Embed Size (px)
Citation preview
ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Sept. 1994, p. 1953-19580066-4804/94/$04.00+0Copyright C 1994, American Society for Microbiology
In Vivo Efficacy of a Broad-Spectrum Cephalosporin, Ceftriaxone,against Penicillin-Susceptible and -Resistant Strains of
Streptococcus pneumoniae in a MousePneumonia Model
PIERRE MOINE,l* ERIC VALLtE,"2 ESTHER AZOULAY-DUPUIS,1 PHILIPPE BOURGET,3JEAN-PIERRE BEDOS,' JACQUELINE BAUCHET,1 ANDJEAN-JACQUES POCIDALO'
Institut National de la Sante et de la Recherche Medicale Unite 13, 75944 Paris, 1 Service de Microbiologie,Centre Hospitalier Universitaire Xavier Bichat-Claude Bemard, 75877 Paris,2 and Laboratoire de
Pharmacologie et de Toxicologie, Hopital Antoine Beckre, 92141 Clamart,3 France
Received 7 September 1993/Returned for modification 16 January 1994/Accepted 27 June 1994
The increasing emergence of penicillin-resistant (P') strains of Streptococcus pneumoniae could pose a
therapeutic problem in the next few years. Ceftriaxone (CRO), a broad-spectrum cephalosporin, exhibits asmaller increase in MICs against pr S. pneumoniae strains than amoxicillin (AMO) (usually referred as to the"gold standard" therapy for pneumococcal infections). Therefore, we compared their respective efficacies in aleukopenic Swiss mouse model of pneumococcal pneumonia. Infection was induced with two serotype 19strains: a penicillin-susceptible (PS) strain (MICs of <0.01 for penicillin, 0.03 for AMO, and 0.03 for CRO) anda pr strain (MICs of 4 for penicillin, 2 for AMO, and 0.5 for CRO). Untreated mice died within 2 or 3 days.Against the PS strain, the minimal protective dose (two subcutaneous injections at 12-h intervals for 3 days)for both CRO and AMO was 5 mg/kg of body weight (87% survivors). Ten-fold-increased doses of CRO (50mg/kg) gave similar protection (75% survivors) against the pr strain, whereas 20- and 40-fold-increased dosesof AMO protected 0 and 34% of the animals, respectively, against the PS strain. CRO had a marked andprolonged antibacterial effect in the lungs (2.7-log-unit reduction of CFU in 24 h after a single 50-mg/kginjection) against the Pr strain in comparison with AMO. A standard dosage of 50 mg of CRO per kg in miceresulted in peak levels in serum and protein binding comparable to those observed with 1 g given intravenouslyin humans. This dosage remained effective against a highly pr S. pneumoniae strain in this model. Themicrobiological activity and pharmacodynamic and pharmacokinetic properties of CRO (time during whichconcentrations exceed the MIC for the test pathogen [AtMIC], .8 h; and peak/MIC ratio, >90 for free activedrug) accounted for its efficacy relative to AMO (50 mg/kg: AtMIC, <2 h; peak/MIC ratio, <25) against thehighly Pr S. pneumoniae strain used in this study.
Ceftriaxone (CRO) is a cephalosporin characterized by avery broad spectrum of activity (1, 6, 8, 10) and especially by anextraordinarily long elimination half-life in serum, which is anunusual pharmacological property for this class of antibiotics(5, 8, 30, 33). It has been established that in both healthysubjects and most patients, the mean half-life ofCRO in serumis approximately 8 h (8, 9, 33). CRO exhibits a broad spectrumof antimicrobial activity, including common respiratory patho-gens (e.g., Streptococcus pneumoniae, Streptococcus pyogenes,Haemophilus influenzae, and members of the family Enterobac-teriaceae) (1, 6, 8, 10, 11, 15).
S. pneumoniae remains the most frequently isolated organ-ism in community-acquired pneumonia (22, 28). Pneumococciretained a uniformly high degree of susceptibility to penicillin(MICs, 0.005 to 0.01 mg/ml) throughout the first 2 to 2.5decades of the antibiotic era. However, after this latent periodand particularly during the 1980s, penicillin-resistant (Pr)strains have been reported, and the frequency has increased invirtually every part of the world (2). In some countries, theincidence of resistant bacteria isolated from clinical specimensrose to extremely high levels (50 to 70% in Spain and Hungary)(2, 13, 23). Increasing numbers of resistant and multiresistant
* Corresponding author. Mailing address: INSERM U 13, 190 Bd.Mac Donald, 75944 Paris Cedex 19, France. Phone: 40-35-36-44. Fax:40-36-16-99.
pneumococcal strains appeared in parallel with their increasein geographical spread (25).
Broad-spectrum cephalosporins such as CRO showed betterin vitro activity than penicillin against resistant strains (18, 20,29, 35), which suggested their potential usefulness in thetreatment of pr S. pneumoniae infections. We therefore com-pared the efficacy of CRO with that of amoxicillin (AMO),usually referred as to the "gold standard" therapy for S.pneumoniae infections (21), in mouse models of acute pneu-monia induced by penicillin-susceptible (PS) and pr S. pneu-moniae strains.
MATERIALS AND METHODS
Animals. Female Swiss mice (body weight, 20 to 22 g) wereobtained from Iffa-Credo Laboratories, France.
Challenge organisms. We failed to induce pneumonia withany pr strain in immunocompetent mice. All of these strainsbelonged to serotypes 6, 9, 14, 19, and 23, which are naturallyavirulent for mice independently of their isolation sites inhumans (4, 7). Thus, pneumonia was induced in leukopenicSwiss mice with two serotype 19 strains: a PS strain originallyisolated from a blood culture (strain P52181, provided byHopital Bichat, Paris, France) and a highly pr strain (MIC = 4p,g/ml) originally isolated from middle ear fluid (strain P15986,provided by the Centre de Reference du Pneumocoque [P.Gelin], Creteil, France).
1953
Vol. 38, No. 9
ANTIMICROB. AGENTS CHEMOTHER.
TABLE 1. Microbiological data for S. pneumoniae challengestrains and study drugs
MIC/MBC (,ug/ml)aStudy drug
P52181 P15986
Penicillin 0.03/0.03 4/8AMO 0.03/0.03 2/4CRO 0.03/0.03 0.5/1
a Determined by macrodilution in nonsupplemented Mueller-Hinton brothwith an initial inoculum of 106 CFIJ/il.
Antibiotics. The drugs used in this study were CRO (RocheLaboratories, Neuilly-sur-Seine, France) and AMO sodiumsalt (Beecham Laboratories, Paris, France). The antibioticswere reconstituted according to the instructions on the pack-age insert and diluted in sterile water to the desired concen-trations.
In vitro studies. MICs and MBCs were determined inMueller-Hinton infusion broth (Diagnostic Pasteur, Marnes-la-Coquette, France) by means of the tube dilution method(26). Each tube contained twofold dilutions of antibiotic and afinal bacterial density of 106 CFU/ml. After aerobic incubationfor 18 h at 37°C, the MIC was defined as the lowest concen-tration of antibiotic at which no turbidity was visible to thenaked eye. The MBC was determined by plating 0.01-mlaliquots from tubes with no visible growth onto Columbia agarsupplemented with 5% sheep blood (Bio-Merieux, Lyon,France). The plates were incubated overnight at 37°C, and theMBC was defined as the lowest concentration of antibiotickilling .99.9% of the original inoculum.
Leukocyte depletion in mice. We induced sustained leuko-penia in Swiss mice by daily intraperitoneal injections (150mg/kg of body weight) of cyclophosphamide (Endoxan; SargetLaboratories, Merignac, France) starting 3 days before infec-tion. Counts of circulating leukocytes per cubic millimeter ofblood were reduced from about 7,000 to 880 on the day ofinfection. Under these conditions, mice became more suscep-tible to the two poorly virulent P5 and pr serotype 19 strains.
Experimental pneumococcal pneumonia in mice. Animalswere infected by intratracheal instillation via the mouth asdescribed in detail elsewhere (3). Briefly, animals were anes-thetized intraperitoneally with 0.2 ml of 0.65% sodium pento-barbital and were suspended by the upper incisors. The tracheawas cannulated via the mouth with a blunt needle, and 50 ,ul ofbacterial suspension (107 CFU of P5 and pr S. pneumoniae permouse) was instilled. Leukopenic mice developed acute pneu-monia and died within 2 or 3 days. All the animals quicklybecame bacteremic. Bacterial counts exceeded 108 CFU perlung for the infected mice at the time of their death (>106CFU/ml of blood).
Survival studies. Therapy was initiated 3 h after bacterialchallenge. A total of six subcutaneous (s.c.) injections wereadministered at 12-h intervals. Treatment schedules are pre-sented in the figures, with the results. Fifteen animals pertreatment group were used, and in each experiment theanimals were infected simultaneously. Experiments were re-peated at least twice. The observation period was 14 days.Death rates were recorded daily, and cumulative survival rateswere compared.
Bactericidal activity in vivo. The study drugs were assessedfor their ability to eradicate bacteria in the lungs. Drugadministration was initiated 3 h after infection and consisted ofa single dose ofAMO and CRO. Various doses (5, 10, 50, and100 mg/kg of body weight) of each drug, depending on the
Percent survivors
80
60
40
20
ceftriaxone 10 mg/kg@ ceftriaxone 5 mg/kg
-0-'- amoxicillin 5 mg/kgControl
3 h pi
0 2 4 6 8 10 12 14Days post infection
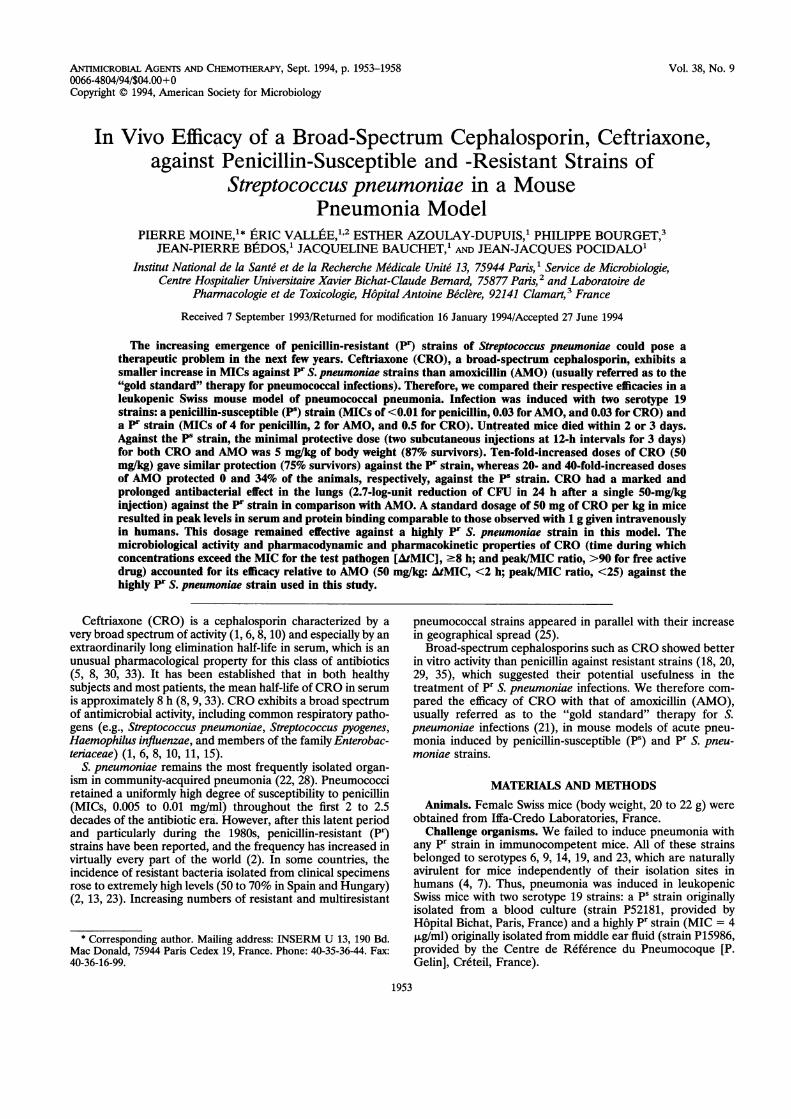
FIG. 1. Cumulative survival of treated and control leukopenicSwiss mice after intratracheal challenge with 107 CFU of the P5 S.pneumoniae strain (P52181). As of 3 h postinfection (pi), mice receivedsix s.c. administrations of the indicated amounts of drug at 12-hintervals.
infective strain, were administered in 0.5 ml of sterile water.Controls received the same volume of isotonic saline. The totalCFU recovered from whole-lung homogenates was determinedat 1, 3, 6, 8, and 24 h after one injection. Mice were killed byCO2 asphyxiation and were exsanguinated by cardiac puncture(the blood was used for cultures). The lungs were removed andhomogenized in 2 ml of saline. Serial 10-fold dilutions of thehomogenates were plated onto Columbia agar (0.1 ml/9-cm-diameter plate). Results are expressed as the mean log CFUper lung ± standard deviation for groups of three mice. Thelower limit of detection was 2 log CFU per lung, whichcorresponded to the weakest dilution of tissue homogenates(10-1) that avoided significant drug carryover with controlinocula.
Pharmacokinetic studies. The pharmacokinetic profiles ofAMO and CRO were examined in parallel in infected Swissmice.
(i) Bioassay. Concentrations in lungs and sera were deter-mined after single s.c. doses of 50 mg of AMO and CRO perkg. In infected mice, the antibiotic was given 3 h after challengewith strain P15986. At 0.5, 1, 2, 4, 6, 8, 10, and 24 h followingdrug administration, three animals per group were killed withCO2 and exsanguinated by intracardiac puncture. Blood sam-ples were centrifuged to isolate serum, pooled, and frozen at-80°C until assay. Lungs were harvested from exsanguinatedmice, washed in sterile sodium chloride solution, and frozen.On the day of assay, organs were weighed, pooled, andhomogenized in phosphate buffer (pH = 6.8). Homogenateswere centrifuged and the supernatants were used for assay.AMO concentrations were determined by the agar well diffu-sion method, using Sarcina lutea ATCC 9341 as the bioassayorganism and Antibiotic Medium 1 (Difco Laboratories, De-troit, Mich.) as the growth medium. CRO concentrations weredetermined by the agar well diffusion method, using Esche-richia coli ATCC 39118 as the bioassay organism and Antibi-otic Medium 1 (Difco Laboratories) as the growth medium.Standard curves were determined with solutions of AMO and
1954 MOINE ET AL.
IN VIVO EFFICACY OF CEETRIAXONE AGAINST S. PNEUMONMIE 1955
Percent survivors
0 2 4 6 8 10Days post infection
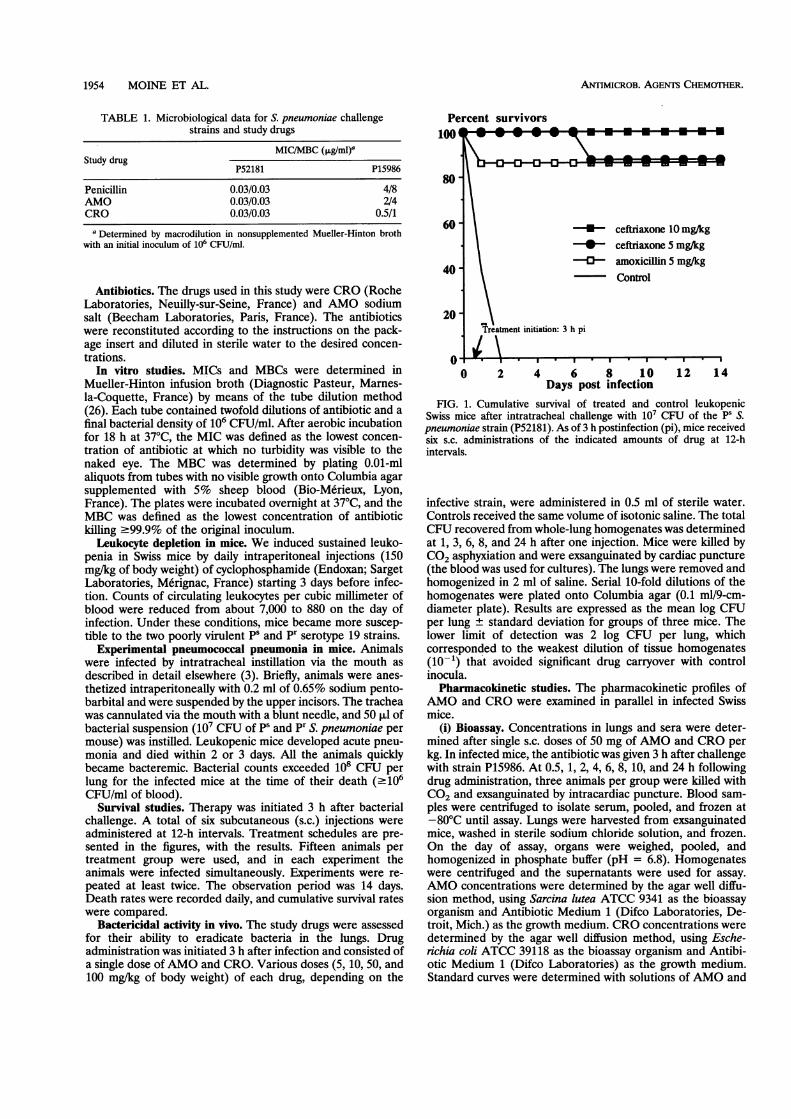
FIG. 2. Cumulative survival of treated and cont:Swiss mice after intratracheal challenge with 107 CFpneumoniae strain (P15986). As of 3 h postinfection (pisix s.c. administrations of the indicated amounts ofintervals.
CRO in phosphate buffer for serum and tissueevaluate the active fractions of the drugs. Respressed as micrograms per milliliter of blood oI
lung tissue. The standard curve was linear fron,ug/ml. The sensitivity of the assay was aboutsample, and the coefficients of between- and witltions for replicates (n = 5) were c7.5% at 0.5,:R±g/ml.
(ii) HPLC. CRO samples were also assayed b)mance liquid chromatography (HPLC) combinspectrophotometric detection at 274 nm. The HP](ion pair reversed-phase chromatography) companalytical recommendations of Trautmann and(34). The method used a test specimen of 100 RIits lower limit of sensitivity was 0.5 ,ug/ml. The acassay method, which was studied at target values (250 mg/liter (serum loaded with CRO in vitro)cients of between- and within-day variations of s'CRO. The linear range of the assay was betweimg/liter. Under the analysis conditions, the reten
CRO and the internal standard were 2.1 and 2.8 min, respec-tively. All samples were assayed in duplicate. Control runs
50 mg/kg performed regularly.
50mg/kg(iii) Protein binding. The extent of CRO binding to plasma
300mg/kg proteins was determined with an ultrafiltration system. The
Ultrafree CL device (UFC4LG25; Millipore, Saint-Quentin-en-Yvelines, France) was used (27). In brief, 700 ,ul of pooled
* **-- plasma samples from six mice was placed in the filter cup
(upper part of the device), which is separated from the filtraten200mg/kg cup by an ultrafiltration membrane. Ultrafiltration was ob-
e 25 mg/kg tained under nitrogen pressure (4 kg/cm2). The device was
kept under these conditions for 2 h (at 37°C). In the ultrafil-trate (filtrate cup), the concentrations of unbound CRO were
_0-0-0 determined by the method described above. The accuracy ofthe assay method, which was studied at target values of 0.5, 7.5,and 20 mg/liter, gave coefficients of between- and within-day
l S* variations of c8.5% for unbound CRO.(iv) Analysis. Pharmacokinetic analyses were performed by
routine graphical methods, and parameters were estimated by12 14 (17). tl/2,,life at ,B phase calculated by using linear least-square regres-
sion for the log linear terminal-elimination phase; AtMIC is therol leukopenic time during which concentrations exceed the MIC for the testU of the Pr S. pathogen (P15986); and AUC,-24 is the area under the con-mice received centration-time curve from 0 to 24 h, calculated by the
f drug at 12-h trapezoidal rule.
Statistical analysis. Survival rate data were analyzed byunpaired t test. Analysis of variance (repeated measures) wasperformed to compare CFU values. P values of 0.05 or less
in order to were considered statistically significant.ults were ex-
rper gram of RESULTS
n 0.125 to 320.1 ,ug/ml of In vitro data. Against the PS strain, penicillin, AMO, andhin-day varia- CRO showed identical low MICs and MBCs. However, against1, 7.5, and 20 the pr strain, AMO was four times less active than CRO (Table
1).y high-perfor- Therapeutic efficacy in experimental pneumonia. With our
ied with UV treatment schedule (treatment initiated 3 h after infection andLC technique consisting of 6 s.c. injections at 12-h intervals), both AMO andlied with the CRO treatments at 5 mg/kg were associated with an 87%Haefelfinger survival rate (P < 0.001 versus untreated control group [0%])of serum, and (Fig. 1). A 100% survival rate was achieved with CRO at 10xcuracy of the mg/kg.
)f 1.0, 75, and With the pr strain, results were as follows. A 10-fold-, gave coeffi- increased dose of CRO (50 mg/kg) gave protection (75%2.7% for total survivors) (P = 0.22) similar to that against the PS strain,en 0 and 300 whereas 20- and 40-fold-increased doses of AMO protected 0tion times for and 34% of the animals, respectively (Fig. 2). Treatment with
TABLE 2. Clearance of S. pneumoniae from lungs and blood of Swiss mice infected with PS strain P52181 followinga single s.c. injection of study drugs
Value after treatment with:
Time (h) Nothing (control) AMO, 5 mg/kg CRO, 5 mg/kg CRO, 10 mg/kg
Lunga Bloodb Lung Blood Lung Blood Lung Blood
1 5.33 ± 0.35 1/3 4.58 ± 0.51 0/3 4.95 ± 0.33 0/3 4.33 ± 0.58C 0/33 5.74 ± 1.04 1/3 3.97 ± 0.45C 1/3 4.38 ± 0.38C 0/3 3.42 ± 0.39C 0/36 3.69 ± 0.81 0/3 3.54 ± 1.20 0/3 2.43 ± 0.93 0/38 5.50 ± 0.71 3/3 4.26 ± 0.24 0/3 3.95 ± 0.49 0/3 3.00 ± 1.41C 0/3
24 4.87 ± 0.55 2/3 3.95 ± 0.91 2/3 3.26 ± 0.83 1/3a log10 CFU per milliliter of lung homogenate. Values are means ± standard deviations (n = 3).b Number of animals with positive blood cultures/total number of animals.c Value lower than for the control group (P < 0.03).
VOL. 38, 1994
ANTIMICROB. AGENTS CHEMOTHER.
TABLE 3. Clearance of S. pneumoniae from lungs and blood of Swiss mice infected with pr strain P15986 followinga single s.c. injection of study drugs
Value after treatment with:
Time (h) Nothing (control) AMO, 100 mg/kg CRO, 50 mg/kg CRO, 100 mg/kg
Luhga Bloodb Lung Blood Lung Blood Lung Blood
1 7.1 ± 0.22 1/3 6.82 ± 0.04 0/3 6.77 ± 0.67 0/3 7.05 ± 0.19 0/33 7.63 ± 0.06 1/3 6.69 ± 0.21c 2/3 6.39 ± 0.27c 2/3 6.31 ± 0.36C 1/36 6.77 ± 0.24 1/3 6.29 ± 0.13d 2/3 5.51 ± 0.22de 0/38 7.42 ± 0.4 3/3 7.35 ± 0.08 2/3 5.41 ± 0.46Cd 1/3 5.26 ± 0.44c4 1/3
24 7.74 ± 0.37 3/3 7.35 ± 0.32 3/3 4.13 ± 0.98cd 3/3 4.35 ± 0.58c4 3/3a log10 CFU per milliliter of lung homogenate. Values are means ± standard deviations (n = 3).bNumber of animals with positive blood cultures/total number of animals.c Value lower than for the control group (P < 0.002 to 0.0001).d Lower than value for AMO at 100 mg/kg (P < 0.03 to 0.0001).I Lower than value for CRO at 50 mg/kg (P = 0.003).
AMO at 300 mg/kg was associated with 67% survival. For bothantibiotics, the survival rate did not significantly improve withlarger doses.
Bacterial clearance from lungs. Results with the PS strainare presented in Table 2. Three hours after a single-doseinjection (AMO at 5 mg/kg; CRO at S and 10 mg/kg), theintrapulmonary bacterial decrease was significant with eithercompound relative to the control value (P < 0.03).
Results with the pr strain were as follows (Table 3). Threehours after a single s.c. injection of CRO (50 and 100 mg/kg)or AMO (100 mg/kg), bacterial counts in the lungs were
significantly lower than those in controls. However, CRO hada prolonged antibacterial effect compared with that of AMO,as shown by a 2.7-log-unit reduction in CFU 24 h after a singleadministration. In contrast, pulmonary bacterial counts in theAMO-treated group remained unchanged over the 8-h periodfollowing a single administration.Serum and lung pharmacokinetics. After a single s.c. injec-
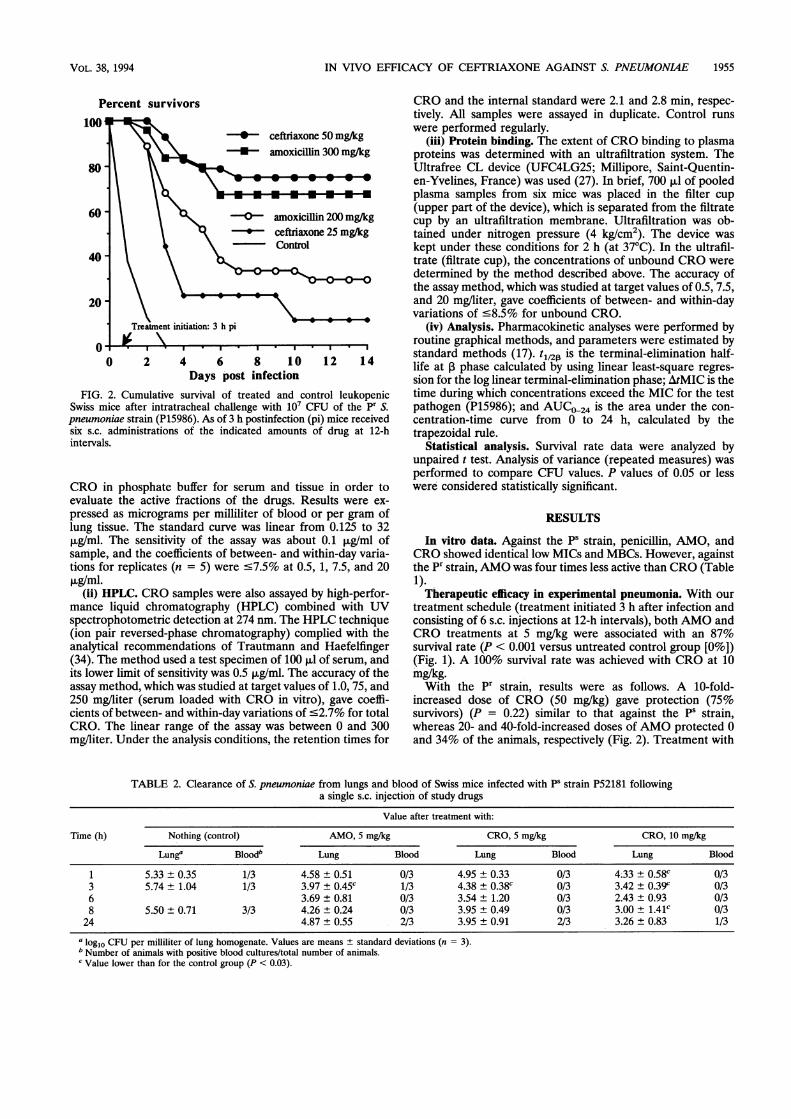
tion of 50 mg/kg, CRO showed the same peak concentration inserum but with a larger serum AUC than AMO (97 versus 61,ug * h/ml) (Table 4). The elimination half-life in serum was
longer for CRO than AMO (1.41 versus 0.41 h). Similarly,CRO showed higher peak levels in the lung (36.7 ug/nml), a
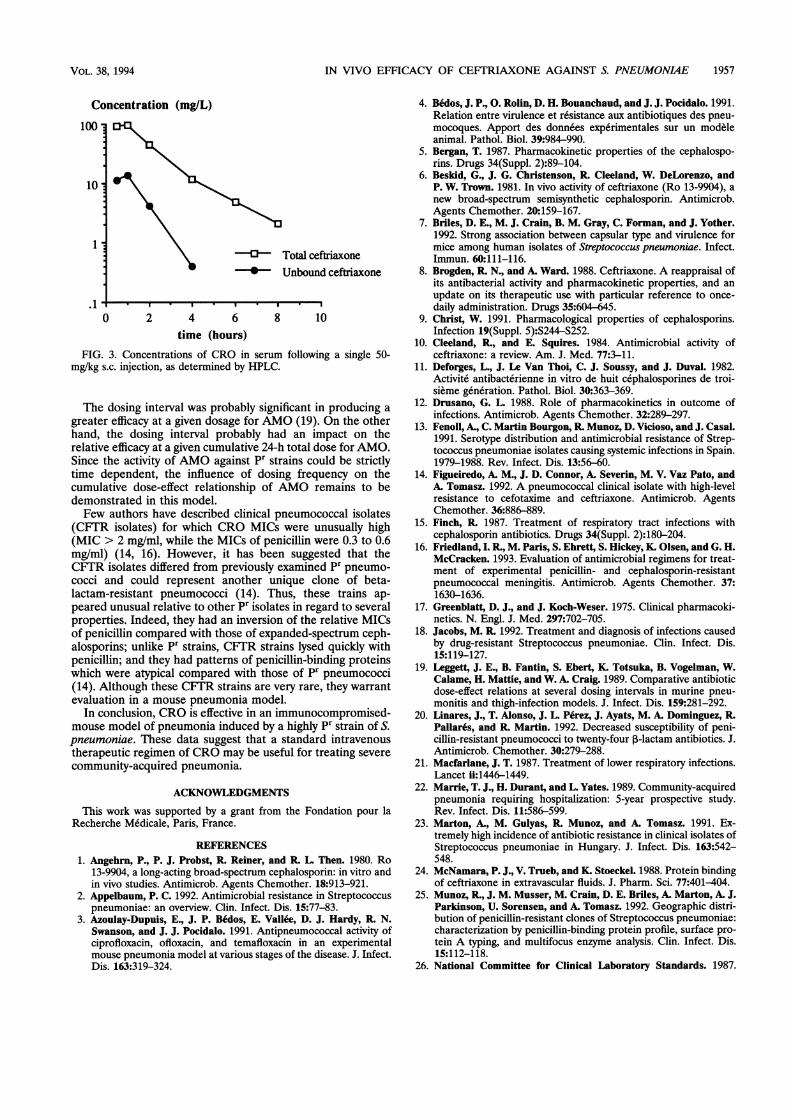
longer ptulmonary half-life (1.12 h), and a larger serum AUC(79 ,ug * h/ml) than AMO (15 ,ug/ml, 0.79 h, and 15 ,ug * h/ml,respectively). Within the range of the observed total concen-trations in serum (0.6 to 94.5 ,ug/ml), the protein binding ofCRO decreases with increasing drug concentration from 96.4to 85.6% (Fig. 3).
DISCUSSIONS. pneumoniae is the most frequent causative pathogen of
community-acquired pneumonia (22, 28). The increasing prev-alence of antimicrobial resistance in strains from invasiveinfections has severe implications for future antimicrobialstrategies against pneumococci. Alternatives to penicillin ther-apy must be considered, especially for the management ofpneumonia caused by highly resistant strains (29). Treatmentof pneumococcal infections must take into account the suscep-tibility patterns of the strains in the community. CRO showedrelatively good activity against resistant strains, despite theassociation between a high penicillin resistance level andhigher MICs of this agent (18, 20, 29, 35). For such isolates, theMICs of CRO were nevertheless two to eight times lower thanthe respective MICs of penicillin (20). Thus, these increasedMICs remain far below levels of this agent in serum (30).Our data from a mouse model of pneumonia showed that
CRO had greater efficacy than AMO against a highly pr S.pneumoniae strain (penicillin MIC = 4 ,ug/ml). At a dose of 50mg/kg, CRO showed a sustained bactericidal activity in rela-tion to levels in serum and tissues that remained far higherthan the MIC for the challenge strain (CRO MIC, 0.5 ,ug/ml).A sixfold-higher dose of AMO was required to achieve thesame efficacy. In addition, CRO had longer half-lives in serumand lungs and a greater AUC than AMO. The lower MICs andMBCs and more favorable pharmacokinetics of CRO thanthose of AMO were the determinant factors involving efficacyagainst highly resistant pneumococci in vivo. The /tMICappeared to be a major pharmacodynamic parameter correlat-ing with efficacy in this model. There is considerable contro-versy over the relevance of drug-protein binding in terms ofdrug efficacy (12, 24, 32). Protein binding has long beenrecognized as an important factor in determining antimicrobialactivity (31, 36). Results of the present study showed that thehigh rate of protein binding of CRO, relative to that usuallyreported for AMO, did not disadvantage its activity in vivo. Onthe contrary, the prolonged AtMIC suggested that the protein-bound fraction of the drug may serve as a reservoir andcontribute to the therapeutic efficacy of this agent.
In our mouse model, peak concentrations in serum obtainedafter an s.c. dose of 50 mg of CRO per kg are similar to thoseachieved in humans after a 1-g intravenous administration (133to 151 ,ug/ml) (8, 30). Despite a shorter elimination phase(t01/2 1.4 versus 7.6 h) (30) and a smaller serum AUC (97versus 1,146 ,ug* h/ml) (32) in mice, the experimental level ofefficacy of CRO was high and suggested that at least the sameactivity would be achieved in humans.
TABLE 4. Pharmacokinetic parameters of AMO and CRO ininfected Swiss mice following a single s.c. dose of 50 mg/kge
Drug Site Cmax (g/ml t(h) AtMIC (Ag h/ml
AMO Serum 47.0 ± 18.0 0.41 1- 2 60.8Lung 15.0 ± 9.0 0.79 1- 2 14.6
CRO Serum 46.5 ± 0.5 1.41 8-10 96.6Lung 36.7 ± 7.9 1.12 6- 8 79.5
Values are calculated from mean concentrations in serum and lung tissuesamples taken at 0.5, 1, 2, 4, 6, 8, 10, and 24 h postdosing. AMO and CROconcentrations were determined by the agar well diffusion method.
b C,,,,C maximum concentration observed.c Values calculated for the pr strain (P15986; MICs = 2 for AMO and 0.5 for
CRO).
1956 MOINE ET AL.
IN VIVO EFFICACY OF CEFTRIAXONE AGAINST S. PNEUMONIE 1957
Concentration (mg/L)
100
10
1
.1
0} Total ceftriaxone*- Unbound ceftriaxone
0 2 4 6 8 10time (hours)
FIG. 3. Concentrations of CRO in serum following a single 50-mg/kg s.c. injection, as determined by HPLC.
The dosing interval was probably significant in producing a
greater efficacy at a given dosage for AMO (19). On the otherhand, the dosing interval probably had an impact on therelative efficacy at a given cumulative 24-h total dose for AMO.Since the activity of AMO against pr strains could be strictlytime dependent, the influence of dosing frequency on thecumulative dose-effect relationship of AMO remains to bedemonstrated in this model.Few authors have described clinical pneumococcal isolates
(CFTR isolates) for which CRO MICs were unusually high(MIC > 2 mg/ml, while the MICs of penicillin were 0.3 to 0.6mg/ml) (14, 16). However, it has been suggested that theCKIR isolates differed from previously examined pr pneumo-
cocci and could represent another unique clone of beta-lactam-resistant pneumococci (14). Thus, these trains ap-
peared unusual relative to other pr isolates in regard to severalproperties. Indeed, they had an inversion of the relative MICsof penicillin compared with those of expanded-spectrum ceph-alosporins; unlike pr strains, CFTR strains lysed quickly withpenicillin; and they had patterns of penicillin-binding proteinswhich were atypical compared with those of pr pneumococci(14). Although these CFTR strains are very rare, they warrantevaluation in a mouse pneumonia model.
In conclusion, CRO is effective in an immunocompromised-mouse model of pneumonia induced by a highly pr strain of S.pneumoniae. These data suggest that a standard intravenoustherapeutic regimen of CRO may be useful for treating severe
community-acquired pneumonia.
ACKNOWLEDGMENTS
This work was supported by a grant from the Fondation pour laRecherche Medicale, Paris, France.
REFERENCES1. Angehrn, P., P. J. Probst, R Reiner, and R L. Then. 1980. Ro
13-9904, a long-acting broad-spectrum cephalosporin: in vitro andin vivo studies. Antimicrob. Agents Chemother. 18:913-921.
2. Appelbaum, P. C. 1992. Antimicrobial resistance in Streptococcuspneumoniae: an overview. Clin. Infect. Dis. 15:77-83.
3. Azoulay-Dupuis, E., J. P. Bedos, E. Vallee, D. J. Hardy, R N.Swanson, and J. J. Pocidalo. 1991. Antipneumococcal activity ofciprofloxacin, ofloxacin, and temafloxacin in an experimentalmouse pneumonia model at various stages of the disease. J. Infect.Dis. 163:319-324.
4. Bedos, J. P., 0. Rolin, D. H. Bouanchaud, and J. J. Pocidalo. 1991.Relation entre virulence et r6sistance aux antibiotiques des pneu-mocoques. Apport des donnees experimentales sur un modeleanimal. Pathol. Biol. 39:984-990.
5. Bergan, T. 1987. Pharmacokinetic properties of the cephalospo-rins. Drugs 34(Suppl. 2):89-104.
6. Beskid, G., J. G. Christenson, R. Cleeland, W. DeLorenzo, andP. W. Trown. 1981. In vivo activity of ceftriaxone (Ro 13-9904), anew broad-spectrum semisynthetic cephalosporin. Antimicrob.Agents Chemother. 20:159-167.
7. Briles, D. E., M. J. Crain, B. M. Gray, C. Forman, and J. Yother.1992. Strong association between capsular type and virulence formice among human isolates of Streptococcus pneumoniae. Infect.Immun. 60:111-116.
8. Brogden, R. N., and A. Ward. 1988. Ceftriaxone. A reappraisal ofits antibacterial activity and pharmacokinetic properties, and anupdate on its therapeutic use with particular reference to once-daily administration. Drugs 35:604-645.
9. Christ, W. 1991. Pharmacological properties of cephalosporins.Infection 19(Suppl. 5):S244-S252.
10. Cleeland, R, and E. Squires. 1984. Antimicrobial activity ofceftriaxone: a review. Am. J. Med. 77:3-11.
11. Deforges, L., J. Le Van Thoi, C. J. Soussy, and J. Duval. 1982.Activite antibacterienne in vitro de huit cephalosporines de troi-sieme generation. Pathol. Biol. 30:363-369.
12. Drusano, G. L. 1988. Role of pharmacokinetics in outcome ofinfections. Antimicrob. Agents Chemother. 32:289-297.
13. Fenoll, A., C. Martin Bourgon, R Munoz, D. Vicioso, and J. Casal.1991. Serotype distribution and antimicrobial resistance of Strep-tococcus pneumoniae isolates causing systemic infections in Spain.1979-1988. Rev. Infect. Dis. 13:56-60.
14. Figueiredo, A. M., J. D. Connor, A. Severin, M. V. Vaz Pato, andA. Tomasz. 1992. A pneumococcal clinical isolate with high-levelresistance to cefotaxime and ceftriaxone. Antimicrob. AgentsChemother. 36:886-889.
15. Finch, R 1987. Treatment of respiratory tract infections withcephalosporin antibiotics. Drugs 34(Suppl. 2):180-204.
16. Friedland, L. R, M. Paris, S. Ehrett, S. Hickey, K. Olsen, and G. H.McCracken. 1993. Evaluation of antimicrobial regimens for treat-ment of experimental penicillin- and cephalosporin-resistantpneumococcal meningitis. Antimicrob. Agents Chemother. 37:1630-1636.
17. Greenblatt, D. J., and J. Koch-Weser. 1975. Clinical pharmacoki-netics. N. Engl. J. Med. 297:702-705.
18. Jacobs, M. R 1992. Treatment and diagnosis of infections causedby drug-resistant Streptococcus pneumoniae. Clin. Infect. Dis.15:119-127.
19. Leggett, J. E., B. Fantin, S. Ebert, K. Totsuka, B. Vogelman, W.Calame, H. Mattie, and W. A. Craig. 1989. Comparative antibioticdose-effect relations at several dosing intervals in murine pneu-monitis and thigh-infection models. J. Infect. Dis. 159:281-292.
20. Linares, J., T. Alonso, J. L. Perez, J. Ayats, M. A. Dominguez, RPallares, and R Martin. 1992. Decreased susceptibility of peni-cillin-resistant pneumococci to twenty-four 3-lactam antibiotics. J.Antimicrob. Chemother. 30:279-288.
21. Macfarlane, J. T. 1987. Treatment of lower respiratory infections.Lancet ii:1446-1449.
22. Marrie, T. J., H. Durant, and L. Yates. 1989. Community-acquiredpneumonia requiring hospitalization: 5-year prospective study.Rev. Infect. Dis. 11:586-599.
23. Marton, A., M. Gulyas, R. Munoz, and A. Tomasz. 1991. Ex-tremely high incidence of antibiotic resistance in clinical isolates ofStreptococcus pneumoniae in Hungary. J. Infect. Dis. 163:542-548.
24. McNamara, P. J., V. Trueb, and K. Stoeckel. 1988. Protein bindingof ceftriaxone in extravascular fluids. J. Pharm. Sci. 77:401-404.
25. Munoz, R, J. M. Musser, M. Crain, D. E. Briles, A. Marton, A. J.Parkinson, U. Sorensen, and A. Tomasz. 1992. Geographic distri-bution of penicillin-resistant clones of Streptococcus pneumoniae:characterization by penicillin-binding protein profile, surface pro-tein A typing, and multifocus enzyme analysis. Clin. Infect. Dis.15:112-118.
26. National Committee for Clinical Laboratory Standards. 1987.
VOL. 38, 1994

ANTIMICROB. AGENTS CHEMOTHER.
Methods for dilution antimicrobial susceptibility tests for bacteriathat grow aerobically. Approved standard M7-A. National Com-mittee for Clinical Laboratory Standards, Villanova, Pa.
27. Ohshima, T., I. Johno, and S. Kitazawa. 1988. Comparativeevaluation of microultraffitration devices for determination ofprotein binding. Ther. Drug Monit. 10:310-315.
28. Ortqvist, A., J. Hedlund, L. Grillner, E. Jalonem, I. Kallings, M.Leinonen, and M. Kalin. 1990. Aetiology, outcome and prognosticfactors in community-acquired pneumonia requiring hospitaliza-tion. Eur. Respir. J. 3:1105-1113.
29. Pallares, R., F. Gudiol, J. Linares, J. Ariza, G. Rufi, L Murgui, J.Dorca, and P. F. Viladrich. 1987. Risk factors and response toantibiotic therapy in adults with bacteremic pneumonia caused bypenicillin-resistant pneumococci. N. Engl. J. Med. 317:18-22.
30. Patel, L. H., and S. A. Kaplan. 1984. Pharmacokinetic profile ofceftriaxone in man. Am. J. Med. 77:17-25.
31. Rolinson, G. N. 1980. The significance of protein binding ofantibiotics in antibacterial chemotherapy. J. Antimicrob. Che-mother. 6:311-317.
32. Scaglione, F., M. Raichi, and F. Fraschini. 1990. Serum proteinbinding and extravascular diffusion of methoxyimino cephalospo-rins. Time courses of free and total concentrations of cefotaximeand ceftriaxone in serum and pleural exudate. J. Antimicrob.Chemother. 26(Suppl. A):1-10.
33. Scully, B. E., K. P. Fu, and H. C. Neu. 1984. Pharmacokinetics ofceftriaxone after intravenous infusion and intramuscular injection.Am. J. Med. 77:112-116.
34. Trautmann, K. H., and P. Haefelfinger. 1981. Determination ofthe cephalosporin Ro 13-9904 in plasma, urine, and bile by meansof ion-pair reversed phase chromatography. High Resolut. Chro-matogr. Commun. 4:54-59.
35. Viladrich, P. F., F. Gudiol, J. Linares, G. Rufi, J. Ariza, and RPallares. 1988. Characteristics and antibiotic therapy of adultmeningitis due to penicillin-resistant pneumococci. Am. J. Med.84:839-846.
36. Wise, R 1983. Protein binding of ,B-lactams: the effects on activityand pharmacology, particularly tissue penetration. J. Antimicrob.Chemother. 12:1-18.
1958 MOINE ET AL.





























