Embed Size (px)
DESCRIPTION
IN THE NAME OF GOD. MEDICAL MANAGEMENT OF BLOOD GLUCOSE IN TYPE 2 DIABETES MELLITUS. Criteria for the diagnosis of DM. Symptoms of diabetes plus random blood glucose concentration ≥ 200 mg/dl OR FPG ≥ 126 mg/dl OR - PowerPoint PPT Presentation
Citation preview
Criteria for the diagnosis of DMSymptoms of diabetes plus random blood glucose concentration ≥ 200 mg/dl OR
FPG ≥ 126 mg/dl ORTwo –hour plasma glucose ≥ 200 mg/dl during an oral glucose tolerance test
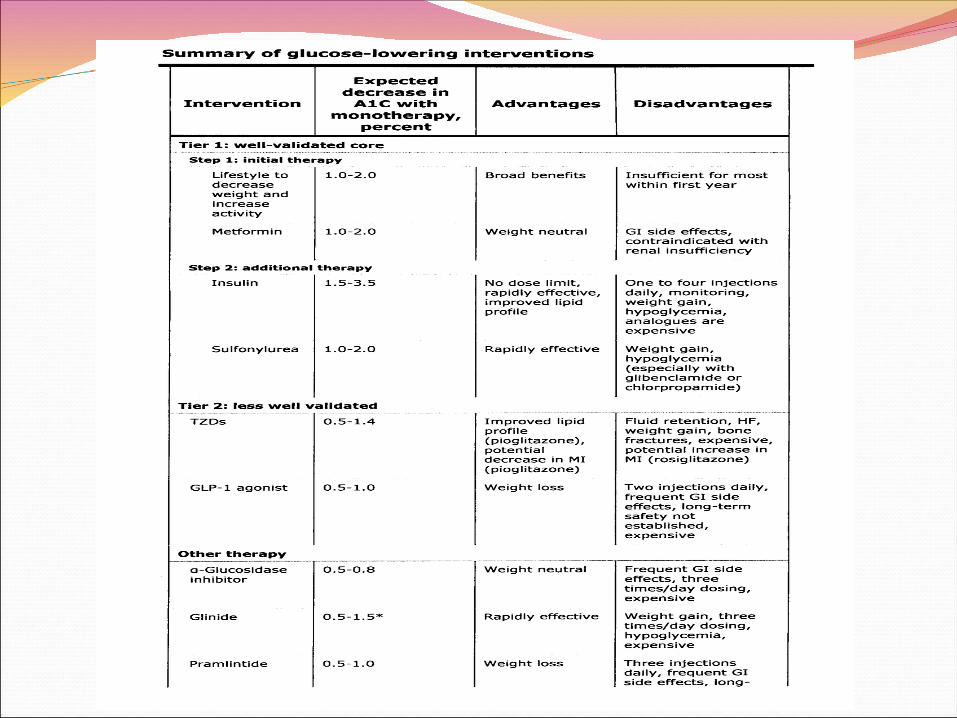
MEDICATIONS FOR INITIAL THERAPY ADA and EASD recommends that
metformin therapy (in the absence of contraindications) be initiated, concurrent with lifestyle intervention, at the time of diabetes diagnosis .
Metformin was chosen for initial therapy because of glycemic efficacy, absence of weight gain and hypoglycemia, general tolerability, and favorable cost.
In patients with contraindications to metformin, the ADA/EASD consensus guideline suggests either insulin or a sulfonylurea
In patients with contraindications to metformin, we suggest a shorter acting sulfonylurea, such as glipizide.
Insulin is also a reasonable option for initial therapy in patients who present with symptomatic or poorly controlled diabetes or in patients in whom it is difficult to distinguish type 1 from type 2 diabetes.
Pioglitazone may be considered in patients with lower initial A1C values or if there are specific contraindications to sulfonylureas.
Metformin reduces A1C by 1.5 percentage points often leads to modest weight reduction
or weight stabilization.reductions in the risk of macrovascular
complications Gastrointestinal side effects are
commonmetformin monotherapy does not
usually cause hypoglycemia.
Metformin Metformin can rarely cause lactic acidosis. metformin should not be administered when
conditions predisposing to lactic acidosis are present.
Such conditions include impaired renal function (plasma creatinine above 1.4 mg/dL in women and 1.5 mg/dL in men), decreased tissue perfusion or hemodynamic instability due to infection or other causes, concurrent liver disease or alcohol abuse, and heart failure.
Metformin Patients who are about to receive
intravenous iodinated contrast material or undergo a surgical procedure (with
potential compromise of circulation) should have metformin held until renal
function and circulation can be established. Serum creatinine is typically assessed two
to three days after contrast administration.
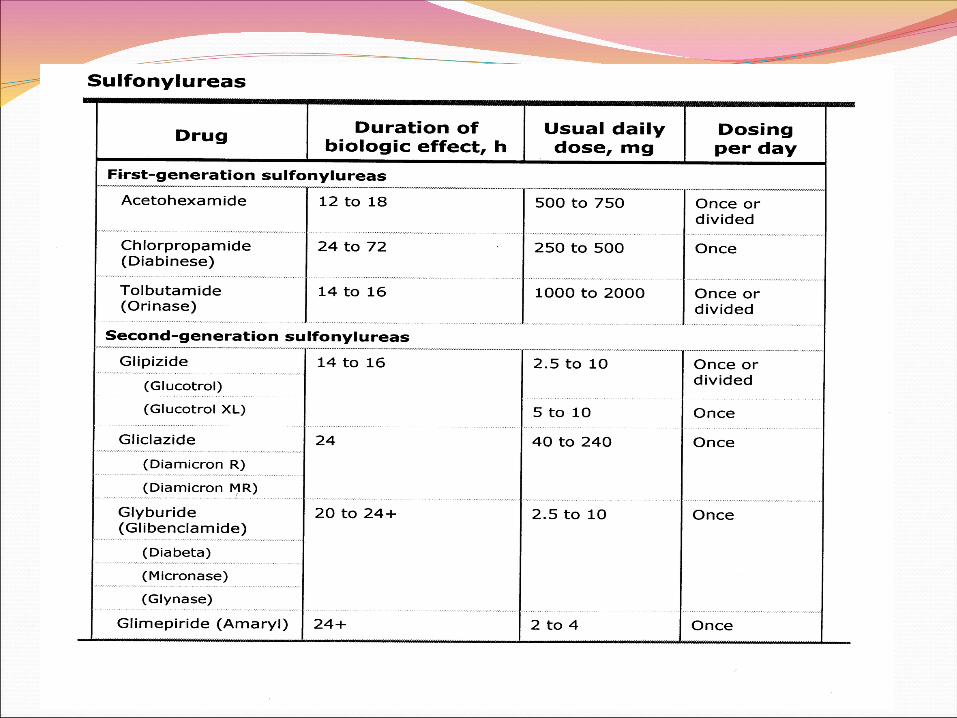
Sulfonylureas Sulfonylureas are the oldest class of oral hypoglycemic agents.
They are moderately effective, lowering blood glucose concentrations by 20 percent and A1C by 1 to 2 percent.
SulfonylureasThe major adverse effect of sulfonylureas is
hypoglycemia.Hypoglycemia induced by long-acting
sulfonylureas may be severe and is often prolonged in the absence of appropriate therapy.
Risk factors for hypoglycemia include increasing age, alcohol abuse, poor nutrition, and renal insufficiency
Shorter acting sulfonylureas, such as glipizide , are less likely to cause hypoglycemia than the older, long-acting sulfonylureas and therefore are the preferred sulfonylureas, especially in older patients.
SulfonylureasIn a patient who is not a candidate for metformin or who cannot tolerate metformin, we suggest a shorter-duration sulfonylurea, such as glipizide.
Meglitinides Repaglinide short-acting glucose-lowering
drug that act similarly to the sulfonylureas and have similar or slightly less efficacy in decreasing glycemia.
Meglitinides are pharmacologically distinct from sulfonylureas and may be used in patients who have allergy to sulfonylurea medications.
They have a similar risk for weight gain as sulfonylureas but possibly less risk of hypoglycemia. However, they are considerably more expensive than sulfonylureas.
Meglitinides Repaglinide is principally metabolized by
the liver, with less than 10 percent renally excreted.
Dose adjustments with this agent do not appear to be necessary in patients with renal insufficiency.
Repaglinide could be considered as initial therapy in a patient with chronic kidney disease who is intolerant of sulfonylureas.
Thiazolidinediones The thiazolidinediones ,pioglitazone, lower blood
glucose concentrations by increasing insulin sensitivity.
lower A1C by 0.5 to 1.4 percentage points They are also associated with more weight gain
and fluid retention than metformin. Are considerably more expensive than generic
sulfonylureas and metformin. Drugs in this class are not recommended in
patients with symptomatic heart failure and are contraindicated in patients with New York Heart Association class III or IV heart failure.
Thiazolidinedioneswe do not generally choose thiazolidinediones for initial therapy and reserve their use for second-line treatment in combination with other anti-diabetic medications where synergistic effects can lower A1C substantially.
Alpha-glucosidase inhibitors Because they act by a different
mechanism, the alpha-glucosidase inhibitors, acarbose and miglitol, have additive hypoglycemic effects in patients receiving diet, sulfonylurea, metformin, or insulin therapy .
This class of drugs is less potent than the sulfonylureas or metformin, lowering A1C by only 0.5 to 0.8 percentage points.
Insulin Although historically insulin has been used for
type 2 diabetes only when inadequate glycemic control persists despite oral agents and lifestyle intervention,
there are increasing data to support using insulin earlier and more aggressively in type 2 diabetes.
By inducing near normoglycemia with intensive insulin therapy, both endogenous insulin secretion and insulin sensitivity improve; this results in better glycemic control, which can then be maintained with diet, exercise and oral hypoglycemics for many months thereafter.
Insulin Insulin therapy in type 2 diabetes is initially aimed at increasing basal insulin concentrations .
Patients with type 2 diabetes require relatively large doses of insulin, compared with those needed for type 1 diabetes.
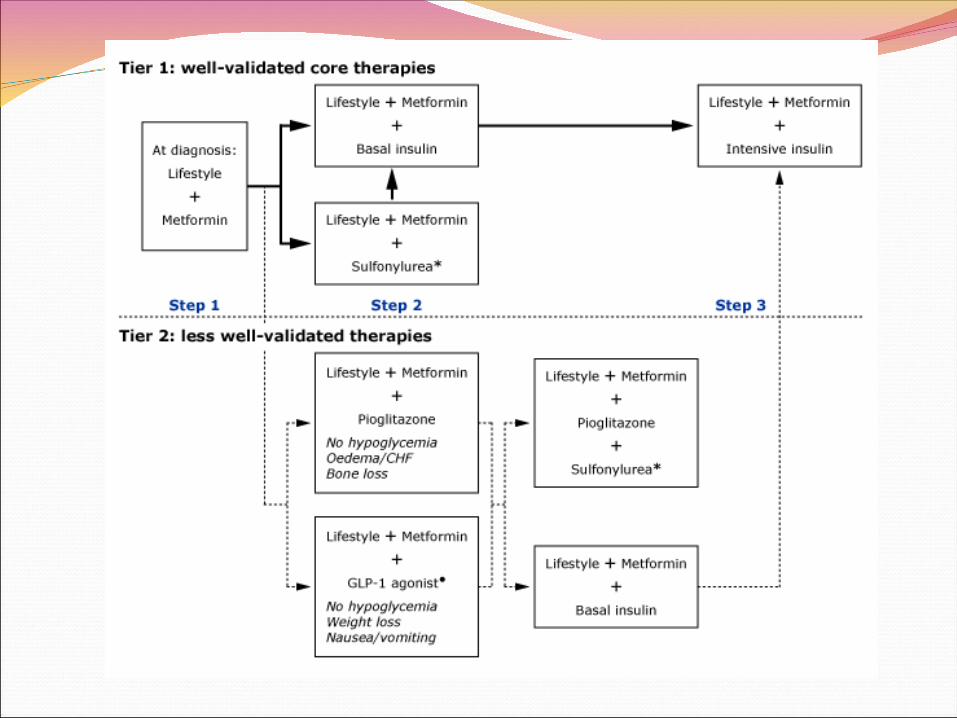
Management of persistent hyperglycemia in type 2 diabetes mellitusADA and EASD consensus guideline for
pharmacotherapy to control hyperglycemia in type 2 diabetes recommends testing A1C levels every three months and addition of a second medication when the treatment goal of A1C <7 percent with metformin plus lifestyle intervention is not achieved within three months .
In order to achieve the A1C goal, the glucose goals below are usually necessary:
• Fasting glucose 70 to 130 mg/dL • Postprandial glucose (90 to 120 minutes after
a meal) <180 mg/dL
TREATMENT OPTIONSThe guidelines favor insulin or sulfonylurea as
the second step, and insulin is preferred for patients whose A1C is further from target (>8.5 percent) or who have symptoms related to hyperglycemia.
If target A1C is not achieved with metformin, and sulfonylurea or basal insulin, the ADA/EASD suggest starting or intensifying insulin therapy.
In patients on sulfonylureas and metformin who are starting insulin therapy, sulfonylureas are generally tapered and discontinued.
TREATMENT OPTIONSThiazolidinediones (TZDs) are not
considered first choice agents due to the risk of CHF and fractures and expense.
As an example, in a patient who would be at particularly high risk if hypoglycemia occurred (eg, a construction worker) and inadequate glycemic control on metformin (A1C >7 but <8.5 percent), pioglitazone could be used.
TREATMENT OPTIONSFor those close to target, we prefer
to add a shorter-duration sulfonylurea (such as glipizide, to reduce the risk of hypoglycemia compared with longer-acting sulfonylureas), rather than insulin.
For those further from target (A1C >8.5 percent) we prefer to add insulin, rather than an oral agent.
Metformin monotherapy failureIn patients with inadequate glycemic control on metformin and A1C >8.5 percent, we suggest adding insulin .
In patients with inadequate glycemic control on metformin (A1C >7.0 percent), with A1C close to target (≤8.5 percent), we suggest adding a short acting sulfonylurea, such as glipizide .
Metformin monotherapy failureThe addition of pioglitazone is an alternative
option in individuals without risk factors for heart failure or fracture, who do not reach glycemic goals with metformin alone, if there are contraindications to sulfonylureas or patient preference limits the use of sulfonylureas or insulin .
Another reasonable alternative is the addition of repaglinide, which can be considered in individuals who do not reach glycemic goals with metformin, if there are contraindications to sulfonylureas or patient preference limits the use of insulin .
Contraindications to metformin and sulfonylurea monotherapy failure In individuals with contraindications to
metformin, sulfonylureas are often first-line therapy.
In patients with inadequate glycemic control on sulfonylureas, with A1C >8.5 percent, we suggest switching to insulin .
In patients with inadequate glycemic control on sulfonylureas (A1C >7 percent), with A1C close to target (≤8.5 percent), we suggest adding pioglitazone .
Dual oral agent failureIn individuals with inadequate glycemic
control (A1C >7 percent) on two oral agents (usually metformin and sulfonylurea), we suggest switching to insulin (discontinue sulfonylurea and continue metformin) .
alternative that is less likely to work is three oral agents.
However, three oral agents (metformin, sulfonylurea, pioglitazone) can be considered in patients with A1C values that are not too far from goal (A1C ≤8.5 percent).
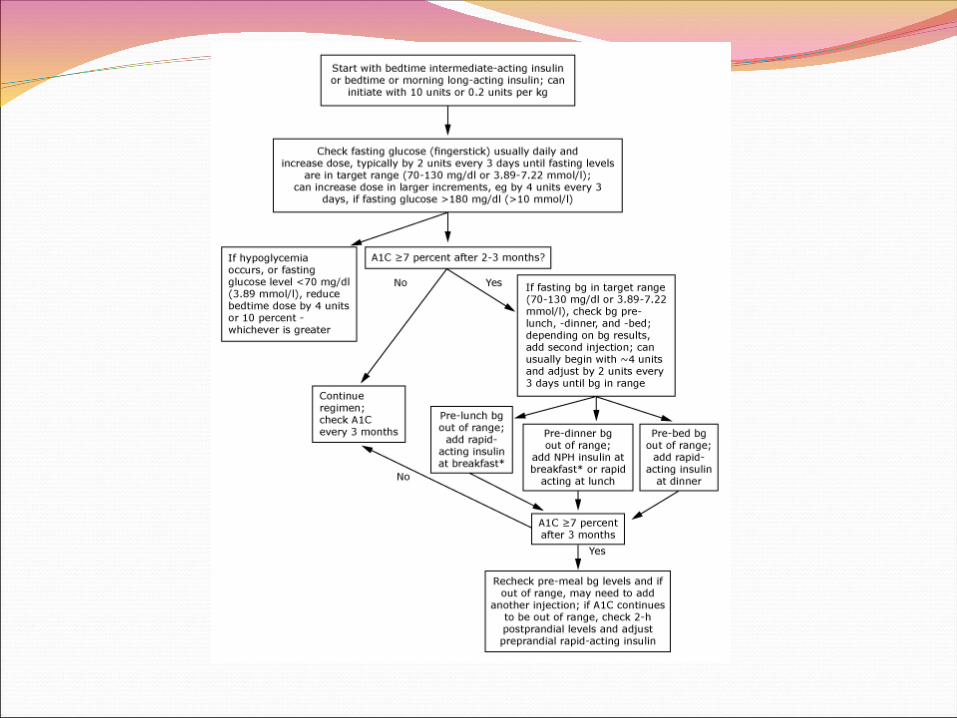
Combination oral and insulin therapy While NPH has been used commonly at bedtime to supplement oral hypoglycemic drug therapy, longer acting insulins, such as insulin glargine (once daily) added to oral agents are similarly effective for reducing A1C values and may cause less nocturnal hypoglycemia.
Insulin therapy in type 2 diabetes mellitusIf once per day insulin is added to oral hypoglycemic therapy in patients with type 2 diabetes, insulin NPH given at bedtime or insulin glargine given in the morning or at bedtime is a reasonable initial regimen.
Insulin therapy in type 2 diabetes mellitusWhen switching to insulin monotherapy, it is reasonable to begin with a similar regimen consisting of basal insulin (NPH or glargine insulin) given once or twice daily .
Subsequent modifications can be made according to blood glucose and A1C values.
Insulin therapy in type 2 diabetes mellitus Insulin can be considered initial therapy for all patients with type 2 diabetes, particularly patients presenting with A1C >10 percent,
fasting plasma glucose >250 mg/dL
random glucose consistently >300 mg/dL
or ketonuria.
Insulin therapy in type 2 diabetes mellitus A potential problem is that patients who
are initially thought to have type 2 diabetes may actually have type 1 diabetes, and therefore require insulin as initial therapy.
In patients in whom it is difficult to distinguish type 1 from type 2 diabetes (patients who are underweight, are losing weight, or are ketotic), initial treatment with insulin is required.
Insulin therapy in type 2 diabetes mellitus Although we do not recommend premixed insulin for the treatment of type 1 diabetes, it is a reasonable option for patients with type 2 diabetes who are doing well on a stable, fixed ratio.