Embed Size (px)
Citation preview

Pediatrics Grand Rounds12 April 2013
University of Texas Health Science Center at San Antonio, Texas
1
Hypertension in the well rounded child
ICD9 401.1 “benign” essential HTN ¿
Jane Lockwood Lynch, MDUniversity of Texas Health Science Center
San Antonio, Texas
April 12, 2013
Disclosures
I disclose the following relationships with commercial companies:
Grant and Research Support from:Eli Lill M dt i D ii hi S k P l– Eli Lilly, Medtronic, Daiichi Sankyo, Parexel
– National Institute of Health
I do not intend to reference the investigational use of these drugs or products in my presentation today.
Learning Objectives
• At the end of this presentation, the participant will be able to:
1. Recognize stage 1 & 2 hypertension in children and adolescentsand adolescents
2. Treat primary hypertension in children using nonpharmacologic and drug therapy options
3. Understand the risk for hypertension in children with type 2 diabetes
Hypertension in American children is common:Hypertension is estimated to be prevalent in 4.5% of children
101214161820
%
02468
10
Hypertension Asthma
%
• Analysis of the medical records of 507 hypertensive and pre‐hypertensive children and adolescents over a span of seven years
• All the children visited an outpatient clinic at least three times
Underdiagnosis of hypertension:
• 376 patients (74%) had undiagnosed hypertension 80 patients (15.8%) had a true hypertension diagnosis 7 patients had undiagnosed stage 2 hypertension
• Data to make the diagnosis of hypertension or prehypertension was present in the patients' records
Adult Definition of Hypertension &“JNC 7” 2003 guidelines
• Adult 140/90 goals are based on evidence correlating BP data with adverse events
MI i k d d b 20 25%– MI risk reduced by 20‐25%
– Stroke risk reduced by 34‐40%
• 159/100= stage 1
• >160 =stage 2

Pediatrics Grand Rounds12 April 2013
University of Texas Health Science Center at San Antonio, Texas
2
U.S. Department of Health and Human
Services The 4th Report on High Blood Pressure in Children and
National Heart, Lung, and Blood InstituteNational High Blood Pressure Education Program
National Institutes of Health
National Heart, Lung, and Blood Institute
August 2004 supplement of Pediatrics
Children and Adolescents
JNC7 vs. 4th Report
• In children, the definition of hypertension is based exclusively on frequency‐distribution curves for BP.
• As a consequence, estimates of the q ,prevalence of pediatric hypertension lack a scientific basis.
• The relevance of pediatric hypertension data to the risk of developing complications during adulthood remain unknown.
4th Report on High Blood Pressure in Children and Adolescents
• BP standards based on sex, age, and height provide a precise classification of BP according to body size.
• The revised 2004 BP tables included the 5th ‐ 99th BP percentiles; which allow for the staging of hypertension in children.
August 2004 supplement of Pediatricswww.nhlbi.nih.gov
SBP (mmHg) DBP (mmHg)Age BP Percentile of Height Percentile of Height
(Year) Percentile 5th 10th 25th 50th 75th 90th 95th 5th 10th 25th 50th 75th 90th 95th
12 50th 101 102 104 106 108 109 110 59 60 61 62 63 63 64
90th 115 116 118 120 121 123 123 74 75 75 76 77 78 79
Example: Blood Pressure Levels for 12 year old Girls by Age and Height Percentile
95th 119 120 122 123 125 127 127 78 79 80 81 82 82 83
99th 126 127 129 131 133 134 135 86 87 88 89 90 90 91
Classification of Stage 1 vs. 2 Hypertension in Children*(done on 3 occasions to confirm)
SBP or DBP Percentile
Normal <90th percentile
Prehypertension 90th percentile to <95th percentile, or if BP exceeds 120/80 even if below theBP exceeds 120/80 even if below the 90th percentile up to <95th percentile
Stage 1 hypertension 95th percentile to the 99th percentile plus 5 mmHg
Stage 2 hypertension >99th percentile plus 5 mmHg
www.nhlbi.nih.gov/guidelines/hypertension/child_tbl.htm
So Let’s Practice
• SAP is a 12 yo female in the 50th percentile of height and 95% for weight. Her manual BP on is 123/82 as she arrives for a visit.
• What is her BP percentile?• What is her BP percentile?
• What do we do with this information?

Pediatrics Grand Rounds12 April 2013
University of Texas Health Science Center at San Antonio, Texas
3
SBP (mmHg) DBP (mmHg)Age BP Percentile of Height Percentile of Height
(Year) Percentile 5th 10th 25th 50th 75th 90th 95th 5th 10th 25th 50th 75th 90th 95th
12 50th 101 102 104 106 108 109 110 59 60 61 62 63 63 64
90th 115 116 118 120 121 123 123 74 75 75 76 77 78 79
Blood Pressure 123/83 BP: 12 year old Girl with 50% Height Percentile
95th 119 120 122 123 125 127 127 78 79 80 81 82 82 83
99th 126 127 129 131 133 134 135 86 87 88 89 90 90 91
Pre‐Hypertension
90‐95% or >120/80
Stage 1 Hypertension95% to 5 mm above 99%
Stage 2 Hypertension> 5 mm above 99%
Normal
< 90%
Auscultation blood pressure measurement is gold standard
Manual auscultation blood pressure measurement is gold standard
• Cuff too small → high reading
• Cuff too big → usually not falsely lowg y y• Prefer right arm if possible for comparison with BP normal values
• Repeat BP in both arms and one leg if elevated
Arm & Leg BP
B A = B < CBP can be 10‐20
mmHg higher in the legs than the arms!
A
C
Korotkoff Sounds
• Artery collapses completely until the systolic pressure is greater than the cuff pressure with first audible sound of a thud or tap = SYSTOLIC
• Phase 2‐4: systolic pressure opens the artery to produce increasing stage 2,3 sounds then muffled blowing sound at phase 4.
• Silence at phase 5= diastolic BP reading

Pediatrics Grand Rounds12 April 2013
University of Texas Health Science Center at San Antonio, Texas
4
Oscillometric blood pressures**measure mean arterial pressureand calculates SPB and DBP
Pediatric Symptoms of Hypertension
“silent disease”? A recent study by Croix found that 51% of untreated hypertensive children when surveyed reported 1‐4 Symptoms, and 14% reported more than four symptoms
3 most common symptoms– headache – difficulty initiating sleep – daytime tiredness These were all reduced with treatment
Expert Panel On Integrated Guidelines for Cardiovascular Health and Risk
Reduction in Children and Adolescents
Pediatrics Dec 2011
NHLBI guidelines are designed for integration into the recommended pediatric health supervision visits in the
AAP Bright Futures Guidelines
Conditions Under Which Children <3 Years oldShould Have BP Measured
• History of prematurity, very low birth weight or other neonatal complication requiring intensive care
• Congenital heart disease• Recurrent urinary tract infections, hematuria or proteinuria• Known renal disease or urologic malformations• Family history of congenital renal disease• Solid organ transplant, malignancy or bone marrow
transplant• Treatment with drugs known to raise BP• Other systemic illnesses associated with hypertension• Evidence of elevated intracranial pressure
Integrated Cardiovascular Health Schedule
• Family History of Cardiovascular Disease– Obtain history by age 3 years– Men < 55 yo, Women < 65 yo with MI, stroke– dyslipidemia, HTN, DM, obesity, sedentary lifestyley p , , , y, y y
• Tobacco Exposure or Medications/Drug Use
• Nutrition/ Diet– Support breastfeeding optimal to 12 months– 2% milk at age 1‐2 yr, fat free milk > 2 yr– Dietary guidance per growth curve
Integrated Cardiovascular Health Schedule • Blood Pressure: Measure annually > 3 yo
• If < 90th % ‐ repeat in 1 year
• If 90‐95th % = prehypertension• Repeat by auscultation x 2 to confirm and repeat in 6 months
• Diet, Activity, Weight management intervention
• If 95% to (99th% + 5 mmHg) = stage 1 HTN• If 95% to (99th% + 5 mmHg) = stage 1 HTN• Confirm on three occasions at least one week apart
• Diet, Activity, Weight management *salt restriction
• Review medications, examination and laboratory evaluation
• If > 99th% + 5 mmHg = stage 2 HTN• Refer to HTN expert within 1 week if possible and begin basic workup with dietary changes
• Start anti‐HTN medication
• Follow q1‐2 weeks until controlled

Pediatrics Grand Rounds12 April 2013
University of Texas Health Science Center at San Antonio, Texas
5
Clinical Evaluation of Confirmed Hypertension
Study or Procedure Purpose Target PopulationEvaluation for identifiable causesHistory, including sleep history, family history, risk factors, diet, and habits such as smoking and drinking
History and physical examination help focus subsequent evaluation
All children with persistent BP >95th percentile
alcohol; physical examinationBUN, creatinine, electrolytes, urinalysis, urine culture
R/O renal disease and chronic pyelonephritis
All children with persistent BP >95th percentile
CBC R/O anemia, consistent with chronic renal disease
All children with persistent BP >95th percentile
Renal ultrasound R/O renal scar, congenital anomaly, or disparate renal size
All children with persistent BP >95th percentile
Clinical Evaluation of Confirmed Hypertension
Study or Procedure Purpose Target PopulationEvaluation for comorbidityFasting lipid panel, fasting glucose
To identify hyperlipidemia, identify metabolic abnormalities
Overweight patients with BP at 90th–94th percentiles; all patients with BP >95th percentilepFamily history of hypertension or cardiovascular diseaseChild with chronic renal disease
Drug screen To identify substances that might cause hypertension
History suggestive of possible contribution by substances or drugs
Polysomnography To identify sleep disorder in association with hypertension
History of loud, frequent snoring
“MONSTER”
• Medication (stimulants, OCP, NSAID, tricyclicscocaine, ecstasy)
• Obesity• Neonatal• Neonatal• Symptoms
• Trends in Family
• Endocrine (hyperthyroid, pheochromocytoma)
• Renal
White Coat Hypertension
• A patient with BP levels above the 95th percentile in a physician’s office or clinic who is normotensive outside a clinical setting.
• Ambulatory Blood PressureMonitoring: a newer technologyWhich measures blood pressure every 15 minutes while awakeand every 30 minutes while asleep (*Night time blood pressure
should drop by 10%)
Infants Children Adolescents1‐6 year 7‐12 year
• renal vein thrombosis, prior UAC
• Renal artery
• Renalparenchymal disease
• Renal artery
• Renal parenchymal
• Renovascular disease
• Essential HTN• Renal
parenchymal disease
Common Causes of Hypertension by Age:
ystenosis
• Congenital renal anomalies
• Coarctation • BPD
ystenosis
• Coarctation of aorta
**82% is secondary HTN
• Essential HTN
>50% Essential HTN
• Renovascular disease
85‐95% is Essential HTN
Clinical and demographic characteristics of children with hypertension. Flynn J, Zhang Y, Solar‐Yohay S, Shi V. Hypertension. 2012 Oct;60(4):1047‐54.
Primary vs. secondary HTN?Diagnosis for 246 patients aged 5–18 years with a mean age of 13.04±3.10 years from 4 pediatric nephrology centers:
15 (6%) secondary hypertension*
151 (61%) primary hypertension*
25 (10%) prehypertension, 8 (3%) white‐coat hypertension
47 (20%) no hypertension
*There was no significant difference in the distribution of patients with stage 1 and 2 hypertension in the primary and secondary hypertension groups
Kapur G et al. Clin Hypertens (Greenwich). 2010; 12(1):34‐9

Pediatrics Grand Rounds12 April 2013
University of Texas Health Science Center at San Antonio, Texas
6
Percentage of U.S. Children and Adolescents Classified as Obese, 1963–2008*
19.6
18.1
*>95th percentile for BMI by age and sex based on 2000 CDC BMI‐for‐age growth charts.
**1963–1970 data are from 1963–1965 for children 6–11 years of age and from 1966–1970 for adolescents 12–17 years of age.
Source: NCHS. Health, United States, 2010: With Special Feature on Death and Dying. Hyattsville, MD. 2011
4.6
4.2
The “Great” State of Texas :
• 2nd youngest population
• Highest number of children per
family
• ~10% of US children
• ~25% of Hispanic children• ~25% of Hispanic children
• South Texas ~ 6.5 million people
• ~1.8 million children <18 years of
age
• several of the fastest growing
areas (Austin, San Antonio
McAllen, and Laredo)
SBP (mmHg) DBP (mmHg)Age BP Percentile of Height Percentile of Height
(Year) Percentile 5th 10th 25th 50th 75th 90th 95th 5th 10th 25th 50th 75th 90th 95th
12 50th 101 102 104 106 108 109 110 59 60 61 62 63 63 64
90th 115 116 118 120 121 123 123 74 75 75 76 77 78 79
Back to our San Antonio patient: she has now had repeat BPs on three occasions which were >95% and she has no
laboratory or clinical evidence for an underlying etiology:
95th 119 120 122 123 125 127 127 78 79 80 81 82 82 83
99th 126 127 129 131 133 134 135 86 87 88 89 90 90 91
Therapeutic LifestyleChanges
• Family‐based intervention improves success.
• Weight reduction = primary therapy for obesity‐related prehypertension and hypertension .
• Physical activity* can improve efforts at weight management and may prevent future increase in BP.
*Participation in sports — Children who have controlled high blood pressure are generally allowed to participate in competitive sports. Children and adolescents with high blood pressure are advised to avoid weight lifting until the blood pressure is better controlled. Exceptions to these recommendations include children with uncontrolled stage 2 hypertension, who are generally advised to avoid competitive sports.
DASH: Dietary approaches to stop Hypertension
• Eliminate sugar containing drinks (soda, juice, sugared drinks)
• Decrease White Foods (pasta, rice, potatoes & SALT!)
• Increase Bright Color Foods (vegetables, fruits)
• Goal of < 2,300 mg salt for healthy people (one leveled teaspoon) and 1,500 mg for those with high blood pressure.

Pediatrics Grand Rounds12 April 2013
University of Texas Health Science Center at San Antonio, Texas
7
Insulin Resistance and PubertyHyperinsulinism further increases reabsorption of Na and
increases sympathetic tone
37Moran et al., J Clin Endocrinol Metab 2002; 87:4817-4820
Salt recommendations
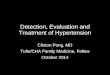
What we’re up against
The contiguous United States, visualized by distance to the nearest McDonald’s
Dietary Fruit and Vegetables Daily intake in children Intervention Effect Size Estimates of Behavioral Interventions on Systolic Blood Pressure
• BMI reduction of 10%: 5‐15 mmHg• Exercise intervention: 1‐5 mmHg• Salt restriction: 3‐5 mmHg short termSalt restriction: 3 5 mmHg short term• DASH type diet unknown but positive effect likely

Pediatrics Grand Rounds12 April 2013
University of Texas Health Science Center at San Antonio, Texas
8
Indications for Antihypertensive Drug Therapy in Children
• Symptomatic hypertension
• Secondary hypertension
• Hypertensive target organ damage• Hypertensive target‐organ damage
• Diabetes (types 1 and 2)
• Persistent hypertension despite nonpharmacologic measures
Antihypertensive medications
Evidence based dosing and FDA approval for pediatric use is available in ALL these categories
– ACE‐I :after age 2 preferred– ARB: age 6 and older– Diuretics– Calcium Channel Blocker– Beta Blockers– Centrally acting alpha agonists– direct renin inhibitor, aldosterone antagonist not yet approved for
children:
Antihypertensive medications
ACE‐Inhibitors block angiotensin II productionEx. benzapril , enalapril, fosinopril, lisinopril
ACE Inhibitor:
• Avoid if suspecting renal artery stenosis
• Minimal rise in K, cough SE • Discontinue ACE if markedly sco t ue C a ed y
elevated hepatic serum enzymes develop or pregnant
Angiotensin Receptor Blockers
ARBs block Angiotensin II actionex. irbesartan, losartan – age 6 and ldolder
ARB
Angiotensin Receptor Blockerinterferes with the binding of angiotensin II to angiotensin I receptors
‐do not use in pregnancy or marked liver elevation

Pediatrics Grand Rounds12 April 2013
University of Texas Health Science Center at San Antonio, Texas
9
RAAS targets
Angiotensin Receptor Blocker
Aldosterone antagonist
Direct renin inhibitor
ACE Inhibitor
Diuretics
http://sprojects.mmi.mcgill.ca/nephrology/presentation/images/86no2.gif
Calcium channel blockers
Block the entry of calcium into the cells which decreases vascular peripheral resistanceperipheral resistanceEx: amlodipine‐ long half life
Other agents
–Beta Blockers: propranolol – avoid in DM, asthma, athletes
–Centrally acting alpha agonists: clonidine
– Not yet approved for children: direct renin inhibitor, aldosterone antagonist
Step‐wise Approach to Therapy
1. Start with a small dose of an ACE, ARB or CCB anti‐hypertensive drug with once daily monotherapy preferred
2. Increase initial anti‐hypertensive drug until BP <95%: expect 5 10 mm HG change forBP <95%: expect 5‐10 mm HG change for each dosage increase
3. Add a small dose of a second drug (often diuretic) once monotherapy at maximal dose
4. Increase dose of second anti‐hypertensive medication until BP <95%*
Target‐Organ Abnormalities in Children with Hypertension
• Target‐organ abnormalities are detectable in hypertensive children and adolescents.
• LVH is the most prominent evidence of target‐organ damage and can be evaluated with echocardiographyechocardiography
• The presence of LVH is an indication to initiate or intensify antihypertensive therapy

Pediatrics Grand Rounds12 April 2013
University of Texas Health Science Center at San Antonio, Texas
10
Important Adult BP Trials with Pediatric Implications
• ALLHAT– All drug classes equally effective in BP treatment and CVD mortality reduction
– 64% of adults required 2 drugs for BP control– Some classes had better outcomes in secondary analyses (diuretics, ACE inhibiters usually)
• Trophy– Treating pre‐hypertension (ARB) prevents the onset of future hypertension
ABCD2,3 (132 mm Hg)
AASK1 (134 mm Hg)
High‐Risk Hypertensive Patients Require Multiple Agents to Achieve Goal
ALLHAT4 (135 mm Hg)
AchievedSBP
1Wright JT, et al. JAMA. 2002;288:2421-2431. 2Bakris GL. J Clin Hypertens. 1999;1:141-147. 3Estacio RO, et al. N Engl J Med. 1998;338:645-652. 4The ALLHAT Officers and Coordinators. JAMA. 2002;288:2981-2997. 5Hansson L, et al. Lancet. 1998;351:1755-1762. 6Lewis EJ, et al. N Engl J Med. 2001;345:851-860. 7Bakris GL, et al. Arch Intern Med. 2003;163:1555-1565. 8UK Prospective Diabetes Study Group. BMJ. 1998;317:703-713.
1 2 3 4Number of BP Medications
RENAAL7 (140 mm Hg)
IDNT6 (140 mm Hg)
UKPDS2,8 (144 mm Hg)
HOT2,5 (141 mm Hg)
Sad but True
80% of Diabetic patients will either die from or have a major cardiovascular
event
One of my first patients that I treated at UTHSCSA for Type 2 Diabetes lost 140 lbs before he died of a heart attack at
age 23 at UHS
Primary Aim: Comparison of three treatment regimens on time to failure (loss of glycemic control) in children and adolescents with Type 2 Diabetes
Multiple secondary Outcomes
Included:Included:
• Cardiovascular disease risk
• Microvascular & Macrovascularcomplications
TODAY Study Group, NEJM, 2012
Major Comorbidities at Baseline and New(New = <4 years average time in study)
Met alone Met + rosi Met + lifestyle Hypertensionbaseline 12% 12% 11%new 25% 23% 19%
Dyslipidemia – LDL
baseline 4% 3% 3%
60
new 8% 7% 6%Dyslipidemia – Trig
baseline 22% 16% 16%new 9% 12% 9%
Microalbuminuria
baseline 9% 3% 6%new 11% 12% 9%
TODAY Study Group, NEJM, 2012

Pediatrics Grand Rounds12 April 2013
University of Texas Health Science Center at San Antonio, Texas
11
Echocardiography Measures by Treatment Group
(median and quartiles)
by h
eigh
t
2.5
2.6
2.72.8
eigh
t**2
.7
40
45
50
LA diameter indexed by height(population median 2.0 cm/m)
LV mass indexed by height2.7
(population median 30 g/m2.7)
61
LA d
iam
eter
inde
xed
b
1.8
1.9
2.0
2.1
2.2
2.3
2.4
Treatment group
M M+R M+L
LV m
ass
inde
xed
by h
e
20
25
30
35
40
Treatment group
M M+R M+L
In Summary
• Hypertension in American children is a growing epidemic
• High blood pressure is estimated to be prevalent in 4.5% of children and up to 75% of p pcases may be missed in clinical care
• Hypertensive obese children have metabolic factors increasing their risk for early cardiovascular disease which is accelerated by hyperinsulinemia and/or T2Diabetes
The way to keep your health is to eat what you don't want, drink what you don't like, and do what you'd rather not. Mark Twain
References
• Allen DB, Nemeth BA, Clark RR, Peterson SE, Eickhoff J, Carrel AL. Fitness is a stronger predictor of fasting insulin levels than fatness in overweight male middle‐school children. J Pediatr 2007 Apr;150(4):383‐387.
• Chae HW, Kwon YN, Rhie YJ, Kim HS, Kim YS, Paik IY, et al. Effects of a structured exercise program on insulin resistance, inflammatory markers and physical fitness in obese Korean children. J PediatrEndocrinol Metab 2010 Oct;23(10):1065‐1072.
• Orsi CM, Hale DE, Lynch JL. Pediatric obesity epidemiology. Curr Opin Endocrinol Diabetes Obes. 2011 Feb;18(1):14‐22.
• TODAY Study Group A clinical trial to maintain glycemic control in youth with type 2 diabetes N Engl J• TODAY Study Group. A clinical trial to maintain glycemic control in youth with type 2 diabetes. N Engl J Med 2012. DOI: 10.1056/NEJMoa1109333.
• Childs, Dan. "Kids' High Blood Pressure Often Missed." ABC News 21 Aug. 2007. <http://www.abcnews.go.com/Health/CardiacHealth/>.
• Couch, Sarah C., Stephen Daniels. "Diet and Blood Pressure in Children." Current Opinion in Pediatrics Oct. 2005: 648‐652.
• Croix, Beth, and Daniel I. Feig. "Childhood Hypertension is Not a Silent Disease." Pediatric Nephrology 21 (2006): 527‐532. Medline. University of Kentucky. 2 Oct. 2007.
• Din‐Dzietham, Rebecca, Yong Liu, Marie‐Vero Bielo, and Falah Shamsa. "High Blood Pressure Trends in Children and Adolescents in National Surveys, 1963‐2002." Circulation Journal of the American Heart Association (2007): 1392‐1400. PubMed. University of Kentucky. 12 Sept. 2007.
References
Hanevoid, Coral, Jennifer Waller, Stephen Daniels, Ronald Portman, and Jonathan Sorof. "The Effects of Obesity, Gender, and Ethnic Group on Left Ventricular Hypertrophy and Geometry in Hypertensive Children: a Collaborative Study of the International Pediatric Hypertension Association." Pediatrics 113 (2004): 328‐333. University of Kentucky. 2 Oct. 2007.
Hansen, Matthew L., Paul W. Gunn, and David C. Kaelber. "Underdiagnosis of Hypertension in Children and Adolescents." JAMA 298.8 (2007): 874‐879. University of Kentucky. 28 Oct. 2007.
Kavey, Rae‐Ellen W., Daniel A. Kveselis, Nader Atallah, and Frank C. Smith. "White Coat Hypertension in Childhood: Evidence for End‐Organ Effect." The Journal of Pediatrics 150.5 (2007): 491‐497. Science Direct. University of Kentucky. 2 Oct. 2007.
Belfort, Mandy. Size at Birth, Infant Growth, and Blood Pressure at 3 years of Age. Pediatrics. 2007; 151: 670‐674
Dasgupta, Kaberi. Emergence of Sex Differences in Prevalence of High Systolic Blood Pressure. Circulation. 2006; 114:2663‐2670
Falkner, Bonita, et al. The Relationship of Body Mass Index and Blood Pressure in Primary Care Pediatric Patients. Pediatrics. 2006; 148: 195‐200
Sorof JM, et al. Overweight, Ethnicity, and the Prevalence of Hypertension in School aged Children. Pediatrics. 2004; 113:475‐482
Strauss RS, Pollack HA. Epidemic increase in childhood overweight, 1986‐1998. JAMA. 2001; 286:2845‐2848
U.S. Census Bureau: http://factfinder.census.gov/

Pediatrics Grand Rounds12 April 2013
University of Texas Health Science Center at San Antonio, Texas
12
Computation of Blood Pressure Percentiles for Arbitrary Sex, Age, and Height
Refer to the most recent CDC growth charts, which are available online, and convert the height of h inches to a height Z‐score relative to boys of the same age; this is denoted by Zht.
2. Compute the expected SBP (μ) for boys of age y years and height h inches given by μ = α + Σβj (y‐10)j+ Σγ k (Zht)kwhere α, β1…, β4 and γ1…, γ4 are given in the 3rd column of appendix table B–1.
3. Then convert the boy’s observed SBP to a Z‐score (Zbp) given by Zbp = (x – μ)/σwhere σ is given in the 3rd column of appendix table B–1.
4. To convert the bp Z‐score to a percentile (P), compute P = Φ (Zbp) x 100% where Φ (Z) = area under a standard normal distribution to the left of Z. Thus, if Zbp = 1.28, then Φ (Zbp) = .90 and the bp percentile = .90 x 100% = 90%.
5. To compute percentiles for SBP for girls, diastolic blood pressure (DBP) (K5) for boys, and DBP (K5) for girls, use the regression coefficients from the 4th, 5th, and 6th columns of appendix table B–1.
For example, a 12‐year‐old boy, with height at the 90th percentile for his age‐sex group, has a height Z‐score = 1.28, and his expected SBP (μ) is μ = 102.19768 + 1.82416 (2) + 0.12776 (22) + 0.00249 (23) –0.00135 (24) + 2.73157(1.28) –0.19618 (1.28)2 –0.04659 (1.28)3 + 0.00947 (1.28)4 = 109.46 mmHg.
Suppose his actual SBP is 120 mmHg (x); his SBP Z‐score is then: SBP Z‐score = (x – μ)/σ = (120–109.46)/10.7128 = 0.984The corresponding SBP percentile = Φ (0.984) x 100% = 83.7th percentile.
ACE inhibitors• Renal side effects: Patients with renal artery stenosis should not receive
ACE inhibitors because they maintain glomerular filtration by efferent arteriolar vasoconstriction, which is blocked by ACE.
• Metabolic side effects: moderate, often clinically insignificant rise in potassium due to a mild reduction in serum aldosterone concentrations and beneficial effect on plasma insulin levels
• Hepatic side effects: a rare syndrome that begins with cholestatic jaundice and progresses to fulminant hepatic necrosis and (sometimes) death. DiscontineACE if markedly elevated hepatic serum enzymes develop
• Racial Differences: African American children do not respond to ACE inhibitor therapy as well as children of other races
• Pregnancy: major congenital malformations after first‐trimester exposure to ACE inhibitors. It is not known whether this may apply to all other classes of drugs that block the renin–angiotensin system*
BP tables for Infants
*Task Force on Blood Pressure Control in Children. Report of the Second Task Force on Blood Pressure Control in Children—1987.Pediatrics.1987;79:1–25(PR)
Measure BP and Height and Calculate BMIDetermine BP category for sex, age, and height
Educate on Heart Healthy
LifestyleFor the family
Prehypertensive
90–<95% <90%
>95%
Normotensive
TherapeuticLifestyleChanges
Stage 2 Hypertension Stage 1 Hypertension
Repeat BPOver 3 visits
90–<95% or 120/80 mmHg
or 120/80 mmHg
Management Algorithm
Rx Specificfor Cause
Drug Rx‡ MonitorQ 6 Mo
>95%
Diagnostic Workup IncludesEvaluation for Target-Organ Damage
SecondaryHypertension
OverweightNormal BMI Overweight
Repeat BPIn 6 months
Consider Diagnostic Workup and Evaluation for Target-Organ Damage
If overweight or comorbidity exists
Weight Reduction
PrimaryHypertension
Normal BMI
Consider ReferralTo provider with expertisein pediatric hypertension
Drug Rx Weight Reductionand Drug Rx
Overweight
Weight Reduction
Still >95%
90–<95% or 120/80 mmHg
Normal BMI
Diagnostic Workup IncludesEvaluation for Target-Organ Damage
Therapeutic LifestyleChanges
SecondaryHypertension
or PrimaryHypertension