Embed Size (px)
Citation preview

6/9/2014
1
In‐vivo detectionofdeepretinalneuronallayerchangesfollowing
acuteopticneuritis
OmarAl‐Louzi,MD;PavanBhargava,MD;ScottNewsome,DO;PeterCalabresi,MD;ShivSaidha,MD
DepartmentofNeuroimmunologyandNeuroinfectiousdisordersJohnsHopkinsUniversity
May31,2014
Disclosures
• Dr.Al‐Louzi reportsnodisclosures.
• Dr.Bhargavareportsnodisclosures.
• Dr.NewsomehasreceivedconsultationfeesfromBiogen‐IdecandGenzymeaswellasresearchsupportfromBiogen‐IdecandNovartis.
• Dr.Calabresi hasreceivedcompensationforconsultingandservingonscientificadvisoryboardsfrom:Vaccinex,Vertex,Prothena,andAbbvie; andhasreceivedresearchfundingforimagingresearchfromNIHR01NS082347,NMSS,RacetoEraseMS,andNovartis;andforunrelatedresearchprojectsfromBiogen‐IDECandMedImmune.
• Dr.SaidhareceivesfundingsupportfromtheRacetoEraseMS,andhasreceivedconsultingfeesfromMedicalLogix forthedevelopmentofCMEprogramsinneurology,consultingfeesfromAxonAdvisorsLLC,EducationalGrantSupportfromNovartis&Teva Neurosciences,andspeakinghonorariafromtheNationalAssociationofManagedCarePhysicians.

6/9/2014
2
Multiplesclerosis(MS)
• MSisanimmune‐mediateddemyelinatingdisorderoftheCentralNervousSystem(CNS)withbothinflammatoryanddegenerativecomponents.
• MScommonlyinvolvestheopticnerves;acuteopticneuritis(AON)isthepresentingfeaturein~20%ofpatients,while50%experienceitatsomepointduringthecourseoftheirdisease1.
• AutopsystudiesdemonstratethatopticnervepathologyispresentinthemajorityofMSpatientsevenintheabsenceofovertclinicalinvolvement2.
1. Balcer,L.J.OpticNeuritis.NEngl JMed 354, 1273–1280(2006)2. Toussaint,D.,Périer,O.,Verstappen,A.&Bervoets. J.Clin.Neuroophthalmol. 3, 211–20(1983).
Retinalhistology
Microscopiccross‐sectionalviewthroughtheopticnerveincludingtheretinallayershttp://hubel.med.harvard.edu
OPTICNERVE
RetinalNerveFiberLayer
OPTICDISC
GanglionCellLayer

6/9/2014
3
Opticalcoherencetomography(OCT)
• OCTisatechniquethatemployslowcoherenceinterferometryofnear‐infraredlight.
• Itisusedtogeneratein‐vivo high‐resolution(<5µm),cross‐sectionalimagesoftheretina.
• Becauseofthedepth‐resolvingcapacityofOCT,itenablesvisualizationofretinaltissuestructuressimilartotissuesectionsunderamicroscope.
EvidencethatretinalneuronallossoccursinMS
• Retrogradeneurodegenerationisthoughttoculminateindropoutofretinalganglioncells.
• Ourgrouphaspreviouslyshownusingmacularsegmentationthatthinningofthecompositeganglioncell+innerplexiform(GCIP)layersoccursfollowingAON1.
• However,comprehensivelongitudinalin‐vivo assessmentofdeepretinalneuronallayersfollowingONremainslargelyunexplored.
1. Syc,S.B.etal..Brain 135, 521–33(2012).
Ganglioncelldropout(79%ofMSpatienteyeballs)
Innernuclearlayerneurondropout(40%ofMSpatienteyeballs)
Greenetal.Brain2010;133:1591‐601

6/9/2014
4
Objectives
• TodeterminewhetherobjectivechangesinINLandONLthicknessesoccurfollowingAON.
• Toexplorewhetherthesechangesmaybetemporallyrelatedtothicknesschangesofthecompositeganglioncell+innerplexiformlayerthickness(GCIP).
Methods‐ Participants
• 34patientsdiagnosedwithacuteunilateraldemyelinatingON.
• Baselineevaluationwasperformedwithameandelayof14daysfromonset(SD8.8,range:1‐33days).
• Acomparisoncohortof34MSpatients,whodidnotdevelopAON,werematched1:1basedonage,sex,anddurationofOCTfollow‐up.

6/9/2014
5
Demographicandclinicalcharacteristics
Abbreviations:AON=Acuteopticneuritis;MS=multiplesclerosis;CIS=clinicallyisolatedsyndrome;RRMS=relapsing‐remittingmultiplesclerosis;SPMS=secondaryprogressivemultiplesclerosis;IQR=inter‐quartilerange.
PatientspresentingwithAONatbaseline
PatientswithMSwhodidnotdevelopAONatbaselineorduring
follow‐up
P‐value
Age,y,mean(SD) 36.4(9.4) 35.9(9.1) 0.83a
Female,n(%) 30(88) 30(88) 1.00b
Diagnosis,n(%)
CIS
RRMS
SPMS
7(20.6)
26(76.5)
1(2.9)
0(0.0)
33(97.1)
1(2.9)
0.01b
EyeswithaprevioushistoryofAON,n(%)
12(17.6) 19(27.9)0.15d
Follow‐upduration,months,median(IQR;range)
22.5(12.6‐34.2) 22.9(14.2‐36.4)0.65c
a Two‐sampleStudent’st‐test.bFisher’sexacttest.c Mann–WhitneyUtest.dChi‐squaredtest.
Retinalimaging• PatientsunderwentCirrus‐HDOCTimaging,withautomatedintra‐retinallayersegmentation,ateachstudyvisit.
• Twomacularsegmentationmethodswereusedtoobtainmeasuresofretinallayerthickness:1. Manufacturer’salgorithm
2. Graph‐based,open‐accessmethod
0.54mm
2.4mm
5mm
5mm
6/9/2014
6
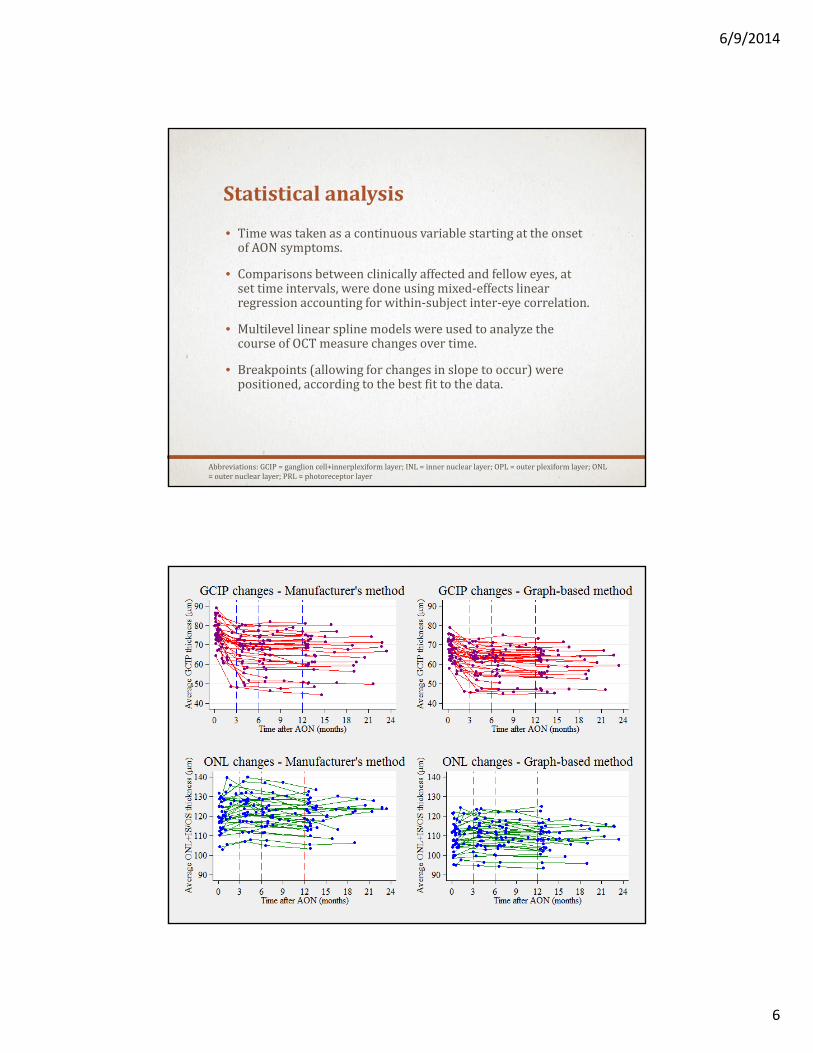
Statisticalanalysis
• TimewastakenasacontinuousvariablestartingattheonsetofAONsymptoms.
• Comparisonsbetweenclinicallyaffectedandfelloweyes,atsettimeintervals,weredoneusingmixed‐effectslinearregressionaccountingforwithin‐subjectinter‐eyecorrelation.
• MultilevellinearsplinemodelswereusedtoanalyzethecourseofOCTmeasurechangesovertime.
• Breakpoints(allowingforchangesinslopetooccur)werepositioned,accordingtothebestfittothedata.
Abbreviations:GCIP=ganglioncell+innerplexiform layer;INL=innernuclearlayer;OPL=outerplexiformlayer;ONL=outernuclearlayer;PRL=photoreceptorlayer
6/9/2014
7
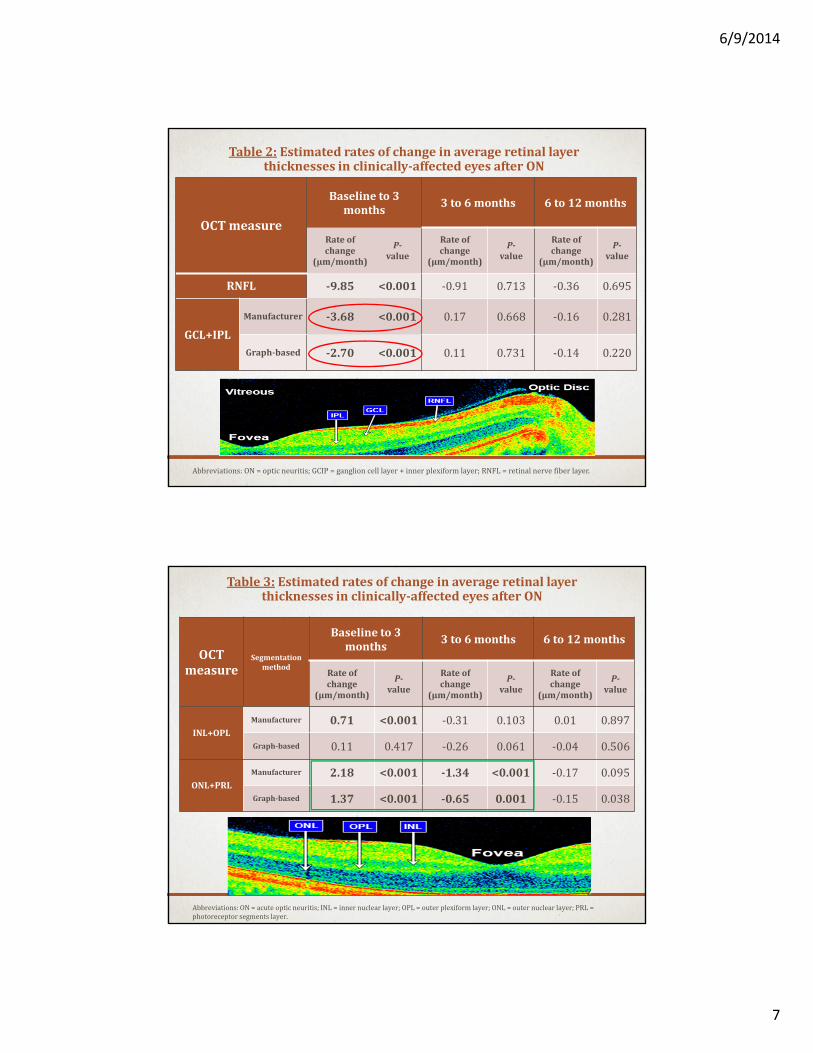
Table2: Estimatedratesofchangeinaverageretinallayerthicknessesinclinically‐affectedeyesafterON
OCTmeasure
Baselineto3months
3to6months 6to12months
Rateofchange
(µm/month)
P‐value
Rateofchange
(µm/month)
P‐value
Rateofchange
(µm/month)
P‐value
RNFL ‐9.85 <0.001 ‐0.91 0.713 ‐0.36 0.695
GCL+IPL
Manufacturer ‐3.68 <0.001 0.17 0.668 ‐0.16 0.281
Graph‐based ‐2.70 <0.001 0.11 0.731 ‐0.14 0.220
Abbreviations:ON=opticneuritis;GCIP=ganglioncelllayer+innerplexiformlayer;RNFL=retinalnervefiberlayer.
Table3: Estimatedratesofchangeinaverageretinallayerthicknessesinclinically‐affectedeyesafterON
OCTmeasure
Segmentationmethod
Baselineto3months
3to6months 6to12months
Rateofchange
(µm/month)
P‐value
Rateofchange
(µm/month)
P‐value
Rateofchange
(µm/month)
P‐value
INL+OPLManufacturer 0.71 <0.001 ‐0.31 0.103 0.01 0.897
Graph‐based 0.11 0.417 ‐0.26 0.061 ‐0.04 0.506
ONL+PRLManufacturer 2.18 <0.001 ‐1.34 <0.001 ‐0.17 0.095
Graph‐based 1.37 <0.001 ‐0.65 0.001 ‐0.15 0.038
Abbreviations:ON=acuteopticneuritis;INL=innernuclearlayer;OPL=outerplexiformlayer;ONL=outernuclearlayer;PRL=photoreceptorsegmentslayer.

6/9/2014
8
RelationshipbetweenGCIPlossandONLthickeningatthe4±1monthvisit
Takehomemessages• GanglioncelllayerthinningfollowingAONappearstobemostrapidintheearlymonths.
• OCTsegmentationdemonstratesatransientincreaseinONLthicknessthatappearstobeproportionaltothedegreeofGCIPlossinaffectedeyes.
• Thisraisesthepossibilityofbiologicaltrans‐synapticchangesoccurringinthedeepretinalneuronallayersandmayhelpusunderstandthecellularresponsetoinjuryinMS.

6/9/2014
9
Acknowledgements
JohnsHopkinsNeurology
• PeterA.Calabresi
• ShivSaidha
• PavanBhargava
• ScottNewsome
JohnsHopkinsElectricalandComputerEngineering
• JerryPrince
• AndrewLang
• AaronCarass
JohnsHopkinsBiostatisticsdepartment:
• Ciprian Crainiceanu
Funding:
• NIHgrant:5R01NS082347‐02
• RacetoEraseMS





























