Embed Size (px)
Citation preview

ARTHRITIS & RHEUMATISMVol. 43, No. 12, December 2000, pp 2818–2822© 2000 American College of Rheumatology
INCREASED RISK OF DEVELOPING ANKYLOSING SPONDYLITISAMONG FIRST-BORN CHILDREN
P. BAUDOIN, I. E. VAN DER HORST-BRUINSMA, A. J. DEKKER-SAEYS, S. WEINREICH, P. D. BEZEMER,and B. A. C. DIJKMANS
Objective. Studies in mice have demonstrated anincreased risk of ankylosing enthesopathy in earlierlitters compared with later-born offspring. In humans,birth order and maternal age as risk factors for anky-losing spondylitis (AS) have not been investigated pre-viously. This study was undertaken to investigatewhether first-born children have a higher risk of ASthan later-born children and whether maternal age atdelivery is another risk factor.
Methods. The birth order of 162 AS patients wascompared with that of their healthy siblings, both forthe total group and with stratification for maternal ageat first delivery. Maternal age at the time of delivery ofAS patients who were first-born children was comparedwith the mean maternal age at first delivery in theDutch population.
Results. The number of first-born children withAS was significantly higher than would be expected incase of an equal risk between first-born and later-bornchildren (26 versus 20 for families with 2 children [P 5550.029] and 63 versus 47.6 for all families [P 555 0.004]).Also, the mean maternal age at first delivery was lowerin mothers of AS patients (24.8 years) compared withmothers of healthy controls (26.1 years).
Conclusion. Low birth order is a risk factor for ASin humans.
Most rheumatic diseases are thought to be theresult of multifarious events because environmental and
genetic circumstances seem to influence the risk ofdisease onset. In reactive arthritis the disease starts afteran infection of the gastrointestinal or urogenital tract.Environmental factors, like infections, seem to influencethe onset of spondylarthropathy in combination withgenetic factors, which contribute strongly to the onset ofankylosing spondylitis (AS) (1,2). Although HLA–B27 ismost commonly associated with AS, non-B27 geneticfactors are of pathogenetic importance as well (3–5).
Multiple sclerosis (MS) is another chronic in-flammatory disease whose development cannot be ex-plained by a single known environmental or geneticfactor (6,7). Birth order has been considered as apossible predisposing factor in MS because, in somestudies, low birth order has been associated with in-creased risk of the disease (8–10). Low birth order wasalso found to be associated with the development ofrheumatoid arthritis (RA) in 1 study (11).
However, no studies have addressed birth orderas a modifying factor in susceptibility to AS in humans.In an HLA–B27 transgenic mouse model, it was dem-onstrated that the risk of ankylosing enthesopathy (AE)in offspring was related to birth order (12). Mice thatwere born when the mother was young (,8 months ofage) had a higher risk of AE compared with the off-spring of older mothers (.8 months of age). Therefore,offspring born in earlier litters had a higher risk of AE.This phenomenon has not previously been investigatedin humans.
The aim of the present study was to assesswhether birth order itself, maternal age at the time ofbirth, or both are risk factors for AS in humans. Thefocus was on 2 questions. First, is the number of ASpatients who are first-born offspring increased com-pared with the number who are later-born offspring?Second, is the maternal age at first delivery amongmothers of AS patients lower than the age of mothers ofhealthy controls at first delivery?
P. Baudoin, MD, I. E. van der Horst-Bruinsma, MD, B. A. C.Dijkmans, MD: University Hospital, Vrije Universiteit, Amsterdam,The Netherlands; A. J. Dekker-Saeys, MD: Jan van Breemen Institute,Amsterdam, The Netherlands; S. Weinreich, MD: Central Laboratoryfor Blood Transfusion, Amsterdam, The Netherlands; P. D. Bezemer,BSci: University Hospital Vrije Universiteit, Amsterdam, The Neth-erlands.
Address reprint requests to I. E. van der Horst-Bruinsma,MD, University Hospital Vrije Universiteit, Department of Rheuma-tology, PO Box 7057, 1007 MB Amsterdam, The Netherlands.
Submitted for publication February 3, 2000; accepted inrevised form July 28, 2000.
2818

PATIENTS AND METHODS
Patient ascertainment. AS patients were recruitedfrom the Jan van Breemen Institute, an outpatient clinic andreferral center for ambulatory rheumatic disease patients inthe region of Amsterdam. Only patients with definite AS whohad at least 1 sibling were included. Definite AS was definedaccording to the modified New York criteria (13). One hun-dred eighty-seven patients were randomly selected from adatabase containing all 810 patients of the Institute with adiagnosis of AS who had had an outpatient visit within the 2years prior to initiation of the study.
Data collection. After confirmation of the diagnosis ofAS by review of the medical record, review of pelvic radio-graphs, and physical examination, the 187 patients were con-tacted by telephone and asked to complete a questionnaire.This included questions concerning the time of onset of firstsymptoms, the date of birth of the mother, and informationconcerning the siblings, e.g., birth order, age, and history ofAS. HLA–B27 typing was performed serologically in thepatients with definite AS.
In cases in which a history of AS in a sibling wasreported, it was decided not to confirm this diagnosis byphysical or radiologic examination because these relatives didnot visit the Institute. Therefore, these siblings of patients withdefinite AS were considered to have possible AS. Althoughthis study focused primarily on patients with a confirmeddiagnosis of definite AS, an additional analysis of the risk ofAS in first-born children was performed using data from all ASpatients (definite and possible combined), although the resultsmight be less reliable.
Apart from birth order itself, the influence of the ageof the mother at the time of delivery as an independent riskfactor for AS was studied. This was done by comparing themean maternal age at the time of delivery of first-born ASpatients with the mean maternal age at the time of delivery offirst-born healthy controls. Data on the mean age of mothers attime of their first delivery were obtained from The Nether-lands Central Department of Statistics (14) for the years1950–1960, the same decade in which the majority of thestudied AS patients were born. A second analysis of maternalage as an independent risk factor for AS was performed byclassifying the mothers of AS patients according to low versushigh maternal age at the time of delivery and comparing thebirth order of AS patients in the 2 groups.
Statistical analysis. The number of patients needed toidentify a clear increase in the frequency of first-born statusamong AS patients (i.e., 60% rather than 50% among familieswith 2 children) with 80% power is 152 when using thestatistical methods described below with a 5% significancelevel. The number needed for families with various sibshipsizes is lower.
Because of the large variability of birth orders (sibshipsize 2–14) and because an increased risk of AS among first-born children was expected, the patients were grouped asfirst-born versus not first-born. After stratification by familysize, the number of children with definite AS who werefirst-born that would be expected on the basis of an equaldistribution within birth orders was computed. The observedand expected numbers were compared using a 1-sided x2 test,both for families with 2 children and for all family sizes taken
together. In 1 family, there were 2 patients with definite AS,and 1 of them was chosen at random for this study. Asmentioned above, a second analysis was done in the same way,using data from patients with definite AS combined with datafrom their siblings with possible AS.
The mean maternal age at time of first delivery amongthe mothers of patients with definite AS was compared withthe mean age at first delivery in the Dutch population in thesame decade (14) by computing a 95% confidence interval forthe AS mothers. The birth order of AS patients whose motherswere younger (,25 years) at first delivery was compared withthe birth order of patients whose mothers were older ($25years).
RESULTS
Of the initial 187 randomly selected outpatientswith a confirmed diagnosis of definite AS, 25 could notbe included in the study: 9 had moved away, 8 could notbe located, 1 refused to participate, 6 did not have anysiblings, and 1 was randomly excluded because he had asibling who also had definite AS (as described above).Therefore, 162 patients with definite AS were eligiblefor the study. In the 162 families, there were 729 children(37% female), and the number of children in the fami-lies ranged from 2 to 14. Thirty-nine percent of the 162patients with definite AS were first-born (Table 1).There was no significant difference in sex ratio, medianage, or age at disease onset between first-born andlater-born patients.
HLA typing was performed in 96% of the pa-tients with definite AS. Of those typed, 88% were B27positive (87% of the male patients and 89% of thefemale patients).
Stratification of the patients with definite AS byfamily size (Table 2) showed that the prevalence offirst-born children was significantly higher than would beexpected based on an equal risk of AS among first-bornand later-born children. For instance, in the 40 families
Table 1. Characteristics of patients with definite AS stratified bybirth order (first-born versus later-born)*
Characteristic
First-born(n 5 63[39%])
Later-born(n 5 99[61%])
Total(n 5 162[100%])
% male 81 83 82Age 53 (29–79) 52 (19–79) 52 (19–79)Age of mother at time of
delivery24.8 (17–36) 31 (18–45) 28 (18–45)
Age at first symptoms 24 (9–46) 20 (8–65) 21 (8–65)% HLA–B27 positive 87 90 88
* Definite ankylosing spondylitis (AS) 5 a confirmed diagnosis of ASaccording to the modified New York criteria (13). Except whereotherwise indicated, values are the median (range) years.
BIRTH ORDER AND AS 2819
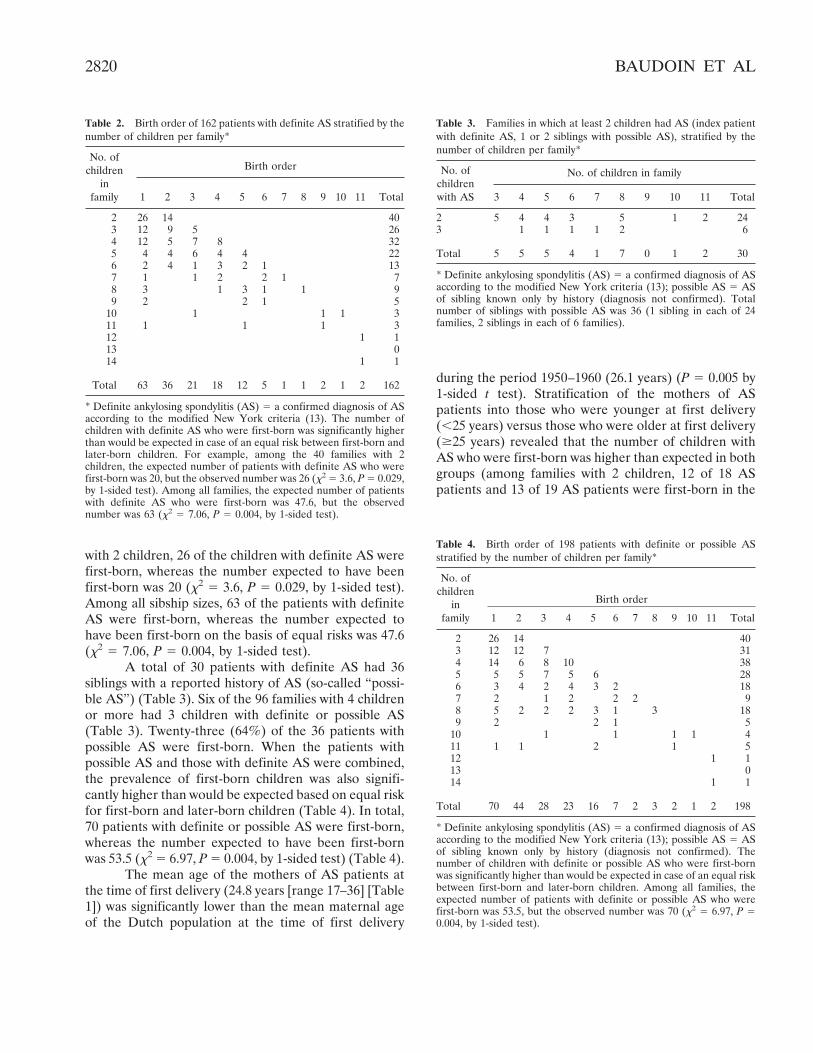
with 2 children, 26 of the children with definite AS werefirst-born, whereas the number expected to have beenfirst-born was 20 (x2 5 3.6, P 5 0.029, by 1-sided test).Among all sibship sizes, 63 of the patients with definiteAS were first-born, whereas the number expected tohave been first-born on the basis of equal risks was 47.6(x2 5 7.06, P 5 0.004, by 1-sided test).
A total of 30 patients with definite AS had 36siblings with a reported history of AS (so-called “possi-ble AS”) (Table 3). Six of the 96 families with 4 childrenor more had 3 children with definite or possible AS(Table 3). Twenty-three (64%) of the 36 patients withpossible AS were first-born. When the patients withpossible AS and those with definite AS were combined,the prevalence of first-born children was also signifi-cantly higher than would be expected based on equal riskfor first-born and later-born children (Table 4). In total,70 patients with definite or possible AS were first-born,whereas the number expected to have been first-bornwas 53.5 (x2 5 6.97, P 5 0.004, by 1-sided test) (Table 4).
The mean age of the mothers of AS patients atthe time of first delivery (24.8 years [range 17–36] [Table1]) was significantly lower than the mean maternal ageof the Dutch population at the time of first delivery
during the period 1950–1960 (26.1 years) (P 5 0.005 by1-sided t test). Stratification of the mothers of ASpatients into those who were younger at first delivery(,25 years) versus those who were older at first delivery($25 years) revealed that the number of children withAS who were first-born was higher than expected in bothgroups (among families with 2 children, 12 of 18 ASpatients and 13 of 19 AS patients were first-born in the
Table 2. Birth order of 162 patients with definite AS stratified by thenumber of children per family*
No. ofchildren
infamily
Birth order
1 2 3 4 5 6 7 8 9 10 11 Total
2 26 14 403 12 9 5 264 12 5 7 8 325 4 4 6 4 4 226 2 4 1 3 2 1 137 1 1 2 2 1 78 3 1 3 1 1 99 2 2 1 5
10 1 1 1 311 1 1 1 312 1 113 014 1 1
Total 63 36 21 18 12 5 1 1 2 1 2 162
* Definite ankylosing spondylitis (AS) 5 a confirmed diagnosis of ASaccording to the modified New York criteria (13). The number ofchildren with definite AS who were first-born was significantly higherthan would be expected in case of an equal risk between first-born andlater-born children. For example, among the 40 families with 2children, the expected number of patients with definite AS who werefirst-born was 20, but the observed number was 26 (x2 5 3.6, P 5 0.029,by 1-sided test). Among all families, the expected number of patientswith definite AS who were first-born was 47.6, but the observednumber was 63 (x2 5 7.06, P 5 0.004, by 1-sided test).
Table 3. Families in which at least 2 children had AS (index patientwith definite AS, 1 or 2 siblings with possible AS), stratified by thenumber of children per family*
No. ofchildrenwith AS
No. of children in family
3 4 5 6 7 8 9 10 11 Total
2 5 4 4 3 5 1 2 243 1 1 1 1 2 6
Total 5 5 5 4 1 7 0 1 2 30
* Definite ankylosing spondylitis (AS) 5 a confirmed diagnosis of ASaccording to the modified New York criteria (13); possible AS 5 ASof sibling known only by history (diagnosis not confirmed). Totalnumber of siblings with possible AS was 36 (1 sibling in each of 24families, 2 siblings in each of 6 families).
Table 4. Birth order of 198 patients with definite or possible ASstratified by the number of children per family*
No. ofchildren
infamily
Birth order
1 2 3 4 5 6 7 8 9 10 11 Total
2 26 14 403 12 12 7 314 14 6 8 10 385 5 5 7 5 6 286 3 4 2 4 3 2 187 2 1 2 2 2 98 5 2 2 2 3 1 3 189 2 2 1 5
10 1 1 1 1 411 1 1 2 1 512 1 113 014 1 1
Total 70 44 28 23 16 7 2 3 2 1 2 198
* Definite ankylosing spondylitis (AS) 5 a confirmed diagnosis of ASaccording to the modified New York criteria (13); possible AS 5 ASof sibling known only by history (diagnosis not confirmed). Thenumber of children with definite or possible AS who were first-bornwas significantly higher than would be expected in case of an equal riskbetween first-born and later-born children. Among all families, theexpected number of patients with definite or possible AS who werefirst-born was 53.5, but the observed number was 70 (x2 5 6.97, P 50.004, by 1-sided test).
2820 BAUDOIN ET AL

younger-mother group and the older-mother group,respectively).
DISCUSSION
From the results of this study, it can be concludedthat 1) the prevalence of AS among first-born children issignificantly higher than expected on the basis of equalrisks for first- and later-born children and 2) maternalage at first delivery among mothers of AS patients issignificantly lower than maternal age at first delivery inthe overall Dutch population. Stratification of the moth-ers of AS patients according to younger age versus olderage at the time of first delivery revealed an increasedrisk of the disease in first-born children of mothers inboth groups.
The pathogenetic mechanism that might explainthese observations remains unknown. It can be hypoth-esized that both maternal age and birth order influencesusceptibility to AS by delaying childhood infectionstoward an age at which the immune system is morevulnerable to derangement and these infections mightinduce chronic inflammatory diseases such as AS. Theinfluence of maternal age at delivery in AE has beenobserved in an experimental transgenic mouse model,which showed that the risk of AE was inversely corre-lated with the age of the mother at the time of delivery(12). The mechanism for this susceptibility in mice wasthought to be related to the higher level of antibodies inolder mice compared with the younger animals. Theantibodies in older mothers might offer a higher protec-tion in the offspring against infections related to AE. Inhumans, however, the association between lower mater-nal age and increased susceptibility to AS does not seemto be as strong as was observed in the mouse model. Thisdifference might be related to the fact that the fertilelifespan in humans is relatively shorter than in mice,making it unlikely that there is a large difference inlevels of antibodies.
Another interesting mechanism that might ex-plain the risk of AS in relation to birth order is theinduction of HLA–B27 antibodies from B27-positivechildren in a B27-negative mother who is pregnant. Infuture pregnancies the level of B27 antibodies in themother might be increased, and these might be trans-ferred to the fetus during pregnancy and alter thepathogenetic role of the B27 molecule. Further studiesshould focus on these antibodies, which might diminishthe risk of AS onset in later-born children.
The relationship between birth order and onsetof AS may be due to an increased risk of infections at a
higher age in children with lower birth orders comparedwith children with higher birth orders, who are easilyinfected by their older siblings. Exposure to infection ata young age may occur more frequently in children witholder siblings who attend school or other programs withgroups of children (9). In the absence of older siblings,there may be a delay in the occurrence of childhooddiseases, and the child might be more vulnerable toderangements of the immune system if infections occurat a later age. There are some indications that repeatedinfections may inhibit the proliferation of Th2 clonesand increase the proliferation of Th1 clones (15,16).Therefore, delay in the age at which infections occurmay increase the risk of autoimmune diseases andTh2-mediated conditions such as atopic diseases. Tworecent studies on hay fever and asthma showed thatsmall family size and low birth order make childrenmore prone to these diseases (17,18). The prevalence ofmeasles infections, increased by multiple sibling con-tacts, was found to reduce the risk of atopy (17). Theresults of these studies may, however, be confounded bythe fact that high socioeconomic level is associated withhigher maternal age at the time of the first delivery aswell as with smaller family size, although the risk ofasthma seems to be associated with lower socioeconomiclevel.
There have been no other studies addressing thesubject of birth order and the risk of AS in humans, butan effect of low birth order has been observed in RA (in1 study [11]) and in MS (8–10,19–21). The reportedresults concerning the effect of birth order on the risk ofMS, however, are contradictory. A relationship betweenlow birth order and Hodgkin’s disease has been de-scribed in 1 report (22).
Being first-born and having a mother who isyounger at the time of delivery both seem to be associ-ated with an increased risk of developing AS, possiblycaused by differences in development of the immunesystem. It remains to be seen whether the currentgeneral trend toward an increase in the mean maternalage at first delivery will decrease the risk of AS.
REFERENCES
1. Brewerton DA, Hart FD, Nicholls A, Caffrey M, James DCO,Sturrock RD. Ankylosing spondylitis and HLA-B27. Lancet 1973;11:904–7.
2. Rubin LA, Amos CI, Wade JA, Martin JR, Bale SJ, Little AH, etal. Investigating the genetic basis for ankylosing spondylitis: link-age studies with the major histocompatibility complex region.Arthritis Rheum 1994;37:1212–20.
3. Brown MA, Kennedy LG, MacGregor AJ, Darke C, Duncan E,Shatford JL, et al. Susceptibility to ankylosing spondylitis in twins:
BIRTH ORDER AND AS 2821

the role of genes, HLA, and the environment. Arthritis Rheum1997;40:1823–8.
4. Feltkamp TE. Non-HLA B27 genetic factors in HLA-B27 associ-ated diseases. Clin Rheumatol 1996;15 Suppl 1:40–3.
5. Miele W. HLA DR4 in ankylosing spondylitis with differentpatterns of joint involvement. Ann Rheum Dis 1985;44:39–44.
6. Sadovnick AD, Ebers GC. Genetics of multiple sclerosis. NeurolClin 1995;13:99–118.
7. Kurzke JF. Epidemiological evidence for multiple sclerosis as aninfection. Clin Microbiol Rev 1993;6:382–427.
8. Gaudet JPC, Hashimoto L, Sadovnick AD, Ebers GC. A study ofbirth order and multiple sclerosis in multiplex families. Neuroepi-demiology 1995;14:188–92.
9. Isager H., Andersen E., Hyllested K. Risk of multiple sclerosisinversely associated with birth order position. Acta Neurol Scand1980;61:393–6.
10. Alperovitch A, le Canuet P, Marteau R. Birth order and risk ofmultiple sclerosis: are they associated and how? Acta NeurolScand 1981;63:136–8.
11. Sayeeduddin S, Ishaq M, Rao URK. Birth order effect in rheu-matoid arthritis [letter]. Br J Rheumatol 1994;33:598–9.
12. Weinreich S, Hoebe B, Ivanyi P. Maternal age influences risk forHLA-B27 associated ankylosing enthesopathy in transgenic mice.Ann Rheum Dis 1995;54:754–6.
13. Van der Linden S, Valkenburg HA, Cats A. Evaluation of
diagnostic criteria for ankylosing spondylitis: a proposal for mod-ification of the New York criteria. Arthritis Rheum 1984;27:361–8.
14. Centraal Bureau voor de Statistiek. Vademecum gezondheidsstatistiek. Amsterdam; 1995. p. 92.
15. Mosmann TR, Coffman RL. TH1 and TH2 cells: different pat-terns of lymphokine secretion lead to different functional proper-ties. Annu Rev Immunol 1989;7:145–73.
16. Romagni S. Induction of TH1 and TH2 responses: a key role forthe natural immune response? Immunol Today 1992;13:379–81.
17. Lewis SA, Britton JR. Measles infection, measles vaccination andthe effect of birth order in the aetiology of hay fever. Clin ExpAllergy 1998;28:1493–500.
18. Rona RJ, Hughes JM, Chinn S. Association between asthma andfamily size between 1977 and 1994. J Epidemiol CommunityHealth 1999;53:15–9.
19. Visscher BR, Liu K-S, Sullivan CB, Valdiviezo L, Detels R. Birthorder and multiple sclerosis. Acta Neurol Scand 1982;66:209–15.
20. Hanrahan PS, Russell AS, McLean DR. Ankylosing spondylitisand multiple sclerosis: an apparent association? J Rheumatol1988;15:1512–4.
21. Zilber N, Kutai-Berman M, Kahana E, Korcyn AD. Multiplesclerosis and birth order. Acta Neurol Scand 1988;78:313–7.
22. Gutensohn N, Cole P. Childhood social environment andHodgkin’s disease. N Engl J Med 1981;304:135–40.
2822 BAUDOIN ET AL












![Ankylosing spondylitis and related conditions - NHS Wales1].pdf · Condition Ankylosing spondylitis Ankylosing spondylitis and related conditions This booklet provides information](https://img.pdfslide.us/doc/110x75/5d53eb2788c993a4728b841d/ankylosing-spondylitis-and-related-conditions-nhs-1pdf-condition-ankylosing.jpg)