Embed Size (px)
Citation preview

Journal ofAthletic Training 2000;35(3):248-255C) by the National Athletic Trainers' Association, Incwww.journalofathletictraining.org
Functional Anatomy of the ShoulderGlenn C. Terry, MD; Thomas M. Chopp, MDThe Hughston Clinic, Columbus, GA
Objective: Movements of the human shoulder represent theresult of a complex dynamic interplay of structural bony anat-omy and biomechanics, static ligamentous and tendinousrestraints, and dynamic muscle forces. Injury to 1 or more ofthese components through overuse or acute trauma disruptsthis complex interrelationship and places the shoulder at in-creased risk. A thorough understanding of the functional anat-omy of the shoulder provides the clinician with a foundation forcaring for athletes with shoulder injuries.Data Sources: We searched MEDLINE for the years 1980 to
1999, using the key words "shoulder," "anatomy," "glenohu-meral joint," "acromioclavicular joint," "sternoclavicular joint,""scapulothoracic joint," and "rotator cuff."Data Synthesis: We examine human shoulder movement by
breaking it down into its structural static and dynamic compo-
M ovements of the human shoulder represent a complexdynamic relationship of many muscle forces, liga-ment constraints, and bony articulations. Static and
dynamic stabilizers allow the shoulder the greatest range ofmotion of any joint in the body and position the hand andelbow in space. This extensive range of motion affords theathlete- the ability to engage in a myriad of sports activities;however, this range of motion is not without risk. The bonyarchitecture of the glenohumeral joint, with its large articulat-ing humeral head and relatively small glenoid surface, reliesheavily on ligamentous and muscular stabilizers throughout itsmotion arc (as opposed to the hip with its congruent"ball-in-socket" anatomy). If any of the static or dynamicstabilizers are injured by trauma or overuse, the shoulder isat increased risk for injury. Shoulder injuries account for 8%to 20% of athletic injuries." 2We examine the shoulder girdle from the standpoint of its
component structures, namely the (1) bony anatomy (humerus,clavicle, scapula), (2) bony and muscular articulations (glenohu-meral, acromioclavicular, sternoclavicular, and scapulothoracic),(3) static stabilizers (labrum, capsule, ligaments), and (4) musclesor dynamic stabilizers (rotator cuff, deltoid, and scapular stabiliz-ers). Although these components will be discussed separately,they function to produce shoulder movement as a dynamic,interrelated unit. Understanding the functional anatomy and asso-ciated frequent sources of injury of the shoulder permits the sportsmedicine professional a more structured approach to the care ofathletic shoulder injuries. The following material provides anoverview of the functional components. The reader is encouragedto research fur-ther specific topics of interest.
nents. Bony anatomy, including the humerus, scapula, andclavicle, is described, along with the associated articulations,providing the clinician with the structural foundation for under-standing how the static ligamentous and dynamic muscleforces exert their effects. Commonly encountered athletic inju-ries are discussed from an anatomical standpoint.Conclusions/Recommendations: Shoulder injuries repre-
sent a significant proportion of athletic injuries seen by themedical provider. A functional understanding of the dynamicinterplay of biomechanical forces around the shoulder girdle isnecessary and allows for a more structured approach to thetreatment of an athlete with a shoulder injury.Key Words: anatomy, static, dynamic, stability, articulation
BONY ANATOMY
HumerusThe humerus is the largest and longest bone of the upper
extremity, with its proximal portion consisting of the half-spheroid articulating surface or head, greater tuberosity, bicip-ital groove, lesser tuberosity, and proximal humeral shaft(Figure 1). The head is inclined relative to the shaft at theanatomical neck at an angle of 1300 to 150° and is retroverted26° to 310 from the medial and lateral epicondylar plane(Figure 2).3 The greater tuberosity has 3 facets into which thetendons of the supraspinatus, infraspinatus, and teres minorinsert. The lesser tuberosity is the site of insertion of thesubscapularis, completing the rotator cuff. The facets providefor a continual ring insertion of the rotator cuff from posterior-inferior to anterior-inferior on the neck of the humerus. Thisinsertion is interrupted only by the bicipital groove, throughwhich the long head of the biceps brachii passes laterally anddistally from its origin on the superior lip of the glenoid.Substantial forces applied to the shoulder (such as those seen in
contact sports) often result in glenohumeral dislocation, with or
without associated fracture of the proximal humerus. Whenfractures do occur, they commonly involve 1 or more of thetuberosities, which are then displaced in line with the forcegenerated by the portion of the rotator cuff attached to thattuberosity. For example, a fracture of the greater tuberosity willbe pulled superiorly and posteriorly secondary to the combinedpulls of the supraspinatus, infraspinatus, and teres minor. Thefinal fracture position is also influenced by the superior forceon the humeral shaft by the deltoid and the medial force of thepectoralis major muscle.4The surgical neck of the humerus is located just distal to the
tuberosities at the level of the metaphyseal flare and is acommon site of fractures in the elderly.5 The incidence of
248 Volume 35 * Number 3 * September 2000
Address correspondence to Glenn C. Terry, MD, The Hughston Clinic,6262 Veterans Parkway, Columbus, GA 31909. E-mail address:[email protected]

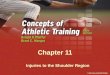
Clavicle
Humerus
Figure 1. The 3 bones of the shoulder are the humerus, the clavicle,and the scapula.
Figure 2. The humeral head:shaft angle is 1300 to 1500; the head isretroverted 260 to 310.
proximal humerus fractures increases with age over 40 yearsand is felt to be due to osteoporosis.6 The surgical neck has alsobeen implicated as a possible factor in glenohumeral disloca-tion through abutment on the acromion in extreme positions,such as hyperabduction.7 In this case, the humeral head islevered inferiorly out of the glenoid fossa.8
ScapulaThe scapula is a large, thin, triangular bone lying on the
posterolateral aspect of the thorax, overlying ribs 2 through 7,that serves mainly as a site of muscle attachment. As a result ofthe protection of the overlying soft tissues, fractures occurthrough indirect trama to the processes (coracoid, spine,acromion, and glenoid).9 The superior process, or spine,separates the supraspinatus muscle from the infraspinatus andextends superiorly and laterally to form the base of theacromion. The spine functions as part of the insertion of thetrapezius muscle, as well as the origin of the posterior deltoidmuscle. The acromion serves as a lever arm for function of thedeltoid and articulates with the distal end of the clavicle,forming the acromioclavicular joint. The acromion forms aportion of the roof of the space for the rotator cuff, andvariations in acromial shape can affect contact and wear on thecuff (impingement).10 Tendinitis and bursitis are the result ofimpingement of the humeral head and overlying rotator cuffagainst the coracoacromial arch, which is composed of theacromion, coracoacromial ligament, and coracoid process.Impingement is often seen in overhead athletes who performrepetitive motions.
The coracoid process projects anteriorly and laterally fromthe upper border of the head of the scapula. The superiorsurface serves as the origin of the 2 coracoclavicular ligamentsthat are torn, along with the acromioclavicular ligament, inacromioclavicular (AC) joint separations. The most commoncause of injury is a fall onto the point of the shoulder, as infootball. The coracoid tip serves as the origin of the coraco-brachialis muscle and the short head of the biceps brachii, aswell as the insertion of the pectoralis minor muscle. Thecoracohumeral and coracoacromial ligaments originate on thecoracoid as well. The scapular notch lies just medial to the baseof the coracoid and is spanned by the transverse scapularligament. The suprascapular nerve passes beneath the ligamentto innervate the supraspinatus and infraspinatus muscles.1'12The glenoid fossa, or cavity, represents the bony articulating
surface for the humerus. Its articular surface is only one thirdto one fourth that of the humeral head (Figure 3), and hence,provides only a small contribution to glenohumeral stability.The glenoid surface is retroverted on average 40 to 120 withrespect to the scapular plane.'3 The scapular plane lies 300 to450 anterior with respect to the coronal plane of the body and,thus, articulates with the retroverted humeral head.'4 Thisorientation of the scapula to the coronal plane of the body andhumeral head provides the bony foundation for the extensivenormal range of shoulder motion.
ClavicleThe clavicle serves as the sole bony strut connecting the
trunk to the shoulder girdle via the sternoclavicular jointmedially and the acromioclavicular joint laterally. The claviclehas a double curve along its long axis and is subcutaneous inits full extent. The flat outer third serves as an attachment pointfor muscles and ligaments, whereas the tubular medial thirdaccepts axial loading. The middle-third transitional zone is thethinnest portion and is a weak area mechanically, which maybe 1 reason for the predominance of fractures in this area.'5The clavicle serves as a site for muscle attachments, a barrierto protect underlying neurovascular structures, and a strut tostabilize the shoulder complex and prevent it from displacingmedially with activation of the pectoralis and other axiohum-
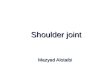
Articularcartilageof humeralhead
Articularcarblage ofglenoid surfaceof scapula
Subscapularis
InfraspinatusFigure 3. Note the large humeral head and the small glenoidarticular surface. The glenoid arUcular cartilage is thicker at theperiphery, and the humeral head is thicker at the center.
Journal of Athletic Training 249

eral muscles.'6 Additionally, the clavicle prevents inferiormigration of the shoulder girdle through the strong coracocla-vicular ligaments. In high-grade AC joint separations, whenthis stability is lost, the shoulder girdle displaces inferiorlyaway from the clavicle.8 As a result, on physical examination,the distal clavicle appears to displace superiorly.
JOINT ARTICULATIONS
Glenohumeral Joint
The glenohumeral joint is suited for extreme mobility withits mismatched large humeral head and small glenoid articularsurface. At any given time, only 25% to 30% of the humeralhead is in contact with the glenoid fossa.17 However, despitethis lack of articulating surface coverage, the normal shoulderprecisely constrains the humeral head to within 1 to 2 mm ofthe center of the glenoid cavity throughout most of the arc ofmotion.'8-20 This precise constraint of the center of rotationthrough a large arc of motion is the result of an interplay ofstatic (no active energy required, ie, capsule, labrum, liga-ments) and dynamic (muscle) forces. The stabilizing effect ofthe articular surfaces and capsulolabral ligamentous complex ismagnified by muscle forces, which produces a concavity-compression effect directed toward the glenoid center.2' Bio-mechanical dysfunction from injury to the bony anatomy, staticcapsulolabral ligamentous structures, or dynamic muscle sta-bilizers through a single traumatic event or a series of repetitivemicrotrauma results in loss of this precise constraint of thecenter of rotation, or instability. Depending on the injuredstructures involved, the direction of instability may be primar-ily anterior, inferior, or posterior, or a combination of these.The degree of instability may range from mild subluxation todislocation, with associated injury to the bony or capsulolabralstructures, or both, and surrounding musculature. Treatment ofinstability in the athlete is aimed at surgically restoring thestructural integrity of the injured capsulolabral ligamentouscomplex, followed by rehabilitation of the dynamic stabilizers.Restoration of normal glenohumeral biomechanics throughreestablishment of the dynamic interplay of bony, static, anddynamic stabilizers is the final goal. If any of the componentscontributing to stability are not fully repaired or rehabilitated,the athlete will fail to return to the preinjury level of perfor-mance.
Passive Mechanisms
Articular Surface. The bony radius of the curvature of theglenoid is slightly flattened with respect to the humeral head.However, the glenoid articular cartilage is thicker at theperiphery, thus creating significant articular surface conformityand resultant stability.22 This resultant articular conformityadditionally provides the foundation for the concavity-compression effect provided by the rotator cuff and surround-ing musculature. The normal glenohumeral joint is fully sealedby the capsule and normally contains less than 1 mL of jointfluid under slightly negative intra-articular pressure, whichprovides a suction effect to resist humeral head translation,thereby increasing stability. In addition, adhesion and cohesionforces are created when fluid separates 2 closely opposingsurfaces and, thus, the surfaces cannot be pulled apart easily(an example is 2 wet microscopic slides placed together).23 The
contribution of these factors in stability are probably minor andfunctional only at low loads.24
Glenoid Labrum. The glenoid labrum is a dense, fibrousstructure, which is triangular on cross-section.25 Located at theglenoid margin, the labrum serves to extend the conformingarticular surfaces, thereby increasing contact surface area andadding to stability. The labrum also enhances stability bydeepening the concavity of the glenoid socket, an average of9 mm and 5 mm in the superoinferior and anteroposteriorplanes, respectively,26 and loss of the integrity of the labrum(through injury) decreases resistance to translation by 20%.21The labrum also acts as an anchor point for the capsuloliga-mentous structures.27 Bankart28 deemed the detachment of thelabrum from the anterior-inferior glenoid rim the "essentiallesion" responsible for the high incidence of recurrent anteriordislocations. In this case, the labrum detaches traumaticallyalong with the anchoring point of the inferior and middleglenohumeral ligaments. Also disrupted is the deepening effectof the labrum. Treatment is aimed at surgically restoring thefunctional integrity of the labrum and capsuloligamentousanchor. Pagnani et al29'30 demonstrated the importance ofsuperior labrum and biceps tendon injuries, noting increasedanteroposterior and superoinferior translations in the lower andmiddle ranges of elevation.
Joint Capsule. The surface area of the capsule is approxi-mately twice that of the humeral head, allowing for extensiverange of motion. The capsule is truncated in shape, and theinferior portion, or axillary pouch, is redundant. The capsuletightens or "winds up" in various extremes of position; forexample, the inferior pouch tightens in extreme abduction andexternal rotation, serving to stabilize the joint (Figure 4).31Although the capsule and glenohumeral ligaments are oftendescribed separately, they are intimately adherent anatomi-cally. The capsuloligamentous structures reciprocally tightenand loosen during rotation of the arm to limit translation. In themidrange of motion, these structures are relatively lax, andstability is mainly provided by the actions of the rotator cuffand biceps through the concavity-compression effect.21 At theextremes of motion, the ligaments tighten and become func-tional; they are especially important in providing stabilizationwhen all other stabilizing mechanisms are overwhelmed.8
Ligaments. The coracohumeral ligament is a thick band ofcapsular tissue originating from the base of the lateral coracoidand inserting into the lesser and greater tuberosities. Thisligament is taut with the arm in the adducted position andconstrains the humeral head on the glenoid.32 Additionally, thecoracohumeral ligament and superior glenohumeral ligamentstabilize the humeral head from inferior translation in adduc-tion and from posterior translation in forward flexion, adduc-tion, and internal rotation.33The superior glenohumeral ligament extends from the an-
terosuperior edge of the glenoid to the top of the lessertuberosity (Figure 5). It parallels the course of the coracohu-meral ligament, and these 2 structures are considered similar infunction. Together they constitute the rotator interval regionbetween the anterior border of the supraspinatus and thesuperior border of the subscapularis.34'35The middle glenohumeral ligament is the most variable of
the 3 glenohumeral ligaments, being absent in 8% to 30% ofpatients. It originates from the supraglenoid tubercle, superiorlabrum, or scapular neck and inserts on the medial aspect of thelesser tuberosity. Its function is to limit anterior translation of
250 Volume 35 * Number 3 * September 2000

A
B
Figure 4. A, Ugaments of the shoulder joint. B, The capsuletightens in extreme abduction and extemal rotation, taking up theredundant capsule.
Coracodavicular ligament
Biceps tendon
.genohumeral ligamentMiddleglenohumeral ligament
Posterior inferiorglenohumeral ( , Anterior inferiorligament glenohumeral ligament
Inferiorpouch
Figure 5. Cross-sectional view of the glenohumeral joint (with thehumeral head removed showing the glenohumeral ligaments andassociated structures.
the humeral head in the lower ranges of abduction (600 to 90°)and inferior translation in the adducted position at the side.36The inferior glenohumeral ligament is the thickest and most
consistent of the 3 glenohumeral ligaments. It is often de-scribed as a complex containing an anterior band, axillarypouch, and posterior band. The anterior band extends from theanteroinferior labrum and glenoid lip to the lesser tuberosity of
the humerus and is the thickest portion and the primarystabilizer against anterior translation of the humeral head in thethrowing position of abduction and external rotation.31'36 Inthis position, the complex moves anteriorly and becomes abarrier to anterior translation. Injury to the inferior glenohu-meral ligament through repetitive microtrauma (as in pitching)or a single traumatic episode (dislocation) plays an integral rolein recurrent instability. As noted above, treatment is aimed atsurgically restoring the functional integrity of the inferiorglenohumeral ligamentous complex.
Dynamic StabilizersRotator Cuff Muscles. The rotator cuff is a group of
muscles consisting of the subscapularis, supraspinatus, in-fraspinatus, and teres minor, which act as a dynamic steeringmechanism for the humeral head (Figure 6). Three-dimensional movements or rotations of the humeral head arethe result of the dynamic interplay between the musclescomprising the rotator cuff and the static stabilizers. Rotatorcuff activation results in humeral head rotation and depressionin positions of abduction. As a group, the rotator cuff musclesare smaller in cross-sectional area and size when comparedwith the larger, more superficial muscles such as the deltoid,pectoralis major, latissimus dorsi, and trapezius. Also, becausethey lie much closer to the center of rotation on which they act,their lever arm is shorter, and a smaller generated force results.Given this anatomical location, the rotator cuff is very wellsituated to provide stability to a dynamic fulcrum duringglenohumeral abduction (Figure 7A).
Contraction of the rotator cuff results in concavity-compression, and asymmetric contraction acts to cause hu-meral head rotation or "steering" during shoulder motion.Additionally, force couples occur at the glenohumeral joint inmultiple planes (Figures 7B, 7C). Force couples occur whenthe resultant force of 2 opposing muscle groups achieves agiven moment. Inman et a137 described the cephalad force ofthe deltoid counteracted by the inferior, or depressing, force ofthe subscapularis, infraspinatus, and teres minor.The supraspinatus originates from the supraspinous fossa to
insert forward and laterally at the superior aspect of the greatertuberosity. The tendon blends into the joint capsule andinfraspinatus tendon below. The supraspinatus stabilizes the
p0sTER
0R
ANTERI0R
Infraspinatus
Teres major
Figure 6. Sites of origin for the rotator cuff muscles.
Journal of Athletic Training 251

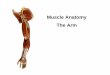
A
f1
B
C
Figure 7. A, The muscles about the shoulder can be thought of asprimary movers and primary stabilizers. This situation is somewhatanalogous to that of a large man and small boy teaming up to raisea long, heavy ladder. Typically the stronger one will lift (move) theladder while the weaker one will hold it from sliding or lIffing off theground (stabilize it). There comes a point at which the forcegenerated by the stronger one can overpower the resistance of theweaker one and stability is lost. (Reprinted with permission fromO'Driscoll SW. Atraumatic instability pathology and pathogenesis.In: Matsen FA, Fu FH, Hawkins RJ, eds. The Shoulder. A Balance ofMobility and Stability. Rosemont, IL: American Academy of Ortho-paedic Surgeons; 1993:307.) B, Force couple in the adductedposition. C, Force couple in the abducted position.
glenohumeral joint and serves, along with the deltoid, toelevate the arm. Innervation is from the suprascapular nerve.The infraspinatus originates from the infraspinous fossa and
extends laterally to its tendinous insertion on the middle facetof the greater tuberosity. The infraspinatus, along with the teres
minor, provides the primary external rotation force and alsostabilizes the glenohumeral joint against posterior subluxation.Innervation is from the suprascapular nerve.The teres minor originates from the mid to upper regions of
the axillary border of the scapula and extends laterally andsuperiorly to its insertion on the most inferior facet of thegreater tuberosity. In concert with the infraspinatus, the teresminor is an external rotator and glenohumeral stabilizer.Innervation is from the axillary nerve.The subscapularis muscle comprises the anterior portion of
the rotator cuff. It originates from the subscapular fossa toextend laterally to its insertion on the lesser tuberosity of thehumerus. The tendon of the subscapularis is intimately asso-ciated with the anterior capsule. The axillary nerve passesalong the inferior border of the scapula and is, therefore,subject to trauma from anterior dislocation. The subscapularisfunctions as an internal rotator, especially in maximum internalrotation. Innervation is from the upper and lower subscapularnerves.The long head of the biceps must also be considered here,
because it functions intimately with the rotator cuff as ahumeral head depressor. Rodosky et a138 have noted thatcontraction of the long head of the biceps during the latecocking phase of throwing can significantly reduce anteriortranslation and increase torsional rigidity of the joint resistingexternal rotation. Pagnani et a129 also noted that in lowerelevated positions, the long head of the biceps stabilized thejoint anteriorly when the arm was internally rotated andstabilized the joint posteriorly when the arm was externallyrotated. Injuries to the long head of the biceps and superiorlabrum may result from an excessively strenuous throwingprogram and produce loss of stability, decreased performance,and increasing symptoms.
Acromioclavicular Joint
The acromioclavicular joint is a diarthrodial joint betweenthe lateral border of the clavicle and the medial edge of theacromion. The average joint size in the adult is 9 X 19 mm, andthe joint is covered by a capsule. Because of the high axialloads transferred through this small surface area, contactstresses on the articular surface are high and may result in earlyfailure, such as osteolysis in weight lifters or osteoarthritis.Stability of the acromioclavicular joint is provided mainlythrough the static stabilizers composed of the capsule, intra-articular disc, and ligaments.39The capsule, which is thicker superiorly and anteriorly,
surrounds the joint. It is reinforced by the acromioclavicularligaments superiorly, inferiorly, posteriorly, and anteriorly.The fibers of the superior acromioclavicular ligament are thestrongest and blend with the fibers of the deltoid and trapeziusmuscles. The intra-articular fibrocartilaginous disc occurs in 2forms: partial and complete. The disc varies substantially insize and shape. It undergoes rapid degeneration (perhaps as aresult of the high contact stress loads) and is functionallyabsent by the fourth decade.39
Additional stability of the acromioclavicular joint is derivedthrough the coracoclavicular ligaments, which serve as the pri-mary suspensory ligaments of the upper extremity. Two distinctligaments, the trapezoid and conoid, span the distance from thesuperior surface of the coracoid to insert on the trapezoid ridgeand conoid tuberosity of the clavicle, respectively. These stoutligaments suspend the shoulder girdle from the clavicle at an
252 Volume 35 * Number 3 * September 2000

average distance of 13 mm. The acromioclavicular ligaments arethe primary restraint to AC joint posterior translation, while thecoracoclavicular ligaments are the primary restraint to verticaldisplacement. The common AC separation injury representsgradations of injury level, first to the acromioclavicular joint andthen to the coracoclavicular ligaments, and is usually the result ofan inferiorly directed force to the superior aspect of the shoulder(such as a fall onto the point of the shoulder).8
Sternoclavicular JointThe sternoclavicular joint represents the only true articula-
tion between the upper extremity and the axial skeleton (Figure8). It is a sellar (saddle) joint formed by the articulation of themedial end of the clavicle and the upper portion of the sternum.Given the great disparity in size between the large bulbous endof the clavicle and the smaller articular surface of the sternum,stability is provided by the surrounding ligamentous structures.The intra-articular disc-ligament is a dense, fibrous structure
arising from the junction of the first rib, passing through thesternoclavicular joint, and attaching to the superior and medialclavicle. This disc-ligament acts as a checkrein against medialdisplacement of the inner clavicle.The costoclavicular ligament arises from the upper surface of
the first rib to attach to the inferior surface of the medial clavicle.Bearnmo has shown experimentally that the anterior fibers resistexcessive upward rotation and the posterior fibers resist excessivedownward rotation. The interclavicular ligament connects thesuperomedial aspect of the clavicle with the capsular ligamentsand upper sternum. This ligament acts as a checkrein againstexcessive downward rotation of the clavicle. The capsular liga-ment covers the anterosuperior and posterior aspects of thesternoclavicular joint. The anterior portion is heavier and strongerthan the posterior portion and is the primary stabilizer againstupward displacement of the inner clavicle caused by a downwardforce on the distal end of the shoulder.40 Under normal circum-stances, the sternoclavicular joint is capable of 30° to 350 ofupward elevation, 350 of combined forward and backward move-ment, and 450 to 500 of rotation around its long axis.4'
A CJavide
First rib
B
Scapulothoracic ArticulationNot a true joint, the scapulothoracic articulation represents a
space between the convex surface of the posterior thoracic cageand the concave surface of the anterior scapula. It is occupiedby neurovascular, muscular, and bursal structures that allow arelatively smooth motion of the scapula on the underlyingthorax. With the scapula serving as the bony foundation of theshoulder girdle, the scapulothoracic articulation allows in-creased shoulder movement beyond the 1200 offered solely bythe glenohumeral joint. On average, there are approximately 20of glenohumeral elevation for every 10 of scapulothoracicelevation, although the actual ratio can vary for any portion ofthe arc of motion.42
Seventeen muscles attach to or originate from the scapulaand function to stabilize the scapula and provide motion.Among these, the most important are the serratus anterior,which maintains the medial angle against the chest wall, andthe trapezius, which helps to rotate and elevate the scapulasynchronously with glenohumeral motion (Figure 9). Rehabil-itation of the overhead or throwing athlete must include thescapular-stabilizing musculature for optimal results.
Three bursae surround the scapula: 1 at the superomedialangle between the serratus anterior and the subscapularis,another between the serratus anterior and the lateral chest wall,
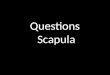
A
Levatorscapulae
Rhomboidminor
Rhomboidmajor
Outline ofinferior sectionof trapezius
B
Articular
Figure 8. A, Anterior, and B, cross-sectional views of the stemo- Figure 9. A, The scapulothoracic muscles, including B, the serratusclavicular joint, anterior.
Journal of Athletic Training 253

and the third at the inferior angle. All 3 have been associatedwith scapulothoracic bursitis and "snapping" scapula.43
Scapulothoracic Muscles
The trapezius has an extensive origin from the base of the skuhllto the upper lumbar vertebrae and inserts on the lateral aspect ofthe clavicle, acromion, and scapular spine. It functions mainly as
a scapular retractor and elevator of the lateral angle of the scapula.It is innervated by the spinal accessory nerve.
The rhomboids, consisting of the major and minor muscles,originate from the spinous processes of C7 and Ti and T2 toT5, respectively. They insert on the medial aspect of thescapula and retract and elevate the scapula. The dorsal scapularnerve innervates the rhomboids.The levator scapulae originates on the transverse processes
of the cervical spine and inserts on the superior angle of thescapula. The levator scapule elevates the superior angle,resulting in upward and medial rotation of the scapular body.Innervation is from the third and fourth cervical spinal nerves.
The serratus anterior takes origin from the bodies of the first9 ribs and the anterolateral aspect of the thorax and insertsthrough 3 portions from the superior to the inferior angle of thescapula. Activation of the serratus anterior causes scapularprotraction and upward rotation. Innervation is by the longthoracic nerve, and nerve injuries here often manifest as a
winged scapula.43The pectoralis minor originates from the anterior portion of
the second through fifth ribs and inserts on the base of thecoracoid. It protracts and rotates the scapula inferiorly. Inner-vation is from the medial pectoral nerve.
The deltoid muscle consists of 3 portions: an anterior portionoriginating from the lateral clavicle, a middle portion originat-ing from the acromion, and a posterior portion originating fromthe spinious process of the scapula. All 3 portions convergedistally to insert on the deltoid tuberosity of the humerus. Theanterior and middle portions allow for elevation in the scapularplane and assist in forward elevation with help from thepectoralis major and biceps. Innervation is by the axillarynerve.43 As noted above, the deltoid acts in the force couplesoccurring at the glenohumeral joint.
Other Shoulder Muscles
The latissimus dorsi is a large triangular muscle arising fromthe spines of the lower 6 thoracic vertebrae and thoracolumbarfascia, through which it is attached to the lumbar and sacralvertebrae and to the supraspinous ligaments and posterior iliaccrest. It converges from its wide origin to pass laterally around thelower border of the teres major, attaching to the intertuberculargroove of the humerus. It functions to adduct, extend, andinternally rotate the humerus. Innervation is by the thoracodorsalnerve from the posterior cord of the brachial plexus.The teres major originates at the inferior angle of the scapula
and rotates 180° toward its insertion into the medial lip of theintertubercular groove of the humerus. Its tendinous insertionblends with the insertion of the latissimus dorsi. It is primarilyan internal rotator and adductor of the shoulder and extender ofthe arm. Innervation is from the lower subscapular nerve.
The coracobrachialis originates from the coracoid processand inserts on the anteromedial aspect of the humerus. Alongwith the short head of the biceps, the coracobrachialis flexes
Pectoralisrmajor
B
DeltoidPectoralismajor(cut)
Pectoralismajor
Biceps
Figure 10. Other muscles of the shoulder. A, Note the pectoralismajor and the deltoid, and B, the pectoralis minor and the 2 headsof the biceps.
and adducts the glenohumeral joint. Innervation is from themusculocutaneous nerve.The pectoralis major originates medially from the medial
aspect of the clavicle, the sternum, and the fifth and sixth ribs(Figure 10). The muscle extends laterally to insert on the laterallip of the bicipital groove. The muscle primarily functions inadduction and internal rotation of the humerus. Innervation isby the lateral and medial pectoral nerves.
The biceps has 2 heads. The long head originates from thesupraglenoid tuberosity and superior labrum; the short headoriginates from the coracoid, along with the coracobrachialisand pectoralis minor. The biceps then extends distally to insertin the bicipital tuberosity of the radius. The long head of thebiceps is located in the rotator interval between the supraspi-natus and subscapularis tendons and serves as a primary headdepressor during abduction. Innervation is from the musculo-cutaneous nerve.
SUMMARYShoulder motion is the result of the complex interplay of static
and dynamic stabilizers. All 4 joints of the shoulder (glenohumer-al, acromioclavicular, stemoclavicular, and scapulothoracic) musthave free movement as a prerequisite. The bony anatomy provides
254 Volume 35 * Number 3 * September 2000
A

the structural foundation from which the forces are generated andsubsequently acted on. With regard to the glenohumeral joint, thecapsuloligamentous complex provides static restraint, while therotator cuff muscles (along with their respective force-coupleantagonists) guide, steer, and maintain the head dynamically in theglenoid fossa. Glenohumeral injury and instability can result when1 or more of the bony, static, or dynamic components of thisinteraction are disrupted. Additionally, when injury involvesstructures other than the glenohumeral joint specifically, theeffects may be noted secondarily through decreased shoulderperformance. Only when all the components contributing toshoulder motion are retumed to their fully functional state can theathlete perform to the highest expectations. A thorough knowl-edge of the functional anatomy of the shoulder allows the medicalprovider to take a sound approach in the evaluation and manage-ment of the athlete's shoulder.
REFERENCES1. Powell JW, Barber-Foss KD. Injury patterns in selected high school sports: a
review of the 1995-1997 seasons. J Athl Traim 1999;34:277-284.2. Steinbruck K. Epidemiology of sports injuries: 25-year analysis of sports
orthopedic-traumatologic ambulatory care. Sportverletz Sportschaden.1999;13:38-52.
3. Kronberg M, Brostrom LA, Soderlund V. Retroversion of the humeralhead in the normal shoulder and its relationship to the normal range ofmotion. Clin Orthop. 1990;253:113-117.
4. Bigliani LU, Craig EV, Butters KP. Fractures of the shoulder, part I:fractures of the proximal humerus. In: Rockwood CA Jr, Green DP,Bucholz RW, eds. Rockwood and Green's Fractures in Adults. Vol 1. 3rded. Philadelphia, PA: JB Lippincott; 1991:871-927.
5. Hall MC, Rosser M. The structure of the upper end of the humerus withreference to osteoporotic changes in senescence leading to fractures. CanMed Assoc J. 1963;8:290-294.
6. Rose SH, Melton LJ, Monfey BF, Ilstrup DM, Riggs LB. Epidemiologicfeatures.of humeral fractures. Clin Orthop. 1982;168:24-30.
7. Codman EA. The Shoulder, Rupture of the Supraspinatus Tendon andOther Lesions in or about the Subacromial Bursa. Boston, MA: ThomasTodd; 1934:313-331.
8. Rockwood CA Jr, Williams GR, Young DC. Injuries to the acromio-clavicular joint. In: Rockwood CA Jr, Green DP, Bucholz RW, eds.Rockwood and Green's Fractures in Adults. Vol 1. 3rd ed. Philadelphia,PA: JB Lippincott; 1991:1181-1252.
9. Jobe CM. Gross anatomy of the shoulder. In: Rockwood CA Jr, Matsen FAII, eds. The Shoulder. Vol 1. Philadelphia, PA: WB Saunders; 1998:34-97.
10. Bigliani LU, Morrison DS, April EW. The morphology of the acromionand rotator cuff impingement. Orthop Trans. 1987;1 1:234.
11. Wamer JJP, Krushell RJ, Masquelet A, Gerber C. Anatomy and relation-ships of the suprascapular nerve: anatomical constraints to mobilization ofthe supraspinatus and infraspinatus muscles in the management of massiverotator-cuff tears. J Bone Joint Surg Am. 1992;74:36-45.
12. Ticker JB, Djurasovic M, Strauch RJ. Incidence of ganglion cysts andother variations in anatomy along the course of the suprascapular nerve. JShoulder Elbow Surg. 1998;7:472-478.
13. Randelli M, Gambroli PL. Glenohumeral osteometry by computed tomogra-phy in normal and unstable shoulders. Clin Orthop. 1986;208:151-156.
14. Morrey BF, Itoi E, Kai-Nan A. Biomechanics of the shoulder. In:Rockwood CA Jr, Matsen FA HI, eds. The Shoulder. Vol 1. Philadelphia,PA: WB Saunders; 1998:233-263.
15. Ljunggren AE. Clavicular function. Acta Orthop Scand 1979;50:261-268.16. Craig EV. Fracures of the clavicle. In: Rockwood CA Jr, Matsen FA m, eds.
The Shoulder. Vol 1. Philadelphia, PA: WB Saunders; 1998:428-482.17. Hertz H. Die bedeutung des limbus glenoidalis fur die stabilitat des
schultergelenks. Wein Klin Wochenschr Suppl. 1984;152:1-23.18. Poppen NK, Walker PS. Normal and abnormal motion of the shoulder.
J Bone Joint Surg Am. 1976;58:195-201.19. Howell SM, Galinat BJ, Renzi AJ, Marone PJ. Normal and abnormal
mechanics of the glenohumeral joint in the horizontal plane. J Bone JointSurg Am. 1988;70:227-232.
20. McMahon P, Debski R, Thompson W, Warner J, Fu F, Woo S. Shouldermuscle forces and tendon excursions during glenohumeral abduction in thescapular plane. J Shoulder Elbow Surg. 1995;4:199-208.
21. Lippitt SB, Vanderhooft JE, Harris SL, Sidles JA, Harryman DT II,Matsen FA HI. Glenohumeral stability from concavity-compression: aquantitative analysis. J Shoulder Elbow Surg. 1993;2:27-35.
22. Soslowsky LJ, Flatow EL, Bigliani LU, Mow VC. Articular geometry ofthe glenohumeral joint. Clin Orthop. 1992;285:181-190.
23. Gibb TD, Sidles JA, Harryman DTI McQuade KJ, Matsen FA mI. The effectof capsular venting on glenohumeral laxity. Clin Orthop. 1991;268:120-127.
24. Cole BJ, Warner JJP. Anatomy, biomechanics, and pathophysiology ofglenohumeral instability. In: lannotti JP, Williams GR Jr, eds. Disordersofthe Shoulder: Diagnosis and Management. Philadelphia, PA; LippincottWilliams & Wilkins; 1999:207-232.
25. Cooper DE, Arnoczky SP, O'Brien SJ, Warren RF, DiCarlo E, Allen AA.Anatomy, histology, and vascularity of the glenoid labrum: an anatomicalstudy. J Bone Joint Surg Am. 1992;74:46-52.
26. Howell SM, Galinat BJ. The glenoid-labral socket: a constrained articularsurface. Clin Orthop. 1989;243:122-125.
27. Moseley H. Overgaard B. The anterior capsular mechanism in recurrentanterior dislocation of the shoulder: morphological and clinical studieswith special reference to the glenoid labrum and the glenohumeralligaments. J Bone Joint Surg Br. 1962;44:913-927.
28. Bankart ASB. The pathology and tratment of recurrent dislocation of theshoulder joint. Br Med J. 1923;2:1132-1133.
29. Pagnani M, Deng XH, Warren R, Torzilli P, O'Brien S. Role of the longhead of the biceps brachii in glenohumeral stability: a biomechanical studyin cadavera. J Shoulder Elbow Surg. 1996;4:255-262.
30. Pagnani M, Deng XD, Warren R, Torzilli P, Altchek D. Effect of lesionsof the superior portion of the glenoid labrum on glenohumeral translation.J Bone Joint Surg Am. 1995;77:1003-1010.
31. O'Brien SJ, Neves MC, Arnoczky SP, et al. The anatomy and histology ofthe inferior glenohumeral ligament complex of the shoulder. Am J SportsMed. 1990;18:449-456.
32. Warner JJP, Deng XH, Warren RF, Torzilli PA. Static capsuloligamentousrestraints to superior-inferior translation of the glenohumeral joint. Am JSports Med. 1992;20:675-685.
33. Cole BJ, Warner JJP. Anatomy, biomechanics, and pathophysiology ofglenohumeral instability. In: Iannotti JP, Williams GR Jr, eds. Disordersofthe Shoulder: Diagnosis andManagement. Philadelphia, PA: LippincottWilliams & Wilkins; 1999:207-232.
34. Basmajian JV, Bazant FJ. Factors preventing downward dislocation of theadducted shoulder joint. J Bone Joint Surg Am. 1959;41:1182-1186.
35. Boardman ND HI, Debski RE, Warner JJP, et al. Tensile properties of thesuperior glenohumeral ligament and coracohumeral ligaments. J ShoulderElbow Surg. 1996;5:249-254.
36. Turkel SJ, Panio MW, Marshall JL, Girgis FG. Stabilizing mechanismspreventing anterior dislocation of the glenohumeral joint. J Bone JointSurg Am. 1981;63:1208-1217.
37. Inman VT, Saunders JB, Abbott LC. Observations on the function of theshoulder joint. J Bone Joint Surg. 1944;26:1-30.
38. Rodosky MW, Harner CD, Fu FH. The role of the long head of the bicepsmuscle and superior glenoid labrum in anterior stability of the shoulder.Am J Sports Med. 1994;22:121-130.
39. McCluskey GM III, Todd J. Acromioclavicular joint injuries. J SouthOrthop Assoc. 1995;4:206-213.
40. Bearn JG. Direct observations on the function of the capsule of thesternoclavicular joint in clavicular support. J Anat. 1967;101:159-170.
41. Rockwood CA Jr. Injuries to the stermoclavicular joint. In: Rockwood CAJr, Green DP, Bucholz RW, eds. Rockwood and Green's Fractures inAdults. Vol 1. 3rd ed. Philadelphia, PA: JB Lippincott; 1991:1253-1308.
42. Sidles JA, Harryman DT, Matsen FA III. Glenohumeral and scapulotho-racic contributions to shoulder motion. Orthop Trans. 1991;15:762.
43. Flatow EL. Shoulder anatomy and biomechanics. In: Post M, Flatow EL,Bigliani LU, Pollock RG. The Shoulder: Operative Technique. Baltimore,MD: Williams & Wilkins; 1998:1-42.
Journal of Athletic Training 255