Embed Size (px)
Citation preview

BJUIB J U I N T E R N A T I O N A L
© 2 0 1 2 T H E A U T H O R S
B J U I N T E R N A T I O N A L © 2 0 1 2 B J U I N T E R N A T I O N A L | doi:10.1111/j.1464-410X.2012.11190.x 1
What ’ s known on the subject? and What does the study add? Previous reports, with small numbers of patients, have described the problem of incomplete testosterone suppression ( > 1.1 or 1.7 nmol/L) with LHRH agonists. Various predisposing factors have been suggested: different drug agents and patient factors such as age, pretreatment testosterone levels and weight. Such incomplete testosterone suppression has been shown in one small report to be associated with increased PSA failure rates and in another report in those with metastases, with worse survival.
This study used testosterone assays that are more accurate at low levels than those used in most previous reports in a large dataset of 2196 men, and confi rmed incomplete testosterone suppression (breakthrough) rates > 1.7 nmol/L of 3.4% and > 1.1 nmol/L of 6.6%. We showed that younger age was strongly associated with the risk of breakthrough, with a minor effect of increasing body mass index. Repeated breakthroughs were more common (16%) in those who had already had one breakthrough. Interim measures of cancer control (PSA kinetics during LHRH therapy) were inferior in those with a breakthrough, and those with breakthroughs between 1.1 and 1.7 nmol/L had worse long-term biochemical control rates.
OBJECTIVES
• To describe breakthrough rates above castrate levels of testosterone, in a population-based series of men undergoing adjuvant luteinizing hormone-releasing hormone (LHRH) agonist therapy with curative radiation therapy. • To explore the predisposing factors for such breakthroughs and their impact on subsequent outcomes.
PATIENTS AND METHODS
• All men treated for prostate cancer between 1998 and 2007 with curative radiation in the province of British Columbia, Canada were potentially eligible ( n = 11 752). Of these, 2196 fulfi lled the eligibility criteria. • Serial testosterone measurements were obtained during continuous LHRH therapy. • Breakthrough rates > 1.1 nmol/L and > 1.7 nmol/L were calculated for each LHRH injection and for each patient course. • Predisposing factors were identifi ed, and early surrogates of oncological outcome (neoadjuvant nadir and post-treatment nadir) were determined.
RESULTS
• The risk of a breakthrough > 1.1 nmol/L was 6.6%, and > 1.7 nmol/L was 3.4% per patient course and 5.4% and 2.2% per LHRH injection (inclusive ranges). • Repeated breakthroughs occurred in 16% of patients. • Younger men were more liable to breakthroughs ( P < 0.001). • Early PSA kinetic surrogates of cancer control were inferior in those with breakthroughs. • Neither overall biochemical non-evidence of disease (bNED) nor survival were compromised, although subgroup analysis showed inferior 5-year bNED in those with breakthroughs of 1.1 – 1.7 nmol/L vs those
without (58% vs 73%, respectively; P = 0.048).
CONCLUSIONS
• Breakthroughs with LHRH agonists occur occasionally per injection, but occur commonly per patient course of treatment, and adversely affect early surrogate measures of outcome. • The monitoring of testosterone levels during therapy is therefore advised.
KEYWORDS
Testosterone suppression , LHRH agonist , androgen deprivation therapy , breakthrough
Study Type – Therapy (case series) Level of Evidence 4
Incomplete testosterone suppression with luteinizing hormone-releasing hormone agonists: does it happen and does it matter? Tom Pickles , Jeremy Hamm * , W. James Morris , William E. Schreiber † and Scott Tyldesley Radiation Programme, BC Cancer Agency, and Department of Radiotherapy and Developmental Radiotherapeutics, University of British Columbia, * Cancer Surveillance and Outcomes, BC Cancer Agency , and † Department of Pathology and Laboratory Medicine, Vancouver General Hospital and The University of British Columbia, Vancouver, Canada Accepted for publication 8 February 2012
Presented orally at the Canadian Association of Radiation Oncology Annual Scientifi c Meeting, Vancouver, September 2010.

P I C K L E S E T A L .
© 2 0 1 2 T H E A U T H O R S
2 B J U I N T E R N A T I O N A L © 2 0 1 2 B J U I N T E R N A T I O N A L
INTRODUCTION
Recent discoveries concerning the androgen receptor (AR) show that intracellular and adrenal sources of testosterone may be a driver of so-called castrate-resistant prostate cancer [ 1 ] . Inadequate suppression of testicular testosterone may provide further AR activation and it has been suggested that some of the effi cacy of the newer agents targeting the AR may be attributable to ongoing testosterone activity [ 1 ] . With this background, we undertook the present study of the completeness of testosterone suppression with LHRHa agonists. The ‘ conventional ’ castrate level for testosterone obtained with LHRHa is usually reported as < 1.7 nmol/L (50 n/dL) [ 2 ] , but > 1.1 nmol/L PSA is no longer fully suppressed, according to one small report [ 3 ] , and the testosterone level with surgical orchiectomy is much lower at < 0.7 nmol/L [ 4 ] . Testosterone levels with LHRHa may not achieve such levels, and higher testosterone levels have been associated with an increased death rate in those with castrate-resistant prostate cancer [ 4,5 ] . Previous reports, with small numbers of patients, have identifi ed such LHRHa breakthroughs (also described as escapes) as being relatively common: e.g. cumulative breakthrough rates of 31.5% for 1.1 – 1.7 nmol/L and 24.7% for ≥ 1.7 nmol/L in a series of 73 patients [ 6 ] ; however, most of these rates occurred at the 1-month time point, when initial LHRHa receptor stimulation ( ‘ fl are ’ ) may still be occurring [ 7 ] . Particular LHRHa formulations may differ in this phenomenon [ 8,9 ] .
The present study was designed to explore the frequency of testosterone breakthroughs in a large population-based dataset so as to identify associated patient and pharmacological factors, and to investigate if breakthroughs affected subsequent outcome.
MATERIAL AND METHODS
The British Columbia Cancer Agency (BCCA) is the sole provider of radiation therapy to the residents of BC (population 4.5 million). The BC Cancer Registry is maintained by the BCCA and captures details of all patients diagnosed with malignant disease in the province.
DATA SOURCES
The BCCA radiation warehouse table captures details on all radiotherapy delivered in the province. This was queried for all patients treated with radiation therapy with curative intent between 1998 and 2007 ( n = 11 752). All approved anti-cancer medications are dispensed or reimbursed by the BCCA, and prescribing records are available electronically. The provincial pharmacy database contains records of LHRHa and anti-androgen prescriptions. Each record details the date of prescription, drug dispensed, dose and quantity. The start date of adjuvant androgen deprivation therapy (ADT), as well as stop date, and any use of secondary intervention for relapse were calculated. Gaps in prescribing were identifi ed by comparing the sum of duration of each prescription with the total elapsed time of the ADT course. Four products were used: goserelin (Zoladex ® , Astra-Zeneca, Mississauga, ON, Canada), leuprolide i.m. (Lupron ® , Abbott Laboratories, Montr é al, QC, Canada), buserelin (Suprefact ® , Sanofi -Aventis, Laval, QC, Canada). Leuprolide s.c. (Eligard ® , Sanofi -Aventis) also became available in 2005. The assumed duration of action of the products was taken from the drug monographs (i.e. 4 weeks for short-acting products, and 2 – 6 months for the longer-acting products). The BCCA Tumour Marker Laboratory is a reference laboratory for the province of British Columbia. During the era of this study several testosterone assays were in use: a manual radioimmunoassay (RIA) produced by Diagnostic Products Corp. (USA) from January 1989 until June 2004, and an automated chemiluminescent immunoassay (Elecsys) produced by Roche-Boehringer-Mannheim (Mannheim, Germany) from June 2004 to the present. In addition, an automated immunoassay produced by Abbott (Architect Chemiluminescent Microparticle Immunoassay [ CMIA ] ) was used briefl y from July 2001 until February 2002, when it was replaced by the RIA assay for results below 3 nmol/L. It had been determined that assays at such low levels may be unreliable, with overreading of the true result by factors of 2 – 5-fold [ 10 ] , and therefore results with the CMIA assay and those from other laboratories (where it was usually not possible to reliably identify the testosterone assay used) at levels < 3 nmol/L were discarded. Of a potential 5566 testosterone results (during ADT therapy for
eligible patients) 89% were included according to these criteria.
The practice of frequent testosterone measures arose in BC, to allow us to more accurately carry out analysis of outcomes and be alerted to any patient whose testosterone profi le indicated the use of an ADT agent. In practice, our ability to independently query the provincial pharmacy database made this unnecessary. Measurement of testosterone was performed at any time of day, and tended to coincide with a clinical appointment, not necessarily at the same time as LHRHa administration, as ‘ home injection programmes ’ are used by many patients, whereby the agent is administered outside the clinic.
Breakthrough levels of testosterone were a priori defi ned as (i) ≥ 1.7 nmol/L and (ii) ≥ 1.1 nmol/L. Because we did not want to investigate the fl are phenomenon, any testosterone results obtained within 4 weeks of starting a course of LHRHa were excluded. PSA kinetics were examined as an early measure of subsequent outcome. Firstly, the neoadjuvant nadir PSA (that is, the minimum PSA level reached on ADT before initiation of radiation) has been shown to be a strong correlate of subsequent prostate cancer survival [ 11,12 ] . Secondly, the post-radiation nadir PSA is also of prognostic importance [ 13 ] . Subsequent PSA outcomes were assessed using the Phoenix (nadir + 2) defi nition of relapse in a subgroup of patients treated with external beam radiation, excluding those participating in an ongoing randomized study, whose PSA results were not obtained [ 14 ] , and those treated with brachytherapy.
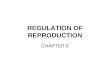
Clinical data were obtained from chart review or from existing databases. Patients were eligible for the present study if they received an LHRHa with curative radiation therapy for prostate cancer, and had at least one testosterone measurement during that time. Systematic and random chart audits were performed, with 67% of all cases being audited. All patient charts with a breakthrough were reviewed to ensure data accuracy. Detailed exclusion reasons are given in Fig. 1 . From the potential 11 752 patients, after the eligibility criteria were applied, 2196 patients were included. Ethical approval was given by the University of

I N C O M P L E T E T E S T O S T E R O N E S U P P R E S S I O N
© 2 0 1 2 T H E A U T H O R S
B J U I N T E R N A T I O N A L © 2 0 1 2 B J U I N T E R N A T I O N A L 3
British Columbia to allow access to these data sources, and to carry out the present study.
ANALYSIS METHOD
The frequency of breakthrough was calculated both as the occurrence of breakthrough per patient (maximum where > 1), and also per injection, where the LHRHa prescription had been accompanied by a valid testosterone measure. With the latter, the frequency of breakthroughs will be independent of the frequency of testosterone testing, but the rate per patient course will depend on the testosterone testing frequency. Patient factors studied for breakthrough risk were tumour risk group [ 15 ] , age, body mass index (BMI) and pre-treatment testosterone, grouped according to Damber et al . [ 16 ] . Treatment-related factors examined were the LHRHa type and year of treatment. These factors were analysed in relation to breakthroughs > 1.1 nmol/L, using a generalized estimating equations logistic regression model to handle intra-subject variation (owing to multiple injections per patient). Analysis was conducted using SAS v9.2 (Cary, NC, USA; http://www.sas.com )
RESULTS
Patient and treatment characteristics are shown in Table 1 . The median duration of ADT was 11.3 months and the median number of LHRHa injections per patient was 4. The most common product used was goserelin in 59% of cases, and the least common, leuprolide s.c., 5%.
The risk of a breakthrough > 1.1 nmol/L was 5.4% and > 1.7 nmol/L was 2.2% per LHRHa patient course. As patients typically received four injections each (36% of injections being accompanied by a testosterone measurement), the risk per patient course was higher: 6.6% and 3.4%. (ranges are inclusive). Table 2 contains more details of the testosterone measurement and breakthrough rates. When examined for the
3-month preparations, once established on the drug, breakthroughs appeared at a constant rate in relation to the time elapsed since injection, being neither more common just before or after each injection.
Repeated breakthroughs occurred in 16% of those with a fi rst breakthrough > 1.1 nmol/L, compared with a per-injection breakthrough rate of 5.4% ( P < 0.001, chi-squared test).
FIG. 1. Valid TT, testosterone results with an approved assay.
Radiation Warehouse tables 1998–2007 n = 11,752
Not treated with ADT
Exclusions
n = 4583
No valid TT results n = 3767
Neoadjuvant ADT duration >12 months n = 545
Gap in prescribing n = 251
Non-LHRHa ADT used n = 63
Incomplete record, not resolved by audit n = 86
Total eligible n = 2196
Total ADT duration <3 months n = 261
TABLE 1 Patient and treatment characteristics
Total no. of eligible patients 2196
NCCN Risk group [ 15 ] , n (%) Low 276 (13) Intermediate 796 (38) High 1043 (49) Missing 81 (3.7) Median age , years (range) 70 (45 – 86)
BMI , n (%) < 25 kg/m 2 (normal) 152 (25) 25-30 kg/m 2 (overweight) 292 (48) ≥ 30 kg/m 2 (obese) 159 (26) Not recorded 1593 (73) Pre-treatment testosterone * Mean, nmol/L 11.1 Median (range), nmol/L 10.9 (2 – 30) < 12.15 nmol/L, n (%) 504 (41) 12.15 – 17.35 nmol/L, n (%) 451 (37) > 17.35 nmol/L, n (%) 277 (23) Missing, n (%) 964 (44) ADT duration and LHRH details Median (range) total duration, months 11.3 (3 – 125) Median (range) neoadjuvant component, months 5.8 months (0 – 11.8) Median (range) adjuvant component, months 2.8 months (0 – 124) No. of LHRH injections per patient Mean 5.3 Median (range) 4 (1 – 45) Initial LHRH type used per patient, n (%) Buserelin 387 (18) Goserelin 1296 (59) Leuprolide i.m. 391 (18) Leuprolide s.c. 122 (5.6) Designated duration of LHRH injections, % of patients 4 weeks 7.2 2 months 3.5 3 months 82.5 4 months 6.4 6 months 0.3 Testosterone measurements Mean,no. of testosterone results per patient during ADT. 2 Median (range) no. of testosterone results per patient during ADT 2 (1 – 17) Mean ratio of no. of testosterone measures to LHRH scripts: 0.38
* Pre-treatment testosterone intervals are divided according to Damber et al . [ 16 ] .

P I C K L E S E T A L .
© 2 0 1 2 T H E A U T H O R S
4 B J U I N T E R N A T I O N A L © 2 0 1 2 B J U I N T E R N A T I O N A L
For those with a lower initial breakthrough (1.1 – 1.7 nmol/L) further breakthroughs occurred in 19%, compared with 11.5% in those with higher breakthroughs ( > 1.7 nmol/L). Of those where a breakthrough was noted by the oncologist ( n = 20), seven of those with a breakthrough > 1.7 nmol/L were switched to a different LHRHa, compared with none where the breakthrough was 1.1 – 1.7 nmol/L. Of the seven patients switched to a different LHRHa, castrate testosterone was obtained in three patients after switching, in two further patients after a further injection of
the same drug before the switch had occurred, and in two patients still failing to achieve castrate levels with a different product.
Univariate analysis identifi ed younger age as the only defi nite factor associated with breakthrough > 1.1 nmol/L ( P < 0.001, confi rmed on multivariate analysis [ Fig. 2 ] ). Higher BMI, and lower risk group was of borderline signifi cance and not confi rmed on multivariate analysis ( Table 3 ). Pre-intervention testosterone level was not associated with breakthrough risk.
With regard to the different LHRHa preparations, the risk of breakthrough > 1.1 nmol/L per LHRHa injection appeared to be greater for the leuprolide s.c. (Eligard ® ) product, with an overall rate of 11% vs 5% for others, ( P < 0.001 chi-squared test, Table 2 ). However, because this product was only prescribed in the last 3 years of our study when we had switched to the Elecsys testosterone assay, and because other unknown factors may have changed, multivariate analysis incorporating year and drug type, as well as those factors already shown to be signifi cant, was undertaken.
TABLE 2 Testosterone breakthrough details
Testosterone breakthrough rate per LHRH injection None (%) 3177/4417 (94.6) 1.1 – 1.7 nmol/L (%) 143/4417 (3.2) > 1.7 nmol/L (%) 97/4417 (2.2) Highest recorded and breakthrough rate per patient None (%) 2051/2196 (93) 1.1 – 1.7 nmol/L (%) 70/2196 (3.2) > 1.7 nmol/L (%) 75/2196 (3.4) Testosterone breakthrough rate by LHRH product ( > 1.1 nmol/L) Buserelin (%) 53/938 (5.7) Leuprolide s.c. (%) 32/293(10.9) Goserelin (%) 118/2462 (4.8) Leuprolide i.m. (%) 37/724 (5.1%) Repeated breakthroughs: frequency after fi rst occurrence 1st breakthrough 1.1 – 1.6 nmol/L 1st breakthrough ≥ 1.7 nmol/L 2 breakthroughs (%) 9/96 (9) 7/78 (9) 3 breakthroughs (%) 3/96 (3) 2/78 (3) ≥ 4 breakthroughs (%) 6/96 (6) 0 Testosterone breakthrough frequency ( ≥ 1.1 nmol/L) by LHRH duration 4 weeks (%) 1/46 (2.2) 2 months (%) 5/134 (3.7) 3 months (%) 207/3886 (5.3) 4 months (%) 26/332 (7.8) 6 months (%) 1/19 (5.3)
FIG. 2. Testosterone breakthrough in relation to age. The risk of a breakthrough was greater with younger age ( P < 0.001).
0%
5%
10%
45–64 65–69 70–74 75–86Age, Quartiles
≥1.7 nmol/L1.1–1.6 nmol/L
Perc
enta
ge w
ith b
reak
thro
ugh
4.2%2.5% 2.5%
4.4%
3.7%
3.7%
2.8% 2.7%
TABLE 3 Univariate analysis of factors predicting testosterone breakthrough ( > 1.1 nmol/L)
Variable Level Odds ratio 95% CI P Age per year 0.95 0.93 – 0.98 0.001BMI < 25 kg/m 2 0.67 0.34 – 1.31 0.25
25 – 30 kg/m 2 0.58 0.31 – 1.06 0.08 > 30 kg/m 2 1.00 1.00 (ref)
Pre-testosterone < 12.14 nmol/L 1.25 0.72 – 2.21 0.4212.15 – 17.34 nmol/L 0.88 0.52 – 1.48 0.62 ≥ 17.35 nmol/L 1.00 1.00 (ref)
Risk group Low 1.73 1.01 – 2.98 0.046Intermediate 1.38 0.92 – 2.08 0.12High 1.00 1.00 (ref)

I N C O M P L E T E T E S T O S T E R O N E S U P P R E S S I O N
© 2 0 1 2 T H E A U T H O R S
B J U I N T E R N A T I O N A L © 2 0 1 2 B J U I N T E R N A T I O N A L 5
The overall hazard of breakthrough per patient with leuprolide s.c. was 1.7 (CI 0.79 – 3.74, P = 0.2) compared with leuprolide i.m. (Lupron ® ) and this was not statistically signifi cant. There were no differences in the ADT duration, age or BMI in patients receiving leuprolide s.c. compared with other products. It should be noted that relatively few patients (5%) received leuprolide s.c., thus limiting the power of this analysis.
Patient outcomes, as assessed by early PSA kinetics, showed an adverse effect of testosterone breakthrough. The neoadjuvant nadir PSA was signifi cantly higher in those with a breakthrough in the neoadjuvant period (median 0.68 ng/mL v 0.41 ng/mL; P < 0.001). The post-treatment nadir was also higher in those with breakthroughs: 0.02 ng/mL for those without a breakthrough, compared with 0.04 ng/mL for testosterone > 1.1 nmol/L or > 1.7 nmol/L ( P = 0.008 and P = 0.003, respectively). Full details are given in Table 4 . Subsequent biochemical non-evidence of disease (bNED) rates (i.e. biochemical control rates) after 5 years (with a median follow-up time of 45 months), was 73.1% in those without a testosterone breakthrough vs 62% with ( P = 0.09). The subgroup of men with a breakthrough of 1.1 – 1.7 nmol/L, had a 5-year bNED rate of 57.6% ( P = 0.048), and those with a breakthrough of > 1.7 nmol/L, had a 5-year bNED rate of 68% ( P = 0.6). It
is noteworthy that, while 31% of those with breakthroughs > 1.7 nmol/L had some action taken as a result of the breakthrough (most usually the addition of an anti-androgen), this only happened in 13% of the 1.1 – 1.7 nmol/L group patients, ( P = 0.038, chi-squared test), probably because these breakthroughs were less pronounced and, therefore, either unrecognized or presumed to be of lesser importance.
DISCUSSION
Previous series and case reports, most with fewer than 100 patients [ 3,5,17 – 21 ] , have shown that failure to achieve castrate levels of testosterone < 1.7 nmol/L occurs in up to 12% of patients [ 22,23 ] . The largest report (to date as abstract only) on 451 patients showed an 11% risk [ 24 ] . The present series, from a population-based study of over 2000 men, confi rms that breakthroughs occur with rates per patient of 3.4% ≥ 1.7 nmol/L and 6.6% ≥ 1.1 nmol/L.
Rates in the present study are lower than those in other reports because we restricted our analysis to those testosterone assays that have been shown to be more accurate at low levels; whereas other series have not done this and may therefore have overestimated the true rate. The rates taken from the drug monographs are typically 1 – 2% [ 25,26 ] .
The conventional castrate level (1.7 nmol/L or 50 ng/dL) that is quoted in the literature was chosen based on testosterone assays that were insensitive below this level, but actual testosterone achieved with surgical castration is < 0.7 nmol/L, according to the few studies examining this [ 4,27 ] . Although more modern testosterone assays have allowed the measurement of such low testosterone levels, it is not appreciated how poor many of the assays in current use may be. Ratios of measured to true results in women with testosterone values of ∼ 1.6 nmol/L showed overmeasurement by a factor of ≥ 3 in six of 10 assays studied [ 10 ] . Many laboratories do not quote the assay used in their reports, nor do they provide guidance about interpretation of accuracy. The present study only included testosterone results at levels < 3 nmol/L with the RIA and Elecsys assay, which had performed well in comparison with the ‘ gold standard ’ isotope dilution-liquid chromatography (IDLC)-tandem mass spectrometry [ 10 ] . Few reports on testosterone breakthrough make mention of assay variability. A recent report of testosterone levels obtained with IDLC-tandem mass spectrometry showed that LHRHa agonists performed as well as orchiectomy, with only one of 32 subjects failing to achieve a testosterone of 0.7 nmol/L; however, assays were only performed once per patient, and the LHRHa preparation was not specifi ed [ 28 ] .
We found repeated breakthroughs occurred in 16% of those experiencing a fi rst breakthrough, compared with an initial breakthrough rate of 5.4%. This suggests that breakthroughs are likely to be related to patient factors such as age and BMI, or are LHRHa-specifi c, rather than being random events. Similar results have been reported by Morote et al . [ 6 ] , where the risk of subsequent breakthroughs was related to the magnitude of previous testosterone level on ADT. Those with 1, 2, or 3 consecutive readings < 0.7 nmol/L had chances of 11%, 5.7% and 0%, respectively, of having a subsequent breakthrough > 1.7 nmol/L. Most did not change to a different LHRHa as the breakthrough was not recognized by the treating oncologist, but, of those that did switch, 29% still failed to achieve low testosterone levels.
The large patient numbers in the present study permitted investigation into such potential predisposing factors. We identifi ed
TABLE 4 Effect of testosterone breakthrough on PSA kinetics
Neoadjuvant nadir PSAMean PSA (ng/ml)
Median PSA (ng/ml)
Signifi cance (Kruskall-Wallis) v. no breakthrough
No breakthrough 0.90 0.41 referenceBreakthrough 1.1 – 1.7 nmol/L 1.00 0.60 P = 0.11Breakthrough > 1.7 nmol/L 1.8 0.78 P < 0.001
Post-treatment nadir PSAMean PSA (ng/ml)
Median PSA (ng/ml)
Signifi cance (Mann Whitney U Test)
No breakthrough 0.16 0.02 referenceBreakthrough 1.1 – 1.7 nmol/L 0.13 0.04 P = 0.008Breakthrough > 1.7 nmol/L 0.33 0.04 P = 0.003
PSA control rate at 5 years (nadir + 2 defi nition)
Signifi cance (log rank)
No breakthrough 73.1% referenceBreakthrough > 1.1 nmol/L 57.6% P = 0.048Breakthrough > 1.7 nmol/L 68.4% P = 0.6

P I C K L E S E T A L .
© 2 0 1 2 T H E A U T H O R S
6 B J U I N T E R N A T I O N A L © 2 0 1 2 B J U I N T E R N A T I O N A L
younger age as a factor predisposing to breakthrough, which has previously been postulated [ 18 ] , but the present study is the fi rst to provide confi rmation. The probable mechanism is a more robust hypothalamic-gonadal pathway in the young. The effect of increasing BMI was of only borderline statistical signifi cance, but may be related to a dose/kg effect.
The patients in the present study received a variety of LHRHa products, and this allowed a direct, albeit non-randomized, comparison of breakthrough rate by product. Crude increased rates with leuprolide s.c. (Eligard ® ) were not confi rmed in a multivariate model with no signifi cant differences by product. Nonsignifi cantly increased rates for leuprolide s.c. were found in a large Spanish study (14.5% vs 10% for others, P = 0.22) [ 24 ] . The randomized data that is referenced in the Eligard ® product monograph quote breakthrough rates ≥ 1.74 nmol/L in 2% of patients with the 4-month preparation [ 25 ] and 1% with the 3-month and 6-month preparations [ 26,29 ] , rates which are lower than the 4.4% rate per injection in the present study. Leuprolide s.c. has also been reported to fail to suppress testosterone according to Koupparis [ 8 ] and Koupparis and Tyrrell [ 17 ] perhaps owing to a granulomatous reaction to the microcapsules of the formulation, and others have suggested an autoimmune-mediated resistance [ 2 ] . In Sweden, the Medical Protections Agency alerted physicians about 12 cases of failure of testosterone suppression with leuprolide [ 30 ] and consequently recommended close monitoring of testosterone while patients are on LHRHa. At least one author believes that ‘ not all LHRHa agonists are equal ’ [ 31 ] . A review of LHRHa effi cacy compares breakthrough rates reported according to product [ 9 ] and shows that all products are prone to this phenomenon; apparent differences between products are diffi cult to interpret because of design differences in the studies reviewed.
While it may appear that the effi cacy of intermittent androgen deprivation therapy (IADT) is inconsistent with the present results, we do not believe that it is. Firstly, the recently reported results of a large randomized comparison of IADT vs continuous therapy showed an increased prostate cancer death rate, suggesting inferiority for this endpoint (although
quality of life was improved, and overall survival was similar) [ 32 ] . Secondly, it has been shown that effective IADT requires a good PSA response, which in turn is dependent on an adequate castrate testosterone level [ 33 ] , as reviewed by Shore and Crawford [ 34 ] , who recommend ‘ keeping testosterone levels as low as possible while patients are on treatment results in the lowest possible serum PSA levels and likely improves outcomes ’ . Likewise, anti-androgen monotherapy, a non-castrating treatment for advanced and metastatic prostate cancer, is established in European practice; however, survival is inferior compared with orchiectomy [ 35 ] , but it is used owing to perceived quality-of-life advantages [ 36 ] .
The limitations of the present study are its retrospective and non-randomized design, and the lack of standardized testosterone measurements during the ADT course. Confi rmatory testosterone measures were generally only obtained when a higher level of breakthrough had been recognized by the oncologist, and more complete measures of endocrine function, such as gonadotrophins, were not measured. Another limitation is the inaccuracy of testosterone assays, which required 10.6% of all results to be discarded, but the strength of a registry-based and consequently large data source mitigates this to some degree. In addition, our pharmacy database records the date of dispensing of medication, with no guarantee that the drug was given on that date; however, all patient charts with breakthrough were audited, and where any unresolved concern about administration dates remained, the patients were removed from the study.
The breakthroughs described in the present report are associated with adverse effects on initial PSA kinetics, which have been shown to correlate with prostate cancer death on longer follow-up [ 13,37 ] . We did not detect a defi nite impact on subsequent PSA relapse ( P = 0.09), although sub-group analysis did show that men with breakthroughs of 1.1 – 1.7 nmol/L (but not higher) had inferior biochemical outcomes. This may be because of intervention when the breakthrough occurred or, alternatively, the saturation theory of AR stimulation [ 38 ] is also compatible with these fi ndings. The theory is that prostate cancer is exquisitely sensitive to testosterone levels in the near-castrate range, but becomes insensitive
to higher testosterone levels. The present study was not designed to examine long-term PSA control rates and the relatively short PSA follow-up of 45 months may be insuffi cient to detect a difference if one truly does exist. There was no effect on prostate cancer death; however, again follow-up is short for this endpoint. In those at higher risk of relapse or death from prostate cancer, full castration may be of greater importance, with one retrospective report of 129 men showing the risk of death from castrate-resistant prostate cancer being related to the testosterone level after 6 months of LHRHa therapy [ 5 ] .
If achieving true castrate testosterone levels is important, then testosterone should be monitored as recommended by several others [ 6,18,30 ] and, if necessary, a different LHRHa agonist or antagonist should be used.
In conclusion, we have confi rmed that breakthroughs of testosterone suppression above conventional castrate levels of 1.7 nmol/L occur after 2.2% of LHRHa injections. Repeated breakthroughs are more than twice as common as initial breakthroughs, and breakthroughs > 1.7 nmol/L per patient course were observed in up to 7.4% of patients, depending on the LHRHa used. There is an impact on early PSA kinetic outcomes, and possibly on longer-term biochemical control. It is prudent therefore to recommend that testosterone be monitored closely using an assay that has the required sensitivity.
ACKNOWLEDGMENTS
Research Support: This project was the recipient of an ACURA (Abbott-Canadian Association of Radiation Oncology Uro-Radiation) award. We thank Jerusha Miller, Medical Student and the oncologists who cared for the patients included in this study. Dr Scott Tyldesley has a Career Investigator Award from the Michael Smith Foundation for Health Research.
CONFLICT OF INTEREST
Tom Pickles has received honoraria/speaker fees from Abbott Labs and Ferring Pharma. Scott Tyldesley has received honoraria/speaker fees from Astra-Zeneca and Sanofi .

I N C O M P L E T E T E S T O S T E R O N E S U P P R E S S I O N
© 2 0 1 2 T H E A U T H O R S
B J U I N T E R N A T I O N A L © 2 0 1 2 B J U I N T E R N A T I O N A L 7
REFERENCES
1 Ryan CJ , Tindall DJ . Androgen receptor rediscovered: the new biology and targeting the androgen receptor therapeutically . J Clin Oncol 2011 ; 29 : 3651 – 8
2 Oefelein MG , Resnick MI . Effective testosterone suppression for patients with prostate cancer: is there a best castration? Urology 2003 ; 62 : 207 – 13
3 Morote J , Orsola A , Planas J et al . Redefi ning clinically signifi cant castration levels in patients with prostate cancer receiving continuous androgen deprivation therapy . J Urol 2007 ; 178 ( 4 Pt 1 ): 1290 – 5
4 Oefelein MG , Feng A , Scolieri MJ , Ricchiutti D , Resnick MI . Reassessment of the defi nition of castrate levels of testosterone: implications for clinical decision making . Urology 2000 ; 56 : 1021 – 4
5 Perachino M , Cavalli V , Bravi F . Testosterone levels in patients with metastatic prostate cancer treated with luteinizing hormone-releasing hormone therapy: prognostic signifi cance? BJU Int 2009 ; 105 : 648 – 51
6 Morote J , Planas J , Salvador C , Raventos CX , Catalan R , Reventos J . Individual variations of serum testosterone in patients with prostate cancer receiving androgen deprivation therapy . BJU Int 2009 ; 103 : 332 – 5 ; discussion 335
7 Bubley GJ . Is the fl are phenomenon clinically signifi cant? Urology 2001 ; 58 ( 2 Suppl . 1 ): 5 – 9
8 Koupparis A . Individual variations of serum testosterone in patients with prostate cancer receiving androgen deprivation therapy. Commentary . BJU Int 2009 ; 104 : 124 ; author reply 124 – 5
9 Tombal B , Berges R . How good do current LHRH agonists control testosterone? Can this be improved with Eligard ® ? Eur Urol Suppl 2005 ; 4 : 30 – 6
10 Taieb J , Mathian B , Millot F et al . Testosterone measured by 10 immunoassays and by isotope-dilution gas chromatography-mass spectrometry in sera from 116 men, women, and children . Clin Chem 2003 ; 49 : 1381 – 95
11 Ludgate CM , Bishop DC , Pai H et al . Neoadjuvant hormone therapy and external-beam radiation for localized high-risk prostate cancer: the importance of PSA nadir before
radiation . Int J Radiat Oncol Biol Phys 2005 ; 62 : 1309 – 15
12 Foo M , Lavieri M , Pickles T . Impact of Neo-adjuvant PSA kinetics on biochemical failure and prostate cancer mortality: results from a prospective patient database . American Society of Radiation Oncology Annual Scientifi c Meeting; 2010; San Diego, CA: International Journal of Radiation Oncology * Biology * Physics . 2010 ; S362
13 Crook J , Malone S , Perry G , Bahadur Y , Robertson S , Abdolell M . Postradiotherapy prostate biopsies: what do they really mean? Results for 498 patients . Int J Radiat Oncol Biol Phys 2000 ; 48 : 355 – 67
14 Roach M 3rd , Hanks G , Thames H Jr et al . Defi ning biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: recommendations of the RTOG-ASTRO Phoenix Consensus Conference . Int J Radiat Oncol Biol Phys 2006 ; 65 : 965 – 74
15 National _ Comprehensive _ Cancer _ Network . NCCN Clinical Practice Guidelines in Oncology . 2010
16 Damber J , Tammela T , Abrahamsson P et al . Comparing testosterone and PSA for different baseline testosterone concentrations during initiation of degarelix and leuprolide treatment . Eur Urol Suppl 2009 ; 8 : 130
17 Koupparis AJ , Tyrrell C . Non-suppression of testosterone in patients with a rising prostatespecifi c antigen level receiving luteinising hormone-releasing hormone analogues for metastatic prostate cancer . Clin Oncol (R Coll Radiol) 2006 ; 18 : 571 – 2
18 Oefelein MG , Cornum R . Failure to achieve castrate levels of testosterone during luteinizing hormone releasing hormone agonist therapy: the case for monitoring serum testosterone and a treatment decision algorithm . J Urol 2000 ; 164 ( 3 Pt 1 ): 726 – 9
19 Sharifi R , Browneller R . Serum testosterone suppression and potential for agonistic stimulation during chronic treatment with monthly and 3-month depot formulations of leuprolide acetate for advanced prostate cancer . J Urol 2002 ; 168 : 1001 – 4
20 Smith MR , McGovern FJ . Gonadotropin-releasing hormone agonist failure in a man with prostate cancer . J Urol 2001 ; 166 : 211
21 Zinner NR , Bidair M , Centeno A , Tomera K . Similar frequency of testosterone surge after repeat injections of goserelin (Zoladex) 3.6 mg and 10.8 mg: results of a randomized openlabel trial . Urology 2004 ; 64 : 1177 – 81
22 Tombal B , Berges R . Optimal control of testosterone: a clinical case-based approach of modern androgen-deprivation therapy . Eur Urol Suppl 2008 ; 7 : 15 – 21
23 Morote J , Esquena S , Abascal JM et al . Failure to maintain a suppressed level of serum testosterone during long-acting depot luteinizing hormone-releasing hormone agonist therapy in patients with advanced prostate cancer . Urol Int 2006 ; 77 : 135 – 8
24 Cabeza A , G ó mez A , Vilar S et al . Assessing the incidence of escapes of testosterone in the treatment with LHRH analogs: escape study . ASTRO Annual Scientifi c Meeting; 2009; Chicago: International Journal of Radiation Oncology, Biology, Physics ; 2009 ; S355
25 Sartor O , Dineen MK , Perez-Marreno R , Chu FM , Carron GJ , Tyler RC . An eight-month clinical study of LA-2575 30.0 mg: a new 4-month, subcutaneous delivery system for leuprolide acetate in the treatment of prostate cancer . Urology 2003 ; 62 : 319 – 23
26 Chu FM , Jayson M , Dineen MK , Perez R , Harkaway R , Tyler RC . A clinical study of 22.5 mg. La-2550: a new subcutaneous depot delivery system for leuprolide acetate for the treatment of prostate cancer . J Urol 2002 ; 168 : 1199 – 203
27 Rohl HF , Beuke HP . Effect of orchidectomy on serum concentrations of testosterone and dihydrotestosterone in patients with prostatic cancer . Scand J Urol Nephrol 1992 ; 26 : 11 - 4
28 van der Sluis FJ , Heijboer A , Meuleman M et al . Serum concentration of testosterone measured by isotope dilutionliquid Chromatography-tandem mass spectrometry (id-lcms/ ms) in men after bilateral orchiectomy or luteinizing hormone releasing Hormone (lhrh) agonist therapy . Americal urology Association Annual meeting; 2011; Washington, DC.: The Journal of Urology ; 2011
29 Sanofi -aventis . Eligard: Product

P I C K L E S E T A L .
© 2 0 1 2 T H E A U T H O R S
8 B J U I N T E R N A T I O N A L © 2 0 1 2 B J U I N T E R N A T I O N A L
Monograph , 2010 . Available at http://www.sanofi -aventis.ca
30 Medical _ Products _ Agency _ (Sweden) . Bristande kastrationseffekt vid GnRHanalogbehandling (Lack of effect of castration on GnRH analogue treatment) . Agency MP ed. 2010
31 Morote J . Re: Individual variations of serum testosterone in patients with prostate cancer receiving androgen deprivation therapy. Reply to Koupparis BJU Int 104(1) p124 . BJU Int 2009 ; 104 : 124 – 5
32 Crook J , O ’ Callaghan CJ , Ding K et al . A phase III randomized trial of intermittent versus continuous androgen suppression for PSA progression after radical therapy (NCIC CTG PR.7/SWOG JPR.7/CTSU JPR.7/UK Intercontinental Trial CRUKE/01/013) . J Clin Oncol 2011 ; Supplement ASCO meeting abstracts, Vol 29 issue 15S (part 1 of 2) p2925, abstr# 4514. Chicago; 2011. p. abstr 4514
33 Hussain M , Tangen CM , Higano C et al . Absolute prostate-specifi c antigen
value after androgen deprivation is a strong independent predictor of survival in new metastatic prostate cancer: data from Southwest Oncology Group Trial 9346 (INT-0162) . J Clin Oncol 2006 ; 24 : 3984 – 90
34 Shore ND , Crawford ED . Intermittent androgen deprivation therapy: redefi ning the standard of care? Rev Urol 2010 ; 12 : 1 – 11
35 Tyrrell CJ , Kaisary AV , Iversen P et al . A randomised comparison of ‘ Casodex ’ (bicalutamide) 150 mg monotherapy versus castration in the treatment of metastatic and locally advanced prostate cancer . Eur Urol 1998 ; 33 : 447 – 56
36 Iversen P , Tyrrell CJ , Kaisary AV et al . Casodex (bicalutamide) 150-mg monotherapy compared with castration in patients with previously untreated nonmetastatic prostate cancer: results from two multicenter randomized trials at a median follow-up of 4 years . Urology 1998 ; 51 : 389 – 96
37 Alexander A , Crook J , Jones S et al . Is
biochemical response more important than duration of neoadjuvant hormone therapy before radiotherapy for clinically localized prostate cancer? An analysis of the 3- versus 8-month randomized trial . Int J Radiat Oncol Biol Phys 2011 ; 76 : 23 – 30
38 Morgentaler A , Traish AM . Shifting the paradigm of testosterone and prostate cancer: the saturation model and the limits of androgen-dependent growth . Eur Urol 2009 ; 55 : 310 – 20
Correspondence: Tom Pickles, BC Cancer Agency, 600 West 10th Ave, Vancouver, BC, Canada V5Z 4E6. e-mail: [email protected]
Abbreviations : AR , androgen receptor ; BCCA , British Columbia Cancer Agency ; ADT , androgen deprivation therapy ; RIA , radioimmunoassay ; LHRHa , LHRH analogue ; BMI , body mass index ; bNED , biochemical non-evidence of disease ; IDLC , isotope dilution-liquid chromatography ; IADT , intermittent androgen deprivation therapy .