Embed Size (px)
Citation preview

Editorial
Increased iron in HCV infection: Collateral damageor antiviral defense?
Sebastian Mueller*
Department of Medicine and Center for Alcohol Research, Liver Disease and Nutrition, Salem Medical Center, University ofHeidelberg, Zeppelinstraße 11 – 33 69121 Heidelberg, Germany
See Article, pages 995–999
Despite two decades of research in antiviral therapy, we still havenot overcome a roughly 50% failure rate in the treatment ofpatients infected with the hepatitis C virus (HCV). Understandingthe interactions between host and virus seems to be a prerequi-site for any new therapeutic approach. Multiple axes of interac-tion have been suggested: cytokines, alterations of intracellularsignaling and metabolism e.g. of fatty acids. An imbalanced ironhomeostasis is another one: pathological iron deposits have beenobserved in about 50% of patients with chronic HCV infection.Increased hepatic iron stores are not a mere innocent bystander,but an important independent risk factor for the development ofhepatocellular cancer (HCC) in HCV-infected patients [1]. In addi-tion, we have learnt from hereditary hemochromatosis that ironoverload is one of the most profibrogenic and carcinogenic fac-tors increasing the risk of HCC by approximately 200-fold [2].The combination of free iron and reactive oxygen species (ROS)leads to the production of highly toxic hydroxyl radicals via theFenton reaction causing severe cell damage. Since increasedhepatic oxidative stress is considered a key factor in chronicHCV infection and coexists with increased levels of iron, progres-sion of liver disease by toxic radicals is very likely.
The underlying mechanisms of the hepatic iron accumulationin HCV-infected livers are still poorly understood and availabledata remain mostly descriptive: parenchymal iron accumulationin HCV patients has been linked to suppressed levels of the sys-temic iron hormone hepcidin [3,4]. These studies suggest thatiron accumulation by HCV is somehow comparable to hereditaryhemochromatosis where an inadequate hepcidin response toreplenished iron stores is a key feature [5] leading to unrestrictedduodenal iron absorption and iron release from macrophages viathe iron transporter ferroportin [6]. In addition, several othergenes previously not related to iron metabolism are also dis-cussed that potentially contribute to iron accumulation in HCV[7].
The work of Fillebeen and Pantopoulos in the present issue ofthe Journal of Hepatology leads the discussion about iron andHCV one step further, by demonstrating that iron directly blocksviral replication [8]. In the previous work the authors had shownthat iron can exert direct antiviral effects. Thus, iron binds tightly
Journal of Hepatology 20
⇑ Tel.: +49 6221 483 210; fax: + 49 6221 484 494.E-mail address: [email protected]
to NS5B, the RNA-dependent RNA polymerase of HCV, andinhibits its catalytic activity by displacing magnesium from theenzymatically active site [9]. The authors validated these findingsin a subgenomic HCV replicon model, where administration ofexogenous iron blocked viral replication and attenuated the pro-duction of viral RNA and proteins [9]. More interestingly, the datasuggested that expression of the subgenomic HCV replicon leadsto an iron-poor phenotype in host Huh7 cells, possibly to bypassthe iron-dependent block in viral replication [10]. In the presentissue of the Journal, they show that the administration of exoge-nous iron drastically inhibits the progression of HCV infection inpermissive Huh7.5.1 cells, obviously independent of the HCVgenotype.
These findings deserve particular attention in light of clinicaldata where HCV patients with hereditary iron overload, due tomutations in HFE, paradoxically respond better to antiviraltherapy [11–13]. Despite potential disturbances in macrophagefunction due to iron overload, it is tempting to speculate thatincreased hepatic iron content may contribute to viral RNA clear-ance and antagonize the relapse of HCV infection following ther-apy (Fig. 1). Fillebeen and Pantopoulos suggest, in anotherpublication [10], that HCV-infected hepatocytes tend to accumu-late iron which suppresses viral infection while the virus hasstrategies to eliminate iron (Fig. 1). While increasing intracellulariron levels reduced HCV replication, preloading of Huh7.5.1 cellswith iron failed to protect them against HCV infection, suggestingthat the iron bound to ferritin is unavailable for binding to NS5Band the active agent is free intracellular iron only. To achieve spe-cific intracellular iron loading and to avoid potentially confound-ing effects of heme oxygenase 1, the authors used a specific cellpermeable iron donor (Fe-SIH) instead of the routinely usediron-donor hemin. This specific iron donor may also explain themore profound effects on viral replication as compared to previ-ous reports using FeCl3 or iron-loaded lactoferrin.
Why then does iron overload secondary to HCV or otherchronic liver diseases such as alcoholic liver disease not improve,but rather worsen the clinical outcome?
Iron-induced oxidative stress very likely plays a major role.Iron is known to affect immune responses and cytokine produc-tion [14]. Moreover, the distribution of hepatic iron varies consid-erably between primary and secondary iron overload states andcould also affect the clinical outcome. Thus, in hereditary
10 vol. 53 j 990–992

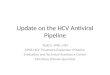
Fig. 1. Iron accumulation of an HCV-infected hepatocyte as an antiviralstrategy? Among other sources, ROS are generated by NADPH-dependentoxidases of innate immune cells (NOX1) and hepatocytes (NOX4) in HCV infectedlivers. This oxidative stress eventually leads to intracellular iron accumulation viasuppressed hepcidin or activation of IRP1 or TfR1. This iron can clear thehepatocyte from the virus since iron is a potent inhibitor of viral replication. Incontrast, infection with the hepatitis C virus leads to an iron-depleted hepatocytephenotype via still unknown mechanisms. IRP1, iron regulatory protein 1, TfR1,transferrin receptor 1.
JOURNAL OF HEPATOLOGY
hemochromatosis, iron is almost exclusively deposited in paren-chymal cells while in secondary iron overload, including transfu-sional siderosis, excess iron is stored mainly in macrophages. Thismay explain why excess iron appeared to improve antiviral ther-apy in HCV-infected patients with hereditary hemochromatosis[11–13] but not in patients with secondary iron overload suchas ß-thalassemia [15]. Likewise, intravenous iron administrationdoes not improve the virological response of hemodialyzedHCV-infected patients to antiviral therapy [16]. Consequently,the inhibitory effects of iron on HCV replication may not beexploitable for simple treatment strategies. This complex situa-tion may also explain why studies, that analyzed the beneficialeffects of iron depletion (phlebotomy) on the progression ofHCV, reported contradictory results and still warrant confirma-tion in larger cohorts [17,18].
What could be the molecular mechanisms driving iron accu-mulation in chronic HCV infection? Interestingly, ROS do not onlycontribute to the toxicity of iron but can directly lead to its intra-cellular accumulation using specific signaling sequences. This hasbeen demonstrated at various regulatory levels e.g. via activationof iron regulatory protein 1 [19], suppression of hepcidin [20], ordirect translational activation of transferrin receptor 1 [21]. Theconcept summarized in Fig. 1 suggests that hepatocytes activelyaccumulate iron via specific ROS-induced mechanisms as partof their innate antiviral immunity while the virus has found
Journal of Hepatology 201
evolutionary strategies to suppress iron accumulation via stillunknown mechanisms. Much more needs to be learnt about thedetailed molecular mechanisms of iron accumulation and ROSgeneration during HCV infection. Unraveling where protectiveiron accumulation turns into harmful iron overload will be oneof the challenging tasks for the future. Only then we will be ableto use the modulation of iron metabolism wisely in order to sup-port antiviral strategies.
Conflict of interest
The author declared that he does not have anything to discloseregarding funding or conflict of interest with respect to thismanuscript.
References
[1] Ko C, Siddaiah N, Berger J, Gish R, Brandhagen D, Sterling RK, et al. Prevalenceof hepatic iron overload and association with hepatocellular cancer in end-stage liver disease: results from the National Hemochromatosis TransplantRegistry. Liver Int 2007;27:1394–1401.
[2] Kowdley KV. Iron, hemochromatosis, and hepatocellular carcinoma. Gastro-enterology 2004;127:S79–S86.
[3] Fujita N, Sugimoto R, Takeo M, Urawa N, Mifuji R, Tanaka H, et al. Hepcidinexpression in the liver: relatively low level in patients with chronic hepatitisC. Mol Med 2007;13:97–104.
[4] Nishina S, Hino K, Korenaga M, Vecchi C, Pietrangelo A, Mizukami Y, et al.Hepatitis C virus-induced reactive oxygen species raise hepatic iron level inmice by reducing hepcidin transcription. Gastroenterology 2008;134:226–238.
[5] Lee PL, Beutler E. Regulation of hepcidin and iron-overload disease. Annu RevPathol 2009;4:489–515.
[6] Nemeth E, Ganz T. The role of hepcidin in iron metabolism. Acta Haematol2009;122:78–86.
[7] Hagist S, Sultmann H, Millonig G, Hebling U, Kieslich D, Kuner R, et al. Invitro-targeted gene identification in patients with hepatitis C using agenome-wide microarray technology. Hepatology 2009;49:378–386.
[8] Fillebeen C, Pantopoulos K. Iron inhibits replication of infectious hepatitis Cvirus in permissive Huh7.5.1 cells. J Hepatol 2010:995–999.
[9] Fillebeen C, Rivas-Estilla AM, Bisaillon M, Ponka P, Muckenthaler M, HentzeMW, et al. Iron inactivates the RNA polymerase NS5B and suppressessubgenomic replication of hepatitis C virus. J Biol Chem 2005;280:9049–9057.
[10] Fillebeen C, Muckenthaler M, Andriopoulos B, Bisaillon M, Mounir Z, HentzeMW, et al. Expression of the subgenomic hepatitis C virus replicon alters ironhomeostasis in Huh7 cells. J Hepatol 2007;47:12–22.
[11] Bonkovsky HL, Naishadham D, Lambrecht RW, Chung RT, Hoefs JC, Nash SR,et al. Roles of iron and HFE mutations on severity and response to therapyduring retreatment of advanced chronic hepatitis C. Gastroenterology2006;131:1440–1451.
[12] Distante S, Bjoro K, Hellum KB, Myrvang B, Berg JP, Skaug K, et al. Raisedserum ferritin predicts non-response to interferon and ribavirin treatment inpatients with chronic hepatitis C infection. Liver 2002;22:269–275.
[13] Lebray P, Zylberberg H, Hue S, Poulet B, Carnot F, Martin S, et al. Influence ofHFE gene polymorphism on the progression and treatment of chronichepatitis C. J Viral Hepat 2004;11:175–182.
[14] Schaible UE, Kaufmann SH. Iron and microbial infection. Nat Rev Microbiol2004;2:946–953.
[15] Harmatz P, Jonas MM, Kwiatkowski JL, Wright EC, Fischer R, Vichinsky E,et al. Safety and efficacy of pegylated interferon alpha-2a and ribavirin forthe treatment of hepatitis C in patients with thalassemia. Haematologica2008;93:1247–1251.
[16] Kahraman S, Yilmaz R, Genctoy G, Arici M, Altun B, Erdem Y, et al. Efficacyand safety of intravenous iron therapy for HCV-positive haemodialysispatients. Nephron Clin Pract 2005;100:c78–c85.
[17] Kato J, Kobune M, Nakamura T, Kuroiwa G, Takada K, Takimoto R, et al.Normalization of elevated hepatic 8-hydroxy-20-deoxyguanosine levels inchronic hepatitis C patients by phlebotomy and low iron diet. Cancer Res2001;61:8697–8702.
0 vol. 53 j 990–992 991

Editorial
[18] Di Bisceglie AM, Bonkovsky HL, Chopra S, Flamm S, Reddy RK, Grace N, et al.Iron reduction as an adjuvant to interferon therapy in patients with chronichepatitis C who have previously not responded to interferon: a multicenter,prospective, randomized, controlled trial. Hepatology 2000;32:135–138.
[19] Mueller S, Pantopoulos K, Hübner CA, Stremmel W, Hentze MW. IRP1activation by extracellular oxidative stress in the perfused rat liver. J BiolChem 2001;276:23192–23196.
992 Journal of Hepatology 201
[20] Miura K, Taura K, Kodama Y, Schnabl B, Brenner DA. Hepatitis C virus-induced oxidative stress suppresses hepcidin expression through increasedhistone deacetylase activity. Hepatology 2008;48:1420–1429.
[21] Andriopoulos B, Hegedusch S, Mangin J, Riedel HD, Hebling U, Wang J, et al.Sustained hydrogen peroxide induces iron uptake by transferrin receptor-1independent of the iron regulatory protein/iron-responsive element net-work. J Biol Chem 2007;282:20301–20308.
0 vol. 53 j 990–992












![Diagnostic and Prognostic Value of Nuclear Factor Kappa-B ... · HCV-related lymphoma demonstrated by that the anti-lymphoma activity of [AVT] Antiviral therapy is associated closely](https://img.pdfslide.us/doc/110x75/5fcecd07644a7b1bfc699b19/diagnostic-and-prognostic-value-of-nuclear-factor-kappa-b-hcv-related-lymphoma.jpg)