Embed Size (px)
Citation preview

Incarceration, Reentry and Disparities in Health: What are
the connections?
Nicholas FreudenbergHunter College, May 5, 2006
Presented at the Prisoner Reentry Institute’s
Occasional Series on Reentry Research

Overview Do incarceration and reentry policies in US
contribute to disparities in health between socioeconomic and racial/ethnic groups?
What are the pathways by which incarceration and reentry influence health?
What changes in incarceration and reentry policies can improve population health and reduce disparities in health?

Racial/ethnic disparities in health



Disparities in Criminal Justice Involvement
Blacks more likely than whites to be: Arrested Incarcerated Released under continuing
supervision Given longer sentences Reincarcerated

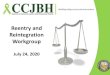
Lifetime Likelihood of Serving a State or Federal Prison Sentence for Males Born in 1974 and 2001, by Race and Ethnicity
2,2%
13,4%
4,0%
5,9%
32,2%
17,2%
0,0%
5,0%
10,0%
15,0%
20,0%
25,0%
30,0%
35,0%
Non-Hispanic White Non-Hispanic Black Hispanic
Life
time
Like
lihoo
d of
Goi
ng to
Pri
son
1974
2001


So what’s the connection between disparities in health and incarceration?
Model 1 Model 2
Poverty, inequality and
racism
Poorhealth
Incarceration
Poverty, inequality and racism
Incarceration
Poor health

So what’s the connection between disparities in health and incarceration?
Model 3
Poverty, inequality and racism
Poorhealth
Incarceration

What are the pathways by which incarceration contributes to disparities?
1. Exposure to unhealthy jail/prison environment
2. Incarceration as stigma3. Revolving door contributes to
community disorganization4. Missed opportunities for intervention5. Diversion of resources from other
social problems

1. Exposure to unhealthy jail/prison environments
Crowding contributes to transmission of infectious diseases
Jails as schools for crime Jails as site of risky behavior Jails as generators of violence Jails as amplifiers of coercive masculinity Jails as source of social stress

Risk Behavior on Entry and During Incarceration, USA
IDU MSM
On Entry 25% - 40% 0% - 7%
During Incarceration
12% 33%

Correctional Facilities Concentrate People with Infectious Diseases
Condition Releasees with condition in 1997 as % of total in US with condition
HIV infection 22.2-31.3%
Hepatitis C 29.4-43.2%
Tuberculosis 39.6%
Source: Hammett et al, 2002.

Incarceration as stigma
Increased isolation post-release Reduced opportunities for employment Reduced opportunities for education Alienation from family and friends Loss of benefits such as Medicaid, public
assistance, public housing

Revolving door between prison and community contributes to community disorganization
Cycle disrupts family life and parenting Contributes to housing, employment and
educational instability, key anchors for communities
Impact most severe on high incarceration communities
“Churning” reduces social cohesion, thus diminishing community capacity to respond to threats to health

Missed opportunities for intervention... a public health disaster
Failure to screen, treat and refer for infectious diseases, psychiatric problems, substance use and chronic conditions respresents lost opportunity for improving health of most vulnerable populations.

Diversion of resources from other problems
New York City and State spend $250 million per year to incarcerate Harlem residents. Could this money be spent to achieve better outcomes?
In NYC, it costs $92,500 to jail one person for one year.
Many states are facing fiscal crises as a result of increasing expenditures for corrections and Medicaid.

What strategies can reduce adverse health impact of incarceration and reentry?
Strategy 1: Reduce number of people going to jail.
Strategy 2: Ensure that every person leaves jail or prison in better health than when he or she entered.
Strategy 3: Reduce stigma of incarceration; end punishment at jail gate.

Strategy 1: Reduce number of people going to jail
Expand and improve alternatives to incarceration.
Divert people with mental illness and substance abuse problems into treatment.
Reduce school dropout rates. Restructure probation and parole to
reduce revocations. Rethink goals of policing.

Strategy 2: Ensure that every person leaves jail or prison in better health than when he or she entered.
Restructure health services in jail to emphasize chronic disease management, health promotion, and resolution of acute problems.
Establish working system for electronic medical records to share information.
Re-establish full range of drug treatment services in jail.
Shift resources into reentry services. Connect people to Medicaid. Fund health centers in high incarceration
communities to serve those returning.

Strategy 3: Reduce stigma of incarceration; end punishment at jail gate.
Bar employment discrimination based on incarceration status absent direct evidence of harm.
Public campaigns to encourage positive support for people returning from incarceration.
Public dialogue on how best to improve public safety, protect community health and use tax payer dollars efficiently