Embed Size (px)
Citation preview
In Pursuit of High Value
Health Care
Shari M. Ling, MD
Deputy Chief Medical Officer
Centers for Medicare & Medicaid Services
CAP Policy Meeting
7 May 2013

2
CMS Vision
CMS is a major force and a
trustworthy partner for the
continual improvement of health
and health care for all
Americans.

3
Size and Scope of
CMS Responsibilities
CMS is the largest purchaser of health care in the world.
Combined, Medicare and Medicaid pay approximately
one-third of national health expenditures (approx $800B)
CMS programs currently provide health care coverage
to roughly 105 million beneficiaries in Medicare,
Medicaid and CHIP (Children’s Health Insurance
Program); or roughly 1 in every 3 Americans
Millions of consumers will receive health care coverage
through new health insurance programs authorized in
the Affordable Care Act

4
National Quality Strategy promotes
better health, healthcare, and lower cost
The Affordable Care Act (ACA) requires the
Secretary of the Department of Health and Human
Services (HHS) to establish a national strategy that
will improve:
The delivery of health care services
Patient health outcomes
Population health

The strategy is to concurrently pursue
three aims
5
Better Care Improve overall quality by making health care more patient-centered, reliable, accessible and safe.
Healthy People /
Healthy Communities
Improve population health by supporting proven interventions to address behavioral, social and environmental determinants of health, in addition to delivering higher-quality care.
Affordable Care Reduce the cost of quality health care for individuals, families, employers and government.
And focus on six priorities
1) Making care safer by reducing harm caused in the delivery of care
2) Ensuring that each person and family are engaged as partners in their care
3) Promoting effective communication and coordination of care
4) Promoting the most effective prevention and treatment practices for the
leading causes of mortality, starting with cardiovascular disease
5) Working with communities to promote wide use of best practices to enable
healthy living
6) Making quality care more affordable for individuals, families, employers,
and governments by developing and spreading new health care delivery
models
6

7
CMS Measurement Framework
Maps to the
National Quality Strategy Priorities
• Measures should
be patient-
centered and
outcome-oriented
whenever
possible
• Measure concepts
in each of the six
domains that are
common across
providers and
settings can form
a core set of
measures
Person- and Caregiver-
centered experience and
outcomes
•CAHPS or equivalent
measures for each
settings
•Functional outcomes
Efficiency and cost
reduction
•Spend per beneficiary
measures
•Episode cost measures
•Quality to cost
measures
Care Coordination
•Transition of care
measures
•Admission and
readmission measures
•Other measures of
care coordination
Clinical Care
•HHS primary care and
CV quality measures
•Prevention measures
•Setting-specific
measures
•Specialty-specific
measures
Population &
Community Health
•Measures that assess
health of the community
•Measures that reduce
health disparities
•Access to care and
equitability measures
Safety
•HCACs, including
HAIs
•All cause harm

8
Quality can be measured and improved at multiple levels
•Three levels of measurement critical to achieving three aims of National Quality Strategy •Measure concepts should “roll up” to align quality improvement objectives at all levels •Patient-centric, outcomes oriented measures preferred at all three levels •The six domains can be measured at each of the three levels
Inc
rea
sin
g in
div
idu
al a
cc
ou
nta
bilit
y
Incre
asin
g c
om
mo
nali
ty a
mo
ng
pro
vid
ers
Community
Practice setting
Individual physician/EP
•Population-based denominator •Multiple ways to define denominator, e.g., county, HRR •Applicable to all providers
•Denominator based on practice setting, e.g., hospital, group practice
•Denominator bound by patients cared for •Applies to all physicians/EPs

9
Quality Reporting Towards
Value-Based Purchasing
2011
• ACA, HITECH
• 190 individual
measures
• 14 Measures
Groups
• eRx
• Individual
Reporting via
Claims, Registry, or
EHRs
• GPRO I
• GPRO II
•Maintenance of
Certification
Program Incentive
2007
• TRHCA
• 74
measures
• Claims-
based
reporting
only
2008
• MMSEA
• 119
measures
• 4 Measures
Groups
• Reporting via
Claims or
Registry
2009
• MIPPA
• 153 individual
measures
• 7 Measures
Groups
• eRx
• Reporting via
Claims or
Registry
• EHR-testing
VBP
2010
• MIPPA
• 179 individual
measures
• 13 Measures
Groups
• eRx
• Individual
Reporting via
Claims, Registry,
or EHRs
• Group reporting
option (GPRO)
2012 2013
• ACA, HITECH 13 participation options
• 210 individual measures 258 measures
• 22 Measures Groups
• eRx
• Individual Reporting via Claims, Registry,
or EHRs
• Single GPRO for groups with at least 25
eligible professionals
• Incentive payments for PQRS, GPRO, and
eRx reporting
•Payment Adjustments for non-successful
eRx reporters
•Maintenance of Certification Program
Incentive

10
PQRS Program Overview
PQRS is a Medicare Part B reporting program that uses a
combination of incentive payments and payment adjustments to
promote reporting of PFS quality information by eligible
professionals, or group practices participating in GPRO The applicable PQRS incentive amounts are:
1.5% for 2007 1.0% for 2011
1.5% for 2008 0.5% for 2012
2.0% for 2009 0.5% for 2013
2.0% for 2010 0.5% for 2014
The applicable PQRS payment adjustment amounts are:
1.5% in 2015
2.0% in 2016
The 2013 PFS Final Rule sets forth requirements for the PQRS
incentive payment, and for the 2015 PQRS payment adjustments
No PQRS incentive payments are scheduled past 2014

11
Pathology Participation
Percentage of eligible professionals participating in PQRS has increased each year
4,539 in 2009 (58.9% of eligible)
4,749 in 2010 (61.5% of eligible)
4,829 in 2011 (63.2% of eligible)

12
How to Participate in 2013

13
Avoiding the 2015 1.5%
PQRS Payment Adjustment For services provided through 12/31/13, must report by 2/28/14:
Report Satisfactory for 2013 PQRS Incentive Payment, OR
http://cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-
Instruments/PQRS/Downloads/2013MLNSE13__AvoidingPQRSPaymentAdjustme
nt_020113.pdf
Report one valid measure or one valid measures group for one
Medicare Part B beneficiary, OR
Elect the administrative claims reporting mechanism (reference the
Value-Based Payment Modifier website for upcoming details about
the election process)
◊ Admin claims election (likely occur between 7/15 and 10/15/13)
http://www.cms.gov/Medicare/Medicare-Fee-for-Service-
Payment/PhysicianFeedbackProgram/ValueBasedPaymentModifier.html
Participate now!

14
Relevant 2013 Measures
PQRS #99/NQF #0391: Breast Cancer Resection Pathology
Reporting: Breast Cancer Resection Pathology Reporting: pT
Category (Primary Tumor) and pN Category (Regional Lymph
Nodes) with Histologic Grade Percentage of breast cancer resection pathology reports that include the pT category
(primary tumor), the pN category (regional lymph nodes), and the histologic grade
◊ Reporting options: Claims, Registry
PQRS #100/NQF #0392: Colorectal Cancer Resection Pathology
Reporting: pT Category (Primary Tumor) and pN Category
(Regional Lymph Nodes) with Histologic Grade Percentage of colon and rectum cancer resection pathology reports that include the pT
category (primary tumor), the pN category (regional lymph nodes) and the histologic
grade
◊ Reporting options: Claims, Registry

15
Relevant 2013 Measures (cont.)
PQRS #249: Barrett's Esophagus Percentage of esophageal biopsy reports that document the presence of Barrett’s mucosa
that also include a statement about dysplasia
◊ Reporting options: Claims, Registry
PQRS #250: Radical Prostatectomy Pathology Reporting Percentage of radical prostatectomy pathology reports that include the pT category, the
pN category, the Gleason score and a statement about margin status
◊ Reporting options: Claims, Registry
PQRS #251: Immunohistochemical (IHC) Evaluation of Human
Epidermal Growth Factor Receptor 2 Testing (HER2) for Breast
Cancer Patients This is a measure based on whether quantitative evaluation of Human Epidermal Growth
Factor Receptor 2 Testing (HER2) by immunohistochemistry (IHC) uses the system
recommended in the ASCO/CAP Guidelines for Human Epidermal Growth Factor
Receptor 2 Testing in breast cancer
◊ Reporting options: Claims, Registry

16
PQRS, Value-Modifier, & the Medicare EHR
Incentive Program (MU) Incentive & Payment
Adjustment Timelines
PQRS Incentive: ends in 2014
PQRS Payment Adjustment: starts in 2013 (affects 2015
payment); overlaps with the incentive for 2 years
Value-Modifier: first reporting year is 2013; affects
payment in 2015
Must include all providers by payment year 2017
(measurement year 2015)

17
Definition and Purpose
Value-based purchasing is a tool that allows
CMS to link the National Quality Strategy with
fee-for-service payments at a national scale.
It is an important driver in revamping how
services are paid for, moving increasingly
toward rewarding providers and health systems
that deliver better outcomes in health and health
care at lower cost to the beneficiaries and
communities they serve.

VanLare JM, Conway PH. Value-Based Purchasing – National Programs to
Move from Volume to Value. NEJM July 26, 2012 18
Value-Based Purchasing
• Goal is to reward providers and health systems that
deliver better outcomes in health and health care at lower
cost to the beneficiaries and communities they serve.
• Five Principles
- Define the end goal, not the process for achieving it
- All providers’ incentives must be aligned
- Right measure must be developed and implemented in
rapid cycle
- CMS must actively support quality improvement
- Clinical community and patients must be actively
engaged

19
What is the Value-Based
Modifier? • The Affordable Care Act requires that Medicare phase in a value-based
payment modifier (VM) that would apply to Medicare Fee for Service
Payments starting in 2015; phase-in complete by 2017
• The VM assesses both quality of care furnished and the cost of that care
• The Value-based Payment Modifier aligns with PQRS
• The proposals
• Encourage physician measurement and alignment with PQRS
• Offer choice of quality measures and reporting mechanisms
• Focus payments on outliers in the first year
• Provide actionable information
• Challenging and complex program
• Must be budget neutral

Value-based modifier links quality with
physician payment
•Physician Feedback/Value-Based Modifier Program provides
comparative performance information to physicians
•Objective is to align quality measurement and incentives across
programs and care settings to establish common goals for quality
improvement and shared accountability for performance
•Two primary components of the program:
•Reports–provided to participating physicians since 2009;
beginning in 2015 and beyond, for physicians who will be
impacted by the VBPM, the QRURs will contain composite
measures of quality and cost that display the bases for the VBPM
•Value-based Payment Modifier–Starting in 2015, some
physicians' payments by Medicare will be affected by application
of the VBPM; by 2017, most physicians paid under the MPFS will
see the VBPM applied to claims they submit to Medicare

21
PQRS and the Value Modifier
Beginning in 2013, group practices consisting of 100+ eligible
professionals, will be subject to the Value-based Payment Modifier
We finalized applying the VM to physician payment in all
groups of 100 or more eligible professionals (EPs) starting
in 2015
A group practice with 100 or more eligible professionals may
avoid a 2015 VBM downward payment adjustment by self-
nominating for the PQRS as a group and reporting at least one
measure
A group practice is defined as a single Taxpayer Identification
Number (TIN)
Note: The 2015 and 2016 Value-based payment modifier does
not apply to groups that are ACOs or ACO participants
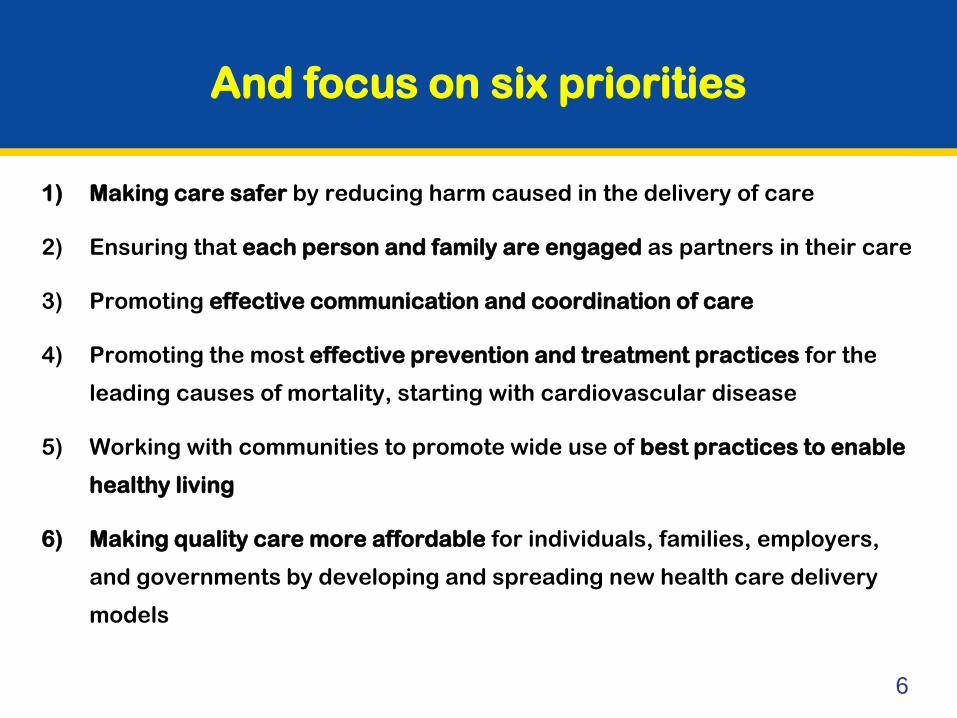
Value-Based Purchasing Program Objectives
over Time Towards Attainment of the
Three-part Aim
Initial
programs
FY2012-2013
Proposed and near-term
programs
FY2014-2016
Longer-term FY2017+
•Limited to hospitals (HVBP)
and dialysis facilities (QIP)
•Existing measures providers
recognize and understand
•Focus on provider
awareness, participation,
and engagement
•Expand to include physicians
•New measures to address
HHS priorities
•Increasing emphasis on
patient experience, cost, and
clinical outcomes
•Increasing provider
engagement to drive quality
improvements, e.g., learning
and action networks
•VBP measures and incentives
aligned across multiple settings
of care and at various levels of
aggregation (individual
physician, facility, health
system)
•Measures are patient-centered
and outcome oriented
•Measure set addresses all 6
national priorities well
•Rapid cycle measure
development and
implementation
•Continued support of QI and
engagement of clinical
community and patients
•Greater share of payment
linked to quality Vision for VBP
23
Contact Information
Dr. Shari Ling
CMS Deputy Chief Medical Officer
Center for Clinical Standards and Quality
410-786-6841

24
Resources
CMS PQRS Website
http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-
Instruments/PQRS
CMS Value-Based Payment Modifier http://www.cms.gov/Medicare/Medicare-Fee-for-Service-
Payment/PhysicianFeedbackProgram/ValueBasedPaymentModifier.html
Medicare and Medicaid EHR Incentive Programs
http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms
Portal and Communication Support Page
https://www.qualitynet.org/portal/server.pt/community/pqri_home/212
FFS Provider Listserv
https://list.nih.gov/cgi-bin/wa.exe?A0=PHYSICIANS-L
Frequently Asked Questions (FAQs)
https://questions.cms.gov/

25
Where to Call for Help
QualityNet Help Desk: Portal password issues
PQRS/eRx feedback report availability and access
IACS registration questions
IACS login issues
PQRS and eRx Incentive Program questions
866-288-8912 (TTY 877-715-6222) 7:00 a.m.–7:00 p.m. CST M-F
[email protected] You will be asked to provide basic information such as name, practice, address, phone, and e-
EHR Incentive Program Information Center:
Medicare/Medicaid EHR Incentive Program
888-734-6433 (TTY 888-734-6563)
Value-based Payment Modifier:
FFS Physician Feedback Program/Value-based Payment Modifier