Embed Size (px)
Citation preview
Physicians’ Update In partnership with the Academy of Medicine Ottawa
Issue 97, May 2014 In this issue: Message from the Medical Officer of Health News Flash:
· Changes to immunization requirements for school attendance · Revision to the reporting of designated communicable diseases · Measles update
New tools and info at your fingertips: · Addressing Poverty in your Patients: Tools for Physicians · Tools to assess language development in bilingual children · Champlain Primary Care Digest – A New Collaborative Resource for Physicians · New Resources for Caregivers of Older Adults · Information and support for cancer patients and caregivers
Articles: Communicable Diseases and Immunization:
· Lyme Disease 101 · Info ‘bites’ on Rabies · MERS-CoV and Human Avian Influenza – current statistics and recommendations · Fever in the returning traveller · Should pregnant women get pertussis vaccine?
Mental Health: · Have that Talk
Older Adults: · Geriatric assessment outreach teams - Update
Upcoming professional development: · OPH TB prevention workshop · Immunization Competencies Education Program (ICEP)
Other: · Why become an AMO member? · Contact Us · Reminder: You must subscribe to receive future communications from OPH! · Version française · Read previous issues

2
Message from the Medical Officer of Health Dear colleagues,
It has been a cold and unusually long winter but it appears that spring has finally arrived in Ottawa. You or your patients may have had the opportunity to escape to warmer climates for a respite from the cold and others may be planning summer vacations. Therefore, it is timely that travel is a common theme for a number of the articles in this issue of Physician’s Update. Recent measles cases in Ottawa and Ontario have all been directly or indirectly related to travel to countries where measles is more prevalent. This underscores the importance of ensuring that your adult patients who are
travelling to areas with measles outbreaks (within or outside of Canada) have had two doses of MMR vaccine and that children are up to date for age. It is also important to always ask about recent travel in patients presenting with fever - to detect more common infections such as malaria or rare, but serious ones like MERS-coV or avian influenza infections. Finally, travel to areas in southern Ontario and the northern U.S. is responsible for almost all reported cases of Lyme disease in Ottawa; this issue includes a ‘Lyme Disease 101’ just in time for tick season. For those who have prenatal patients, the issue provides recommendations on pertussis immunization and nicotine replacement therapy. And once again, we point you to resources and links to a variety of tools to help you in your practice, with topics ranging from poverty to assessing language development to supports for caregivers of older adults or cancer patients. Ottawa Public Health is committed to working with you and our other partners to improve the health and wellbeing of our population. Please do not hesitate to contact me or my colleagues at OPH if you have suggestions as to how we can collaborate more effectively or have ideas for future topics for Physician’s Update. I wish you a safe and healthy summer! Yours, Isra [ Top ]
Changes in School Immunization Requirements In the February issue of Physician's Update we informed you of the changes in the Ontario Immunization of School Pupils Act (ISPA), which now requires students to be vaccinated against three additional diseases (pertussis, varicella and meningococcal disease) or to provide a valid medical or philosophical exemption to Ottawa Public Health. The Ministry of Health and Long Term Care has developed a Fact Sheet and Questions and Answers for health care providers, as well as a parent handout. These can be accessed at: http://www.health.gov.on.ca/en/pro/programs/immunization/ispa.aspx. Please inform your patients that they now need to report their children's vaccination against nine diseases to Ottawa Public Health (pertussis, varicella, meningococcal disease, diphtheria, tetanus, polio, measles, mumps and rubella). Parents can report by phone, or via OPH's website ottawa.ca/immunization
[Top]
3
Revision to the reporting of designated communicable diseases Effective December 4, 2013, Ontario Regulation 559/91 (Specification of Reportable Diseases) under the Health Protection and Promotion Act was amended and the following diseases are now reportable to the Medical Officer of Health:
· Acute Flaccid Paralysis (AFP) · Paralytic Shellfish Poisoning (PSP)
The following diseases are no longer reportable to the Medical Officer of Health:
· Cytomegalovirus infection, congenital · Neonatal herpes · Hepatitis D (Delta hepatitis) · Transmissible Spongiform Encephalopathies: Fatal Familial Insomnia, Gerstmann-
Sträussler-Scheinker Syndrome, and Kuru (Creutzfeldt-Jakob Disease, all types, remains reportable)
The Reporting of Designated Communicable Diseases Form has been revised to reflect these amendments. For more information or to report a designated communicable disease during regular business hours, Monday to Friday from 8:30 a.m. to 4:30 p.m., call the Communicable Disease Control Program at 613-580-6744 ext. 24224. After hours, call 3-1-1 and ask to speak with the Communicable Disease Control Program Manager on-call. Written by Juliana Pari, RN, BScN, Public Health Nurse, Communicable Disease Control Program, Ottawa Public Health
[Top]
Measles Update As you likely know, in 2014, there has been an increase in measles cases in various parts of Canada. As of April 30 there have been 19 cases in Ontario; this includes four cases in Ottawa. All 2014 Ontario cases have been directly or indirectly related to travel to countries with measles outbreaks. This highlights the need to ensure that all travellers are vaccinated according to current recommendations. Two doses of MMR vaccine are recommended and publicly funded for Ontarians who are travelling internationally. Measles vaccine should be given at an earlier age than usual for children travelling to countries outside of North America. MMR vaccine may be given as early as 6 months of age; however, two additional doses of measles-containing vaccine must be administered after the child is 12 months old to ensure long lasting immunity to measles. Although we have not had measles cases in Ottawa since late March, OPH asks that you continue to be vigilant and consider measles in both returning travellers and in individuals who are known to have been in contact with a case of measles. Visit Public Health Ontario to find the latest information on the measles situation in Ontario. [Top]
4
Addressing poverty in your patients: tools for physicians The link between poverty and health is well documented and income is a well-recognized social determinant of health. People living with low incomes experience higher burdens of illness, decreased life expectancy, and higher rates of mortality than high-income earners.1 In the past decade, income inequality has increased in Ontario. Along with this, so has the number of people facing precarious employment, the number of households waiting for assisted-housing and the number of families using food banks.2 In Ottawa 50,000 residents cannot afford sufficient and nutritious foods. Food bank usage is increasing five percent per year3 and women, recent immigrants and racial groups account for a disproportionate number of Ontarians working for minimum wage.4 Poverty is an independent risk factor for disease. It is on par with traditional risk factors such as smoking, high cholesterol or hypertension.5 Family physicians are in a unique position to ask patients about poverty and intervene with appropriate follow-up and referral.1 The Ontario College of Family Physicians recently distributed a clinical tool to family physicians for use with their patients. The tool contains three ways to address poverty in primary care:
1. Screening: Screen everyone. We can’t make assumptions about poverty. Ask all your patients if they ever have difficulty making ends meet at the end of the month.
2. Adjusting risk: for patients experiencing difficulties from low income, adjust the risk by factoring poverty into your clinical decision-making, as you would for other risk factors. For example, consider poverty a risk factor for having a low birth weight infant just as you would consider smoking in a pregnant patient.
3. Intervening: Help your patients access income supports - the tool lists the government supports and how physicians can help. Intervening can also be linking patients to a community program or resource. Using the pregnant patient example, interventions may be providing information on child benefits and filing a tax return once she is a parent, and linking her with a local prenatal nutrition program.
The poverty tool is available online at http://champlainccac.files.wordpress.com/2014/03/poverty-clinical-tool-champlain.pdf Written by Kerry Kennedy R.N. BScN, SDOH Public Health Nurse, Ottawa Public Health
References: 1. Dorman, K. Pelizzari, R., Rachlis, M. & Green, S. (2013). Why poverty is a medical
problem. Ontario Medical Review 2. Mehra, N. (2012). Falling behind: Ontario’s backslide into widening inequality, growing
poverty and cuts to social programs. Ontario Common Front. Toronto, ON. Available at: http://ofl.ca/wp-content/uploads/2012.08.29-Report-FallingBehind.pdf
3. Food Banks Canada. (2012). Hunger count 2012. Toronto. Food Banks Canada. 4. Broadbent Institute. (2012).Towards a more equal Canada: A report on Canada’s
economic & social inequality. Available at: http://www.broadbentinstitute.ca/equality 5. Canadian Medical Association. (2013). Health care in Canada: what makes us sick?
Canadian Medical Association Town Hall Report. Available at http://www.cma.ca [ Top ]
5
Tools to assess language development in bilingual children Current data estimates that 10-19% of preschool children have a speech or language disorder. Early identification and intervention can improve interaction between parent and child, improve the child’s overall communication development, and enhance brain development.
The importance of strong first language development Recent pediatric research clearly establishes the importance of first language use in the context of speech and language development in preschool- aged children. When it comes to dual-language learners, research states:
1. Preschool children who develop a strong first language base learn a second language more easily.
2. Preschool children with strong language skills in their first language do better at school with reading and writing.
3. Parents should speak their home language with their child. Children must learn language from people who speak that language well.
The impact of bilingualism on child development: Contrary to popular beliefs, bilingualism does not trigger confusion or negatively impact the development of language in young children. Bilingual children reach the same communication milestones as monolinguals do (e.g., as babbling, vocabulary, combining words, etc.). Although it is common for a bilingual child to have fewer words in each language, the vocabulary size of both languages combined similar to the one of a monolingual.
How to assess if a bilingual child has a speech or language disorder: When families of a bilingual child seek support from primary care professionals, use the pediatric tools and milestones for monolinguals such as the Rourke Baby Record, Nipissing District Developmental Screen. The Ontario Ministry of Children and Youth Services also provides Speech & Language milestones brochures in 16 different languages.
Refer to first words: WHEN:
· When a child is not meeting the speech and language milestones in his first language.
· When a bilingual child, learning two languages from birth, is not meeting the speech and language milestones in both languages. Usually the errors and the severity of the language delay will be similar in both languages.
6
WHERE: · To a free First Words Community Screening clinic. Parents can
visit www.firstwords.ca or contact Ottawa Public Health either by phone at 613-580-6744 or by e-mail at [email protected] to obtain a list of screening clinics.
· Directly to the First Words Intake Office at CHEO either by phone (613-737-7600 ext. 2500) or by fax (613-738-4893)
Please visit firstwords.ca or contact Roxane Belanger, Speech-Language Pathologist with First Words, at 613-820-4925 ext. 3457 or by e-mail: [email protected] Written by Roxane Bélanger, MOA, SLP-C, reg. CASLPO
[Top]
Champlain Primary Care Digest – A New Collaborative Resource for Physicians The Champlain Primary Care Digest is a new website for physicians and other primary care practitioners in the region. It provides a common space for experts to share articles on a wide variety of topics, and offers useful information about health and community services. Articles posted in the digest are written and reviewed by an editorial team of primary care leads in the following areas of specialization:
· Cancer · Cardiovascular Disease Prevention · Child and Teen Health · Diabetes · Geriatrics and Falls Prevention · Mental Health · Sport and Exercise Medicine · Palliative Care · Electronic Medical Records
Visit the Champlain Primary Care Digest at www.primarycaredigest.org. Comments are open and encouraged. Please feel free to start a discussion at the bottom of any article or share it with your colleagues. This project is led by Dr. Lee Donohue, in collaboration with the Champlain Community Care Access Centre (CCAC). All content on the website is posted and managed by dedicated staff at the CCAC. Written by: Robert Henri, Communications Specialist, Champlain CCAC
[Top]
7
New Resources for Caregivers of Older Adults Over 1 in 4 (27.8%) Canadians who work also take care of elderly friends or family. Caregivers play a significant role in maximizing the health and quality of life of those they are caring for. Support from physicians contributes to a balanced caregiving experience and positively affects the health of both the caregiver and the patient. Ottawa Public Health has resources to help you support the caregivers in your practice!
1. New online guide: Ottawa Public Health Caregiver Guide. Provides concrete information and tips on caring for a loved one as well as information about self- care for caregivers. Available in English and French, this free guide contains videos, and many links to municipal, provincial and federal resources. Throughout the guide caregivers are invited to contact a Public Health Nurse by phone or email if they have further questions or require additional support.
2. New interactive learning session: Caring for an Older Adult. Provides caregivers with the opportunity to discuss the challenges they face and explore strategies for coping with these challenges. Participants will learn about community resources and create a plan to help them in their caregiving role. Available in English and French, each session is tailored to meet the individual needs of the participants and is facilitated by one of our experienced public health nurses. These 1-hour sessions are free. Book a session for your workplace or your community. Contact Ottawa Public Health at 613-580-6744 TTY/ATS: 613-580-9656 or [email protected]
3. Free Resource Guide of community resources available to caregivers of Older adults(seniors). Printed copies are available by order.
4. Print resources which can be ordered from Ottawa Public Health: o Posters to promote the online Ottawa Public Health Caregiver Guide o Tear off pads for easy referral of your caregivers to OPH services o Printed copies of Caring for a senior? Resource Guide for your waiting room.
Contact Ottawa Public Health at 613-580-6744 TTY/ATS: 613-580-9656 or [email protected]. Written by Ann Marie Marn, BScN, Public Health Nurse, OPH
[Top]
8
Information and support for cancer patients and caregivers When a patient receives a cancer diagnosis they and their loved ones may have many questions and may feel fear, anxiety, helplessness or anger. The Canadian Cancer Society offers a range of free cancer information and support services for your patients, their family, friends and caregivers. These services are confidential and many are available in multiple languages. The Society provides:
· Answers to their questions about all types of cancer and many other cancer-related topics through Cancer Information Service . An Information Specialist will take all the time a patient needs to answer their questions and provide information without giving medical advice or recommendations
· Peer Support from someone who’s experienced cancer - Evidence has shown that talking to others who’ve gone through a similar experience is reassuring. The Society’s Peer Support service connects patients and caregivers with fully screened and trained volunteers who’ve had cancer or cared for someone with cancer. Volunteers provide hope, offer encouragement and share ideas for coping
· Information about services available in their community
o Support from an online community of patients and caregivers o Rides to cancer-related appointments and treatment (*A one-time registration
fee may apply) o Help with quitting smoking through Smokers’ Helpline
A recent study by the Propel Centre for Population Health Impact at University of Waterloo showed that the Society’s services have a positive impact on cancer patients and their families. Many people who have used the Society’s services say it helped them get a better understanding of what to expect throughout their own or their loved one’s cancer experience, making them feel more hopeful, in control of their life and less anxious. You can make a difference in the lives of your patients, their family, friends and caregivers by referring them to the Canadian Cancer Society’s cancer information and support services at cancer.ca or toll-free at 1-888-939-3333 (TTY 1-866-786-3934). Submitted by Susan Fekete ([email protected]), Canadian Cancer Society, 613-723-1744 ext. 3616
[Top]
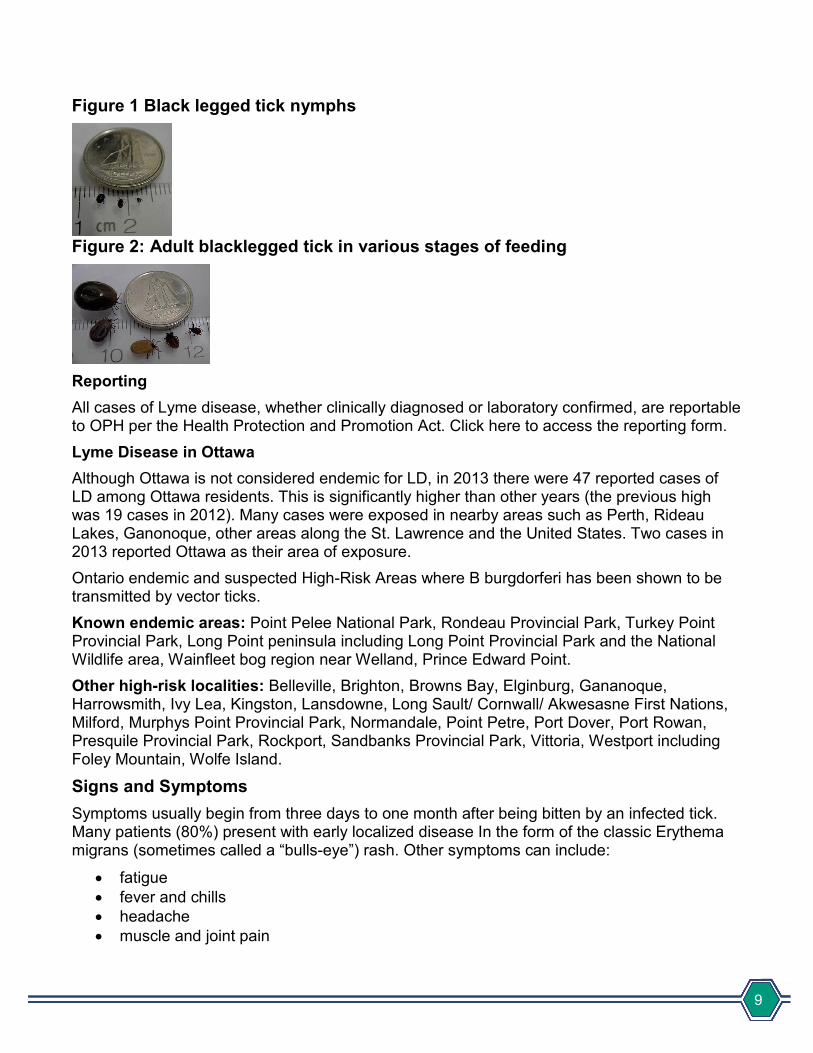
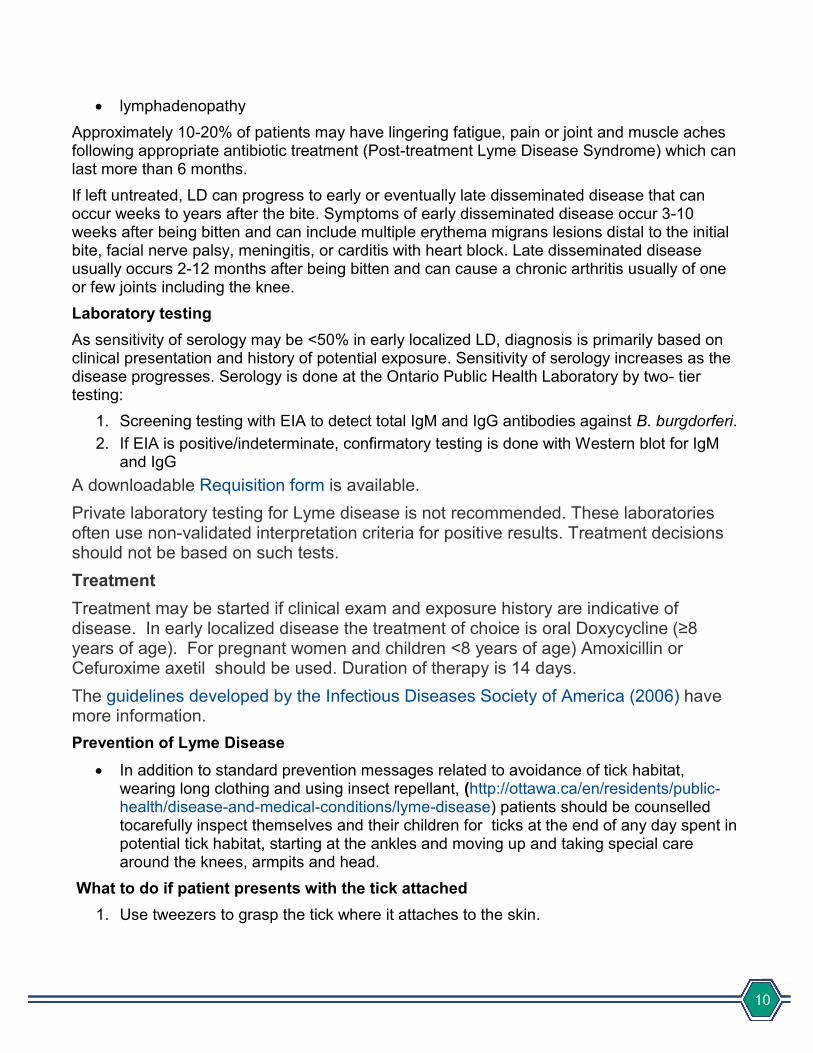
Lyme Disease 101 Lyme disease (LD) is an infection caused by Borrelia burgdorferi, a bacteria transmitted in Ontario through the bite of an infected black-legged tick, commonly known as the deer tick. Most humans are infected through the bite of an immature tick (nymph) during the spring, summer and fall months. Nymphs are the size of poppy seeds and difficult to see. Therefore, they have ample time to feed unnoticed (ticks need to be attached at least 24 hours to transmit the infection). Adult ticks (before feeding) are the size of sesame seeds and are most active during late summer and fall.
9
Figure 1 Black legged tick nymphs
Figure 2: Adult blacklegged tick in various stages of feeding
Reporting All cases of Lyme disease, whether clinically diagnosed or laboratory confirmed, are reportable to OPH per the Health Protection and Promotion Act. Click here to access the reporting form. Lyme Disease in Ottawa Although Ottawa is not considered endemic for LD, in 2013 there were 47 reported cases of LD among Ottawa residents. This is significantly higher than other years (the previous high was 19 cases in 2012). Many cases were exposed in nearby areas such as Perth, Rideau Lakes, Ganonoque, other areas along the St. Lawrence and the United States. Two cases in 2013 reported Ottawa as their area of exposure. Ontario endemic and suspected High-Risk Areas where B burgdorferi has been shown to be transmitted by vector ticks. Known endemic areas: Point Pelee National Park, Rondeau Provincial Park, Turkey Point Provincial Park, Long Point peninsula including Long Point Provincial Park and the National Wildlife area, Wainfleet bog region near Welland, Prince Edward Point. Other high-risk localities: Belleville, Brighton, Browns Bay, Elginburg, Gananoque, Harrowsmith, Ivy Lea, Kingston, Lansdowne, Long Sault/ Cornwall/ Akwesasne First Nations, Milford, Murphys Point Provincial Park, Normandale, Point Petre, Port Dover, Port Rowan, Presquile Provincial Park, Rockport, Sandbanks Provincial Park, Vittoria, Westport including Foley Mountain, Wolfe Island.
Signs and Symptoms Symptoms usually begin from three days to one month after being bitten by an infected tick. Many patients (80%) present with early localized disease In the form of the classic Erythema migrans (sometimes called a “bulls-eye”) rash. Other symptoms can include:
· fatigue · fever and chills · headache · muscle and joint pain
10
· lymphadenopathy Approximately 10-20% of patients may have lingering fatigue, pain or joint and muscle aches following appropriate antibiotic treatment (Post-treatment Lyme Disease Syndrome) which can last more than 6 months. If left untreated, LD can progress to early or eventually late disseminated disease that can occur weeks to years after the bite. Symptoms of early disseminated disease occur 3-10 weeks after being bitten and can include multiple erythema migrans lesions distal to the initial bite, facial nerve palsy, meningitis, or carditis with heart block. Late disseminated disease usually occurs 2-12 months after being bitten and can cause a chronic arthritis usually of one or few joints including the knee. Laboratory testing As sensitivity of serology may be <50% in early localized LD, diagnosis is primarily based on clinical presentation and history of potential exposure. Sensitivity of serology increases as the disease progresses. Serology is done at the Ontario Public Health Laboratory by two- tier testing:
1. Screening testing with EIA to detect total IgM and IgG antibodies against B. burgdorferi. 2. If EIA is positive/indeterminate, confirmatory testing is done with Western blot for IgM
and IgG A downloadable Requisition form is available. Private laboratory testing for Lyme disease is not recommended. These laboratories often use non-validated interpretation criteria for positive results. Treatment decisions should not be based on such tests. Treatment Treatment may be started if clinical exam and exposure history are indicative of disease. In early localized disease the treatment of choice is oral Doxycycline (≥8 years of age). For pregnant women and children <8 years of age) Amoxicillin or Cefuroxime axetil should be used. Duration of therapy is 14 days. The guidelines developed by the Infectious Diseases Society of America (2006) have more information. Prevention of Lyme Disease
· In addition to standard prevention messages related to avoidance of tick habitat, wearing long clothing and using insect repellant, (http://ottawa.ca/en/residents/public-health/disease-and-medical-conditions/lyme-disease) patients should be counselled tocarefully inspect themselves and their children for ticks at the end of any day spent in potential tick habitat, starting at the ankles and moving up and taking special care around the knees, armpits and head.
What to do if patient presents with the tick attached 1. Use tweezers to grasp the tick where it attaches to the skin.
11
2. Pull the tick straight out, slowly and firmly, and do not jerk or twist the tick as this can cause the tick's mouthparts to break off, and cause infection at the feeding site. Avoid squeezing the tick’s abdomen.
3. Disinfect the feeding site after the tick is removed. 4. Place the tick in a sterile container and submit it to the Public Health Laboratory for
identification and testing for B. burgdorferi. Click here to access submission details. Alternatively, the patient can submit the tick to OPH (call 613-580-6744 for submission details).
Chemoprophylaxis Most instances of tick bites do not require antibiotic prophylaxis. Prompt removal of attached ticks is important to prevent Lyme disease. A single 200 mg dose of oral doxycycline may be offered to adult patients and to children 8 years of age and older, when all of the following conditions are met:
· patient presents with an engorged Black-legged tick or history of one that was attached to them for more than 24 hours
· exposure in endemic or high risk area · it has been less than 72 hours since removal of the tick · doxycycline is not contraindicated
Doxycycline is relatively contraindicated for pregnant and breast-feeding women and for children less than 8 years. In these cases, the patient and their provider should make an informed choice between a single dose of doxycycline and no prophylaxis with close observation for typical Erythema migrans rash. For children <8, consultation with an Infectious Disease physician is recommended. For further information:
· Technical Report: Update on Lyme Disease Prevention and Control · Ontario Ministry of Health
o http://www.health.gov.on.ca/en/public/publications/disease/lyme.aspx o http://www.health.gov.on.ca/en/ms/lyme/pdf/pro_cmoh.pdf
· Let's Target Lyme! Ministry of Health Campaign · Lyme Disease Fact Sheet - Public Health Agency of Canada
Written by Claudia Sarbu MD, MSc(c), Medical Resident (PGY-4), Public Health and Preventive Medicine University of Ottawa
References: 1. Heyman, DL. American Public Health Association. Control of communicable diseases
manual. 19th Ed. 2008. Lyme disease; p. 364-9 2. Wormser GP et al. The Clinical Assessment, Treatment, and Prevention of Lyme
Disease, Human Granulocytic Anaplasmosis, and Babesiosis: Clinical Practice Guidelines by the Infectious Diseases Society of America. Clin Inf Dis. 2006; 43:1089-134.
12
3. Warschafsky S et al. Efficacy of antibiotic prophylaxis for the prevention of Lyme Disease: an updated systematic review and meta-analysis. J Antimicrob Chemother. 2010; 65: 1137-1144.
4. Nadelman RB, et al. Prophylaxis with single-dose doxycycline for the prevention of Lyme disease after an ixodes scapularis tick bite. N Engl J Med. 2001;345(2).
5. Feder Jr HM et al. A critical appraisal of « chronic Lyme disease”. N Engl J Med. 2007; (357):1422
6. Lyme disease and other tick-borne diseases: Information for health professionals: http://www.phac-aspc.gc.ca/id-mi/tickinfo-eng.php
7. Guidelines for removal and submission of ticks for identification and possible screening for disease-causing agents: http://www.phac-aspc.gc.ca/id-mi/guide-dir-ti-eng.php
8. Vector-Borne Diseases 2011 Summary Report. June 2012. Prepared by Public Health Ontario: http://www.publichealthontario.ca/en/DataAndAnalytics/Documents/PHO_Vector_Borne_Disease_Report_2011_June_26_2012_Final.pdf
[Top]
Info ‘bites’ on Rabies During the summer months, physicians often see more patients with animal bites or who have had contact with bats and may have questions about potential rabies risk. Here are some information “bites” to help prepare for rabies season:
· Rabies is an infectious disease caused by a virus which infects the central nervous system. If untreated, rabies is fatal to both animals and humans.
· Rabies is usually contracted from scratches or bites by a rabid animal, or alternatively, through contact with animal saliva on mucous membranes, such as the mouth or eyes.
· Symptoms of rabies in humans can take 20-60 days to appear; however, this can vary from days to years depending on the severity and location of the wound, as well as the amount and strain of the virus contracted.
· In Eastern Ontario, rabies is uncommon but can infect a range of animals, including bats, skunks, racoons, livestock, dogs, cats, and foxes.
· From 2011-2013, the majority of confirmed animal rabies cases in Ontario were in bats. Of the 82 cases, 76 (93%) were in bats1, including 4 bats (5%) from the Ottawa-Carleton region2.
If you see a patient with an animal bite or other possible exposure to rabies:
· Clean the wound well. · Ask about where they were exposed, the animal in question, and the animal’s
behaviour. Any abnormal animal behaviour should cause suspicion for rabies. This includes extreme excitement and aggression, unusually friendly wild animals, and animals showing signs of paralysis.
· If your patient was bitten by a domestic animal, ask about up to date rabies vaccination. · Rabies post-exposure prophylaxis is recommended for anyone exposed to an animal
with confirmed or suspected rabies and is provided at no cost to Ottawa residents by Ottawa Public Health regardless of whether the exposure occurred locally or elsewhere.
13
What if my patient was exposed to a bat but I am not sure if they were bitten?
· Post-exposure rabies prophylaxis (PEP) following bat contact is recommended when BOTH the following conditions apply: o There has been direct contact with a bat (i.e. the bat touches or lands on the
person), AND o A bite, scratch, or saliva exposure into a wound or mucous membrane cannot be
ruled out3. o When there is no direct contact with a bat, the risk of rabies is extremely rare and
rabies post-exposure prophylaxis is NOT recommended4.
How to report a possible rabies exposure: · Animal bites or exposures to potentially rabid animals are reportable to Ottawa Public
Health under the Health Protection and Promotion Act. · To report an encounter call Ottawa Public Health at 613-580-6744 (Monday to Friday,
from 8:30 a.m. to 4:30 p.m.) or 3-1-1 outside of these hours. OPH requires the following information: o the reporting physician’s information (name, telephone number, and clinic address) o the patient’s information (name, date of birth, weight, health card number, dates of
any past rabies vaccinations) o date of the incident, the animal involved, incident details and a description of the
wound(s) (number, size, location on body). References
1. Canadian Food Inspection Agency, Animals. (2014). Positive Rabies in Canada. Retrieved from the Canadian Food Inspection Agency website: http://www.inspection.gc.ca/animals/terrestrial-animals/diseases/reporta...
2. Ontario Ministry of Natural Resources. (2014). Rabies Reporter. Retrieved from the Ontario Ministry of Natural Resources Website: http://www.mnr.gov.on.ca/en/Business/Rabies/2ColumnSubPage/196811.html
3. Public Health Agency of Canada. (2012). Canadian Immunization Guide, Part 4 – Active Vaccines. Retrieved from the Public Health Agency of Canada website: http://www.phac-aspc.gc.ca/publicat/cig-gci/p04-rabi-rage-eng.php
4. Ibid [Top]
MERS-CoV and Human Avian Influenza – current statistics and recommendations A travel history is critical to the diagnosis, detection of source and pattern of spread for many infectious diseases, be they spread by person-to-person contact, vector-borne or from a point source such as contaminated food, drink or water. Public Health Ontario recommends that health care providers assess travel history in any patient with signs or symptoms suggestive of severe acute respiratory illness (SARI) and consider the possibility of novel pathogens, such as coronavirus or various influenza viruses.
14
The Ontario Ministry of Health and Long Term Care (MOHLTC) provides guidance for investigating and caring for persons suspected to have an emerging respiratory pathogen. If you are considering an emerging respiratory pathogen in the differential diagnosis of one of your patients, please report the case immediately to Ottawa Public Health at 613-580-6744 ext 24224 (after regular business hours: 3-1-1)A brief summary and additional resources are provided below for infectious SARI agents being monitored globally. Middle East Respiratory Syndrome Coronavirus (MERS-CoV)
· As of 5 May 2014, the World Health Organization (WHO) has reported 263 confirmed human cases, including 93 deaths.1 The epidemic had been stable at low levels in 2013, with about 15 cases notified monthly. This has changed dramatically over the past weeks when we faced an unprecedented increase in cases and community transmission as well as transmission in hospital settings2.
· Assess history of travel to, or residence in, the Arabian Peninsula or neighbouring countries within 14 days before onset of illness
· See the MOHLTC website for information on treatment, case and contact management, case definitions, laboratory testing, reporting, occupational health and safety, and infection prevention and control measures. o Information for health care professionals at MERS-CoV guidance for health workers
and health sector employers, o MERS-CoV Emergency Planning and Preparedness website at
www.ontario.ca/novelcoronavirus.
Human Avian Influenza Influenza A(H7N9)
· As of 6 May 2014, the WHO has reported 430 confirmed human cases, including 146 deaths.3
· No evidence of sustained, ongoing person-to-person spread has been found. To date, China is the only country where avian influenza A(H7N9) viruses are known to be circulating in animals or where human cases have become infected. Cases in other countries were travel-related.
· See the MOHLTC websites for additional information:
o Information for health care professionals: http://www.health.gov.on.ca/en/pro/programs/emb/avian/workers.aspx
o Avian Influenza A(H7N9) Virus - Emergency Planning and Preparedness http://www.health.gov.on.ca/en/pro/programs/emb/avian/
Influenza A(H5N1) · As of March 24, 2014, there have been 661 cumulative cases and 393 deaths since
20034. While human infection is rare, it often results in serious illness with high mortality (60%). Virtually all cases occurred in people who are known to have had direct contact with infected poultry. The risk of human to human transmission is extremely low.
· In January 2014 a case of H5N1 occurred in an Albertan who had travelled to China. This was the first reported case of H5N1 in North America.
15
· A fact sheet is available on the Ministry web site at http://www.health.gov.on.ca/en/news/bulletin/2014/hb_20140110_1.aspx
Influenza A(H10N8) · Influenza A (H10N8) was first reported in humans in December 2013. As of February 4,
2014 there have been two confirmed cases and 1 death in China. The specific source of the infection is unknown. As wild birds/poultry have been known to carry this virus, further sporadic cases may be detected5. Submitted by Kathy Beauregard, RN, and Dr. Rosamund Lewis
References
1. Public Health Agency of Canada http://www.phac-aspc.gc.ca/eri-ire/coronavirus/risk_assessment-evaluatio...
2. Eurosurveillance http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20783
3. Public Health Agency of Canada. http://www.phac-aspc.gc.ca/eri-ire/h7n9/risk_assessment-evaluation_risqu...
4. Public Health Agency of Canada. http://www.phac-aspc.gc.ca/h5n1/index-eng.php
5. World Health Organization. Avian influenza A (H10N8) http://www.wpro.who.int/china/mediacentre/factsheets/h10n8/en/
[Top]
Fever in the returning traveller Fever in the international traveller post-travel is a common scenario. A fever may herald a serious, life-threatening illness; therefore, all returning travellers who are febrile or complaining of a fever should be promptly and thoroughly evaluated. The top infectious causes of fever in international travellers include: malaria (20-30%), acute traveller’s diarrhea (10-20%), and respiratory tract infections (10-15%). Therefore, febrile patients who have travelled to malaria endemic areas should be considered to have malaria until proven otherwise. Accurate diagnosis and appropriate management of the febrile traveller requires a comprehensive travel history that should include:
· pre-travel preparations (e.g., pre-travel immunizations, malaria prophylaxis) · itinerary (e.g., destination, arrival and departure dates) · style of travel (e.g., accommodation, camping, contact with local populations) · purpose of travel (e.g., tourism, business, visiting friends and relatives) · potential exposures (e.g., blood/body fluids, street foods, local water, uncooked meat,
unpasteurized dairy products, fresh water activities, arthropod bites, animal exposures) · medical care or treatment received abroad
16
The pattern (e.g., continuous, biphasic, relapsing) and duration of fever, as well as the apparent incubation period (i.e., time from potential exposure/infection to symptom onset) are also helpful in suggesting possible infectious etiologic agents. The patient also requires a complete physical examination with particular attention paid to localizing symptoms or signs. Although the risk is otherwise extremely low, viral hemorrhagic fever (VHF) should be considered in the differential diagnosis of febrile persons who have returned from endemic regions or specific local areas of a country where VHF cases have recently occurred. In addition to malaria, typhoid fever, shigellosis, cholera, leptospirosis, plague, rickettsiosis, relapsing fever, meningitis, and hepatitis may also be considered in these patients. For additional information, please see “Fever in the Returning International Traveller Initial Assessment Guidelines”, CCDR, ACS-3, July 2011, and “Ebola virus disease: background and summary”, WHO, April 2014 Source : Public Health Ontario. Viral Hemorrhagic Fever: Update for Clinicians. April 9, 2014 http://www.publichealthontario.ca/en/eRepository/VHF_Update_for_Clinicians.pdf [Top]
Should pregnant women be vaccinated against pertussis? In light of the current pertussis epidemiology in Canada, the National Advisory Committee on Immunization (NACI) recently reviewed the issue of whether pregnant women should be vaccinated against pertussis. In January 2014, NACI recommended that women not be universally immunized against pertussis during pregnancy. However, pregnancy is a key opportunity to review immunization status with mothers and offer a pertussis vaccine at that time if the woman has not already received one in adulthood. In Ontario, adults 19-64 years of age are eligible for publicly funded acellular pertussis vaccine if they did not receive the adolescent booster Tdap dose. The issue of pertussis immunization of pregnant women has been a topic of discussion in medical circles in recent years. The greatest morbidity and mortality from pertussis occurs in infants under 6 months of age prior to infants being protected by getting immunized themselves. While the vaccine is safe and immunogenic in pregnancy, and immunization of women late in pregnancy has the potential to protect the infant in the first few months of life through increased transplacental antibody transfer, its effectiveness to prevent severe disease in the newborn is not yet established and the potential to interfere with the infant’s immune response is not yet defined. The full NACI statement, including rationale and references, can be found at: http://publications.gc.ca/collections/collection_2014/aspc-phac/HP40-93-2014-eng.pdf . Dr. Carolyn Pim, Associate Medical Officer of Health
[Top]
17
Ottawa Public Health launches new video mental health resource for parents As physicians, you probably receive questions from parents about their child’s or teen’s mental health. Questions such as:
· “What should I look for if I think my teen is depressed or suicidal?”
· “How can I help my teen cope with stress?” · “Where can I access mental health services for my
teen in Ottawa?” Mental health conditions affect 1 in 5 Canadians and 75% of all mental health conditions have their onset before the age of 24 years. Ottawa Public Health‘s (OPH) “Have That Talk” campaign, a mental health parent education video series, was launched in January 2014. The 4-part video series is intended to equip parents with the knowledge and resources they need to talk openly about mental health with their child or teen. Physicians can help to promote positive mental health in our community by watching these videos at HaveThatTalk.com and sharing them with your patients, community partners, colleagues, friends, and family through Facebook, Twitter, or email. By talking about mental health openly, we are combating mental health stigma and helping to connect individuals to support sooner. For more information on mental health, visit ottawa.ca/MentalHealthResources or call the Ottawa Public Health Information Line at 613-580-6744 (TTY: 613-580-9656). You can also connect with OPH on Facebook, Twitter (@OttawaHealth), Tumblr, Pinterest or YouTube.
[Top]
Geriatric Assessment Outreach Teams - Update The Regional Geriatric Program of Eastern Ontario Specialized Geriatric Services have made numerous changes to the Geriatric Assessment Outreach teams (GAOT) that ensures patients are directed to the right service at the right time. As a result of an evidence based review, the outreach team has revised their home assessment and developed a new telephone assessment for a specific patient population that would benefit from further Specialized Geriatric Services, thus reducing wait times between services. Our Purpose:
· Provide a comprehensive multidimensional screening assessment for people over 65 years of age in their homes or by telephone to improve quality of life, promote functional independence and autonomy and prevent or delay institutionalization unless appropriate
· Work with other health services and community agencies in referring individuals for further assessment, information, or health and social services
When should you consider a referral to GAOT? · Recent changes in physical, mental, or functional abilities; falls, accidents, incontinence,
impaired mobility, decreased ability for self-care, dementia, and delirium. · Major changes in support needs –caregiver stress, institutional placement being
considered.
18
· Safety concerns – physical, psychological, social, and environmental. · Frequent use of the health care system (i.e. in the last 6 months)
o Increasing number of visits to the family physician o Multiple visits to Emergency Department and/or multiple hospital admissions o Escalating home care needs
Referrals Process:
The Outreach Teams are committed to working with the family physician and community service agencies. Referrals are made by telephone or FAX Monday to Friday from 08:00 – 1600. If using the FAX option, the Intake form can be found on the RGPEO website: www.rgpeo.com, and must be completed prior to faxing. The information that will be required when making a referral includes:
· Demographic data · Referral source (who is referring the patient) · Reason for referral · Present problem(s) · Patient’s knowledge of referral · Alternate contact person (family, friend) · Professional services involved
The referrals are triaged; the patient and/or contact person and referral source will be contacted to obtain more information and an appointment will be scheduled at the next available date. Please refer to the Specialized Geriatric Services wait times at www.rgpeo.com for more information. [Top]
Upcoming professional development:
Ottawa Public Health TB Prevention Workshop Date: Spring 2014 (date to be determined) Cost: $20 per person, paid in advance Learn about:
· TB national, provincial, and local · TB pathology epidemiology: · Patient education about TB and the tuberculin skin test · The tuberculin skin test – how to perform, read and interpret the test · Follow-up of positive reactors
For further information and/or to indicate your interest in attending, contact OPH by phone at 613-580-6744 or by e-mail at [email protected] [ Top ]
19
Immunization Competencies for Health Professionals Immunizations are being provided by a growing number and wider range of health professionals. The CPS recognizes the importance of providing interdisciplinary education in this area. The Immunization Competencies Education Program (ICEP) is a 1-day course based on the Immunization Competencies for Health Professionals, which were created by the Professional Education Working Group of the Public Health Agency of Canada. The competencies reflect a national consensus on the education and training required by immunization providers. When: Saturday May 24, 2014 Where: Westin Ottawa 11 Colonel By Drive Ottawa Ontario K1N 9H4 For more information: http://www.cps.ca/en/icep-pfci [ Top ]
Why become an AMO member? The Academy of Medicine Ottawa (AMO) is your local medical organization. Led by a team of elected physicians from Ottawa, the AMO works hard to advocate on behalf of physicians in the Ottawa region and to serve as an excellent source of collegiality, support, and leadership. The AMO is a branch society of the Ontario Medical Association (OMA), and delegates from the Ottawa region represent your interests at the OMA. Please see the AMO’s Report to OMA Council for highlights of our active involvement last year. AMO fees will not increase in 2014 AMO membership provides an opportunity for interaction with colleagues and a way to stay connected with the local medical community through educational, social and representational opportunities. Membership fees support operational costs of the Academy, which permit physician volunteers to work on projects and programs that benefit local physicians and patients. Not an AMO member? Join now! Enjoy the current issue of DocToc, the newsletter for AMO members. The AMO is always keen to have more physicians involved in AMO projects, so if you're interested, please let us know. For more information about the AMO, or to share your ideas, please call or send an e-mail: Dr. Alykhan Abdulla, President Academy of Medicine Ottawa 1867 Alta Vista Drive Ottawa, ON K1G 5W8 Phone: 613-733-2604 Fax : 613-733-9083 E-mail: [email protected] [ Top ]
20
Contact Us:
Ottawa Public Health Monday to Friday 8:30 am to 4:30 pm Phone: 613-580-6744 (Please identify yourself as a physician’s office.) TTY: 613-580-9656 Toll-free: 1-866-426-8885 E-mail: [email protected] Ottawa Public Health website Follow us on Twitter @ottawahealth | @ottawasante Follow us on Pinterest Like us on Facebook (French) Check out our Blog OttawaPublicHealth.ca | SantePubliqueOttawa.ca Medical Officer of Health: Dr. Isra Levy: Medical Officer of Health ext. 23681 Dr. Vera Etches: Associate Medical Officer of Health, Clinical Programs: ext. 23675 Dr. Carolyn Pim: Associate Medical Officer of Health, Community Health Protection ext. 23684 Dr. Rosamund Lewis: Associate Medical Officer of Health, Policy and Partnerships ext. 23684 Medical Officer of Health after hours: Call 3-1-1 and ask for the Ottawa Public Health Manager on call.
Academy of Medicine Ottawa
Academy of Medicine Ottawa 1867 Alta Vista Drive Ottawa, ON, K1G 5W8 Tel 613-733-2604 Fax 613-733-9083 E-mail: [email protected] Website: academymedicineottawa.org Facebook: facebook.com/AMOdocs Twitter: twitter.com/AMOdocs Linkedin: linkedin.com/groups?gid=4688462 [ Top ]
21
Reminder: You must subscribe to receive future communications from OPH! [ Top ]
Version française disponible La Mise à jour pour les médecins est aussi disponible en français. [ Top ]
Read previous issues:
· February 2014 (96) · September 2013 (95) · June 2013 (94) · February 2013 (93) · September 2012 (92) · Special Issue on Mental Health, April 2012 (91) · Special Issue on Seniors, June 2011 (89) · January 2011 (88) · Fall 2010 (87) · Spring/Summer 2010 (86)
[ Top ]