Embed Size (px)
Citation preview

In situ substantivity of the essential oils in the oral cavity
I. Prada-López1, V. Quintas1, N. Donos2, M. Álvarez-Fernández3 and I. Tomás1
1Oral Sciences Research Group. School of Medicine and Dentistry. Santiago de Compostela University. Spain. 2Periodontology Unit. UCL Eastman Dental Institute. London. United Kingdom. 3Microbiology. CHUVI, Xeral-Cíes Hospital. IBIV. Spain.
The proven antimicrobial and anti-inflammatory activities of Essential Oils (EO) led, in 1879, to their combination with a phenolic based formula to reach a higher potential. This new product was called Listerine®. After that, it gradually acquired more importance as an oral antiseptic until nowadays, when it is considered the most popular phenolic compound used in the oral cavity. Due to this, the number of studies about its mechanism of action has been increasing, especially in the last decade. The antiseptic activity of EO comes from their hydrophobicity, which produces a disturbance in the bacterial membrane that affects diverse cellular compounds causing a cascade effect. One of the ideal characteristics that antiseptics must have is the ability to adhere to the substrate and persist at effective concentrations, which is called substantivity. The purpose of this chapter is to review the previously published studies about the in situ antibacterial activity and substantivity of the EO in different oral micro-niches, as well as presenting our own results in this field.
Up to now, there have been no papers published comparing the EO antibacterial activity with that of Chlorhexidine (CHX) –the Gold-standard- after a single application, and there are only few cases in which the immediate antibacterial activity of the EO was evaluated. Thus, there are some published papers about the substantivity of EO in the saliva, which concluded that these last ones kept lower bacterial vitality levels than the negative control between 1-5 hours after their application; nevertheless, there are few papers which have studied the in situ antibacterial activity of the EO on structured biofilm and, in those cases, their application was performed ex vivo. What is common to most of the papers is the using of the Confocal Laser Scanning Microscope (CLSM) technique combined with a staining solution. This is due to its consideration as an effective technique when analysing both the structure and the bacterial viability in an oral biofilm.
Consequently, it seems to be interesting and necessary to continue studying the EO antibacterial activity with CLSM techniques. The methodology should be directed to in situ antiseptic application, and the results obtained should be compared with other antiseptics. Thereby, a more reliable approach about the ability of EO as oral antiseptics could be obtained.
Keywords essential oils; Listerine; substantivity; oral biofilm; bacterial viability; confocal laser scanning microscopy; staining.
1. Introduction
Since ancient times, essential oils (EO) have been used for the treatment of a large variety of diseases all over the world, from the Egyptians to the Mayans or Aztecs [1]. In 1879, Dr Josep Lawrence and the pharmacist Jordan Wheat Lambert developed a phenolic compound [2] whose antimicrobial activity was enhanced by the combination with some EO (Thyme, Eucalyptus, Baptisia, Gahulteria and Mentha Arvensis) [3]. This formula was called Listerine® in honour of Sir Joseph Lister, father of the antisepsis in medicine [4]. Although it had been designed as an antiseptic for surgeries and its antimicrobial abilities had also been demonstrated, it had a poor acceptance among the surgical medicine field. It soon acquired other indications such as: treatment of gonorrhoea, floor cleaner, anti-dandruff solution, aftershave lotion or remedy for baldness. After that, it was observed that it was especially effective against microorganisms commonly found in the oral cavity. As a result, in 1895, Lambert extended the sale and promotion of his product to the dental profession [2]. It was his son, Gerald, who introduced the product to Americans as a palliative for halitosis, becoming so popular that in 1914 was one of the first prescription oral products and technically reached the category of mouthwash. By this time, the oils included in the original formula had been already replaced by eucalyptol, thymol, menthol and methyl salicylate - the latter two are replaced by synthetic derivatives today [5]. In the decades of the 70s and 80s, it started to be considered a mouthwash against not only for halitosis but for other oral diseases [6]. This was confirmed in 1986 when the American Dental Association approved them for the control of the dental plaque and gingivitis [7] based on some existing studies that satisfied their criteria [8-11]. Nowadays, Listerine® is widely used all over the world and has been used by millions of customers, particularly in the United States [12]. Furthermore, it has been considered as effective and safe by the Expert Committee in Oral Health of the Food and Drug Administration (FDA) [13]. One of the most important characteristics of EO is their ability to adhere to the substrate and persist at effective concentrations, which is called substantivity. The purpose of this chapter is to review the findings published in the literature on the in situ antibacterial activity and substantivity of EO in the oral cavity, and to report our own results in this field.
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
1112
2. General characteristics of the essential oils
The EO are natural products that plants produce for their own needs. Different types of techniques are used to extract them which include: microwaves, liquid carbon dioxide or steam distillation [1, 14]. At present, the pharmaceutical industry has replaced plant extraction by chemical synthesis in case its natural production is difficult [5].
2.1. Chemical structure
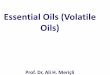
They can be classified in two groups: terpenes (and terpenoids) or aromatic derivatives (Fig. 1). The first are the most common group and are characterised by an extensive variety in their structural groups [15]. In this group there are also terpenoids which are terpenes with an oxygen group. The second group is based on an aromatic compound that, being less common than terpenes, comes from phenylpropane by-products.
Fig. 1 Chemical formulas exemplifying the different types of EO.
2.2. Physical properties
They are volatile and water-insoluble, which makes the determination of their antibacterial effect very difficult [16]. Moreover, their high hydrophobicity and viscosity cause an irregular distribution when testing this antiseptic activity. Due to this, it is always necessary to use a solvent agent to prevent the unequal dilution in the culture medium [17].
2.3. Mechanism of antibacterial action
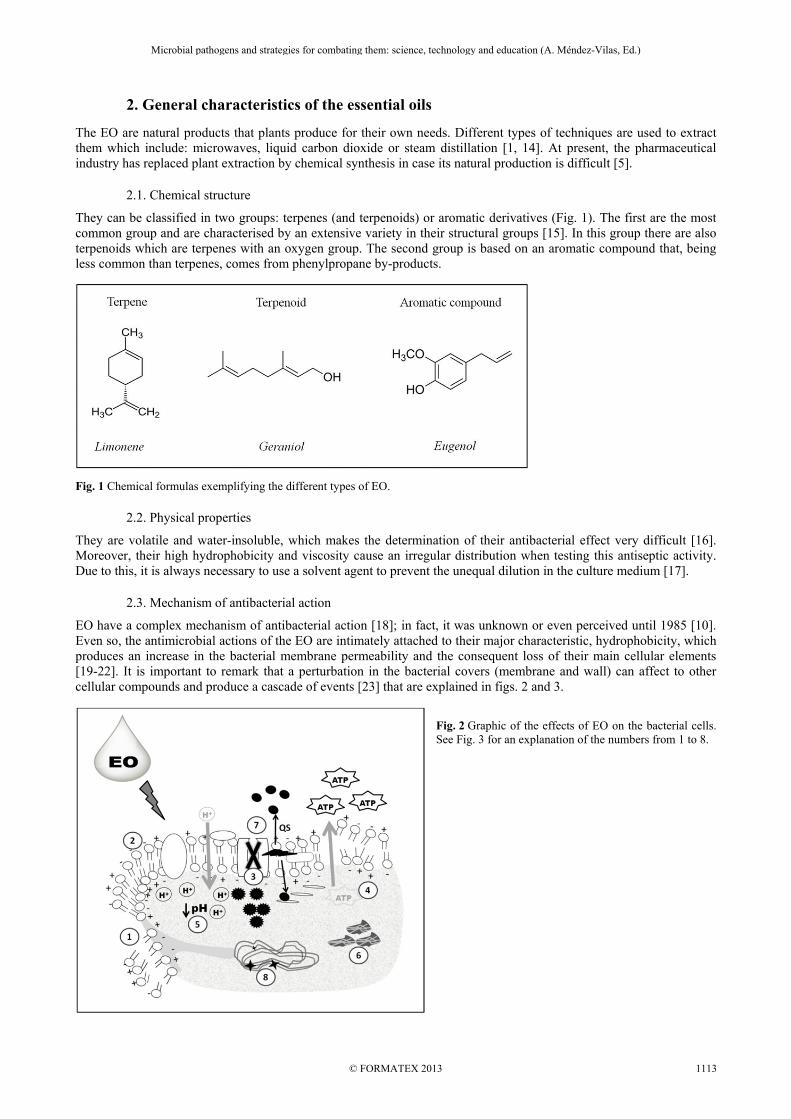
EO have a complex mechanism of antibacterial action [18]; in fact, it was unknown or even perceived until 1985 [10]. Even so, the antimicrobial actions of the EO are intimately attached to their major characteristic, hydrophobicity, which produces an increase in the bacterial membrane permeability and the consequent loss of their main cellular elements [19-22]. It is important to remark that a perturbation in the bacterial covers (membrane and wall) can affect to other cellular compounds and produce a cascade of events [23] that are explained in figs. 2 and 3.
Fig. 2 Graphic of the effects of EO on the bacterial cells. See Fig. 3 for an explanation of the numbers from 1 to 8.
[24] [25] [21, 26] [21, 27][28][29, 30]
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
1113

Fig. 3 Scheme of the mechanism of antibacterial action of the EO.
2.4 Chemical composition of Listerine®
The exact composition of Listerine® (Cool Mint) is an aqueous-ethanolic solution (21.6%-26.9%), which serves as a vehicle of a combination of four EO: eucalyptol, thymol, methyl salicylate and menthol (see Table 1) [5, 18, 31, 32]. Table 1 Listerine containing EO with its chemical structure, natural origin, chemical synthesis, pharmaceutical properties and its concentration.
Name Chemical Structure
Natural Origin Chemical Synthesis Pharmaceutical
Properties Concentration in
Listerine
Eucalyptol
C10H18O
Eucalyptus globulus
Ø Anaesthetic & antiseptic
0.092%
Thymol
C10H14O
Thymus vulgans Phenolic Alquiderivate Bactericide &
fungicide 0.064%
Methyl Salicilate
C8H8O3
Gaultheria and/or Betülla
Esterification of salicylic acid with methanol
Antiseptic 0.06%
Menthol
C10H20O
Mentha arvensis Hydrogenation of thymol Antiseptic 0.042%
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
1114

3. In situ antimicrobial activity of EO in different oral ecosystems
Study of the antibacterial activity of an antiseptic involves an analysis of its immediate effect and substantivity. This term is defined as the prolonged adherence of the antiseptic to the oral surfaces (teeth and mucosa) and its slow release in effective doses, that guarantee the persistence of its antimicrobial activity [33]. This property is essential for an antiseptic to be clinically effective. Although in vitro studies do not have to be predictive of clinical activity, they may elucidate its subsequent mechanism and guide the objectives of the in situ studies. Thereby, in vitro studies, whose objective is to determine the antimicrobial activity of the EO, can be found in the literature. In this same way, Fine et al. [34] concluded that a single application of EO could achieve a decrease in the bacterial charge of up to 97%, and for Streptococcus spp. this was up to 99.7%. In other studies, their results are compared with those of CHX with diverse conclusions depending on the consulted paper. That is the case of the study of Pan et al. [35] who found that after a 60 second-single application of EO and CHX, the former was 57.5% more effective than CHX. In the contrary, Sliepen et al. [36] concluded that CHX reduced the bacterial vitality in a higher proportion than the EO. However, the scientific community recognises that in vitro oral biofilms are not comparable to those formed in situ [37-39]. For this reason, some authors consider that the results of in vitro studies should be interpreted with caution [37, 40, 41] and highlight the necessity of the development of in situ biofilm models that permit their posterior analysis without being disturbed [37, 41-43]. To achieve a better understanding of the clinical effects that the antiseptic agents produce on the oral biofilm is necessary to apply a methodology in which this biofilm can directly grow inside the oral cavity. Moreover, its three-dimensional structure should not be distorted with manipulation [44, 45].
3.1. In situ antimicrobial activity of the EO on salivary flora
The analysis of the salivary flora provides information on antiseptic agent antimicrobial activity and is considered to be predictive of its substantivity [46, 47]. This is due to the ability of the saliva to be a microorganism dissemination medium inside the oral cavity, since it wets the entire inner mouth surface. For this reason, Weiger et al. [48] suggested that the first phenomena of microbial colonisation after contact with a clean tooth surface occur mainly due to the adhesion of salivary bacteria. However, other authors argued that a single determination of the reduction in the bacterial load in saliva does not demonstrate any correlation with effects on plaque inhibition [49].
3.1.1. Methodological approach
In the majority of published studies, the quantification of the antimicrobial activity of EO in saliva was performed using plate culture microbiological techniques [34, 50-53]. However, some authors have questioned the reliability of this methodology [54], reporting numerous difficulties that could underestimate the bacterial vitality [55] or, in some cases, overestimate specific bacterial genera. As a consequence, the epifluorescence microscopy technique (Fig. 4) with specific fluorochromes such as LIVE/DEAD® BacLight™ [55, 56], has been posed as an alternative for the plate culture techniques. This fluorescent solution detects bacterial viability based on the integrity of the cytoplasmic membrane. The combination of fluorochromes offers the possibility of staining live and dead bacteria in a selective manner. That is why they have been widely used to analyse bacterial viability before and after the application of oral antiseptics such as CHX on saliva [57, 58] or EO on oral biofilm [59, 60] (no data has been found over its use on saliva after the application of EO). The main advantages of this technique include: the rapidity and simplicity of the technique, which quantifies bacterial viability in real-time [55]; the SYTO-9/propidium iodide dual staining allows vital and non-vital bacteria to be counted simultaneously [55]; and the possibility of detecting bacteria that cannot be cultured using plate culture techniques [54, 61].
Fig. 4 Images from epifluorescence microscope, bacterial viability shown before and after a mouthwash. Note the predominance of green in the image before the mouthwash (live bacteria) and after rinsing, when there is a predominance of red (dead bacteria).
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
1115

3.1.2. Immediate effect and substantivity of EO in saliva
As previously stated, published data about EO substantivity have been obtained through culture plate techniques, measuring the CFU/mL. There are only two articles which studied the immediate effect and the substantivity of the EO in saliva. DePaola et al. [51] stated that the EO might have clinical utility as a pre-procedural rinse to decrease the level of viable microorganisms in aerosols generated during dental procedures. They studied its activity on saliva after 2, 5, 15, 30 and 60 minutes, concluding that a single EO mouthwash decreased, at 2 minutes, up to 60-65% the bacterial counts with regard to the baseline, keeping its effects for at least until 1 hour after a single application, and obtaining a 44-48% decrease in the bacterial vitality in comparison to the basal sample. Jenkins et al. [50] studied the antibacterial activity and its permanence on salivary microbiota in 14 volunteers using five different mouthwashes. They concluded that the effect at 30 minutes after EO mouthwash significantly decreased the bacterial counts in regard to the baseline. The antimicrobial effect of the EO was already patent 7 hours after a single application, with this effect being lower than 0.2% CHX. Other authors studied the EO mouthwashes used daily for a short period of time. Botelho et al. [53] added some clinical indexes to the plaque culture techniques to compare the effect of rinsing with EO or CHX after 7 days. There was a decrease in all analysed indexes and Streptococcus mutans in saliva with regard to the basal in both mouthwashes, with their effects being quite similar. Other results partially related to this are those obtained by the group of Fine [34], which they showed a decrease of 50.8% in Streptococcus spp. in comparison to the negative control after 11 days rinsing twice a day with a containing EO mouthwash. The EO not only appear to be effective against oral bacteria but also against viruses. In this sense, there is an interesting study conducted by Meiller et al. [62], who concluded that after a single EO mouthwash there was a significant decrease in the presence of the HSV in saliva. In this case, they used direct immunofluorescence of cytological smears of the oral fluids.
3.2. In situ antimicrobial activity of EO on plaque-like biofilm
In the oral cavity, biofilms are developed spontaneously on the teeth surface, prosthesis, dental implants and on the oral epithelium [63]. The scientific community has demonstrated that the growth of structured bacterial populations over a surface differs phenotypically from their counterpart in planktonic phase [42, 64, 65]. As a result, it has been suggested that the bacteria present in the biofilms behaves like cells in a multicellular organism, collaborating and communicating like a basic circulatory system [66]. This affirmation can explain the reason why the bacteria in biofilms may be from 10 to 1000 times more resistant to an antimicrobial treatment than those grown in planktonic phase [67, 68]. This finding could be related to the slower growth rate of biofilm, to problems of antimicrobial agent penetration into biofilm, or to inactivation of the agent in the biofilm [44]. It is a fact that for the success of an antiseptic, the bacteria present in the biofilm must be exposed to an appropriate concentration of the antimicrobial agent for a certain time [69]. Therefore, the antiseptic penetration rate, which is related not only to its physicochemical characteristics, but also with other biofilm-related factors such as its structure and composition [39, 44], although its thickness [70] and physicochemical characteristics are probably more important [39, 44].
3.2.1. Methodological approach
The in vitro studies highlight the necessity of developing in situ biofilm models to provide samples which can be analysed ex vivo without any disturbance. In the first in situ studies of the antimicrobial activity of EO in oral biofilm, dental plaque was recollected from the teeth surfaces using paper points [71] or with a dental scaler [59, 72]. These techniques produced an interruption in the delicate three-dimensional existing relationship between cells, the extracellular matrix and the substrate [44, 73]. Another disadvantage is that the penetration rate of the antimicrobial agent cannot be evaluated due to the fact that dental plaque samples do not conserve the original in situ architecture and organization. To enable a better understanding of the clinical effects of the antimicrobial agents inside the biofilm, it is necessary to apply a specific methodology to permit the biofilm growing directly in the oral cavity. This will ensure that its three-dimensional structure is not distorted with manipulation [44, 45]. As a consequence, the most recent studies about in situ antimicrobial activity of the EO analyse a biofilm which is growing on the surface of small disks made by different materials. These disks are introduced in the mouth for a certain period of time during which they are exposed to the oral cavity conditions [60, 74]. At this point, it should be remarked that they are not analysing dental plaque itself, but a biofilm which is presumably very similar, which is generated in the same conditions and it is set on an artificial substrate, which is called plaque like-biofilm (PL-Biofilm). In 1998, following the objective of studying the “non-destructured” biofilm, the confocal laser scanning microscope (CLSM) was incorporated. This technique combined with a fluorescence staining solution permits the analysis of the biofilm structure and the distribution of the vital and non-vital bacteria in the biofilm [75, 76]. With CLSM, biofilms can be studied in their natural hydrated state, with no need for dehydration, fixation, or staining [37, 38, 77].
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
1116

In addition, the optical sectioning properties of CLSM mean that very thin optical sections in the horizontal plane (X-Y axes) can be taken at 0.5 to 2 μm intervals, at increasing depths through the biofilm (from the surface of the biofilm to its base), and they will be free from out-of-focus blurring [40, 73, 77-79]. Consequently, at present, the scientific community considers that the methodological design based on the use of special removable appliances (including disks) to obtain biofilm samples and its analysis by CLSM together with a fluorescence staining (in combination with other microscopic and microbiological techniques) is the most suitable approach for studying the in situ architecture and physiology of undisturbed PL-biofilm formed on surfaces, as well as the antibacterial effect of antiseptics on this microbial structure [41, 44, 80]. The CLSM associated with a fluorescence staining solution are an essential part of the methodology followed by some of the studies existing in the literature about the in situ antimicrobial activity of the EO [59, 60]. Other used techniques are the spectrophotometric method [71, 74], which quantifies the bacterial mass existing in a dissolution by the diffraction of the light when passing through it. The biggest limitation of this technique is the fact that it is impossible to determine whether the bacteria found in the solution are alive or dead. Fine et al. [72] used the culture in plaque technique which presents considerable limitations already explained. Furthermore, these latter two techniques do not permit the study of the biofilm structure. Apart from the methodological limitations of the named studies, it lacks the comparison of the effect of EO, not only with a negative control or with an antiseptic with lower efficacy, but also with a positive control, the Gold-standard, CHX. Thus, a more accurate view of the EO activity as an antiseptic could be obtained.
3.2.2. Immediate effect and substantivity of EO
To the best of the author’s knowledge, there are only five studies in the literature which analyse the in situ antimicrobial activity of the EO in the PL-Biofilm [59, 60, 71, 72, 74]. Also, in only two of them authors studied a “non-destructured” biofilm [60, 74]; and the antiseptic was applied ex vivo [60, 74], and just Gosau et al. [60] used CLSM. Gosau et al. [60] evaluated the antimicrobial activity of the EO in the 12 hour PL-biofilm formed on the surface of titan disks hold in an upper splint in a total of four volunteers. The application of the mouthwash was done ex vivo for one minute. After the using of the fluorescence staining solution LIVE/DEAD® BacLightTM and the CLSM for the visualisation of the PL-biofilm in situ, the dead bacteria rate was 76.8% (range = 65.09-95.87%). Dong et al. [74] tried to establish a new in situ model to recollect intact PL-biofilm for the evaluation of its structure, the immediate penetration tax and the antibacterial effect of a single EO mouthwash. For this, they used hydroxyapatite disks in which they made 500 µm deep grooves. A total of 6 volunteers wore these disks for 6, 24 and 48 hours. Disks were subsequently divided in 2 halves. One of them was submerged (ex vivo) in an EO solution for 1 minute and the plaque was visualised 5, 15 and 30 minutes after. They obtained a significant reduction in the bacterial vitality in comparison to the control group. One interesting point that should be remarked about these two studies is the fact that having developed a model which permits the growth of the biofilm in the oral cavity, it seems surprising that they applied the EO mouthwash ex vivo; what they did was just take the disks from the mouth and immerse them in the EO solution for a certain period of time (60 seconds). By doing this, they were assuming that this immersion was the same as doing an active mouthwash, obviating the intrinsic factors of the rinse itself such as the washing effect and the strength applied by the muscle movement. Charles et al. [71] evaluated the interproximal antibacterial activity of the EO. For that, they used 34 volunteers who did a mouthwash (EO or saline negative control) after dental brushing. Five minutes after that, they collected interproximal plaque samples using paper points. After a single EO mouthwash, they obtained a decrease in the bacterial vitality of 44% in the interproximal spaces with regard to the negative control, 5 minutes post-application. After their in vitro test [81], the research group of Pan [59] examined the one day-formation PL-biofilm in 17 subjects. For that purpose, using a dental scaler, they collected the dental plaque from the vestibular surfaces of an upper quadrant and its lower contralateral before the EO mouthwash. The plaque was deposed on a glass disk and stained with the fluorescence solution LIVE/DEAD® BacLightTM to differ from live and dead bacteria, obtaining a viability of 22.3% at 30 minutes, while the level was 72.1% at that specific moment with the control. Fine et al. [72] carried out a study in which they determined the antimicrobial effect of a single EO mouthwash 12 hours after its application and 14 days after a continuous daily use. A curette was used as the recollection method for the dental plaque. This study gives a light idea about the substantivity of the EO in the biofilm. They obtained a decrease in the vitality that went from 56.3% to 87.7% compared to the negative control (5% hydro-alcoholic solution) 12 hours after the mouthwash application. After the daily use (twice a day/2 weeks) the decrease rate for the bacterial vitality was 72.5-93.8% with regard to the negative control.
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
1117

3.3. In situ substantivity of EO vs. 0.2% CHX on PL-biofilm
According to the theory of the investigation in the evidence based science new techniques, treatments, drugs or substances should be always compared with their respective considered Gold-standard. Up to now, to the author’s knowledge, there has been no study published which compares the in situ antimicrobial effect on the biofilm of the application of a single EO mouthwash with CHX. Quintas et al. (unpublished data), studied the in situ antimicrobial activity of a single EO mouthwash on a two days “non-destructured” PL-biofilm formed on glass disks in comparison to a single water mouthwash (negative control) and a single 0.2% CHX mouthwash (positive control). In the field of the methodology, they used the Intraoral Device of Overlaid Disk-holding Splints (IDODS) (Fig. 5).
Fig. 5 Clinical views of the Intraoral Device of Overlaid Disk-holding Splints. Note in the second photograph the places where the glass disks are positioned.
The apparatus carried six glass disks which permitted the formation of the PL-biofilm in similar conditions to the dental plaque itself from the volunteers. Each of the six disks were analysed at different moments: at baseline, 30 seconds after the mouthwash, and 1, 3, 5 and 7 hours after the application. The samples were analysed using CLSM after the LIVE/DEAD® BacLightTM fluorescence staining solution. They studied the bacterial viability and the thickness of all samples and the penetration rate of each mouthwash. After the application of the EO mouthwash, the bacterial viability was 1.18%, while after the 0.2% CHX the bacterial viability was 5.08%. The antimicrobial activity of the EO was detected until 7 hours after the mouthwash application when the bacterial viability reduction was still the 61% with regard to the basal (Fig. 6). The effects of the water mouthwash were almost imperceptible (Fig. 6).
Fig. 6 Images of different samples at different moments before and after the three mouthwashes; they are obtained with the CLSM after the fluorescence staining solution LIVE/DEAD® BacLightTM (SYTO 9/propidium idodide – green = live bacteria/red = dead bacteria-). Note that 7 hours after the EO and 0.2 CHX mouthwashes the effects are clearly visible, while after the water mouthwash the changes in the PL-biofilm are almost imperceptible.
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
1118

An interesting aspect that this study showed was the higher penetration ability of the EO in comparison to 0.2% CHX. There were significant differences between both antiseptics in the bacterial viability reduction in the deepest layers of the biofilm (Fig. 7), the differences increased as time passed by (difference in terms of viability at 7 hour mouthwash post-application EO vs. 0.2% CHX in the deepest layer = -36.88%; p<0.001). This may indicate that the penetration ability of a single EO mouthwash is higher than that of 0.2% CHX; besides, its effect lasts longer in the deepest layers (those which are nearest to what in theory is the tooth surface).
Fig. 7 Sectional images from basal and 7 hour samples for EO and 0.2% CHX. Note that starting from a similar bacterial viability at basal, this viability remains lower in the deepest layers of the PL-biofilm 7 hours after a single EO mouthwash.
In terms of thickness reduction, the EO mouthwash did not show any significant effects (the same as the water), while the 0.2% CHX showed significant differences between basal and post-application measures (difference in terms of thickness between basal and 1 and 7 hour samples for 0.2% CHX = 9.97 µm and 7.88 µm, respectively; p<0.05). This result could suggest a possible antiplaque effect caused by 0.2% CHX after a single antiseptic application.
4. Conclusions
Despite the scarce literature about the immediate effect and substantivity of the EO in saliva, they are presented as effective when reducing the salivary microorganisms and keeping them in low levels until at least 7 hours after the mouthwash. Even so, further research is needed to confirm this. The immediate effect of EO in biofilm appears to be similar to its effect in saliva. On the other hand, its substantivity seems to be higher, maintaining a perceptible action until 12 hours after the mouthwash. Furthermore, the plaque culture techniques do not seem to be the most efficient manner to prove the EO in situ antibacterial effect due to their limitations. On the other hand, there have not been many studies in which the epifluorescence microscopy and/or CLSM associated with bacterial viability techniques were used to determine the in situ effects of EO in the oral cavity. CLSM associated with fluorochromes seems to be one good option for the in situ study of the antimicrobial effect of the EO in the oral biofilm. This last one must grow inside the oral cavity and should be analysed without being destructured. In this case, it will be possible to study the architecture, the viability distribution inside the biofilm and its thickness. Moreover, the immediate effect, substantivity and penetration rate of an antiseptic could be analysed. Finally, the application of EO should be in vivo and the obtained results should be compared with a positive and negative control and with the antiseptic effects observed in other oral ecosystems such as the saliva. Thereby, a more reliable approach about the ability of the EO as oral antiseptics could be obtained.
References
[1] Chemat F, Vian MA, Cravotto G. Green extraction of natural products: concept and principles. International Journal of Molecular Sciences. 2012;13:8615-8627.
[2] Fischman SL. The history of oral hygiene products: how far have we come in 6000 years? Periodontology 2000. 1997;15:7-14. [3] Company LF. Listerine Label of 1885. 1912. [4] Fine DH. Listerine: past, present and future--a test of thyme. Journal of Dentistry. 2010;38 Suppl 1:S2-5. [5] Vlachojannis C, Winsauer H, Chrubasik S. Effectiveness and safety of a mouthwash containing essential oil ingredients.
Phytotherapy Research. 2012. [6] Mandel ID. Chemotherapeutic agents for controlling plaque and gingivitis. Journal of Clinical Periodontology. 1988;15:488-
498. [7] Therapeutics CoD. Guidelines for acceptance of chemotherapeutic agents for the control of supragringival plaque and gingivitis.
Journal of the American Dental Association. 1986:529-532. [8] Fornell J, Sundin Y, Lindhe J. Effect of listerine on dental plaque and gingivitis. Scandinavian Journal of Dental Research.
1975;83:18-25.
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
1119

[9] Lamster IB AM, Seiger MC, Gordon JM. The effect of Listerine antiseptic on reduction of existing plaque and gingivitis. Clinical Preventive Dentistry. 1983;5:12-16.
[10] Fine DH, Letizia J, Mandel ID. The effect of rinsing with Listerine antiseptic on the properties of developing dental plaque. Journal of Clinical Periodontology. 1985;12:660-666.
[11] Gordon JM, Lamster IB, Seiger MC. Efficacy of Listerine antiseptic in inhibiting the development of plaque and gingivitis. Journal of Clinical Periodontology. 1985;12:697-704.
[12] P. A. Preventive Materials, Methods, and Programs. Surrey, U.K.: Quintessence. 2004; 184. [13] Department of Health and Human Services. Food and Drug Administration. Oral health care drug products for over-the-counter
human use; antigingivitis/ antiplaque drug products; establishment of a monograph; proposed rules Part III. Federal Register 203;68:32232-32282.
[14] Prakash O, Sahoo D, Rout PK. Liquid CO2 extraction of Jasminum grandiflorum and comparison with conventional processes. Natural Product Communications. 2012;7:89-92.
[15] Degenhardt J, Kollner TG, Gershenzon J. Monoterpene and sesquiterpene synthases and the origin of terpene skeletal diversity in plants. Phytochemistry. 2009;70:1621-1637.
[16] Hammer KA, Carson CF, Riley TV. Antimicrobial activity of essential oils and other plant extracts. Journal of Applied Microbiology. 1999;86:985-990.
[17] Scorzoni L BT, Almeida AMF, Silva DHS, Bolzani VS, Gianinni MJSM. The use of standar methodology for determination of antifungical activity of natural products against medical yeasts Candida spp. and Crytococcus spp. Brazilian Journal of Microbiology. 2007;38:391-397.
[18] Stoeken JE, Paraskevas S, van der Weijden GA. The long-term effect of a mouthrinse containing essential oils on dental plaque and gingivitis: a systematic review. Journal of Periodontology. 2007;78:1218-1228.
[19] Dorman HJ, Deans SG. Antimicrobial agents from plants: antibacterial activity of plant volatile oils. Journal of Applied Microbiology. 2000;88:308-316.
[20] Lambert RJ, Skandamis PN, Coote PJ, Nychas GJ. A study of the minimum inhibitory concentration and mode of action of oregano essential oil, thymol and carvacrol. Journal of Applied Microbiology. 2001;91:453-462.
[21] Turgis M, Han J, Millette M, Salmieri S, Borsa J, Lacroix M. Effect of selected antimicrobial compounds on the radiosensitization of Salmonella Typhi in ground beef. Letters in Applied Microbiology. 2009;48:657-662.
[22] Ouhayoun JP. Penetrating the plaque biofilm: impact of essential oil mouthwash. Journal of Clinical Periodontology. 2003;30 Suppl 5:10-12.
[23] Carson CF, Mee BJ, Riley TV. Mechanism of action of Melaleuca alternifolia (tea tree) oil on Staphylococcus aureus determined by time-kill, lysis, leakage, and salt tolerance assays and electron microscopy. Antimicrobial Agents and Chemotherapy. 2002;46:1914-1920.
[24] Bouhdid S, Abrini J, Zhiri A, Espuny MJ, Manresa A. Investigation of functional and morphological changes in Pseudomonas aeruginosa and Staphylococcus aureus cells induced by Origanum compactum essential oil. Journal of Applied Microbiology. 2009;106:1558-1568.
[25] de Souza EL, de Barros JC, de Oliveira CE, da Conceicao ML. Influence of Origanum vulgare L. essential oil on enterotoxin production, membrane permeability and surface characteristics of Staphylococcus aureus. International Journal of Food Microbiology. 2010;137:308-311.
[26] Burt SA, van der Zee R, Koets AP, de Graaff AM, van Knapen F, Gaastra W, et al. Carvacrol induces heat shock protein 60 and inhibits synthesis of flagellin in Escherichia coli O157:H7. Applied and Environmental Microbiology. 2007;73:4484-4490.
[27] Becerril R, Gomez-Lus R, Goni P, Lopez P, Nerin C. Combination of analytical and microbiological techniques to study the antimicrobial activity of a new active food packaging containing cinnamon or oregano against E. coli and S. aureus. Analytical and Bioanalytical Chemistry. 2007;388:1003-1011.
[28] Kjelleberg S, Molin S. Is there a role for quorum sensing signals in bacterial biofilms? Current Opinion in Microbiology. 2002;5:254-258.
[29] Mezzoug N, Elhadri A, Dallouh A, Amkiss S, Skali NS, Abrini J, et al. Investigation of the mutagenic and antimutagenic effects of Origanum compactum essential oil and some of its constituents. Mutation Research. 2007;629:100-110.
[30] De Martino L, De Feo V, Nazzaro F. Chemical composition and in vitro antimicrobial and mutagenic activities of seven Lamiaceae essential oils. Molecules. 2009;14:4213-4230.
[31] Fine DH. Mouthrinses as adjuncts for plaque and gingivitis management. A status report for the American Journal of Dentistry. American Journal of Dentistry. 1988;1:259-263.
[32] Department of Health and Human Services.Food and Drug Administration. Oral health care drug products for over-the-counter human use; establishment of a monograph. Federal Register 1982;47:22760-22930.
[33] Manau-Navarro C, Guasch-Serra S. Métodos de control de placa bacteriana. In: Cuenca E, Manau C, Serra LL. Odontología Preventiva y Comunitaria. Principios Métodos y Aplicaciones. Barcelona: Masson; 2003:69-88.
[34] Fine DH, Furgang D, Barnett ML, Drew C, Steinberg L, Charles CH, et al. Effect of an essential oil-containing antiseptic mouthrinse on plaque and salivary Streptococcus mutans levels. Journal of Clinical Periodontology. 2000;27:157-161.
[35] Pan PC, Harper S, Ricci-Nittel D, Lux R, Shi W. In-vitro evidence for efficacy of antimicrobial mouthrinses. Journal of Dentistry. 2010;38 Suppl 1:S16-20.
[36] Sliepen I, Van Essche M, Quirynen M, Teughels W. Effect of mouthrinses on Aggregatibacter actinomycetemcomitans biofilms in a hydrodynamic model. Clinical Oral Investigations. 2010;14:241-250.
[37] Auschill TM, Hellwig E, Sculean A, Hein N, Arweiler NB. Impact of the intraoral location on the rate of biofilm growth. Clinical Oral Investigations. 2004;8:97-101.
[38] Auschill TM, Hein N, Hellwig E, Follo M, Sculean A, Arweiler NB. Effect of two antimicrobial agents on early in situ biofilm formation. Journal of Clinical Periodontology. 2005;32:147-152.
[39] Watson PS, Pontefract HA, Devine DA, Shore RC, Nattress BR, Kirkham J, et al. Penetration of fluoride into natural plaque biofilms. Journal of Dental Research. 2005;84:451-455.
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
1120

[40] Al-Ahmad A, Wunder A, Auschill TM, Follo M, Braun G, Hellwig E, et al. The in vivo dynamics of Streptococcus spp., Actinomyces naeslundii, Fusobacterium nucleatum and Veillonella spp. in dental plaque biofilm as analysed by five-colour multiplex fluorescence in situ hybridization. Journal of Medical Microbiology. 2007;56:681-687.
[41] Hannig C, Hannig M. The oral cavity--a key system to understand substratum-dependent bioadhesion on solid surfaces in man. Clinical Oral Investigations. 2009;13:123-139.
[42] Costerton JW, Stewart PS, Greenberg EP. Bacterial biofilms: a common cause of persistent infections. Science. 1999;284:1318-1322.
[43] Palmer RJ, Jr., Wu R, Gordon S, Bloomquist CG, Liljemark WF, Kilian M, et al. Retrieval of biofilms from the oral cavity. Methods in Enzymology. 2001;337:393-403.
[44] Wood SR, Kirkham J, Marsh PD, Shore RC, Nattress B, Robinson C. Architecture of intact natural human plaque biofilms studied by confocal laser scanning microscopy. Journal of Dental Research. 2000;79:21-27.
[45] Beyth N, Yudovin-Farber I, Perez-Davidi M, Domb AJ, Weiss EI. Polyethyleneimine nanoparticles incorporated into resin composite cause cell death and trigger biofilm stress in vivo. Proceedings of the National Academy of Sciences of the United States of America. 2010;107:22038-22043.
[46] Roberts WR, Addy M. Comparison of the in vivo and in vitro antibacterial properties of antiseptic mouthrinses containing chlorhexidine, alexidine, cetyl pyridinium chloride and hexetidine. Relevance to mode of action. Journal of Clinical Periodontology. 1981;8:295-310.
[47] Addy M, Jenkins S, Newcombe R. Toothpastes containing 0.3% and 0.5% triclosan. II. Effects of single brushings on salivary bacterial counts. American Journal of Dentistry. 1989;2 Spec No:215-219.
[48] Weiger R, Netuschil L, Wester-Ebbinghaus T, Brecx M. An approach to differentiate between antibacterial and antiadhesive effects of mouthrinses in vivo. Archives of Oral Biology. 1998;43:559-565.
[49] Rosin M, Welk A, Bernhardt O, Ruhnau M, Pitten FA, Kocher T, et al. Effect of a polyhexamethylene biguanide mouthrinse on bacterial counts and plaque. Journal of Clinical Periodontology. 2001;28:1121-1126.
[50] Jenkins S, Addy M, Wade W, Newcombe RG. The magnitude and duration of the effects of some mouthrinse products on salivary bacterial counts. Journal of Clinical Periodontology. 1994;21:397-401.
[51] DePaola LG, Minah GE, Overholser CD, Meiller TF, Charles CH, Harper DS, et al. Effect of an antiseptic mouthrinse on salivary microbiota. American Journal of Dentistry. 1996;9:93-95.
[52] Balbuena L, Stambaugh KI, Ramirez SG, Yeager C. Effects of topical oral antiseptic rinses on bacterial counts of saliva in healthy human subjects. Otolaryngology--head and neck surgery : Official Journal of American Academy of Otolaryngology-Head and Neck Surgery. 1998;118:625-629.
[53] Botelho MA, dos Santos RA, Martins JG, Carvalho CO, Paz MC, Azenha C, et al. Comparative effect of an essential oil mouthrinse on plaque, gingivitis and salivary Streptococcus mutans levels: a double blind randomized study. Phytotherapy Research. 2009;23:1214-1219.
[54] Berney M, Hammes F, Bosshard F, Weilenmann HU, Egli T. Assessment and interpretation of bacterial viability by using the LIVE/DEAD BacLight Kit in combination with flow cytometry. Applied and Environmental Microbiology. 2007;73:3283-3290.
[55] Boulos L, Prevost M, Barbeau B, Coallier J, Desjardins R. LIVE/DEAD BacLight: application of a new rapid staining method for direct enumeration of viable and total bacteria in drinking water. Journal of Microbiology Methods. 1999;37:77-86.
[56] Nadkarni MA, Martin FE, Jacques NA, Hunter N. Determination of bacterial load by real-time PCR using a broad-range (universal) probe and primers set. Microbiology. 2002;148:257-266.
[57] Tomás I, Garcia-Caballero L, Cousido MC, Limeres J, Álvarez M, Diz P. Evaluation of chlorhexidine substantivity on salivary flora by epifluorescence microscopy. Oral Diseases. 2009;15:428-433.
[58] Cousido MC, Tomás Carmona I, Garcia-Caballero L, Limeres J, Álvarez M, Diz P. In vivo substantivity of 0.12% and 0.2% chlorhexidine mouthrinses on salivary bacteria. Clinical Oral Investigations. 2010;14:397-402.
[59] Pan P, Barnett ML, Coelho J, Brogdon C, Finnegan MB. Determination of the in situ bactericidal activity of an essential oil mouthrinse using a vital stain method. Journal of Clinical Periodontology. 2000;27:256-261.
[60] Gosau M, Hahnel S, Schwarz F, Gerlach T, Reichert TE, Burgers R. Effect of six different peri-implantitis disinfection methods on in vivo human oral biofilm. Clinical of Oral Implants Research. 2010;21:866-872.
[61] Joux F, Lebaron P. Use of fluorescent probes to assess physiological functions of bacteria at single-cell level. Microbes and infection / Institut Pasteur. 2000;2:1523-1535.
[62] Meiller TF, Silva A, Ferreira SM, Jabra-Rizk MA, Kelley JI, DePaola LG. Efficacy of Listerine Antiseptic in reducing viral contamination of saliva. Journal of Clinical Periodontology. 2005;32:341-346.
[63] Slavkin HC. Biofilms, microbial ecology and Antoni van Leeuwenhoek. Journal of American Dental Association. 1997;128:492-495.
[64] Hoyle BD, Williams LJ, Costerton JW. Production of mucoid exopolysaccharide during development of Pseudomonas aeruginosa biofilms. Infection and Immunity. 1993;61:777-780.
[65] Costerton JW, Lewandowski Z, Caldwell DE, Korber DR, Lappin-Scott HM. Microbial biofilms. Annual Review of Microbiology. 1995;49:711-745.
[66] Pratten J, Andrews CS, Craig DQ, Wilson M. Structural studies of microcosm dental plaques grown under different nutritional conditions. FEMS Microbiology Letters. 2000;189:215-218.
[67] Fine DH, Furgang D, Barnett ML. Comparative antimicrobial activities of antiseptic mouthrinses against isogenic planktonic and biofilm forms of Actinobacillus actinomycetemcomitans. Journal of Clinical Periodontology. 2001;28:697-700.
[68] Davies D. Understanding biofilm resistance to antibacterial agents. Nature Reviews Drug Discovery. 2003;2:114-122. [69] von Ohle C, Gieseke A, Nistico L, Decker EM, DeBeer D, Stoodley P. Real-time microsensor measurement of local metabolic
activities in ex vivo dental biofilms exposed to sucrose and treated with chlorhexidine. Applied and Environmental of Microbiology. 2010;76:2326-2334.
[70] Stewart PS. Diffusion in biofilms. Journal of Bacteriology. 2003;185:1485-1491.
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
1121

[71] Charles CH, Pan PC, Sturdivant L, Vincent JW. In vivo antimicrobial activity of an essential oil-containing mouthrinse on interproximal plaque bacteria. Journal of Clinical Dentistry. 2000;11:94-97.
[72] Fine DH, Furgang D, Sinatra K, Charles C, McGuire A, Kumar LD. In vivo antimicrobial effectiveness of an essential oil-containing mouth rinse 12 h after a single use and 14 days' use. Journal of Clinical Periodontology. 2005;32:335-340.
[73] Dige I, Nyengaard JR, Kilian M, Nyvad B. Application of stereological principles for quantification of bacteria in intact dental biofilms. Oral Microbiology Immunology. 2009;24:69-75.
[74] Dong WL, Zhou YH, Li CZ, Liu H, Shang SH, Pan BQ. [Establishment and application of an intact natural model of human dental plaque biofilm]. Shanghai Kou Qiang Yi Xue. 2010;19:196-201.
[75] Netuschil L, Reich E, Unteregger G, Sculean A, Brecx M. A pilot study of confocal laser scanning microscopy for the assessment of undisturbed dental plaque vitality and topography. Archives of Oral Biology. 1998;43:277-285.
[76] Auschill TM, Arweiler NB, Netuschil L, Brecx M, Reich E, Sculean A. Spatial distribution of vital and dead microorganisms in dental biofilms. Archives of Oral Biology. 2001;46:471-476.
[77] Arweiler NB, Lenz R, Sculean A, Al-Ahmad A, Hellwig E, Auschill TM. Effect of food preservatives on in situ biofilm formation. Clinical Oral Investigations. 2008;12:203-208.
[78] Dige I, Nilsson H, Kilian M, Nyvad B. In situ identification of streptococci and other bacteria in initial dental biofilm by confocal laser scanning microscopy and fluorescence in situ hybridization. European Journal of Oral Science. 2007;115:459-467.
[79] Konishi N, Torii Y, Kurosaki A, Takatsuka T, Itota T, Yoshiyama M. Confocal laser scanning microscopic analysis of early plaque formed on resin composite and human enamel. Journal of Oral Rehabilitation. 2003;30:790-795.
[80] Arweiler NB, Hellwig E, Sculean A, Hein N, Auschill TM. Individual vitality pattern of in situ dental biofilms at different locations in the oral cavity. Caries Research. 2004;38:442-447.
[81] Pan PH, Finnegan MB, Sturdivant L, Barnett ML. Comparative antimicrobial activity of an essential oil and an amine fluoride/stannous fluoride mouthrinse in vitro. Journal of Clinical Periodontology. 1999;26:474-476.
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
1122