Embed Size (px)
Citation preview

Cancer Therapy: Preclinical
In Vitro Sensitivity of CLL Cells to Fludarabine May BeModulated by the Stimulation of Toll-like Receptors
Eleonora Fonte1,4, Benedetta Apollonio1,2, Lydia Scarf�o1,2,3, Pamela Ranghetti1, Claudia Fazi1, Paolo Ghia1,2,3,Federico Caligaris-Cappio1,2,3, and Marta Muzio1
AbstractPurpose: The emerging role of Toll-like receptors (TLR) in the pathogenesis of chronic lymphocytic
leukemia (CLL) led us to ask whether TLR stimulation may protect CLL cells from drug-induced apoptosis.
Experimental Design:We cultured in vitromalignant B cells freshly isolated from 44 patients with CLLs
in the presence or the absence of different concentrations of fludarabine before or after 24-hour TLR
stimulation with specific ligands and evaluated cell viability, apoptosis, and molecular pathways involved.
Results: Heterogeneity was observed among samples. In leukemic cells from patients bearing adverse
prognostic factors, TLR stimulation caused a significant increase of protection to fludarabine treatment,
whereas this did not occur in the cells from patients with good prognosis. To identify novel molecular
mechanisms accounting for thedichotomyof response between the two groupsof patients,we conducted an
apoptosis gene expression profile on leukemic cells either unstimulated or stimulated with TLR9 ligand.
Strikingly, TLR9 stimulation specifically upregulated the expression of lymphotoxin-a in cells where an
increased protection to fludarabine treatment was observed. Also, the expression of miR-155-3p was
significantly increased after stimulation of distinct TLR in cells where fludarabine treatment was less
effective.
Conclusions: These results suggest that at least in a proportion of patients, in vitro sensitivity to
fludarabine may be modulated by the stimulation of TLR, likely mimicking microenvironmental signals
occurring in vivo. Clin Cancer Res; 19(2); 1–13. �2012 AACR.
IntroductionChronic lymphocytic leukemia (CLL) is heterogeneous in
its clinical course. Some patients have an indolent disease,whereas others have an aggressive clinical outcome. Poorprognosis patients tend to express negative prognostic fac-tors including the expression of ZAP70 or CD38, the pres-ence of deleterious cytogenetic abnormalities (17p and/or11q deletion), and the absence of somatic mutations in theimmunoglobulin heavy chain variable (IGHV) genes (1).Despite significant progress in the treatment modalities,CLL remains incurable, and drug resistance is a major causeof treatment failure. Resistance to purine analogues is a
challenging issue in clinical practice; patients who are orbecome refractory to fludarabine-based regimens have lowresponse rates to salvage therapy and poor survival (2, 3). Inmany instances, such resistance is associated with the pres-ence of 17p deletions and/or p53 mutations (4–6); morerecently, distinct mutations in SF3B1 splicing factor orBIRC3 signaling molecules were associated with fludara-bine refractoriness (7, 8). Nevertheless, other so farunknown biologic factors may contribute, an examplebeing CD40-induced chemoresistance (9, 10). Within thiscontext, we concentratedour attentionuponToll-like recep-tors (TLR). TLR are key players in host defense from infec-tion; they recognize a set of different molecular patternsfound inmicrobial components or autoantigens and, uponstimulation trigger NF-kB signaling pathway, induce theproduction of inflammatory cytokines and the expressionof costimulatory molecules (11, 12).
Previous reports (mainly focused onto TLR9) showedthat CpG immunostimulatory oligonucleotides induce pro-liferation, cytokine production, and shape an immunogen-ic phenotype in CLL cells (13, 14). However, it was alsoreported that TLR9 signaling by CpG-B oligonucleotidesinduces an apoptotic pathway in CLLs (15, 16). Further-more, several groups described a heterogeneous response toTLR9 stimulation in terms of proliferation and apoptosiswithin different groups of patients (15, 17); in detail, it wasreported that CpG induced apoptosis in mutated and
Authors' Affiliations: 1San Raffaele Scientific Institute, Division of Molec-ular Oncology; 2Universit�a Vita-Salute San Raffaele; 3San Raffaele Scien-tific Institute, Department of Onco-Hematology, Milano; and 4Universit�adegli Studi di Pavia, Pavia, Italy
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Authors: Federico Caligaris-Cappio, Universit�a Vita-Salute San Raffaele, Via Olgettina 58, Milano 20132, Italy. Phone: 39-02-2643-2390; Fax: 39-02-2643-2408; E-mail: [email protected];and Marta Muzio, San Raffaele Scientific Institute, Via Olgettina 58, Milano20132, Italy. Phone: 39-02-2643-4969; Fax: 39-02-2643-2408; E-mail:[email protected]
doi: 10.1158/1078-0432.CCR-12-1922
�2012 American Association for Cancer Research.
ClinicalCancer
Research
www.aacrjournals.org OF1
Research. on April 28, 2021. © 2012 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2012; DOI: 10.1158/1078-0432.CCR-12-1922

proliferation in unmutated patient samples (18, 19). Thesecomplex results indicate that additional molecular charac-terization of the functional role of different TLR recognizingdifferent microbial components is needed. We recentlyshowed that TLR1/2 and TLR2/6 heterodimers can activateand protect leukemic cells from spontaneous apoptosis invitro (20, 21). Again, heterogeneity was observed betweenpatients samples and apoptosis induction was reported in aproportion of cases (15); nevertheless, we recently showedthat distinct innate immunity pathways can be activated insubgroups of CLL with distinct immunoglobulin receptors(21).
In addition,we reported that inmousemodels, the lackofthe inhibitory receptor TIR8, which allows an unabatedTLR-mediated stimulation, triggers CLL progression in vivo(22). Considering the potential role of TLR in CLL naturalhistory, we here tested the hypothesis that signals throughthe TLR might also have a role in the regulation of drugresistance in CLLs. To this end, we treated freshly isolatedleukemic cells with fludarabine before and after TLR trig-gering in vitro and we dissected the molecular pathwaysinvolved.
Materials and MethodsReagents
Antibodies used for Western blot analysis were Bcl-2(Millipore),Mcl-1 (Santa Cruz), PARP (Cell Signaling Tech-nology), Bcl-xL (Cell Signaling Technology), XIAP (CellSignaling Technology), LTA/TNF-b (Genetex), cleaved cas-pase-3 (Cell Signaling Technology), and anti-b-Actin horse-radish peroxidase (HRP)-conjugated (Sigma). Reagentsused for flow cytometry were anti-LTA/TNF-b Fluorescein(R&D systems), AnnexinV-FITC, and propidium iodide-PE(PI-PE) (BenderMed System). For intracellular flow cyto-metric analysis of LTA/TNF-b, cells were treated with Bre-
feldin for 4 hours, stained with anti-LTA/TNF-b, and ana-lyzed. Concentrations of TLR ligands were chosen as pre-viously published, as following manufacturer’s indications(20). In details, Pam3CysSerLys4 (Pam3CSK4; Invivogen),a synthetic tripalmitoylated lipopeptide specific for TLR1/TLR2 heterodimer, was used at the concentration of 1 mg/mL. Macrophage-activating lipopeptide-2 (MALP-2; AxxoraPlatform), a specific ligand for TLR2/TLR6heterodimer,wasused at the concentration of 0.2 mg/mL. CpG oligonucleo-tide type B-Human (ODN 2006; Invivogen), a specificligand for TLR9, was used at the concentration of 2.5 mg/mL. Human recombinant TNF-b (Peprotech), was used atthe concentration of 10 ng/mL. Fludarabine (fludarabinephosphate) was from TEVA.
Tissue samples and cell purificationLeukemic lymphocytes were obtained from peripheral
blood of patients with CLLs diagnosed according to therecent IWCLL/NCI guidelines (23) and analyzed in dif-ferent experiments. In parallel, the following parameterswere analyzed for each patient: age, sex, disease stage atdiagnosis, CD38 expression, IGHV gene mutational sta-tus, and ZAP70 expression. Patients included into thisstudy were representative of the whole cohort aboutthe distribution of parameters listed in SupplementaryTable S1.
All patientswere either untreated or off therapy for at least6 months before the study.
Leukemic cells were negatively purified using a B-cell-enrichment kit (RosetteSep; StemCell Technologies) fol-lowing manufacturer’s instructions and/or MACS-mbeadsfor negative selection (Miltenyi Biotec). Purity of all CD19þ
CD5þ preparations was always more than 98% as checkedby flow cytometry (FC500; BeckmanCoulter). Preparationswere virtually devoid of natural killer (NK), T lymphocytes,and monocytes.
All tissue samples were obtained with the approval of theInstitutional Ethics Committee of San Raffaele ScientificInstitute (Milan, Italy), after informed consent.
Cell culture and analysisPurified leukemic cellswere cultured inRPMI-1640medi-
um supplemented with 10%heat-inactivated FBS, 2mmol/L L-glutamine, and 15 mg/mL gentamicin (Euroclone) at aconcentration of 3 � 106 cells/mL. Cells were either leftunstimulated or stimulated with TLR ligands for 24 hours;we then added increasing concentrations of fludarabine (10nmol/L–10 mmol/L) for additional 24 to 48 hours (withoutremoving the TLR ligands). At each time point, cells werecollected and analyzed for viability by using CellTiter-GloLuminescent Cell Viability Assay as according to manufac-turer’s protocol (Promega); the assay determines the relativenumber of viable cells in culture based on quantitation ofthe ATP present. Samples with a difference in cellularviability more than 10% were considered "resistant." Apo-ptosis induction was measured by AnnexinV/PI stainingand flow cytometric analysis (Cytomics FC500 Series FlowCytometry System, Beckman Coulter).
Translational RelevanceDespite significant progress in the treatment modal-
ities, chronic lymphocytic leukemia (CLL) remainsincurable, and drug resistance is a major cause of treat-ment failure. Genetic defects as well as microenviron-mental interactions concur to the development of drugresistance. Considering the potential role of Toll-likereceptors (TLR) in the natural history of the disease, theauthors tested the hypothesis that signals through theTLRmight also have a role in inducing drug resistance inleukemic cells. This study shows that distinct TLR ligandsinduce, at least in a proportion of patients, a uniqueantiapoptotic program that eventually leads to protec-tion of leukemic cells from fludarabine-induced apopto-sis and that ismarked by upregulation of lymphotoxin-aand miR-155-3p. Therefore, these molecules could beexploited as novel potential biomarkers of fludarabineresistance to be validated in future studies involving largecohorts of refractory patients.
Fonte et al.
Clin Cancer Res; 19(2) January 15, 2013 Clinical Cancer ResearchOF2
Research. on April 28, 2021. © 2012 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2012; DOI: 10.1158/1078-0432.CCR-12-1922

Western blot analysisTotal cell lysates were resolved by SDS-PAGE, and pro-
teins from gel were electron-transferred onto nitrocellulosemembranes and incubated overnight at 4�C with indicatedantibodies. Immunoreactivity was revealed by incubationwith HRP-anti-rabbit Ig or HRP-anti-mouse Ig (GE-Health-care), followed by ECL reaction (Pierce) and film exposures.
Gene expression profilingAfter 24-hour culture, cells stimulated or not with CpG
were collected, washed twice with PBS, and total cellularRNA was isolated with Qiagen RNAeasy mini kit (Qiagen).One microgram of RNA was reversed transcribed to cDNAusing the RT2 First Strand Kit (SABiosciences). Gene expres-sion profiling of the apoptosis pathway in stimulated andunstimulated CLL cells was conducted by real-time quan-titative PCR using the Human Apoptosis RT2 Profiler PCRArray kit (PAHS-012A, SABiosciences) according to manu-facturer’s instructions. The Human Apoptosis Array profilesthe expression of 84 key genes involved in programmed celldeath. The array consists of a panel of 96primer sets used forthe amplification of 84 genes relevant to the apoptosispathway (Supplementary Table S2) plus 5 housekeepinggenes (B2M,HPRT1, RPL13A,GAPDH, and ACTB), a gDNAcontrol, 3 reverse transcription, and 3 PCR quality controls.Data were obtained as threshold cycle (Ct) values. Thethreshold value was set at 0.01 for all experiments. Accord-ing to themanufacturer’s instructions,Ct values greater than35 were indicative of no expression and further consideredequal to 35 for mathematical reasons. The differencebetween the Ct value of each gene of interest (GOI), andthe average Ct value of housekeeping genes in each sample(DCt) was then measured. Fold differences (FD) in geneexpression between different subgroups of patients were
measured by the 2�DDCt algorithm (24). The difference inexpression of a certain gene between 2 subgroups was
reported only if: (i) the fold difference in average 2�DDCt
values was >4 or <�4 (indicative of up- or downregulation,
respectively); and (ii) the difference in 2�DCt values wasfound statistically significant (P <0.05) by the t testmethod.In addition, multiple comparisons analysis was conducted(ANOVA and Bonferroni test).
Real-time PCRRNA was purified and the reverse transcription was con-
ducted as previously described (see above, gene expressionprofiling). Expression of LT-a (TNF-b) mRNAwas analyzedby using a specific TaqMan gene expression assay (AppliedBiosystems). The experiments were carried out in triplicate,and they were normalized with glyceraldehyde-3-phos-phate dehydrogenase (GAPDH) expression for each condi-
tion. Data are expressed as relative expression (2�DCt).
miRNA expressionRNA was purified by TRIzol. Reverse transcription and
real-time PCR for mature microRNA were carried out byusing hsa-miR-155-3p TaqMan MicroRNA assay (AppliedBiosystems). The results are the average of triplicate, data
were normalized on the expression of RNU6B and
expressed as relative expression (2�DCt).
ELISASupernatants were collected after 24 hours of TLR stim-
ulation, and the amount of soluble LT-a (TNF-b) cytokinewas quantified by using a specific ELISA assay following themanufacturer’s instructions (Human TNF beta ELISA,eBioscience).
Statistical analysisThe datasets of viability, apoptosis, activation, and PCR
were analyzedwith aWilcoxonmatched pairs test orMann–Whitney unpaired test or Spearman correlation analysis orStudent t test or Dunnett multiple comparison test asindicated (GraphPad Prism 5.01 software).
All statistical computations on clinical data were doneusing GraphPad Prism 5.01 software. All P values were 2-sided and were regarded as statistically significant if <0.05.
ResultsTLR prestimulation modulates viability of CLL cellstreated with fludarabine
To test the hypothesis that TLR stimulation might affectfludarabine sensitivity, we cultured in vitro fresh purifiedleukemic cells isolated from an unselected group of 44patients withCLL (Supplementary Table S1) in the presenceor the absence of distinct TLR ligands (Pam3CSK4 for TLR1/2, MALP-2 for TLR2/6, or CpGODN2006 for TLR9). Twen-ty-four hours later, cells were either left untreated or treatedwith fludarabine at increasing concentrations (withoutremoving TLR ligands), incubated for additional 24 hours,and analyzed with a specific chemiluminescent assay tomeasure relative viability (Fig. 1A for a representative exper-iment). As expected, after 48 hours of in vitro culture,untreated samples showed a heterogeneous index of via-bility (Supplementary Fig. S2A–S2C). At cohort level, rel-ative viability increased afterMALP andCpG treatment (Fig.1B and Supplementary Fig. S1A–S1C). For each conditionof drug exposition (1, 3, and 10 mmol/L fludarabine), therelative viability of CLL cells as compared with untreatedcells was calculated after fludarabine treatment with orwithout TLR prestimulation. As shown in Fig. 1B, all theTLR ligands analyzed increased relative viability of CLL cellsat cohort level. TLR9 stimulation emerged as inducingsignificant protective effect in all the conditions tested(Supplementary Fig. S1). Time course analysis showed thata single TLR9 prestimulation protected cells up to 48 hours,irrespective of the concentrations of fludarabine tested; asshown in Fig. 1C and Supplementary Fig. S1D and S1E,whereas untreated cells were virtually all dead after longfludarabine treatment, TLR-stimulated samples contained asignificant proportion of viable cells.
TLR stimulation induces fludarabine protection in aproportion of CLL cases
Response heterogeneity was observed between samples(Supplementary Fig. S2A and S2B); specifically, in 29 of 44
TLR Protects CLL Cells from Fludarabine-Induced Apoptosis
www.aacrjournals.org Clin Cancer Res; 19(2) January 15, 2013 OF3
Research. on April 28, 2021. © 2012 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2012; DOI: 10.1158/1078-0432.CCR-12-1922

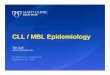
Figure1. Pam3CSK4,MALP-2. andCpGprestimulation induces fludarabine resistance inCLLcells. A, a representative experiment is reported (Pt 4); CLL cells,prestimulated for 24 hours with specific TLR ligands (Pam3CSK4 for TLR1/2, MALP-2 for TLR2/6, and CpG ODN2006 for TLR9), are protected from deathinduced by treatment with increasing fludarabine concentrations. Mean � SD of technical triplicate is reported. B, Wilcoxon matched pairs testconfirms the statistically significant TLR-induced resistance effect at a cohort level (44 patients with CLL analyzed for CpG, 33 for MALP-2, and 29 forPam3CSK4; 3 mmol/L fludarabine). Mean CLL cells viability � SEM is reported for 1, 3, or 10 mmol/L fludarabine treatment as indicated. C, theprotective effect of TLR prestimulation was maintained after 48-hour treatment with fludarabine (10 patients were analyzed for all the ligands, namely:1, 2, 4, 6, 9, 10, 13, 19, 33, 39). Mean CLL cells viability � SEM is reported for 3 or 10 mmol/L fludarabine treatment as indicated. D, patients with acellular viability increase more than 10% after CpG stimulation are arbitrarily considered as "resistant," whereas patients with a cellular viability increase lessthan 10% after CpG stimulation are considered "sensitive." E, relative viability was calculated for each sample in fludarabine-treated versus untreatedcells. Fold change was calculated for each sample as follows: Fold change CTRL ¼ (relative viability with fludarabine)/(relative viability without fludarabine).Fold change CpG ¼ (relative viability with CpG and fludarabine)/(relative viability with CpG and without fludarabine). CTRL indicates sampleswithout TLR addition; PAM-3, MALP-2, and CpG indicate samples with the addition of TLR ligands. A total of 23 "resistant" samples were analyzed forPAM-3, 23 for MALP-2, and 29 for CpG (patient number 1–29); mean fold change � SEM is reported in the graph. F–H, Spearman correlation analysisof TLR-induced cell viability differences of samples treated with 3 mmol/L fludarabine. F, CpG versus Pam3CSK4. G, CpG versus MALP. H, Pam3CSK4versus MALP (P < 0.0001 for all panels). �, P < 0.05; ��, P < 0.01; ���, P < 0.001.
Fonte et al.
Clin Cancer Res; 19(2) January 15, 2013 Clinical Cancer ResearchOF4
Research. on April 28, 2021. © 2012 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2012; DOI: 10.1158/1078-0432.CCR-12-1922

cases analyzed, TLR stimulation induced a robust protectiveeffect, as determinedby aTLR9-mediated increase of relativecellular viability 10% or more as compared with untreatedcells (mean percentage of viable cells was 37.1 � 18.8 forcontrol and 110.1� 52,1 for CpG; 3 mmol/L fludarabine for24 hours after TLR prestimulation for 24 hours). In theremaining 15 patients with CLLs, the effect of TLR was lessthan 10% (n ¼ 6) or negative (n ¼ 9; mean percentage ofviable cells was 31.6� 17.6 for control and 26.6� 19.7 forCpG; Supplementary Table S1). For clarity purposes, sam-ples with a cellular viability increase more than 10% afterCpG stimulation will be defined as "resistant," whereassamples with a cellular viability increase less than 10% afterCpG stimulation will be considered "sensitive" (Fig. 1D fora schematic representation).To further evaluate the intrinsic sensitivity of CLL cells to
fludarabine before and after TLR stimulation and to analyzewhether the observed effects are specific for that stimulationand are independent of the cell viability without treatment,a fold changewas calculated for each sample. In details, foldchange of control "resistant" sample was calculated as(relative viability with fludarabine)/(relative viability with-out fludarabine); fold change for TLR-treated "resistant"samples was calculated as (relative viability with TLR ligandand fludarabine)/(relative viability with TLR ligand andwithout fludarabine).At 3 mmol/L of fludarabine treatment (24 hours of TLR
prestimulation and 24 hours of fludarabine), unstimulatedcells showed a significantly lower mean ratio of viabilitythan TLR-stimulated cells (Fig. 1E).Moreover, analysis of spontaneous cellular viability index
showed no significant difference between the "resistant"and the "sensitive" group (Supplementary Fig. S2C andS2D). Therefore, triggering TLR on leukemic cells induced,in a proportion of cases, intrinsic fludarabine resistance.The response to TLR stimulation in terms of relative
viability of the cells was heterogeneous among the patients;that notwithstanding, significant associations were notedbetween the pattern of response (in terms of protectiveeffect) after stimulation with the different ligands. Dataanalysis showed that the differences in viability of CLL cellsstimulated with CpG correlated with the differences inviability of cells stimulated with Pam3CSK4 (Fig. 1F);similarly, CpG and MALP-2 or MALP-2 and Pam3CSK4significantly correlated (Fig. 1G and H, respectively).
TLR stimulation preferentially protects cells frompatients with adverse prognostic factorsGiven the observed response heterogeneity among
patients (Supplementary Table S1), we asked whetherpatients with different clinical course and prognostic factorsmight have a differential response to CpG in terms ofprotection from fludarabine treatment (24 hours of TLRprestimulation and 24 hours of fludarabine; Fig. 2A–E). Weobserved a significant difference in the change of cell via-bility after treatment with CpG in samples with: (i) stableversus progressive disease (Fig. 2A); (ii) low Rai stage versusintermediate Rai stage (ref. 25; Fig. 2B), (iii) mutated versus
unmutated IGHV genes (Fig. 2C); (iv) >30% CD38 versus<30% CD38 positive cells (Fig. 2D); (v) favorable (13qdeletion and/or trisomy 12 or normal FISH karyotype)versus unfavorable (17p deletion and/or 11q deletion)cytogenetic aberrations (Fig. 2E and Supplementary Fig.S1). Leukemic cells from patients with adverse prognosticfactors (unmutated IGHV genes and/or CD38-positive and/or unfavorable cytogenetic carriers) had significantly highercell viability increase after TLR stimulation than those withfavorable prognosis (mutated IGHV genes and/or CD38-negative and/or favorable cytogenetic carriers). Overall,these data show that the functional in vitro response to CpGand fludarabine reflects a different clinical behavior inpatients with CLLs.
TLR stimulation protects CLL cells from fludarabine-induced apoptosis
To understand the mechanism of the observed TLR-induced protection from fludarabine treatment, we calcu-lated the percentage of viable, apoptotic, and necrotic cellsafter incubation of CLL cells with different concentration offludarabine (3 and 10 mmol/L). Thirteen patients wereanalyzed for the response to Pam3CSK4 (TLR1/2), 17 forthe response to MALP-2 (TLR2/6), and 22 for the responseto CpGODN2006 (TLR9). As expected from previous workfrom different groups including ours, heterogeneousresponse was observed after treatment of the cells withdifferent TLR ligands for 3 days; overall, at cohort level, nosignificant differences were observed at this time point (Fig.3A; ref. 21). As depicted in Fig. 3A, at cohort levels, thepercentage of viable, nonapoptotic cells significantlyincreased when cells were pretreated with TLR2/6 and TLR9ligands and following treated with increasing concentra-tions of fludarabine. In details, mean percentage value ofAnnexinV�PI� cells was 17.18� 16.01 (SD) for control and33.43� 28.2 for CpG at a dose of 3 mmol/L fludarabine and13.4� 11.7 for control and 32.9� 26.2 for CpG at a dose of10 mmol/L fludarabine. In the same experiments, similarresults were obtained with TLR2/6 ligand (mean percentagevalue of AnnexinV�PI� cellswas 24.6�21.64 forMALP-2 ata dose of 3 mmol/L fludarabine and 22.4� 13.6 at a dose of10 mmol/L fludarabine) and with TLR1/2 ligand (meanpercentage value of AnnexinV�PI� cells was 27.4 � 17.4for Pam3CSK4 at a dose of 3mmol/L fludarabine and 20.5�11.7 for Pam3CSK4 at a dose of 10 mmol/L fludarabine).
If we consider the group of "resistant" samples only (Fig.3B), a highly significant difference was observed betweenunstimulated and TLR-stimulated samples before and afterfludarabine treatment (see Fig. 3C for a representativeexperiment). To investigate whether the effects observedafter treatment with fludarabine/TLR stimulation are spe-cific for that stimulation and are independent of the spon-taneous cell apoptosis, we calculated the percentage ofapoptotic cells (without any treatment) in both the "resis-tant" and the "sensitive" samples, and we observed nosignificant difference between the 2 groups (SupplementaryFig. S2D). These findings are in line with the resultsobtained with the viability assay (Fig. 1) and suggest that
TLR Protects CLL Cells from Fludarabine-Induced Apoptosis
www.aacrjournals.org Clin Cancer Res; 19(2) January 15, 2013 OF5
Research. on April 28, 2021. © 2012 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2012; DOI: 10.1158/1078-0432.CCR-12-1922

TLR stimulation specifically protected CLL cells from flu-darabine-induced apoptosis. This possibility was confirmedby Western blot analysis which showed that TLR ligationprevented the apoptotic cleavage of PARP and caspase-3(Fig. 3D). Of note, the TLR-mediated antiapoptotic activitywas evident only in combination with fludarabine furthersupporting the concept of TLR-induced protection.
TLR stimulation upregulates activation and anti-apoptoticmolecules in both "sensitive" and "resistant"samples
To investigate the molecular mechanisms on the basis ofthe observed heterogeneity between patients, we askedwhether it was reflected by a differential TLR-mediatedcellular activation. We analyzed expression of CD86 andCD25 activation molecules before and after TLR1/2, TLR2/6, and TLR9 stimulation in both the "resistant" and the"sensitive" group; we observed no significant difference
between the 2 groups of patients analyzed; nevertheless,a trend of lower activation in the "sensitive" group wasreported (Fig. 4A and B for CD25 and CD86, respectively).
Next, we analyzed by Western blotting, the expression ofkey antiapoptotic proteins known to play an important rolein CLL such as Mcl-1, XIAP, Bcl-2, and Bcl-xL. As expected(26, 27), CLL cells expressed high basal levels of Bcl-2; nofurther evident increase of the corresponding bandwas observed after TLR stimulation. XIAP protein band wasonly modulated by fludarabine and CpG treatment. Bandscorresponding to Mcl-1 and Bcl-xL antiapoptotic moleculeswere not evident in untreated samples while becomingstrongly evident after TLR stimulation in all cases analyzed(n¼ 11 and n¼ 5, respectively), including both "resistant"and "sensitive" samples (Fig. 4C and D, respectively).Importantly, the increased levels of Mcl-1 and Bcl-xL weremaintained also after treatment of leukemic cells with highdoses of fludarabine (10 mmol/L; Fig. 4C and D).
Figure 2. Different TLR-inducedviability of the cells according to themain prognostic factors andclinical outcome (24 hours of TLRprestimulation and 24 hours offludarabine). A, higher cellularviability increase in patients withprogressive clinical course versusstable patients. B, higher cellularviability increase after CpGstimulation in patients classified asintermediate stage at diagnosisaccording to the revised Raistaging system. C, the cellularviability increase after CpGstimulation is significantly higher inpatients with unmutated IGHVgenes in comparison with mutatedIGHV genes. D, CD38-positive(�30% expression) subjects had ahigher cellular viability increaseafter CpG stimulation incomparison with CD38-negative(<30%) patients. E, patients withunfavorable cytogeneticaberrations (del11q and/or del17p)showed a higher cellular viabilityincrease after CpGstimulation thansubjectswith a favorable (del13q orand/or trisomy 12 or normal)cytogenetic profile.
Fonte et al.
Clin Cancer Res; 19(2) January 15, 2013 Clinical Cancer ResearchOF6
Research. on April 28, 2021. © 2012 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2012; DOI: 10.1158/1078-0432.CCR-12-1922

To examine whether TLR engagement affected themRNAexpression levels of additional genes specifically involved inthe apoptotic process, we studied a large number of genesusing a specific gene expression array (see SupplementaryTable S2 for a complete gene list). Cells were cultured for 24hours in the presence or the absence of CpG (TLR9 ligand);
gene expression analysis was conducted in leukemic cellsisolated from 4 "resistant" CLL samples. The data showedthat 3 geneswere upregulated (>4-folddifference; LTA/TNF-b, NOL3, CD40) and 3 genes were downregulated (<4-folddifference; PYCARD, CD27, TNFSF10; Fig. 4E). However,only LTA, CD40, and CD27 upregulations are statistically
Figure 3. TLRs protect CLL cellsfrom fludarabine-induced apoptosis.A, CLL cells prestimulated withPam3CSK4, MALP-2, and CpGODN2006 for 24 hours and followingtreated with 3 or 10 mmol/L offludarabine for additional 48 hours(14 patients were analyzed forPam3CSK4 and 18 for MALP-2 and19 for CpG, namely patients number1, 2, 6, 9, 10, 13, 14, 15, 16, 17, 19, 20,30, 33, 37, 39). Mean percentage �SEM of viable cells is reported.Wilcoxon matched pairs test wasconducted. B, resistant sampleswere analyzed as in A. Elevenpatients were analyzed forPam3CSK4 and 13 for MALP-2 and14 for CpG.Mean percentage�SEMof viable cells is reported. C, arepresentative example of AnnexinV/PI staining of CLL cells eitheruntreated or treated for 48 hours with3 and 10 mmol/L of fludarabine,before and after 24-hour TLRstimulation (Pt 2). D, Western blotanalysis of the apoptotic cleavage ofPARP and caspase-3 confirms theprotective effect of the TLR ligandson fludarabine-induced apoptosis.Two representative examples (n ¼ 6for PARP and n ¼ 3 for caspase-3)are shown. Relative optical density(OD) of each band is indicated at thebottom of the panel; the ratio of theOD of protein of interest and the ODof b-actin was calculated for eachsample. �, P < 0.05; ��, P < 0.01.
TLR Protects CLL Cells from Fludarabine-Induced Apoptosis
www.aacrjournals.org Clin Cancer Res; 19(2) January 15, 2013 OF7
Research. on April 28, 2021. © 2012 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2012; DOI: 10.1158/1078-0432.CCR-12-1922

significant after applying correction test for multiple com-parisons (ANOVA and Bonferroni test).
TLRs selectively upregulate LTA/TNF-b in "resistant"samples
We were particularly intrigued by the important upregu-lation of LTA/TNF-b (>20-fold regulation), and we set up areal-time PCR analysis that revealed significant upregula-tion of LTA/TNF-b mRNA after CpG treatment (Fig. 5A).
Interestingly, a trend for lower expression of LTA/TNF-bmRNAwas apparent, after CpG treatment, in the "sensitive"group as compared with the "resistant" group (Fig. 5B).
Next, we conducted Western blot analysis to detect LTA/TNF-b protein which was evident only in the "resistant"samples (Fig. 5C). Intracellular staining andflowcytometricanalysis of leukemic cells (CD5þCD19þ) allowed to iden-tify CLL cells as the cells of origin of LTA/TNF-b (Fig. 5D andE). Finally, we measured, by specific ELISA assay, the
Figure 4. TLRs upregulate severalactivation molecules andantiapoptotic molecules in CLLcells. A and B, TLR-inducedactivation in CLL cells upon 24hours of stimulation was analyzedby flow cytometric analysis ofCD25þ- and CD86þ-positive cells(A and B, respectively). Mann–Whitney test was conducted tocompare "resistant" and "sensitivegroup"; no significant differencewas observed. C and D, Westernblot analysis of XIAP, Bcl-2, Bcl-xL,and Mcl-1 shows an increase ofBcl-xL and Mcl-1 in samplestreated with TLR ligands(2 representative experimentsare shown). C, "resistant"; D,"sensitive." b-Actin was used asinternal control. Relative OD ofeach band is indicated at thebottom of the panel; the ratio of theODof protein of interest and theODof b-actin was calculated for eachsample. E, real-timePCRarraywasconducted to evaluate the mRNAexpression levels of 84 genesregulating apoptosis (seeSupplementary Table S1 for thecomplete list of genes) in purifiedCLL cells (%CD19þ > 98%).Scatter plot shows data expressedas log10 2�DCt of control groupversus CpG-treated group andreveals modulation of severalgenes (fold regulation >4 or <4)between untreated and CpG-treated samples (n ¼ 4, patient1, 2, 10, 11). In the table, only genesthat were significantly up- ordownregulated are reported (t test);after multiple comparisonscorrection, only 3 genes remainedsignificantly up- or downregulated(shown in bold).
Fonte et al.
Clin Cancer Res; 19(2) January 15, 2013 Clinical Cancer ResearchOF8
Research. on April 28, 2021. © 2012 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2012; DOI: 10.1158/1078-0432.CCR-12-1922

amount of cytokine released by CpG-treated cells; as shownin Fig. 5F, CpG only significantly increased the productionand release of LTA/TNF-b by CLL cells. Remarkably, whenwe compared the total amount of LTA/TNF-b released, weobserved a significant differencebetween the "resistant" and"sensitive" samples (mean amount of LTA/TNF-b was 364and 160 pg/mL, respectively; Fig. 5G).As a proof of principle, we then pretreated leukemic
cells from 7 patients with LTA/TNF-b, and we observed amodest but significant increase of cellular viability (Sup-plementary Fig. S3A and S3B), and protection from apo-ptosis (Supplementary Fig. S3C and S3D); this effect wasspecific for "resistant" samples (Supplementary Fig. S3Band S3D), further supporting a specific role of LTA/TNF-b
in mediating CpG-induced resistance in a selected groupof patients.
TLR-induced protection fromfludarabine ismarked byupregulation of miR-155-3p
To analyze the molecular differences between the 2groups of patients and in an effort to explain the resistanceeffect induced by CpG, we analyzed the expression ofmicroRNA-155-3p. We chose this miRNA starting from theobservation that CpG was previously shown to upregulatemiR-155 in normal leukocytes (28–30); moreover, itwas shown that lack of bic/miR-155 in mouse modelsresulted in impaired production of lymphotoxin-a by Bcells (30). It was also recently shown that mature miR-155�
Figure 5. TLR-induced resistanceis accompanied by LTA/TNF-bupregulation. A, real-time PCRanalysis shows a significant increaseof LTA/TNF-b mRNA expressionlevels after 24 hours of CpGtreatment (n¼14;Wilcoxonmatchedpairs test); mean � min/max isreported. B, the relative expressionofLTA mRNA shows a trend of higherexpression in patients from the"resistant" group than in the"sensitive" group (Mann–Whitneytest); mean�min/max is reported. C,Western blot analysis for LTA/TNF-bof 2 representative "sensitive" and 2"resistant" patients (of 8 analyzed).CpG treatment induced increase inLTA/TNF-b protein levels only in therestricted group of "resistant"patients. �, P < 0.05; ��, P < 0.01;���, P < 0.001. D and E, flowcytometric analysis reveals theincrease of LTA/TNF-b–positive CLLcells (gated on CD5þ/CD19þ
leukemic cells); a representativeexperiment is shown in D. E,Wilcoxon matched pairs testconfirms the significant increase ofthe percentage of LTA/TNF-b–positive CLL cells (n ¼ 8); meanpercentage�min/max is reported. Fand G, ELISA assay was conductedto measure the concentration ofsoluble LTA released in thesupernatant upon 24 hours of in vitroculture with CpG and MALP-2. LTA/TNF-b is significantly increased uponCpG stimulation (Wilcoxon matchedpairs test; n¼ 20) but notMALP-2 (F);mean values � SEM are reported. G,total amount of CpG-induced LTAwas significantly lower in the"sensitive" group than in the"resistant" group (Mann–Whitneytest); mean values � min/max arereported.
TLR Protects CLL Cells from Fludarabine-Induced Apoptosis
www.aacrjournals.org Clin Cancer Res; 19(2) January 15, 2013 OF9
Research. on April 28, 2021. © 2012 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2012; DOI: 10.1158/1078-0432.CCR-12-1922

(miR-155-3p) is strikingly upregulated byCpG treatment ofCLL cells with unmutated IGHV (31). We asked whetherCpG could upregulate this microRNA in CLL cells beforeand after fludarabine treatment. CpG, and to a lesser extentMALP-2, significantly increased miR-155-3p expressionlevels (Fig. 6A); higher levels of miR-155-3p were main-tained also in the presence of fludarabine (Fig. 6C). Strik-ingly, higher levels of CpG-induced miR-155-3p werepresent in the "resistant" samples as compared with the"sensitive" samples (Fig. 6B) and this differencewas evidentalso in the presence of fludarabine (Fig. 6D).
DiscussionSpecific combination of cell types and soluble factors
present in microenvironment niches protect CLL cells fromcell death. Microenvironmental interactions also influencedrug resistance, an example being CD40-induced chemore-sistance which is mediated by NF-kB activation andincreased levels of Bcl-xL and Mcl-1 (32, 33). In this work,we tested the hypothesis that TLR triggering may influencedrug resistance of CLL cells. Our results suggest that reducedsensitivity to fludarabine treatmentmay be ascribed, at leastin a proportion of patients, to the stimulation operated bymicroenvironment TLR ligands.
Recent reports have shown that distinct TLR may act asmodulators of chemoresistance in solid tumors. TLR7 andTLR8 triggering induce cell survival and resistance to dif-ferent drugs in human lung cancer cells (34), and TLR4signaling promotes tumor growth and paclitaxel resistancein ovarian cancer (35).
In our study, several parameters were analyzed includingactivation, cell viability, and apoptosis. At cohort level,despite a heterogeneous response, we observed a generalprotective effect to fludarabine treatment when CLL cellswere prestimulatedwith TLR1/2, TLR2/6, and TLR9 ligands.Interestingly, patients with progressive disease and bearingdifferent unfavorable prognosis markers (unmutated IGHVgenes, surface CD38, cytogenetic abnormalities) were sig-nificantly enriched for those in whom TLR stimulation ledto protection from drug activity. In line with these observa-tions, different studies showed that CpG induces prolifer-ation mainly in CLL B cells from patients with progressivedisease and unmutated IGHV genes, whereas cell-cyclearrest and apoptosis are induced in leukemic B cells fromstable/IGHV-mutated CLL (15, 18, 19, 36), further support-ing a dichotomy of response between mutated and unmu-tated cases. Importantly, our study shows that a single TLRprestimulation (24 hours) was sufficient to trigger an anti-apoptotic program which resulted in drug protection inleukemic cells isolated from patients bearing adverse prog-nosis markers. Time course analysis showed that TLR9prestimulation (24 hours) protected cells up to 48 hourslater; however, prosurvival effect diminished overtime,suggesting that a "chronic stimulation" may be required tosustain the effect. Recently, it was reported that combinedCD40/TLR9 triggering differentially affects NF-kB signalingand chemoresistance. However, in vitro TLR9 prestimula-tion (for 3–5 days) did not protect cells nor augmented theCD40-mediated chemoprotective effect even in unmutatedCLL cases (19). This apparent discrepancy with our results
Figure 6. miR-155-3p induction byTLR stimulation. A, relative miR-155-3pexpressionafter 24hoursofMALP-2 and CpG stimulation.Real-time assay was conducted intriplicate and the RNA for U6 wasused as internal control (n ¼ 12 forMalp-2 and CpG; n ¼ 6 forPAM3CSK4); mean values � SEMare reported.B,Mann–Whitney testreveals higher levels of CpG-induced miR-155-3p in the"resistant" samples than in the"sensitive" samples (n ¼ 8 andn ¼ 4, respectively). C, CpGupregulates miR-155-3pexpression also at later time points(48 hours) and in the presence offludarabine (10 mmol/L; Wilcoxonmatched pairs test; n ¼ 4"resistant" samples analyzed)mean values � SEM are reported.D, comparison between "resistant"and "sensitive" samples stimulatedwith CpG and treated withfludarabine shows significantlyhigher levels of expression of miR-155-3p in the "resistant" group(Mann–Whitney test; n ¼ 4 andn ¼ 4, respectively). �, P < 0.05;��, P < 0.01; ���, P < 0.001.
Fonte et al.
Clin Cancer Res; 19(2) January 15, 2013 Clinical Cancer ResearchOF10
Research. on April 28, 2021. © 2012 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2012; DOI: 10.1158/1078-0432.CCR-12-1922

may be due to the different experimental conditions usedand kinetics. It will be interesting to analyze whether thecontinuous addition of TLR ligands (somehowmimicking achronic inflammatory and/or infectious condition) mayimpact on the kinetic of drug resistance.When we specifically analyzed apoptosis, we observed
that TLR ligation protected from drug-induced apoptosis;however, antiapoptotic effect was less significant than gen-eral cellular viability. As the viability assay is based on themeasurement of ATP concentration, these results suggestthat, in addition to apoptosis, either energy metabolismand/or proliferation may be regulated by TLR ligation aspreviously described (18, 36).We previously showed that TLR stimulation induces
activation of the NF-kB pathway as determined by phos-phorylation of IKK (20); we herein show the induction ofspecific antiapoptotic proteins including Bcl-xL and Mcl-1.In addition, the increase of antiapoptotic proteins wasmaintained also when cells were subsequently treated withfludarabine, thus supporting the hypothesis that TLR-induced Bcl-xL and Mcl-1 may participate in the observedfludarabine protection; however, as these molecules wereupregulated also in "sensitive" samples, we searched foradditional molecular mechanisms involved.Searching for novel molecules specifically modulated
by TLR and possibly involved into the observed protectiveeffect,we identified several genes up- ordownregulated afterCpG (TLR9 ligand) treatment in "resistant" samples. Dif-ferent TNF family members (LTA/TNF-b, CD40) and anti-apoptotic molecules (NOL3) were strikingly upregulated.TNF family members were described as key regulators of
CLL cell biology. LTA/TNF-b can support the proliferationof in vitro activated CLL cells (37, 38), suggesting that thispathway may also contribute to the observed TLR-inducedprotection from drug-induced cell death. Additional cyto-kines and antiapoptotic molecules may concur to the finalchemoresistance effect. Our observation that TLR stimula-tion increases CD40 transcripts suggests that this pathwaymay also play a relevant role in TLR-induced chemoresis-tance. NOL3 gene encodes an antiapoptotic protein thatinhibits the enzymatic activities of caspases and of tumorprotein p53.Among the genes specifically downregulated by CpG, we
detected distinct proapoptotic proteins including a proa-poptotic TNF receptor familymember (CD27; ref. 39) and aproapoptotic TNF familymember (TNFSF10 also known asTRAIL; ref. 40); and PYCARD is an adapter molecule reg-ulating inflammatory and apoptotic pathways (41).Overall, the gene expression analysis supports the
hypothesis that TLR induces a potent antiapoptotic tran-scriptional program in CLL cells. Therefore, it is tempting topropose LTA/TNF-b as novel potential biomarkers of flu-darabine resistance to be validated in future studies involv-ing large cohorts of refractory patients.miRNAs are an abundant class of small noncoding RNAs
that modulate the expression of target mRNAs at posttran-scriptional level. Many miRNAs have been shown to play arole in different tumors including CLLs. We previously
showed that the miR-221/222 cluster is upregulated in CLLcells by CpG treatment and modulates the expression ofp27KIP1 protein (42). Of note, miR-221 andmiR-222 wererecently shown to play a key role in chemoresistance of solidtumors (43) and to be upregulated in vivo in patients withCLLs refractory to fludarabine treatment (44). Our previousdata (42) suggest that the observed TLR-mediated drugresistance in CLL may also be influenced by upregulationof miR221/222 cluster.
In our current work, we focused our attention on miR-155, a key regulator of inflammation, immunity, and cancer(30, 45–47); miR-155 was previously shown to be upregu-lated by different TLR ligands in normal leukocytes (28–30)and to be highly expressed in CLLs (29, 45, 48). Recently, itwas also reported that CpG can induce several miRNAincluding miR-155/miR-155-5p and miR-155�/miR-155-3p in CLL cells with unmutated IGHV (31). Interestingly,it was reported that lymphotoxin-a production is impairedin bic/miR-155–deficient mice (30). Our novel data show-ing that CpG specifically induces miR-155-3p/miR155� in"resistant" CLL samples, either untreated or treated withfludarabine, suggest that a specific program of miRNAregulation may play a role also in lymphotoxin regulationand chemoresistance.
In conclusion, we show that specific TLR ligands induce,at least in a proportion of patients, a robust prosurvivalprogramwhich is marked by upregulation of lymphotoxin-a and miR-155-3p and eventually leads to protection ofleukemic cells from drug-induced cell death. Targeting TLRsignaling pathways by specific inhibitorsmight be suggestedas a novel therapeutic strategy to overcome fludarabinerefractoriness in CLLs.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: E. Fonte, M. MuzioDevelopment of methodology: E. Fonte, B. Apollonio, C. FaziAcquisitionofdata (provided animals, acquired andmanagedpatients,provided facilities, etc.): E. Fonte, L. Scarf�o, P. GhiaAnalysis and interpretation of data (e.g., statistical analysis, biosta-tistics, computational analysis): E. Fonte, L. Scarf�o, P. Ghia, F. Caligaris-Cappio, M. MuzioWriting, review, and/or revision of the manuscript: E. Fonte, P. Ghia, F.Caligaris-Cappio, M. MuzioAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): P. RanghettiStudy supervision: F. Caligaris-Cappio, M. Muzio
Grant SupportThis project was supported by: Leukemia Research Foundation (IL);
Cariplo Foundation (Milano, Italy); Program Molecular Clinical Oncolo-gy-5permille number 9965 and InvestigatorGrant, Associazione Italiana perla Ricerca sul Cancro (AIRC – Milano, Italy); U.S./European Alliance for theTherapy of CLL, CLLGlobal Research Foundation (TX); Progetti di RilevanzaNazionale (PRIN), Ministero dell’Istruzione, Universit�a e Ricerca (Roma,Italy); and Ricerca Finalizzata, Ministero della Salute (Roma, Italy).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received June 12, 2012; revisedOctober 29, 2012; acceptedNovember 27,2012; published OnlineFirst December 5, 2012.
TLR Protects CLL Cells from Fludarabine-Induced Apoptosis
www.aacrjournals.org Clin Cancer Res; 19(2) January 15, 2013 OF11
Research. on April 28, 2021. © 2012 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2012; DOI: 10.1158/1078-0432.CCR-12-1922

References1. Zenz T, Mertens D, Kuppers R, Dohner H, Stilgenbauer S. From
pathogenesis to treatment of chronic lymphocytic leukaemia. Nat RevCancer 2010;10:37–50.
2. KeatingMJ, O'Brien S, Kontoyiannis D, Plunkett W, Koller C, Beran M,et al. Results of first salvage therapy for patients refractory to afludarabine regimen in chronic lymphocytic leukemia. LeukLymphoma2002;43:1755–62.
3. Tam CS, O'Brien S, Lerner S, Khouri I, Ferrajoli A, Faderl S, et al. Thenatural history of fludarabine-refractory chronic lymphocytic leukemiapatients who fail alemtuzumab or have bulky lymphadenopathy. LeukLymphoma 2007;48:1931–9.
4. Catovsky D, Richards S, Matutes E, Oscier D, Dyer MJ, Bezares RF,et al. Assessment of fludarabine plus cyclophosphamide for patientswith chronic lymphocytic leukaemia (theLRFCLL4Trial): a randomisedcontrolled trial. Lancet 2007;370:230–9.
5. Grever MR, Lucas DM, Dewald GW, Neuberg DS, Reed JC, Kitada S,et al. Comprehensive assessment of genetic and molecular featurespredicting outcome in patients with chronic lymphocytic leukemia:results from the US Intergroup Phase III Trial E2997. J Clin Oncol2007;25:799–804.
6. Zenz T, Habe S, Denzel T, Mohr J, Winkler D, Buhler A, et al. Detailedanalysis of p53 pathway defects in fludarabine-refractory chroniclymphocytic leukemia (CLL): dissecting the contribution of 17p dele-tion, TP53 mutation, p53-p21 dysfunction, and miR34a in a prospec-tive clinical trial. Blood 2009;114:2589–97.
7. RossiD,BruscagginA,SpinaV,Rasi S,KhiabanianH,MessinaM, et al.Mutations of the SF3B1 splicing factor in chronic lymphocytic leuke-mia: association with progression and fludarabine-refractoriness.Blood 2011;118:6904–8.
8. Rossi D, Fangazio M, Rasi S, Vaisitti T, Monti S, Cresta S, et al.Disruption of BIRC3 associates with fludarabine chemorefractorinessin TP53 wild-type chronic lymphocytic leukemia. Blood 2012;119:2854–62.
9. RomanoMF, Lamberti A, Tassone P, Alfinito F, Costantini S, ChiurazziF, et al. Triggering of CD40 antigen inhibits fludarabine-inducedapoptosis in B chronic lymphocytic leukemia cells. Blood 1998;92:990–5.
10. Kitada S, Zapata JM, Andreeff M, Reed JC. Bryostatin and CD40-ligand enhance apoptosis resistance and induce expression of cellsurvival genes in B-cell chronic lymphocytic leukaemia. Br J Haematol1999;106:995–1004.
11. Kawai T, Akira S. Toll-like receptors and their crosstalk with otherinnate receptors in infection and immunity. Immunity 2011;34:637–50.
12. Lanzavecchia A, Sallusto F. Toll-like receptors and innate immunity inB-cell activation and antibody responses. Curr Opin Immunol 2007;19:268–74.
13. Decker T, Schneller F, Sparwasser T, Tretter T, Lipford GB, Wagner H,et al. Immunostimulatory CpG-oligonucleotides cause proliferation,cytokine production, and an immunogenic phenotype in chronic lym-phocytic leukemia B cells. Blood 2000;95:999–1006.
14. Jahrsdorfer B, Hartmann G, Racila E, Jackson W, Muhlenhoff L,Meinhardt G, et al. CpG DNA increases primary malignant B cellexpression of costimulatory molecules and target antigens. J LeukocBiol 2001;69:81–8.
15. Rozkova D, Novotna L, Pytlik R, Hochova I, Kozak T, Bartunkova J,et al. Toll-like receptors on B-CLL cells: expression and functionalconsequences of their stimulation. Int J Cancer 2010;126:1132–43.
16. Liang X, Moseman EA, Farrar MA, Bachanova V, Weisdorf DJ, BlazarBR, et al. Toll-like receptor 9 signaling by CpG-B oligodeoxynucleo-tides induces an apoptotic pathway in human chronic lymphocyticleukemia B cells. Blood 2010;115:5041–52.
17. Jahrsdorfer B, Jox R, Muhlenhoff L, Tschoep K, Krug A, RothenfusserS, et al. Modulation ofmalignant B cell activation and apoptosis by bcl-2 antisense ODN and immunostimulatory CpG ODN. J Leukoc Biol2002;72:83–92.
18. Longo PG, Laurenti L, Gobessi S, Petlickovski A, Pelosi M, ChiusoloP, et al. The Akt signaling pathway determines the different prolif-erative capacity of chronic lymphocytic leukemia B-cells from
patients with progressive and stable disease. Leukemia 2007;21:110–20.
19. Tromp JM, Tonino SH, Elias JA, Jaspers A, Luijks DM, Kater AP, et al.Dichotomy in NF-kappaB signaling and chemoresistance in immuno-globulin variable heavy-chain-mutated versus unmutated CLL cellsupon CD40/TLR9 triggering. Oncogene 2010;29:5071–82.
20. Muzio M, Scielzo C, Bertilaccio MT, Frenquelli M, Ghia P, Caligaris-Cappio F. Expression and function of toll like receptors inchronic lymphocytic leukaemia cells. Br J Haematol 2009;144:507–16.
21. Ntoufa S, Vardi A, Papakonstantinou N, Anagnostopoulos A, Ale-porou-Marinou V, Belessi C, et al. Distinct innate immunity pathwaysto activation and tolerance in subgroups of chronic lymphocyticleukemia with distinct immunoglobulin receptors. Mol Med. 2012 Mar19. [Epub ahead of print].
22. Bertilaccio MT, Simonetti G, Dagklis A, Rocchi M, Veliz Rodriguez T,Apollonio B, et al. Lack of TIR8/SIGIRR triggers progression ofchronic lymphocytic leukemia in mouse models. Blood 2011;118:660–9.
23. Hallek M, Cheson BD, Catovsky D, Caligaris-Cappio F, Dighiero G,Dohner H, et al. Guidelines for the diagnosis and treatment of chroniclymphocytic leukemia: a report from the International Workshop onChronic Lymphocytic Leukemia updating the National Cancer Insti-tute-Working Group 1996 guidelines. Blood 2008;111:5446–56.
24. Livak KJ, Schmittgen TD. Analysis of relative gene expression datausing real-time quantitative PCR and the 2(-delta delta C(T)) method.Methods 2001;25:402–8.
25. Rai K. A critical analysis of staging in CLL. In: Chronic lymphocyticleukemia recent progress and future direction. UCLA Symposia onMolecular and Cellular Biology, New Series, Vol. 59. New York, NY:1987. p. 253.
26. SchenaM, Larsson LG, Gottardi D, Gaidano G, CarlssonM, Nilsson K,et al. Growth- and differentiation-associated expression of bcl-2 in B-chronic lymphocytic leukemia cells. Blood 1992;79:2981–9.
27. Hanada M, Delia D, Aiello A, Stadtmauer E, Reed JC. bcl-2 genehypomethylation and high-level expression in B-cell chronic lympho-cytic leukemia. Blood 1993;82:1820–8.
28. O'Connell RM, Taganov KD, Boldin MP, Cheng G, Baltimore D.MicroRNA-155 is induced during the macrophage inflammatoryresponse. Proc Natl Acad Sci U S A 2007;104:1604–9.
29. Li S, Moffett HF, Lu J, Werner L, Zhang H, Ritz J, et al. MicroRNAexpression profiling identifies activated B cell status in chronic lym-phocytic leukemia cells. PLoS ONE 2011;6:e16956.
30. Thai TH, Calado DP, Casola S, Ansel KM, Xiao C, Xue Y, et al.Regulation of the germinal center response by microRNA-155. Sci-ence 2007;316:604–8.
31. Bomben R, Gobessi S, Dal Bo M, Volinia S, Marconi D, Tissino E, et al.ThemiR-17 approximately 92 family regulates the response to Toll-likereceptor 9 triggering of CLL cells with unmutated IGHV genes. Leu-kemia 2012;26:1584–93.
32. Hallaert DY, Jaspers A, van Noesel CJ, van Oers MH, Kater AP,Eldering E. c-Abl kinase inhibitors overcome CD40-mediated drugresistance in CLL: implications for therapeutic targeting of chemore-sistant niches. Blood 2008;112:5141–9.
33. Vogler M, Butterworth M, Majid A, Walewska RJ, Sun XM, Dyer MJ,et al. Concurrent up-regulation of BCL-XL and BCL2A1 inducesapproximately 1000-fold resistance to ABT-737 in chronic lympho-cytic leukemia. Blood 2009;113:4403–13.
34. Cherfils-Vicini J, Platonova S, Gillard M, Laurans L, Validire P, Calian-dro R, et al. Triggering of TLR7 and TLR8 expressed by human lungcancer cells induces cell survival and chemoresistance. J Clin Invest2010;120:1285–97.
35. Kelly MG, Alvero AB, Chen R, Silasi DA, Abrahams VM, Chan S, et al.TLR-4 signaling promotes tumor growth and paclitaxel chemoresis-tance in ovarian cancer. Cancer Res 2006;66:3859–68.
36. Tarnani M, Laurenti L, Longo PG, Piccirillo N, Gobessi S, Mannocci A,et al. The proliferative response toCpG-ODNstimulation predicts PFS,TTT and OS in patients with chronic lymphocytic leukemia. Leuk Res2010;34:1189–94.
Fonte et al.
Clin Cancer Res; 19(2) January 15, 2013 Clinical Cancer ResearchOF12
Research. on April 28, 2021. © 2012 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2012; DOI: 10.1158/1078-0432.CCR-12-1922

37. Alvarez-Mon M, Garcia-Suarez J, Prieto A, Manzano L, Reyes E,Lorences C, et al. Heterogeneous proliferative effect of tumornecrosis factor-alpha and lymphotoxin on mitogen-activated Bcells from B-chronic lymphocytic leukemia. Am J Hematol 1993;43:81–5.
38. Kulmburg P, Radke M, Digel W. Lymphotoxin-alpha is an autocrinegrowth factor for chronic lymphocytic leukemia B cells. Leukemia1998;12:493–8.
39. Prasad KV, Ao Z, Yoon Y, Wu MX, Rizk M, Jacquot S, et al. CD27, amember of the tumor necrosis factor receptor family, induces apo-ptosis andbinds toSiva, aproapoptotic protein. ProcNatl AcadSciUSA 1997;94:6346–51.
40. Wiley SR, Schooley K, Smolak PJ, DinWS, HuangCP, Nicholl JK, et al.Identification and characterization of a new member of the TNF familythat induces apoptosis. Cell 1995;3:9.
41. Masumoto J, Taniguchi S, Ayukawa K, Sarvotham H, Kishino T,Niikawa N, et al. ASC, a novel 22-kDa protein, aggregates duringapoptosis of human promyelocytic leukemia HL-60 cells. J Biol Chem1999;26:4.
42. Frenquelli M, Muzio M, Scielzo C, Fazi C, Scarfo L, Rossi C, et al.MicroRNA and proliferation control in chronic lymphocytic leukemia:functional relationship between miR-221/222 cluster and p27. Blood2010;115:3949–59.
43. Pogribny IP, Filkowski JN, Tryndyak VP, Golubov A, Shpyleva SI,Kovalchuk O. Alterations of microRNAs and their targets are associ-atedwith acquired resistanceofMCF-7 breast cancer cells to cisplatin.Int J Cancer 2010;127:1785–94.
44. Moussay E, Palissot V, Vallar L, Poirel HA,Wenner T, El Khoury V, et al.Determination of genes and microRNAs involved in the resistance tofludarabine in vivo in chronic lymphocytic leukemia. Mol Cancer2010;9:115.
45. Calin GA, Ferracin M, Cimmino A, Di Leva G, Shimizu M, Wojcik SE,et al. A MicroRNA signature associated with prognosis and progres-sion in chronic lymphocytic leukemia. N Engl J Med 2005;353:1793–801.
46. Costinean S, Zanesi N, Pekarsky Y, Tili E, Volinia S, Heerema N, et al.Pre-B cell proliferation and lymphoblastic leukemia/high-grade lym-phoma in E(mu)-miR155 transgenic mice. Proc Natl Acad Sci U S A2006;103:7024–9.
47. Rodriguez A, Vigorito E, Clare S, Warren MV, Couttet P, Soond DR,et al. Requirement of bic/microRNA-155 for normal immune function.Science 2007;316:608–11.
48. WangM, Tan LP, Dijkstra MK, van LomK, Robertus JL, Harms G, et al.miRNA analysis in B-cell chronic lymphocytic leukaemia: proliferationcentres characterized by low miR-150 and high BIC/miR-155 expres-sion. J Pathol 2008;215:13–20.
TLR Protects CLL Cells from Fludarabine-Induced Apoptosis
www.aacrjournals.org Clin Cancer Res; 19(2) January 15, 2013 OF13
Research. on April 28, 2021. © 2012 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2012; DOI: 10.1158/1078-0432.CCR-12-1922

Published OnlineFirst December 5, 2012.Clin Cancer Res Eleonora Fonte, Benedetta Apollonio, Lydia Scarfò, et al. Modulated by the Stimulation of Toll-like Receptors
Sensitivity of CLL Cells to Fludarabine May BeIn Vitro
Updated version
10.1158/1078-0432.CCR-12-1922doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2012/12/05/1078-0432.CCR-12-1922.DC1Access the most recent supplemental material at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://clincancerres.aacrjournals.org/content/early/2013/01/04/1078-0432.CCR-12-1922To request permission to re-use all or part of this article, use this link
Research. on April 28, 2021. © 2012 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2012; DOI: 10.1158/1078-0432.CCR-12-1922