Embed Size (px)
Citation preview

In the Clinic: Evidence Based Management of Infections
Daniel Deck, Pharm.D.
San Francisco General Hospital

Overview
Community-acquired pneumonia
Upper respiratory tract infections
Urinary tract infections
Skin and Soft-tissue infections

Community-acquired pneumonia

Community Acquired Pneumonia (CAP): definition
At least 2 new symptoms
New infiltrate on chest x-ray and/or abnormal chest exam
No hospitalization or other nursing facility prior to symptom onset
Fever or hypothermia Cough
Rigors and/or diaphoresis Chest pain
Sputum production or color change Dyspnea
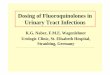
Diagnosis Chest radiograph – needed in all cases?
Avoid over-treatment with antibiotics
Differentiate from other conditions
Specific etiology, e.g. tuberculosis
Co-existing conditions, such as lung mass or pleural effusion
Evaluate severity, e.g. multilobar
Unfortunately, chest physical exam not sensitive or specific and significant variation between observers Arch Intern Med 1999;159:1082-7

Microbiological Investigation
Sputum Gram stain and cultureRemains somewhat controversial
30-40% patients cannot produce adequate sample
Most helpful if single organism in large numbers
Usually unnecessary in outpatients
Culture (if adequate specimen < 10 squamous cells/LPF; > 25 PMNs/LPF): antibiotic sensitivities
Limited utility after antibiotics for most common organisms

Etiology Clinical syndrome and CXR not reliably predictive
Streptococcus pneumoniae 20-60%
Haemophilus influenzae 3-10%
Mycoplasma pneumoniae up to 10%
Chlamydophila pneumoniae up to 10% “Atypicals”
Legionella up to 10%
Enteric Gram negative rods up to 10%
Staphylococcus aureus up to 10%
Viruses up to 10%
No etiologic agent 20-70%
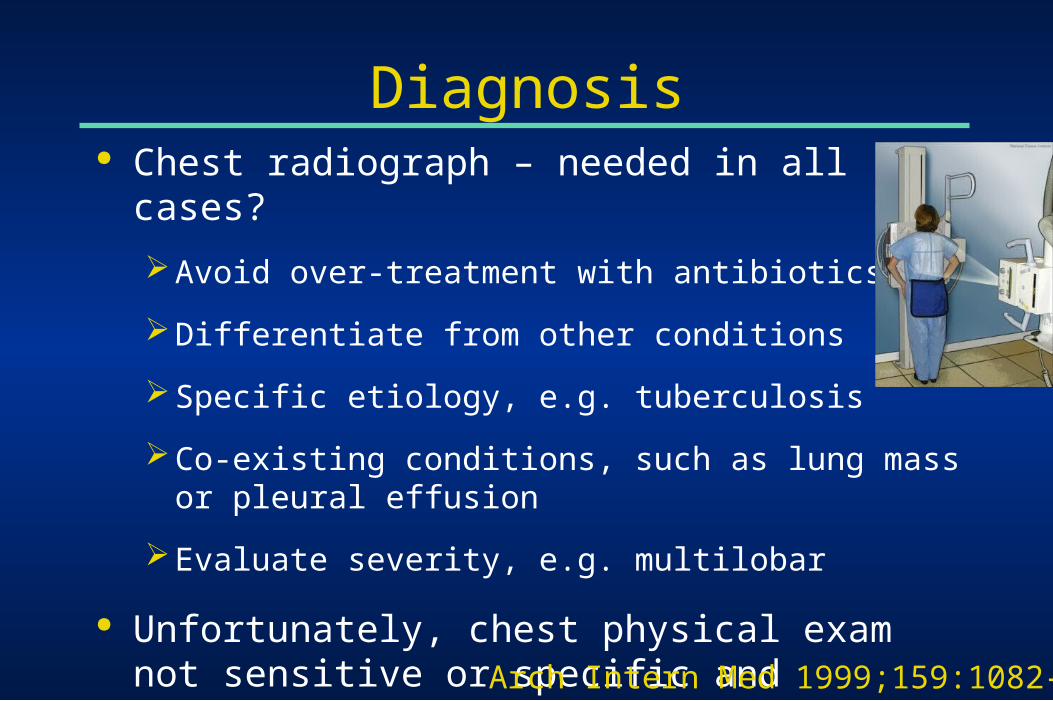
S. pneumoniae
2/3 of CAP cases where etiology known
2/3 lethal pneumonia
2/3 bacteremic pneumonia
Apx. 20% of cases with pneumococcal pneumonia are bacteremic (variable)
Risk factors include
Extremes of ageAlcoholismCOPD and/or smokingNursing home residence
InfluenzaInjection drug useAirway obstruction*HIV infection

S. pneumoniae – drug resistance
~ 25-35% penicillin non-susceptible by old standard nationwide, but most < 2 g/mL
Using the new breakpoints for patients without meningitis, 93% would be considered susceptible to IV penicillin
Other beta-lactams are more active than pencillin, especially
Ceftriaxone, cefotaxime, cefepime, amoxicillin, amoxicillin-clavulanate

S. pneumoniae – drug resistance Other drug resistance more common with increasing
penicillin minimum inhibitory concentration (MIC)
Macrolides and doxycycline more reliable for PCN susceptible pneumococcus, less for penicillin non-susceptible
Trimethoprim-sulfamethoxazole not reliable
Fluoroquinolones – most S. pneumoniae are susceptible
Clinical failures have been reported
No resistance with vancomycin, linezolid

Risk Factors for Drug-Resistant Pneumococcal Pneumonia
Age < 2 year or > 65 years
-lactam antibiotics within 3 months
Alcoholism
Immunocompromised patients
Multiple comorbidities
Exposure to children in day care centers

Conditions that Increase the Morbidity/Mortality of CAP
COPD
Alcoholism
Leukopenia
Bacteremia
Diabetes mellitus
Renal insufficiency
CHF
CAD
Malignancy
Neurologic disease
Chronic liver disease
Immunosuppression

IDSA Outpatient Empiric Therapy Recommendations
Previously Healthy & Previously Healthy & NONO DRSP Risk FactorsDRSP Risk Factors
DRSP Risk Factors DRSP Risk Factors oror High Level High Level Macrolide Resistance > 25%Macrolide Resistance > 25%
Macrolide (e.g azithromycin)Macrolide (e.g azithromycin)
oror
DoxycyclineDoxycycline
1) Fluoroquinolone1) Fluoroquinolone** oror
2) a 2) a ββ-Lactam-Lactam## plusplus
a Macrolide or Doxycyclinea Macrolide or Doxycycline
*moxifloxacin, gemifloxacin, or levofloxacin (750mg)*moxifloxacin, gemifloxacin, or levofloxacin (750mg)##Amoxicillin 1 gm PO tid or Augmentin® XR 2 gm PO bid are preferred. Ceftriaxone, Amoxicillin 1 gm PO tid or Augmentin® XR 2 gm PO bid are preferred. Ceftriaxone,
cefpodoxime proxetil, and cefuroxime axetil 500 mg PO bid are alternativescefpodoxime proxetil, and cefuroxime axetil 500 mg PO bid are alternatives

We love doxycycline
Adult inpatients June 2005 – December 2010
Compared those who received ceftriaxone + doxycycline to those who received ceftriaxone alone
2734 hospitalizations: 1668 no doxy, 1066 with doxy
Outcome: CDI within 30 days of doxycycline receipt
CDI incidence 8.11 / 10,000 patient days in those receiving ceftriaxone alone; 1.67 / 10,000 patient days in those who received ceftriaxone and doxycycline
Doernberg et al, Clin Infect Dis 2012;55:615-20

Duration of Therapy
5 days should be the minimum duration of therapy
Patients should be afebrile for 48-72 hours
No more than 1 CAP-associate sign of clinical instability (T > 37.8ºC, HR >100, RR > 24, SBP < 90, O2 sat < 90%, pO2 < 60)

Short-Course Therapy
Defined as less than 7 days of therapy
Short course therapy may reduce side effects, cost, and resistance
Azithromycin has been used for 3-5 days
Ceftriaxone, amoxicillin, and fluoroquinolones have been used for 5 days

Reasons for Inadequate Response to Empiric Therapy
Inadequate Antibiotic Selection
Unusual Pathogens
Complications of Pneumonia
Incorrect Diagnosis
Drug-resistant organisms

Upper Respiratory Tract Infections

Upper respiratory tract infections
Rhinosinusitis
~13 million outpatient visits per year
Viral causes >>>> bacterial
Minimal to NO benefit from antibiotics given for short duration of disease
Xray/CT not helpful in distinguishing cause

Rhinosinusitis diagnosis
Major Criteria Purulent anterior nasal discharge
Purulent posterior nasal discharge
Nasal congestion or obstruction
Facial congestion or fullness
Facial pain or pressure
Hyposomia or anosmia
Fever (acute disease)
Minor Criteria Headache
Ear pain, pressure, or fullness
Halitosis
Dental pain
Cough
Fever (chronic disease)
Fatigue
Need at least 2 major or 1 major and ≥ 2 minor criteria

IDSA guidelines: rhinosinusitis
Antibiotics may be helpful if….
1. Persistent signs/symptoms > 10 days
2. Severe symptoms
Fever > 39C
Purulent nasal drainage for 3 consecutive days
Facial pain
3. Biphasic illness

IDSA guidelines: rhinosinusitis
Recommened 1st line therapy =
Amoxicillin/clavulante (standard dose)
Consider high dose (XR formulation) with severe disease, elderly, recent antibiotic use or hospitalization
Alternatives: doxycycline, levofloxacin
Treatment duration: 5-7 days
Not Recommended
• Macrolides
• TMP/SMX
• Oral cephalosporins
• Routine MRSA coverage

IDSA guidelines: rhinosinusitis
DO Antibiotic duration 5-7 days
Nasal saline irrigation
Intranasal corticosteroids
Consider changing abx if
Clinically worse at 48-72 hours
No improvement at 3-5 days
DO NOT Decongestants
Antihistamines
NP swab

GAS pharyngitis
Accounts for 15% of adult sore throat visits
Dx: culture or rapid antigen test
Tx :
1st line = PCN or amoxicillin x 10 days
Mild PCN allergy = cephalexin x 10 days
Alternatives = clindamycin or clarithromycin x 10 days OR azithromycin x 5 days

Antibiotic allergies: History is key!
Past reaction Source
Timeline: symptoms & meds
Detailed description
Treatment
Concurrent illness
Workup
Other exposure
Current reaction Timeline: symptoms & meds
Labs, histology
Concurrent illness

Algorithm for the use of cephalosporins in patients with reported penicillin allergy
Practical management of antibiotic allergy in adults. McLean-Tooke et al, J ClinPathol 2011;64:192-199

Acute bronchitis
10 million healthcare visits annually
80% of patient prescribed antibiotics
95% of case have a viral etiology
Antibiotics = No clinical benefit plus increased cost, adverse reactions, increased antibiotics resistance

Skin and Soft Tissue Infections

Skin Infection Anatomy
Epidermis
Dermis
Subcut. Fat
Fascia
Muscle
Impetigo
Erysipelas
Cellulitis
Abscess, furuncle, carbuncle
Fasciitis
Pyomyositis

S. pyogenes Resistance in the U.S. 2002-2003
Antimicrobial Agent Percent Resistant*
Penicillin 0.0%
Cefdinir 0.0%
Clindamycin 0.5%
Erythromycin 6.8%
Azithromycin 6.9%
Clarithromycin 6.6%
Levofloxacin 0.05%
*Richter SS. Clinical Infectious Diseases 2005; 41:599–608

S. aureus Susceptibilities from Outpatient Wound Isolates
Antimicrobial Agent Percent Susceptible*
Oxacillin 52.0%
Trimethoprim-Sulfamethoxazole 99.6%
Clindamycin 86.7%
Erythromycin 41.5%
Tetracycline 93.8%
Vancomycin 100%
*http://ww2.cdph.ca.gov/PROGRAMS/MDL/Pages/CaliforniaAntibiogramProject.aspx

Risk Factors for CA-MRSA
Prior history of MRSA infection
Close contact with person with similar infection
Recent antibiotic use
Reported “spider bite”
Outbreaks in IVDU, prisoners, athletes, children, Native Americans

Cellulitis vs Abscess
Cellulitis Abscess Pathogen Beta-hemolytic streptococci Staph aureus (CA-MRSA)
Treatment Antibiotics Incision and Drainage+/- ABX
Antibiotics • Penicillin (amoxicillin)• Cephalosporins (cephalexin)• Clindamycin (PCN allergic)• TMP/SMX???
• TMP/SMX • Doxycycline • Clindamycin • Linezolid $$$
Duration 5-10 days; monitor clinical response

Abscess: when to prescribe abx?
Antibiotics may be warranted if
Abscess is large (> 5 cm) or incompletely drained
Significant surrounding cellulitis
Systemic signs and symptoms of infection are present
Patient is immunocompromised
Difficult to drain area (face, hand, genitalia)
Extremes of age

Animal & Human Bite Wounds
One half of all Americans bitten in their lifetime
80% of wounds are minor, 20% require medical care
Human and cat bites frequently become infected so always require treatment even if not grossly infected
Only 5% of dog bites get infected so treatment indicated if bite is severe, grossly infected, or significant comorbidity (e.g. diabetes)

Bite Wound Treatment
Wound cleaning, irrigation and debridement!
Antibiotics directed against skin flora of patient and oral flora of biting animal/human
Humans (viridans strep, Eikenella, mixed anaerobes)
Dogs (Pasteurella, Capnocytophaga, anaerobes)
Cats (Pasteurella, anaerobes)
Antibiotic Regimens
Oral
Amoxicillin/clavulante 875/125 mg BID
Clindamycin + Fluoroquinolone OR TMP/SMX
IV : Ampicillin/sulbactam 1.5G Q6h

Urinary Tract Infections
Increasing resistance in urinary pathogens
E.coli accounts for ~95% of all cases
TMP/SMX resistance in E.coli > 20% in many parts of the United States
Resultant shift to use of quinolones as first-line empirical therapy over the past 10-20 years
Quinolones have been associated with “collateral damage”
Increased rates of MRSA
Selection for resistant GNRs including ESBL- producers
Clostridium difficile-associated diarrhea

When to get a culture?
Suspect multidrug-resistant organism
Recent abx
Prior infection or colonization
Recent travel
Suspect pyelonephritis
Follow up cultures unnecessary in patients whose symptoms resolve

2010 IDSA recommended treatment regimens for uncomplicated cystitis
First Line Regimens Nitrofurantoin macrocrystals
(Macrobid®) 100 mg BID X 5 days (avoid if early pyelo suspected)
Trimethoprim-sulfamethoxazole 1DS tablet BID X3 days (avoid if resistance prevalence exceeds 20% or if used for a UTI in previous 3 months)
Fosfomycin trometamol 3 grams x 1 dose (lower efficacy than some other agents, avoid if early pyelo suspected)
Second Line Regimens Ciprofloxacin 500 mg BID x 3 days
(resistance prevalence high in some areas)
Oral β-lactams (including amoxicillin/clavulante, cefdinir, cefaclor, cefpodoxime, cephalexin (less data); avoid ampicillin or amoxicillin alone; lower efficacy than other available agents, treat for 3 to 7 days)
Gupta K et al. Clin Infect Dis. 2011;52(5):103-20.

What is fosfomycin? Phosphonic acid derivative that inhibits cell wall synthesis
Activity against many gram positive and gram negative organisms
In U.S., only oral salt available as a powder sachet dissolved in water
High concentration in the urine
Usual dose 3g x 1 (single dose)
Can also consider 3g every other day x 3 doses or 3g q 72 hrs. x 14 days
3g packet costs about $50

Treatment of cystitis: Back to the future
Nitrofurantoin (Macrobid®)
PROS
As effective as TMP/SMX
Minimal drug resistance
Low propensity for collateral damage
CONS
Blood levels not sufficient to treat early pyelonephritis
Avoid in pts with CrCl < 50 ml/min
Nausea, headache (similar adverse effect rate as TMP/SMX)
Rare pulmonary hypersensitivity
Fosfomycin trometamol
PROS
Clinical efficacy similar to TMP/SMX
Low propensity for collateral damage
Single dose therapy
CONS
Microbiologic efficacy lower than TMP/SMX and nitrofurantoin
Not sufficient to treat early pyelo
Susceptibility testing not routinely performed
Diarrhea, nausea, headache (similar adverse effect rate as nitrofurantoin)

Other oral options for cystitis due to resistant organisms
Amoxicillin-clavulanate (susceptible ESBL-producing E. coli)
Nitrofurantoin
Fosfomycin references:
Falagas et al, Lancet Infect Dis 2010;10:43-50
Neuner et al, Antmicro Agents Chemother 2012;56:5744-48

Asymptomatic Bacteriuria
Do not screen if no symptoms are present
Except in pregnancy
Other special situations
Do not prescribe antibiotics!
Relative Risk ~3x for recurrence of symptomatic bacteriuria when asymptomatic patients receive antibiotics

Final Questions?
Contact Info
Extension: 415-206-5574
Email: [email protected]
SFGH “As real as it gets”