Embed Size (px)
Citation preview

J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 0 , N O . 1 5 , 2 0 1 7
ª 2 0 1 7 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 1 9 3 6 - 8 7 9 8 / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j c i n . 2 0 1 7 . 0 5 . 0 4 2
CORONARY
In-Hospital Outcomes ofPercutaneous Coronary Interventionin America’s Safety NetInsights From the NCDR Cath-PCI Registry
Tushar Acharya, MD,a Adam C. Salisbury, MD, MSC,b,c John A. Spertus, MD, MPH,b,c Kevin F. Kennedy, MS,b,c
Amarbir Bhullar, MD,a H. Kiran K. Reddy, MD,a Bipin K. Joshi, MD,a John A. Ambrose, MDa
ABSTRACT
Fro
Mi
fro
of
rel
Ma
OBJECTIVES This study compared risk-adjusted percutaneous coronary intervention (PCI) outcomes of safety-net
hospitals (SNHs) and non-SNHs.
BACKGROUND Although risk adjustment is used to compare hospitals, SNHs treat a disproportionate share of
uninsured and underinsured patients, who may have unmeasured risk factors, limited health care access, and poorer
outcomes than patients treated at non-SNHs.
METHODS Using the National Cardiovascular Data Registry CathPCI Registry from 2009 to 2015, we analyzed
3,746,961 patients who underwent PCI at 282 SNHs (hospitals where $10% of PCI patients were uninsured) and
1,134 non-SNHs. The relationship between SNH status and risk-adjusted outcomes was assessed.
RESULTS SNHs were more likely to be lower volume, rural hospitals located in the southern states. Patients treated at
SNHs were younger (63 vs. 65 years), more often nonwhite (17% vs. 12%), smokers (33% vs. 26%), and more likely to
be admitted through the emergency department (48% vs. 38%) and to have an ST-segment elevation myocardial
infarction (20% vs. 14%) than non-SNHs (all p < 0.001). Patients undergoing PCI at SNHs had higher risk-adjusted
in-hospital mortality (odds ratio: 1.23; 95% confidence interval: 1.17 to 1.32; p < 0.001), although the absolute risk
difference between groups was small (0.4%). Risk-adjusted bleeding (odds ratio: 1.05; 95% confidence interval: 1.00
to 1.12; p ¼ 0.062) and acute kidney injury rates (odds ratio: 1.01; 95% confidence interval: 0.96 to 1.07; p ¼ 0.51)
were similar.
CONCLUSIONS Despite treating a higher proportion of uninsured patients with more acute presentations,
risk-adjusted PCI-related in-hospital mortality of SNHs is only marginally higher (4 additional deaths per 1,000 PCI
cases) than non-SNHs, whereas risk-adjusted bleeding and acute kidney injury rates are comparable.
(J Am Coll Cardiol Intv 2017;10:1475–85) © 2017 by the American College of Cardiology Foundation.
m the aUniversity of California, San Francisco, Fresno, California; bSaint Luke’s Mid-America Heart Institute, Kansas City,
ssouri; and the cUniversity of Missouri-Kansas City, Kansas City, Missouri. Dr. Salisbury has received research grant support
m Boston Scientific; and speaking fees/honoraria from Abiomed. Dr. Spertus has an analytic contract from the American College
Cardiology Foundation to analyze the National Cardiovascular Data Registry. All other authors have reported that they have no
ationships relevant to the contents of this paper to disclose.
nuscript received April 3, 2017; revised manuscript received May 15, 2017, accepted May 18, 2017.

ABBR EV I A T I ON S
AND ACRONYMS
ACS = acute coronary
syndrome
AKI = acute kidney injury
CI = confidence interval
NCDR = National
Cardiovascular Data Registry
O/E = observed/expected
OR = odds ratio
PCI = percutaneous coronary
intervention
SNH = safety-net hospitals
Acharya et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 0 , N O . 1 5 , 2 0 1 7
PCI-Associated Outcomes in Safety-Net Hospitals A U G U S T 1 4 , 2 0 1 7 : 1 4 7 5 – 8 5
1476
T he complex fabric of Americanhealth care results in some hospitals,often called safety-net hospitals
(SNHs), disproportionately treating a poor,more underserved group of patients thanother hospitals. The Institute of Medicine de-fines SNHs as having 2 distinguishing charac-teristics: they maintain an “open door”policy, offering access to services regardlessof the patient’s ability to pay; and they treata disproportionate share of patients withouthealth insurance and other vulnerable popu-lations (1). As such, SNHs seek to overcomesignificant disparities in access to health in-
surance in the United States. More than 48.6 millionpeople (16% of the U.S. population) had no health in-surance in 2010 (2). Lack of health insurance is associ-ated with less regular outpatient care, greater burdenof cardiovascular risk factors, and a greater likelihoodto present to the hospital with an acute medical emer-gency (3–7). Accordingly, studies have reported higherall-cause mortality among uninsured patients ascompared with the age- and sex-matched insured pa-tients (8,9). Given that SNHs care for this unique, andpotentially higher risk population of uninsured pa-tients in a potentially limited-resource setting, it isimportant to understand how outcomes of SNHscompare with non-SNHs.
SEE PAGE 1486
Although regional studies have reported higherpercutaneous coronary intervention (PCI)-associatedmortality in underinsured patients (10,11), it isunclear whether these outcomes are caused by thepatients’ risk factors, or are attributable to the carethat they receive at SNHs. This is a complex issue todisentangle, but can have an important impact onpublic policy. To address the different populationstreated at different hospitals, efforts to createrisk-adjustment models have been undertaken bynational organizations, such as the American Collegeof Cardiology’s National Cardiovascular Data Registry(NCDR). The NCDR has created risk models for peri-procedural outcomes after PCI to enable hospitalcomparisons. However, many of the unique featuresof patients treated at SNHs may not be incorporatedinto these models. Comparing the risk-adjusted out-comes of SNHs and non-SNHs can provide importantinsights into the validity of NCDR risk models incomparing different types of hospitals.
To address this gap in knowledge, we assessed keyin-hospital PCI outcomes, including mortality,bleeding, and acute kidney injury (AKI), bycomparing risk-adjusted outcomes for SNHs and
non-SNHs using the NCDR CathPCI registry (12).Identifying substantial discordance in outcomescould indicate either substantially worse care atSNHs, or poor model performance because of impor-tant, unmeasured confounders.
METHODS
PATIENT POPULATION. Details of the NCDR CathPCIRegistry have been described previously (12,13).Briefly, the registry prospectively collects data onpatient characteristics, clinical features, angiographicand procedural details, and in-hospital outcomes ofpatients receiving diagnostic angiography or PCI atparticipating hospitals to facilitate comparativeassessment and to affect guideline adherence andquality improvement. Participating institutions enterdata locally using NCDR-certified software. Standarddata definitions are used at all participating sites toensure uniformity and comparability. The CathPCIdata collection form includes information on de-mographics, comorbidities, medications, clinicalpresentation, clinical course, diagnostic testing, pro-cedures (along with indications and multiple angio-graphic variables), complications, and outcomes.Forms submitted to the NCDR undergo auditing toensure completeness and accuracy before beingentered into the database (12).
A total of 1,585 U.S. hospitals reported data for3,783,700 PCIs to the NCDR CathPCI registry betweenthird quarter of 2009 and first quarter of 2015, theperiod of Version 3 of the NCDR data collection form.After excluding hospitals that reported <8 quarters ofdata and those performing <30 PCIs per year, 1,416hospitals and 3,746,961 patients were included in thefinal analysis.
DEFINITION OF SNHS. There is no universallyaccepted definition for SNHs. The Agency of Health-care Research and Quality has suggested that theuninsured may comprise more than 9% of SNH stays(14). Accordingly, for this study, we defined SNHs asthose hospitals that perform 10% or more PCIs onuninsured patients. Using data from the NCDR Cath-PCI data collection form, which collects insurancepayer status at the time of PCI (categories areMedicaid, Medicare, private health insurance, mili-tary health care, state-specific plan, Indian healthservice, non-U.S. insurance, or “none”), we consid-ered SNHs as those hospitals for whom $10% of theirpatients had no health insurance.
OUTCOMES OF INTEREST. The NCDR has publishedrisk models for periprocedural bleeding (15), AKI (16),and in-hospital mortality (17). For each outcome,

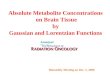
FIGURE 1 Study Design
NCDR ¼ National Cardiovascular Data Registry.
TABLE 1 Hospital Characteristics
Safety Net Hospital
p ValueYes
(n ¼ 282)No
(n ¼ 1,134)
Census region <0.001
Midwest 54 (19.2) 349 (30.8)
Northeast 9 (3.2) 181 (16.0)
South 186 (66.2) 356 (31.4)
West 32 (11.4) 248 (21.9)
Hospital location 0.221
Rural 62 (22.0) 199 (17.5)
Suburban 98 (34.8) 408 (36.0)
Urban 122 (43.3) 527 (46.5)
Participant type <0.001
Government 13 (4.6) 10 (0.9)
Private/community 239 (84.8) 1,034 (91.2)
University 30 (10.6) 90 (7.9)
Teaching hospital 91 (32.3) 441 (38.9) 0.039
Public hospital 99 (35.1) 402 (35.4) 0.914
Onsite surgical backup 158 (56.0) 819 (72.2) <0.001
Average hospital PCIvolume per year
364.5 � 309.7 537.7 � 454.6 <0.001
Average operator PCIvolume per year
82.3 � 50.5 99.8 � 65.6 <0.001
Quarters of data submission 20.0 � 4.2 20.4 � 4.2 0.142
Values are n (%) or mean � SD.
PCI ¼ percutaneous coronary intervention.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 0 , N O . 1 5 , 2 0 1 7 Acharya et al.A U G U S T 1 4 , 2 0 1 7 : 1 4 7 5 – 8 5 PCI-Associated Outcomes in Safety-Net Hospitals
1477
we used the previously published definitions thatwere used to develop the risk models. Periproceduralbleeding was defined as any of the following eventsoccurring within 72 h after PCI: arterial access sitebleeding (either external or a hematoma >10 cm forfemoral access, >5 cm for brachial access, or >2 cm forradial access); retroperitoneal, gastrointestinal, orgenitourinary bleeding; intracranial hemorrhage;cardiac tamponade; post-procedure hemoglobindecrease of 3 g/dl in patients with a pre-procedurehemoglobin level #16 g/dl; or post-procedure non-bypass-surgery-related blood transfusion for patientswith a pre-procedure hemoglobin level $8 g/dl. ForAKI, the Acute Kidney Injury Network stage 1 orgreater definition was used: a $0.3 mg/dl absoluteor $1.5-fold relative increase in post-PCI creatinine ornew initiation of dialysis.
STATISTICAL ANALYSIS. Baseline hospital andpatient characteristics of SNHs and non-SNHs werereported as proportions and groups were comparedusing chi-square test. Continuous variables werereported as mean � SD and compared using Student ttests. Skewed data were reported as median (inter-quartile range) and were compared using Wilcoxonrank sum test.
Hierarchical multivariable logistic regression wasused to assess the relationship between SNH statusand risk-adjusted mortality, bleeding, and AKI. Pub-lished NCDR risk models for bleeding (15), AKI (16),and mortality analysis (17) were used to adjust forpotential confounding. In all of these models, impu-tation of missing data was handled as defined by thepublished risk models (15–17). Strength of associationwas expressed by odds ratio (OR) with 95% confi-dence intervals (CI). Two sided p values of <0.05were considered statistically significant. We thencalculated predicted or expected outcomes from thepreviously mentioned regression models, and theobserved outcome rate of SNHs and non-SNHs wasdivided by their predicted rate to obtain theobserved/expected (O/E) outcome ratios (18). Allanalyses were performed with SAS version 9.4 (SASInstitute, Cary, North Carolina).
SUBGROUP ANALYSES. Because hospital volume isan important predictor of PCI-associated mortality,we performed subgroup analysis in low (<400 cases/year), intermediate (400 to 1,000 cases/year), andhigh (>1,000 cases/year) volume hospitals todetermine if mortality difference between SNH andnon-SNHs was a function of their volume status.Similarly, subgroup analysis was performed based onPCI indication (acute coronary syndrome [ACS] andnon-ACS). Temporal trends were analyzed.

TABLE 2 Patient Characteristics
Safety-Net HospitalStandard
Difference (%)* p ValueYes (n ¼ 531,441) No (n ¼ 3,215,520)
Age, yrs 63.1 � 12.1 65.1 � 12.0 3.3 <0.001
Male 358,401 (67.4) 219,2317 (68.2) 4.2 <0.001
Body mass index, kg/m2 30.2 � 14.2 30.1 � 11.3 0.5 <0.001
Race
White 441,142 (83.0) 2,832,385 (88.1) 14.5 <0.001
Black or African American 70,964 (13.4) 244,030 (7.6) 18.9 <0.001
Hispanic or Latino ethnicity 43,416 (8.2) 159,024 (5.0) 13.1 <0.001
Asian 10,563 (2.0) 83,765 (2.6) 4.1 <0.001
American Indian or Alaskan Native 3,312 (0.6) 19,151 (0.6) 0.4 0.015
Native Hawaiian or Pacific Islander 806 (0.2) 7,516 (0.2) 1.9 <0.001
Insurance
Uninsured 74,185 (14.0) 173,597 (5.4) 29.3 <0.001
Medicaid 55,133 (10.4) 319,981 (10.0) 1.4 <0.001
Medicare 249,397 (46.9) 1,688,613 (52.5) 11.2 <0.001
Private health insurance 280,715 (52.8) 2,104,597 (65.5) 25.9 <0.001
Military health care 17,329 (3.3) 92,551 (2.9) 2.4 <0.001
State-specific plan 9,061 (1.7) 45,376 (1.4) 2.4 <0.001
Indian Health Service 496 (0.1) 5,929 (0.2) 2.5 <0.001
Comorbidities
Hypertension 431,358 (81.2) 2,645,866 (82.3) 2.9 <0.001
Diabetes mellitus 201,365 (37.9) 1,196,115 (37.2) 1.4 <0.001
Dyslipidemia 398,329 (75.0) 2,549,235 (79.4) 10.4 <0.001
Current/recent smoking (within 1 year) 176,303 (33.2) 846,900 (26.4) 15.0 <0.001
Family history of premature coronary artery disease 130,701 (24.6) 759,275 (23.6) 2.3 <0.001
Prior myocardial infarction 157,491 (29.6) 973,611 (30.3) 1.4 <0.001
Prior heart failure 64,226 (12.1) 406,625 (12.6) 1.7 <0.001
Prior PCI 196,625 (37.0) 1,319,712 (41.0) 8.3 <0.001
Prior coronary artery bypass grafting 82,959 (15.6) 594,167 (18.5) 7.6 <0.001
Prior valve surgery/procedure 6,407 (1.2) 50,828 (1.6) 3.2 <0.001
Cerebrovascular disease 61,462 (11.6) 408,230 (12.7) 3.5 <0.001
Peripheral arterial disease 59,082 (11.1) 405,544 (12.6) 4.6 <0.001
Chronic lung disease 82,601 (15.5) 489,902 (15.2) 0.9 <0.001
On dialysis 15,223 (2.9) 79,423 (2.5) 2.4 <0.001
GFR 72.2 � 18.1 71.7 � 18.0 2.4 <0.001
Admission source
Emergency department 255,798 (48.2) 1,209,437 (37.7) 21.4 <0.001
Transfer in from another acute care facility 93,572 (17.6) 606,336 (18.9) 3.3 <0.001
Other 181,694 (34.2) 1,396,314 (43.5) 19.1 <0.001
PCI status
Elective 178,146 (33.5) 1,318,704 (41.0) 15.5 <0.001
Urgent 224,930 (42.3) 1,322,447 (41.1) 2.4 <0.001
Emergency 125,072 (23.5) 561,494 (17.5) 15.1 <0.001
Salvage 3,025 (0.6) 11,702 (0.4) 3.0 <0.001
Continued on the next page
Acharya et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 0 , N O . 1 5 , 2 0 1 7
PCI-Associated Outcomes in Safety-Net Hospitals A U G U S T 1 4 , 2 0 1 7 : 1 4 7 5 – 8 5
1478
SENSITIVITY ANALYSIS. In the absence of a univer-sally acceptable definition of SNHs, 2 sensitivityanalyses were performed with PCI-performing hos-pitals stratified according to their Medicaid rate andDisproportionate Share Hospital Index. Details ofthese analyses are documented in the OnlineAppendix. Finally, we examined unadjusted in-hospital mortality rates among the uninsured versusinsured patients.
RESULTS
A total of 282 SNHs performed 531,441 PCIs betweenthe third quarter of 2009 and first quarter of 2015, and3,215,520 PCIs were performed at 1,134 non-SNHs(Figure 1). SNHs were more likely to be rural hospi-tals and were twice as likely to be located in thesouthern U.S. states (66% vs. 31%). They had asignificantly lower annual PCI volume (365 vs. 538 PCI

TABLE 2 Continued
Safety-Net HospitalStandard
Difference (%)* p ValueYes (n ¼ 531,441) No (n ¼ 3,215,520)
PCI indication
Immediate PCI for STEMI 106,384 (20.0) 451,895 (14.1) 15.9 <0.001
PCI for STEMI (unstable, >12 h from symptom onset) 5,934 (1.1) 29,852 (0.9) 1.9 <0.001
PCI for STEMI (stable, >12 h from symptom onset) 2,923 (0.6) 14,238 (0.4) 1.5 <0.001
PCI for STEMI (after successful thrombolysis) 1,974 (0.4) 11,457 (0.4) 0.3 <0.001
Rescue PCI for STEMI (after failed thrombolysis) 2,929 (0.6) 16,024 (0.5) 0.7 <0.001
PCI for high-risk non-STEMI or unstable angina 271,904 (51.2) 1,618,340 (50.3) 1.7 <0.001
Staged PCI 35,280 (6.6) 226,639 (7.1) 1.4 <0.001
Other 103,978 (19.6) 846,060 (26.3) 16.1 <0.001
Coronary artery disease presentation
No angina 29,197 (5.5) 233,965 (7.3) 7.3 <0.001
Symptom unlikely to be ischemia 11,439 (2.2) 76,654 (2.4) 1.6 <0.001
Stable angina 61,082 (11.5) 495,560 (15.4) 11.5 <0.001
Unstable angina 191,454 (36.0) 1,249,041 (38.9) 5.8 <0.001
Non-STEMI 120,970 (22.8) 648,746 (20.2) 6.3 <0.001
STEMI or equivalent 117,183 (22.1) 510,687 (15.9) 15.8 <0.001
Angina classification within 2 weeks
No symptoms 56,344 (10.6) 341,646 (10.6) 0.1 0.627
CCS I 20,507 (3.9) 137,617 (4.3) 2.1 <0.001
CCS II 76,759 (14.5) 503,992 (15.7) 3.4 <0.001
CCS III 181,905 (34.3) 1,120,424 (34.9) 1.2 <0.001
CCS IV 194,456 (36.7) 1,105,225 (34.4) 4.7 <0.001
Antiangina medication within 2 weeks 359,548 (67.7) 2,309,943 (71.9) 9.1 <0.001
Heart failure within 2 weeks 59,823 (11.3) 345,023 (10.7) 1.7 <0.001
Cardiomyopathy or left ventricular systolic dysfunction 58,823 (11.1) 352,763 (11.0) 0.3 0.034
Pre-PCI left ventricular ejection fraction 51.6 � 12.7 52.3 � 12.6 5.9 <0.001
Cardiogenic shock within 24 h 14,774 (2.8) 66,483 (2.1) 4.6 <0.001
Cardiac arrest within 24 h 14,694 (2.8) 65,352 (2.0) 4.8 <0.001
Angiographic variables
Number of diseased vessels 4.2 <0.001
1 275,946 (51.9) 1,607,772 (50.0)
2 153,684 (28.9) 942,090 (29.3)
3 93,917 (17.7) 616,739 (19.2)
Class C lesion 308,000 (58.1) 1,796,576 (56.0) 4.3 <0.001
Coronary thrombus 108,464 (20.5) 490,059 (15.3) 13.6 <0.001
Bifurcation lesion 72,048 (13.6) 422,990 (13.2) 1.2 <0.001
Proximal left anterior descending PCI 97,868 (18.5) 595,012 (18.6) 0.2 0.146
Left main PCI 10,220 (1.9) 83,752 (2.6) 4.6 <0.001
Chronic total occlusion 17,089 (3.2) 111,155 (3.5) 1.3 <0.001
In-stent thrombosis 12,965 (2.4) 60,057 (1.9) 3.9 <0.001
Significant dissection 6,598 (1.2) 38,057 (1.2) 0.5 <0.001
Perforation 2,092 (0.4) 11,883 (0.4) 0.4 0.007
Total stent length 23.0 (16.0–36.0) 23.0 (16.0–36.0) 3.4 <0.001
Minimum stent diameter 3.0 (2.5–3.0) 3.0 (2.5–3.0) 1.0 <0.001
IABP 14,970 (2.8) 80,608 (2.5) 1.9 <0.001
Contrast volume 197.8 � 88.8 189.8 � 87.8 9.1 <0.001
Fluoroscopy time 14.5 � 11.3 15.0 � 11.9 4.4 <0.001
Values are mean � SD, n (%), or median (IQR). *Standard difference of $10% is considered statistically significant.
CCS ¼ Canadian Cardiovascular Society; GFR ¼ glomerular filtration rate; IABP ¼ intra-aortic balloon pump; IQR ¼ interquartile range; PCI ¼ percutaneous coronaryintervention; STEMI ¼ ST-segment elevation myocardial infarction.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 0 , N O . 1 5 , 2 0 1 7 Acharya et al.A U G U S T 1 4 , 2 0 1 7 : 1 4 7 5 – 8 5 PCI-Associated Outcomes in Safety-Net Hospitals
1479
cases/year) and lower operator volume (82 vs. 100cases/year), compared with non-SNHs (Table 1). Pa-tients treated at SNHs were younger (63 vs. 65 years)and more often nonwhite (17% vs. 12%). Their
smoking rates were higher (33% vs. 26%). They weremore frequently admitted for PCI through the emer-gency department (48% vs. 38%) rather than throughoutpatient referral. PCIs performed at SNHs were

TABLE 3 Observed Outcomes
Outcomes
Safety-Net Hospital
p ValueYes
(n ¼ 531,441)No
(n ¼ 3,215,520)
Death 10,279 (1.9) 49,115 (1.5) <0.001
Bleeding 30,812 (5.8) 169,721 (5.3) <0.001
Bleeding requiringtransfusion
12,881 (2.4) 79,064 (2.5) 0.125
Acute kidney injury 31,744 (7.4) 182,343 (7.1) <0.001
Vascular complicationsrequiring treatment
2,258 (0.4) 13,209 (0.4) 0.137
Stroke 1,421 (0.3) 7,789 (0.2) <0.001
Periprocedural myocardialinfarction
11,581 (2.2) 62,967 (2.0) <0.001
Urgent coronary arterybypass grafting
4,501 (0.8) 23,704 (0.7) <0.001
Tamponade 480 (0.1) 2,979 (0.1) 0.605
Length of stay 3.4 � 5.3 3.1 � 4.3 <0.001
Values are n (%) or mean � SD.
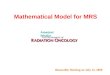
FIGURE 2 O/E Rat
O/E ratios for percut
O/E ¼ observed/exp
Acharya et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 0 , N O . 1 5 , 2 0 1 7
PCI-Associated Outcomes in Safety-Net Hospitals A U G U S T 1 4 , 2 0 1 7 : 1 4 7 5 – 8 5
1480
more likely to be emergent (24% vs. 18%) and lesslikely to be elective procedures (34% vs. 41%). Theywere also more frequently primary PCIs for ST-segment elevation myocardial infarction (20% vs.14%) than for other indications (Table 2).
ios for Percutaneous Coronary Intervention
aneous coronary intervention–associated (A) in-hospital mortality, (B) bleed
ected; SNH ¼ safety-net hospital.
In unadjusted analyses, patients undergoing PCI atSNHs had a 0.4% higher absolute risk of mortality,0.5% higher absolute risk of periprocedural bleeding,and 0.3% higher absolute risk of AKI related to the PCIprocedure (Table 3). After adjusting for patients’characteristics using the NCDR risk model, patientstreated at SNHs had higher risk-adjusted in-hospitalmortality (OR: 1.23; 95% CI: 1.17 to 1.32; p < 0.001), butsimilar risk-adjusted bleeding (OR: 1.05; 95% CI: 1.00to 1.12; p¼0.62) and AKI (OR: 1.01; 95% CI: 0.96 to 1.07;p ¼ 0.51). Similarly, patients treated at SNHs hadhigher O/E mortality risk (1.20 vs. 0.99; p < 0.001), butsimilar O/E bleeding (1.09 vs. 1.06; p ¼ 0.157) and AKI(0.96 vs. 0.93; p ¼ 0.259) rates (Figure 2).
Results of the subgroup analyses are detailedin Figure 3. There was modest attenuation of thein-hospital mortality difference between SNH andnon-SNH when stratified by PCI volume. High-volume hospitals had a lower mortality difference(OR: 1.15; 95% CI: 0.95 to 1.41; p ¼ 0.159) followed byintermediate-volume (OR: 1.16; 95% CI: 1.07 to 1.27;p < 0.001), and low-volume hospitals having thelargest mortality difference (OR: 1.26; 95% CI: 1.16to 1.37; p < 0.001). Both ACS (OR: 1.18; 95% CI: 1.11to 1.25; p < 0.001) and non-ACS groups (OR: 1.26;
ing, and (C) acute kidney injury in SNH versus non-SNH.

FIGURE 3 Risk-Adjusted Outcomes and Subgroup Analysis
Effect of SNH status on (A) in-hospital mortality, (B) in-hospital bleeding, and (C) in-hospital AKI. ACS ¼ acute coronary syndrome; AKI ¼ acute kidney injury;
OR ¼ odds ratio; other abbreviations as in Figure 2.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 0 , N O . 1 5 , 2 0 1 7 Acharya et al.A U G U S T 1 4 , 2 0 1 7 : 1 4 7 5 – 8 5 PCI-Associated Outcomes in Safety-Net Hospitals
1481
95% CI: 1.14 to 1.39; p < 0.001) had statistically higherPCI mortality when treated at SNHs. Subgroupanalyses for bleeding and AKI are similarly shown inFigure 3.
Temporal trends comparing in-hospital mortalityover the time period of this analysis are shown in
Figure 4. There was no significant trend toward eitherharm or improvement from 2009 through 2015 andthe O/E in-hospital mortality ratios of SNH and non-SNHs remained fairly unchanged.
To put the results of the primary analysis inperspective, PCI-associated in-hospital mortality for

FIGURE 4 Temporal Trends
Temporal trends in observed to expected ratios for percutaneous coronary intervention–
associated in-hospital mortality in SNH versus non-SNH. Abbreviation as in Figure 2.
Acharya et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 0 , N O . 1 5 , 2 0 1 7
PCI-Associated Outcomes in Safety-Net Hospitals A U G U S T 1 4 , 2 0 1 7 : 1 4 7 5 – 8 5
1482
insured and uninsured patients were calculated fromthis data set. The unadjusted in-hospital mortalityrate of the uninsured was 2.2% compared with 1.5% inthe insured (p < 0.001).
DISCUSSION
In the absence of universal health care coverage,uninsured and underinsured patients in the UnitedStates depend on the medical safety-net for medicaland procedural care. In this study, we found thatdespite treating a large proportion of uninsured pa-tients with more acute presentations, key PCI-relatedoutcome of in-hospital mortality was only marginallyhigher in SNHs (23% relative risk difference; 0.4%absolute risk difference) compared with non-SNHs,whereas periprocedural bleeding and AKI weresimilar. These findings were robust to sensitivity an-alyses, including stratification by hospitals’ PCI vol-ume and presentation with either ACS or stablecoronary artery disease.
Underinsurance is a risk factor for poor PCI-associated outcomes. Because SNHs treat moreuninsured patients, it is important to evaluate howtheir outcomes differ from non-SNHs. In 2011, a studyfrom the Washington Hospital Center examining a10-year experience of PCI found that uninsured pa-tients had a higher rate of risk-adjusted cardiacevents (composite of death, Q-wave myocardialinfarction, and target vessel revascularization) at 1year when compared with patients with private
insurance (10). Similarly, an analysis of a contempo-rary PCI cohort from 4 New York teaching hospitalsshowed an increased risk of in-hospital mortalityamong patients without insurance or with Medicaid(11). The causes of these differences in outcome areunclear. Some have suggested this may reflect dif-ferences in time to revascularization and revascular-ization strategies (e.g., use of drug-eluting stents)between those with and without insurance (19–23), orthat these patients may be less likely to receiveevidence-based medications for coronary artery dis-ease (24). In the present study cohort, the PCI-associated in-hospital mortality for the uninsuredwas 2.2% compared with 1.5% in the insured (p <
0.001). We evaluated if these differences in outcomesat the patient level would translate to hospitalstreating them. It has been shown that hospitals withdifferent organizational characteristics and owner-ship status have different PCI outcomes (25). In thepresent study, we found that although there weresignificant differences in insured rates and key riskfactors for outcomes (e.g., more acute presentations)clinical outcomes of SNHs and non-SNHs were onlyslightly dissimilar after standard risk adjustment.
There were important geographical and de-mographic differences between SNHs and non-SNHs.Consistent with prior reports that have noted largeuninsured populations in southern U.S. states, wefound that SNHs were more common in the south(26). We also found that SNHs treated more nonwhitepatients with higher smoking rates. Despite baselinedifferences between groups, we found statisticallyhigher rates of in-hospital mortality but no differencein bleeding and AKI rates. Even though the relativerisk of PCI-associated mortality was 20% higher, theabsolute risk difference between outcomes at SNHand non-SNHs difference was small (4 additionaldeaths in SNHs per 1,000 patients treated; numberneeded to harm ¼ 250). Similarly, comparison of O/Eratios revealed a modest statistically higher mortalityin the SNH group with no difference in bleeding andAKI.
The drivers of this small increase in mortality atSNHs may be a consequence of higher mortality in theuninsured population. We evaluated if clustering ofmore acutely ill patients at SNHs (11% more emer-gency department admissions; 6% more ST-segmentelevation myocardial infarction presentations) maylead to higher mortality; but in subgroup analysis,mortality at SNHs was higher in both ACS and stablecoronary artery disease groups treated at SNHs.Lower PCI volume of SNHs (365 vs. 538 PCIs per year)could also be a contributor to the excess mortality(27–37). On substratification of hospitals based on

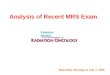
FIGURE 5 Graphic Representation of Percutaneous Coronary Intervention Hospitals Arranged According to Their Percentage Share
Graphic representation of percutaneous coronary intervention hospitals arranged according to their percentage share of (A) uninsured
patients, (B) Medicaid patients, and (C) DSH. Observed percutaneous coronary intervention outcomes (in-hospital mortality, AKI,
and bleeding) are represented as labeled. DSH ¼ Disproportionate Share Hospital Index; other abbreviations as in Figures 2 and 3.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 0 , N O . 1 5 , 2 0 1 7 Acharya et al.A U G U S T 1 4 , 2 0 1 7 : 1 4 7 5 – 8 5 PCI-Associated Outcomes in Safety-Net Hospitals
1483
volume, we found that higher hospital volume doesattenuate the mortality difference between SNHs andnon-SNHs to some extent, although with larger CI(Figure 2). High-volume SNHs may be performing atpar with non-SNHs.
Regardless, it is reassuring that despite multiplereasons for faring worse on important periproceduraloutcomes, in-hospital mortality of patients undergo-ing PCI at SNHs was, in reality, only slightly worsethan non-SNHs. This better-than-expected perfor-mance of SNHs may partly be explained by the factthat most patients treated at SNHs or non-SNHswere insured (Table 2). Thus, the actual contributionof uninsured patients to the overall outcome of ahospital may be small. Another possibility is thatthe definition used in this study (based on the lackof insurance) may not accurately represent SNHs.To test this possibility, we performed sensitivity
analyses by stratifying hospitals by their share ofMedicaid patients and by their DisproportionateShare Hospital Index (Figure 5). Regardless of the SNHdefinition used (based on uninsured rate, Medicaidrate, or Disproportionate Share Hospital Index), theoutcomes did not vary in any significant manner.
Going forward, it is important to note that since theintroduction of the Affordable Care Act, the percent-age of uninsured patients in the United States hassteadily declined (from 16.0% in 2010 to 9.2% in early2015) (38). This changing landscape may narrow thecurrent health care gap and could redefine the role ofSNHs. However, recent events leading to the immi-nent repeal and/or replacement of the AffordableCare Act could add further flux to an already fluidfield. In the absence of a foreseeable scenario ofuniversal health care, it is perhaps safe to assume thatSNHs will continue to play a vital role in providing

PERSPECTIVES
WHAT IS KNOWN? Uninsured patients, because of
unmeasured risk factors and limited health care
access, have poorer PCI-associated outcomes than the
insured. SNHs treat a disproportionate share of
uninsured and underinsured patients. PCI-associated
in-hospital outcomes of SNHs are not known.
WHAT IS NEW? Despite treating a higher proportion
of uninsured patients with more acute presentations,
risk-adjusted PCI-related in-hospital mortality of
SNHs is only marginally higher (4 additional deaths
per 1,000 PCI cases) than non-SNHs, whereas
risk-adjusted bleeding and acute kidney injury rates
are comparable. This difference in mortality has been
stable from 2009 through 2015.
WHAT IS NEXT? Whether obtaining health
insurance leads to better health care access and
translates into improvement of outcomes including
procedural mortality requires further study.
Acharya et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 0 , N O . 1 5 , 2 0 1 7
PCI-Associated Outcomes in Safety-Net Hospitals A U G U S T 1 4 , 2 0 1 7 : 1 4 7 5 – 8 5
1484
much needed medical care to the underprivileged.Patients with “less desirable” insurance may still tendto cluster at SNHs, because other hospitals may bereluctant to accept them. It is also fairly common-place that under-resourced patients treated at SNHsare less mobile and are likely to present to SNHs neartheir home regardless of insurance status.
STUDY LIMITATIONS. Because of its observationalnature, our findings are subject to unmeasured andresidual confounding. As with all registries, theaccuracy of documentation and submission of data isdependent on participating hospitals, although thereis no evidence of variation in the quality of datacapture between SNHs and non-SNHs. The possibilityof a revascularization selection bias (surgery vs. PCIvs. medical therapy) between comparisons cannot beruled out. The NCDR CathPCI registry does not collectdata elements on degree of risk factor control atbaseline, socioeconomic status, and access to healthcare. These potentially important determinants ofoutcome were not part of the study. Results of thisstudy may, perhaps, not apply to a small minority ofhospitals not participating in the registry. However,Cath PCI registry collects data from most, if not all ofthe U.S. hospitals offering PCI to patients. Because ofthis large representation, these results should begeneralizable. Finally, this study only evaluatedin-hospital outcomes and it is conceivable thatlong-term outcomes of patients getting PCI at SNHsmay differ.
CONCLUSIONS
Despite treating large numbers of uninsured patientswith more acute presentations, risk-adjusted PCI-related in-hospital mortality of SNHs is only margin-ally higher than non-SNHs, with no difference inperiprocedural bleeding and AKI rates. This suggests
that current risk models can serve as a foundation forcomparing SNHs and non-SNHs. It is perhaps evenreassuring that America’s PCI SNHs, despite treating acomplex and acutely ill population, are able to ach-ieve satisfactory if not similar outcomes as non-SNHs.Whether obtaining health insurance will lead to bet-ter health care access and translate into improvementof outcomes including procedural mortality remainsunclear and requires further study.
ADDRESS FOR CORRESPONDENCE: Dr. John A.Ambrose, UCSF Fresno, Division of Cardiology AcademicOffices, 2335 East Kashian Lane, Suite 460, Fresno,California 93721. E-mail: [email protected].
RE F E RENCE S
1. National Research Council. America’s HealthCare Safety Net: Intact but Endangered. Wash-ington, DC: The National Academies Press, 2000.
2. Cohen RA, Ward BW, Schiller JS. Health insurancecoverage: early release of estimates from theNationalHealth Interview Survey, 2010. National Center forHealthStatistics. June2011.Available at: http://www.cdc.gov/nchs/nhis.htm. Accessed February 12, 2016.
3. Institute of Medicine Committee on the Conse-quences of Uninsurance. Coverage Matters: In-surance and Health Care. Washington, DC:National Academy Press, 2001.
4. Institute of Medicine Committee on the Con-sequences of Uninsurance. A Shared Destiny:Community Effects of Uninsurance. Washington,DC: National Academies Press, 2003.
5. Asplin BR, Rhodes KV, Levy H, Lurie N, Crain AL,Carlin BP, Kellermann AL. Insurance status andaccess to urgent ambulatory care follow-up ap-pointments. JAMA 2005;294:1248–54.
6. Newton MF, Keirns CC, Cunningham R,Hayward RA, Stanley R. Uninsured adults pre-senting to US emergency departments: assump-tions vs data. JAMA 2008;300:1914–24.
7. Weber EJ, Showstack JA, Hunt KA, Colby DC,Callaham ML. Does lack of a usual source of careor health insurance increase the likelihood of anemergency department visit? Results of a nationalpopulation-based study. Ann Emerg Med 2005;45:4–12.
8. Hadley J, Steinberg EP, Feder J. Comparison ofuninsured and privately insured hospital patients.Condition on admission, resource use, andoutcome. JAMA 1991;265:374–9.
9. Wilper AP, Woolhandler S, Lasser KE,McCormick D, Bor DH, Himmelstein DU. Health

J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 0 , N O . 1 5 , 2 0 1 7 Acharya et al.A U G U S T 1 4 , 2 0 1 7 : 1 4 7 5 – 8 5 PCI-Associated Outcomes in Safety-Net Hospitals
1485
insurance and mortality in US adults. Am J PublicHealth 2009;99:2289–95.
10. Gaglia MA Jr., Torguson R, Xue Z, et al. Effectof insurance type on adverse cardiac events afterpercutaneous coronary intervention. Am J Cardiol2011;107:675–80.
11. Parikh PB, Gruberg L, Jeremias A, et al. Asso-ciation of health insurance status with presenta-tion and outcomes of coronary artery diseaseamong nonelderly adults undergoing percuta-neous coronary intervention. Am Heart J 2011;162:512–7.
12. Brindis RG, Fitzgerald S, Anderson HV,Shaw RE, Weintraub WS, Williams JF. The Amer-ican College of Cardiology-National CardiovascularData Registry (ACC-NCDR): building a nationalclinical data repository. J Am Coll Cardiol 2001;37:2240–5.
13. Anderson HV, Shaw RE, Brindis RG, et al.A contemporary overview of percutaneous coro-nary interventions. The American College ofCardiology-National Cardiovascular Data Registry(ACC-NCDR). J Am Coll Cardiol 2002;39:1096–103.
14. Andrews RM, Stull DE, Fraser I, Friedman B,Houchens RL. Serving the Uninsured: Safety-NetHospitals, 2003. HCUP Fact Book No. 8, AHRQPublication No. 07–0006. Rockville, MD: Agencyfor Healthcare Research and Quality, 2007.
15. Rao SV, McCoy LA, Spertus JA, Krone RJ,Singh M, Fitzgerald S, Peterson ED. An updatedbleeding model to predict the risk of post-procedure bleeding among patients undergoingpercutaneous coronary intervention: a report us-ing an expanded bleeding definition from theNational Cardiovascular Data Registry CathPCIRegistry. J Am Coll Cardiol Intv 2013;6:897–904.
16. Tsai TT, Patel UD, Chang TI, et al. Validatedcontemporary risk model of acute kidney injury inpatients undergoing percutaneous coronary in-terventions: insights from the National Cardio-vascular Data Registry Cath-PCI Registry. J AmHeart Assoc 2014;3:e001380.
17. Peterson ED, Dai D, DeLong ER, et al.Contemporary mortality risk prediction for percu-taneous coronary intervention: results from 588,398 procedures in the National CardiovascularData Registry. J Am Coll Cardiol 2010;55:1923–32.
18. Klein LW, Kolm P, Xu X, et al. A longitudinalassessment of coronary interventional programquality: a report from the American College ofCardiology-National Cardiovascular Data Registry.J Am Coll Cardiol Intv 2009;2:136–43.
19. Sada MJ, French WJ, Carlisle DM, Chandra NC,Gore JM, Rogers WJ. Influence of payor on use ofinvasive cardiac procedures and patient outcomeafter myocardial infarction in the United States.Participants in the National Registry of MyocardialInfarction. J Am Coll Cardiol 1998;31:1474–80.
20. Hannan EL, Racz M, Walford G, Clark LT,Holmes DR, King SB 3rd, Sharma S. Differences inutilization of drug-eluting stents by race andpayer. Am J Cardiol 2007;100:1192–8.
21. Kao J, Vicuna R, House JA, Rumsfeld JS,Ting HH, Spertus JA. Disparity in drug-elutingstent utilization by insurance type. Am Heart J2008;156:1133–40.
22. Gaglia MA Jr., Torguson R, Xue Z, et al. In-surance type influences the use of drug-elutingstents. J Am Coll Cardiol Intv 2010;3:773–9.
23. Amin AP, Spertus JA, Cohen DJ, et al. Use ofdrug-eluting stents as a function of predictedbenefit: clinical and economic implications of cur-rent practice. Arch Intern Med 2012;172:1145–52.
24. Smolderen KG, Spertus JA, Tang F, Oetgen W,Borden WB, Ting HH, Chan PS. Treatment differ-ences by health insurance among outpatients withcoronary artery disease: insights from the nationalcardiovascular data registry. J Am Coll Cardiol2013;61:1069–75.
25. Cram P, House JA, Messenger JC, Piana RN,Horwitz PA, Spertus JA. Percutaneous coronaryintervention outcomes in US hospitals with vary-ing structural characteristics: analysis of theNCDR. Am Heart J 2012;163:222–9.
26. US Census Bureau, current population reports.Health Insurance Coverage in the United States:2014. Washington, DC: US Government PrintingOffice, 2015.
27. Canto JG, Every NR, Magid DJ, et al. The vol-ume of primary angioplasty procedures and sur-vival after acute myocardial infarction. NationalRegistry of Myocardial Infarction 2 Investigators.N Engl J Med 2000;342:1573–80.
28. McGrath PD, Wennberg DE, Dickens JD Jr.,et al. Relation between operator and hospitalvolume and outcomes following percutaneouscoronary interventions in the era of the coronarystent. JAMA 2000;284:3139–44.
29. Magid DJ, Calonge BN, Rumsfeld JS, Canto JG,Frederick PD, Every NR, Barron HV, NationalRegistry of Myocardial Infarction 2 and 3 In-vestigators. Relation between hospital primaryangioplasty volume and mortality for patientswith acute MI treated with primary angioplasty vsthrombolytic therapy. JAMA 2000;284:3131–8.
30. Vakili BA, Kaplan R, Brown DL. Volume-outcome relation for physicians and hospitalsperforming angioplasty for acute myocardialinfarction in New York state. Circulation 2001;104:2171–6.
31. Epstein AJ, Rathore SS, Volpp KG,Krumholz HM. Hospital percutaneous coronaryintervention volume and patient mortality, 1998to 2000: does the evidence support current pro-cedure volume minimums? J Am Coll Cardiol2004;43:1755–62.
32. Hannan EL, Wu C, Walford G, et al. Volume-outcome relationships for percutaneous coronaryinterventions in the stent era. Circulation 2005;112:1171–9.
33. Kumbhani DJ, Cannon CP, Fonarow GC, et al.Association of hospital primary angioplasty vol-ume in ST-segment elevation myocardial infarc-tion with quality and outcomes. JAMA 2009;302:2207–13.
34. Khattab AA, Hamm CW, Senges J, et al.Sirolimus-eluting stent treatment at high-volumecenters confers lower mortality at 6-monthfollow-up: results from the prospective multi-center German Cypher Registry. Circulation 2009;120:600–6.
35. Srinivas VS, Hailpern SM, Koss E, Monrad ES,Alderman MH. Effect of physician volume on therelationship between hospital volume and mor-tality during primary angioplasty. J Am Coll Car-diol 2009;53:574–9.
36. Post PN, Kuijpers M, Ebels T, Zijlstra F.The relation between volume and outcomeof coronary interventions: a systematic reviewand meta-analysis. Eur Heart J 2010;31:1985–92.
37. Badheka AO, Patel NJ, Grover P, et al. Impactof annual operator and institutional volume onpercutaneous coronary intervention outcomes: a5-year United States experience (2005-2009).Circulation 2014;130:1392–406.
38. Health Insurance Coverage: Early Release ofEstimates From the National Health InterviewSurvey, January–March 2015. Available at: http://www.cdc.gov/nchs/nhis.htm. Accessed February12, 2016.
KEY WORDS outcomes, percutaneouscoronary intervention, safety-net hospital
APPENDIX For a supplemental appendix,please see the online version of this article.