Embed Size (px)
Citation preview

Int. J . Cancer: 46, 356-361 (1990) 0 1990 Wiley-Liss, Inc.
INCIDENCE AND DETERMINANTS OF SKIN CANCER IN A HIGH-RISK
Publication of the International Union Against Cancer Publication de I'Union lnternationale Contre le Cancer
AUSTRALIAN POPULATION Adele GREEN' and Diana BATTISTUTTA Queensland Institute of Medical Research, Bramston Terrace, Brisbane 4006, Queensland, Australia.
In a Queensland community, we surveyed the incidence of basal-cell carcinoma (BCC) and squamous-cell carcinoma (SCC), and associated risk factors. In December, 1986, 2,095 residents were examined by dermatologists for skin cancer. Of these, 1,770 further participated in a follow-up postal sur- vey in December, 1987, regarding all skin cancers in the pre- ceding 2 years, and 87 reported being treated for skin cancer in the 2-year period between December 1985 and November 1987. The estimated annual incidence rates of non-melanoma skin cancer in men and women aged 2 e 6 9 years were 2,3891 100,000 and I ,908/100,000 respectively, with an overall ratio of BCC cases to SCC cases of 4.5 to one. While both tumour types occurred more commonly in fair-complexioned people, the risk associated with high sun exposure was greater for SCC than for BCC. Clinical signs of solar skin damage, espe- cially the number of solar keratoses on the face, were the strongest predictors of both types of skin cancer.
It is paradoxical that the most common cancer, non-me- lanocytic skin cancer (NMSC), is one of the least researched (Harvey et al., 1989). The lack of baseline data is even more disturbing in the light of observed large increases in skin cancer in white populations in the past 20 years (Urbach, 1989) and under the threat of future world-wide increases following stratospheric ozone depletion (Scotto et al., 1988; Urbach, 1989). Although incidence rates of cutaneous melanoma have been routinely and extensively documented, the unknown pro- portions of NMSC that are histologically confirmed or regis- tered in any population prevent accurate estimation of inci- dence (Sobin et al . , 1982), and analysis of risk factors is hand- icapped.
Some of the few descriptive data that are available for pop- ulations in the northern hemisphere have come from 2 skin cancer surveys conducted in various areas of the United States in 1971-72 and 1977-78 by the National Cancer Institute (Fears and Scotto, 1982). All non-recurring NMSCs treated in the survey periods in hospital outpatient departments or re- corded by dermatologists, pathologists, surgeons or other phy- sicians treating skin cancer, were recorded in the study loca- tions. In the 1977-78 survey the annual age-adjusted incidence rate of NMSC among whites over 25 years was estimated to be 233/100,000 (Scotto and Fraumeni, 1982), and people resident at latitudes 30"-35"N were at appreciably greater risk than those at high latitudes; e .g . in New Mexico and in Seattle the respective age-adjusted incidence rates were 337/ 100,000 and 189/100,000. The highest rate in a US population has been reported among Hawaiian Caucasians: residents of Kauai liv- ing at 22"N had an age-adjusted NMSC incidence of 9061 100,000 in 1983 (Stone et al., 1986). In Australia, recent information about skin cancer was obtained during a national random household survey conducted by a market research company in 1985 (Giles et al., 1988). Among 30,976 respon- dents aged 14 or over, there were 253 medically confirmed skin cancers, giving an age-adjusted incidence estimate of 823/ 100,000 person years. There was also a latitude gradient in NMSC incidence in Australia: people living north of 29"s lat- itude (which included all residents of the states of Queensland, the Northern Territory and a small proportion from Western Australia) had an estimated incidence rate of 1,242/100,000, compared with 489/100,000 among people living at latitudes higher than 37"s (Giles et al., 1988). Rates increased with age,
were significantly higher in men than in women after 60 years of age, and in people born in Australia compared with British migrants. Those who said they always burnt and never tanned in strong sun had an NMSC incidence of 1,764/100,000, while those who tanned without burning had a rate of 616/100,000.
Within Australia, people living in Queensland have long been considered to have the highest skin cancer risk of all (Urbach, 1971; Green et al., 1988), yet there are no data regarding determinants of this risk among those with incident skin cancers in this population. Gordon el al. (1972) carried out extensive investigations into the epidemiology of skin can- cer in Queensland in the 1960s, but relative risks were esti- mated for persons having a positive history of skin cancer compared with those without such a history. The lack of in- fluence of environmental factors, especially outdoor occupa- tions, which they observed, could be explained if modification of outdoor habits had occurred after a previous diagnosis of skin cancer.
In order to gain information about skin cancer occurrence in Queensland, and current factors influencing the development of NMSC, we have surveyed the incidence of these tumours in a typical south-east community.
METHODS
Study population Subjects were first seen and medically examined in the first
week of December, 1986, during a prevalence survey of skin cancer in young and middle-aged adults in a Queensland pop- ulation, as described elsewhere (Green et al., 1988). A sample of 3,000 residents of Nambour, an urban centre situated at 26"S, was chosen at random from the electoral roll, of whom 2,685 were still residents at the time of this initial survey. Of these, 2,095 people took part in the survey, a response rate of 78% among permanent residents aged 20 to 69 years. Infor- mation was obtained about occupational and recreational sun exposure, experience of sunburns that were painful for at least 24 hr and previous skin cancer. Each person was examined by one of a team of dermatologists to assess colour of eyes, hair and unexposed skin, and for the presence of skin cancer (bi- opsied for histologic confirmation) and other signs of actinic damage defined and graded in standard fashion (Green et al., 1988), including solar keratoses, solar lentigines, facial telan- giectasia and elastosis of the neck. In 90% of subjects only the head and neck, backs of hands and forearms were examined, and in a random 10% the upper chest, back and shoulders, upper arms, thighs and legs were also examined.
One year after the examination survey (December, 1987), all participants were mailed a questionnaire requesting details of any skin cancers treated by a doctor in the preceding 2 years (December 1, 1985 to November 30, 1987). Treating doctors were contacted subsequently to confirm that either a definite
'To whom reprint requests should be sent.
Received: February 5 , 1990 and in revised form May 3, 1990.

SKIN CANCER I N A N AUSTRALIAN POPULATION 357
clinical or a lhistologic diagnosis of basal-cell carcinoma (BCC) or squamous#-cell carcinoma (SCC) had been made in the spec- ified period.
Data analysis Cases of skin cancer that were prevalent on December 1-6,
1986 (Green et al., 1988), were excluded from all analyses. Age- and sen-specific incidence rates were calculated from the number of new cases of confirmed BCC and SCC (excluding carcinoma in situ and Bowen’s disease) diagnosed in the study population between December 1, 1985 and November 30, 1987. Unless otheirwise stated, a case of BCC or SCC refers to a person affected rather than to an incident lesion, so that a person who had developed multiple skin cancers of the same type was counted once only. Incidence rates were adjusted by direct standardization to the corresponding age distribution of the world population.
The relative risk of BCC or SCC was estimated as the inci- dence rate among persons in a certain exposure category di- vided by the corresponding rate among those not exposed. Multivariate modding of relative risk to obtain estimates ad- justed for all potential confounding variables was performed using logistic regression techniques (Breslow and Day, 1980) and the EGRET (1988) statistical package. For final risk esti- mates calculated under multivariate models, 95% confidence limits of the true values have been computed using the esti- mated log relative risk and associated variances (Schlesselman, 1982).
RESULTS
Of the original study population, 1,770 persons took part in the follow-up survey, a response rate of 84.5%. There were 87 new cases of confirmed non-melanocytic skin cancer diag- nosed from December 1, 1985 to November 30, 1987: 39 cases in 1985-86, and 48 cases in 1986-87. Among males aged 20-69 years the age-adjusted incidence rate of NMSC was 2,247/100,000 in 1985-86 and 2,531/100,000 in 1986-87 (av- erage 2,398/100,000); among women of this age group the rates were 1,775/100,000 in 1985-86 and 2,040/100,000 in 1986-87 (average 1,908/100,000). The age-adjusted ratio of incident BCC cases to SCC cases diagnosed over the 2 years was 4.5 to 1. Seven persons developed more than one lesion in
1985-86, and 11 in 1986-87, giving an age-adjusted ratio of basal-cell lesions to squamous-cell lesions of 5.1 to 1. (For this calculation, if a subject had been confirmed as having “multi- ple” BCCs, number unspecified, a total of 3 was counted.)
Age-specific rates of reported BCCs and SCCs rose steeply with age, although no SCCs occurred before age 40 years, and only one before age 50 years (Table I). Compared to females under 70 years, males did not have uniformly higher rates of BCC or of SCC in all age groups: for example, females aged 4 0 4 9 years had higher rates of BCC, while rates of SCC and of BCC were similar for males and females in the 50-59 and 60-69 year age groups, respectively.
Relative risks of BCC and SCC were estimated in multivari- ate analyses (Table 11). Controlling for age and sex, the RRs of BCC and SCC in persons with the fairest complexions were highest, compared to those with dark skin and hair (colour of complexion and hair assessed by a dermatologist). The RR (95% confidence limits) of BCC in persons with fair skin was 2.9 (0.7, 12.9); in those with blonde or light brown hair, 2.1 (1.1,4.0); and with red hair, 2.9 (1 . I , 7.6), and corresponding RRs of SCC were similar. Controlling for age, sex, skin colour and past history of NMSC, no increased risk of BCC was associated with multiple sunburns, or recreational sun expo- sure, and the RR of BCC associated with mainly outdoor oc- cupations was 1.3 (0.6, 2.8). On the other hand, elevated risks of SCC were observed in association with all these indicators of sun exposure: there was a 3-fold increase in risk of SCC in persons who had reported 2 or more painful sunburns, com- pared to those reporting none or one, and the RRs associated with predominantly outdoor occupations and leisure activities were 5.5 (1.1, 28.2) and 3.9 (0.5, 30.9), respectively.
We next assessed modification by skin colour on the effects of age, and other risk factors for BCC (Table III; Figs. 1 4 ) and SCC (Table In). Although risk factor status was estab- lished at the mid-point of the study period, the stable nature of the factors (e.g., natural skin colour, overall level of occupa- tional sun exposure) was such that substantial change in status from that existing 12 months previously was considered un- likely. Among persons of dark or olive complexion, there were no cases of SCC and only 2 of BCC; however, there were sufficient incident cases to calculate point estimates of relative risks, stratified according to whether persons were of medium or fair complexion. Risk of BCC was higher with increasing
TABLE I - PREVALENCE AND INCIDENCE OF BASAL-CELL CARCINOMA (BCC) AND SQUAMOUS-CELL CARCINOMA (SCC) PER 100,ooO AMONG PERSONS AGED 20-69 YEARS IN NAMBOUR, QUEENSLAND, 1985-1987
Age group (years)
20-29 30-39 40-49 50-59 60-69 All’
BCC Prevalence rate - 616.0 3,490.7 4,972.2 12,743.9 3,523.8
Dec., 1986 (0;o) ( 3 0 (11;1) (9;4) (29;6) (number of case+
Male 329.0 1,234.6 915.0 3,546.0 4,362.4 1,772.7 Female 314.5 625.0 2,320.7 1,651.0 4,248.4 1,610.0 (number of cases) (2) (7) (14) (17) (26) (66)
Prevalence rate - - 211.4 750.0 1,524.4 383.8 Dec., 1986 (0) (0) (1) (3) (5) (9)
Incidence rate3
SCC
(number of cases)
Male - - 304.9 709.2 3,020.0 599.8 Female - - - 707.6 1,301.2 298.4
Incidence rate3
(number of cases) (0) (0) (1) (7) (13) (21) ‘Standardized to the age distribution (20-69 years) of the world population.-’Fint number refers to number of subjects with
BCCs diagnosed on head and forearms in total sample; second number refers to number of subects with BCCs diagnosed on
per 100,OOO population. sites other than head and forearms in a random 10% sample who had full body examinations.- 3 Average annual incidence rate

358 GREEN A N D BATTISTUTTA
TABLE II - RELATIVE RISKS (RR) OF BASAL-CELL CARCINOMA (BCC) AND SQUAMOUS-CELL CARCINOMA (SCC) IN RELATION TO SKIN AND HAIR COLOUR, NUMBER OF PAINFUL SUNBURNS, AND OCCUPATIONAL AND
LEISURE-TIME SUN EXPOSURE. ADJUSTED FOR AGE AND SEX
Factor BCC RR (95% CLI
SCC RR (95% CLI
Skin colour Olive 1.0 Medium 1.3 (0.3, 6.1) Fair 2.9 (0.7, 12.9)
Dark browdblack 1 .o Blonde/light brown 2.1 ( 1 . 1 , 4.0) Red/auburn 2.9 ( 1 . 1 , 7.6)
0 1 .o 1 0.5 (0.2, 1.4) 2-5 0.6 (0.3, 1.5) 6 + 1.0 (0.4, 2.5)
Hair colour
Number of painful sunburns
Occupational exposure Mainly indoors 1 .o Indoors and outdoors 1.5 (0.8, 2.9) Mainly outdoors 1.3 (0.6, 2.8)
Leisure exposure Mainly indoors 1 .o Indoors and outdoors 1.0 (0.4, 2.2) Mainlv outdoors 0.6 (0.3. 1.3)
1.0'
2.3 (0.9, 6.2)
1 .o 1.8 (0.6, 5.3) 3.3 (0.7, 14.4)
1 .O'
3.3 (0.9, 12.3) 3.0 (0.7, 12.2)
1 .o 4.4 (0.9, 20.9) 5.5 ( 1 . 1 , 28.2)
1 .o 2.0 (0.2, 19.9) 3.9 (0.5. 30.9)
'Reference category taken as the first 2 categories combined due to insufficient cases with baseline exposure.
age in persons with fair skin than in those with medium com- plexion, though this was not true of SCC. Both BCC and SCC were associated with red hair, and with blonde hair in medium- skinned but not fair-skinned persons. The RR of BCC after multiple painful sunburns was slightly raised but less than 2.0, skin colour notwithstanding, while there was no observable pattern of risk of SCC in relation to episodes of sunburn. Occupational sun exposure, on the other hand, showed a clear association with SCC in both skin colour strata, but only with BCC in persons of medium complexion.
Because of their strong association with prevalent skin can-
cers (Green et al., 1988), we examined clinical signs of solar skin damage and risk of BCC and SCC (Table IV). Taking absence of a sign as the reference category for calculations, the highest RR estimates for both BCC and SCC were observed in relation to the number of solar keratoses present on the face after adjustment for age and sex. Risk was increased with increasing numbers of facial keratoses: those persons with more than 5 keratoses had an RR of 5.6 for BCC (2.3, 13.3), and those with more than 20 had an RR of 10.0 (3.5, 28.2). Elevations in risk of SCC were of the same order. Increasing severity of telangiectasia of the face or elastosis of the neck was similarly associated with increasing risks of BCC and SCC, though florid telangiectasia was more strongly associated with risk of BCC [RR 7.3 (2.1, 26.0)], and severe nuchal elastosis was more strongly associated with SCC [RR 8.3 (1.0, 72.7)]. In relation to number of solar lentigines on the hand, the risk of BCC rose steadily with increasing numbers, to an RR of 3.7 (1.2, 11.7) with more than 20 lentigines. Risk of SCC was unrelated to presence of solar lentigines on the hand.
Finally, there were no significant differences between par- ticipants in the follow-up study and non-participants with re- spect to any identified risk factors apart from the frequency of occurrence of solar lentigines which were observed in more participants (26%) than non-participants (19%) @ < 0.05).
DISCUSSION
These incidence rates of NMSC in Queensland in 1985-87 are among the highest rates of cancer ever reported in a defined population. Between the ages of 20 and 69 years we have estimated that a minimum of 2,389 males/100,000 population (average age-adjusted) were newly affected by skin cancer each year, and among females the rate was 1,9081100,000 with an overall ratio of BCC cases to SCC cases of 4.5 to 1. The rates of incident lesions (rather than persons) treated each year in Queensland were much higher because multiple NMSCs developed in the same year in 20% of the cases. Peak rates were observed in those aged 60-69 years, with little difference between males and females in the occurrence of BCC, and a much reduced BCC to SCC ratio. Only BCCs were reported in persons under 40 years in the study period.
TAJSLE III - AGE-ADJUSTED RELATIVE RISKS (RR) OF BASAL-CELL CARCINOMA (BCC) AND SQUAMOUS-CELL CARCINOMA (SCC) IN RELATION TO HAIR COLOUR, NUMBER OF PAINFUL SUNBURNS AND OCCUPATIONAL SUN
EXPOSURE, SHOWING EFFECTS OF SKIN COLOUR
BCC SCC
Factor Skin Colour' Olive' Medium Fair Olive' Medium Fair
(n) RR (n) RR (n) (n) RR (n) RR (n)
Age (years) <40 40-49 50-59 60-69
(0) 1.0 (4) 1.0 (4) (0) - (0) - (0) (1) 1.3 (3) 3.7 (7) (0) 1.0 (1) - (0) (0) 1.5 (3) 5.7 (11) (0) 2.4 (2) 1.0 (4) (1 ) 3.2 (4) 8.0 (17) (0) 5.9 (3) 2.2 (10)
Hair colour Dark browdblack (2) 1.0 (4) 1.0 (8) (0) 1.0 (1) l.O(4) Blonde/light brown (0) 4.0 (11) 1 . 1 (24) (0) 4.0 (5) 0.6 (7) Red/auburn (0) -2 (0) 1.9 (7) (0) -2 (0) 1.4 (3)
0 (1) 1.0 (3) 1.0 (5) (0) - (0) - (0) Number of painful sunburns
1 (0) 0.9 (1) 1.3 (5) (0) 1.0 (2) l . O ( l ) 2-5 (1) 0.9 (4) 1 . 1 (13) (0) 0.6 (3) 4.9 (7) 6 + (0) 1.8 (7) 1.5 (16) (0) 0.2 (1) 2.6 (6)
Mainly indoor (0) 1.0 (2) 1.0 (16) (0) 1.0 (1) 1.0 (1) Indoor and outdoor (1) 4.9 (8) 1 . 1 (14) (0) 3.4 (5) 7.5 (11) Mainly outdoor (1) 6.8 (5) 0.8 (9) (0) 2.7 ( 1 ) 10.5 (2)
Occupational exposure
'Unexposed skin colour as assessed by a dermatologist.-%R not calculable due to lack of cases in this category.

SKIN CANCER IN AN AUSTRALIAN POPULATION 359
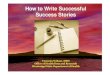
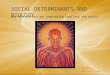
FIGURE I -- Rates of basal-cell carcinoma (BCC) per 100,000 among peoplr: aged 20-69 years according to age and unexposed skin colour. FIGURE 3 - Rates of basal-cell carcinoma (BCC) per 1 ~ ~ , 0 ~ ~
among people aged 20-69 years according to unexposed skin colour and lifetime number of painful sunburns.
The incidence rates in adults under 70 years presented here are some 110 times higher than rates recorded in the USA a decade earlier among whites aged over 25 years (Scotto and Fraumeni, L982), and are almost twice as high as those that were estimated in the national survey for Queensland adults of all ages (Giles et al., 1988). In the latter survey, information about skin cancer was obtained from a sample of 30,747 people across Australia aged over 14 years by a commercial organi- zation. In the course of an omnibus survey to canvass political opinions, consumer preferences and so on, respondents were asked whether they had ever been treated by a doctor for skin cancer, andl the doctor’s name and address if treatment had occurred in the previous 12 months. Besides the quite different methodology used to obtain estimates of NMSC treated in Queensland by Giles et al. (1988), there may be several other reasons for the differences in results. Although we excluded from our calculations all lesions that were prevalent at the mid-point of the study period, which would have biased the estimated incidence downwards, especially in the oldest age group, there was likely to be a heightened awareness of NMSC
in the 12 months following the prevalence survey, which may have inflated the usual incidence of treated lesions for 1986- 87. Also, underestimation due to recall bias here was perhaps less of a problem than in the national survey for the same reason of the Queensland community’s sensitization to skin cancer. Overestimation due to the accepting of clinical diag- noses is not known but is likely to have operated in the national and Queensland surveys to a similar degree (though counter- balancing deficiencies in documentation by treating doctors cannot be excluded: for instance there were almost 4 times as many skin cancers recalled by patients in Nambour as there were confirmed by doctors. In the majority, patients had re- ported solar keratoses as skin cancers, but for a certain pro- portion no record of any lesion treated in the period was avail- able). Finally, bias due to a selected sample of the Nambour population being followed is unlikely, since there were no significant differences between participants in the follow-up study and non-participants with respect to any identified risk factors. Only solar lentigines occurred more frequently in par-

360 GREEN AND BATTISTUTTA
TABLE IV - RELATIVE RISKS (RR) OF BASAL-CELL CARCINOMA (BCC) AND SQUAMOUS-CELL CARCINOMA (SCC) IN RELATION TO PRESENCE OF
CLINICAL SIGNS OF SOLAR SKIN DAMAGE. ADJUSTED FOR AGE AND SEX
BCC RR (95% CL)' Clinical sign
Number of solar keratoses on face None 1 .o 1-5 6-20
3.9 (1.9, 8.0) 5.6 (2.3. 13.3)
> 20 10.0 (3.5, 28.2)
None 1 .o Mild 2.3 (1.1, 4.7) Moderate 2.9 (1.2, 7.1) Severe 7.3 (2.1, 26.0)
None 1.0 Mild-moderate 3.7 (1.6, 8.3) Severe 3.6 (1.3, 9.8)
None 1 .o
Telangiectasia of face
Elastosis of the neck
Number of solar lentigines on hands
SCC RR (95% CL)'
1 .o 1.7 (0.4, 6.5) 4.2 (1.1, 16.1)
11.0 (2.6, 46.6)
1 .o 1.5 (0.4, 5.8) 3.9 (1.0, 16.1) 3.3 (0.3, 36.0)
1 .o 5.4 (0.7, 43.7) 8.3 (1.0, 72.7)
1 .o I-lo 1.5 (0.8, 2.8) 0.8 (0.3, 2.1)
11-20 2.9 (1.2, 7.0) 0.6 (0.1, 4.5) > 20 3.7 (1.2, 11.7) 1.2 (0.1, 9.6)
'95% confidence limits given in parentheses
trast to SCC, other factors appear to be involved in the aetiol- ogy of BCC. These other factors are not known, although there may be a clue in the different anatomic distribution of BCC compared to SCC (Urbach, 1969; Diffey et al., 1979). (De- tailed site-distribution data were not gathered in our follow-up study.) Pearl and Scott (1986) calculated relative tumour den- sities of skin cancer for anatomical subsites accounting for surface area, using a variety of data from clinical studies and tumour registry investigations. They found that relatively more BCCs than SCCs occurred on the nose, around the eyes, and on the back, while relatively fewer occurred on the arms and, in particular, the hands. Using solar dosimetry, Diffey et al. (1979) described a 100-fold range of solar ultraviolet (UV) intensity over facial subsites, and found that, although the distribution of BCCs on the face was compatible with solar aetiology, the correlation between tumour density and UV dose was poor. Zaynoun et al. (1985) studied the relationship of solar elastosis at the sites of occurrence of 262 BCCs, and drew similar conclusions. Various theories of the other factors which might influence BCCs include the thickness of the stratum corneum (Diffey et al., 1979), and the distribution of seba- ceous glands (Graham and McGavran, 1964).
The stronger association of elastosis of the neck observed for SCC compared with BCC in the present study is consistent with the higher sun exposure of SCC patients. It is not known whether the different risks associated with solar lentieines of
ticipants than in non-participants, but this is to have inflated the incidence rates of BCC when the other signs of actinic damage were evenly distributed.
Risk factors for BCC and SCC were similar with respect to skin and hair colour' but the risk Of associated with sun exposure than was BCC. RRs of SCC were 3 to 5.5 times higher in persons reporting excessive sun expo-
(through predominantly outdoor occupations and leisure activ- ities) than those who had at most a single painful sunburn, or who had indoor jobs or leisure activities, respectively. Al- though numbers of cases of SCC were limited and thus confi- dence intervals wide, the differences in point estimates of ef- fect in relation to sun exposure between BCC and SCC were clear, and are consistent with the findings of Urbach (1989). Differences in modification of effect by skin colour between the 2 types of NMSC were also of interest in that there was an increasing risk observed for BCC in association with increasing occupational exposure in medium-complexioned persons, but no effect in the fair-skinned, whereas the fair-skinned outdoor workers were at substantially higher risk of SCC than those of medium complexion. In the light of the somewhat paradoxical associations observed between sun exposure and BCC, in con-
the hands and severe facial telangiectasia are of any vbiologic significance or are chance effects. That solar keratoses are particularly good predictors of risk of NMSC was confirmed, though we saw no evidence of a greater link to SCC, as has been observed elsewhere (Marks et az . , . 1988).
In conclusion, these data indicate how great the problem of NMSC may be among people who have little pigment to protect them from high ambient levels of solar uv radiation.
unless there is a change in public attitudes to sun protection and the symbolism of the suntan, and people in the northern hemi- sphere may need to take similar precautions if UV levels in- crease. Meanwhile, a better understanding of the occurrence and distribution of NMSC, especially of BCCs in white- skinned populations, would Seem desirable.
was more
Sure either (though sunburns) Or chronically The rates in this population can be expected to rise even higher
ACKNOWLEDGEMENTS
We thank the residents of Nambour and their doctors who assisted us in the study, the dematologists who performed the baseline examinations, and the Queensland Cancer Fund and the Australian Cancer Society for their support. Drs. C . Bain and R. MacLennan gave helpful comments on drafts of the text.
REFERENCES
BRESLOW, N. and DAY, N . , Statistical methods in cancer research Vol I : the analysis of case-control studies, pp. 192-246, IARC Publication 32, Lyon (1980). DIFFEY, B.L., TATE, T.J. and DAVIS, A, , Solar dosimetry of the face: the relationship of natural ultraviolet radiation exposure to basal cell carci- noma localisation. Phys. Med. Biol., 24, 931-939 (1979). EGRET users, ~ ~ ~ ~ 1 , statistics and Epidemi,,logy Research corpora- tion, Seattle (1988).
1971-72 and 1977-78. J . nar. Cancer Inst., 69, 365-370 (1982). GILES, G.G., MARKS, R. and FOLEY, P. , Incidence of non-melanocytic skin cancer treated in Australia. Brir. med. J . , 296, 13-17 (1988).
GOWN, D., SILVERSTONE, H. and SMITHURST, B.A. , The epidemiology of skin cancer in Australia. In: W.H. McCarthy (ed.), Melanoma and skin cancer, pp. 1-37, Govt. Printer, Sydney (1972). GRAHAM, P.G. and MCGAVRAN, M.H., Basal cell carcinoma and seba- ceous glands. Cancer, 17, 803-806 (1964).
GREEN, A. , BEARDMORE, G., HART, V . , LESLIE, D. , MARKS, R. and STAINES, D. , Skin cancer in Queensland population. J . Amer. Acad. Der- matol., 19, 1045-1052 (1988). HARVEY, I., SHALOM, D . , MARKS, R.M. and FRANKEL, S . J . , Non- mehnoma Skin cancer. Brit. med. J . , 299, 118-120 (1989). MARKS, R. , RENNIE, G. and SELWOOD, T., The relationship of basal cell carcinomas to squamous cell carcinomas to solar keratoses. Arch Derma- rol., 124, 1039-1042 (1988).
Int. J . Epidemiol., 15, 502-506 (1986). SCHLESSELMAN J . J . , Case-control studies: design and analysis, p. 247, Oxford university press, N~~ york (1982). SCOTTO, J . , COTTON, G., URBACH, F., BERGER, D. FEARS, T. , Bio- logically effective ultraviolet radiation: surface measurement in the United States, 1974 to 1985. Science, 239, 762-764 (1988). SCOTTO, J. and FRAUMENI, J . , J R . , Skin (other than melanoma), In: D. Schottenfeld and J. Fraumeni, JR. (ed.), Cancer epidemiology and pre- vention, pp. 996-101 1, WB Saunders, Philadelphia, (1982).
F ~ ~ ~ ~ , T.R. and sCOTTO, J , , changes in cancer morbidity between PEARL, D.K. and SCOTT, E., The anatomical distribution of S k i n cancers.

SKIN CANCER IN AN AUSTRALIAN POPULATION 361
The biologic effects of ultraviolet radiation, pp. 635-650, Pergamon Press, Oxford (1969). URBACH, F., Geographic distribution of skin cancer. J. surg. Oncol., 3 ,
SOBIN, L., WHELAN, S. and MUIR, C., Coding practices. In. J.A.H. Waterhouse, C . Muir. K. Shanmungaratnam and J. Powell (eds.) Cancer incidence in five continents. Vol. IV, IARC Publication 42, Springer, Berlin (1982). 219-234 (1971). sTONE, J.L., R ~ ~ ~ ~ ~ ~ , G , , s ~ ~ ~ ~ ~ , J . , E ~ ~ ~ ~ ~ , D,J, and F ~ ~ ~ ~ , E.R., The incidence of non-melanoma skin cancer in Kauai during 1983. Hawaii
URBACH, F., The biological effects of increased ultraviolet radiation: an update. Photochem. Photobiol., 439-441 (1989).
I
med. J . , 45, 281-286 (1986).
URBACH, F., Geographic pathology of skin cancer. In: F. Urbach (ed.),
ZAYNOUN, S., ABI ALI, L., SHAIB, J . and KURBAN, A., The relationship of sun exposure and solar elastosis to basal cell carcinoma. J. Amer. Acad. Dermafol., 12, 522-525 (1985).