Embed Size (px)
Citation preview
European Heart Journal (2004) 25, 1127–1138
Dow
nloaded from h
Clinical research
Incidence and significance of pleomorphismin patients with postmyocardial infarctionventricular tachycardia
Acute and long-term outcome of radiofrequency catheterablation
ttps://academic.oup.com
/eurheartj/a
Paolo Della Bellaa,*, Stefania Rivaa, Gaetano Fassinia, Francesco Giraldia,Marco Bertia, Catherine Klersyb, Nicola Trevisia
a Arrhythmia Department, Centro Cardiologico Monzino, Institute of Cardiology, University of Milan, Via Parea 4,Milan 20138, Italyb Biometry and Clinical Epidemiology, Research Department, IRCCS San Matteo Hospital, University of Pavia,Pavia, Italy
Received 14 February 2003; revised 15 January 2004; accepted 22 January 2004Available online 17 April 2004
rticle-abstract/25/13/1127/465311 by guest on 04 April 2019
Aims The prognostic significance of multiple ventricular tachycardia (VT) morpho-logies, whether spontaneous or induced, was investigated in patients who underwentradiofrequency catheter ablation (RFCA) for postinfarction ventricular tachycardia.Methods and results We studied 137 patients with postinfarction ventricular tachy-cardia. Catheter ablation of all induced ventricular tachycardias was attempted.A single ventricular tachycardia morphology was documented in 102/137 patients
(MONO group); 35 patients had spontaneous pleomorphism (PLEO group). Multiple VTmorphologies were induced in 58/102 (57%) MONO patients and in all PLEO patients. Ahigher rate of arrhythmia suppression was obtained in MONO as compared to PLEOpatients (162/212 [76%] vs. 43/110 [39%]). Clinical presentation (VT pleomorphism)(OR: 0.22, CI: 0.08–0.62) and the induced VT cycle (mean PLEO/MONO: 338/385 ms,OR: 1.06) were independent predictors of acute RFCA success. Among MONO patients,the procedure was successful in 75% of the patients with a single induced ventriculartachycardia compared to 64% of those with multiple tachycardias. The acute successrate was lower in PLEO patients (23%). PLEO patients had a significantly higher 3- and5-year arrhythmia recurrence rate than MONO patients. RFCA acute success was theonly independent predictor of long-term outcome in multivariate analysis.Conclusions Spontaneous, but not induced, VT pleomorphism in patients with priormyocardial infarction adversely affects the acute and long-term success rate ofRFCA.
�c 2004 Published by Elsevier Ltd on behalf of The European Society of Cardiology.
KEYWORDSVentricular tachycardia;
Catheter ablation
* Corresponding author. Tel.: þ39-2-580021/58002340/58002275; fax:þ39-2-504-667.
E-mail address: [email protected] (P. Della Bella).
0195-668X/$ - see front matter �c 2004 Published by Elsevier Ltd on behalf of The European Society of Cardiology.doi:10.1016/j.ehj.2004.01.021

1128 P. Della Bella et al.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article-abstract/25/13/1127/46
Introduction
Multiple morphologies of sustained monomorphicventricular tachycardia (VT) may occur spontaneouslyor by induction during electrophysiological testing atdifferent times in the same patient. This phenomenon,defined as pleomorphism,1;2 is frequently observedfollowing a myocardial infarction. The presence ofmultiple exit sites from a single or multiple re-entrycircuits is one possible explanation and this feature ispotentially present in all patients with a prior myo-cardial infarction.3–9
Previous studies have demonstrated the relation be-tween VT pleomorphism and multiple infarctions, com-promised ventricular function, and the extent ofcoronary artery disease.1;2 The number of documentedVT morphologies is influenced by clinical variables, suchas the number of VT occurrences and the number ofantiarrhythmic drug treatments.2
A reduced efficacy of antiarrhythmic drugs has beendescribed in patients with multiple VT morpholog-ies10;11; likewise, multiple VT configurations are lesslikely to be cured by surgery, particularly when varioussites of origin can be demonstrated in intraoperativemapping.3;12;13
The creation of a line of blockade between the mitralannulus and posterior rim of infarcted myocardial areasresulted in the ablation of dual VT morphologies in a se-lected series of patients with previous inferior myocardialinfarction.14 Aside from this series of patients with a verydistinct arrhythmia pattern, the relation between theoccurrence of multiple clinical VTs and the results ofcatheter ablation has not been investigated.
This issue was addressed in the present study, wherethe occurrence of multiple VT morphologies, bothspontaneous and induced, was related to the acute andlong-term outcome of catheter ablation in a consecutiveseries of patients suffering from recurrent ventriculartachycardia following myocardial infarction.
5311 by guest on 04 April 2019
Methods
Population
The clinical and electrophysiological data of 177 consecutivepatients who underwent catheter ablation for recurrent sus-tained monomorphic VT following a myocardial infarction fromApril 1993 to November 2000 were retrospectively analysed.
The inclusion criteria were:1. Availability of complete clinical data, including 12-lead ECG
recordings of spontaneous and all induced VTs.2. A complete electrophysiological study and catheter ablation
protocol available for analysis.3. Reliable follow-up data, including documentation of recur-
rent arrhythmias by 12-lead ECG or ICD interrogation.4. An electrophysiological procedure performed at least 6
months before enrolment in the present study.
The final population included 137 patients (91 males) with amean age of 67� 6 years.
An ethics committee approved the study and all patientsgave written consent to the procedure.
Electrophysiological mapping and ablation data
Under local anaesthesia, multiple electrode catheters wereintroduced percutaneously and advanced to the right atrium,His bundle region, and right ventricular apex. A 4-mm tip 7F steerable catheter was introduced into the left ventricleby a retrograde transaortic or a transseptal approach. Pa-tients were kept mildly sedated by intravenous boluses ofmorphine and/or midazolam while blood pressure and oxygensaturation were continuously monitored invasively. Anticoag-ulation with heparin infusion, titrated to achieve an ACTvalue near 200–250 s, was instituted before the procedure.Programmed stimulation with up to three extrastimuli atmultiple drives (600–500–430 ms) from the right and theleft ventricle was performed to induce clinical arrhythmia orother sustained VTs. Computerised multichannel recordingsof all 12 standard ECG leads and bipolar intracardiac tracingswere obtained.
Sustained VTs causing a persistent systolic blood pressurereduction to <50 mm Hg 30 s after induction and requiringtermination by overdrive pacing or external DC shock wereconsidered hemodynamically intolerable and were not targetedunless non-conventional mapping techniques had been insti-tuted (see below).
Catheter ablation was guided by conventional activationmapping and entrainment techniques, as previously de-scribed,15–21 and was performed under temperature (up to 60 �C)and impedance control. All the VTs considered in this study wereablated in the left ventricle. VT ablation was considered ef-fective if VT interruption occurred within 10 seconds of theonset of delivery of radiofrequency energy, without any ven-tricular premature beat.
Thereafter, a repeated stimulation protocol was undertakento assess the inducibility of the target or any other sustainedmonomorphic VT.
In 12 patients (9 with multiple clinical VT morphologies),non-contact mapping (10 patients)22–25 or electroanatomicalmapping (2 patients)26 were used to guide catheter ablation.
Definitions
Spontaneous pleomorphismMultiple clinical VT configurations were defined by ECGs re-corded at different times showing different bundle-branch-blockpatterns in V1 or a QRS axis on the frontal plane differing by 45�or more.2 The same criteria were also used to define multiple VTmorphologies induced by electrophysiological study. Minorchanges in VT cycle length (<50 ms) were not considered todefine different VT morphologies.
Acute resultThe procedure was defined as successful (Class A) any sus-tained monomorphic VT was interrupted and inducibility wasprevented.27
Effective ablation of clinical VT and/or other VT morpho-logies with persistent inducibility of one or more non-clinicalsustained VTs was defined as a partial success (Class B).
Failure to interrupt even clinical VT was defined as a Class Cresult.
In patients without an ICD implanted before the procedure,the device was implanted following a Class B or C ablationresult.
In patients presenting with intolerable VT, an ICD wasimplanted even after a completely successful procedure.
Incidence and significance of pleomorphism in patients with postmyocardial infarction ventricular tachycardia 1129
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article-abst
Ablation site
When two distinct VT morphologies were ablated at the samesite, a single slow conduction isthmus was judged to be sharedby the VTs.
Electrophysiological confirmation of this definition wasprovided:– by proving concealed entrainment of both morphologies at
the same site.
– by producing an accurate 12-lead pacemap of both VTs duringsinus rhythm.28
Multiple isthmuses and/or exit sites were considered to bepresent when ablation had to be performed at clearly differentsites (spaced at least 2 cm apart as judged by fluoroscopy). In 12patients either non-contact mapping (ESI) for intolerable VT orelectroanatomical mapping (CARTO) for tolerated VT was un-dertaken to define the endocardial activation pattern duringVTorthe scar contour during SR. In patients undergoing a non-contactmapping procedure, the following definitions were used22;23;25:(1) Exit point. The site where a QS unipolar virtual electrogram
is recorded on the map, which corresponds to the site of ear-liest activation followed by a rapid activation front, spread-ing to the surrounding healthy endocardium.
(2) Diastolic pathway. A defined region of endocardium, usuallybordered by scar tissue, where the diastolic electrical activ-ity preceding the exit point is recorded over a variableamount of the diastolic interval.
For any induced VT, both the exit point and the part of thediastolic pathway that could be reliably tracked were marked onthe same ventricle as defined by virtual geometry.
Activation mapping during multiple morphologies of hemo-dynamically tolerated VTs was obtained by electroanatomicalmapping by the CARTO system; the landmarks of the ablationsites for different VTs were superimposed typically on the sinusrhythm voltage map to visually relate the ablation site to de-fined areas of the infarction.
Table 1 Population characteristics according to clinical VT prese
Variable Single clin
Patients characteristics (102 pts)
Myocardial infarction site (N (%))Anterior 66 (65%)Inferior 30 (29%)Multiple 6 (6%)
LVEF % (mean (SD)) 36.9 (7.4)Impaired (<30%) LVEF (N (%)) 15 (15%)Cardiac arrest (N (%)) 4 (4%)Syncope/hemodynamic compromised (N (%)) 19 (19%)Previous ICD implanted with shock (N (%)) 21 (21%)Amiodarone (N (%)) 99 (98%)b-Blockers (N (%)) 63 (62%)
Induced VT characteristics (212 VT)Number of VT induced per pt (median (IQR)) 2 (1–3)Percentage of VT ablated (median (IQR)) 100 (50–10VT cycle (mean (SD))d 385 (83)VT induced and not tolerated (N (%)) 23 (11%)aFisher exact test.bUnpaired t test.cMann–Whitney U test.dSD does not account for intra-patient correlation.eLogistic model with robust standard errors.
In these cases, a precise estimate of the distance betweenablation sites was made and used to confirm findings derivedfrom fluoroscopic observations.
Follow-up
All patients, in the absence of major side effects, were dis-charged with amiodarone therapy (200 mg/day), which wascontinued during follow-up unless contraindicated.
Follow-up after hospital discharge was carried out by visits tothe outpatient clinic at 2-month intervals and by ICD interrogationevery 4 months or whenever an arrhythmic event occurred.
The endpoints were recurrence of any VT, documented eitherby 12-lead ECG and/or by ICD interrogation, sudden death (de-fined as death after sudden cardiocirculatory collapse occurringwithin an hour of the onset of symptoms)29, and cardiac death.
r
Statistical analysis
Descriptive statistics were computed as the mean and standarddeviation (SD) for continuous variables, median and quartiles(IQR) for skewed distributions, and absolute frequencies andpercentage for categorical variables. Clinical and electrophysio-logical characteristics were compared between patients withmonomorphic or pleomorphic clinical VTbymeans of the unpairedt test, Mann–Whitney U test for continuous variables, or theFisher exact test for categorical variables, or by logisticmodellingwith robust standarderrors toaccount for intrapatient correlationwhen evaluating the characteristics of single VTs.
Multiple logistic regression analysis with a robust standarderror was used to assess the association between VT pleomor-phism and the acute catheter ablation result, controlled forclinically meaningful potential confounders (site of previousmyocardial infarction, left ventricular ejection fraction, induc-tion of multiple VTs, and induced VT cycle). All covariates
ntation
ical VT Clinical VT Pleomorphism p-Value
(35 pts)
0.435a
19 (54%)12 (34%)4 (11%)31.6 (5.7) 0.0002b
10 (29%) 0.079a
1 (7%) 0.349a
9 (26%) 0.630a
13 (39%) 0.094a
34 (99%) 0.999a
18 (51%) 0.230a
(110 VT)3 (3–4) <0.0005c
0) 33 (0–75) <0.0005c
338 (68) <0.0005e
49 (45%) <0.0005e
act/25/13/1127/465311 by guest on 04 April 2019
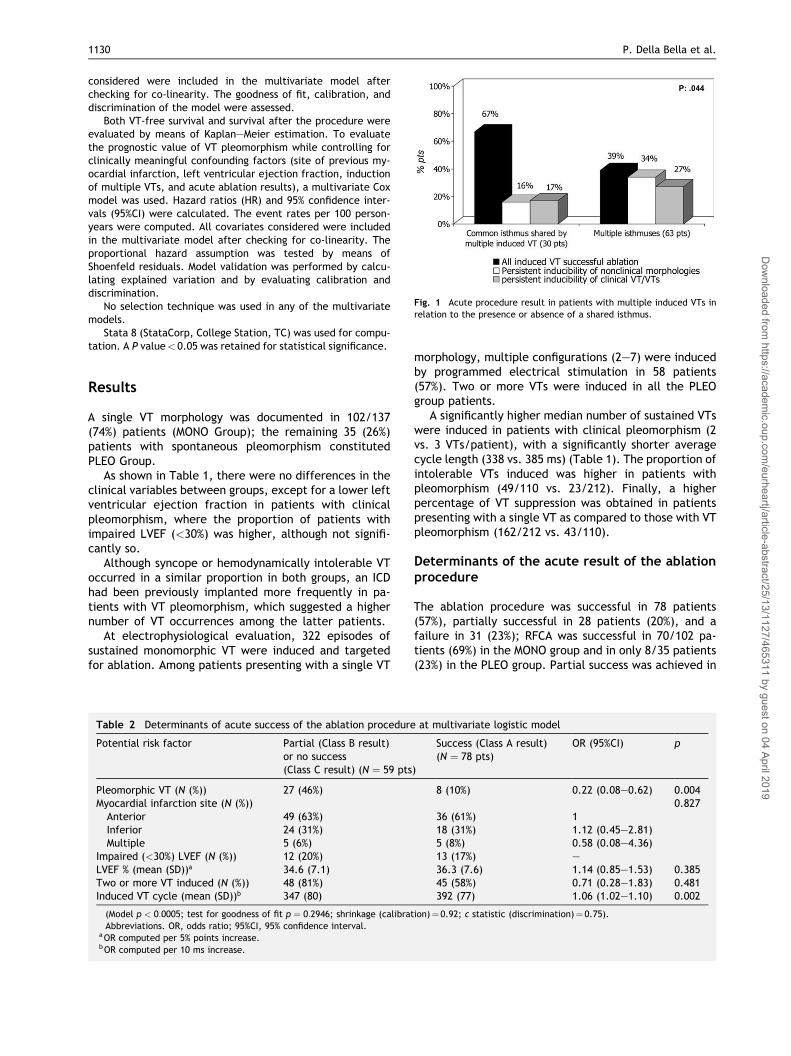
Fig. 1 Acute procedure result in patients with multiple induced VTs inrelation to the presence or absence of a shared isthmus.
1130 P. Della Bella et al.
Dow
nloaded from http
considered were included in the multivariate model afterchecking for co-linearity. The goodness of fit, calibration, anddiscrimination of the model were assessed.
Both VT-free survival and survival after the procedure wereevaluated by means of Kaplan–Meier estimation. To evaluatethe prognostic value of VT pleomorphism while controlling forclinically meaningful confounding factors (site of previous my-ocardial infarction, left ventricular ejection fraction, inductionof multiple VTs, and acute ablation results), a multivariate Coxmodel was used. Hazard ratios (HR) and 95% confidence inter-vals (95%CI) were calculated. The event rates per 100 person-years were computed. All covariates considered were includedin the multivariate model after checking for co-linearity. Theproportional hazard assumption was tested by means ofShoenfeld residuals. Model validation was performed by calcu-lating explained variation and by evaluating calibration anddiscrimination.
No selection technique was used in any of the multivariatemodels.
Stata 8 (StataCorp, College Station, TC) was used for compu-tation. A P value< 0.05 was retained for statistical significance.
s://academic.oup.com
/eurheartj/article-abstract/25/13/1127/465311
Results
A single VT morphology was documented in 102/137(74%) patients (MONO Group); the remaining 35 (26%)patients with spontaneous pleomorphism constitutedPLEO Group.
As shown in Table 1, there were no differences in theclinical variables between groups, except for a lower leftventricular ejection fraction in patients with clinicalpleomorphism, where the proportion of patients withimpaired LVEF (<30%) was higher, although not signifi-cantly so.
Although syncope or hemodynamically intolerable VToccurred in a similar proportion in both groups, an ICDhad been previously implanted more frequently in pa-tients with VT pleomorphism, which suggested a highernumber of VT occurrences among the latter patients.
At electrophysiological evaluation, 322 episodes ofsustained monomorphic VT were induced and targetedfor ablation. Among patients presenting with a single VT
Table 2 Determinants of acute success of the ablation procedure
Potential risk factor Partial (Class B result)or no success(Class C result) (N ¼ 59 pts
Pleomorphic VT (N (%)) 27 (46%)Myocardial infarction site (N (%))Anterior 49 (63%)Inferior 24 (31%)Multiple 5 (6%)
Impaired (<30%) LVEF (N (%)) 12 (20%)LVEF % (mean (SD))a 34.6 (7.1)Two or more VT induced (N (%)) 48 (81%)Induced VT cycle (mean (SD))b 347 (80)
(Model p < 0:0005; test for goodness of fit p ¼ 0:2946; shrinkage (calibratAbbreviations. OR, odds ratio; 95%CI, 95% confidence interval.
aOR computed per 5% points increase.bOR computed per 10 ms increase.
morphology, multiple configurations (2–7) were inducedby programmed electrical stimulation in 58 patients(57%). Two or more VTs were induced in all the PLEOgroup patients.
A significantly higher median number of sustained VTswere induced in patients with clinical pleomorphism (2vs. 3 VTs/patient), with a significantly shorter averagecycle length (338 vs. 385 ms) (Table 1). The proportion ofintolerable VTs induced was higher in patients withpleomorphism (49/110 vs. 23/212). Finally, a higherpercentage of VT suppression was obtained in patientspresenting with a single VT as compared to those with VTpleomorphism (162/212 vs. 43/110).
Determinants of the acute result of the ablationprocedure
The ablation procedure was successful in 78 patients(57%), partially successful in 28 patients (20%), and afailure in 31 (23%); RFCA was successful in 70/102 pa-tients (69%) in the MONO group and in only 8/35 patients(23%) in the PLEO group. Partial success was achieved in
at multivariate logistic model
)
Success (Class A result)(N ¼ 78 pts)
OR (95%CI) p
8 (10%) 0.22 (0.08–0.62) 0.0040.827
36 (61%) 118 (31%) 1.12 (0.45–2.81)5 (8%) 0.58 (0.08–4.36)13 (17%) –36.3 (7.6) 1.14 (0.85–1.53) 0.38545 (58%) 0.71 (0.28–1.83) 0.481392 (77) 1.06 (1.02–1.10) 0.002
ion)¼ 0.92; c statistic (discrimination)¼ 0.75).
by guest on 04 April 2019
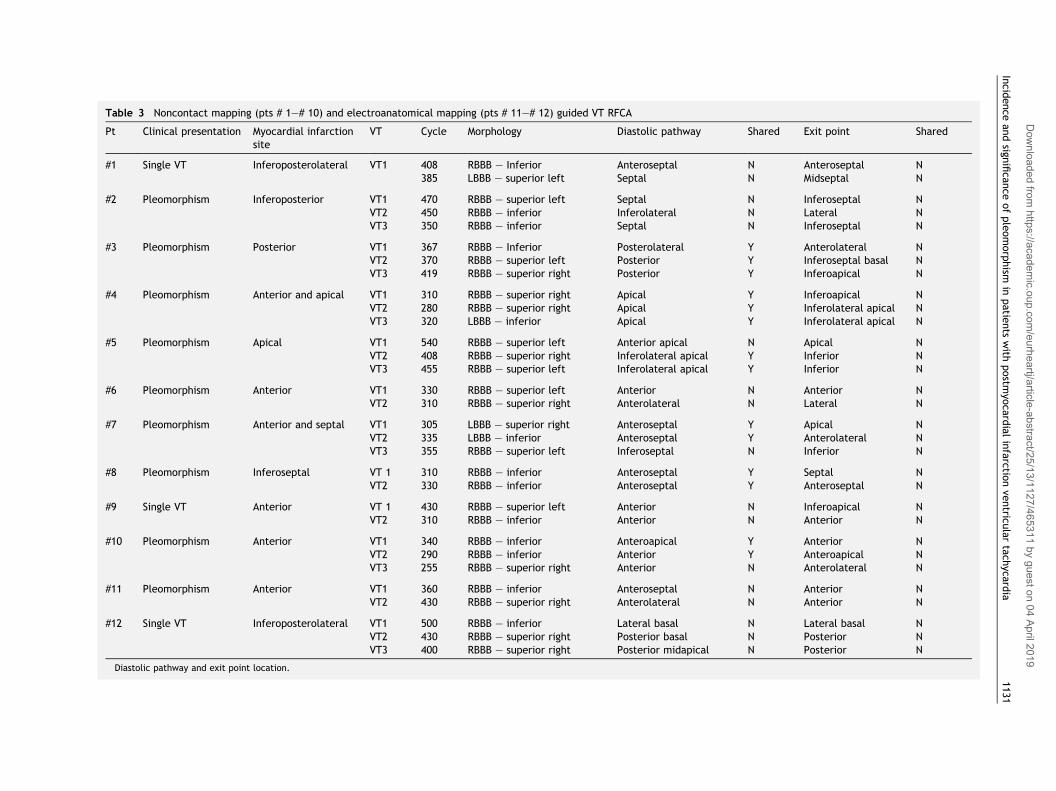
Table 3 Noncontact mapping (pts # 1–# 10) and electroanatomical mapping (pts # 11–# 12) guided VT RFCA
Pt Clinical presentation Myocardial infarctionsite
VT Cycle Morphology Diastolic pathway Shared Exit point Shared
#1 Single VT Inferoposterolateral VT1 408 RBBB – Inferior Anteroseptal N Anteroseptal N385 LBBB – superior left Septal N Midseptal N
#2 Pleomorphism Inferoposterior VT1 470 RBBB – superior left Septal N Inferoseptal NVT2 450 RBBB – inferior Inferolateral N Lateral NVT3 350 RBBB – inferior Septal N Inferoseptal N
#3 Pleomorphism Posterior VT1 367 RBBB – Inferior Posterolateral Y Anterolateral NVT2 370 RBBB – superior left Posterior Y Inferoseptal basal NVT3 419 RBBB – superior right Posterior Y Inferoapical N
#4 Pleomorphism Anterior and apical VT1 310 RBBB – superior right Apical Y Inferoapical NVT2 280 RBBB – superior right Apical Y Inferolateral apical NVT3 320 LBBB – inferior Apical Y Inferolateral apical N
#5 Pleomorphism Apical VT1 540 RBBB – superior left Anterior apical N Apical NVT2 408 RBBB – superior right Inferolateral apical Y Inferior NVT3 455 RBBB – superior left Inferolateral apical Y Inferior N
#6 Pleomorphism Anterior VT1 330 RBBB – superior left Anterior N Anterior NVT2 310 RBBB – superior right Anterolateral N Lateral N
#7 Pleomorphism Anterior and septal VT1 305 LBBB – superior right Anteroseptal Y Apical NVT2 335 LBBB – inferior Anteroseptal Y Anterolateral NVT3 355 RBBB – superior left Inferoseptal N Inferior N
#8 Pleomorphism Inferoseptal VT 1 310 RBBB – inferior Anteroseptal Y Septal NVT2 330 RBBB – inferior Anteroseptal Y Anteroseptal N
#9 Single VT Anterior VT 1 430 RBBB – superior left Anterior N Inferoapical NVT2 310 RBBB – inferior Anterior N Anterior N
#10 Pleomorphism Anterior VT1 340 RBBB – inferior Anteroapical Y Anterior NVT2 290 RBBB – inferior Anterior Y Anteroapical NVT3 255 RBBB – superior right Anterior N Anterolateral N
#11 Pleomorphism Anterior VT1 360 RBBB – inferior Anteroseptal N Anterior NVT2 430 RBBB – superior right Anterolateral N Anterior N
#12 Single VT Inferoposterolateral VT1 500 RBBB – inferior Lateral basal N Lateral basal NVT2 430 RBBB – superior right Posterior basal N Posterior NVT3 400 RBBB – superior right Posterior midapical N Posterior N
Diastolic pathway and exit point location.
Incid
ence
andsign
ifican
ceofpleomorphism
inpatie
nts
with
postm
yocard
ialinfarctio
nve
ntricu
lartach
ycardia
1131
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article-abstract/25/13/1127/465311 by guest on 04 April 2019
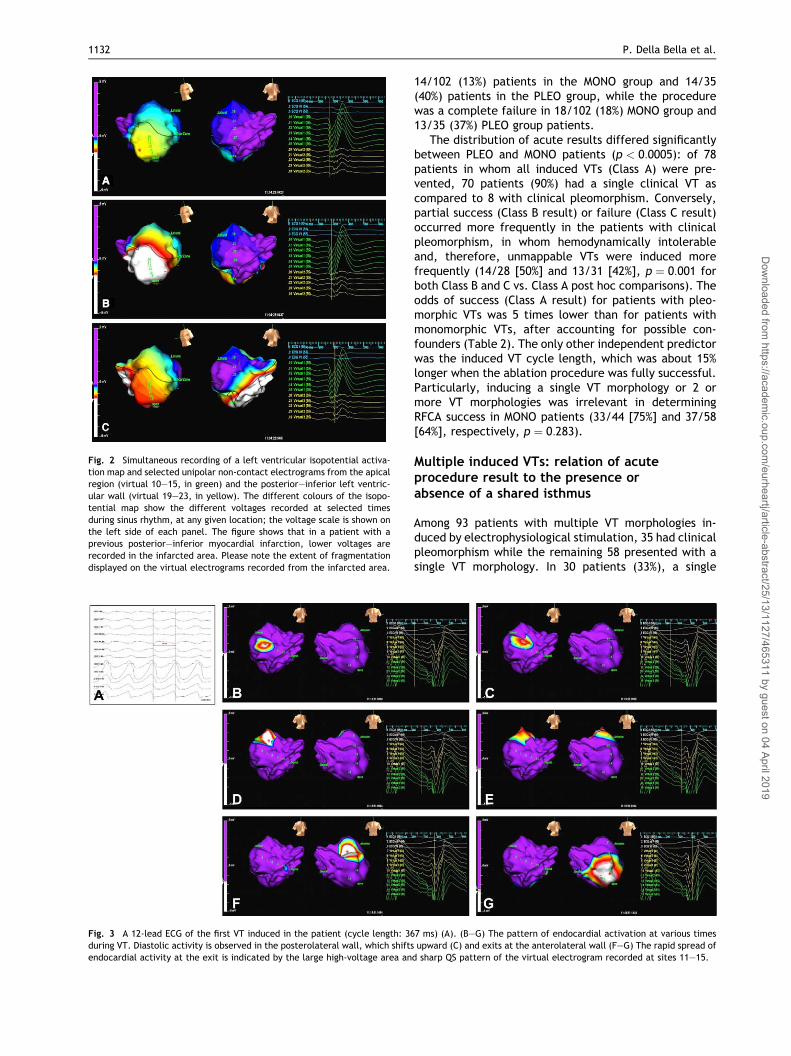
Fig. 2 Simultaneous recording of a left ventricular isopotential activa-tion map and selected unipolar non-contact electrograms from the apicalregion (virtual 10–15, in green) and the posterior–inferior left ventric-ular wall (virtual 19–23, in yellow). The different colours of the isopo-tential map show the different voltages recorded at selected timesduring sinus rhythm, at any given location; the voltage scale is shown onthe left side of each panel. The figure shows that in a patient with aprevious posterior–inferior myocardial infarction, lower voltages arerecorded in the infarcted area. Please note the extent of fragmentationdisplayed on the virtual electrograms recorded from the infarcted area.
Fig. 3 A 12-lead ECG of the first VT induced in the patient (cycle length: 36during VT. Diastolic activity is observed in the posterolateral wall, which shiftsendocardial activity at the exit is indicated by the large high-voltage area an
1132 P. Della Bella et al.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article-abstract
14/102 (13%) patients in the MONO group and 14/35(40%) patients in the PLEO group, while the procedurewas a complete failure in 18/102 (18%) MONO group and13/35 (37%) PLEO group patients.
The distribution of acute results differed significantlybetween PLEO and MONO patients (p < 0:0005): of 78patients in whom all induced VTs (Class A) were pre-vented, 70 patients (90%) had a single clinical VT ascompared to 8 with clinical pleomorphism. Conversely,partial success (Class B result) or failure (Class C result)occurred more frequently in the patients with clinicalpleomorphism, in whom hemodynamically intolerableand, therefore, unmappable VTs were induced morefrequently (14/28 [50%] and 13/31 [42%], p ¼ 0:001 forboth Class B and C vs. Class A post hoc comparisons). Theodds of success (Class A result) for patients with pleo-morphic VTs was 5 times lower than for patients withmonomorphic VTs, after accounting for possible con-founders (Table 2). The only other independent predictorwas the induced VT cycle length, which was about 15%longer when the ablation procedure was fully successful.Particularly, inducing a single VT morphology or 2 ormore VT morphologies was irrelevant in determiningRFCA success in MONO patients (33/44 [75%] and 37/58[64%], respectively, p ¼ 0:283).
Multiple induced VTs: relation of acuteprocedure result to the presence orabsence of a shared isthmus
Among 93 patients with multiple VT morphologies in-duced by electrophysiological stimulation, 35 had clinicalpleomorphism while the remaining 58 presented with asingle VT morphology. In 30 patients (33%), a single
7 ms) (A). (B–G) The pattern of endocardial activation at various timesupward (C) and exits at the anterolateral wall (F–G) The rapid spread of
d sharp QS pattern of the virtual electrogram recorded at sites 11–15.
/25/13/1127/465311 by guest on 04 April 2019
Incidence and significance of pleomorphism in patients with postmyocardial infarction ventricular tachycardia 1133
isthmus was shared by two VT morphologies based uponthe aforementioned criteria. In 20/30 (67%) of thesepatients, ablation of dual VT morphologies was accom-
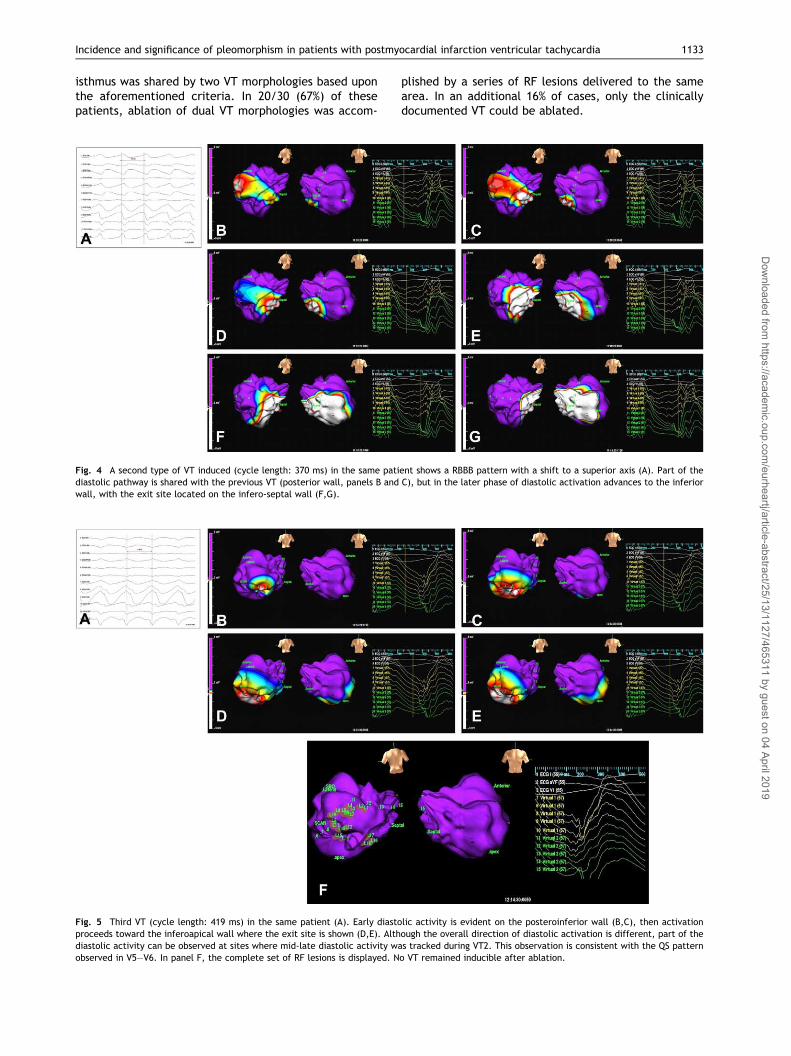
Fig. 4 A second type of VT induced (cycle length: 370 ms) in the same patidiastolic pathway is shared with the previous VT (posterior wall, panels B andwall, with the exit site located on the infero-septal wall (F,G).
Fig. 5 Third VT (cycle length: 419 ms) in the same patient (A). Early diastoproceeds toward the inferoapical wall where the exit site is shown (D,E). Althdiastolic activity can be observed at sites where mid-late diastolic activity wobserved in V5–V6. In panel F, the complete set of RF lesions is displayed. N
plished by a series of RF lesions delivered to the samearea. In an additional 16% of cases, only the clinicallydocumented VT could be ablated.
ent shows a RBBB pattern with a shift to a superior axis (A). Part of theC), but in the later phase of diastolic activation advances to the inferior
lic activity is evident on the posteroinferior wall (B,C), then activationough the overall direction of diastolic activation is different, part of theas tracked during VT2. This observation is consistent with the QS patterno VT remained inducible after ablation.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article-abstract/25/13/1127/465311 by guest on 04 April 2019
1134 P. Della Bella et al.
Dow
nloaded from https://academ
ic.oup.com/eurhear
At variance with this, successful abolition of all in-duced VTs was achieved in only 39% of patients withmultiple isthmuses or areas of slow conduction. In anadditional 34%, only clinical VTs could be ablated andpersistent inducible non-clinical morphologies remained(Fig. 1).
Results improved when non-conventional mappingtechniques had been implemented to guide catheterablation. Prevention of all induced VTs could beachieved in 9/12 patients (75%), all of them displayingdifferent exit sites or diastolic pathways during differentVTs; all these patients had pleomorphic VT at clinicalpresentation.
Non-contact mappingIn 10 patients (8 presenting with clinical pleomorphism),non-contact mapping of the left ventricle was under-taken to guide catheter ablation of at least one form ofhemodynamically intolerable VT. Twenty-six episodes ofVT were induced and mapped (2–3 per patient). Detailsare shown in Table 3.
In all these patients different VTs had clearly differ-ent exit sites; on the other hand, in 6/10 patients at leastpart of the diastolic pathway of one morphology could betracked within the same area of at least one of the othermorphologies (Figs. 2–5).
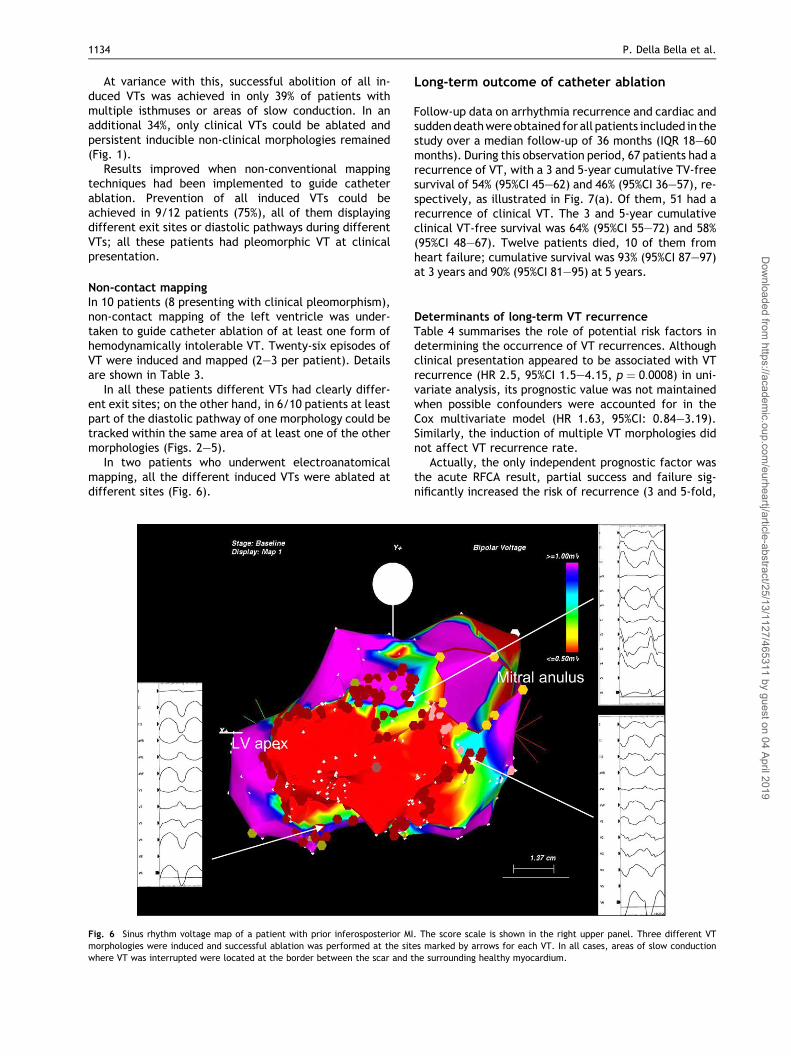
In two patients who underwent electroanatomicalmapping, all the different induced VTs were ablated atdifferent sites (Fig. 6).
Fig. 6 Sinus rhythm voltage map of a patient with prior inferosposterior MImorphologies were induced and successful ablation was performed at the sitwhere VT was interrupted were located at the border between the scar and t
Long-term outcome of catheter ablation
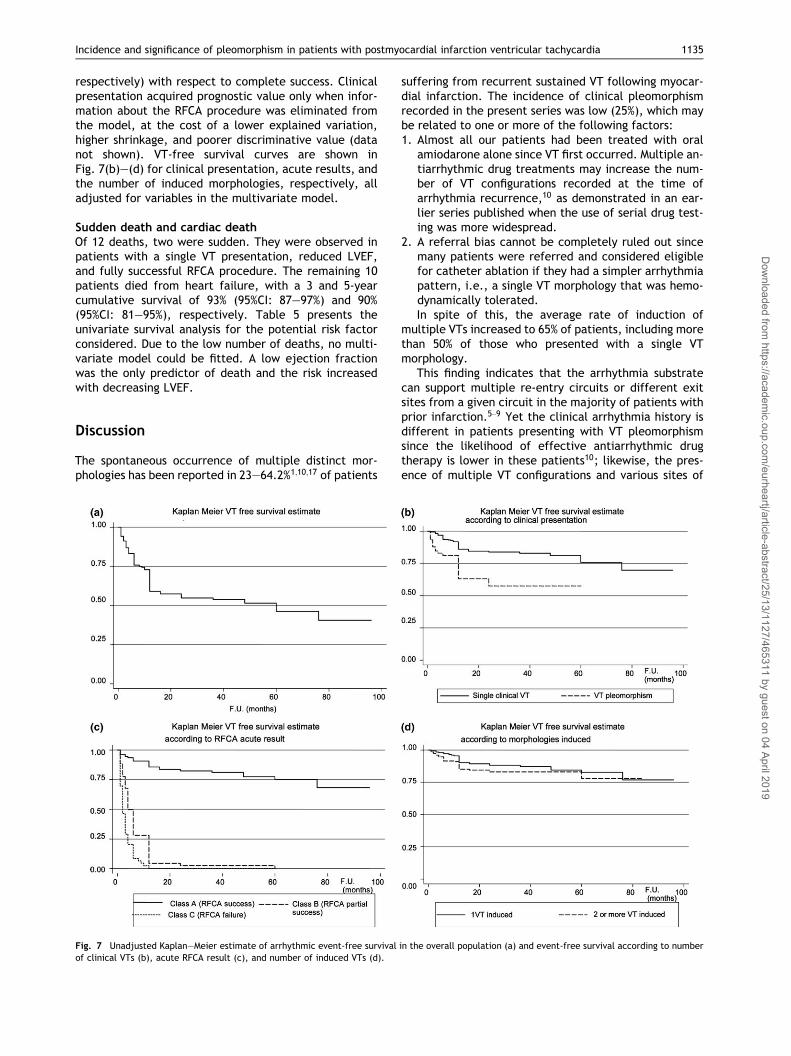
Follow-up data on arrhythmia recurrence and cardiac andsuddendeathwereobtained for all patients included in thestudy over a median follow-up of 36 months (IQR 18–60months). During this observation period, 67 patients had arecurrence of VT, with a 3 and 5-year cumulative TV-freesurvival of 54% (95%CI 45–62) and 46% (95%CI 36–57), re-spectively, as illustrated in Fig. 7(a). Of them, 51 had arecurrence of clinical VT. The 3 and 5-year cumulativeclinical VT-free survival was 64% (95%CI 55–72) and 58%(95%CI 48–67). Twelve patients died, 10 of them fromheart failure; cumulative survival was 93% (95%CI 87–97)at 3 years and 90% (95%CI 81–95) at 5 years.
Determinants of long-term VT recurrenceTable 4 summarises the role of potential risk factors indetermining the occurrence of VT recurrences. Althoughclinical presentation appeared to be associated with VTrecurrence (HR 2.5, 95%CI 1.5–4.15, p ¼ 0:0008) in uni-variate analysis, its prognostic value was not maintainedwhen possible confounders were accounted for in theCox multivariate model (HR 1.63, 95%CI: 0.84–3.19).Similarly, the induction of multiple VT morphologies didnot affect VT recurrence rate.
Actually, the only independent prognostic factor wasthe acute RFCA result, partial success and failure sig-nificantly increased the risk of recurrence (3 and 5-fold,
. The score scale is shown in the right upper panel. Three different VTes marked by arrows for each VT. In all cases, areas of slow conductionhe surrounding healthy myocardium.
tj/article-abstract/25/13/1127/465311 by guest on 04 April 2019
Incidence and significance of pleomorphism in patients with postmyocardial infarction ventricular tachycardia 1135
Dow
nloaded from https://acade
respectively) with respect to complete success. Clinicalpresentation acquired prognostic value only when infor-mation about the RFCA procedure was eliminated fromthe model, at the cost of a lower explained variation,higher shrinkage, and poorer discriminative value (datanot shown). VT-free survival curves are shown inFig. 7(b)–(d) for clinical presentation, acute results, andthe number of induced morphologies, respectively, alladjusted for variables in the multivariate model.
Sudden death and cardiac deathOf 12 deaths, two were sudden. They were observed inpatients with a single VT presentation, reduced LVEF,and fully successful RFCA procedure. The remaining 10patients died from heart failure, with a 3 and 5-yearcumulative survival of 93% (95%CI: 87–97%) and 90%(95%CI: 81–95%), respectively. Table 5 presents theunivariate survival analysis for the potential risk factorconsidered. Due to the low number of deaths, no multi-variate model could be fitted. A low ejection fractionwas the only predictor of death and the risk increasedwith decreasing LVEF.
mic.oup.com
/eurh
Discussion
The spontaneous occurrence of multiple distinct mor-phologies has been reported in 23–64.2%1;10;17 of patients
Fig. 7 Unadjusted Kaplan–Meier estimate of arrhythmic event-free survivalof clinical VTs (b), acute RFCA result (c), and number of induced VTs (d).
suffering from recurrent sustained VT following myocar-dial infarction. The incidence of clinical pleomorphismrecorded in the present series was low (25%), which maybe related to one or more of the following factors:1. Almost all our patients had been treated with oral
amiodarone alone since VT first occurred. Multiple an-tiarrhythmic drug treatments may increase the num-ber of VT configurations recorded at the time ofarrhythmia recurrence,10 as demonstrated in an ear-lier series published when the use of serial drug test-ing was more widespread.
2. A referral bias cannot be completely ruled out sincemany patients were referred and considered eligiblefor catheter ablation if they had a simpler arrhythmiapattern, i.e., a single VT morphology that was hemo-dynamically tolerated.In spite of this, the average rate of induction of
multiple VTs increased to 65% of patients, including morethan 50% of those who presented with a single VTmorphology.
This finding indicates that the arrhythmia substratecan support multiple re-entry circuits or different exitsites from a given circuit in the majority of patients withprior infarction.5–9 Yet the clinical arrhythmia history isdifferent in patients presenting with VT pleomorphismsince the likelihood of effective antiarrhythmic drugtherapy is lower in these patients10; likewise, the pres-ence of multiple VT configurations and various sites of
in the overall population (a) and event-free survival according to number
eartj/article-abstract/25/13/1127/465311 by guest on 04 April 2019
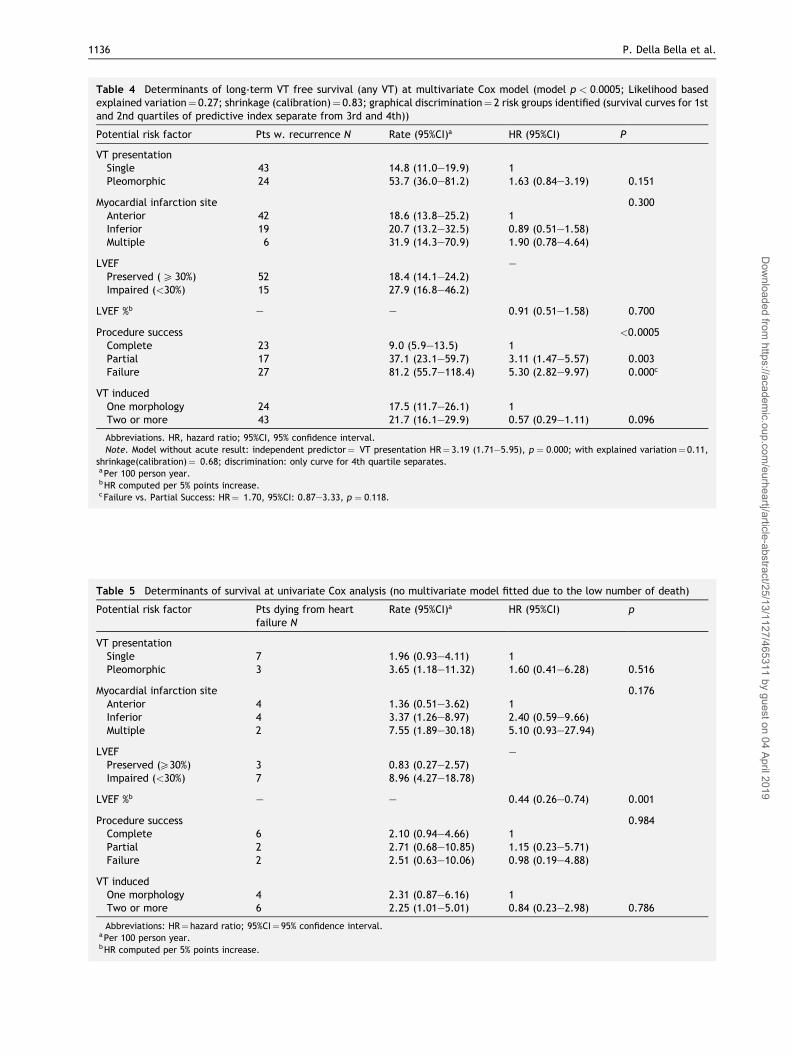
Table 4 Determinants of long-term VT free survival (any VT) at multivariate Cox model (model p < 0:0005; Likelihood basedexplained variation¼ 0.27; shrinkage (calibration)¼ 0.83; graphical discrimination¼ 2 risk groups identified (survival curves for 1stand 2nd quartiles of predictive index separate from 3rd and 4th))
Potential risk factor Pts w. recurrence N Rate (95%CI)a HR (95%CI) P
VT presentationSingle 43 14.8 (11.0–19.9) 1Pleomorphic 24 53.7 (36.0–81.2) 1.63 (0.84–3.19) 0.151
Myocardial infarction site 0.300Anterior 42 18.6 (13.8–25.2) 1Inferior 19 20.7 (13.2–32.5) 0.89 (0.51–1.58)Multiple 6 31.9 (14.3–70.9) 1.90 (0.78–4.64)
LVEF –Preserved (P 30%) 52 18.4 (14.1–24.2)Impaired (<30%) 15 27.9 (16.8–46.2)
LVEF %b – – 0.91 (0.51–1.58) 0.700
Procedure success <0.0005Complete 23 9.0 (5.9–13.5) 1Partial 17 37.1 (23.1–59.7) 3.11 (1.47–5.57) 0.003Failure 27 81.2 (55.7–118.4) 5.30 (2.82–9.97) 0.000c
VT inducedOne morphology 24 17.5 (11.7–26.1) 1Two or more 43 21.7 (16.1–29.9) 0.57 (0.29–1.11) 0.096
Abbreviations. HR, hazard ratio; 95%CI, 95% confidence interval.Note. Model without acute result: independent predictor¼ VT presentation HR¼ 3.19 (1.71–5.95), p ¼ 0:000; with explained variation¼ 0.11,
shrinkage(calibration)¼ 0.68; discrimination: only curve for 4th quartile separates.aPer 100 person year.bHR computed per 5% points increase.cFailure vs. Partial Success: HR¼ 1.70, 95%CI: 0.87–3.33, p ¼ 0:118.
Table 5 Determinants of survival at univariate Cox analysis (no multivariate model fitted due to the low number of death)
Potential risk factor Pts dying from heartfailure N
Rate (95%CI)a HR (95%CI) p
VT presentationSingle 7 1.96 (0.93–4.11) 1Pleomorphic 3 3.65 (1.18–11.32) 1.60 (0.41–6.28) 0.516
Myocardial infarction site 0.176Anterior 4 1.36 (0.51–3.62) 1Inferior 4 3.37 (1.26–8.97) 2.40 (0.59–9.66)Multiple 2 7.55 (1.89–30.18) 5.10 (0.93–27.94)
LVEF –Preserved (P30%) 3 0.83 (0.27–2.57)Impaired (<30%) 7 8.96 (4.27–18.78)
LVEF %b – – 0.44 (0.26–0.74) 0.001
Procedure success 0.984Complete 6 2.10 (0.94–4.66) 1Partial 2 2.71 (0.68–10.85) 1.15 (0.23–5.71)Failure 2 2.51 (0.63–10.06) 0.98 (0.19–4.88)
VT inducedOne morphology 4 2.31 (0.87–6.16) 1Two or more 6 2.25 (1.01–5.01) 0.84 (0.23–2.98) 0.786
Abbreviations: HR¼ hazard ratio; 95%CI¼ 95% confidence interval.aPer 100 person year.bHR computed per 5% points increase.
1136 P. Della Bella et al.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article-abstract/25/13/1127/465311 by guest on 04 April 2019

Incidence and significance of pleomorphism in patients with postmyocardial infarction ventricular tachycardia 1137
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article-abstract/25/13/1127/465311 by guest on 04 April 2019
origin of VT has been described as a predictor of failureof surgical arrhythmia treatment.12;13
The complexity of the arrhythmia substrate is proba-bly the most important limitation to more extensive useof catheter ablation in treating postmyocardial infarc-tion VT. It is a widespread concern that selectiveinterruption of the diastolic pathway resulting in effec-tive ablation of the target arrhythmia may not be suffi-cient to prevent further recurrences due to the possibleonset, in the subsequent period, of functional re-entrycircuits related to the scar tissue.
The induction of multiple VT morphologies has beenseen as a relative contraindication to catheter ablationby some authors17–19 since the persistent inducibility ofnon-clinical VT after catheter ablation is associated withan increased likelihood of arrhythmia recurrence.20;21;27
On the other hand, in patients presenting with he-modynamically tolerated VTs, the long-term outcome isprimarily related to the acute result of catheter ablationand is unaffected by the number of presenting or inducedVT morphologies.27
The question of whether the occurrence of sponta-neous pleomorphism carries the same adverse prognosticsignificance as the induction of multiple VTs has neverbeen addressed. Furthermore, it remains unclear whe-ther the induction of multiple VTs in a patient with only asingle clinically documented morphology carries thesame adverse prognostic significance as the spontaneousoccurrence of multiple VTs.
Clinical vs. induced VTs
In our study, the induction of multiple VT morphologieswas the rule among patients with clinical pleomorphismbut it also occurred in more than 55% of those who hadhad only one VT morphology, as has also been describedin other series.20;21
Prevention of the target arrhythmia (fully successfuland partially successful RFCA) was achieved in 75% ofpatients in whom a single VT was induced compared to86% of those with 2 or more induced morphologies;overall prevention of any inducible VT was obtained in64% of patients who had suffered only one VT but inwhom multiple VTs could be induced at electrophysio-logical study. It appears, therefore, that in patients witha single clinical VT morphology the induction of multipleVT morphologies did not affect the acute success ofcatheter ablation.
At variance with this, acute results were much pooreramong patients with clinically documented VT pleomor-phism, in whom a fully successful procedure could beachieved in only 23%; a partial result (i.e., prevention ofsingle clinical VT, with persistent inducibility of otherVTs) was achieved in an additional 40% of these patients.The most frequent cause for the impossibility to achievea complete success in this group of patients was hemo-dynamic intolerance of the induced VTs, that could bedemonstrated in a significantly higher percentage ofpatients with VT pleomorphism. This may result from themore advanced degree of left ventricular dysfunction inthis group of patients and the shorter cycle length of the
induced VTs, both features that have already been re-cognised in other series20 describing the electrophysio-logical properties of patients with multiple VTs.
The possibility of demonstrating multiple separatesites of origin of arrhythmias adversely affects the out-come of the acute procedure. On the one hand, detailedexperimental mapping studies in a canine post-MI VTmodel5 have shown that in a substantial number of casesdifferent surface VT morphologies are related to differ-ent patterns of endocardial activation that, however,spread from the same single site of breakthrough(probably a shared isthmus).
The non-contact mapping data in the small subgroupof this patient population support this view. A sharedpart of the diastolic pathway followed by different pat-terns of endocardial activation in a later phase of dias-tole and clearly separate exit points was a frequentfinding in pleomorphic VTs. Usually, in spite of thesefindings, distinct ablation lines crossing the diastolicpathways were required to prevent further induction ofthe different VTs. It follows that information on the ac-tivation pattern of any induced VT should probably bepart of the mapping procedure for patients undergoingcatheter ablation of pleomorphic VT. The use of non-contact mapping techniques offers a significant advan-tage in this setting, since it can be also applied tohemodynamically intolerable arrhythmia.
Determinants of long-term outcome
While clinical presentation with multiple VTmorphologiesadversely affected long-term arrhythmia-free survival,the induction of different VTs in the pre-ablation elec-trophysiological study did not confer a worse prognosis,provided that complete arrhythmia suppression could beachieved by the catheter ablation procedure. The data ofour study, however, stress the importance of so-callednon-clinical VT induced after ablation in predicting ar-rhythmia recurrence. The target of a VT-ablation proce-dure should be the completeprevention of any inducedVT.
The relevance of the extent of arrhythmia suppressionis further supported by the finding at multivariate anal-ysis that the only factor associated to enhanced ar-rhythmia-free survival was a fully successful procedure;partially successful results, i.e., prevention of clinical VTwith persistent inducibility of other forms of sustainedventricular arrhythmias, are in fact equivalent to com-plete failure.
Conclusions
Caution is advised before considering documented mor-phology as the only relevant target in patients with re-current VTs following myocardial infarction.20;21;27
Treatment with different antiarrhythmic drugs mayaffect the functional properties of the arrhythmia sub-strate, originating a different QRS configuration.5 Theextent of abnormal myocardial tissue and number ofarrhythmia recurrences are factors facilitating the onsetof multiple VT morphologies,2 and it may well be that the

1138 P. Della Bella et al.
Dow
nloaded from https://academ
ic.oup.com/eurh
ultimate fate of patients with VT following myocardialinfarction is the occurrence of multiple arrhythmiamorphologies.
However, patients who present a single VT morphol-ogy seem to be more favourably suited to a catheterablation procedure, even if multiple VT morphologies aredemonstrated in the electrophysiological study.
As shown in a recent study,27 catheter ablation andantiarrhythmic drug treatment are a reasonable strategyin patients presenting with hemodynamically toleratedpostmyocardial infarction ventricular tachycardias re-fractory to pharmacological treatment. The number ofpreviously induced VTs did not affect arrhythmia recur-rence, while prevention of any induced arrhythmia fol-lowing the procedure was a significantly favourableprognostic factor.
A second relevant point is the poorer result of cath-eter ablation in patients presenting with multiple VTmorphologies, where the higher occurrence of intolera-ble arrhythmias poses major limitations.
More advanced mapping techniques allowing theanalysis of endocardial activation during fast VTs, such asnon-contact mapping23–25 or electroanatomical locationand isolation of the scar tissue,26 should probably beused to guide catheter ablation when the treatment of apatient with spontaneous multiple VTs is considered,since the result of the procedure rather than the clinicalpresentation is what affects long-term outcome.
eartj/article-abstract/25/13/1127/465311 by guest on 04 April 2019
References
1. Josephson ME, Horowitz LN, Farshidi A et al. Recurrent sustainedventricular tachycardia. 4. Pleomorphism. Circulation 1979;59(3):459–68.
2. Wilber DJ, Davis MJ, Rosenbaum M et al. Incidence and determinantsof multiple morphologically distinct sustained ventricular tachycar-dias. J Am Coll Cardiol 1987;10(3):583–91.
3. Miller JM, Kienzle MG, Harken AH et al. Morphologically distinctsustained ventricular tachycardias in coronary artery disease: signif-icance and surgical result. J Am Coll Cardiol 1984;4(6):1073–9.
4. Stevenson W. Ventricular tachycardia after myocardial infarction:from arrhythmia surgery to catheter ablation. J Cardiovasc Electro-physiol 1995;6:942–50.
5. Osswald S, Wilber DJ, Lin JL et al. Mechanism underlying differentsurface ECG morphologies of recurrent monomorphic ventriculartachycardia and their modification by procamide. J CardiovascElectrophysiol 1997;8(1):11–23.
6. De Baaker JMT, van Capelle FJL, Janse MJ et al. Reentry as a cause ofventricular tachycardia in patients with chronic ischemic heartdisease: electrophysiologic and anatomic correlation. Circulation1988;77(3):589–606.
7. Costeas C, Peters NS, Waldecker B et al. Mechanism causing sustainedventricular tachycardia with multiple QRS morphologies: result ofmapping studies in the infarcted canine heart. Circulation1997;96(10):3721–31.
8. Downar E, Kimber S, Harris L et al. Endocardial mapping ofventricular tachycardia in the intact human ventricle. II. Evidenceof multiuse reentry in a functional sheet of surviving myocardium. JAm Coll Cardiol 1992;20(4):869–78.
9. Downar E, Saito J, Doig C et al. Endocardial mapping of ventriculartachycardia in the intact human ventricle. III. Evidence of multiuse
reentry with spontaneous and induced block in portions of reentrantpath complex. J Am Coll Cardiol 1995;25(7):1591–600.
10. Mitrani RD, Biblo RA, Carlson MD et al. Multiple monomorphicventricular tachycardia configurations predict failure of antiarrhyth-mic drug therapy guided by electrophysiologic study. J Am CollCardiol 1993;22(4):1117–22.
11. Trappe HJ, Brugada P, Talajic M et al. Value of induction ofpleomorphic ventricular tachycardia during programmed stimulation.Eur Heart J 1989;10(2):133–41.
12. Kron IL, Lerman BB, Nolan SP et al. Sequential endocardial resectionfor the surgical treatment of refractory ventricular tachycardia. JThorac Cardiovasc Surg 1987;94(6):843–7.
13. Miller JM, Kienzle MG, Harken AH et al. Subendocardial resection forventricular tachycardia: predictors of surgical success. Circulation1984;70(4):624–31.
14. Wilber DJ, Kopp DE, Glascock DN et al. Catheter ablation of themitral isthmus for ventricular tachycardia associated with inferiorinfarction. Circulation 1995;92(12):3481–9.
15. Morady F, Kadish A, Rosenheck S et al. Concealed entrainment as aguide for catheter ablation of ventricular tachycardia in patients withprior myocardial infarction. J Am Coll Cardiol 1991;17(3):678–89.
16. Aizawa Y, Chinushi M, Naitoh N et al. Catheter ablation of ventriculartachycardia with radiofrequency currents, with special reference tothe termination and minor morphologic change of reinduced ven-tricular tachycardia. Am J Cardiol 1995;76:574–9.
17. Morady F, Harvey M, Kalbfeisch SJ et al. Radiofrequency catheterablation of ventricular tachycardia in patients with coronary arterydisease. Circulation 1993;87(2):363–72.
18. Kim YH, Sosa-Suarez G, Trouton TG et al. Treatment of ventriculartachycardia by transcatheter radiofrequency ablation in patientswith ischemic heart disease. Circulation 1994;89(3):1094–102.
19. Gonska BD, Cao K, Schaumann A et al. Catheter ablation ofventricular tachycardia in 136 patients with coronary artery disease:result and long-term follow-up. J Am Coll Cardiol 1994;24(6):1506–14.
20. Rothman SA, Hsia HH, Coss�u SF et al. Radiofrequency catheterablation of post-infarction ventricular tachycardia. Long-term suc-cess and the significance of inducible nonclinical arrhythmias.Circulation 1997;96(10):3499–508.
21. Stevenson WG, Friedman PL, Kocovic D et al. Radiofrequencycatheter ablation of ventricular tachycardia after myocardial infarc-tion. Circulation 1998;98(28):308–14.
22. Schilling RJ, Peters NS, Davies DW. Feasibility of a non-contactcatheter for endocardial mapping of human ventricular tachycardia.Circulation 1999;99:2543–52.
23. Schilling RJ, Peters NS, Davies DW. Mapping and ablation ofventricular tachycardia with the aid of a non-contact mappingsystem. Heart 1999;81(6):570–5.
24. Strickberger SA, Knight BP, Michaud GF et al. Mapping and ablation ofventricular tachycardia guided by virtual electrograms using anoncontact, computerized mapping system. J Am Coll Cardiol2000;35(2):414–21.
25. Della Bella P, Pappalardo A, Riva S et al. Non contact mapping toguide catheter ablation of untolerated ventricular tachycardia. EurHeart J 2002;23:742–52.
26. Marchlinski FE, Callans DJ, Gottlieb CD et al. Linear ablation lesionsfor control of unmappable ventricular tachycardia in patients withischemic and nonischemic cardiomyopathy. Circulation2000;101(11):1288–96.
27. Della Bella P, De Ponti R, Uriarte JAS et al. Catheter ablation andantiarrhythmic drugs for hemodynamically tolerated ventriculartachycardia. Eur Heart J 2002;23:414–24.
28. Bogun F, Li YG, Groenefeld G et al. Prevalence of a shared isthmus inpostinfarction patients with pleiomorphic, hemodynamically toler-ated ventricular tachycardias. J Cardiovasc Electrophysiol2002;13(3):237–41.
29. Poole JE, Bardy GH. Sudden Cardiac Death. In: Zipes DP, Jalife J,editors. Cardiac Electrophysiology - From Cell to Bedside. second ed.WB Saunders; 1995. p. 812–32.