthcareprofessionalstakingactiontoscreen,test,andrefer
patientswithprediabetestoCDC-recognizedorganizations(organizationswithpending,preliminary,orfullrecognition).
CriteriaforScreeningandTesting:
Source: National Diabetes Prevention Program, CDC
12
• Beatleast18yearsoldand• Beoverweight(bodymassindex≥25;≥23ifAsian)and• Havenopreviousdiagnosisoftype1ortype2diabetesand• Haveabloodtestresultintheprediabetesrangewithinthepastyear:
--HemoglobinA1C:5.7--6.4%or--Fastingplasmaglucose:100--125mg/dLor--Two-hourplasmaglucose(aftera75gmglucoseload):140--199mg/dLor
• Bepreviouslydiagnosedwithgestationaldiabetes
Prediabetescanbediagnosedviaafastingplasmaglucose,anoralglucosetolerancetest,oranA1Ctest.Blood-basedtestingisthemostaccuratewaytodetermineifapatienthasprediabetes.

ViaacompetitiveRequestforProposal(RFP)process,ACPMelectedtofundorganizationsthatrepresentedavarietyofclinicalpracticesettings,aseachsettingwaslikelytobeuniqueinthetypesofstrategiesandresourcesneededtoestablishascalablereferralmodel.Providergroupswereselectedfromeachofthethreecategorieslistedbelow,andeachprovidergroupreceived$15,000todevelopscalablemodelsforscreening,testing,andreferral.AwardrecipientsworkedwithACPMtodocumenttheirexperiencesandlessonslearnedascasestudiestoinformandteachothers.Thegranteeswereselectedfromthefollowinghealthcaresettings:CommunityHealthCentersorFederallyQualifiedHealthCenters(FQHC);FQHCLook-Alikes;RuralHealthClinics;FreeandCharitableClinics:
• FQHC:AnyproviderworkinginaFederallyQualifiedHealthCenter,asdesignatedbytheHealthResourcesandServicesAdministration(HRSA),waseligibletoapplyforthegrant.Thisincludedhealthcentersthatservehomelesspatients,farmworkerpatients,publichousingpatients,andveteranpatients.
• FQHCLook-Alike:AnyproviderworkinginaFQHCLook-Alike,asdesignatedbyHRSA,waseligibletoapplyforthegrant.
• RuralHealthClinic:AnyproviderworkinginaRuralHealthClinic(RHC),asdesignatedHRSA,waseligibletoapplyforthegrant.
• FreeandCharitableClinics:ThesearehealthclinicslocatedacrossthecountrythatdonotreceiveanyfederalfundsthataregiventoFQHCsandRHCs.Theyalsoreceivelittletonostatefunds.Anyproviderwhovolunteeredasignificantportionofhis/hertime(atleasttwodaysaweek)atafreeorcharitableclinicwaseligibletoapply.
• IndependentPhysicianAssociations(IPA)andMedicalGroups:AnyproviderinanIPApursuingopportunitiessuchascontractswithemployers,accountablecareorganizations(ACO),ormanagedcareorganizations(MCO)wasencouragedtoapply.Physiciansinmedicalgroupsalsoengagedinpatient-centeredmedicalhomes(PCMH)wereencouragedtoapply.
• IntegratedDeliverySystem(IDS):Anyproviderworkinginanintegrateddeliverysystem(IDS)thatis
verticallyandhorizontallyalignedtoprovideacontinuumofcaretoaspecificgeographicareainneedwaseligibletoapply.AnyproviderwithinanIDSthatfunctionsasanACOwasalsoeligibletoapply.
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 13

14
Duringtheinitialyearofthedemonstrationproject,ACPMselectedthreeorganizations*:• EmoryHealthcareSystem–Atlanta,GA(IDS)• WheatRidgeInternalMedicine–WheatRidge,CO(IPA)• AltaMedHealthServices–LosAngeles,CA(FQHC)
*Formoreinformationontheseorganizations,seeACPM’sYear1NationalDPPdemonstrationprojectcasestudy“IncreasingPhysicianScreening,Testing,andReferralofPatientswithPrediabetestotheNationalDiabetesPreventionProgramLifestyleChangeProgram.”
Duringthesecondyearofthedemonstrationproject,ACPMselectedsixorganizations:• NortheastMissouriHealthCenter–Kirksville,Missouri(FQHC)• ChristopherRuralHealthCorporation–Christopher,Illinois(FQHC)• MaineHealth–Portland,Maine(IDS)• SouthNassauCommunityHospital–Oceanside,NewYork(IDS)• GriffinFacultyAssociates–Derby,Connecticut(IPA)• AccentonHealth–Washington,DC(IPA)
Thiscasestudyreviewstheapproaches,barriers,andscalabilityplansofthreeofthesehealthcareorganizations:
• NortheastMissouriHealthCenter–Kirksville,Missouri(FQHC)• AccentonHealth–Washington,DC(IPA)• GriffinFacultyAssociates–Derby,Connecticut(IPA)

CASE STUDY 1
Federally Qualif ied Health Center: Northeast Missouri Health Council
NortheastMissouriHealthCouncil(NMHC)isaFederallyQualifiedHealthCenterthathasbeenprovidingservicessince1968.In2016,NMHCprovidedservicesto19,499residentsthroughfourfamilyhealthclinics,anOB/GYNclinic,apediatricclinic,aVeteransAdministrationcommunity-basedoutpatientclinic,andthreedentalclinics.NMHCprovidesaslidingfeescalefortheuninsured/underinsuredandacceptstraditionalMedicaid,MedicaidManagedCare,Medicare,andprivateinsurance.NMHC’sserviceareaincludes11countiesinnortheastMissouri,allofwhichareHealthProfessionalShortageAreas.AccordingtotheU.S.Census,over40%ofthepopulationintheserviceareaislivinginhouseholdswithincomesbelowthefederalpovertylevel.Inaddition,thepercentageofadultsintheserviceareawhoareobese(BodyMassIndexgreaterthan30)is32.4%,comparedto30.3%inMissouriand27.1%intheUnitedStates.Residentsinthe11-countyareawerediagnosedwithdiabetesatarateof11.6per100,000,alsoexceedingthenationalbenchmarkof8per100,000.6
Pre-Demonstration Project Approach
Priortothedemonstrationproject,NMHCappliedtotheCDCDiabetesPreventionRecognitionProgramandreceivedpendingrecognitionforitsNationalDPPlifestylechangeprogram.NMHCdevelopedstaffworkflowsforbothclinicvisitsandphonecallstosupportandeducatepatientswithprediabetesabouttype2diabetespreventionandthelifestylechangeprogram.
NMHCHealthInformationSystemsstaffcompletedretroactivescreeningusingtheEHRtoidentify631patientswhowereatriskofdevelopingtype2diabetesandeligiblefortheprogram.Basedonthisdata,NMHCthenextractedpatientswhowereseenbyprovidersattheNortheastFamilyHealthCliniclocatedinKirksville,Missouri,tocreateaprediabetesregistryspecificallyforthisclinic.
15
6NMHCDemonstrationProject2018MidtermReport.

Duringthedemonstrationproject,(NMHC)focusedon:
• UtilizingexistingNationalDPPmarketing,patientawareness,andscreeningandreferralresourcesfromtheCDCandorganizationssuchastheAmericanMedicalAssociation(PreventDiabetesSTATToolkit).
• Organizingandimplementingacommunication/marketingstrategytoincreaseawarenessoftheprogram,includingeducationandscreeningofpatientsandothercommunitymembersandeducationforprovidersandclinicstaff.
• Developingastandardmodelforidentificationofatargetpopulationviaretroactivescreeningoftheclinicpopulationeverysixmonths.
Eachoftheseapproachesisdescribedbelow.
Developing Awareness: Education and Screening of Patients and Community Members
NMHCutilizedavarietyofresourcestopromotetheavailabilityofscreeningandreferraltotheprogramincluding:
• Electronicbillboardwithaprediabetesawarenessmessage.
• Promotionoftheprogramatlocalfestivalsandothercommunityevents.The“CommunityRootsFestival”yieldedapproximately1,500paper-basedscreeningformscompletedbyNortheastMissouriresidentswhowerethenprovidedinformationontheNationalDPPlifestylechangeprogram.
• MeetingsheldattheclinicinpartnershipwiththeAdairCountyYMCAtoprovidebloodpressureandweightscreeningsforapproximately40-50peopleeachmonth.InformationsuchastheCDCPrediabetesRiskTestwasdistributedtoparticipants.
• Meetingsheldmonthlyattheclinicforpatientsandcommunitymemberswantingtolearnmoreabouttheprogram(SessionZeroInformationOverview).
• Postershunginclinicexamrooms(PromotingPrediabetesAwarenesstoyourPatients-providedbytheMissouriDepartmentofHealth).
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 16
Demonstrat ion Project

• Aone-pageflyerforthe65yearsofageandolderpopulationthatfocusedonthe71%type2diabetesriskreductionseeninthosewhocompletedtheoriginalDPPresearchtrial,andthecostsassociatedwithtype2diabetes(PrediabetesIsaBigDeal).
• Informationmailedtopatientstoassistwithself-referrals(CDCPrediabetesRiskTestandprogram/referralinformation).
• Paperscreeningincorporatedintotheworkflowattheclinictoassistwithreferrals(CDCPrediabetesRiskTestandprogram/referralinformation).
Developing Awareness: Education for Providers and Clinic Staff
NMHCusedthefollowingactivitiestoincreaseproviderandclinicstaffscreeningandprogramreferrals:
• TheNMHCDiabetesEducationQualityCoordinatorprovidedanoverviewoftheNationalDPPlifestylechangeprogram,outcomesoftheDPPresearchtrial,andprevalenceofprediabetesinMissouriandtheNMHCserviceareaatmonthlyNMHCproviderandstaffmeetingsandattheNortheastMissouriHealthCouncilBi-AnnualQualityImprovementmeeting.
• Duringmonthlyproviderandstaffmeetings,NMHCstaff(theDiabetesEducationQualityCoordinatorandtheReferralCoordinator)reviewedinstructionsforuseofthepaper-basedriskassessment,laboratoryvaluesforthediagnosisofprediabetes,updatesonthenumberofprogramreferralsandenrollees,andaggregatedataonparticipantoutcomes.
• NMHCproviderstookpartinmonthlyandthenbimonthlymeetingstoassistindevelopingtheworkflowforidentifyingandreferringpatients.
• NMHCstaff(theDiabetesEducationQualityCoordinatorandtheReferralCoordinator)providedfeedbacktoprovidersontheirindividualpatientsviatheEHRregardingreferrals,enrollment,andprogressinthelifestylechangeprogram.

Patient Identification
NMHCusedthePreventDiabetesSTATToolkitalgorithmtoretroactivelyscreentheirpatientpopulationforpatientseligibletoparticipateintheNationalDPPlifestylechangeprogram.HealthInformationSystemsstaffcompletedanEHRreportbasedonthefollowinginclusioncriteria:• Patientsage≥18years.• BMI≥25kg/m2;ANDpositiveresultforanyofthefollowing:HbA1c5.7–6.4%(LOINCcode1558-6)
orFPG100-125mg/dLorhistoryofgestationaldiabetes(ICD–10:Z86.32).• Exclusioncriteria:Currentdiagnosisofdiabetesorcurrentuseofinsulin.
NMHCmailedlettersandsupportinginformationtoallpatientswhoqualifiedbasedontheretroactivealgorithm.Duetothehighvolumeofreferrallettersbeingsent,theclinicdidnotcreatethelettersaspartoftheEHR.NMHCpersonalizedthelettersusingMicrosoftsoftwareandanExcelreport.Theletteraddressedthepatient’sriskofdevelopingtype2diabetesandtheprovider’srecommendationtoenrollintheNationalDPPlifestylechangeprogram.AcopyoftheCDCPrediabetesScreeningTestwasmailedwiththeletter.
NMHCsortedthereportofallqualifyingpatientsbyprovider,givingeachprovideralistofhis/herpatientswhoweredeterminedtobeatrisk.Subsequently,eachprovideridentifiedthosepatientsathighestriskofdevelopingtype2diabeteswhohadexhibitedreadinesstocommittotheprogram.Thesepatientsreceivedaphonecalltofollowupontheletterthathadbeenpreviouslymailed.Threeweeksaftermailingtheletter,iftheNMHCDiabetesPreventionProgramhadnotheardfromthepatient,thecoordinatingnurseworkingwiththeprogramfolloweduponetimeviaphone.ThenurseenteredtheprediabetesriskscreenerscoreintotheEHRandcreatedanEHRreferralifthepatientagreedtoparticipateintheprogram.
NMHCalsoidentifiedadditionalqualifyingcommunitymembersamongwomenwhowerealreadyparticipatinginotherhealtheducationprograms,includingtheShowMeHealthyWomanandtheWISEWOMANprogram.TheMissouriDepartmentofHealthandHumanServicesWISEWOMANprogramdirectorsagreedtoreimburseNMHCforthecostofWISEWOMANparticipantswhoqualifiedforparticipationintheNationalDPPlifestylechangeprogram.TheWISEWOMANprogramrequiresthattheparticipanthaveaBMIof25orgreaterandnothaveadiagnosisoftype1ortype2diabetes.AletterwassenttoallWISEWOMENparticipantswhoqualified,andnursingstaffalsoreferredWISEWOMENparticipantswithaBMI≥25totheprogram.

Altogether,1,076patientswereidentifiedforoutreachutilizingtheretrospectivequeryprocess(1,033)andfromtheWISEWOMANprogram(43).Informationwasmailedtoallidentifiedindividuals,includingtheCDCPrediabetesRiskTest,SessionZeroInformationOverview,and“PrediabetesisaBigDeal”handoutandprogram/referralinformation.The1,076patientswerebrokendownintolistsseparatedbyprimarycareprovider,dietitian,orOB/GYN.Providersthenselected93patientstoreceivefollowupbyphone.Asaresultofthemailerortelephonicfollowup,60patientscompletedtheCDCPrediabetesRiskTestandindicatedinterestinattendingaSessionZeroclassorreceivingadditionalinformationabouttheprogram(Table1).
Table 1. Patient Referrals and Enrollment
Referral Primary Category Number Referred
Number Enrolled
EHR Query: Patient contacted by phone to enroll
93
14
Point of care screening: Referred by provider; NMHC Diabetes Prevention Program employees completed final enrollment
52
20
Point of care screening: Patient received a warm hand-off to the NMHC Diabetes Prevention Program
21 of the 52 total electronic referrals
13/20 enrolled patients
Patients referred friends/family 5 TBD
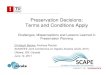
Point of Care Model Referralswerealsoinitializedatthepointofcare.Theworkflowwasdevelopedbythesteeringcommitteethroughmonthlyorbimonthlyface-to-faceandteleconferencemeetings,andthroughemailfollow-up.ThepointofcareSTAT-ToolkitguidelinesandtheAmericanAssociationofClinicalEndocrinologist/AmericanCollegeofEndocrinologyComprehensiveType2DiabetesManagementAlgorithmwereusedasoriginalsourcestoeducatethesteeringcommitteeanddeveloptheworkflowforidentifying,screening,andreferringpatients.AworkflowwasdevelopedtodeterminewhichpatientswouldreceivetheCDCPrediabetesScreeningTestasseeninDiagram4.
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 19

Diagram 4. NMHC Screening and Referral Workflow
Successes, Challenges, and Lessons Learned ThedemonstrationprojectprovidedtheopportunitytoincreaseprediabetesawarenessacrossNMHClocationsbyprovidingtrainingforhealthcareprovidersandstaff.Thetrainingsprovidedopportunitiesfornursesandstafftoaskquestionsabouttheriskfactorscontributingtothedevelopmentoftype2diabetesandincreasedtheirabilitytoidentifyandreferpatientstotheNMHCDiabetesPreventionProgram.NMHChopedtoincreasethenumberofpatientswhoenrolledintheprogrambywarmhand-offreferralby50%.Ofthe52electronicreferralscompleted,21receivedawarmhandoff,therebymeetingthegoal.
Therewerechallengesencounteredwithprovidersduringtheprojectincluding:• PrimarycareprovidersinanFQHCsettingmonitorandaddressmanyitemsatthepatient
appointment.Thus,type2diabetesriskassessmentmaynotbethehighestconcernforthepatientorprovider.
• Ittakestheprovidertimetoaddanewscreeningorprograminformationtotheirworkflowinthealreadylimitedtimeofatypicalclinicappointment.Toaddressthisbarrier,workflowsweredevelopedtoallowotherstaffmemberstoassistinidentifyingpatientsforreferralandcommunicatingthisinformationtotheproviders.
Scalability and Next Steps Attheendoftheproject,thepilotedworkflowwillbeintegratedintothepracticeofallprimarycareproviders’atallfourfamilyhealthclinicsandtheOB/GYNspecialtyclinic.Bimonthlymeetingswillcontinuetoaddressthebarrierstoprediabetesscreening,testing,andreferralateachclinicsiteorwithindividualproviders.
If the NMHC Diabetes Prevention Program did not hear from the
patient within 3 weeks, the coordinating nurse followed up with the patient telephonically
The coordinating nurse entered the prediabetes risk screener
score into the EHR A referral was created in the EHR if the patient agreed to participate in the program
Health Information Systems staff completed an EHR report based
on the inclusion criteria
Providers identified patients at highest risk of developing type
2 diabetes who exhibited program readiness
Providers were given a list of their patients who were determined to be at risk
CDC Prediabetes Screening Test mailed with the letter
Letter created in the patient’s EHR to address type 2 diabetes risk
and recommend the National DPP lifestyle change program

CASE STUDY 2
Independent Practice Association: Accent on
Health
AccentonHealth(Accent)isasmallindependentpracticeinWashington,D.C.,comprisedofonephysician,onephysicianassistant,oneofficemanager,andthreemedicalassistants.Itspatientpopulationis94%AfricanAmericanadultsovertheageof20.Themajorityofpatientsarewomen(61%),andalargemajorityofpatientsareoverweightwithmorethanonehealthcondition(80%).Approximately35%ofpatientsseenattheclinichaveadiagnosisofdiabetes.Inaddition,itisestimatedthatanadditional50%haveprediabetes.
Pre-Demonstration Project Approach Prior to the demonstration project, Accent screened for prediabetes at annual wellness visits, withhemoglobinHbA1ctestingcompletedattheproviders’discretion.Providersalsocounseledpatientswithinthepracticesetting.Demonstration Project Accentdesigneditsdemonstrationprojecttofocuson:• Developingarobustin-clinicawarenessandpromotionmodel(forprovidersandpatients)by
customizingformsandmaterialstomeettheneedsoftheclinicandpatientpopulation.
• ConductingaretroactivereviewofEHRdataeverysixmonthstoidentifypatientswithprediabetesandreferthemtoaCDC-recognizedorganization,theFlexcarePharmacyDiabetesPreventionProgram,whichwasfullyfundedbythelocaldepartmentofhealth.
• Developingaworkflowforpatientcounselingandreferral.
• WorkingwithinexistingEHRsystems(FoxMeadowsEHR)tostreamlineareferralmodel.
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 21

Developing Awareness Accentimplementedthefollowingstepstoincreaseawarenessofprediabetesandtheimportanceofscreeningwithinthepracticesetting:• Patientposterswereplacedinthewaitingarea,examrooms,breakroom,andprovideroffices.
• TheADAType2DiabetesRiskTestwasplacedinthewaitingarea.
• Patientsandcaregiverswereencourageddailytoparticipateinthescreeningprocessaspartofthecheck-inandcheck-outprocess.
Effortstokeepprovidersengagedincludedmonthlylunchmeetingsto:• Evaluateprogramsuccessandchallenges.
• Discusslong-termsustainabilityoftheeffort.
• DiscussbenefitsoftheprogramrelevanttoimprovingpatienthealthoutcomesandmeetingMACRAgoals.
Patient Identification PatientsatriskwereidentifiedthrougharetrospectiveEHRqueryutilizingthealgorithminthePreventDiabetesSTATToolkitandEHRalertsinthesystemandatthepointofcare(seeDiagrams5and6).
Retrospective Query AllpatientsidentifiedthroughtheretrospectiveEHRqueryashavingprediabeteswerenotifiedviaregularmail.TheletterscontainedgeneralinformationabouttheNationalDPPlifestylechangeprogram,itsbenefits,andanumbertocontactforclassinformation.
Point of Care PatientsweregiventheADAType2DiabetesRiskTestwhentheycheckedinfortheirappointments.Thestaffatregistrationmadesurethateachpatientdidnothaveadiagnosisofdiabetesandwasnotpreviouslyidentifiedashavingprediabetes.Ifthepatient’sriskscorewas5orhigher,achartreviewwasperformedforfurtherevaluationfocusingonrecentBMIandHbA1cvalues.
EachpatientwithaBMIandHbA1cwithinthecriteriasetforthintheSTATtoolkitwasautomaticallyflaggedinthesystemasacandidateforadditionaleducationandreferraltotheNationalDPPlifestylechangeprogram.Theprovidersreviewedthisinformationbeforegoingintotheexamrooms,discussedthebenefitsoftheprogramwiththepatient,andsignedareferralformforthepatienttoparticipateintheprogram(Table2).
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 22

Table 2. Accent Patient Referrals and Enrollment
Referral Primary Category Number Referred
Number Enrolled
Point of care: Patient was provided information to self-enroll (EHR Retrospective Query)
89
n/a
Point of care: Patient enrolled by provider/clinic staff
39
38
Patient letter (total)
128
Other n/a
Diagram 5. Accent Retrospective EHR Review
EHR Review
Contact Patients
Fol low Up

Diagram 6. Accent Point of Care Workflow
Successes, Challenges, and Lessons Learned ThrougharetrospectivereviewofEHRdataandregularofficevisits,806patientelectronicrecordswerereviewed,and128patientswerediagnosedwithprediabetes.Ofthosediagnosedwithprediabetes,38enrolledintheFlexcarePharmacyDiabetesPreventionProgramwhichwasfullyfundedbythelocaldepartmentofhealth.TheSTATtoolkitwaseffectiveinscreeningforprediabetesinaprimarycaresetting,andtherewaslittleornoeffectondailyofficeworkflowduringtheimplementationoftheproject.
Therewerechallengesduringtheimplementationofthedemonstrationprojectthatpotentiallylimitedthereferralandenrollmentprocess.TheEHRsoftwareprovideratthetimeofthecasestudywasFoxMeadows.Thesoftwareproviderwasnotfamiliarwithprediabetesscreening,andthesoftwarewasnotdesignedtoincorporateprediabetesscreeningintheEHR.Thus,therewasnoeasyaccesstotheinformationbyprovidersandotherstaff.TherewasalsonodedicatedsectionintheEHRtotrackscreeninganddocumentfollowupefforts.Therewerealsochallengeswithreimbursementforbloodglucosetesting.ThesuggestedCPTcodes(i.e.CPTcode:99401)werenotveryhelpfulinbillingforprediabetestesting/abnormalbloodglucose,andonlytwoclaimswerereimbursedbyinsurancecompaniesusingthecodesprovided.
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 24
Provide patient with
CDC-recognized organization’s contact
information
Follow up with patient and CDC-recognized
organization
Check Out See Provider
Discuss prediabetes results
Discuss benefits of National DPP lifestyle change program
Sign referral form
Provide patient with health literature
Sign In
Prediabetes questionnaire
Check insurance coverage
BMI
Check lab for HbA1c
Flag System

LessonsLearned:• Establisharelationshipwiththeseorganizationsearlyonandobtaininformationontheirclass
schedules.• Anewsoftwareprogramandamoreexperiencedteamhandlingallbillingquestionsandconcerns
arecrucialforsuccess.• Localdepartmentsofhealthcanassistinpromotingtheprogramifinvolvedearlyintheprocess.• Peerleadersanddiabeteseducatorscanalsohelpinpromotingtheprogram.• ItisimportanttoverifythatthereareCDC-recognizedorganizationsinthecommunity,andthattheseprogramsare
abletomeettheneedsofpatientsreferredwithinareasonabletimeframe.• Thepracticemustcontinuetomakethisprogramaprioritytoensureitssuccess.
Scalability and Next Steps Accentisconsideringthefollowingnextsteps:• ChangingtonewEHRsoftwarewithbettercapabilitiestohandlepreventiveefforts.Accent’sexisting
systemwasnotdesignedtohandlesuchaninitiativeinaneffectivemanner.Upgradesrequiredwerecostprohibitive.
• Revisitingreimbursementconcernsforbloodglucosetesting.• AssigningadedicatedstaffmembertofollowupwithenrolledpatientsandwiththeCDC-recognized
organizationonaquarterlybasis.• Stayinginvolvedwiththelocaldepartmentofhealthtotakeadvantageofanyassistanceoffered.• LearningmoreabouttheMedicareDiabetesPreventionProgram.
25

CASE STUDY 3
Independent Practice Association: Griffin Faculty Physicians
GriffinFacultyPhysicians(GFP)hassevenprimarycareofficeswithatotalpatientpanelof20,978.AllofficesarerecognizedasPatientCenteredMedicalHomes.Primarycareprovidersareattendingphysicians,residentphysicians,physicianassistants,andnursepractitionersspecializingininternalmedicineorfamilymedicine.GFPprimarycareofficesacceptmostmajorinsuranceplans.Approximately63%ofpatientshaveprivateinsurance,22%areMedicaid-Connecticutbeneficiaries,14%haveMedicare,and2%areself-pay.Eachprimarycareofficeprovidesgeneralmedicalcare,routinehealthexams,immunizations,labtesting(includingin-officeHbA1ctesting),andreferralstospecialistsandGriffinHospitalpreventionprogramsandsupportgroups.7
GriffinHospitalservesthelowerNaugatuckValleyRegion(“theValley”)ofConnecticut,comprisedofthetownsofAnsonia,BeaconFalls,Derby,Naugatuck,Oxford,Seymour,andShelton.TheValleytownsrepresentthediversityofthe169townsinConnecticut,withsomeconsideredurbanperipherytowns(Ansonia,Derby,andNaugatuck),rural-liketowns(BeaconFallsandSeymour),andhigher-incomesuburbantowns(OxfordandShelton).
Pre-Demonstration Project Approach Priortothedemonstrationproject,therewasnopractice-widesystematicscreeningforprediabetesatGFPoffices.Screeningandreferralsweredependentuponeachprovider’sclinicaljudgment.GriffinisaCDC-recognizedorganizationandofferedtheNationalDPPlifestylechangeprogrampriortothedemonstrationproject.ReferralstothisandotherCenterforPreventionandLifestyleManagement(CPLM)programsofferedthroughtheoutpatientclinicwerehandledthroughtheEHR.Inadditiontothediabetespreventionprogram,patientswithprediabeteswerereferredtoaregistereddietitianformedicalnutritiontherapy/nutritionassessmentandmanagementasneeded.
7GriffinFacultyPhysiciansDemonstrationProject2018MidtermReport

Demonstrat ion Project GFPdesignedthedemonstrationmodeltofocuson:
• Developingpractice-widesystematicscreeningforprediabetesatGFPoffices.• Modifyingexistingpublicdomainresourcestosupporttheprediabetesscreening,testing,andreferral
model.
Provider Engagement Beforeapplyingforthedemonstrationproject,theDirectoroftheCenterforPreventionandLifestyleManagementatGriffinHospital(CenterDirector)metwithseveralkeymembersoforganizationleadershiptoobtaintheirbuy-infortheproject,particularlytheDirectorofPrimaryCareforGriffinFacultyPhysiciansandtheVicePresidentforAccountableCare.TheCenterDirectordiscussedtheproposedprogramwiththeGFPdataleadandRN/MAQualityleadwhotrainsthemedicalassistantsandhelpsensurethatqualitymeasuresaremet.Theideaofusinganewpre-visitplanningformemergedfromthesemeetings.Whendemonstrationprojectfundingwasreceived,theCenterDirectormetwiththeprimarycareproviderstoexplaintheproject,elicitedtheirfeedbackandconcerns,anddiscussedhowtoaddressthem.
AreferencesheetforprovidersandstaffwasdevelopedthatincludedinformationontheNationalDPP,thedemonstrationproject,aswellaspatientinsuranceco-payinformationthattheproviderscoulddiscusswiththepatient.Throughouttheprocess,theCenterDirectormetwiththeDirectorofPrimaryCareandcapitalizedonstrategicopportunitiestospeakwithprimarycareprovidersandstaff.
Developing Awareness GFPutilizedthefollowingmaterialstodevelopawarenessoftheprogramwithinthehospitalsystemandthecommunity(AppendixA):
• CDCNationalDPPpatientbrochures/handouts• CDCNationalDPPpostersandinfographicsinclinicrooms• CDCNationalDPPoverviewinformationforproviders
ThematerialspromotedawarenessofprediabetesandtheNationalDPPamongproviders/staffandpatients.Additionally,presentationswereconductedatproviderandstaffmeetingstopromoteawarenessofprediabetesandtheNationalDPP,andtoorientthemtothenewclinicworkflow.
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 27

Patient Identif ication TheGFPscreeningapproachwasamodifiedcombinationofthe“retrospectiveprediabetesidentification”andthe“point-of-careprediabetesidentification”8modelsnotedinthePreventDiabetesStatToolkit.Specifically,GFPutilizedtheplanningplatformdevelopedbyitsEHRconsultant,SymphonyRM.Forthisproject,SymphonyRMcreateda“prediabetesmodule”forthepre-visitplanning(PVP)tool.Insteadofgeneratingalistofpatientsneedingprediabetesscreening(“retrospectiveEHRquery”),thePVPformalertedprovidersoftheneedforprediabetestesting(donebythemedicalassistant;“point-of-careprediabetesidentification”),ortheneedtodiscussreferraltotheNationalDPPlifestylechangeprogramwithpatientswhometthecriteriaforprediabetes.
Theworkflowforidentifyingpatientswithprediabetesbeganwithscreeningallpatients≥45yearsofageorwithaBMI>25kg/m2(>23kg/m2inAsianAmericans).Theageof≥45wasbasedontheAmericanDiabetesAssociation’s2017StandardsofMedicalCareinDiabetescriteriafordiabetesscreening.
Screen9(1)allpatientsage≥45OR(2)withBMI≥25kg/m2(≥23kg/m2inAsianAmericans)ANDoneormoreofthefollowingriskfactors:1. Firstdegreerelativewithdiabetes2. High-riskethnicity(AfricanAmerican,Latino/Hispanic,AmericanIndian,AlaskanNative,AsianAmerican,
PacificIslander)3. Womenwithhistoryofgestationaldiabetesordeliveringababy>9pounds4. Historyofcardiovasculardisease5. Hypertensiondiagnosis6. HDLcholesterollessthan35mg/dLand/ortriglyceridelevel>250mg/dL7. Womenwithpolycysticovariansyndrome
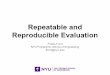
Retrospective Query Intheretrospectiveidentification(Diagram7),theEHR/patientdatabasewasqueriedtoscreenforprediabetesamongpatientswhometthecriteria.Inthepoint-of-careidentification,ifapatientwasage18orolderanddidnothavediabetes,ascreeningtestwasadministered,andbloodglucosetestingwasordereddependentuponthepatient’srisk.
8CentersforDiseaseControlandPreventionandAmericanMedicalAssociation.Preventingtype2Diabetes:Aguidetoreferyourpatientswithprediabetestoanevidence-basedpreventionprogram(PreventDiabetesSTATtoolkit).Retrievedfromhttps://www.cdc.gov/diabetes/prevention/pdf/stat_toolkit.pdf9AmericanDiabetesAssociation.Classificationanddiagnosisofdiabetes.Sec.2.InStandardsofMedicalCareinDiabetes2017.DiabetesCare2017;40(Suppl.1):S11–S24
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 28

GFPcreateda“prediabetesmodule”forthepre-visitplanningtoolthatutilizedthecriteriabelowtogenerateanalertinthePVPformindicatingthatthepatientneedsprediabetestesting(HbA1cin-officeduringthevisit),orneedstheprovidertodiscusstheNationalDPPlifestylechangeprogramandinitiateareferral.Insteadofcreatingalistofpatientsneedingprediabetestesting,thePVPformautomaticallygeneratedanalertforprediabetestestingorreferraltotheprogramforpatientswhometthecriteriabasedontheAmericanDiabetesAssociation’s2018StandardsofDiabetesCare.
Point of Care Prediabetesscreeningandtestingwasincorporatedintothepre-visitplan.Eachtimeapatientatriskfortype2 diabetes came to the clinic, the patient record was flagged, and the provider had a discussion with thepatientatthepointofcare.
TwotypesofpatientswouldtriggerareferraltotheNationalDPPlifestylechangeprogram:(1)apatientwithanHbA1cof5.7-6.4duringthevisitOR(2)apatientwithoutapreviousHbA1cinthecurrentyearwhowasflaggedbythepre-visitplanningtoolasneedinganHbA1ctest,andsubsequentlyhadanHbA1cintheprediabetesrange(5.7-6.4).Forthesetwotypesofpatients,themedicalassistantalertedtheprimarycareprovideroftheneedtodiscusstheNationalDPPlifestylechangeprogram,andtomakeareferralintheEHRifthepatientwasinagreement.
Alternatively,ifthepatientwasnotreadytocommittotheNationalDPPorwasinterestedinotherinterventions,thePCPreferredthepatienttotheCPLMIntakeCoordinatorwhoexplainedthedifferentprogramsavailable.
ReferralstoallCenterforPreventionandLifestyleManagementprograms,includingGriffin’sCDC-recognizeddiabetespreventionprogram,wereincorporatedinthereferralsectionofGFP’soutpatientEHR,Athenanet.Whenaproviderorderedareferraltothediabetespreventionprogram,afaxwassenttotheGriffinHospitalDiabetesEducatorandDiabetesPreventionProgramFacilitatorwhocontactedthepatientregardingenrollingintheprogram.GFPalsoupdatedtheEHRtotrackwhenaproviderdiscussedareferraltothediabetespreventionprogramandthepatientwasnotreadytocommit.
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 29
Pre-Visit Planning Whendesigningthescreeningprotocol,GFPaddedelementsthatwerealreadyinplaceintheirclinicworkflowateachGFPoffice.AspartofPatientCenteredMedicalHomecertification,eachofficeutilizedapre-visitplanningtool/formthatflagsfortheofficestaffwhatneedstobedoneforeachpatientathis/herupcomingvisit.Priortothedemonstrationproject,thepre-visitplanningtool/formdidnotflagpatientswhowereatriskfortype2diabetesforprediabetesscreeningortesting.

Diagram 7. GFP Retrospective Prediabetes Identification Process
Generate a l ist of patient names with relevant information
*BMIcriteriahavechanged(now>25,or>23ifAsian)Source:PrediabetesSTATToolkit,AMA/CDC
Successes, Challenges, and Lessons Learned GFPdidnotmoveforwardwiththescreeningandreferralprocessfortheNationalDPPlifestylechangeprogram.Therewasadelayinimplementingtheprediabetesmoduleofthepre-visitplanningform/toolduetoconcernsraisedbyproviders(e.g.,financialburdenofthebloodglucosetestonpatients,inconsistentproviderknowledgeandcomfortwithICDcodestoensureHbA1ctestingiscovered,andtimingofthetesting),whichGFPhasaddressed.
- Current diagnosis of diabetes (ICD-9: 259.xx) or - Current insulin use
b. Exclus ion cr iteria:
o OGTT 140-199 mg/dl (LOINC code 62856-0) or - History of gestational diabetes (ICD-9: V12.21)
o FPG 100-125 mg/dl LOINC code 1558-6) or o HbA1c 5.7 - 6.4% (LOINC code 4548-4) or
- A Positive lab test result within previous 12 months: - Most recent BMI ≥ 24* (≥22 if Asian) and - Age ≥ 18 years and
a. Inc lusion cr iteria:
Query EHR or patient database every 6-12 months us ing the fol lowing cr iteria:
Measure
- Program Coordinator wil l contact patient directly, and
c. Flag medical record for patient’s next office v isit
b. Send patient info to diabetes prevention program provider
a. Contact patients to inform of risk s tatus, explain prediabetes , and share info on diabetes prevention programs, and/or
Use the pat ient list to:
Act
Discuss program participat ion at next visit
GFPfirstwantedtoaddressproviderconcernsbeforemovingforwardwiththeprediabetesmoduleoftheirpre-visitplanningform,sothatstaffandprovidersareengagedandunderstandthatGFPvaluestheirfeedbackandwantstopartnerwiththemthroughouttheprocess.Duetothisaim,therewerenoreferralsorenrollmentintheNationalDPPlifestylechangeprogramduringthedemonstrationproject.
30
Partner

Onelessonlearnedfromthisprojectwasthatitisessentialtousethe“teach-backmethod”toensurethesoftwarevendorcandeveloptheneededsystemenhancements.Themethodconsistsofaskingtheconsultant/softwaredeveloperto“teachback”/sharetheirunderstandingofthealgorithm.Anotherlessonistomakesurethereisdirectcommunicationwiththeindividualresponsibleforwritingthecode.Asaresultofthesechallenges,GFPpreferredtodelaylaunchingtheprocess,bothtoensureaccuracyofresultsforpatientsandalsocontinuedandsustainedbuy-infromthestaffandproviders.
Three key lessons learned during the GFP demonstration project were: 1. Createandpromoteacollaborativeprocess:
-Empowerstakeholdersintheprocess(listen,iteratefromfeedback,monitor).-Useandmaximizeexistingtools.
2. DemystifytheNationalDPP,andshowcasethepoweroflifestylechange:-Narrativesarepowerful.-Emphasizepatientempowerment.
3. FacilitateeaseofreferralandenrollmentintheNationalDPPlifestylechangeprogram:-IncorporateaprocessforreferralwithintheEHR.-Identifypointsofcontact(forpatientsandproviders).
Whiletherewerechallenges,GFPalsohadsuccessesthroughouttheprocess:PrediabetesInformationSession:Theprediabetesinformationsessionisacommunity-basedinformationsessionwhereparticipantslearnaboutprediabetesandtheNationalDPP.Thesessionwasverywell-receivedbyparticipatingpatientsandthecommunity.GFPplanstohostatleasttwosessionsperyeartoincreasepatientandcommunityawarenessofprediabetesandtheNationalDPPlifestylechangeprogram.GFP’sgoalwastodemystifyprediabetesandtheNationalDPPandencourageandempowerpatientstomakelifestylechangesthathelppreventtype2diabetes.Sessionparticipantsnotedenjoyingbeingabletolearnaboutthepathophysiologyofdiabetes(“mini-medschool”lesson),beingabletoaskpracticalquestionsabouthealthynutrition/lifestylechange,hearingfromindividualswhosuccessfullycompletedtheNationalDPPlifestylechangeprogram,andbeingabletoaskspecificquestionsabouttheprogramcomponentsanditslength.
Scalability and Next Steps ThedifferentcomponentsofthedemonstrationprojectarenowembeddedintheclinicsysteminawaythatwillpromoteawarenessofprediabetesandtheNationalDPPamongpatientsandthecommunity,increasedetectionofprediabetesusingthepre-visitplanningtool(continuingtoiterateandmakesureitisaccurate),includetheseprocessesintheworkflowofthemedicalassistantandtheprimarycareprovider,andcontinuetomaintainbuy-infromtheDirectorofPrimaryCareandotherleadershipandstaffatGFP.Forthelatter,theDirectorcontinuestomeetwithtrainers/qualitycareleadsaswellaswiththeDirectorofPrimaryCareandthemaincontactpersonatSymphonyRM(theconsultantswhodevelopedthepre-visitplanningtool,)andattendsprimarycareprovidermeetingstocontinuetoeducateontheprocess.Additionally,residentsarerequiredtoreviewinformationonallCPLMprograms.
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 31

Learningfromthisdemonstrationproject,GFPwillcontinuetoincreasepatientawarenessofprediabetesandtheNationalDPPlifestylechangeprogramusingthefollowingmethods.• Newsletter:GFPwillhavetwonewslettercampaignsonprediabeteseachyear,onceinthespring
andonceinthefall.Thenewsletterwillbeapersonalizedletter(seeAppendixA)fromthepatient’sprimarycareprovideraddressingvarioushealthtopics,includingprediabetes(seeAppendixA).ThenewsletterwillalsoincludetheADAType2DiabetesRiskTest.GFPprimarycarenewslettersreachthewholepatientpopulationofthepracticegroup,approximately20,000patients.Allpatientswithemailaddressesonfilewillreceivethenewsletterviaemailblast.
• TargetedEmailBlast:Inadditiontothenewsletter,GFPhasfoundthatatargetedemailblastisanothermeanstoincreaseawarenessaboutprediabetesandrelatedinformationsessions,especiallywhentimedappropriately.
• PrediabetesInformationSession:ThisisaparticularlypowerfulwayofincreasingpatientawarenessandcomfortwithsigningupfortheNationalDPPlifestylechangeprogram.Themaingoalofthesesessionsistoempowerpatientswithknowledgethattype2diabetescanbepreventedwithlifestylechange,andthatothershavesucceededinreducingtheirriskthroughtheNationalDPPlifestylechangeprogram.GFPanticipates10-40communitymembersperinformationsession.
AnothergoalistodemystifytheNationalDPPlifestylechangeprogram.Movingforward,GFPwillkeeptheformatoftheinformationsessionusedduringthedemonstrationproject:• Duration:1hour(mimicsthelengthofaNationalDPPlifestylechangeprogramclasssession)• Topics/sectionscoveredduringthesession:
• Prediabetes/diabetesandlifestylechange(speaker(s):internalmedicine/preventivemedicinephysiciansand/orprimarycarephysician)
• TheNationalDPPlifestylechangeprogramanditscomponents(speaker:diabeteseducator)• TheNationalDPPexperienceandlong-termchange/testimonial(speaker(s):1-2program
graduates)
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 32

Summary of Challenges
Thegranteesfacedanumberofchallengesandhaveuncoveredanumberofvaluablelessonslearned.Someencountereddelaysinimplementationduetoconcernsraisedbyproviders.TheconcernsincludedthefinancialburdenofbloodglucosetestingonpatientsandlimitedknowledgeandlackofcomfortwithrelevantICDcodestoensureHbA1ctestingiscovered.
Moreover,thereweredelaysinestablishingpartnershipswithkeystakeholders,suchaslocaldepartmentsofhealth,tocollaborateonpromotingtheNationalDPPlifestylechangeprogram,insomecasesbecauseofthetimeittooktoidentifythedecisionmakersandappropriateleaderswhocouldprovidetheneededsupport.ThegranteesalsoexperienceddifficultiesadjustingEHRsoftwareprogramstoincludethenecessaryworkflowtosupportprediabetesscreening,testing,andreferralandtoaddressbillingissuesforscreeningandtesting.
Retrospectivequeriestoidentifypatientsathighriskfortype2diabetestookmoretimethanexpectedduetoanumberofreasons.Forexample,onegranteehadtoconductin-depthchartreviewstoobtaincompleteinformationtodeterminewhetherpatientsmetprogrameligibilitycriteria.Insomecases,patientswereconfusedduetolackofcommunicationpriortocurrentoutreachefforts.intheprogramOutreachcallswereunwelcomeorincompleteifstaffwereunabletoleavethepatientavoicemail,orifthephonenumberwaswrongorwasoutofservice.Infact,agenerallackofpatientawarenessofprediabetes/diabeteswasfound.Therewasalsoalackofproviderawarenessoftheimportanceofprediabetesscreening,testing,andreferraltoaCDC-recognizedorganizationofferingtheNationalDPPlifestylechangeprogram.
Somepatientportalsystemsrequiredtoomanystepsforpatientstogetintothesystemtocompleteariskassessment.Inaddition,therewereconcernsaboutaskingpatientstofillout“onemorequestionnaire,”andconcernsoverHIPPAcomplianceissues.
Thechallengeofaddressingmanyitemsatthepatientappointmentattimesdetractedfromthescreening,testing,andreferralprocess.
Evenaslocalchampionssupportedprogramefforts,theyencounteredchallengesinmakingtheNationalDPPlifestylechangeprogramanongoingpriorityamongothercompetingpriorities.
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 33

Summary of Successes
As a result of conducting these demonstration projects, grantees identified several promising practices forproviders and clinical systems. These practices i speak to the similarities in health care delivery despitevariationsinpatientpopulations,organizationtype,orinsurancecoverageacrossthedifferentlocations.
GiventheprevalenceofprediabetesanddiabetesintheUnitedStates,atype2diabetesriskassessmentneedstobeincorporatedintotheroutine,standardworkflowofclinicstaffservingpopulationsathighrisk.Onceaworkflowisrepeatedmanytimesandbecomesroutine,itiseasierforstafftoimplement,anditismorelikelytobeimplementedcorrectly.Giventhemanycompetingdemandsduringaprimarycarevisit,itisallthemoreimportantthattheriskassessmentbecomemoreofaroutine,baselinetaskthatiscomfortableforallstaff–notunlikeweighingthepatient,takingbloodpressure,oraskingabouttobaccouse.
Ideally,theproviderisawareoftheriskassessment,incorporatestheinformationintothepatientchart,andactsontheresultsinawaythattherapeuticallysupportspatientaccesstoevidence-basedprevention,includingareferraltotheNationalDPPlifestylechangeprogram.However,becauseaproviderreferralisnotarequirementforparticipationintheNationalDPP,itisalsoidealthattheprovidernotactasabarriertopatientaccess.Thus,ifapatientmeetsthecriteriaforreferralviatheirriskassessmentscore,thepatientshouldbereferredtoaCDC-recognizedorganization,evenifthepatientandproviderdonothavetimetodiscussthereferral–whichmaybealltoocommonduringabusyclinicvisit.Thus,othersupportstaffshouldbeempoweredtoreferpatientswhomeetprogrameligibilitycriteria.Dependingonstatelicenseregulations,alliedhealthprofessionalsmaybeempoweredtoorderappropriatebloodglucosetesting,ifneeded.Theuseof“standingorders,”writtenofficeprotocols,orotherstandardworkflowdocumentshelpclarifyexpectationsinateam-basedcareand/ormultidisciplinaryclinicenvironment,andsupportongoingqualityassuranceandqualityimprovementexercises.

Empoweringalternatestafftoassistinscreeningandreferralsalsocreatesopportunitiesforthesestafftoscreenandreferwhentheyinteractwithpatientsoutsideofthetraditionalofficevisit.Examplesofsuchinteractionsincludewhenpatientscallforappointments,areremindedaboutappointments,aregivenresultsoverthephone,orcomeinforotherservicessuchasimmunizationsorfluvaccines.Theseinteractionsmightbefurthersupportedwithstandardscriptsorhealtheducationmaterialsthatcanbeusedbyalliedhealthstaff.Themanyinteractionsthatthesestaffhavewithpatientsoutsideofthetraditionalofficevisitusuallyinvolvedocumentation,whichaffordsanopportunitytoreviewbasicinformationintheEHRthatcanbehelpfulincompletingatype2diabetesriskassessment(e.g.age,race/ethnicity,pastmedicalhistory[i.e.gestationaldiabetes],currentproblemlist[highbloodpressure,obesity,etc.],familyhistoryoftype2diabetes,BMI,andperhapsevenbloodglucosevalues).Thus,ariskassessmentmaybeeasilycompletedonbehalfofapatientorcompletedwithveryfewquestions.IdentifyingeligiblepatientsmaythenautomaticallypromptareferraltoaCDC-recognizedorganizationoraproviderappointmenttodiscusstype2diabetesrisk.
Eveninaclinicthatemploysatype2diabetesriskassessmentasapartofthestandardworkflowduringpatientregistrationorrooming,therewillbemissedopportunitieswhentheriskassessmentorreferralisforgotten,misplaced,misunderstoodbythepatient,misinterpretedbystaff,ornotcarriedoutbecausethepatientsimplydoesnotpresentattheclinic.Empoweringalliedhealthorsupportstafftoemployaprotocol/standardworkflowinavarietyofsettingsoracrossmultiplepatientinteractionshelpsensurecompletionofthetask,despitehumanerror.
Aswithotheressentialhealthcareservices,qualityassurancetoolsandregularchecksshouldbebuiltintotheprocess.Standardworkflowdocumentsand/orprotocolsareessentialfortrainingandreference.Checklistsanddocumentationtools,includingpreformattednotetemplatesortextmacrosforanEHR(e.g.“smartphrases”or“dotphrases”),arealsohelpfulfortheday-to-dayworkofinteractingwithpatientsanddocumentingintheEHR.Theteamneedstoconductqualityassurancereviewsofdatagathered,suchasverifyingheightandweightandcheckingforfamilyhistoryupdates.Identifyingandcollectingdatarelatedtothegoalofthisproject(increasingprediabetesscreening,testing,andreferraltoaCDC-recognizedorganization)–andthenreviewingthesedataatregularintervals–isnotapartofroutineworkatmostclinics.Howevercollectingandreviewingsuchdataisintegraltoanyqualityimprovementeffort.
35

Focusingonwrittenprocessesandworkflowstoimprovetheefficiencyorexpediencyofprediabetesscreening,testing,andreferralisalsoessential.Forexample,theprocessofcheckingforpatienteligibilitycriteriaviaachartreviewmaybeexpeditedbyutilizingthebulkmessagingfunctionwithintheEHRtogeneratelettersappropriately.EHRsystemsthatsupportthehealthteamcanmakeatremendousdifferenceintermsofcollatingandprovidingcriticalinformationandremindersatthepointofcare.SomeEHRscanbesetuptocalculateriskautomaticallyandcreateremindersoralertsinthepatient’schart.SupportstaffandproviderscanbetrainedontheserelevantfieldsandfunctionalitywithintheEHR.WorkflowscanbedevelopedthatallowstaffmembersotherthanphysicianstoassistinidentifyingpatientseligiblefortheNationalDPPlifestylechangeprogram,initiatingreferrals,andcommunicatingwithprimarycareprovidersaboutthesereferrals.
Effectivecommunicationamongallmembersofthehealthcareteamnotonlyhelpsinitiatenewworkflows,butcanalsohelpinformadjustmentstoimproveexistingworkflows,makingthemsustainableandsuccessfuloverthelongterm.Examplesofeffectivecommunicationincludethefollowing:
1. Conductingmeetingswithmedicalleadership,qualityimprovementleaders,clinical“champions”fromdifferentdisciplines,andmanagers/trainersformedicalassistantsandotheralliedhealthstafftoensureleadershipandmanagementsupport.
2. Conductingpresentationsforprovidersatbothregularclinic-levelmeetingsandspecialeducationaleventsfocusedoncontinuingeducationorqualityimprovement.
3. Holdinginitialmeetingstoeducateallmembersofthehealthcareteamandtoelicittheirconcernsandinputonanydesiredchangesinworkflow.
4. Providingupdatesatregularintervalsonthesuccessesandchallengesandimprovementideasfortheworkflowaftertheprojecthasbegun.
5. Leveragingexistinghealthsystemandhealthteamcommunicationportals,includingmeetings,newsletters/publications,emails,andmailerstopatientsand/orstaff/employees.
Beforeinitiatingaprediabetesscreening,testing,andreferraleffort,thehealthsystemorclinicmustidentifyamultidisciplinaryteamofNationalDPP“champions”whowillhelppromotetheprogramandsupporteffortstoimplementsystematicscreening,testing,andreferralprotocols.ThesechampionsneedtoverifythatpatientshaveaccesstoaCDC-recognizedorganizationofferingclasseslocallyoronline,andthattheseprogramscanmeettheneedsofpatientsinareasonabletimeframe.ThiscanbedonebysettingupregularcommunicationwithactiveCDC-recognizedorganizationsservingyourtargetpopulation.Championsmustalsoactivelypromotetheprogram;conductongoingprediabetesinformationsessions;continuallyanswerquestionsandhelptroubleshoot;andprovidereferencematerialsappropriateforproviders,staff,andpatients.Effectivecommunicationandcollaborationwithproviders,staff,administrators,andconsultantsiscrucial,andmustincludetakingtimetoaddresstheconcernsofkeystakeholders.
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 36

Table 3. Summary of Challenges and Lessons Learned
Pro
vid
er
Co
nce
rns
Chal lenges Key Lessons Learned • The financial burden of HbA1c testing on
patients, and limited knowledge and lack of comfort with relevant ICD codes to ensure the cost of HbA1c screening is covered
• Making the National DPP lifestyle change program an ongoing priority among other competing priorities
• Concerns over HIPPA compliance issues
• Effective collaboration is a must; take time to address the concerns of key stakeholders.
De
lays
• Delays in implementation due to provider concerns
• Delays in establishing partnerships with key stakeholders, such as local departments of health to collaborate on promoting the program
• Look at steps that can minimize delays (e.g. minimizing chart review time by utilizing the bulk messaging function within the EHR to generate letters).
Co
mm
un
icat
ion
/A
war
en
ess
• A general lack of patient awareness of prediabetes/diabetes
• Lack of provider awareness of the importance of prediabetes screening, testing, and referral to a CDC-recognized organization offering the National DPP lifestyle change program
• Communication and education for both patients and providers is essential.
• Provider education is necessary to introduce the National DPP and explain how to utilize the risk score in screening patients for type 2 diabetes.
• To assure system-wide change occurs, local champions must get buy-in from senior leadership, as well as from staff and primary care providers.
• Champions must also promote the necessary materials and tools for providers and staff to use.
Tech
no
logy
• Difficulties adjusting EHR software programs to include the necessary workflow and to address billing issues for screening / testing.
• Patient portal systems requiring too many steps for the patient to get into the system to complete a risk assessment.
• Electronic systems can be set up to calculate risk automatically and place an alert in the health maintenance field.
• Train staff on any new, relevant fields created within the EHR.
• Incorporate referral functionality within the EHR.
Pro
cess
es
and
W
ork
flo
ws
• Recruitment processes, such as retrospective queries, requiring more time than expected
• Addressing many items during the patient appointment detracting from the screening, testing, and referral process.
• Providers challenges in adjusting to new workflows.
• Workflows can be developed that allow staff members other than primary care providers to assist in prediabetes screening, testing, and referral.
• Incorporate screening, testing, and referral protocols into the regular work flow of primary care providers and allied health staff.
• Verify that patients have access to CDC-recognized organizations offering classes locally or online.
• Identify key points of contact for patients and providers.
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 37

Conclusion
Inatwo-yearprojectfocusedonstrengtheningandinstitutionalizingpracticestosupportprediabetesscreening,testing,andreferraltoCDC-recognizedorganizationsofferingtheNationalDPPlifestylechangeprogram,theAmericanCollegeofPreventiveMedicineworkedwithninehealthcareorganizations/practices.
Threeoftheseorganizationswerehighlightedinthiscasestudy,whichreviewedtheirapproaches,barriers,andscalabilityplans:• NortheastMissouriHealthCenter–Kirksville,Missouri(FQHC)• AccentonHealth–Washington,DC(IPA)• GriffinFacultyAssociates–Derby,Connecticut(IPA)
Thegoalssetoutfortheprojectweretoincreasephysicians’/healthcareprofessionals’awarenessofprediabetesasaserioushealthcondition;developandimplementprotocolsforscreening,testing,andreferringpatientswithprediabetestoaCDC-recognizedorganization;andincreasethenumberofphysicians/healthcareprofessionalstakingactiontoscreen,test,andreferpatientswithprediabetestoCDC-recognizedorganizations(organizationswithpending,preliminary,orfullrecognition).
ChallengesandlessonslearnedfromtheNortheastMissouriHealthCenterinclude:• Additionaltrainingsprovidedopportunitiesfornursesandstafftoaskquestionsabouttheriskfactors
contributingtothedevelopmentoftype2diabetes.• Type2diabetesriskassessmentmaynotbethehighestconcernforthepatientorproviderattheinitial
appointmentwithaprimarycareprovider.
• Addingscreeningsornewinformationtoanexistingworkflowinthealreadylimitedtimeofatypicalclinicappointmentcanbechallenging.Workflowsweredevelopedtoallowotherstaffmemberstoassistinidentifyingpatientsforreferralandcommunicatingthisinformationtotheproviders.
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 38

ChallengesandlessonslearnedfromAccentonHealthinclude:• Thesoftwareusedintheenrollmentprocessmayhavelimitedidentificationandreferralofpatients
withprediabetes,becauseitwasnotdesignedtoincorporateprediabetesscreeningintotheEHR.Accentidentifiedtheneedforanewsoftwareprogramandamoreexperiencedteamtohandlebillingquestionsandconcerns.
• Therewerechallengeswithreimbursementforbloodglucose(HbA1c)testing.• LocaldepartmentsofhealthneedtobeinvolvedearlyintheprocesstoassistinpromotingtheNational
DPP.Peerleadersanddiabeteseducatorscanalsohelpinpromotingtheprogram.
ChallengesandlessonslearnedfromtheGriffinFacultyAssociatesPrograminclude:
• InordertofacilitateeaseofreferralandenrollmentintheNationalDPPlifestylechangeprogram,referralfunctionalityisneededwithintheEHR.
• The“teach-backmethod”isnecessarytoensurethesoftwarevendorcandevelopneededsystemenhancements.Directcommunicationwiththeindividualresponsibleforwritingthecodeisalsocritical.
• Acollaborativeprocessisnecessarytoempowerstakeholdersintheprocessanduseandmaximizeexistingtools.
• NarrativesarepowerfulandcanemphasizepatientempowermenttodemystifytheNationalDPPandshowcasethepoweroflifestylechange.
Insummary,thecasestudyfoundthatchallengesandbestpracticesweresimilardespitethediversityamongparticipatinghealthcaresystems/practicesingeographiclocation,patientpopulations,andinsurancecoverage.Providerconcerns,delays,communication/awareness,technology,andprocesses/workflowwerethekeyareasidentifiedandaddressedbythehealthcareorganizationsinthiscasestudy.
Notably,improvedcommunicationandworkflowswereidentifiedastwomainthreadsacrossalltherecommendationsandpromisingpractices.Increasedandimprovedcollaborationbetweenprovidersisessentialtosystem-wideadoptionofnewworkflows.CommunicationandeducationforbothpatientsandprovidersisessentialandcancomewithadoptionofnewtechnologyandtoolsavailablethroughEHRs.Also,forsuccessfulprograms,championsareneeded.Championsareoftenkeyleadershipataclinicorhealthorganizationandareintegraltoincreasingbuy-infromalllevelswithintheorganization,promotingtheuseofnewmaterialsandimplementingandsupportingnewworkflowsandprocesses.
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 39

Resources
Centers for Disease Control and Prevention (CDC) 1. CDC National Diabetes Prevention Program - https://www.cdc.gov/diabetes/prevention/index.html 2. What Is the National DPP? - https://www.cdc.gov/diabetes/prevention/about/index.html 3. Implement a Lifestyle Change Program (for Professionals) -
https://www.cdc.gov/diabetes/prevention/lifestyle-program/index.html 4. Screen & Refer Patients to a Lifestyle Change Program (for Professionals)-
https://www.cdc.gov/diabetes/prevention/lifestyle-program/deliverers/index.html
5. Requirements for CDC Recognition - https://www.cdc.gov/diabetes/prevention/lifestyle-program/requirements.html
6. =
American College of Preventive Medicine (ACPM) 7. Diabetes Prevention Program Resource Center- https://www.acpm.org/page/dppresources 8. ACPM Diabetes Prevention Program Initiatives – www.acpm.org/page/dpp
Centers for Medicare & Medicaid Services (CMS) 9. Medicare Diabetes Prevention Program website - https://innovation.cms.gov/initiatives/medicare-diabetes-
prevention-program/ 10. Medicare Diabetes Prevention Program (MDPP) Medicare Advantage Fact Sheet -
https://innovation.cms.gov/Files/fact-sheet/mdpp-ma-fs.pdf 11. Medicare Diabetes Prevention Program (MDPP) Expanded Model Fact Sheet -
https://innovation.cms.gov/Files/x/MDPP_Overview_Fact_Sheet.pdf
American Medical Association (AMA) 12. Preventing Type 2 Diabetes - https://www.ama-assn.org/delivering-care/preventing-diabetes 13. Prevent Diabetes STAT™ Toolkit - https://preventdiabetesstat.org/toolkit.html 14. What Physicians Can Do to Prevent Diabetes - https://www.ama-assn.org/delivering-care/advocating-
diabetes-prevention#What%20Physicians%20Can%20Do%20to%20Prevent%20Diabetes
American Diabetes Association (ADA) 15. Diagnosing Diabetes and Learning About Prediabetes- http://www.diabetes.org/are-you-at-
risk/prediabetes/?loc=atrisk-slabnav 16. Type 2 Diabetes Risk Test - http://www.diabetes.org/are-you-at-risk/diabetes-risk-test/ 17. Tools to Know Your Risk- http://www.diabetes.org/are-you-at-risk/tools-to-know-your-risk/?loc=atrisk-
slabnav 18. Practice Resources - http://www.diabetes.org/research-and-practice/practice-resources/?loc=rp-slabnav
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) 19. Diabetes Prevention Program (DPP) - https://www.niddk.nih.gov/about-niddk/research-
areas/diabetes/diabetes-prevention-program-dpp 20. Preventing Type 2 Diabetes - https://www.niddk.nih.gov/health-
information/diabetes/overview/preventing-type-2-diabetes
Increasing Physician Screening, Testing, and Referral of Patients with Prediabetes to the National DPP Lifestyle Change Program 40