Embed Size (px)
Citation preview

593ISSN 1746-0913Future Microbiol. (2014) 9(5), 593–601
REVIEW
In orthopedics, prosthetic joint infections (PJIs) and other nonbiological implants are an important concern for the healthcare system, and are associated with many inconveniences for patients, such as prolonged hospitalization, additional surgery associated with higher risk of complications and longtime antimicrobial treatment [1–3]. Despite the relatively low incidence of PJIs (1–2%) [4], the associated economic impact remains enormous: the annual cost of infected prosthesis revisions in the USA increased from US$320 to 566 million from 2001 to 2009, and it is expected to exceed $1.62 billion by 2020 [5].
A wide range of microorganisms are able to produce biofilm on prosthetic materials, causing, in many cases, a fatal course of therapy. Staphylococcus aureus, coagulase-negative staphylococci and Gram-negative rods are the most commonly involved pathogens in PJIs [6]. The first step in PJI pathogenesis is the adherence of bacterial cells to the implant [7], followed by the formation of a biofilm matrix. It is well known that biofilm is a matrix-enclosed microbial population charac-terized by cell–cell adhesion between microorganisms and the nonbiological surface [8]. Biofilm formation is an ancient and integral component of the prokaryotic cell cycle and an important factor for bacterial survival in the environment. The common feature of biofilm-related infections is their intrinsic resistance to host immunity, conventional antimicrobial agents and biocides [9]. Bacteria enclosed in biofilm are in fact known to tolerate levels of antibiotics ten to 1000-times higher than the minimum inhibitory concentrations of the corresponding planktonic form. For these reasons, over the years the study of biofilm has become the subject of many studies, with the
REVIEW
part of
10.2217/FMB.14.20 © 2014 Future Medicine Ltd
RESEARCH ARTICLE
In vitro antibiofilm activity of bioactive glass S53P4
Lorenzo Drago*,1,2, Christian Vassena2, Simone Fenu3, Elena De Vecchi1, Valentina Signori1, Raffaele De Francesco3 & Carlo Luca Romanò4
1Laboratory of Clinical Chemistry & Microbiology, IRCCS Galeazzi Orthopaedic Institute, Via R. Galeazzi 4, 20161 Milan, Italy 2Department of Biomedical Science for Health, University of Milan, Milan, Italy 3Department of Genomics & Molecular Biology, Virology Program, National Institute of Molecular Genetics (INGM), Milan, Italy 4Center for Reconstructive Surgery of Osteoarticular Infections (CRIO), IRCCS Galeazzi Orthopaedic Institute, Milan, Italy
*Author for correspondence: Tel.: +39 0266214839; Fax: +39 0266214774; [email protected]
ABSTRACT: Aim: This work aimed to investigate the ability of different formulations of bioactive glass (BAG)-S53P4 to interfere with bacterial biofilm produced on prosthetic material by methicillin-resistant Staphylococcus aureus and multi-drug-resistant Pseudomonas aeruginosa. Materials & methods: Antibiofilm activity of three formulations of bioglass was assessed at different time points through two different analyses: Crystal Violet and confocal laser scanning microscopy assays. Results: Significant differences in the whole biofilm were observed between BAG-S53P4-treated and control samples, while no marked changes in antibiofilm activity were observed among the tested formulations. Data from colorimetric assay were confirmed by confocal laser scanning microscopy analysis, which evidenced the significant reduction in biomass and a decrease of total cell volume when both S. aureus and P. aeruginosa biofilms were treated with BAG-S53P4. Conclusion: BAG-S53P4 can be considered as an excellent adjuvant in the treatment of prosthetic infections related to biofilm.
KEYWORDS • bacterial biofilm • bioactive glass • confocal laser scanning microscopy • prosthetic joint infections • prosthetic materials
For reprint orders, please contact: [email protected]

Future Microbiol. (2014) 9(5)594
aim to evaluate the ability of various substances to interfere with its complex structure, in order to gain the eradication of microorganisms from the site of infection.
Bioactive glasses (BAGs) have been recently shown to have antibacterial, osteoconductive and angiogenic properties [10–16], which make the use of BAGs advisable in the treatment of biofilm-related PJIs.
BAG-S53P4 (BonAlive® Biomaterials Ltd, Turku, Finland) is a medical device approved in Europe for the treatment of osteomyelitis and it is, to our knowledge, the only biomaterial approved for local application in the treatment of bone infections without being preloaded with antibiotics nor acting as an antibiotic carrier. Its main property, once conditioned in aque-ous solution [17], is the ability to facilitate tissue growth by chemical binding to the bone matrix and thereby to promote the formation of new bone in the implanted area.
Recently, BAG-S53P4 has been successfully used as a component of cranio-maxillofacial implants and as the adjunctive treatment of chronic osteomyelitis of the long bones [18–20]. Peltola et al. reported an accurate obliteration of sinuses in 39 out of 42 patients suffering from chronic frontal sinusitis who could not be cured with other means of treatment when BAG-S53P4 was used as an obliteration material [18]. Furthermore, the same authors reported that no bacterial growth was observed in tissue samples from the same patients. In another study, no signs of infection have been reported in the follow-up of 24 out of 27 patients with osteomyelitis of the long bones who were treated with BAG-S53P4 [20].
Moreover, recent studies have demonstrated that it is also able to reduce bacterial activity by interfering with the onset of infections at the site of surgery owing to its chemical composition (SiO
2, Na
2O, CaO, P
2O
5) [13–17]. A simultaneous
increase in pH values due to sodium ion release and osmotic pressure rise caused by the forma-tion of phosphorus and calcium salts makes the environment hostile for bacterial adhesion and proliferation, reducing the possibility of infec-tion. To the best of our knowledge, no studies on BAG-S53P4 bioglass have been performed in order to evaluate its activity against the biofilm formed by the bacteria responsible for PJIs on prosthetic materials. A reduction in bacterial counts after treatment of staphylococcal bio-film with BAG-S53P4 has been recently reported by Coraça-Huber et al. [21]. This work aims to
investigate the ability of BAG-S53P4 bioglass to interfere with bacterial biofilm on prosthetic material in depth using confocal laser scanning microscopy (CLSM) analysis to evaluate changes in biofilm structure. In particular, the activities of three different formulations of BAG-S53P4 against biofilms produced by clinical isolates of methicillin-resistant S. aureus and Pseudomonas aeruginosa were compared.
Materials & methods●● Bacterial strains
One strain of methicillin-resistant S. aureus and one of P. aeruginosa that were isolated at the Microbiology Laboratory of IRCCS Galeazzi Orthopaedic Institute from infected knee prostheses of patients referring to the Center for Reconstructive Surgery of Osteoarticular Infections (C.R.I.O.) of the same institute for implants revision were used. These strains were selected owing to their strong ability to produce biofilm on prosthetic materials in vitro.
●● Preparation & conditioning of BAG-S53P4Three different formulations of BAG-S53P4 (putty [BAG-S53P4 (500–800 μm) with <45 μm powder embedded in a blend of polyethylene gly-cols (PEGs) and glycerol], powder [with diameter of less than 0.45 μm and granules with diameter of 500–800 μm] and three of inert glass of simi-lar size [R1350 Iittala clear, Iittala, Finland], used as a negative control) were prepared at a final concentration of 400 mg/ml (corresponding to 5% of the clinical working solution) in tryptic soy broth (TSB; Biomerieux, Marcy l’Etoile, France), and 4.8 ml of each solution was placed in ster-ile six-well polystyrene microplates (Jet Biofil; Guangzhou, China). Conditioning of bioglass was obtained in an aqueous environment [17] by incubation at 37°C for a time ranging from 4 to 24 h, depending on the bioglass formulation. More precisely, the conditioning times were 4, 7 and 24 h for putty, powder and granules respec-tively. pH values were measured with a pH meter at regular intervals to determine ion release and pH changing suggestive for conditioning. A pH value equal or higher than 11 was considered sug-gestive of optimal conditioning. Once optimal conditioning was reached, the content of each well was ready to use.
●● Biofilm formationSterile sandblasted titanium discs with a diam-eter of 25 mm and a thickness of 5 mm (Adler
RESEARCh ARTiClE Drago, Vassena, Fenu
future science group

595
Ortho, Cormano [Milan], Italy; batch J04051) were used as a substrate for biofilm forma-tion and growth. Briefly, overnight cultures of S. aureus and P. aeruginosa were resuspended at a final density of 1.0 × 108 CFU/ml in TSB and aliquots (200 μl) of each working solution were inoculated into six-well polystyrene microplates containing titanium discs and 4.8 ml of fresh TSB. After incubation for 24 h at 37°C aerobi-cally, the exhausted growth medium containing non-adherent bacteria was removed and replaced with 5 ml of fresh medium. Plates were incu-bated for a further 48 h to obtain a mature bio-film, then the medium and the remaining non-adhering bacteria, if present, were removed by washing three times with sterile saline.
●● BAG-S53P4 treatmentAfter the conditioning time, titanium discs cov-ered by bacterial biofilm were placed in new ster-ile six-well polystyrene microplates containing either conditioned bioglass or negative control (inert glass). The amount of biofilm on each tita-nium disc was evaluated after 24, 48 and 72 h of incubation.
●● Crystal Violet assayCrystal Violet assay was used as a preliminary test in order to assess the best formulation and the best incubation time of BAG-S53P4 bio-glass to use against S. aureus and P. aeruginosa biofilms.
To evaluate the effect of the tested bioglasses on the biofilm architecture, the whole biomass present on each disc was measured after treat-ment, as described by Christensen et al. [22]. Briefly, at the end of the incubation time, bio-film grown on titanium discs was air dried and stained by disc immersion in a 5% Crystal Violet solution for 15 min. Then, after several wash-ings, the discs were air dried again, and placed in 3 ml of 96% ethanol to elute the Crystal Violet bound to biofilm. Three aliquots (100 μl) of each ethanol dye solution were placed in a 96-multiwell plate and the absorbances were read at 595 nm with a microplate reader (Multiskan FC, Thermo Scientific; Milan, Italy) in triplicate for each disc.
●● CLSM studiesOn the basis of the Crystal Violet assay and for the ease of use and manipulation, we decided to use the granules formulation of BAG-S53P4 bio-glass and 48 h of incubation for CLSM analysis.
As a negative control, we used the same inert glass formulation corresponding to BAG-S53P4 bioglass granules.
Syto9® (FilmTracer™ LIVE/DEAD® Biofilm viability kit, Molecular Probes, Life Technologies Ltd, Paisley, UK) was used to label bacterial cells endowed in the biofilm formed on titanium discs [23].
An appropriate volume of Syto9 (3 μl of dye in 1 ml of sterile saline) was applied above the sur-face of the titanium discs, which were placed in a sterile six-well multiplate and incubated at room temperature for 15 min in the dark. Stained bio-films were examined with a confocal microscope (Leica model TCS SP5; Leica Microsystems CMS GmbH, Mannheim, Germany) using a 20× dry objective (HC PL FLUOTAR 20.0 × 0.50 DRY) plus a 2× electronic zoom.
A 488-nm laser line was used to excite Syto9, while the fluorescent emission was detected from 500 to 540 nm. The laser beam scanned the visual field at a frequency of 700 Hz. Using a second laser line (633 nm) in reflection mode, it was possible to determine both the titanium (starting acquisition point) and the cover slip (ending acquisition point) reflecting surfaces with high accuracy.
Optical sections of 2 μm were collected in sequence along the z-axis over the complete thickness of the sample, and images from five randomly selected positions were acquired for each disc. The resulting stacks of images were analyzed, quantified and subsequently rendered into 3D mode using the software Volocity (Perkin Elmer, MA, USA).
●● Statistical analysisBiofilm amounts as measured by the Crystal Violet assay and biomass volume variation obtained by CLSM images analysis are presented as mean ± SD. Statistical analysis was performed by means of two-way ANOVA followed by Bonferroni t-test and Student’s t-test, as appro-priate. The limit of significance for p-values was set at less than 0.05.
Results●● Crystal violet assay
The antibiofilm activity of BAG-S53P4 is shown in Figure 1. The amount of biofilm present on all titanium discs after treatment was significantly different (p < 0.05) between BAG-S53P4-treated discs and inert glass-treated discs (controls). Although the time of exposure to bioglass
In vitro antibiofilm activity of bioactive glass S53P4 RESEARCh ARTiClE
future science group www.futuremedicine.com

Future Microbiol. (2014) 9(5)596
appeared to not significantly affect the amount of biofilm, after 72 h of treatment a reduction in biofilm was observed, in comparison to those observed after 24 and 48 h. Anti-biofilm activ-ity of BAG-S53P4 did not significantly differ among the three formulations tested.
●● CLSM analysisThe staining properties of Syto9, associated to the instrumental set-up used, allowed us to high-light the biofilm and quantify the biomass and the total bacterial cell volume included in the matrix.
Figure 1. Crystal Violet assay. Absorbance value at 595 nm for methicillin-resistant (A, C & E) Staphylococcus aureus and (B, D & F) Pseudomonas aeruginosa after treatment with different formulation ([A & B] putty, [C & D] powder and [E & F] granules) of inert glass (darker bars) and BAG-S53P4 (lighter bars). *p < 0.05.
T24
*
* * *
**
**
**
*
* *
* **
* *
T48 T72
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
Ab
sorb
ance
T24 T48 T72
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
Ab
sorb
ance
T24 T48 T72
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
Ab
sorb
ance
T24 T48 T72
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
Ab
sorb
ance
T24 T48 T72
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
Ab
sorb
ance
T24 T48 T72
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
Ab
sorb
ance
A
C
B
D
FE
RESEARCh ARTiClE Drago, Vassena, Fenu
future science group

597
Measurement of biomass volume for both S. aureus and P. aeruginosa, expressed as mean ± SD of the five acquired areas for each disc, are represented in Figure 2.
A statistically relevant (p < 0.05) reduction in S. aureus and P. aeruginosa biomass volume was observed for BAG-S53P4 granule-treated sam-ples when compared with the negative controls.
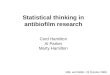
The 3D renderings (Figure 3) confirmed the anti-biofilm activity of BAG-S53P4 bio-glass against both S. aureus and P. aeruginosa, showing a reduction of the biomass (Figure 3B & D), which was not observable when samples were treated with the inert glass (Figure 3A & C). Quantification of bacterial cell volume included in the exopolysaccharide (EPS) matrix was car-ried out by measuring the volume of Syto9 fluorescence. Pie charts (Figure 4) show the com-position of each sample as a percentage of the total volume. As shown in Figure 4A & C, the total cells included within the matrix represented 21% (S. aureus) and 32% (P. aeruginosa) of the volume in the negative controls while, in the BAG-S53P4-treated samples total bacterial cells occupied only 11% (for S. aureus) and 6% (for P. aeruginosa) of the total volume (Figure 4B & D).
DiscussionIn arthroplastic surgery for bone fixation or joint replacement, PJIs sustained by biofilm-produc-ing bacteria represent an important risk in the postoperative follow-up. Usually, the manage-ment of orthopedic implant-related infections consists of complete device removal, long-term antimicrobial therapy with conventional drugs, and eventually prostheses re-implantation [3]. This approach, however, is quite empiric and hindered by the lack of consensus definition to address the optimal treatment of this condition. At present, the most interesting approach is the synergistic effect of different strategies, as the action of biofilm-disrupting agents in combina-tion with antibiotics [24], although an effective anti-biofilm treatment specifically addressed in the treatment of PJI, is not yet available. Bioactive materials are defined as materials that stimulate a particular biological response at the interface between themselves and a biologic tis-sue, which results in bonds forming between them [25]. Bioglass is one of the most interesting biomaterials; however, as the level of bone-bind-ing capacity and resorption rates are significantly influenced by its chemical composition [26], the
Staphylococcus aureus
*
*
Pseudomonas aeruginosa
1,4E+07
1,2E+07
1,0E+07
8,0E+06
6,0E+06
4,0E+06
2,0E+06
0,0E+00
Volu
me
(µm
3 )
Figure 2. Biomass volume of Staphylococcus aureus and Pseudomonas aeruginosa. BAG-S53P4 treatment significantly reduced S. aureus and P. aeruginosa biomass volume after treatment (p < 0.05). Quantification was performed by LAS-AF software obtaining the mean value of biofilm thickness multiplied for total surface of portions acquired (n = 5). Darker bars: biomass volume of inert glass treated samples; lighter bars: BAG-S53P4-treated samples. *p < 0.05.
In vitro antibiofilm activity of bioactive glass S53P4 RESEARCh ARTiClE
future science group www.futuremedicine.com

Future Microbiol. (2014) 9(5)598
evaluation of each bioglass is required to improve its clinical use.
Antibacterial activity is undoubtedly a very important property of bioglass and, in associa-tion with other biochemical characteristics that promote bone regeneration, it helps to prevent the occurrence of infections at surgical sites. For this reason, several studies have been conducted in order to evaluate the antibacterial properties of different commercial bioglasses. It has been shown that BAG-S53P4 is characterized by the greatest antibacterial activity when compared with other bioglasses [14]. Moreover, the BAG-S53P4 spec-trum of activity appears to be very wide includ-ing S. aureus, S. epidermidis and P. aeruginosa, even using small concentrations of bioglass [14]. Moreover, higher concentrations of BAG- S53P4 (100 mg/ml), were able to inhibit bacterial growth of microorganisms that have proven to be resist-ant to the antibacterial activity of other bioglasses, such as Moraxella catharrallis, Klebsiella pneumo-niae or Enterococcus faecium [14]. Its particular composition, in relation to the properties previ-ously described, generate a hostile environment for growth and development of microorganisms. In fact, bioglass antibacterial activity is most likely owing to glass granules being capable of releasing ions in aqueous media, such as sodium, calcium, phosphate and silicate, increasing the pH value
and osmotic pressure of the environment [27].Owing to this, according to Zehnder et al.
[17] BAG-S53P4 granules must be conditioned in order to generate a sufficiently hostile environ-ment for bacterial growth without damaging the host tissue. In this study, in vitro conditioning was implemented by leaving the bioglass in contact with an aqueous solution in order to activate ion release. The conditioning time chosen was 48 h, as no noteworthy pH value variations were docu-mented if the conditioning time was prolonged further. This long time might be explained by the fact that, in the experimental conditions used in the study, the contact surface between the aqueous solution and bioglass was restricted.
Based on these properties, we have tested the ability of BAG-S53P4 to interfere with the biofilm produced on prosthetic material by two clinical strains responsible for prosthetic infection: S. aureus and P. aeruginosa.
Recently, research by Coraça-Huber et al. [21] demonstrated the effectiveness of BAG-S53P4 against biofilm formed by an ATCC strain of S. aureus, evidencing a significant reduction in bacterial counts after treatment with BAG-S53P4. In particular, BAG-S53P4 powder (<0.45 μm) seemed to have better activity compared with granules. In our study, conducted with a thorough analysis of biofilm, we observed no sig-nificant differences between the three formula-tions tested. This may be due to the different bio-glass conditioning procedures used as well as the fact that, in our study, a different methodology for biofilm evaluation was used.
Crystal Violet assay showed excellent activity of BAG-S53P4 bioglass against the biofilm pro-duced by clinical strains of multidrug-resistant S. aureus and P. aeruginosa. These data demon-strate that different formulations of BAG-S53P4, at a concentration of 400 mg/ml, are able to reduce the biofilm mass by approximately 80% if compared with negative controls.
As known, Crystal Violet is an alkaline dye that readily binds to negatively charged molecules and thus to acidic polysaccharides in the extracellular matrix [28], and, in our experience, the solubili-zation with ethanol does not guarantee its com-plete elution, probably causing underestimation of the optical density. With the advances in opti-cal microscopy these semi-quantitative methods have been replaced by more complex technologies that are able to sharpen the sensitivity and also to increase the specificity. CLSM is undoubtedly one of the most sensitive and specific techniques
Figure 3. 3D image of Staphylococcus aureus and Pseudomonas aeruginosa samples. 3D reconstruction of S. aureus and P.aeruginosa biofilm by confocal laser scanning microscopy. Biofilms were grown for 72 h and then treated with BAG-S53P4 (granules) or inert glass for 48 h. Biofilm were stained with Syto9®. (A & B) S. aureus biofilm treated with inert glass (control) and BAG-S53P4; (C & D) P. aeruginosa biofilm treated with inert glass (control) and BAG-S53P4. Green: biofilm; blue: titanium (starting acquisition point), and coverslip (ending acquisition point).
A
C
B
D
Bacteria titanium/coverslip
RESEARCh ARTiClE Drago, Vassena, Fenu
future science group

599
for biofilm structure visualization and analysis. As observed from 3D renderings and confirmed by our measurements, BAG-S53P4 granule treat-ment significantly reduces the biomass volume of both the microorganisms tested. It has to be observed that the values of biomass volume regis-tered by CLSM analysis differs in part from those obtained using the crystal violet assay. Indeed, the reduction of biomass quantified by confocal microscopy was 47% for S. aureus and 36% for P. aeruginosa. This confirms the lack of specificity of the crystal violet assay when compared with CLSM. To the best of our knowledge, CLSM can be considered the gold-standard technique for biofilm study as it requires a structurally inte-grated living biofilm while the Crystal violet assay measures only the whole dry biomass.
Our tests were conducted in vitro in static conditions. As shown by Zhang et al. [29], if a dynamic liquid system would have been used, the antibiofilm effect would probably have been minor. For this reason, it could be interesting to evaluate BAG activity in a dynamic system once established optimal conditioning settings, which could be different from those used in this study.
ConclusionOn the basis of the results obtained, BAG-S53P4 can be considered as an excellent adjuvant, inde-pendently of its formulation, in the treatment of prosthetic infections. Moreover, the dual prop-erties (antibacterial and antibiofilm) of BAG-S53P4 against clinical strains of S. aureus and P. aeruginosa makes this device very interesting for the treatment of prosthetic infections medi-ated by biofilm-producing bacteria. Further studies, in particular using confocal micro scopy, will clarify the mode of action of bioglasses against biofilms formed on prosthetic material.
Future perspectiveRecent studies have demonstrated that 12 mil-lion people are affected by biofilm-related pros-thetic infections and, in the USA, 400,000 peo-ple die each year as a result of these infections. In addition, in spite of the relatively low incidence of PJI (1–2%), the associated healthcare cost remains enormous. The annual cost of infected revisions to USA hospitals increased from $320 million in 2001 to $566 million in 2009, and it is expected that will exceed $1.62 billion by 2020.
Bio�lm
Bio�lm reductionBacteria
79%
21%
32%
68%
47%
11%
42%
36%
6%
58%
Figure 4. Staphylococcus aureus and Pseudomonas aeruginosa percentage composition of the analyzed samples. Pie charts represent S. aureus and P. aeruginosa biomass composition (%) obtained from confocal laser scanning microscopy image analysis, as performed by Volocity software. Blue: biofilm; green: total cells within the biofilm; gray: the amount of biofilm ‘lost’ from BAG-S53P4-treated discs compared with inert glass-treated discs. (A & B) S. aureus biomass components of inert glass control discs and BAG-S53P4-treated discs; (C & D) P. aeruginosa biomass components of inert glass control discs and BAG-S53P4-treated discs.
In vitro antibiofilm activity of bioactive glass S53P4 RESEARCh ARTiClE
future science group www.futuremedicine.com

Future Microbiol. (2014) 9(5)600
The common feature of biofilm-related infec-tions is their resistance to host immunity, as well to conventional antimicrobial agents and bioc-ides. Today, at a time when the pipeline for new antimicrobials is drying up, the development of alternative drugs and/or therapies represents an urgent and growing unsatisfied medical need.
The use of bioglass in the treatment of ortho-pedic infections can surely represent a new frontier in the fight against biofilm-related infec-tions. On the basis of their properties showed in this study, the use of BAG-S53P4 represents an excellent option in the treatment of prosthetic joint infections. The development of new in vitro tests, and the improvement of those already available, will lead scientists to simulate the in vivo conditions as much as possible. We expect
that in microbiology the use of confocal micros-copy will represent the best solution for the bio-film study, allowing not only the visualization of the biomass but also the quantification of the total volume and of the cells contained therein.
Financial & competing interests disclosureThis project was funded by the European Commission within the 7th Framework Programme (Project IDAC – Grant Agreement HEALTH-2011-277988). The authors have no other relevant affiliations or financial involvement with any organization or entity with a finan-cial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
RESEARCh ARTiClE Drago, Vassena, Fenu
future science group
EXECUTiVE SUMMARY
Bioactive glass: a new frontier in prosthetic joint infection treatment
● Bioactive glass (BAG)-S53P4 is a medical device approved in Europe for the treatment of osteomyelitis.
● Its main property is the ability to facilitate tissue growth by chemical binding to the bone matrix, and thereby to promote the formation of new bone in the implanted area.
● Recent studies have shown that it is also able to reduce bacterial activity by interfering with the onset of infections at the site of surgery owing to their chemical composition. Simultaneous increase of pH values due to sodium ion release and osmotic pressure increases caused by the formation of phosphorus and calcium salts makes the environment hostile for bacterial adhesion and proliferation, reducing the possibility of infection.
An in vitro study demonstrates that different formulations of BAG-S53P4 reduce the biofilm formed on prosthetic material
● Crystal Violet assay showed excellent activity of BAG-S53P4 bioglass against the biofilm produced by clinical strains of multidrug-resistant Staphylococcus aureus and Pseudomonas aeruginosa.
● Based on its properties, Crystal Violet does not guarantee an accurate and sensitive analysis.
● Confocal laser scanning microscopy (CLSM) analysis is undoubtedly one of the most sensitive and specific techniques for biofilm structure visualization and analysis.
● CLSM analysis confirms the antibiofilm activity of BAG-S53P4 against the biofilm produced by S. aureus and P. aeruginosa but differs in part from results obtained using the Crystal Violet assay. This confirms the lack of specificity of the Crystal Violet assay if compared with CLSM.
Conclusion
● CLSM can be considered the gold-standard technique for biofilm study as it requires a structurally integrated living biofilm, while the Crystal Volet assay only measures the whole dry biomass.
● BAG-S53P4 can be considered as an excellent adjuvant, independent of its formulation, in the treatment of prosthetic infections.
● Moreover, the dual property (antibacterial and antibiofilm) of BAG-S53P4 against clinical strains of S. aureus and P. aeruginosa makes this device very interesting for the treatment of prosthetic infections mediated by biofilm-producing bacteria.
● Further studies, in particular using confocal microscopy, will clarify the mode of action of bioglasses against biofilms formed on prosthetic material.

601
ReferencesPapers of special note have been highlighted as: • of interest; •• of considerable interest.
1 Peel TN, Buising KL, Choong PF. Diagnosis and management of prosthetic joint infection. Curr. Opin. Infect. Dis. 25(6), 670–676 (2012).
2 Neut D, van der Mei HC, Bulstra SK et al. The role of small-colony variants in failure to diagnose and treat biofilm infections in ortho pedics. Acta. Orthop. 78(3), 299–308 (2007).
3 Darouiche RO. Treatment of infections associated with surgical implants. N. Engl. J. Med. 350(14), 1422–1429 (2004).
4 Sia IG, Berbari EF, Karchmer AW. Prosthetic joint infections. Infect. Dis. Clin. North. Am. 19(4), 885–914 (2005).
5 Kurtz SM, Lau E, Watson H et al. Economic burden of periprosthetic joint infection in the United States. J. Arthroplasty 27(8 Suppl.), 61–65 (2012).
6 Romanò CL, Romanò D, Logoluso N et al. Bone and joint infections in adults: a comprehensive classification proposal. Eur. Orthop. Traumatol. 1(6), 207–217 (2011).
7 Shida T, Koseki H, Yoda I et al. Adherence ability of Staphylococcus epidermidis on prosthetic biomaterials: an in vitro study. Int. J. Nanomed. 8, 3955–3961 (2013).
8 Ellington JK, Reilly SS, Ramp WK et al. Mechanisms of Staphylococcus aureus invasion of cultured osteoblasts. Microb. Pathog. 26(6), 317–323 (1999).
9 Hall-Stoodley L, Stoodley P. Evolving concepts in biofilm infections. Cell. Microbiol. 11(7), 1034–1043 (2009).
10 Day RM. Bioactive glass stimulates the secretion of angiogenic growth factors and angiogenesis in vitro. Tissue Eng. 11(5–6), 768–777 (2005).
11 Arkudas A, Balzer A, Buehrer G et al. Evaluation of angiogenesis of bioactive glass in the arteriovenous loop model. Tissue Eng. Part C Methods 19(6), 479–486 (2013).
• Evaluatesthedifferentpropertiesofbioactiveglassinthearteriovenousloopmodel.
12 Hu S, Chang J, Liu M et al. Study on antibacterial effect of 45S5 bioglass. J. Mater. Sci. Mater. Med. 20(1), 281–286 (2009).
13 Munukka E, Leppäranta O, Korkeamäki M et al. Bactericidal effects of bioactive glasses on clinically important aerobic bacteria. J. Mater. Sci. Mater. Med. 19(1), 27–32 (2008).
•• ThispaperisveryimportantforthisstudybecauseisoneofthefirststudiesthatevaluatethebactericidaleffectofBAG-S53P4onclinicallyimportantaerobicbacteria.
14 Leppäranta O, Vaahtio M, Peltola T et al. Antibacterial effect of bioactive glasses on clinically important anaerobic bacteria in vitro. J. Mater. Sci. Mater. Med. 19(2), 547–551 (2008).
15 Stoor P, Söderling E, Salonen JI. Antibacterial effects of a bioactive glass paste on oral microorganisms. Acta Odontol. Scand. 56(3), 161–165 (1998).
16 Lindfors NC, Hyvönen P, Nyyssönen M et al. Bioactive glass S53P4 as bone graft substitute in treatment of osteomyelitis. Bone 47(2), 212–218 (2010).
17 Zehnder M, Söderling E, Salonen J, Waltimo T. Preliminary evaluation of bioactive glass S53P4 as an endodontic medication in vitro. J. Endod. 30(4), 220–224 (2004).
•• OneofthefirststudiesthatevaluatetheactivityofBAG-S53P4throughin vitro studies.Theunderstandingofbioglassmechanismsisnecessarytoperformaccurateassays.
18 Peltola M, Aitasalo K, Suonpää J, Varpula M, Yli-Urpo A. Bioactive glass S53P4 in frontal sinus obliteration: a long-term clinical experience. Head Neck 28(9), 834–841 (2006).
• RepresentsaclinicalexampleofbioglassuseandisusefulforunderstandingtheclinicaluseofBAG-S53P4.
19 Peltola M, Suonpää J, Aitasalo K et al. Experimental follow-up model for clinical frontal sinus obliteration with bioactive glass (S53P4). Acta Otolaryngol. Suppl. 543, 167–169 (2000).
20 Drago L, Romanò D, De Vecchi E et al. Bioactive glass BAG-S53P4 for the adjunctive treatment of chronic osteomyelitis of the long bones. An in vitro and prospective clinical study. BMC Infect. Dis. 10(13), 584 (2013).
21 Coraça-Huber DC, Fille M, Hausdorfer J et al. Efficacy of antibacterial bioactive glass S53P4 against S. aureus biofilms grown on titanium discs in vitro. J. Orthop. Res. 32(1), 175–177 (2014).
•• OneofthefirststudiestoevaluatetheefficacyofBAG-S53P4againstStaphylococcus aureusbiofilmgrownontitaniumdiscs.
22 Christensen GD, Simpson WA, Younger JJ et al. Adherence of coagulase-negative staphylococci to plastic tissue culture plates: a quantitative model for the adherence of staphylococci to medical devices. J. Clin. Microbiol. 22(6), 996–1006 (1985).
23 Tawakoli PN, Al-Ahmad A, Hoth-Hannig W et al. Comparison of different live/dead stainings for detection and quantification of adherent microorganisms in the initial oral biofilm. Clin. Oral. Investig. 17(3), 841–850 (2013).
24 Arciola CR, Montanaro L, Costerton JW. New trends in diagnosis and control strategies for implant infections. Int. J. Artif. Organs 34(9), 727–736 (2011).
25 Jones JR. Review of bioactive glass: from Hench to hybrids. Acta Biomater. 9(1), 4457–4486 (2013).
26 Cormack AN, Tilocca A. Structure and biological activity of glasses and ceramics. Philos. Trans. A Math. Phys. Eng. Sci. 370(1963), 1271–1280 (2012).
27 Andersson OH, Rosenqvist J, Karlsson KH. Dissolution, leaching, and Al
2O
3 enrichment
at the surface of bioactive glasses studied by solution analysis. J. Biomed. Mater. Res. 27(7), 941–948 (1993).
28 Li X, Yan Z, Xu J. Quantitative variation of biofilms among strains in natural population of Candida albicans. Microbiology. 149(Pt 2), 353–362 (2003).
29 Zhang D, Leppäranta O, Munukka E et al. Antibacterial effects and dissolution behavior of six bioactive glasses. J. Biomed. Mater. Res. A 93(2), 475–483 (2010).
future science group www.futuremedicine.com
In vitro antibiofilm activity of bioactive glass S53P4 RESEARCh ARTiClE

![PDF] Bioactive glass S53P4 vs. autologous bone graft for filling ...Eva Steinhausen1,3, Rolf Lefering2, Martin Glombitza1, Nikolaus Brinkmann1, Carsten Vogel3, Bastian Mester3, and](https://img.pdfslide.us/doc/110x75/612d2ae31ecc51586942054b/bioactive-glass-s53p4-vs-autologous-bone-graft-for-illing-eva-steinhausen13.jpg)