Embed Size (px)
Citation preview

The Knee 16 (2009) 116–120
Contents lists available at ScienceDirect
The Knee
In vivo kinematic determination of total knee arthroplasty from squatting to standing
Fei Liu a,⁎, Toshihiro Ohdera b, Hirohide Miyamoto c, Ray C. Wasielewski d,Richard D. Komistek e, Mohamed R. Mahfouz e
a Midlands Orthopaedics, Columbia, SC, USAb Aichi Medical University, Nagakute, Aichi, Japanc Fukuoka Orthopaedic Hospital, Fukuoka, Japand Grant Medical Center, Columbus, OH, USAe Mechanical, Aerospace and Biomedical Department, The University of Tennessee, Knoxville, TN, USA
⁎ Corresponding author. Midlands Orthopaedics, 1929201, USA. Tel.: +1 803 933 6127; fax: +1 803 933 6339
E-mail address: [email protected] (F. Liu).
0968-0160/$ – see front matter © 2008 Elsevier B.V. Aldoi:10.1016/j.knee.2008.10.011
a b s t r a c t
a r t i c l e i n f oArticle history:
This study analyzed three di Received 21 April 2008Received in revised form 16 October 2008Accepted 26 October 2008Keywords:Total knee arthroplastyFluoroscopyIn vivo kinematicsSquatPosterior stabilized (PS)
mensional (3D) in vivo kinematic data from the squatting to standing position for18 Japanese subjects (18 knees) implanted with either Legacy® Posterior Stabilized (LPS) Flex Fixed BearingTKA or LPS Flex Mobile Bearing TKA. Under weight-bearing conditions, for all patients, the average roll-forward motions for the medial and lateral condyles were 4.0±3.6 mm and 6.3±3.4 mm, and the averageexternal axial rotation was 3.1°±4.1°. For both groups, the weight-bearing range-of-motion (ROM)(110.7°±12.7°) was less than pre (127.2±15.5°) and post (135.6±5.4°) operative non-weight bearing ROM.As hypothesized, the incidence, average and maximum liftoff for the squatting to standing activity weremuch less than those of deep knee bend (DKB), and condylar motions and kinematics were opposite that ofthe DKB. There was little statistical difference of their kinematic patterns during this activity between the LPSfixed and mobile TKA implants.
© 2008 Elsevier B.V. All rights reserved.
1. Introduction
The kinematic characteristics of posterior stabilized (PS) totalknee arthroplasty (TKA) have been widely studied. In vitro studieshave reported that PS TKA can consistently restore femoral rollbackand internal tibial rotation after 60° of flexion [1,2]. In vivofluoroscope studies have shown that PS TKA obtains more normalknee kinematics and weight-bearing range of motion (ROM) com-pared to posterior cruciate-retaining (PCR) TKA [3,4]. Most of thesestudies evaluatedmovements from extension to flexion, such as deepknee bend.
The existing literature contains only a small number of studiesrelating to the kinematics of squatting [5,6]. These studies eithersimply reported the patient's ability to squat after TKA or onlyreported forward in vitro squatting kinematics using cadaver knees.To the best of our knowledge, few three-dimensional (3D) in vivobiomechanical studies have been performed after TKA to evaluate asquatting to standing activity.
It has been assumed that a squatting to standing motion has thereverse motion patterns of a deep knee bend. However, during themovement from squatting to standing, the joint moments andmuscular actions are different than those during a deep knee bend.
10 Blanding St, Columbia, SC.
l rights reserved.
For example, during a deep knee bend, the quadriceps performs adynamic eccentric action to lower the weight; however, during themovement from squatting to standing, the quadriceps performs adynamic concentric action to work against gravity and lift theweight. To better understand the kinematic characteristics of asquatting to standing motion after TKA, a study specific to theactivity had to be done.
The purpose of this study was to quantify 3D in vivo kinematics(roll-forward, external axial rotation, and liftoff) for Japanese subjectsimplanted with either Legacy® Knee Posterior Stabilized (LPS) FlexFixed Bearing TKA or LPS Flex Mobile Bearing TKA. We hypothesizedthat a squatting to standing activity had reversed kinematiccharacteristics compared to a deep knee bend.
We also determined whether the 3D in vivo kinematics differedbetween the LPS Flex Fixed Bearing TKA and the LPS Flex MobileBearing TKA. Compared to the LPS Flex Fixed Bearing TKA, the LPS FlexMobile Bearing TKAwas designed to increase contact area and relativerotation between the femoral and tibial components in order toreduce shear stress. Accordingly, we assumed that there would be astatistical difference between these two high flex implants during asquatting to standing activity.
2. Materials and methods
This comparative study received an institutional review board(IRB) approval through the University of Tennessee, Knoxville. Thestudy group in this retrospective study comprised 18 subjects (18

Table 1Patient demographic data as used in the study
Knee # Prosthesis Sex Age Diseasea Femoral size Tibial size Articular surface(mm)
Follow-up(months)
ROM pre-opb
(degrees)ROM final f/ub
(degrees)Side
1 LPS-Flex Fixed Female 60 RA C 3 10 28 145 135 Left2 LPS-Flex Fixed Male 53 RA E 4 12 32 130 130 Left3 LPS-Flex Fixed Female 79 OA E 6 10 14 145 135 Left4 LPS-Flex Fixed Female 72 OA D 4 10 25 140 130 Right5 LPS-Flex Fixed Female 79 OA D 3 10 25 105 130 Left6 LPS-Flex Fixed Female 67 RA D 2 14 23 120 135 Left7 LPS-Flex Fixed Female 76 OA C 3 14 24 130 140 Left8 LPS-Flex Fixed Female 74 OA D 3 10 23 125 140 Right9 LPS-Flex Fixed Female 76 OA D 4 10 23 145 130 Right10 LPS-Flex Fixed Female 77 OA D 4 12 26 125 140 Right11 LPS-Flex Fixed Female 79 OA D 4 12 20 105 145 Right12 LPS-Flex Mobile Female 76 OA D 4 10 17 135 140 Left13 LPS-Flex Mobile Female 69 OA F 6 9 27 140 140 Left14 LPS-Flex Mobile Male 68 OA D 4 14 23 130 140 Right15 LPS-Flex Mobile Female 74 OA D 4 14 26 90 125 Left16 LPS-Flex Mobile Female 73 OA D 5 10 22 120 130 Right17 LPS-Flex Mobile Female 85 OA E 5 12 23 140 135 Right18 LPS-Flex Mobile Male 65 OA C 3 14 18 120 140 Left
a Osteoarthritis (OA); Rheumatoid arthritis (RA).b Non-weight bearing ROM.
117F. Liu et al. / The Knee 16 (2009) 116–120
knees) implantedwith either a LPS Flex Fixed Bearing TKA or a LPS FlexMobile Bearing TKA (Zimmer, Inc. Warsaw, IN), who were randomlyselected post-operatively. There was no bias in selecting a treatment(Fixed or Flex TKA) in related to their diagnosis before the surgeries.Eleven subjects had the fixed bearing implant, and seven had themobile bearing design. There were three male and 15 female patients,and the mean patient age was 72±7.7 years (range, 53–85 years).There were eight right and 10 left knees. The principal diagnosis wasosteoarthritis for 15 patients and rheumatoid arthritis for the otherthree. All TKAs were performed between December 2001 and June2003 (Table 1).
Fluoroscope experiments were performed after 23.3±4.2 months(range, 14–32 months). When the experiments were performed, allTKA were judged clinically successful with no ligamentous laxity orpain and with Hospital for Special Surgery (HSS) knee scores N90.Each subject was asked to perform a squatting to standingmovement(the reverse motion pattern of a deep knee bend). The foot wasallowed to rotate. The initial flexion position varied because patientsbegan from a comfortable squatting position, which was not nec-essarily the maximum knee flexion value (unlike with deep kneebend).
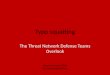
Individual fluoroscopic frames at 20° increments of extensionwerecaptured and analyzed to determine the 3D in vivo kinematics during
Fig. 1. Example of 3D to 2D o
the squatting to standing activity. The images were projected onto theimage plane, and the corresponding implant models were added tothe scene using the custom developed software SAAM (CMR, TheUniversity of Tennessee, Knoxville, USA) (Fig. 1). Using a 3D modelfitting approach, the 3D poses of the knee implants were determinedby registering the appropriate 3D CAD models onto sequential single-perspective fluoroscopic images. Each component's 3D translationaland rotational data were recorded andmeasurements of interest wereextracted.
The anterior/posterior (AP) contact positions for both the medialand lateral condyles and the axial rotation angles of the femoralcomponent relative to the tibial component were determined. Toassess condylar liftoff, the distance from each condyle to the tibialplateau was measured. A measured difference of greater than 1.0 mmsignified liftoff [7].
2.1. Error analysis
The cadaver error analysis experiment involvedmultiple variables:experimental testing including fluoroscopic and kinematic evalua-tions and absolute reference system determination using an Optotraksystem (Northern Digital Inc., Waterloo, Canada). The 3D translationsand rotations were calculated using the fluoroscopic and 3D-to-2D
verlay registered images.

Table 2Anteroposterior translation from the squatting to standing position
LPS fixed TKA LPS Flex Mobile Bearing TKA All
Full squatting positionMedial contacta −4.4±3.1 mm (range, −0.6 to −9.9 mm) −6.6±4.4 mm (range, −1.8 to −12.4 mm) −5.2±3.7 mm (range, −0.6 to −12.4 mm)Lateral contactb −8.7±2.4 mm (range, −5.0 to −13.0 mm) −8.0±1.5 mm (range, −4.9 to −9.7 mm) −8.5±2.1 mm (range, −5.0 to −13.0 mm)
Full extensionMedial contacta −0.8±3.1 mm (range, 2.9 to −6.9 mm) −2.0±3.3 mm (range, 2.9 to −4.5 mm) −1.3±3.1 mm (range, 2.9 to −6.9 mm)Lateral contactb −1.7±2.8 mm (range, 0.8 to −6.9 mm) −2.80±1.6 mm (range, 0.52 to −4.6 mm) −2.1±2.4 mm (range 0.8 to −6.9 mm)
Roll forwardc
Medial condyles 3.7±3.8 mm (range, −1.9 to 11.0 mm) 4.6±3.4 mm (range, −1.4 to 7.8 mm) 4.0±3.6 mm (range, −1.9 to 11.0 mm)Lateral condyles 7.0±3.8 mm (range, 2.5 to 16.1 mm) 5.2±2.5 mm (range, 1.6 to 9.3 mm) 6.3±3.4 mm (range, 1.6 to 16.1 mm)
a Average medial condylar contact position.b Average lateral condylar contact position.c Average anterior femoral roll forward.
118 F. Liu et al. / The Knee 16 (2009) 116–120
image registration method and later evaluated using the results fromthe Optotrak system. The overall root-mean-square (RMS) error wasconsistently less than 1.5° in rotation and 0.65 mm in translation.However, the Optotrak systemhad its own translational and rotationalerror. Further experimentation demonstrated that about 2/3 of theoverall error was due to the Optotrak system [8].
2.2. Statistical analysis
These two groups, patients implanted with LPS Flex Fixed BearingTKA and patients implanted with LPS Flex Mobile Bearing TKA, didnot strictly match each other with respect to critical parameters(such as gender, age, weight, height, preoperational score, andpostoperative score). So, this was an independent samples designstudy. The nonparametric Wilcoxon–Mann–Whitney U-test waschosen to compare the means of the two groups with significancedefined as Pb0.05.
3. Results
The average non-weight bearing ROM for knees in the fixed bearing groupwas 129°preoperatively and 135° after TKA. For knees in the mobile bearing group, the averagenon-weight bearing ROM was 125° preoperatively and 136° after TKA. There is nostatistical differences between two groups (P=0.54). For both groups combined, theaverage preoperative non-weight bearing ROM was 127.2±15.5° (range, 90–145°), andthe average postoperative non-weight bearing ROM was 135.6±5.4° (range, 125–145°).
The average weight-bearing ROM from squatting to standing was 111±13.6° for LPSfixed bearing knees and 110±12.2° for LPS mobile bearing knees. There was nostatistical difference between the two groups (P=0.72). The average weight-bearingROM for the whole group was 110.7°±12.7°.
Overall, 15 of the 18 patients experienced an anterior roll forward motion at themedial condyle during the squatting to standingmotion. All patients also experiencedan anterior roll forwardmotion at the lateral condyle, where it occurs in normal kneesduring the same activity. From squatting to maximum knee extension, anteriorfemoral roll forward averaged 4.0±3.6 mm (range, −1.9 to 11.0 mm) and 6.3±3.4 mm(range, 1.6 to 16.1 mm) for the medial and lateral condyles, respectively (Table 2).
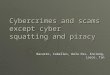
Fig. 2. Statistical analysis between LPS Fixed TKA
There were no statistical differences in roll-forward motion at the lateral (P=0.29)and medial (P=0.60) condyles between the two groups (Fig. 2). From the squatting tostanding position, the fixed bearing group experienced a significantly larger differencebetween lateral and medial AP compared to the mobile bearing group (P=0.03) (Fig. 2).
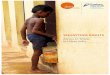
During the squatting to standing activity, the average amount of tibial externalrotation was 3.1±4.1° (range, −4.4° to 10.6°), and the maximum amount of tibialexternal rotation was 6.3±3.3° (range, 3.1° to 12.1°). Twelve patients experienced anormal external axial rotation pattern. The LPS Mobile Bearing TKA had less axialrotation compared to the LPS Fixed TKA. However, statistical differences between thetwo groups were not found when comparing axial rotation at 0, 20, 40, 60, 80, and 100°(P=0.08) nor when comparing the whole motion range (P=0.55) (Fig. 3).
Only six subjects in this study experienced condylar liftoff greater than 1.0 mm foreither condyle. Five patients had liftoff only once and one patient had liftoff at fivepositions. The average liftoff for the whole study group was 0.4±0.4 mm; the averageliftoff for the six knees in which liftoff was observed was 1.5±0.2 mm. The maximumamount of condylar liftoff was 1.9 mm (Fig. 4).
4. Discussion
According to the current study, the overall 3D kinematic contactpatterns and condylar motions after TKA during the squatting tostanding motion were similar, but of lesser magnitude, to those of thenormal knee. Subjects in this study consistently achieved roll forwardmotion, tibial external rotation, and a low occurrence of liftoff. Asanticipated, the kinematic patterns were reverse of those of deep kneebend but with lower incidence of condylar liftoff due to the principleof biomechanics.
The LPS Fixed and Mobile Bearing TKA were designed to providehigh flexion up to 155°. In Asia, where squatting is a routine practice,this ROM is needed to support squatting and other demanding dailyactivities. Previous studies have consistently reported satisfactorylong term clinical results for these two types of TKA when comparingtheir clinical and biomechanical differences [9–13]. Although deepknee bend and gait activities have been studied extensively, this is thefirst 3D in vivo study conducted on patients with either a LPS Fixed or
group and LPS Mobile Bearing TKA group.

Fig. 3. External axial rotations from the squatting to standing position.
119F. Liu et al. / The Knee 16 (2009) 116–120
Mobile Bearing TKA while performing a squatting to standing activityunder fluoroscopic surveillance.
Previous in vitro studies of cadaver knees have reported posteriorfemoral rollback with greater posterior translation at the lateralcondyle than at the medial condyle during knee flexion [14,15].Increased relative lateral condylar posterior movement with increas-ing knee flexion has been corroborated by recent fluoroscopic andMRIin vivo studies of normal knee subjects performing a deep knee bend[16–18]. Dennis et al. reported an average −19.2±8.4 mm posteriortranslation of the lateral condyle and −3.4±4.6 mm posteriortranslation of the medial condyle using fluoroscopy of normal kneesduring deep knee bends. In a fluoroscopic study of PS TKA, they foundsimilar condylar motion but of less magnitude. On average, duringdeep knee bend the posterior motion for the lateral condyle was only−3.7±3.3 mm and for the medial condyle was only −1.2±2.7 mm [17].
Fig. 4. Example of the “minimal” amount o
At the same time, chair rise analyses of normal knees have shown thatwith knee extension the lateral condyle moves more anterior than themedial condyle and the tibia experiences external rotation [16]. Sincethe activity analyzed in our study is essentially a reverse deep kneebend, we hypothesized that the results would be reversed comparedto the results of deep knee bend activity. Our hypothesis wasconfirmed because patients experienced similar roll forward motionof the medial condyle (4.0±3.6 mm; range, −1.9 to 11.0 mm) andlateral condyle (6.3±3.4 mm; range, 1.6 to 16.1 mm) with increasingknee extension from the squatting position. These data had similarmagnitudes (but opposite direction) to rollback data of deep kneebend after TKA.
From the squatting to standing position, the LPS Fixed TKA had asignificantly larger difference between lateral and medial AP transla-tion compared to the LPS Mobile TKA (P=0.028) (Fig. 2). The authors
f condylar liftoff detected in this study.

120 F. Liu et al. / The Knee 16 (2009) 116–120
think that with increasing knee extension, this ostensibly resulted inthe lateral condyle rolling more anterior than the medial condyle,causing external tibial rotation. In a previous in vitro study on cadaverknees, Fukubayashi reported internal tibial rotation during flexion andexternal tibial rotation during extension [10]. Many in vivo studieshave reported internal axial rotation during the flexion motion[9,16,17]. Previous in vitro and in vivo kinematic analyses haveshown external rotation during knee extension [19–21]. This is thefirst study to quantitatively evaluate 3D in vivo external rotationassociated with the squatting to standing motion after TKA. Accordingto a previous study, normal knees should have an average 16.5°internal tibial rotation during deep knee bend. The present researchshowed that the LPS TKA had an average of 3.1°±4.1° external tibialrotation, much less than normal knees during deep knee bend. WhileTKA does appear to create kinematically similar condylar motion fromsquatting to extension (as is the case with condylar motionmagnitudes during deep knee bend), the magnitude is less than thatof the normal knee. Dennis and Komistek found that 80% of PS TKAswith excellent clinical results had an average of 1.4 mm of condylarliftoff under weight-bearing circumstances [22]. In the present study,the average liftoff (0.4±0.4 mm) for the whole study group was muchless than those in Dennis and Komistek's study. The smaller incidenceand magnitude of condylar liftoff with this extension activity is likelydue to the increasing dynamic stabilization characteristics of thismotion relative to the deep knee bend. More specifically, thekinematics during deep knee bend result in an increase in the verticalcontact force and reduction in the transverse forces as more weight isshared in the vertical direction.
Even though the major concert of this study was to report the 3Dkinematics of squatting, this study did compare the differencesbetween the fix and mobile TKA implants. However, the majorlimitations of this comparison involved the inclusion of patients withdiffering diagnoses (osteoarthritis and rheumatoid arthritis) and thestudy size. Owing to the small number of knees, future studiesinvolving greater numbers of knees would be beneficial. Also, it mightbe beneficial to conduct a follow-up study on subjects having a PCRTKA to determine whether these good kinematic patterns, such aslarge rotations and small translations during the movement fromsquatting to standing, are PS TKA dependent or whether they can bereproduced in subjects having a posterior cruciate ligament.
5. Conflict of Interest
In support of their research or preparation of this manuscript, oneor more of the authors received grants or outside funding fromZimmer, Inc. In addition, one or more of the authors receivedpayments or other benefits or a commitment or agreement to providesuch benefits from a commercial entity (Zimmer, Inc). No commercialentity paid or directed, or agreed to pay or direct, any benefits to anyresearch fund, foundation, educational institution, or other charitableor nonprofit organization with which the authors are affiliated orassociated.
References
[1] Li G, Papannagari R, Most E, Park SE, Johnson T, Tanamal L, et al. Anterior tibial postimpingement in a posterior stabilized total knee arthroplasty. J Orthop Res2005;23:536–41.
[2] Li G, Zayontz S, Most E, Otterberg E, Sabbag K, Rubash HE. Cruciate-retaining andcruciate-substituting total knee arthroplasty: an in vitro comparison of thekinematics under muscle loads. J Arthroplasty 2001;16(8 Suppl 1):150–6.
[3] Dennis DA, Komistek RD, Colwell Jr CE, Ranawat CS, Scott RD, Thornhill TS, et al. Invivo anteroposterior femorotibial translation of total knee arthroplasty: a multi-center analysis. Clin Orthop Relat Res 1998;356:47–57.
[4] Dennis DA, Komistek RD, Hoff WA, Gabriel SM. In vivo knee kinematics derivedusing an inverse perspective technique. Clin Orthop Relat Res 1996;331:107–17.
[5] Yoshino S, Nakamura H, Shiga H, Ishiuchi N. Recovery of full flexion after total kneereplacement in rheumatoid arthritis—a follow-up study. Int Orthop 1997;21:98–100.
[6] Coughlin KM, Incavo SJ, Churchill DL, Beynnon BD. Tibial axis and patellar positionrelative to the femoral epicondylar axis during squatting. J Arthroplasty2003;18:1048–55.
[7] Wasielewski RC, Galat DD, Komistek RD. An intraoperative pressure-measuringdevice used in total knee arthroplasties and its kinematics correlations. ClinOrthop Relat Res 2004;427:171–8.
[8] Mahfouz MR, Hoff WA, Komistek RD, Dennis DA. A robust method for registrationof three-dimensional knee implant models to two-dimensional fluoroscopyimages. IEEE Trans Med Imaging 2003;22:1561–74.
[9] Sugita T, Sato K, Komistek RD, Mahfouz MR, Maeda I, Sano T. In vivo determinationof knee kinematics for Japanese subjects having either a low contact stress rotatingplatform or an anteroposterior glide total knee arthroplasty. J Arthroplasty2005;20:154–261.
[10] Fukubayashi T, Torzilla PA, Sherman MF, Warren RF. An in vitro biomechanicalevaluation of anterior–posterior motion of the knee. Tibial displacement, rotation,and torque. J Bone Joint Surg [Am] 1982;64:258–64.
[11] Wohlrab D, Ditl J, Herrschelmann R, Schietsch U, HeinW, Hube R. Does the NexGenLPS flex mobile knee prosthesis offer advantages compared to the NexGen LPS?—acomparison of clinical and radiological results. Z Orthop Ihre Grenzgeb2005;143:567–72.
[12] Komistek RD, Scott RD, Dennis DA, Yasgur D, Anderson DT, Hajner ME. In vivocomparison of femorotibial contact positions for press-fit posterior stabilized andposterior cruciate-retaining total knee arthroplasties. J Arthroplasty 2002;17:209–16.
[13] Karrholm J, Jonsson H, Nilsson KG, Soderqvist I. Kinematics of successful kneeprostheses during weight-bearing: three-dimensional movements and positionsof screw axes in the Tricon-M and Miller-Galante designs. Knee Surg SportsTraumatol Arthrosc 1994;2:50–9.
[14] Draganich LF, Andriacchi TP, Andersson GB. Interaction between intrinsic kneemechanics and the knee extensor mechanism. J Orthop Res 1987;5:539–47.
[15] Kurosawa H, Walker PS, Abe S, Garg A, Hunter T. Geometry and motion of the kneefor implant and orthotic design. J Biomech 1985;18:487–99.
[16] Komistek RD, Dennis DA, Mahfouz M. In vivo fluoroscopic analysis of the normalhuman knee. Clin Orthop Relat Res 2003;410:69–81.
[17] Dennis DA, Komistek RD, Mahfouz MR, Haas BD, Stiehl JB. Multicenter determina-tion of in vivo kinematics after total knee arthroplasty. Clin Orthop Relat Res2003;416:37–57.
[18] Hill PF, Vedi V, Williams A, Iwaki H, Pinskerova V, Freeman MA. Tibiofemoralmovement 2: the loaded and unloaded living knee studied by MRI. J Bone JointSurg [Br] 2000;82:1196–8.
[19] Dennis DA, Komistek RD, MahfouzMR,Walker SA, Tucker A. Amulticenter analysisof axial femorotibial rotation after total knee arthroplasty. Clin Orthop Relat Res2004;428:180–9.
[20] Rosenberg A, Mikosz RP, Mohler CG. Basic knee biomechanics. In: Scott N, editor.The Knee. St Louis: Mosby; 1994. p. 75–94.
[21] Van Dommelen BA, Fowler PJ. Anatomy of the posterior cruciate ligament. Areview. Am J Sports Med 1989;17:24–9.
[22] Dennis DA, Komistek RD, Walker SA, Cheal EJ, Stiehl JB. Femoral condylar lift-off invivo in total knee arthroplasty. J Bone Joint Surg [Br] 2001;83:33–9.